")
Back to Journals » International Journal of General Medicine » Volume 14
Blood Levels of Glutamine and Nitrotyrosine in Patients with Chronic Viral Hepatitis
Authors Murad H , Tayeb H, Mosli M, Rafeeq M , Basheikh M
Received 6 September 2021
Accepted for publication 2 November 2021
Published 24 November 2021 Volume 2021:14 Pages 8753—8762
DOI https://doi.org/10.2147/IJGM.S337909
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Hussam Murad,1,2 Haythum Tayeb,3 Mahmoud Mosli,4 Misbahuddin Rafeeq,1 Mohammed Basheikh5
1Department of Pharmacology, Faculty of Medicine, Rabigh, King Abdulaziz University, Jeddah, Saudi Arabia; 2Department of Pharmacology, Faculty of Medicine, Ain Shams University, Cairo, Egypt; 3Department of Medicine, Division of Neurology, Faculty of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia; 4Department of Medicine, Division of Gastroenterology, Faculty of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia; 5Department of Medicine, Faculty of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia
Correspondence: Hussam Murad Tel + 966541541341
Fax + 966024223031
Email [email protected]; [email protected]
Purpose: Oxidative stress is involved in pathogenesis of chronic viral hepatitis. Glutamine is an antioxidant, but there is a controversy about its risk-benefits. Nitrotyrosine is an oxidative stress marker. This observational cross-sectional study was designed to compare blood levels of glutamine and nitrotyrosine in treated versus untreated chronic viral hepatitis patients.
Patients and Methods: Five groups (n = 250) were included: hepatitis B untreated (HBV), hepatitis C untreated (HCV), HBV treated (HBVT), and HCV treated (HCVT) groups plus a normal control group. Liver function tests and blood levels of glutamine, nitrotyrosine, viral loads, and HBsAg were measured.
Results: Blood levels of glutamine and nitrotyrosine in all patient groups significantly increased compared with normal controls with non-significant differences in-between. Both tests showed significant large correlations with HBV-DNA or HCV-RNA test positivity, high accuracies, and cutoff scores with high sensitivities and specificities. The viral loads and HBsAg levels were significantly lower in treated versus untreated groups. However, they poorly correlated with levels of glutamine and nitrotyrosine in all patient groups.
Conclusion: Blood levels of glutamine and nitrotyrosine significantly increased in treated and untreated chronic viral hepatitis B and C patients compared with normal controls. Both tests showed high accuracies and cutoff scores with high sensitivities and specificities. However, they did not differ significantly in treated versus untreated patients. To our knowledge, this is the first data showing elevation of glutamine and nitrotyrosine in treated and untreated chronic viral hepatitis. A prospective longitudinal study with repeated measurements of glutamine and nitrotyrosine is recommended to verify if they can predict response to treatment. Study of other oxidative stress markers is also advised to clarify if the elevated nitrotyrosine could be an oxidative stress marker in these patients, and whether the increased glutamine could act as an antioxidant or as a predictive agent for deleterious consequences.
Keywords: glutaminolysis, nitrotyrosination, oxidant stress
Introduction
In liver diseases, it seems that glutamine and nitrotyrosine play important roles as biomarkers or as contributors to manifestations. In viral hepatitis, liver injury is caused by immune-related mechanisms. While the virus-specific T cells and the nonspecific cells give to injury, the regulatory T cells and myeloid-derived suppressor cells control it.1 The oxidative stress is a possible mechanism in pathogenesis of chronic viral hepatitis.2 Glutamine is the most plentiful amino acid in the body, and it is an important fuel for the immune system cells. Since glutamine is a precursor of glutathione, it has beneficial anti-inflammatory and antioxidant properties and its addition in the clinical diet can help avoid damage due to oxidative stress.3 In streptozotocin-induced diabetic rats, glutamine supplementation increased antioxidant capacity, normalized antioxidant enzyme activities, and decreased renal nitrotyrosine level.4 Glutamine is included in clinical nutrition supplementation protocols, and it is recommended for immunosuppressed patients. However, based on its recently detected harmful effects, it is difficult to determine whether all individuals will benefit from it.5 It was suggested that high glutamine levels are related to elevated ammonia concentrations and possible occurrence of hepatic encephalopathy.6 Brain ammonia is metabolized to glutamine in astrocytes in hepatic encephalopathy due to a severe liver disease. Glutamine is then transported into mitochondria and hydrolyzed to ammonia causing activation of the mitochondrial permeability transition and oxidative stress. Therefore, targeting mitochondrial transport or hydrolysis of astrocytic glutamine seems to be an effective method for treatment of hepatic encephalopathy.7 Moreover, liver failure may be associated with a high plasma glutamine level which could be regarded as a biomarker or as a contributor to its manifestations.8 Surprisingly, a low blood level of glutamine is found in about 30% of ICU admission, and it was found to be an independent predictor for mortality.9 Nitric oxide is thought to react with superoxide yielding peroxynitrite; a potent oxidant; which oxidizes tyrosine to 3-nitrotyrosine within cells and tissue lesions. It was found that intrahepatic accumulation of nitrotyrosine; resulting from nitration of tyrosine residues by reactive peroxynitrite species; is markedly increased in the inflamed hepatic tissue in chronic viral hepatitis and it appeared to be related to severity of the histological changes.10 The 3-nitrotyrosine is a marker for oxidative stress in different chronic and degenerative diseases because oxidation of tyrosine to 3-nitrotyrosine is irreversible. Effective detoxification of the 3-nitrotyrosine bound to proteins decreases protein oxidation damage in such disorders.11 In addition, nitrotyrosine is considered a biomarker of nitrogen free radical species modified proteins.12 The antioxidant therapy is not always effective as add-on treatment for hepatitis because antioxidants; if not used at the right setting and dosing schedule; they can become pro-oxidants.13 Taken together, the current study was designed to compare blood levels of glutamine and nitrotyrosine in treated versus untreated chronic viral hepatitis patients.
Materials and Methods
Study Design and Participants
This observational cross-sectional study was approved by the King Abdulaziz University (KAU)-Research Ethics Committee (approval number: 609-18) and was performed in accordance with the Helsinki Declaration. The chronic hepatitis patients were randomly recruited from Gastroenterology and Hepatology Department, King Abdulaziz University (KAU) Hospital between January 2018 and December 2020. Four groups of patients (n = 250) were included: hepatitis B untreated group (HBV), hepatitis C untreated group (HCV), HBV treated (HBVT) group, and HCV treated (HCVT) group. The diagnosis of HBV was based on positive HBsAg and HBV DNA testing while that of HCV was based on positive HCV antibodies and HCV RNA testing in addition to elevation of aminotransferases (above the reference range which is 15–37 U/L for AST and 12–78 U/L for ALT).14 Normal control subjects of comparable age and sex (NC) were randomly recruited from those who visit KAU Hospital for routine medical checkups. Written informed consents were taken from all participants. The exclusion of subjects from the study was built on the history, clinical picture, and investigations. The exclusion criteria included patients with liver cirrhosis (APRI score; AST/platelet ratio index; of ≤0.3),15 combined hepatitis B/C infection, and hepatitis B/D co-infection. Others included uncontrolled diabetes (fasting blood glucose level of ≥126 mg/dL, random blood glucose level of ≥200 mg/dL, or Hb A1C level of ≥6.5%), severe renal dysfunction (creatinine clearance 15 – <30 mL/min.), and subjects with metabolic disorders such as those affecting amino acid metabolism and mitochondrial diseases. After overnight fasting blood was taken and serum was separated and stored at –80°C till analyzed. The following measurements were done:
Assay of Liver Functions, HV Serology, HBV DNA, and HCV RNA
The liver function tests including levels of total protein (TP), albumin, alkaline phosphatase (ALP), aspartate aminotransferase (AST), alanine aminotransferase (ALT), γ-glutamyl transferase (GGT), and total bilirubin (TB) were measured using the commercially available kits (MyBioSource, Inc. CA, USA). The HV serology markers were measured by the chemiluminescent microparticle immunoassay method (Abbott Diagnostics, IL, USA) and serum levels of HBV DNA and HCV RNA were measured by the real-time PCR kits (Roche Diagnostics, IN, USA) according to the manufacturer’s protocols.
Assay of Glutamine (GLN)
It was done using an ELISA kit (Aviva Systems Biology Corp., CA, USA). Briefly, the plate is coated with human GLN antibody which binds GLN in the sample or the standard. Then, GLN is bound by biotinylated human GLN antibody which will be bound by streptavidin-HRP. After incubation, the unbound streptavidin-HRP is removed by washing. Substrate is added and color develops in proportion to the concentration of GLN. Stop solution is added to end the reaction and absorbance is measured at 450 nm.
Assay of Nitrotyrosine (NT)
It was done using an ELISA kit (Abcam Comp., Cambridge, UK). Briefly, a method based on the Biotin double antibody sandwich technique was used. The wells are pre-coated with NT monoclonal antibody which binds NT in the sample or the standard. After incubation, NT antibodies labeled with biotin are added to bind NT. Then, streptavidin-HRP is added to bind to the biotinylated NT antibody. Unbound enzymes are removed by washing. Substrate is then added, and color occurs in proportion to NT concentration. The reaction is stopped by addition of the acidic solution and absorbance is measured at 450 nm.16
Statistical Analysis
The SPSS version 22 (SPSS Inc., IL, USA) was used. Data was given as mean values ± SEM. The ANOVA with Tukey’s test was used for multiple comparisons. To calculate a cost-effective sample size, we set the significance level at P < 0.05 and used a statistical power of 80% which is widely used to avoid false-negative associations. The effect size and standard deviation were obtained from scientific literature. The glutamine or nitrotyrosine levels were examined by age, gender, and liver function tests through a linear regression analysis. Pearson correlation was used to detect correlations between viral loads and HBsAG and glutamine or nitrotyrosine levels of hepatitis patients. Moreover, Spearman correlation was used to detect correlations between glutamine and nitrotyrosine levels of normal subjects or hepatitis patients and the standard diagnostic tests for hepatitis. The sensitivity, specificity, and cutoff concentrations were calculated through generation of the receiver operating characteristic (ROC) curve. The area under the ROC curve (AUROC) was calculated as a measure of test performance. Discriminant analysis was done to detect ability of glutamine or nitrotyrosine tests to correctly classify the patients from normal subjects.
Results
Participants
The participants’ demographic characteristics and the liver function tests are shown in Table 1. There were significant reductions in liver function tests in the treated groups versus the untreated ones.
 |
Table 1 Participants’ Demographic Data and Liver Function Tests of NC, HBV, HBV-Treated (HBVT), HCV, and HCV-Treated (HCVT) Groups (n = 250) |
Levels of GLN and NT in HBV, HBVT, HCV, and HCVT Patients
As shown in Table 2, the linear regression analysis between age, gender, and liver function tests as predictor variables and blood GLN or NT levels as dependent variables showed small non-significant values of the coefficient of determination (R2) in untreated and treated chronic HB and HC groups indicating absent or poor correlation. Table 3 shows that the levels of GLN and NT in untreated and treated chronic HB and HC groups increased significantly from their levels of the NC group with non-significant differences in-between. In addition, as shown in Table 4, for chronic hepatitis B untreated and treated patients, Spearman Correlation showed that there were significant large correlations between GLN and NT concentrations and the HBV DNA test positivity. Moreover, the ROC curves (Figure 1) showed that the AUROC for both GLN and NT were more than 0.9 with significant P values, and high sensitivity and specificity values. In addition, the discriminant analysis showed that GLN and NT assays were able to identify HBV patients from NC with eigenvalues more than 1.0 and canonical correlations above 0.7. The sensitivity and specificity values for GLN and NT tests were equal to the values calculated from the ROC curves. The percentage of correctly classified cases of each of the original and cross-validated grouped cases for GLN and NT tests respectively were 95.2% and 88.8% in HBV patients and 96.2% and 86.6% in HBVT patients. In chronic hepatitis C untreated and treated patients, Spearman correlation, the ROC curves (Figure 2), and the discriminant analysis with HCV RNA test positivity showed similar results to those with hepatitis B except that the eigenvalue for NT in HCV group was 0.994. The percentage of correctly classified cases of each of the original and cross-validated grouped cases for GLN and NT tests respectively were (87% and 86.6%) and 83.8% in HCV patients and 93.4% and 87.8% in HCVT patients.
 |
Table 2 Coefficient of Determination (R2) Values of Linear Regression Analysis between Demographic Data and Liver Function Tests as Predictor Variables and Blood Glutamine (GLN) or Nitrotyrosine (NT) Levels (ng/mL) as Dependent Variables in HBV, HBV-Treated (HBVT), HCV, and HCV-Treated (HCVT) Groups (n = 250) |
 |
Table 3 Levels of Glutamine and Nitrotyrosine (ng/mL) in NC, HBV, HBV-Treated (HBVT), HCV, and HCV-Treated (HCVT) Groups (n = 250) |
 |
Table 4 Values of Spearman Correlation Coefficient (Rho), Area Under Receiver Operating Characteristic (AUROC) Curve, Cutoff, Sensitivity (%), Specificity (%), Eigenvalue, and Canonical Correlations between Glutamine (GLN) and Nitrotyrosine (NT) Levels and the HBV DNA Test Positivity in HBV and HBV-Treated (HBVT), and HCV RNA Test Positivity in HCV and and HCV-Treated (HCVT) Groups (n = 250) |
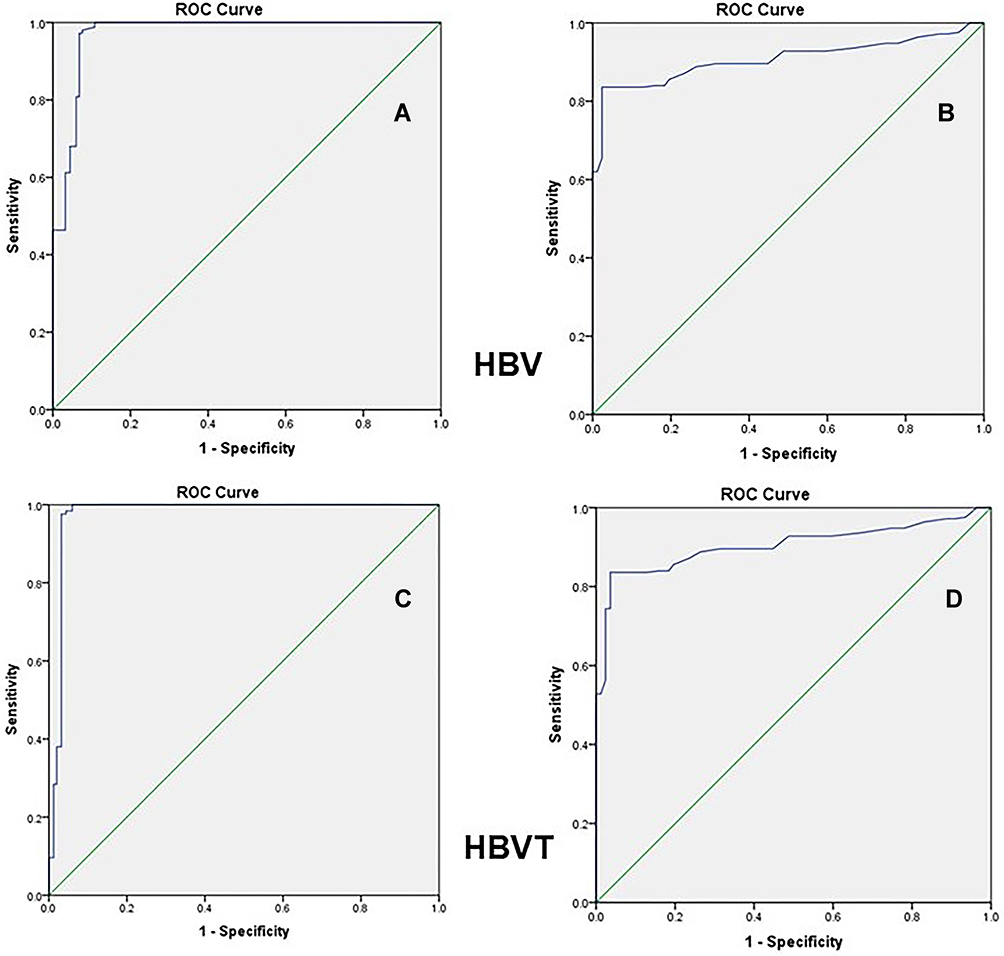 |
Figure 1 The receiver operating characteristic (ROC) curve for glutamine (GLN) and nitrotyrosine (NT) detection of HBV infection according to positive DNA testing in the patient groups: (A) GLU-HBV, (B) NT-HBV, (C) GLU-HBVT, and (D) NT-HBVT. |
 |
Figure 2 The receiver operating characteristic (ROC) curve for glutamine (GLN) and nitrotyrosine (NT) detection of HCV infection according to positive RNA testing in the patient groups: (A) GLU-HCV, (B) NT-HCV, (C) GLU-HCVT, and (D) NT-HCVT. |
Relation Between Viral Loads and GLN and NT in HBV, HBVT, HCV, and HCVT Patients
The viral load levels significantly decreased in the treated versus untreated group. The Pearson correlation between the viral loads and GLN or NT levels showed small non-significant correlation coefficients (r) indicating absent or poor correlation (Table 5).
 |
Table 5 Correlation Coefficient (r) Values of Pearson Correlation Analysis between Viral Load (VL, KIU/mL) and GLN or NT Levels (ng/mL) in HBV, HBV-Treated (HBVT), HCV, and HCV-Treated (HCVT) Groups (n = 250) |
Relation Between HBsAg Level and GLN and NT in HBV and HBVT Patients
The HBsAg levels significantly decreased in HBVT versus HBV group. The Pearson correlation between the HBsAg and GLN or NT levels showed small non-significant correlation coefficients (r) indicating absent or poor correlation (Table 6).
 |
Table 6 Correlation Coefficient (r) Values of Pearson Correlation Analysis between HBsAg Levels (Log10 IU/mL) and GLN or NT Levels (ng/mL) in HBV and HBV-Treated (HBVT) Groups (n = 250) |
Discussion
The sensitivity and specificity of a diagnostic test are used to evaluate its performance in the case of a binary predictor. However, in cases where the predictors are measured on a continuous or ordinal scale, it is appropriate to assess the test performance over the range of possible cut points for the predictor variable using the receiver operating characteristic (ROC) curve.17 In the current study, the ROC analysis showed high overall accuracy of both GLN and NT tests. The area under the ROC curves (AUROCs) were outstanding indicating ability of each test to discriminate diseased cases from normal subjects. Both GLN and NT tests showed cutoffs scores with high sensitivity and specificity, and 83.8–96.2% of the cases in the different groups were correctly classified which is pretty good. The eigenvalues were more than one (except for NT in HCV group which was nearly one) indicating presence of many reliable components according to Kaiser rule.18 The canonical correlation values are considered quite high for the effect size.19
Blood glutamine levels were found elevated in acute and chronic hepatitis, liver cirrhosis, and hepatocellular carcinoma20. Oxidative stress, induced by hepatitis viruses, is one of the triggers of the hepatocellular carcinoma (HCC) associated with chronic hepatitis.21 The hepatitis virus (HV) induces glutaminolysis to help viral replication, but this predisposes the cells to cancer transformation. Thus, targeting glutaminolytic enzymes could be an interesting preventive measure against HV-hepatocellular carcinoma (HCC).22,23 Certain biomarkers for HCV-HCC have been identified in cancerous tissues of HCV-infected patients such as increased expression and phosphorylation of liver glutamine synthetase.24 Also, in chronic hepatitis B patients, the expression level of glutamine synthetase was found elevated in serum and hepatic tissue.25 Moreover, hepatitis C patients; who received treatment with pegylated IFN-α; were found to have increased levels of cortical glutamine.26 There is a wide controversy about risk-benefits of glutamine.27 Glutamine has a useful effect on infectious complications and can decrease hospital stay.28 Both low and high plasma glutamine concentrations were found to be risk factors for mortality in critically ill patients like those with fulminant hepatitis. The mortality rates with plasma glutamine less than 400 nmol/mL or more than 700 nmol/mL were found to be significantly higher than with levels of 400–700 nmol/mL.29 Elevated blood levels of glutamine are occasionally seen in acute and chronic liver failure where they significantly correlated with severity and may be predictive for negative outcomes in critically ill patients.8 Moreover, a high level of glutamine contributed to brain edema and was directly involved in pathogenesis of hepatic encephalopathy.30 In addition, targeting both glutaminase and the glutamine transporter ASCT2 could be a new treatment approach for glutamine addicted liver cancers.31 On the other hand, in rats with ischemia/reperfusion injury of the intestine, administration of glutamine reduced nitrotyrosine formation.32 Also, in portal hypertension gastropathy, glutamine administration markedly improved oxidative/nitrosative stress and decreased the formation of nitric oxide and peroxynitrite.33
Nitrotyrosine is a biomarker of nitrogen free radical species modified proteins and measurement of 3-nitrotyrosine could be a promising biomarker of oxidative stress for major neurological diseases.34 Serum nitrotyrosine was reported to be significantly high in patients with chronic hepatitis B.12 Also, intrahepatic elevation of nitrotyrosine was shown in viral hepatic diseases but not in non-viral diseases.10 In a controlled clinical trial, determination of serum 3-nitrotyrosine was found useful to identify patients with minimal hepatic encephalopathy with good sensitivity, specificity, and positive and negative predictive values.16 In patients with primary biliary cirrhosis and autoimmune hepatitis, expression of intrahepatic inducible nitric oxide synthase was enhanced and the accumulation of nitrotyrosine was related to the severity of liver damage.35 In contrast to our results, there was no statistically significant difference of nitrotyrosine levels between untreated chronic viral hepatitis patients and the controls. And no significant correlations were detected between the levels of malondialdehyde, myeloperoxidase, and nitrotyrosine (as markers of oxidative stress) and the viral load, necro-inflammation, or fibrosis of the liver.14 A possible explanation of these contradictory results is that there is an increase of hepatic nitric oxide in cases of viral liver diseases, however this might not always be shown in blood.13
In the current study, the viral loads and HBsAg level were significantly lower in the treated versus untreated groups confirming their importance as predictors of treatment outcome. Quantitation of HBsAg is an increasingly popular method to predict response to treatment in CHB patients and the HbsAg level at six months post-treatment significantly differed from the baseline HbsAg level.36 In patients with chronic hepatitis B, the DNA load predicts response of treatment.37 Similarly, in hepatitis C patients, the RNA load predicts response of treatment and low levels of quantifiable HCV RNA at end of treatment do not exclude treatment success.38 The current study showed poor correlations between the viral loads or HBsAg level and blood GLN or NT levels in the untreated and treated HV groups. However, these findings need to be evaluated in a prospective longitudinal study with repeated measurements of these parameters over time to detect if they can predict response to treatment.
Limitations of the current study included that blood levels of GLN and NT were not tested as markers for liver fibrosis and/or liver disease within HBV or HCV infected individuals. Also, other markers of oxidative stress were not evaluated. In addition, due to the cross-sectional design of the study, the levels of GLN and NT were measured only once and there was no follow-up of participants to detect if these parameters can predict response to treatment over time.
Conclusion
The blood levels of glutamine and nitrotyrosine significantly increased in untreated and treated chronic viral hepatitis B and C patients compared with normal controls. Both glutamine and nitrotyrosine tests showed high accuracy and cutoff scores with high sensitivity and specificity. They were able to discriminate treated and untreated cases from normal controls; however, they did not differ significantly in treated versus untreated patients. This may be attributed to the cross-sectional nature of our study. To our knowledge, this is the first study demonstrating elevation of glutamine and nitrotyrosine in untreated and treated chronic viral hepatitis. A prospective longitudinal study with repeated measurements of glutamine and nitrotyrosine at different time points is recommended because it could help detect if they can predict response to treatment. Study of other markers of oxidative stress is also recommended to determine if the elevated nitrotyrosine could be a marker of oxidative stress in these patients, and to clarify whether the increased glutamine could act as an antioxidant or as a predictive agent for deleterious consequences.
Abbreviations
HBV, hepatitis B viral infection; HBVT, hepatitis B viral infection treated; HCV, hepatitis C viral infection; HCVT, hepatitis C viral infection treated; NC, normal control; GLN, glutamine; NT, nitrotyrosine; AST, aspartate transaminase; ALT, alanine transaminase; TP, total protein; ALP, alkaline phosphatase; AST, aspartate aminotransferase; ALT, alanine aminotransferase; GGT, γ-glutamyl transferase; TB, total bilirubin; ROC, receiver operating characteristic curve; AUROC, area under ROC curve.
Data Sharing Statement
Data supporting the results reported in the manuscript can be obtained from the corresponding author on a reasonable request.
Acknowledgments
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Shin EC, Sung PS, Park SH. Immune responses and immunopathology in acute and chronic viral hepatitis. Nat Rev Immunol. 2016;16(8):509–523. doi:10.1038/nri.2016.69
2. Yadav D, Hertan HI, Schweitzer P, Norkus E, Pitchumoni C. Serum and liver micronutrient antioxidants and serum oxidative stress in patients with chronic hepatitis C. Am J Gastroenterol. 2002;97(10):2634–2639. doi:10.1111/j.1572-0241.2002.06041.x
3. Amores-Sánchez MI, Medina MÁ. Glutamine, as a precursor of glutathione, and oxidative stress. Mol Genet Metab. 1999;67(2):100–105. doi:10.1006/mgme.1999.2857
4. Tsai PH, Liu JJ, Yeh CL, Chiu WC, Yeh SL. Effects of glutamine supplementation on oxidative stress-related gene expression and antioxidant properties in rats with streptozotocin-induced type 2 diabetes. Br J Nutr. 2012;107(8):1112–1118. doi:10.1017/S0007114511004168
5. Cruzat V, Macedo Rogero M, Noel Keane K, Curi R, Newsholme P. Glutamine: metabolism and immune function, supplementation and clinical translation. Nutrients. 2018;10(11):1564. doi:10.3390/nu10111564
6. Rao KVR, Jayakumar AR, Norenberg MD. Glutamine in the pathogenesis of acute hepatic encephalopathy. Neurochem Int. 2012;61(4):575–580. doi:10.1016/j.neuint.2012.01.012
7. Rama Rao KV, Norenberg MD. Glutamine in the pathogenesis of hepatic encephalopathy: the trojan horse hypothesis revisited. Neurochem Res. 2014;39(3):593–598. doi:10.1007/s11064-012-0955-2
8. Helling G, Wahlin S, Smedberg M, et al. Plasma glutamine concentrations in liver failure. PLoS One. 2016;11(3):e0150440. doi:10.1371/journal.pone.0150440
9. Rodas PC, Rooyackers O, Hebert C, Norberg Å, Wernerman J. Glutamine and glutathione at ICU admission in relation to outcome. Clin Sci. 2012;122(12):591–597. doi:10.1042/CS20110520
10. García-Monzón C, Majano PL, Zubia I, Sanz P, Apolinario A, Moreno-Otero R. Intrahepatic accumulation of nitrotyrosine in chronic viral hepatitis is associated with histological severity of liver disease. J Hepatol. 2000;32(2):331–338. doi:10.1016/S0168-8278(00)80080-X
11. Calderón‑Torres CM, Sarabia‑Curz L, Ledesma‑Soto Y, Murguía‑Romero M, Terrazas LI. Denitrase activity of Debaryomyces hansenii reduces the oxidized compound 3‑nitrotyrosine in mice liver with colitis. Exp Ther Med. 2019;17(5):3748–3754.
12. Meng L, Gao A, Bian J, Han L, Chen H. Study on correlation between oxidation-antioxidation and chronic hepatitis viral B. Occup Health. 2010;23. Available from: https://en.cnki.com.cn/Article_en/CJFDTotal-ZYJK201023095.htm.
13. Alavian SM, Showraki A. Hepatitis B and its relationship with oxidative stress. Hepat Mon. 2016;16(9):e37973. doi:10.5812/hepatmon.37973
14. Namiduru ES, Namiduru M, Tarakçioğlu M, Tanriverdi M. Levels of malondialdehyde, myeloperoxidase and nitrotyrosine in patients with chronic viral hepatitis B and C. Adv Clin Exp Med. 2012;21(1):47–53.
15. De Matteis C, Cariello M, Graziano G, et al. AST to Platelet Ratio Index (APRI) is an easy-to-use predictor score for cardiovascular risk in metabolic subjects. Sci Rep. 2021;11(1):14834. doi:10.1038/s41598-021-94277-3
16. Montoliu C, Cauli O, Urios A, et al. 3-nitro-tyrosine as a peripheral biomarker of minimal hepatic encephalopathy in patients with liver cirrhosis. Am J Gastroenterol. 2011;106(9):1629. doi:10.1038/ajg.2011.123
17. Mandrekar JN. Receiver operating characteristic curve in diagnostic test assessment. J Thorac Oncol. 2010;5(9):1315–1316. doi:10.1097/JTO.0b013e3181ec173d
18. Kanyongo GY. The influence of reliability on four rules for determining the number of components to retain. J Mod Appl Stat Methods. 2005;5(2):7. doi:10.22237/jmasm/1162353960
19. Leach LF, Henson RK. Bias and precision of the squared canonical correlation coefficient under nonnormal data condition. J Mod Appl Stat Methods. 2014;13(1):8. doi:10.22237/jmasm/1398917220
20. Tominaga T, Suzuki H, Mizuno H, et al. Clinical significance of measuring plasma concentrations of glutamine and glutamate in alcoholic liver diseases. Alcohol Alcohol. 1993;28(Supplement_1A):103–109. doi:10.1093/alcalc/28.Supplement_1A.103
21. Ivanov AV, Valuev-Elliston VT, Tyurina DA, et al. Oxidative stress, a trigger of hepatitis C and B virus-induced liver carcinogenesis. Oncotarget. 2017;8(3):3895–3932. doi:10.18632/oncotarget.13904
22. Lévy PL, Duponchel S, Eischeid H, et al. Hepatitis C virus infection triggers a tumor-like glutamine metabolism. Hepatology. 2017;65(3):789–803. doi:10.1002/hep.28949
23. Bard-Chapeau EA, Nguyen AT, Rust AG, et al. Transposon mutagenesis identifies genes driving hepatocellular carcinoma in a chronic hepatitis B mouse model. Nat Genet. 2014;46(1):24–32. doi:10.1038/ng.2847
24. Kuramitsu Y, Harada T, Takashima M, et al. Increased expression and phosphorylation of liver glutamine synthetase in well-differentiated hepatocellular carcinoma tissues from patients infected with hepatitis C virus. Electrophoresis. 2006;27(8):1651–1658. doi:10.1002/elps.200500718
25. Long J, Wang H, Lang Z, Wang T, Long M, Wang B. Expression level of glutamine synthetase is increased in hepatocellular carcinoma and liver tissue with cirrhosis and chronic hepatitis B. Hepatol Int. 2011;5(2):698–706. doi:10.1007/s12072-010-9230-2
26. Taylor MJ, Godlewska B, Near J, et al. Effect of interferon-α on cortical glutamate in patients with hepatitis C: a proton magnetic resonance spectroscopy study. Psychol Med. 2014;44(4):789–795. doi:10.1017/S0033291713001062
27. Smedberg M, Wernerman J. Is the glutamine story over? Crit Care. 2016;20(1):361. doi:10.1186/s13054-016-1531-y
28. Melis GC, Ter Wengel N, Boelens PG, van Leeuwen PA. Glutamine: recent developments in research on the clinical significance of glutamine. Curr Opin Clin Nutr Metab Care. 2004;7(1):59–70. doi:10.1097/00075197-200401000-00011
29. Tsujimoto T, Shimizu K, Hata N, et al. Both high and low plasma glutamine levels predict mortality in critically ill patients. Surg Today. 2017;47(11):1331–1338. doi:10.1007/s00595-017-1511-0
30. Lemberg A, Fernández MA. Hepatic encephalopathy, ammonia, glutamate, glutamine and oxidative stress. Ann Hepatol. 2009;8(2):95–102. doi:10.1016/S1665-2681(19)31785-5
31. Jin H, Wang S, Zaal EA, et al. A powerful drug combination strategy targeting glutamine addiction for the treatment of human liver cancer. eLife. 2020;9. doi:10.7554/eLife.56749
32. Mondello S, Galuppo M, Mazzon E, et al. Glutamine treatment attenuates the development of ischaemia/reperfusion injury of the gut. Eur J Pharmacol. 2010;643(2–3):304–315. doi:10.1016/j.ejphar.2010.06.044
33. Marques C, Licks F, Zattoni I, et al. Antioxidant properties of glutamine and its role in VEGF-Akt pathways in portal hypertension gastropathy. World J Gastroenterol. 2013;19(28):4464–4474. doi:10.3748/wjg.v19.i28.4464
34. Bandookwala M, Sengupta P. 3-Nitrotyrosine: a versatile oxidative stress biomarker for major neurodegenerative diseases. Int J Neurosci. 2020;130(10):1047–1062. doi:10.1080/00207454.2020.1713776
35. Sanz-Cameno P, Medina J, García-Buey L, et al. Enhanced intrahepatic inducible nitric oxide synthase expression and nitrotyrosine accumulation in primary biliary cirrhosis and autoimmune hepatitis. J Hepatol. 2002;37(6):723–729. doi:10.1016/S0168-8278(02)00266-0
36. Kim JH, Moon HW, Ko SY, Choe WH, Kwon SY. Hepatitis B surface antigen levels at 6 months after treatment can predict the efficacy of lamivudine-Adefovir combination therapy in patients with lamivudine-resistant chronic hepatitis B. Clin Mol Hepatol. 2014;20(3):274–282. doi:10.3350/cmh.2014.20.3.274
37. Fu XY, Tan DM, Liu CM, et al. Early hepatitis B viral DNA clearance predicts treatment response at week 96. World J Gastroenterol. 2017;23(16):2978–2986. doi:10.3748/wjg.v23.i16.2978
38. Sidharthan S, Kohli A, Sims Z, et al. Utility of hepatitis C viral load monitoring on direct-acting antiviral therapy. Clin Infect Dis. 2015;60(12):1743–1751. doi:10.1093/cid/civ170
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.