")
Back to Journals » International Journal of General Medicine » Volume 16
Blood Culture Negative Endocarditis: A Review of Laboratory Diagnostic Approaches
Authors Lin KP, Yeh TK , Chuang YC , Wang LA, Fu YC, Liu PY
Received 18 October 2022
Accepted for publication 12 January 2023
Published 24 January 2023 Volume 2023:16 Pages 317—327
DOI https://doi.org/10.2147/IJGM.S393329
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Kuan-Pei Lin,1 Ting-Kuang Yeh,1,2 Yu-Chuan Chuang,1 Li-An Wang,1 Yun-Ching Fu,3,4,* Po-Yu Liu1,4– 6,*
1Division of Infectious Diseases, Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, Taiwan; 2Genomic Center for Infectious Diseases, Taichung Veterans General Hospital, Taichung, Taiwan; 3Children’s Medical Center, Taichung Veterans General Hospital, Taichung, Taiwan; 4Department of Post-Baccalaureate Medicine, College of Medicine, National Chung Hsing University, Taichung, Taiwan; 5Ph.D. Program in Translational Medicine, National Chung Hsing University, Taichung, Taiwan; 6Rong Hsing Research Center for Translational Medicine, National Chung Hsing University, Taichung, Taiwan
*These authors contributed equally to this work
Correspondence: Yun-Ching Fu; Po-Yu Liu, Taichung Veterans General Hospital, No. 1650, Section 4, Taiwan Blvd, Xitun District, Taichung City, 40705, Taiwan, Tel +886-4-2359-2525 ext.3110, Fax +886-4-2359-5046, Email [email protected]; [email protected]
Abstract: Infective endocarditis is a potentially fatal condition, and identifying the pathogen is crucial to optimizing antibiotic treatment. While a blood culture takes time and may yield negative results, it remains the gold standard for diagnosis, blood culture-negative endocarditis, which accounts for up to 20% of infective endocarditis cases, poses a clinical challenge with increasing mortality. To better understand the etiology of blood culture-negative infective endocarditis, we reviewed non-culture-based strategies and compared the results. Serology tests work best in limited pathogens, such as Coxiella burnetii and Bartonella infections. Most of the pathogens identified by broad-range PCR tests are Streptococcus spp, Staphylococcus spp and Propionibacterium spp. adding specific real-time PCR assays to the systematic PCR testing of patients with blood culture-negative endocarditis will increase the efficiency of diagnosis. Recently, metagenomic next-generation sequencing has also shown promising results.
Keywords: endocarditis, diagnosis, serology, PCR, metagenomic sequencing, Streptococcus
Introduction
Infectious endocarditis is one of the most serious and potentially fatal diseases. For the diagnosis of infectious endocarditis, the cornerstone method currently involves culture-based techniques. However, blood culture-negative endocarditis, which constitutes up to 20% of all infective endocarditis cases, poses a significant clinical challenge.1,2 Therefore, a lot of efforts have been made to develop non-culture-based diagnostics.3,4 It is critical to identify the specific underlying microbial etiology in blood culture-negative endocarditis in order to refine the regimen of empirical antibiotics.5
Haemophilus aphrophilus, Aggregatibacter actinomycetemcomitans, Cardiobacterium hominis, Eikenella corrodens, and Kingella kingae, known collectively as the HACEK group, were historically the most prevalent pathogens in blood culture-negative endocarditis; however, modern blood culture can identify the aforementioned organism in at least five days of incubation.6,7 Blood culture-negative endocarditis is now more commonly caused by fastidious, slow-growing bacteria, particularly Coxiella burnetii, Bartonella species, and other nonculturable organisms. The most common causes of culture-negative endocarditis are unculturable microorganisms and previous administration of antimicrobial agents is also a cause of blood culture endocarditis.8
The diagnosis of blood culture-negative endocarditis is frequently delayed, increasing the risk of morbidity and mortality. It has been noted that in culture-negative endocarditis patients, long-term mortality is higher than in culture-positive endocarditis patients. An ancillary analysis study of 3113 infective endocarditis cases found that in the culture-negative groups receiving antimicrobial therapy only, the 30-day mortality was significantly higher in culture-negative endocarditis group compared with the culture-positive endocarditis group, 14.9% and 10.2%, respectively. Furthermore, heart failure and heart murmur were observed more in culture-negative endocarditis patients.9
The prevalence of infective endocarditis is 5 to 14.3 per 100,000 adults per year and is increasing over time. This increase is mainly due to age-related degenerative valvular disease and the increased need for cardiac devices and invasive procedures including hemodialysis for end-stage renal failure.10,11 In a retrospective cohort study, with a total of 405 patients with definite infective endocarditis, showed patients older than 65 years old had more predisposing factors including previous cardiac surgery history and degenerative heart disease compared with younger patients.12 In the past 20 years, with the development of techniques, the etiology of infective endocarditis has changed due to an increase in cardiac device implantation and prosthetic valve proportion.13 Therefore, it is important to improve the accuracy and effectiveness of diagnosis and reduce the mortality rate of endocarditis patients.
Metagenomic next-generation sequencing (mNGS) is currently a powerful method to sequence and identify nucleic acids from a mixed population of microorganisms. Compared to the conventional approach, mNGS has high efficiency and accuracy. It is expected to become a crucial clinical diagnostic tool in the future.14,15 Traditional methods including histology, serology, and culture have been used for decades to diagnose infective endocarditis. Molecular techniques have also been developed to improve the detection of difficult-to-culture agents. Due to existing high mortality of blood culture-negative endocarditis, mNGS has had its role since 2003, and has rapidly evolved over the past 20 years. It is evident that additional diagnostic tools and strategies are necessary. In this paper, we reviewed the tools currently used and the associated approaches in the diagnosis of blood culture-negative endocarditis.
Methods
We searched the English-language medical literature using PubMed/MEDLINE from 1980 to 2022 using the following keywords: blood culture negative, infective endocarditis, diagnostic tool, next-generation sequencing. The references of articles found using this search were also reviewed to identify other potential studies that were not located using the search terms. Studies reporting the method being used to detect of blood culture negative endocarditis were reviewed. Studies that provided data on the microorganism being detected in the blood culture negative endocarditis and the proportion of different tool revealed by trials were also included. Exclusion criteria included studies that only documented a single diagnostic tool to evaluate blood culture negative endocarditis; In total, 18 studies were reviewed in full. Other 9 articles involved in this study were identified while reviewing the similar articles in above mentioned papers.
Non-Culture-Based Diagnostic Tools for Culture-Negative Endocarditis
Serologic Tests
For pathogens that are fastidious or do not grow in conventional culture, serologic analysis has a role. Serologic test has long been the test of choice for detecting Coxiella burnetii infection. Furthermore, serological analysis may also be used to diagnose fastidious organisms such as Bartonella infections. Table 1 illustrates the application of serologic tests in the diagnosis of culture-negative endocarditis. In a study of 348 cases of blood culture-negative endocarditis between 1983 and 2001 in France, the application of indirect immunofluorescence assays successfully identified Coxiella burnetii (IgG titer⩾1:800), Bartonella spp. (IgG titer⩾1:800), and Legionella pneumophila (total antibody filter ⩾1:256) as major causative agents.1 In a study of 1998 suspected cases of endocarditis from April 1994 to December 2004 in Marseilles, France, 427 (21.4%) patients were diagnosed with definite endocarditis, and microbiologic diagnosis was established in 397 (93%) cases. Blood culture identified pathogens in 348 cases (81.5%), and serological testing identified pathogens in 34 cases (8%).16 The detection of Coxiella burnetii and Bartonella spp. by serologic test was therefore thought to be useful in the diagnosis of blood culture-negative endocarditis.3 A similar study was conducted from 2001 to 2009, which included 819 patients suspected of having blood culture-negative endocarditis. Despite the addition of antibodies specific to Brucella melitensis using an immunoenzymatic antibody test (titer, ⩾1:200) and Mycoplasma pneumoniae using an IgM kit, the majority of the identified pathogens were still Coxiella burnetii and Bartonella spp.
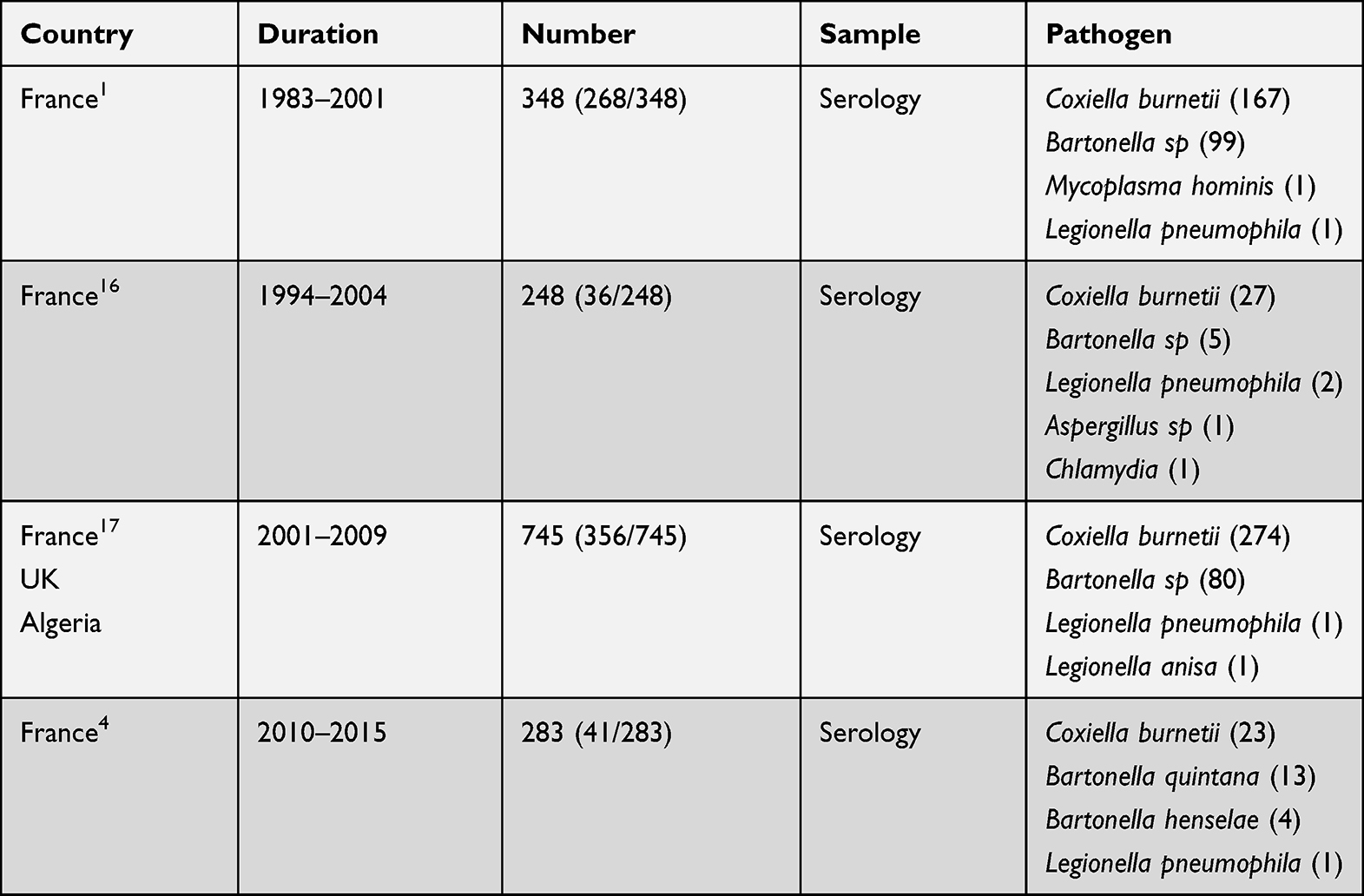 |
Table 1 Studies Using Serologic Tests for the Diagnosis of Blood Culture Negative Endocarditis |
Indirect Fluorescent Antibody Tests (IFAT), Enzyme-linked Immunosorbent Assays (ELISA) and Complement Fixation Tests (CFT) are commonly used serologic tests in Q fever. It is common to use IFAT and CFT in laboratories, but there are a number of disadvantages, including the subjective interpretation of the results. ELISA, on the other hand, is well suited to automation and is easy to perform.18 Serological tests have the advantage of being easily accessible, but have the disadvantage that a single serum sample can be inaccurate, since the IgM phase may persist for a longer period and can result in false-positive tests, which limits its use in acute infections.
Histopathology
In endocarditis cases who underwent operation, the excised valve can be submitted for histopathology and microbiological evaluation, including tissue staining, such as Gram, Giemsa, acid-fast, Warthin-Starry, and Periodic acid-Schiff stain to identify the etiologic agent.19 Furthermore, Bartonella spp., C. burnetii, and T. whipplei could be identified using immunohistochemical studies with specific polyclonal or monoclonal antibodies.20–22 Histopathological studies provide a definite diagnosis in some cases. They may also help distinguish infectious endocarditis from neoplasms and autoimmune disorders that mimic infectious endocarditis. Few identifiable pathogens and low sensitivity limit its use in culture-negative endocarditis.
Polymerase Chain Reaction (PCR)
Over the past twenty years, molecular techniques have been developed for the diagnosis of endocarditis.23 PCR has also been used to detect pathogens in both blood and excised tissues.
Specific PCR and broad-range bacterial PCR have been used in diagnosis of endocarditis. However, low microbial biomass is a great challenge for PCR methods used in blood samples. Infective endocarditis associated with low grade bacteremia could have microbial load as low as 1 CFU/mL.24 Because bacterial DNA often presents in low level in blood and in abundance in valve tissue. One study showed specific PCR was more sensitive when used in excised valve compared with blood. Sensitivity of a Bartonella PCR assay on valve tissue was 92% compared to 33% and 36% in blood and serum, respectively.25 As for broad-range bacterial PCR, although it had been applied to blood samples, sensitivity was still higher when used in excised valve tissue. Another study showed PCR method detected 66% of endocarditis via excised valve versus 14% with blood sample.17 In addition to low biomass, substances presented in blood could also interfere with the 16S/18S PCR reaction. Iron and immunoglobulin were examples of PCR inhibitors. Iron was mainly associated with hemoglobin from erythrocytes and lactoferrin from leucocytes which may inhibit PCR due to its inhibition of DNA synthesis. Immunoglobulin, IgG, on the other hand, could connect with single-strand DNA to inhibit PCR.26 Broad range PCR method was thought to have higher false-positive results due to contamination of specimen during the extraction process and inhibitor–DNA interaction.27,28
Commercial PCR methods are available for identification of common pathogen in sepsis patient. SepsiFast, based on multiplex real-time PCR, is an automated system for identifying 25 pathogens.29 The advantage of the SepsiFast is the short time needed for results (about 5 to 8 hours).26 Another more widely used PCR method is SepsiTest/molzym, which employs semiautomated system based on broad range PCR plus sequence analysis of amplicons to detect and identify a broad range of pathogens. SepsiTest has a crucial degradation step that degrades contaminating human DNA.30 SepsiTest is also used for analysis of blood and excised valve from patients due to wide variety of etiological agents of infective endocarditis patients.31 In addition, SepsiTest allows for identification of 345 pathogens including bacteria and fungus.26 However, a systematic review to determine the clinical effectiveness and cost-effectiveness of SepsiTest and SepsiFast showed no randomized clinical trial evidence indicating any of the tests significantly improved patient outcomes, such as mortality or duration in an intensive care unit or hospital.32 Moreover, the ideal diagnosis tool should be cost-effective for prevalent use, but the cost of SepsiFast system is approximately 75,000 USD, and the SepsiTest costs between 75,000 and 200,000 USD excluding the cost of reagents.33
Broad-range PCR, such as 16SrDNA for bacteria and 18SrDNA for fungi, is highly sensitive to small quantities of casual agents. A PCR-based examination of an excised valve is useful when a microbiologic diagnosis cannot be made based solely on blood culture or serology. An earlier study demonstrated that culture-independent molecular methods significantly enhanced the diagnostic outcome of microbiological examinations of excised heart valves. The sensitivity and specificity of broad-range PCR were 82.6% and 100%, respectively, in cases of infective endocarditis.34 In a prospective study of 759 cases of blood culture-negative endocarditis, the causative microbe was identified in 62.7% of case. With the aid of PCR analysis of valvular biopsies, microbiologic diagnosis was established in 109 more cases, mostly Streptococci, Tropheryma whipplei, Bartonella species, and fungi.17 Broad PCR followed by a high-resolution melting curve analysis can generate melting curve profiles that are unique pathogens. The melting curve profiles is dependent on size and sequence of PCR amplicon.35 However, traditional high-resolution melting cure technology has difficulties in distinguishing individual pathogens in polymicrobial samples.36
In an observational study of 283 patients with blood culture-negative endocarditis, broad-range PCR identified pathogens in 52 patients, Abiotrophia spp, Enterococcus spp, Gemella spp, Propionibacterium spp, Staphylococcus spp, Streptococcus spp, with Propionibacterium acne and Staphylococcus epidermidis being the most common. The addition of specific real-time PCR assays for Bartonella species, C. burnetii, Enterococcus faecalis, E. faecium, Escherichia coli, Staphylococcus aureus, Streptococcus gallolyticus, S. oralis, and Tropheryma whipplei increased the diagnostic efficiency by 24.3%.4 Studies using specific PCR and broad-range PCR for the diagnosis of culture-negative endocarditis are summarized in Tables 2 and 3. Several studies have demonstrated that specific real-time PCR had a significant specificity for Streptococcus gallolyticus and Staphylococcus aureus endocarditis.37,38 Although the use of broad-range PCR to detect bacteria is increasing, specific PCR assays still demonstrate superior sensitivity.37 One study from January 2010 to December 2015, including 283 patients with blood culture negative endocarditis, showed that specific RT-PCR was significantly more sensitive compared to broad range PCR (58 vs 12%).4 In clinical microbiology laboratories, these molecular techniques are not widely available and standardized procedures remain a challenge.
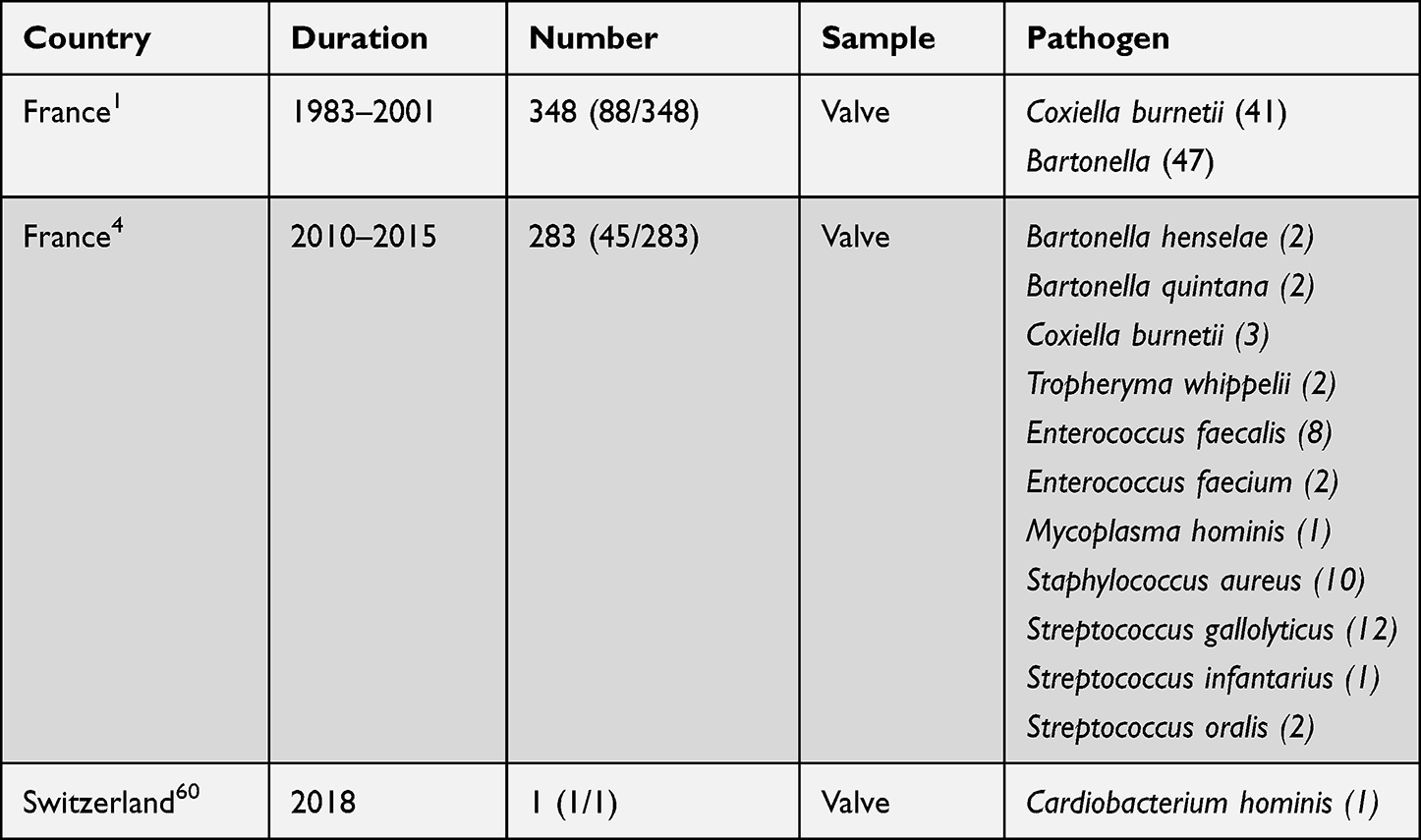 |
Table 2 Studies Using Specific PCR Method for the Diagnosis of Blood Culture-Negative Endocarditis |
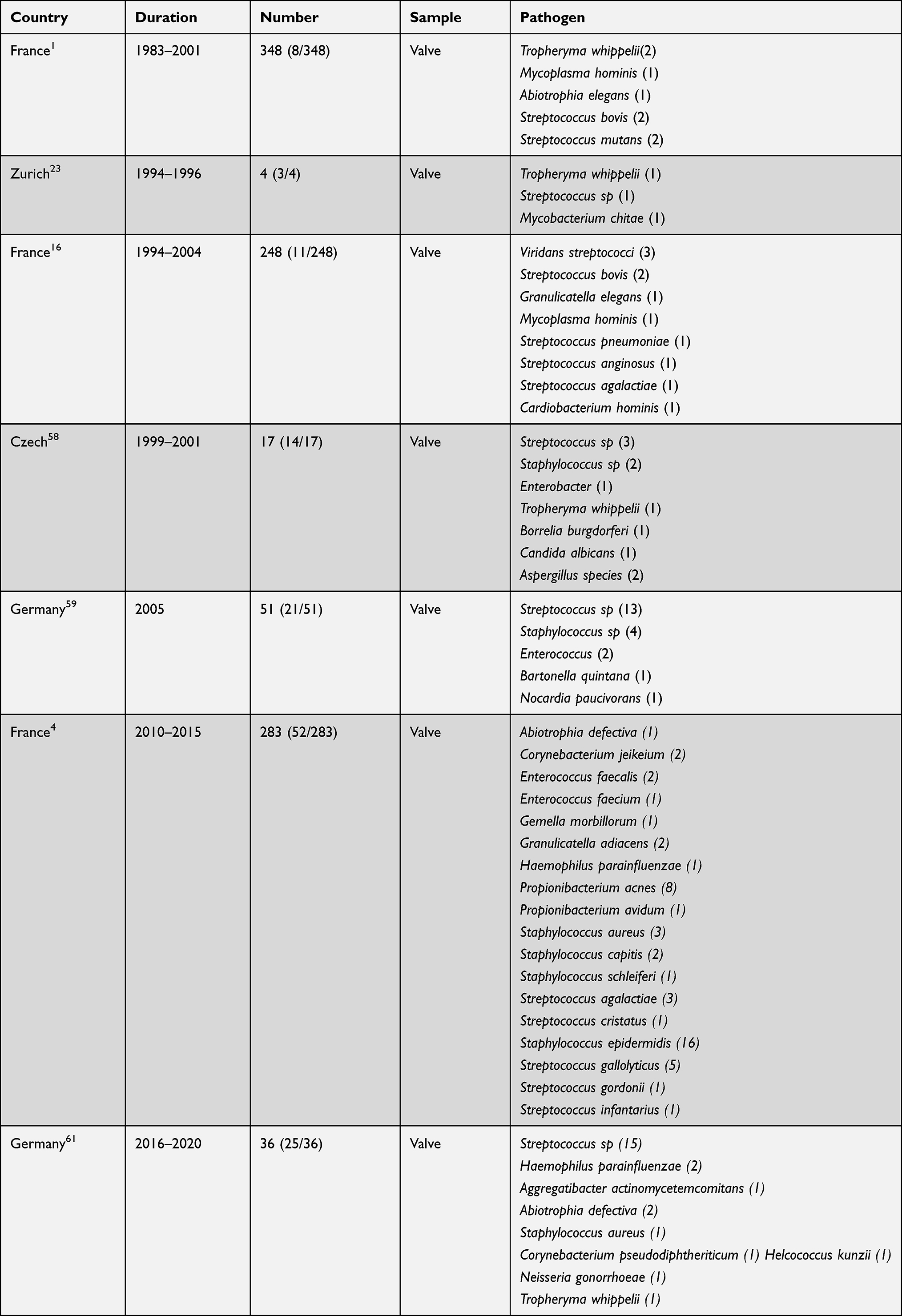 |
Table 3 Studies Using Broad Range PCR for the Diagnosis of Blood Culture Negative Endocarditis |
Metagenomic Sequencing
Infective endocarditis is a life-threatening infection despite having current diagnostic tools including culture, serology, and PCR. In traditional culture method, it takes times to identify microorganisms; at least 48 hours are also required for antimicrobial susceptibility testing. Nowadays, culture negative endocarditis is often caused by more fastidious pathogens, requiring more time for antimicrobial susceptibility testing. Although PCR has decreased turnaround time, up to 60% of infectious cases are caused by unidentified pathogens, leading to delayed or ineffective treatments.26,39,40
High mortality of infective endocarditis has no significant improvement over the past years. A systematic review and meta-analysis of short and long outcomes in infective endocarditis patients from 2000 to 2016 showed the overall pooled mortality estimates for infective endocarditis patients who underwent short- and long-term follow-up were 20% and 37%, respectively.41 In addition, the epidemiology of endocarditis has changed in recent years. Therefore, there should be adjustments to guidelines on diagnostic testing. Instead of the previously mentioned HACEK group, currently, the dominant pathogens include Staphylococcus aureus (27%) and Streptococcus pneumonia (23%).41 Enterococcus spp., especially Enterococcus faecalis, accounts for about 10% of cases. Gram-negative bacilli, including the HACEK group organisms, accounts for 5% of cases.3
With the advance of techniques and increase in endovascular procedures, there has been an increase in nosocomial infective endocarditis.13 In a cohort study of 3116 adult patients with diagnosis of infective endocarditis between January 2016 and March 2018, native valve infective endocarditis accounts for 56.6% of the cases, followed by prosthetic valve infective endocarditis (30.1%) and cardiac device related infective endocarditis (9.9%).42 Microorganisms obtained from cultures of cardiac-device-related infective endocarditis patients were predominantly Staphylococcus spp. (54%), followed by Streptococcus spp. (12%) and Enterococcus spp. (5%).10 Despite the development of diagnostic tools, there are still up to 50% in-hospital mortality.43 No significant improvement compared to the last decades. Therefore, other techniques are emerging as additional diagnostic tools.
In recent years, a method has been developed for detecting pathogens in blood culture-negative endocarditis by sequencing of clinical specimens. The most common methods of next-generation sequencing includes (1) whole-genome sequencing, sequencing and assembly of the genome of a pathogen of interest, especially used in the outbreak of new species to evaluate genetic relatedness.44,45 (2) targeted NGS with different methods for amplification or probe hybridization, for example, using 16S rDNA bacterial profiling or PCR amplification of other specified targets followed by NGS.45,46 (3) metagenomic next-generation sequencing (mNGS). Currently, the data of mNGS suggest that it has high efficiency and accuracy in the diagnosis of blood culture negative endocarditis.14,15 In a study involving 44 patients with endocarditis using mNGS for diagnosis, superior sensitivity and a shorter turnaround time were demonstrated compared with culture-based methods.47 In 99 cases of endocarditis, mNGS demonstrated greater sensitivity than culture-based techniques. Valve mNGS displayed a sensitivity of 85.9%, with a specificity of 72.7% compared to blood/valve culture (sensitivity: 29.3%/16.2%, specificity: 100%/100%). In addition, mNGS identified more Streptococcus sanguis, Streptococcus buccalis, and Streptococcus griseus, as well as Proteobacteria and Actinomycetes cases.48
Streptococcus is an important genus of human and animal pathogens. Based on 16S rRNA gene sequence similarity, the genus had different groups. However, the variability of members in these groups is low and made it difficult for 16S PCR to distinguish.49 In a prospective cohort study, mNGS identified more Streptococcus sanguis, Streptococcus buccalis, and Streptococcus griseus, as well as Proteobacteria and Actinomycetes cases.48
mNGS is also known as unbiased NGS and clinical metagenomics. Its high-throughput parallel sequencing allows for thousands to billions of DNA and/or RNA fragments to be simultaneously and independently sequenced.15 An important factor that impacts results is the extraction used in laboratories. Nucleic acid recovery is not the same for all pathogens. To achieve unbiased sequencing, mNGS needs an efficient extraction method.50
Currently, PCR is most commonly used in infective endocarditis patients for detection of pathogens in excised value tissue. However, mNGS can be applied for patients who do not undergo valve surgeries. One study had recorded using cell-free plasma mNGS in detecting pathogens in 8 out of 10 subjects.51 Although currently there are only a few studies on plasma mNGS due to low microbial biomass, it has great potential for patients not receiving surgeries.
Compared with other methods, the mNGS technique has three main advantages. Firstly, mNGS has an unbiased sampling which enables identification of unexpected pathogens or even novel organisms.52 Secondly, mNGS offers the accessory genomic information for evolution tracing, strain identification, and most importantly, for prediction of drug resistances.53–55 Lastly, mNGS can examine every DNA fragment and classify independently. It can be used to catalog individual species comprising a mixture of organisms. Furthermore, NGS provides quantitative data by counting the sequenced reads, and it is crucial in polymicrobial infection.46
But there are still some drawbacks of mNGS. Firstly, validation of mNGS is time consuming and extremely costly. Besides, there is no clear database being clearly pointed out by the US Food and Drug Administration (FDA).39 Physicians interpreting the data need to have a deep understanding of the method. Secondly, microbial nucleic acids from most patients’ samples are contributed mainly from human host background. This can be addressed by host depletion and microbial enrichment.15 Lastly, drawback of mNGS includes contamination of the sample, such as skin flora or oral flora from the procedure. Therefore, laboratories have to be familiar with the common microbial flora existed in the different types of specimens.56
Although mNGS has been used for undiagnosed infectious disease in many countries since 2008, there are still challenges to overcome with respect to quality control, method standardization, workflow validation and data interpretation.57
Conclusion
A significant proportion of patients with endocarditis have blood culture-negative findings, and thus the identification of the causative organism allows refinement of empirical antibiotic use. The is review highlights the strategies and approaches used in blood culture negative endocarditis patients. We proposed an approach to culture-negative endocarditis in Figure 1 and listed advantages and disadvantages of different methods in Table 4 for comparison.
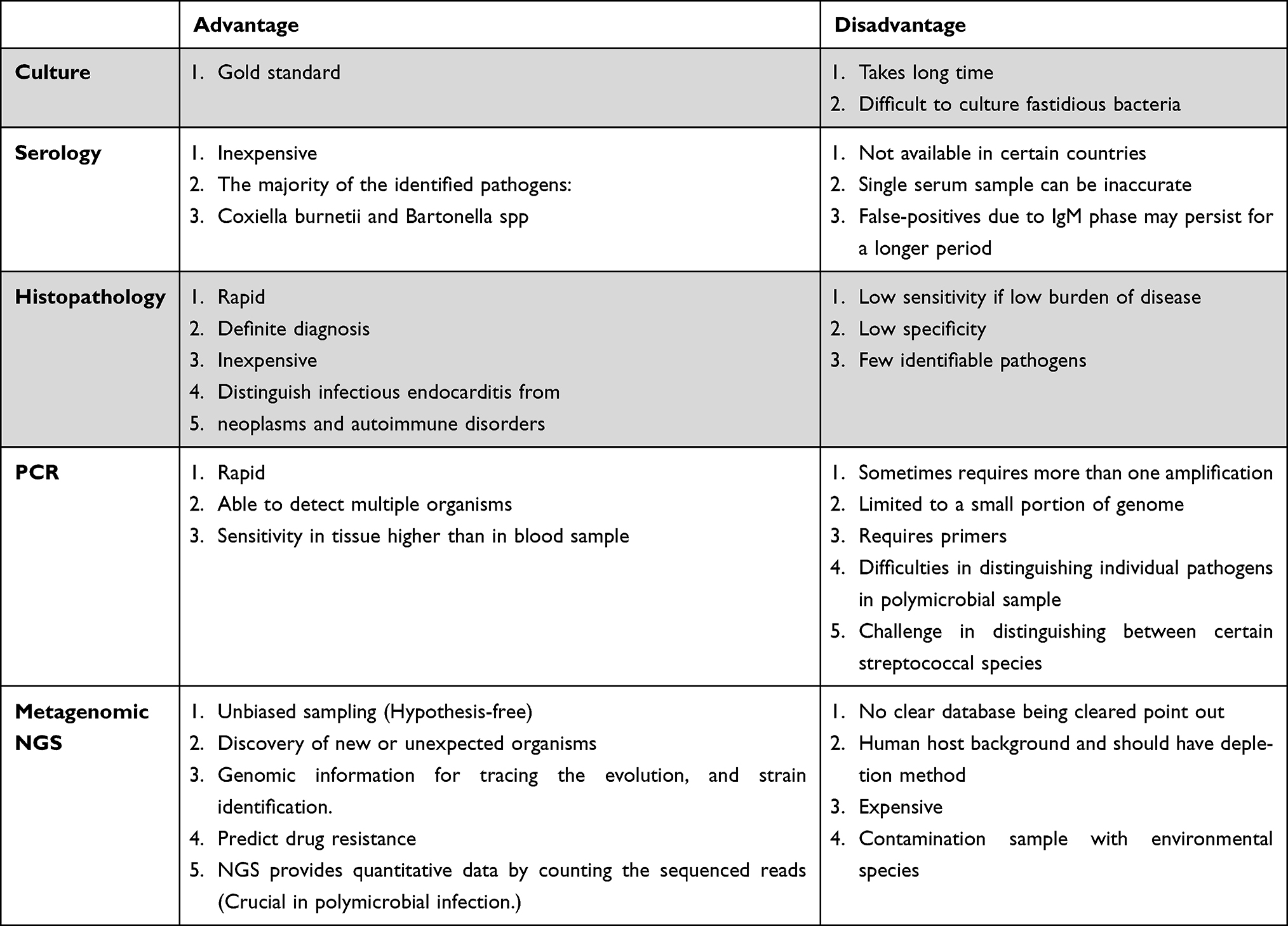 |
Table 4 The Advantage and Disadvantage of Different Methods |
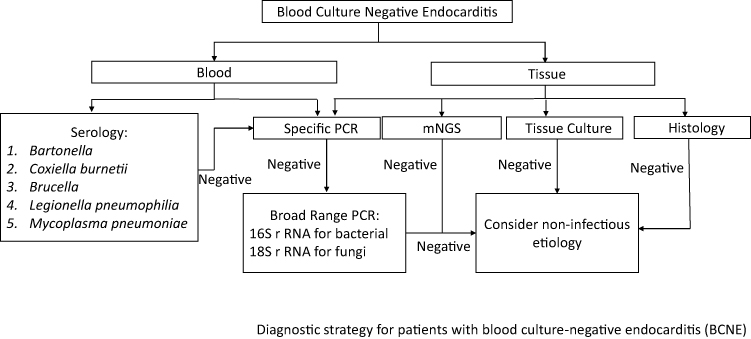 |
Figure 1 A pragmatic approach for determining the causative organism in suspected endocarditis. |
The use of molecular methods is becoming increasingly common for the diagnosis of culture-negative endocarditis in both blood and excised valves. In patients undergoing surgery, the excisional valve should be sent for broad-range and/or specific PCR for identification of the causative pathogen. The presence of bacterial DNA is greater in valve tissue than in blood, which makes the PCR assays used for testing cardiac excised valve tissues more sensitive than those used for testing blood or serum. Besides, specific PCR also superior in sensitivity compared to a broad range PCR. In addition, Streptococcus species and Staphylococcus species also account for a large percentage of blood culture-negative endocarditis using polymerase chain reaction.
Serology and PCR may help to identify fastidious pathogens in blood samples or valves with Coxiella burnetii and Bartonella spp. being the most common identified pathogens. Next-generation sequencing has been applied in the diagnosis of culture-negative endocarditis and has great value in distinguishing streptococcal species and polymicrobial infection.
However, before applying metagenomics analysis in the detection of clinical microorganisms, further studies are required to optimize protocols for sample processing, sequencing, and bioinformatics analysis. For blood culture negative endocarditis patients, serology of Coxiella burnetii and Bartonella spp. are to be surveyed first, Coxiella burnetii and Bartonella spp anti-phase I IgG antibody titer of ⩾1:800 is considered positive. Test Brucella if Coxiella and Bartonella spp. show negative results, and with exposure history, also consider Legionella and Mycoplasma serology. If the patient has undergone surgery, the excised valve should be sent for culture, specific PCR, and broad-range PCR including 16SrRNA and 18SrRNA for bacteria and fungus, respectively. Next-generation sequencing should also be taken into consideration.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Houpikian P, Raoult D. Blood culture-negative endocarditis in a reference center: etiologic diagnosis of 348 cases. Medicine. 2005;84(3):162–173. doi:10.1097/01.md.0000165658.82869.17
2. Lamas CC, Eykyn SJ. Blood culture negative endocarditis: analysis of 63 cases presenting over 25 years. Heart. 2003;89(3):258–262. doi:10.1136/heart.89.3.258
3. Liesman RM, Pritt BS, Maleszewski JJ, Patel R. Laboratory diagnosis of infective endocarditis. J Clin Microbiol. 2017;55(9):2599–2608. doi:10.1128/jcm.00635-17
4. Fournier PE, Gouriet F, Casalta JP, et al. Blood culture-negative endocarditis: improving the diagnostic yield using new diagnostic tools. Medicine. 2017;96(47):e8392. doi:10.1097/md.0000000000008392
5. Godfrey R, Curtis S, Schilling WH, James PR. Blood culture negative endocarditis in the modern era of 16S rRNA sequencing. Clin Med. 2020;20(4):412–416. doi:10.7861/clinmed.2019-0342
6. Baron EJ, Scott JD, Tompkins LS. Prolonged incubation and extensive subculturing do not increase recovery of clinically significant microorganisms from standard automated blood cultures. Clin Infect Dis. 2005;41(11):1677–1680. doi:10.1086/497595
7. Petti CA, Bhally HS, Weinstein MP, et al. Utility of extended blood culture incubation for isolation of Haemophilus, Actinobacillus, Cardiobacterium, Eikenella, and Kingella organisms: a retrospective multicenter evaluation. J Clin Microbiol. 2006;44(1):257–259. doi:10.1128/jcm.44.1.257-259.2006
8. Hoen B, Selton-Suty C, Lacassin F, et al. Infective endocarditis in patients with negative blood cultures: analysis of 88 cases from a one-year nationwide survey in France. Clin Infect Dis. 1995;20(3):501–506. doi:10.1093/clinids/20.3.501
9. Kong WKF, Salsano A, Giacobbe DR, et al. Outcomes of culture-negative vs. culture-positive infective endocarditis: the ESC-EORP EURO-ENDO registry. Eur Heart J. 2022;43(29):2770–2780. doi:10.1093/eurheartj/ehac307
10. Kouijzer JJP, Noordermeer DJ, Van Leeuwen WJ, Verkaik NJ, Lattwein KR. Native valve, prosthetic valve, and cardiac device-related infective endocarditis: a review and update on current innovative diagnostic and therapeutic strategies. Front Cell Dev Biol. 2022;10:995508. doi:10.3389/fcell.2022.995508
11. Shah ASV, McAllister DA, Gallacher P, et al. Incidence, microbiology, and outcomes in patients hospitalized with infective endocarditis. Circulation. 2020;141(25):2067–2077. doi:10.1161/circulationaha.119.044913
12. Wu Z, Chen Y, Xiao T, Niu T, Shi Q, Xiao Y. The clinical features and prognosis of infective endocarditis in the elderly from 2007 to 2016 in a tertiary hospital in China. BMC Infect Dis. 2019;19(1):937. doi:10.1186/s12879-019-4546-6
13. Satriano UM, Nenna A, Spadaccio C, et al. Guidelines on prosthetic heart valve management in infective endocarditis: a narrative review comparing American Heart Association/American College of Cardiology and European Society of Cardiology guidelines. Ann Transl Med. 2020;8(23):1625. doi:10.21037/atm-20-5134
14. Simner PJ, Miller S, Carroll KC. Understanding the promises and hurdles of metagenomic next-generation sequencing as a diagnostic tool for infectious diseases. Clin Infect Dis. 2018;66(5):778–788. doi:10.1093/cid/cix881
15. Gu W, Miller S, Chiu CY. Clinical metagenomic next-generation sequencing for pathogen detection. Annu Rev Pathol. 2019;14:319–338. doi:10.1146/annurev-pathmechdis-012418-012751
16. Raoult D, Casalta JP, Richet H, et al. Contribution of systematic serological testing in diagnosis of infective endocarditis. J Clin Microbiol. 2005;43(10):5238–5242. doi:10.1128/jcm.43.10.5238-5242.2005
17. Fournier PE, Thuny F, Richet H, et al. Comprehensive diagnostic strategy for blood culture-negative endocarditis: a prospective study of 819 new cases. Clin Infect Dis. 2010;51(2):131–140. doi:10.1086/653675
18. Wegdam-Blans MC, Wielders CC, Meekelenkamp J, et al. Evaluation of commonly used serological tests for detection of Coxiella burnetii antibodies in well-defined acute and follow-up sera. Clin Vaccine Immunol. 2012;19(7):1110–1115. doi:10.1128/cvi.05581-11
19. Houpikian P, Raoult D. Diagnostic methods current best practices and guidelines for identification of difficult-to-culture pathogens in infective endocarditis. Infect Dis Clin North Am. 2002;16(2):377–392. doi:10.1016/s0891-5520(01)00010-1
20. Lepidi H, Fournier PE, Raoult D. Quantitative analysis of valvular lesions during Bartonella endocarditis. Am J Clin Pathol. 2000;114(6):880–889. doi:10.1309/R0KQ-823A-BTC7-MUUJ
21. Lepidi H, Houpikian P, Liang Z, Raoult D. Cardiac valves in patients with Q fever endocarditis: microbiological, molecular, and histologic studies. J Infect Dis. 2003;187(7):1097–1106. doi:10.1086/368219
22. Lepidi H, Fenollar F, Dumler JS, et al. Cardiac valves in patients with Whipple endocarditis: microbiological, molecular, quantitative histologic, and immunohistochemical studies of 5 patients. J Infect Dis. 2004;190(5):935–945. doi:10.1086/422845
23. Goldenberger D, Künzli A, Vogt P, Zbinden R, Altwegg M. Molecular diagnosis of bacterial endocarditis by broad-range PCR amplification and direct sequencing. J Clin Microbiol. 1997;35(11):2733–2739. doi:10.1128/jcm.35.11.2733-2739.1997
24. Mancini N, Carletti S, Ghidoli N, Cichero P, Burioni R, Clementi M. The era of molecular and other non-culture-based methods in diagnosis of sepsis. Clin Microbiol Rev. 2010;23(1):235–251. doi:10.1128/cmr.00043-09
25. Edouard S, Nabet C, Lepidi H, Fournier PE, Raoult D. Bartonella, a common cause of endocarditis: a report on 106 cases and review. J Clin Microbiol. 2015;53(3):824–829. doi:10.1128/jcm.02827-14
26. Opota O, Jaton K, Greub G. Microbial diagnosis of bloodstream infection: towards molecular diagnosis directly from blood. Clin Microbiol Infect. 2015;21(4):323–331. doi:10.1016/j.cmi.2015.02.005
27. Corless CE, Guiver M, Borrow R, Edwards-Jones V, Kaczmarski EB, Fox AJ. Contamination and sensitivity issues with a real-time universal 16S rRNA PCR. J Clin Microbiol. 2000;38(5):1747–1752. doi:10.1128/jcm.38.5.1747-1752.2000
28. Hoorfar J, Malorny B, Abdulmawjood A, Cook N, Wagner M, Fach P. Practical considerations in design of internal amplification controls for diagnostic PCR assays. J Clin Microbiol. 2004;42(5):1863–1868. doi:10.1128/jcm.42.5.1863-1868.2004
29. Gies F, Tschiedel E, Felderhoff-Müser U, Rath PM, Steinmann J, Dohna-Schwake C. Prospective evaluation of SeptiFast Multiplex PCR in children with systemic inflammatory response syndrome under antibiotic treatment. BMC Infect Dis. 2016;16:378. doi:10.1186/s12879-016-1722-9
30. Rogina P, Skvarc M, Stubljar D, Kofol R, Kaasch A. Diagnostic utility of broad range bacterial 16S rRNA gene PCR with degradation of human and free bacterial DNA in bloodstream infection is more sensitive than an in-house developed PCR without degradation of human and free bacterial DNA. Mediators Inflamm. 2014;2014:108592. doi:10.1155/2014/108592
31. Kühn C, Disqué C, Mühl H, Orszag P, Stiesch M, Haverich A. Evaluation of commercial universal rRNA gene PCR plus sequencing tests for identification of bacteria and fungi associated with infectious endocarditis. J Clin Microbiol. 2011;49(8):2919–2923. doi:10.1128/jcm.00830-11
32. Stevenson M, Pandor A, Martyn-St James M, et al. Sepsis: the LightCycler SeptiFast Test MGRADE®, SepsiTest™ and IRIDICA BAC BSI assay for rapidly identifying bloodstream bacteria and fungi - A systematic review and economic evaluation. Health Technol Assess. 2016;20(46):1–246. doi:10.3310/hta20460
33. Afshari A, Schrenzel J, Ieven M, Harbarth S. Bench-to-bedside review: rapid molecular diagnostics for bloodstream infection--A new frontier? Crit Care. May. 2012;16(3):222. doi:10.1186/cc11202
34. Bosshard PP, Kronenberg A, Zbinden R, Ruef C, Böttger EC, Altwegg M. Etiologic diagnosis of infective endocarditis by broad-range polymerase chain reaction: a 3-year experience. Clin Infect Dis. 2003;37(2):167–172. doi:10.1086/375592
35. Reed GH, Kent JO, Wittwer CT. High-resolution DNA melting analysis for simple and efficient molecular diagnostics. Pharmacogenomics. 2007;8(6):597–608. doi:10.2217/14622416.8.6.597
36. Zhang Y, Hu A, Andini N, Yang S. A ‘culture’ shift: application of molecular techniques for diagnosing polymicrobial infections. Biotechnol Adv. 2019;37(3):476–490. doi:10.1016/j.biotechadv.2019.02.013
37. Morel AS, Dubourg G, Prudent E, et al. Complementarity between targeted real-time specific PCR and conventional broad-range 16S rDNA PCR in the syndrome-driven diagnosis of infectious diseases. Eur J Clin Microbiol Infect Dis. 2015;34(3):561–570. doi:10.1007/s10096-014-2263-z
38. Lang S, Watkin RW, Lambert PA, Bonser RS, Littler WA, Elliott TS. Evaluation of PCR in the molecular diagnosis of endocarditis. J Infect. 2004;48(3):269–275. doi:10.1016/s0163-4453(03)
39. Schlaberg R, Chiu CY, Miller S, Procop GW, Weinstock G. Validation of Metagenomic Next-Generation Sequencing Tests for Universal Pathogen Detection. Arch Pathol Lab Med. 2017;141(6):776–786. doi:10.5858/arpa.2016-0539-RA
40. Tan KE, Ellis BC, Lee R, Stamper PD, Zhang SX, Carroll KC. Prospective evaluation of a matrix-assisted laser desorption ionization-time of flight mass spectrometry system in a hospital clinical microbiology laboratory for identification of bacteria and yeasts: a bench-by-bench study for assessing the impact on time to identification and cost-effectiveness. J Clin Microbiol. 2012;50(10):3301–3308. doi:10.1128/jcm.01405-12
41. Abegaz TM, Bhagavathula AS, Gebreyohannes EA, Mekonnen AB, Abebe TB. Short- and long-term outcomes in infective endocarditis patients: a systematic review and meta-analysis. BMC Cardiovasc Disord. 2017;17(1):291. doi:10.1186/s12872-017-0729-5
42. Habib G, Erba PA, Iung B, et al. Clinical presentation, aetiology and outcome of infective endocarditis. Results of the ESC-EORP EURO-ENDO (European infective endocarditis) registry: a prospective cohort study. Eur Heart J. 2019;40(39):3222–3232. doi:10.1093/eurheartj/ehz620
43. Mistiaen WP. What are the main predictors of in-hospital mortality in patients with infective endocarditis: a review. Scand Cardiovasc J. 2018;52(2):58–68. doi:10.1080/14017431.2018.1433318
44. Salipante SJ, Roach DJ, Kitzman JO, et al. Large-scale genomic sequencing of extraintestinal pathogenic Escherichia coli strains. Genome Res. 2015;25(1):119–128. doi:10.1101/gr.180190.114
45. Salipante SJ, Sengupta DJ, Cummings LA, et al. Whole genome sequencing indicates Corynebacterium jeikeium comprises 4 separate genomospecies and identifies a dominant genomospecies among clinical isolates. Int J Med Microbiol. 2014;304(8):1001–1010. doi:10.1016/j.ijmm.2014.07.003
46. Salipante SJ, Hoogestraat DR, Abbott AN, et al. Coinfection of Fusobacterium nucleatum and Actinomyces israelii in mastoiditis diagnosed by next-generation DNA sequencing. J Clin Microbiol. 2014;52(5):1789–1792. doi:10.1128/jcm.03133-13
47. Cheng J, Hu H, Fang W, et al. Detection of pathogens from resected heart valves of patients with infective endocarditis by next-generation sequencing. Int J Infect Dis. 2019;83:148–153. doi:10.1016/j.ijid.2019.03.007
48. Zeng X, Wu J, Li X, et al. Application of Metagenomic Next-Generation Sequencing in the Etiological Diagnosis of Infective Endocarditis During the Perioperative Period of Cardiac Surgery: a Prospective Cohort Study. Front Cardiovasc Med. 2022;9:811492. doi:10.3389/fcvm.2022.811492
49. Lal D, Verma M, Lal R. Exploring internal features of 16S rRNA gene for identification of clinically relevant species of the genus Streptococcus. Ann Clin Microbiol Antimicrob. 2011;10:28. doi:10.1186/1476-0711-10-28
50. Hart ML, Meyer A, Johnson PJ, Ericsson AC. Comparative Evaluation of DNA Extraction Methods from Feces of Multiple Host Species for Downstream Next-Generation Sequencing. PLoS One. 2015;10(11):e0143334. doi:10.1371/journal.pone.0143334
51. To RK, Ramchandar N, Gupta A, et al. Use of Plasma Metagenomic Next-generation Sequencing for Pathogen Identification in Pediatric Endocarditis. Pediatr Infect Dis J. 2021;40(5):486–488. doi:10.1097/inf.0000000000003038
52. Chiu CY. Viral pathogen discovery. Curr Opin Microbiol. 2013;16(4):468–478. doi:10.1016/j.mib.2013.05.001
53. Gire SK, Goba A, Andersen KG, et al. Genomic surveillance elucidates Ebola virus origin and transmission during the 2014 outbreak. Science. 2014;345(6202):1369–1372. doi:10.1126/science.1259657
54. Deurenberg RH, Bathoorn E, Chlebowicz MA, et al. Application of next generation sequencing in clinical microbiology and infection prevention. J Biotechnol. 2017;243:16–24. doi:10.1016/j.jbiotec.2016.12.022
55. Sahoo MK, Lefterova MI, Yamamoto F, et al. Detection of cytomegalovirus drug resistance mutations by next-generation sequencing. J Clin Microbiol. 2013;51(11):3700–3710. doi:10.1128/jcm.01605-13
56. Bukowska-Ośko I, Perlejewski K, Nakamura S, et al. Sensitivity of Next-Generation Sequencing Metagenomic Analysis for Detection of RNA and DNA Viruses in Cerebrospinal Fluid: the Confounding Effect of Background Contamination. Adv Exp Med Biol. 2016. doi:10.1007/5584_2016_42
57. Han D, Li Z, Li R, Tan P, Zhang R, Li J. mNGS in clinical microbiology laboratories: on the road to maturity. Crit Rev Microbiol. 2019;45(5–6):668–685. doi:10.1080/1040841x.2019.1681933
58. Grijalva M, Horváth R, Dendis M, Erný J, Benedík J. Molecular diagnosis of culture negative infective endocarditis: clinical validation in a group of surgically treated patients. Heart. 2003;89(3):263–268. doi:10.1136/heart.89.3.263
59. Breitkopf C, Hammel D, Scheld HH, Peters G, Becker K. Impact of a molecular approach to improve the microbiological diagnosis of infective heart valve endocarditis. Circulation. 2005;111(11):1415–1421. doi:10.1161/01.Cir.0000158481.07569.8d
60. Kolb M, Lazarevic V, Emonet S, et al. Next-Generation Sequencing for the Diagnosis of Challenging Culture-Negative Endocarditis. Front Med. 2019;6:203. doi:10.3389/fmed.2019.00203
61. Anton-Vazquez V, Dworakowski R, Cannata A, et al. 16S rDNA PCR for the aetiological diagnosis of culture-negative infective endocarditis. Infection. 2022;50(1):243–249. doi:10.1007/s15010-021-01690-x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.