Back to Journals » International Journal of Women's Health » Volume 17
Bleeding Through a Pandemic: Women’s Lived Experiences with Heavy Menstrual Bleeding During the COVID-19 Pandemic
Authors Anto-Ocrah M ![]() , Affan NJ, Vempalli H, Chen M, Niyomugabo C
, Affan NJ, Vempalli H, Chen M, Niyomugabo C ![]() , Glantz JC
, Glantz JC ![]() , Hollenbach S
, Hollenbach S ![]()
Received 8 July 2024
Accepted for publication 20 March 2025
Published 18 April 2025 Volume 2025:17 Pages 1083—1101
DOI https://doi.org/10.2147/IJWH.S476959
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Marleen van Gelder
Martina Anto-Ocrah,1,2 Nabeeha Jabir Affan,2 Hemika Vempalli,1 Michael Chen,3 Celestin Niyomugabo,4 J Christopher Glantz,5 Stefanie Hollenbach5
1Division of General Internal Medicine, University of Pittsburgh School of Medicine, Pittsburgh, PA, USA; 2Department of Epidemiology, University of Pittsburgh School of Public Health, Pittsburgh, PA, USA; 3JSI Research & Training Institute, Boston, MA, USA; 4VONSUNG, Kigali, Rwanda; 5Department of Obstetrics and Gynecology, University of Rochester School of Medicine and Dentistry, Rochester, NY, USA
Correspondence: Martina Anto-Ocrah, Email [email protected]
Introduction: Heavy menstrual bleeding (menorrhagia) affects 10 million reproductive-age women. Stress is a mechanism for menstrual disorders, and during the COVID-19 pandemic, women reported worsening premenstrual and menstrual symptoms. We hypothesized that there would be a positive association between COVID stress and menorrhagia and a negative association between menorrhagia and mental health. A third objective was to explore women’s lived experiences with menorrhagia during the pandemic, including menstrual pain and impact on socialization, sex life, and product use.
Methods: This was a secondary data analyses of a cross-sectional study that recruited adult women between the ages of 18– 45 years using Dynata, a survey sampling company that maintains a web panel of survey takers across the United States. Menorrhagia was assessed with the Aberdeen Menorrhagia Severity Scale (AMSS), COVID stress with the COVID-19 Pandemic-related Perceived Stress Scale (PSS-10-C), and mental health with the Mental Health Continuum Scale (MHC-SF). We grouped the participants into mild menorrhagia (AMSS score 0– 33)” and moderate/severe menorrhagia (AMSS score 34– 100) and compared the outcomes using descriptive statistics, correlations, and linear regression.
Results: The survey was conducted in May 2021. Among 1,037 initial responses, 360 naturally cycling women met the study eligibility criteria. Women with heavy bleeding reported more COVID-stress than those without heavy bleeding (p < 0.01) and heavy bleeding intensified with increasing COVID-related stress (adj. β = 0.37, 95% CI: 0.21, 0.53). Adjusting for baseline depression, mental health worsened as heavy bleeding increased (adj. β = − 0.1, 95% CI: − 0.24, − 0.03). Compared to those without heavy bleeding, women with heavy bleeding were more likely to report severe pain and bed confinement, less socialization, a negative impact on sex life, and greater use of menstrual products.
Conclusion: COVID-related stress affects menstrual physiology and also complex interactions between life-course, social functioning, financial strain, and psychological stress. Our findings support increased awareness of these interactions in gynecologic care during a global pandemic.
Keywords: women’s health, COVID, menstruation, menorrhagia, heavy bleeding, COVID stress, COVID risk, menstrual cup, pandemic
Introduction
Heavy menstrual bleeding, often referred to as menorrhagia, affects 10 million women in their reproductive years, and accounts for 20–30% of all outpatient gynecological visits in the United States annually.1–3 The condition can have significant physiological, psychosocial, and financial impact on people who menstruate,4 with many needing extensive clinical and surgical management that may impact future fertility.3 Stress has been identified as one of the mechanistic pathways for menstrual cycle irregularities and disorders. Stress pathways are known to interact and modulate the menstrual cycle through hormonally mediated feedback loops via the hypothalamus-pituitary-ovarian axis.5–7 Menstrual cycle characteristics and hormonal symptoms showed significant variation during the COVID-19 pandemic, primarily attributable to the societal and lifestyle shifts triggered by pandemic stress, not the COVID-19 virus itself.8
As lockdown protocols intensified, the gender gap between men and women widened.9–12 Women were tasked with more caregiver and domestic responsibilities, unpaid labor, and not surprisingly, found the pandemic–induced changes to daily activities significantly more stressful than men.9–13 Emerging literature also found that women’s reproductive experiences were exacerbated by pandemic stress. Women consistently reported worsening premenstrual symptoms, changes in cycle length and duration, increased intermenstrual spotting, and amenorrhea during as compared to before the pandemic.14–17 Some women reported adverse pregnancy and birthing experiences,18–20 decreased sexual function,21 and inequities in contraceptive care and access.19,22 However, the relationship between pandemic stress and women’s menstrual bleeding experiences remains under studied. A deeper understanding of the prevalence, morbidity, and “lived experiences” of women with heavy menstrual bleeding during the COVID-19 pandemic is crucial for developing guidelines that support and aid in the management of such patients during future pandemics. This research has important implications for future studies, clinical practice, and policy. Findings could be used in exploring long-term mental health outcomes related to heavy menstrual bleeding and stress, as well as the effectiveness of various interventions (eg, mental health support and menstrual product accessibility) to address these challenges. Clinically, providers can use our findings to screen for mental health concerns and stress in people presenting with heavy bleeding, ensuring comprehensive, patient-centered care. Policymakers can prioritize funding and resources to improve access to menstrual health products, mental health services, and educational programs for vulnerable populations during public health crises.
The World Health Organization has declared chronic pelvic pain due to menorrhagia and other menstrual disorders a neglected reproductive health morbidity.23 Left untreated, these conditions can impact one’s productivity across the life span. An exploration of the pandemic’s impact on menstruator’s reproductive health is critical for the advancement of the fields of gynecological care and reproductive epidemiology. Thus, the purpose of this study was i) to evaluate the association between COVID stress and heavy menstrual bleeding, as well as the relationship between women’s mental health and this condition, and ii) to explore women’s lived experiences with menorrhagia during the pandemic, including menstrual pain, impact on socialization, sex life, and product use.
Methods
Study Sample
This was a secondary data analysis of a cross-sectional study that recruited adult women between the ages of 18–45 using Dynata, a survey sampling company that maintains a web panel of survey takers across the United States.14 The survey was launched on May 4, 2021, and ended on May 7, 2021. The inclusion criteria included: 1) self-identifying as a woman, 2) self-reported age between 18 and 45 years, and 3) a resident of the United States (US) or US territory. Women older than 45 years were excluded to avoid the possibility of menstrual irregularities related to the menopausal transition. To further capture those with natural cycles, we excluded women who were menopausal or postmenopausal before the pandemic, had undergone a hysterectomy, were currently pregnant, were less than 3 months postpartum, were currently receiving exogenous glucocorticoids, had undergone infertility treatments before the pandemic, or were currently taking hormonal birth control. The study was approved by the University of Rochester Institutional Review Board (STUDY00005980). All participants provided informed consent, and the study complies with the Declaration of Helsinki.
Measures
Incidence (a measure of the number of new cases of a condition/disease occurring in a population over a specific period of time24) of menorrhagia was defined as the proportion of participants who responded “Yes, heavier flow” to the question: “Since the COVID-19 pandemic began in March 2020, has your menstrual flow changed? (Amount of bleeding).” Heavy menstrual bleeding was assessed using the Aberdeen Menorrhagia Severity Scale (AMSS),25 a 15-item questionnaire that was designed to reflect clinical questions asked when taking a gynecological history. To properly reflect the landscape of menstrual products available to and used by today’s women, the study’s Obstetrics and Gynecology clinical expert (co-author SH) modified the questionnaire to include menstrual cup usage. The item responses to each question were assigned ordinal scores, summed, and converted to percentages to produce a “menorrhagia severity score” between 0 and 100. An Aberdeen score of 0–33% was classified as mild, 34% to 66% was moderate, and 67–100% as severe.26–29 For a deeper understanding of women’s lived experience with heavy bleeding, we stratified key questions on the AMSS by mild and moderate/severe menorrhagia and compared participants’ responses. The selection of key questions was guided by the expertise of our clinician co-author SH, following the principles of Item Response Theory (IRT). IRT is a branch of psychometrics which seeks to understand and statistically model how a person will respond to items on a survey questionnaire given a certain level of an underlying characteristic (eg, depression, cognitive ability, or in this case, menorrhagia).30
COVID stress was evaluated with the COVID-19 Pandemic-related Perceived Stress Scale (PSS-10-C).31 The PSS-10-C has 10 items that are ranked on a 5-point Likert scale of “0-Never” to “4-Always.” Scores range from 0 to 40, with higher scores indicative of greater stress levels.
Mental health was assessed with the Mental Health Continuum Scale (MHC-SF).32 Each of the 14 items on the MHC-SF can be scored between 0 and 5, which means that the total score on the scale can range from 0 to 70 points. Lower scores indicate poor psychological wellbeing.
Covariates
Covariates of interest included age, race, ethnicity, educational attainment, marital status, number of living children (younger than age 18 years), and smoking status. Participants’ pre-pandemic menstrual functioning was assessed by asking them the number of periods they experienced per year, before the pandemic, along with comorbidities diagnosed before and during the pandemic. Comorbidities of heavy bleeding considered during the analyses included reproductive or gynecologic conditions (endometriosis, leiomyomas or myomas, polycystic ovarian syndrome, and uterine polyps), thyroid disease, obesity, sexually transmitted infections, and self-reported mental health history. We also asked about participants’ COVID-19 vaccination status as research shows an association between menstrual bleeding patterns and the COVID-19 vaccine.33–35
Statistical Analyses
Assuming a 20% population prevalence of menorrhagia3,16,36 an alpha of 0.05 and a 95% confidence interval, an estimated sample size of 246 was required. We over-estimated our sample size by 50% to ensure adequate reach of participants, given the study context-in the middle of the pandemic. We used descriptive statistics (proportions, means, medians, ranges, and standard deviations) to describe the study sample. Pearson’s x2 and t tests were used to compare survey responses in bivariate analyses and to identify important covariates. Effect estimates were determined with correlation coefficients and multivariable linear regression models. We used two-sided p < 0.05 as the cutoff to include covariates in regression models. With regard to subgroup comparisons for menstrual pain, socialization, sex life, and product use, since we compare these ordinal (categorical) variables across subgroups, again, Pearson’s x2 test was used to assess statistical significance. All statistical analyses were performed using Python (version 3.12.0).
Results
A total of 1,037 respondents initially responded to the survey; 59 were excluded for being outside of the study’s age range (n = 14) or not biologically female (n = 45). An additional 604 with reproductive comorbidities were excluded, leaving a sample size of 374 naturally cycling US adult women of reproductive age to analyze (Figure 1). Out of 374 respondents, 14 women indicated that they had not had a menstrual cycle since the beginning of the pandemic and were further excluded, leaving a final sample size of 360 participants to analyze.
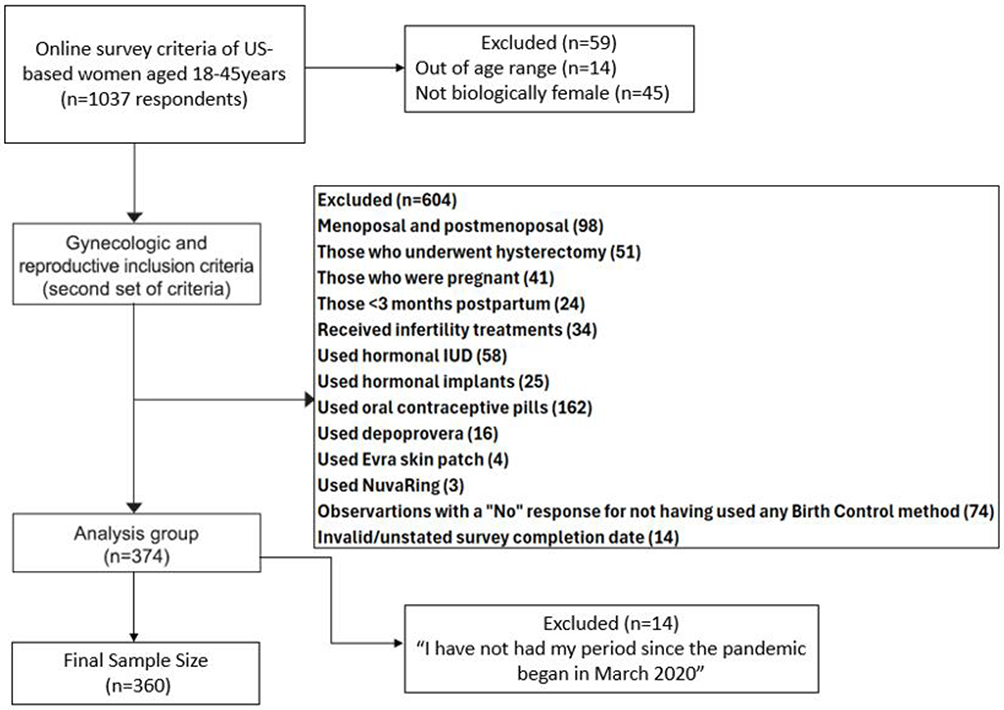 |
Figure 1 Schematic of Final Sample Size of Study Participants. |
As shown in Figure 2, the prevalence of moderate/severe menorrhagia was 30.0% (105 moderate and 3 severe). Since only 3 observations fell under the “severe” group, we re-categorized the sample into “Mild (AMSS score 0–33)” and “Moderate/Severe (AMSS score 34–100)”. Within the moderate/severe group however, the incidence was almost 40% (38.9%), meaning that for four in ten women who experienced moderate/severe menorrhagia during the COVID pandemic, this heavier bleeding pattern was new; a substantial difference from the mild group’s 13.1% incidence rate (p < 0.01) (Table 1).
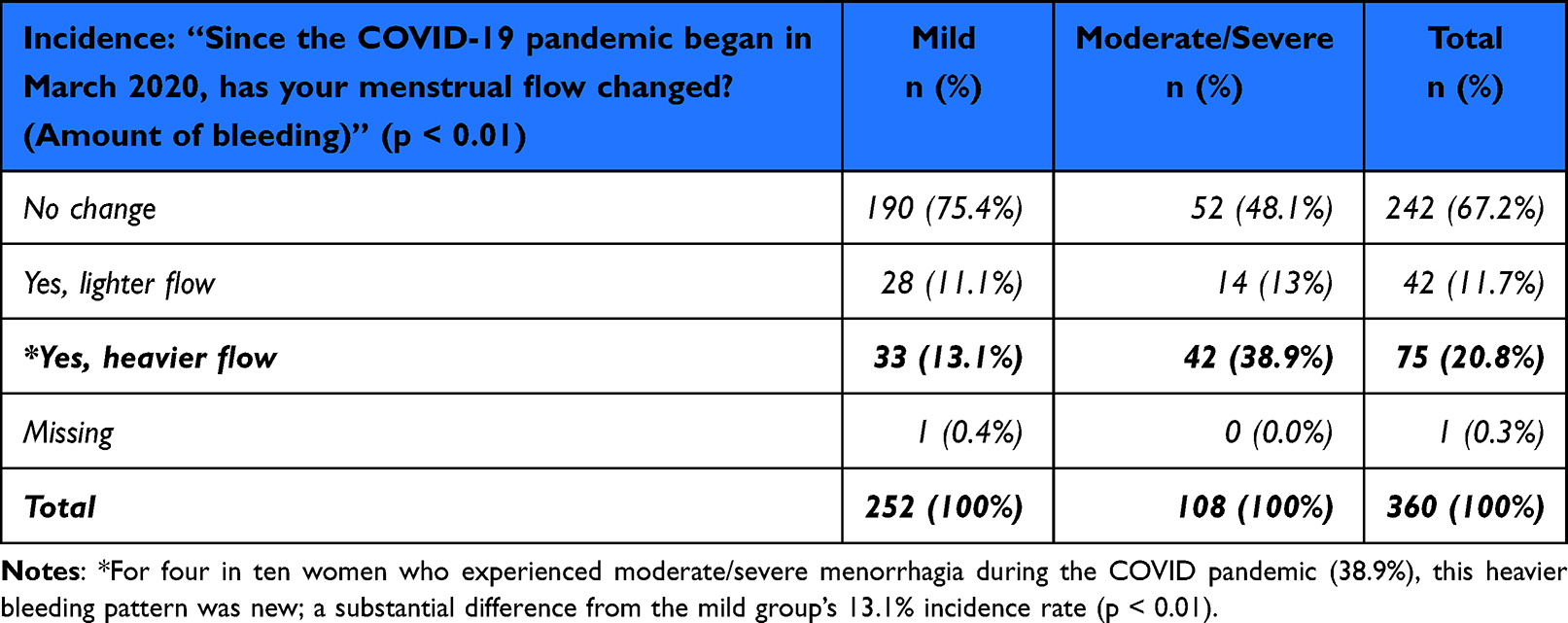 |
Table 1 Incidence of Menorrhagia During the COVID-19 Pandemic in Study Population (n = 360). Evaluated with the Aberdeen Menorrhagia Severity Scale (AMSS). Mild AMSS Score = 0–33; Moderate/Severe AMSS Score=34–100 |
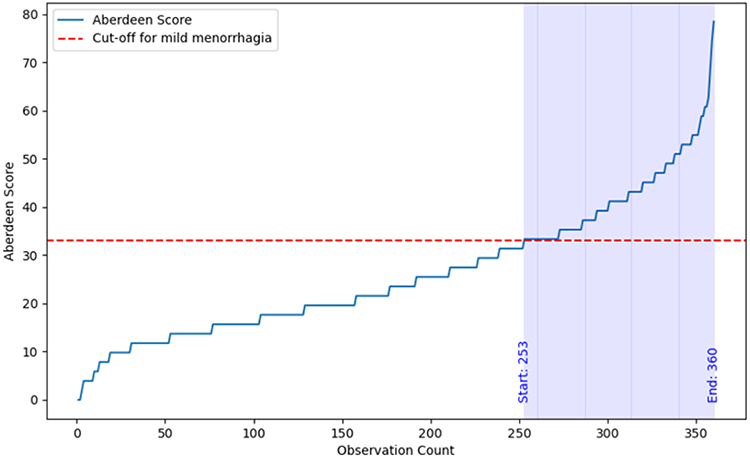 |
Figure 2 Prevalence of Menorrhagia during the COVID-19 Pandemic in the Study Population (n = 360). Evaluated with the Aberdeen Menorrhagia Severity Scale (AMSS). Mild AMSS score = 0–33; Moderate/Severe AMSS score = 34–100. |
Bivariate Analysis
Those with heavy bleeding tended to be African American/Black (p = 0.04), in unmarried relationships (p = 0.01), identify as current smokers (p < 0.01), have pre-pandemic clinical depression history (p < 0.01), and have a history of gynecological/reproductive comorbidities (p = 0.02) (Table 2).
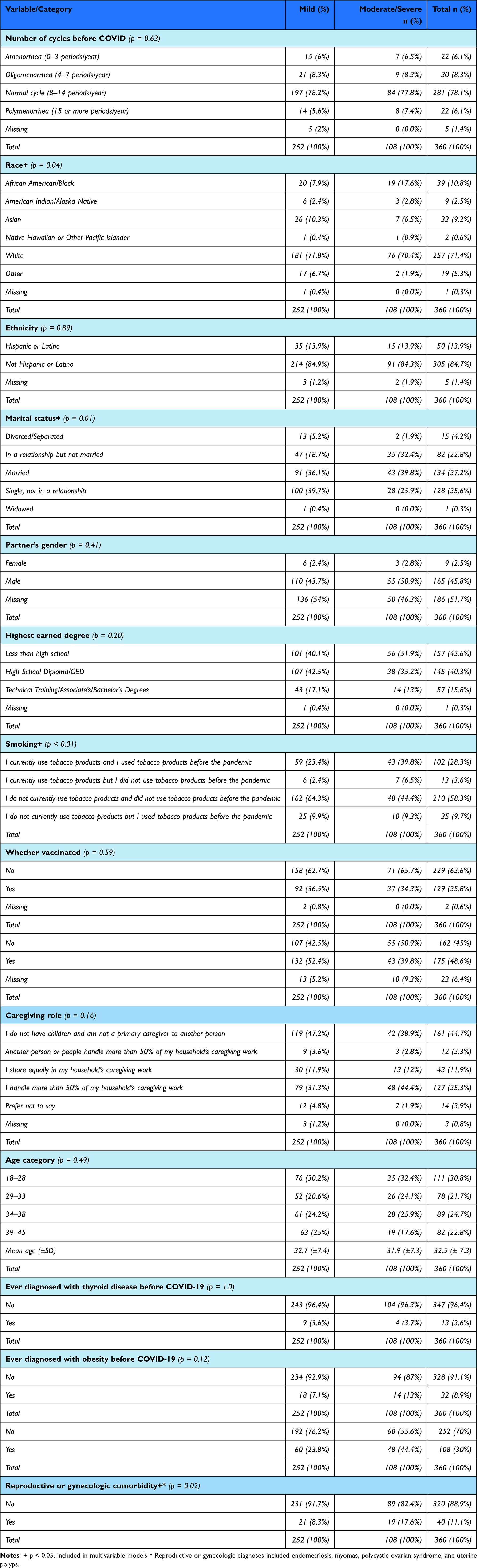 |
Table 2 Bivariate Comparison of Mild and Moderate/Severe Menorrhagia Groups (n = 360). Evaluated with the Aberdeen Menorrhagia Severity Scale (AMSS). Mild AMSS Score = 0–33; Moderate/Severe AMSS Score = 34–100 |
Pre-pandemic menstrual cycles did not differ between the groups (p = 0.63), with most women reporting normal menstrual cycles. There were also no group differences in education (p = 0.20), age (p = 0.49), parity (p = 0.06), thyroid abnormalities (p = 1.0), obesity (p=0.12), or vaccination status (p = 0.59).
Objective 1: COVID Stress and Menorrhagia
Those with heavy bleeding had higher COVID-stress scores than those without heavy bleeding (p < 0.01) (Table 3), and as hypothesized, there was a positive association between COVID stress and menorrhagia (Figure 3). Regression models further supported these findings and showed that, after accounting for relevant covariates, increases in COVID-stress scores were associated with 0.37 unit increases in menorrhagia scores (adj. β = 0.37, 95% CI: 0.21, 0.53; Table 4).
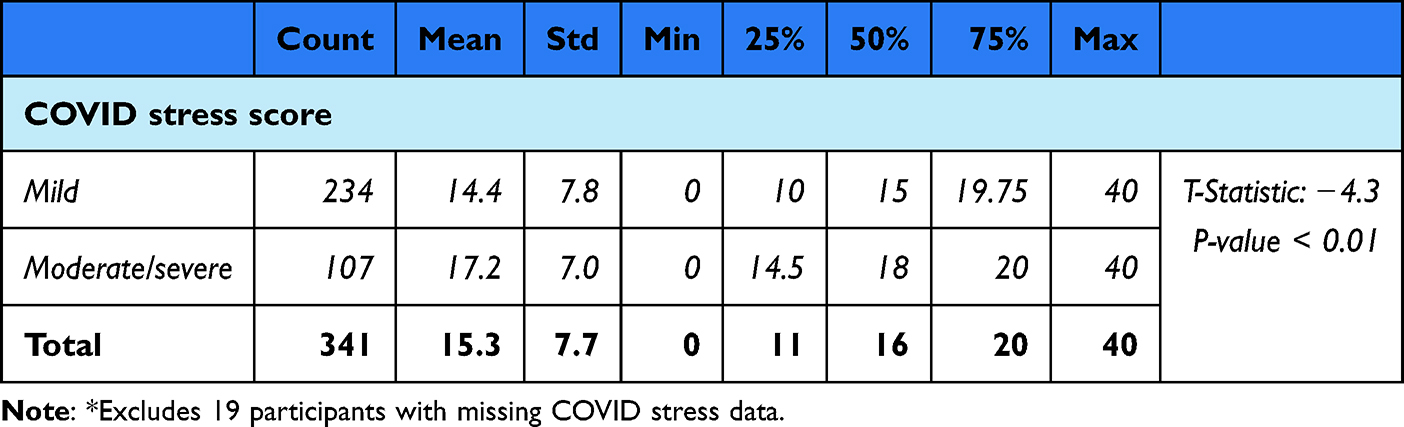 |
Table 3 Comparison of COVID Stress Scores for Participants with Mild Aberdeen Menorrhagia Severity Scale (AMSS) Scores (0–33) and Moderate/Severe Aberdeen Menorrhagia Severity Scale (AMSS) Scores (34–100). n = 341* |
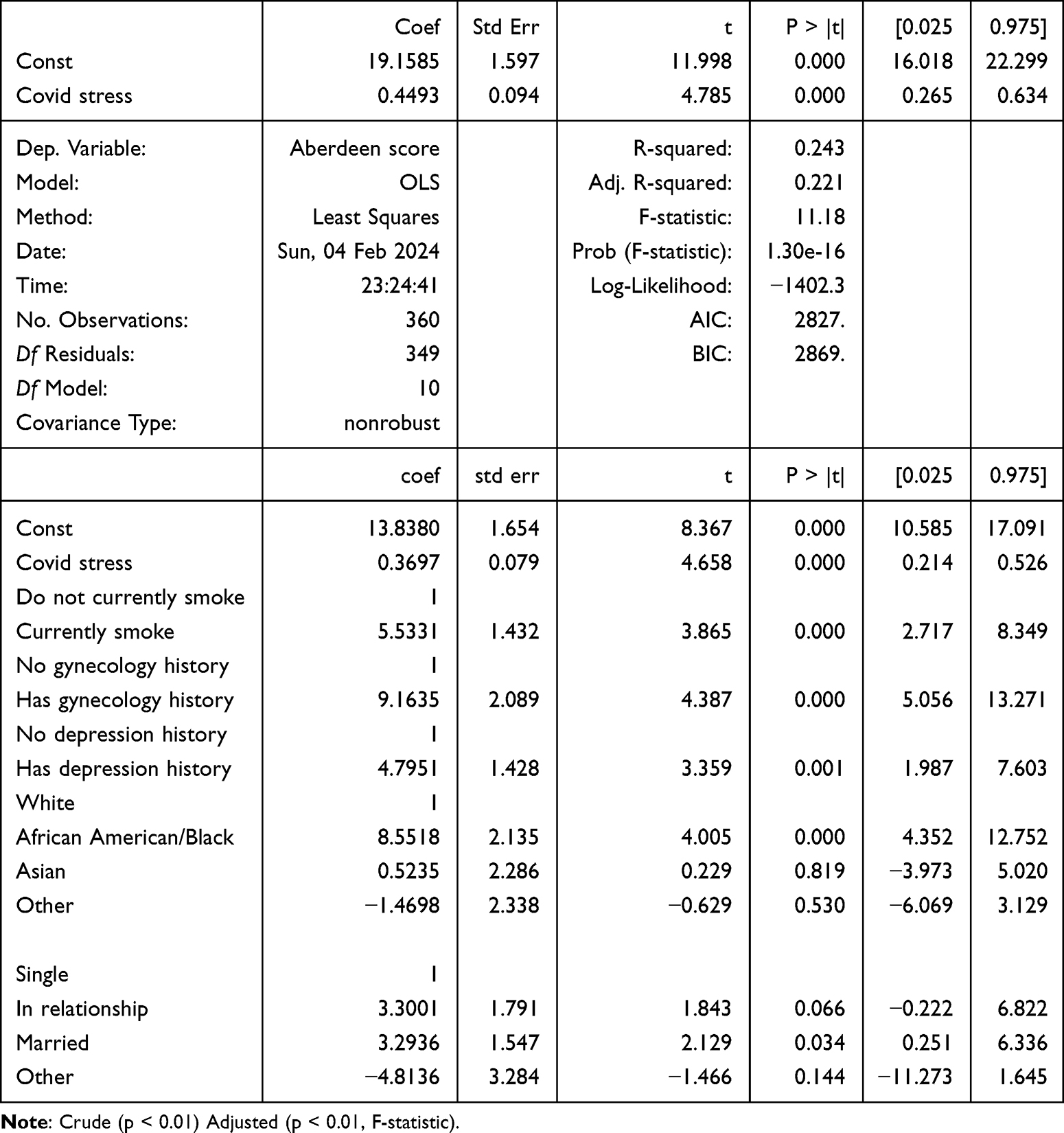 |
Table 4 Unadjusted and Adjusted Linear Regression Models of the Association Between COVID-Stress and Menorrhagia During the COVID-19 Pandemic (n = 360) |
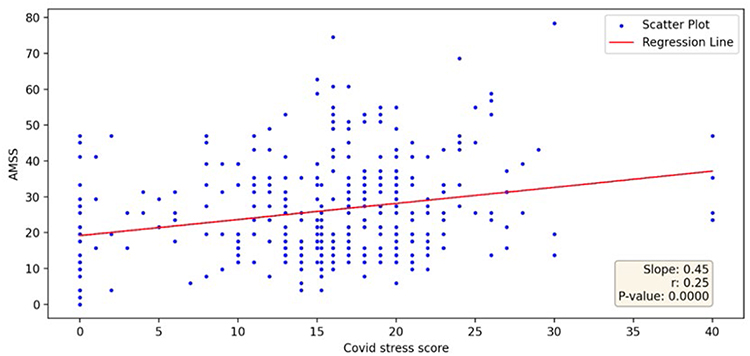 |
Figure 3 Scatter Plot of COVID Stress vs Heavy Menstrual Bleeding, Assessed with the Aberdeen Menorrhagia Severity Scale (AMSS), n = 341*. |
Objective 2: Menorrhagia and Mental Health
To assess the association between heavy bleeding and women’s mental health, we modeled the AMSS as the independent/predictor variable and the MHC as the dependent variable /outcome. As shown in the scatter plot of Figure 4, increased bleeding severity was associated with a decline in women’s mental health (p = 0.03). After accounting for baseline depression, regression models (Table 5) showed that an increase in women’s heavy bleeding was associated with worsened psychological well-being (adj. β = −0.1, 95% CI: −0.24, −0.03); as hypothesized.
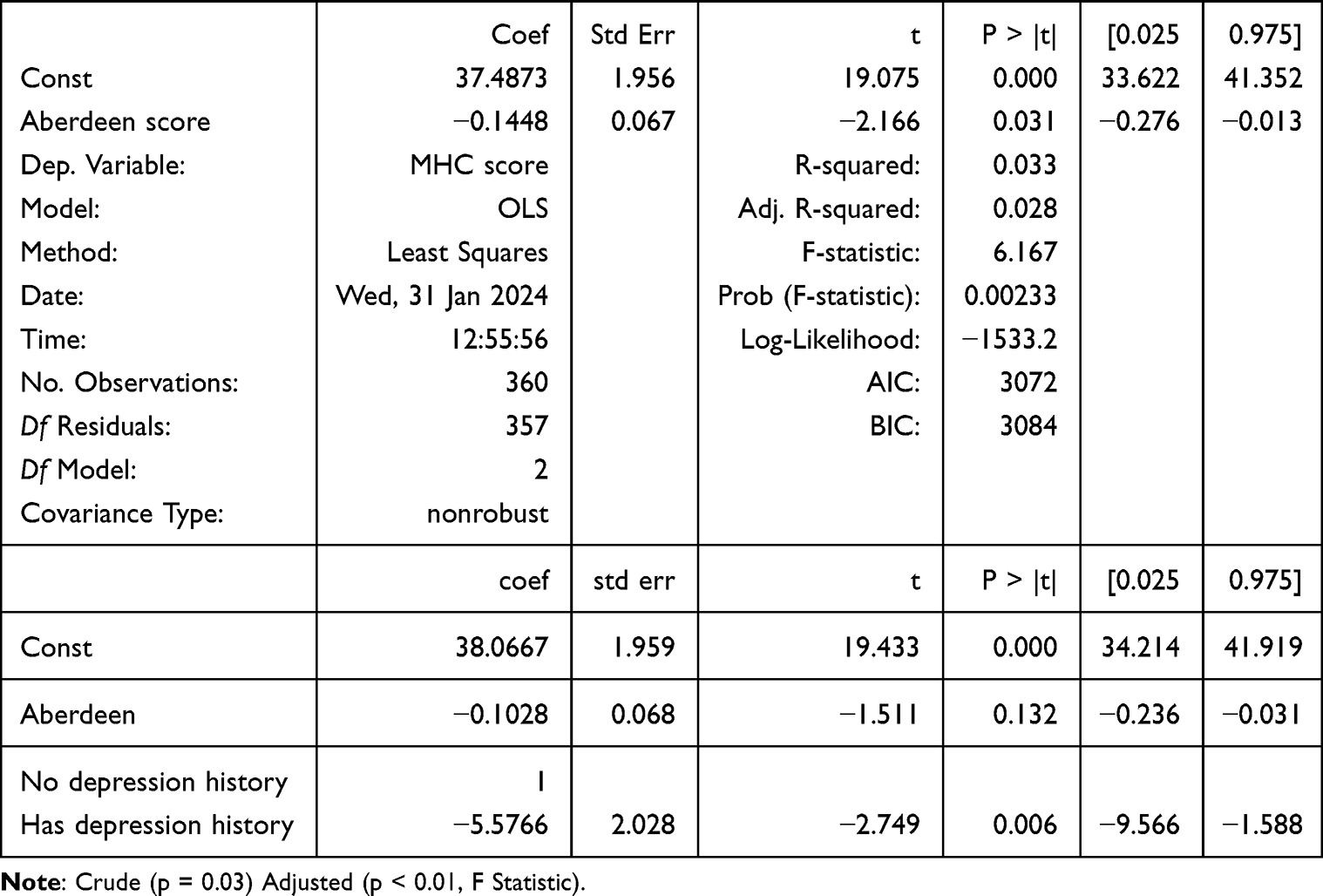 |
Table 5 Unadjusted and Adjusted Linear Regression Models of the Association Between Mental Health Measured by the Mental Health Continuum (MHC) Scale and Menorrhagia Measured by the Aberdeen Menorrhagia Severity Scale (AMSS) During the COVID-19 Pandemic (n = 360) |
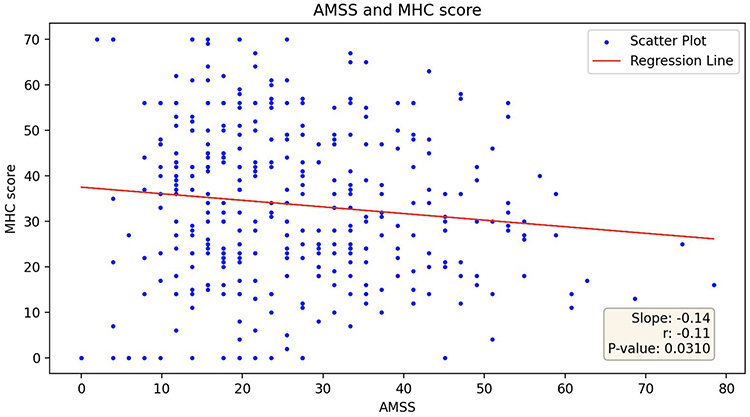 |
Figure 4 Scatter Plot of the Association Between Menorrhagia Measured by the Aberdeen Menorrhagia Severity Scale (AMSS) and Mental Health Measured by the Mental Health Continuum (MHC) Scale (n = 360). |
Objective 3: Women’s Lived Experiences with Heavy Bleeding During the COVID-19 Pandemic (TABLE 6)
As previously stated, we stratified key questions on the AMSS by mild bleeding (AMSS score = 0–33) and moderate/severe bleeding (AMSS score = 34–100) and compared participants’ responses to gain a deeper understanding of women’s lived experience with heavy menstrual bleeding during the pandemic. As previously stated, the selection of key questions was guided by the expertise of our ObGyn co-author SH, following the principles of Item Response Theory.30 All findings were statistically significant as shown in Table 6.
 |
Table 6 Examining Women’s Lived Experiences with Heavy Bleeding During the COVID-19 Pandemic. Mild Aberdeen Menorrhagia Severity Scale (AMSS) Scores (0–33) and Moderate/Severe Aberdeen Menorrhagia Severity Scale (AMSS) Scores (34–100); n = 360 |
With regard to menorrhagia and menstrual pain, compared to those with mild bleeding, women who experienced heavy menstrual bleeding were more likely to report severe/very severe pain as well as incapacitation due to their menorrhagia. When looking at the impact of menorrhagia on daily activities, socialization and sexual wellbeing, we found that compared to the mild group, more heavy bleeders reported that menorrhagia negatively affected their socialization and sex life, all potentially impacting their interpersonal relationships, affecting their overall quality of life. Regarding menorrhagia and menstrual product usage, the data showed that consistently, those with heavy bleeding reported needing to manage their flow with large quantities of menstrual products, at times needing to use multiple products simultaneously, including menstrual cups.
Discussion
Our first objective was to examine the relationship between COVID stress and menorrhagia. Findings from this study showed a positive association between COVID stress and menorrhagia (Figure 3). This suggests that women’s heavy bleeding experiences may have intensified with increasing experiences of COVID-related stress. At the time, the study was conducted - May 2021 - participants had already endured over a year of the pandemic. By April 2020, a month after the World Health Organization’s declaration of the global pandemic and amidst growing reports of intensified gender inequities,10,11 the United Nations Sustainable Development Group declared, that “across every sphere, from health to the economy, security to social protection, the burdens of COVID-19 are exacerbated for women and girls simply by virtue of their sex.13 The World Economic Forum further added that it would take at least 39 years to correct the gender setbacks imposed by the pandemic.12 It was against this backdrop that our study was conducted. A year into the pandemic, study participants were immersed in chronic pandemic stress, as mandatory lockdown and movement restrictions restricted access to childcare and household resources. Despite the overall incidence of heavy menstrual bleeding in our study, (20.8%) approximated population level estimates before (20%), and during the pandemic (18%),3,16 within the group of people who had heavy bleeding, the incidence was almost 40%. Meaning that for four in ten women in our sample who experienced heavy menstrual bleeding during the pandemic, this bleeding pattern was new. A menorrhagia incidence of 40%, though alarming, may not be surprising when contextualized. Out of the 1,031 participants included in a study by Phelan et al, 47% experienced heavy periods and 5% reported that their menorrhagia incidence had increased during the pandemic (p < 0.01).16 Additionally, 49% of the women they surveyed reported painful periods and 7% stated that the incidence of painful periods had also increased during the pandemic (p < 0.01). Similarly, Rehan et al corroborate our findings in a systematic review and report that increasing pandemic stress predicted heavier menstrual bleeding (p = 0.03), as well as increasing incidence of painful periods (p < 0.01).37 Aolymat et al further quantify these estimates and report that the incidence and severity of painful periods increased from 37% pre-pandemic to 50% during the pandemic in their study of Jordanian Medical Students.38 With limited care-seeking options, most self-medicated with over-the-counter pain relievers, such as ibuprofen and non-steroidal anti-inflammatory drugs (NSAIDs), which tend to be less effective than the gold standards of antifibrinolytics, progestogens, and combined hormonal contraceptives.39,40 Thus, many people with heavy bleeding received sub-optimal care during the pandemic. Poorly managed menorrhagia could result in a snowball of complications such as anemia, iron deficiency, and chronic pain syndrome.23 Fertility may be compromised, and the risk of pregnancy-related complications can be heightened, leading to subsequent declines in maternal and fetal outcomes.23
In our second objective, which was to examine the relationship between menorrhagia and mental health, we found that those with increased heavy bleeding also reported worse psychological well-being. The relationship between the menstrual cycle, COVID, and anxiety/stress has been referred to as a triangle, with each of the three impacting the other.41 Stress, particularly stress related to COVID-19, is well-documented as being linked to mental health outcomes,41–44 and several studies have found associations between COVID-19 related stress and changes to the menstrual cycle.14–16,34,41,45 However, it is important to note that this connection is significantly more pronounced in women with heavy menstrual bleeding, as demonstrated by our findings and the literature.14–16,46–48 Disregarding the underlying bleeding condition of these women, and assuming that their COVID stress and mental health challenges mirror those of the general population may lead to suboptimal clinical care. A systematic review investigating the relationship between psychological stress (including COVID-19, academic, and occupational stress) and menstrual cycle irregularity found that most studies report an association between psychological stress and menstrual dysfunction, with the most common disruptions being irregular menstruation and abnormal menstrual flow.46 The authors suggest that psychological stress is a modifiable risk factor for menstrual disorders, supporting the stress-to-menorrhagia pathway. In this research study, we investigate the triangular intersection of heavy menstrual bleeding, COVID-related stress, and mental health, with our findings revealing valid associations between these factors. Notably, 20% of women in our study experienced the onset of menorrhagia during the pandemic, which is a critical finding in the context of COVID-19. Although our study was cross-sectional and causality cannot be implied, the implications of this finding could include: increased patient load for obstetric and gynecological practitioners, greater mental health burden on psychological service providers, economic strain on patients due to higher consumption of menstrual products. Impact on patient (and their partners’) sexual health and well-being, potential long-term effects on fertility for women desiring pregnancy, deleterious impacts on patients’ overall quality of life. When heavy menstrual bleeding is effectively treated, it has been shown to reduce stress and improve mental health by addressing both the physical and psychological burdens of the condition.39 For example, research has shown that anemia resulting from prolonged heavy bleeding is a significant risk factor for depression. Treating the bleeding can alleviate anemia and, in turn, depressive symptoms. Hormonal treatments like contraceptives or other therapies that regulate bleeding can lead to decreased mood-related symptoms by stabilizing hormonal fluctuations.39 This research aims to advocate for the consideration and treatment of menorrhagia, as women’s reproductive health is integral to their overall well-being.
In our final objective, we examine women’s lived experiences with heavy bleeding during COVID. We found that compared to those with mild bleeding, women with heavy bleeding were more likely to report severe/very severe pain, incapacitation, negative changes to socialization and sex lives, and a need for large quantities of menstrual products, or needing to use multiple products simultaneously.
Self-management of heavy and painful menses was further compounded by the financial toll of the pandemic; particularly for those who needed to use multiple products simultaneously. The average menstruator spends approximately $13.25/month on menstrual products. For the approximately 40 years that they menstruate, this totals over $6000 on menstrual products per person (excluding taxes and inflation).49 For those with heavy bleeding, the financial burden can be crippling; particularly if one has to use combinations of tampons, pads and menstrual cups simultaneously. The cost of products during the pandemic - when many were experiencing financial burdens - may have further exacerbated the psychological toll of stress, which could in turn worsen menstrual bleeding patterns, necessitating more product usage, and leading to even more financial pressures.49,50 Due to this, the cycle of psychological stress for people with menstrual periods continues (Figure 5). Research shows that this vicious cycle of stress, menstruation, and poverty was especially worse for those who experienced a loss of income during COVID-19. Many resorted to using makeshift period products and/or prolonging their menstrual product usage, an unhygienic practice that has been associated with toxic shock syndrome and other medical conditions.50,51
 |
Figure 5 The Cycle of Stress, Menstruation, and Poverty. |
Proper clinical management of menorrhagia may have been even more critical during the pandemic due to the impact on patients’ psychosocial outcomes particularly their social isolation. Although menorrhagia is rarely life threatening, its impacts on one’s personal, family, social, and work life, as well as overall quality of life, can be profound. In fact, those with menorrhagia have described the loss or reduction of daily activities as more important than the actual volume of bleeding,52 and our findings support this assertion. Heavy bleeding was associated with worse mental health, even after accounting for depression history. Additionally, those with heavy bleeding reported more isolation, bed confinement, less socialization, and more impacts on their relationships. Social isolation, which co-occurs with loneliness, has been associated with elevated systolic blood pressure, increased risk for heart disease, stroke and dementia.53,54 The excessive bed confinement and limitations in socialization imposed by heavy bleeding in our study may put women with these experiences at even greater risk of being “a statistic” in the loneliness pandemic, increasing their susceptibility to downstream cardiovascular and neurological morbidity. Therefore, despite it being rarely life threatening, treatment of menorrhagia is imperative.
Human rights advocates have criticized governments, civil society organizations, and the international community for not incorporating a comprehensive gender analysis when setting the lockdown policies.9,11,13 COVID guidelines, they claim, failed to consider women’s unique health needs (compared to men’s), and the latitude necessary to manage their various obstetric and gynecological needs. The pandemic highlighted the need for more efficient processes to manage patients with menorrhagia; particularly those whose symptoms could not be alleviated with ibuprofen and other NSAIDs alone.39,40 Lapses in Internet access for minority patient populations (who are most prone to heavy bleeding as shown in our study), digital literacy (on the part of both patients and providers), and telehealth infrastructures made treatment in primary care settings difficult, and referral to secondary care close to impossible.40,55,56 Thankfully, telemedicine became common practice as the pandemic progressed. As mobile health (mHealth) applications (apps) gained ubiquity, insurance coverage and reimbursements improved, giving providers more latitude in their clinical decision-making. The apps facilitated appointment scheduling, communication, and management of reproductive care.57–59 These digital innovations left footprints that can be used to inform the clinical management of menorrhagia patients in the event of future pandemics. Data collected from mHealth and mobile device apps during the COVID-19 pandemic can be used to track the longitudinal impact of heavy bleeding on people’s reproductive life course, including treatment, delays in care seeking, (in)fertility, and other relevant outcomes.57
Limitations
To our knowledge, this study is one of a few to evaluate women’s lived experiences with heavy bleeding and menstrual product use during the COVID-19 pandemic across the United States. The study is not without limitations, however. The first is the lack of objective assessments of menorrhagia. Correlating women’s subjective reporting of blood loss with objective, quantifiable measures of blood loss, eg, with menstrual pictograms,58,60 would have strengthened the study. However, research shows that the validity of women’s self-reports of their own reproductive histories compared with medical records and other gold standards, ranges from 92.9% to 100%, implying that the probability of recall bias is low.58 Additionally, while objective quantification of menstrual blood loss may be valuable for research purposes, the subjective impact of menorrhagia on a patient’s mental health and quality of life may be of greater clinical relevance. A patient with 80 mL of blood loss/period who reports “moderate” menstrual pain accompanied by less than a day of bed confinement, moderate impact on socialization, and needing only 2 sanitary pads for protection is substantially different from another with the same amount of loss, who reports severe menstrual pain, a day or more of bed confinement, severely impacted socialization, and requiring multiple menstrual products to manage their flow. Studies aimed at validating people’s self-reports should not discount their lived experiences. These subjective reports are critical for assessing the severity of the menorrhagia, and subsequent responses to treatment.58
A second limitation is the cross-sectional study design, and the lack of longitudinal data to assess the chronicity of menorrhagia, particularly for the incidental cases. Did these women’s heavy bleeding resolve after the pandemic? How long did that take? What types of treatment did they receive if clinical management was necessary? What was the underlying pathology for the bleeding? Was it merely stress or were there underlying coagulopathies and malignancies?61 Future studies that compare the long-term psychosocial and physiological outcomes of those with and without heavy bleeding prospectively will allow reproductive epidemiologists to better assess the impact of menorrhagia beyond the pandemic. Such longitudinal data could help clinicians and researchers understand the long-term impact of pandemics on menstruator’s reproductive health, including their fertility outcomes.
A third limitation is that, although we report statistically significant associations between COVID stress and several adverse menstrual effects, the regression “r” values were low (as also would be the r2 values), indicating that stress did not explain the majority of variation around the mean. Thus, COVID stress is a factor, but not the only factor in explaining the menstrual changes occurring during the pandemic. It is important to clarify that the aim of this study was not to establish causal relationships between these variables. Rather, our goal was to highlight these associations and influence future research endeavors to meaningfully unpack the associations between menstrual changes and other pandemic-related experiences.
Finally, there may be groups of individuals who menstruate but do not self-identify as women. Our study focused on the lived experiences of those who self-identify as women, limiting its generalizability. More research on the former group is needed to better understand their unique experiences and challenges related to menstruation, as well as how these intersect with gender identity and broader social factors.
These noted limitations are counterbalanced by the particular strengths of our study design including the ability to generate a broadly cross-sectional cohort that represents the regional and demographic distribution of the United States population. Within this cross section, we sought to elicit in qualitative and quantitative fashion the details of menstruating people’s lived experiences with bleeding before and during the COVID-19 pandemic. Although exploring menstrual bleeding patterns in women who were not actively menstruating (eg, menopausal, pregnant, or taking hormonal birth control) was scientifically unsound—and therefore the study’s findings are not generalizable to these groups—the insights gained remain highly relevant. The data can still inform policy development and clinical guidelines specifically for actively bleeding women—those for whom COVID stress appears to have a direct impact on the menstrual health. For instance, screening protocols could incorporate stress assessments as part of a broader diagnostic framework for women with unexplained heavy bleeding, allowing for early identification and intervention. Additionally, the findings highlight the need for mental health support and stress reduction interventions targeted at this population to address the biological pathways connecting stress and heavy menstrual bleeding. Furthermore, even though the study focused on actively bleeding women, it raises another critical question: how does stress impact those not actively bleeding, such as women under the psychological strain of the COVID-19 pandemic or other life stressors? While these women may not be present with menorrhagia, the biological effects of stress could manifest as changes to menstrual patterns, hormonal fluctuations, or mental health challenges. Exploring these dynamics could provide insights into how environmental stressors influence reproductive and mental health over time and inform a broader public health response.
By applying the study findings to shape interventions for actively bleeding women while also examining the ripple effects of stress on those not actively bleeding (eg, through COVID-related stress or other psychological factors), healthcare systems can adopt more nuanced and proactive approaches to address the mental health and reproductive health needs of diverse populations.
Conclusion
Our study found that there is a relationship present between COVID stress and menorrhagia as well as menorrhagia and mental health. Additionally, we examined the lived experiences of women with heavy bleeding and found that they face numerous challenges that they attribute to their bleeding. An increasing body of evidence is emerging to characterize the reproductive implications of living during a global pandemic. The etiologies of observed reproductive implications are likely multi-factorial, representing not only the body’s response to infection and stress but also complex interactions between life-course disruption, changes in physical activity, modifications to interpersonal interactions, financial strain, and psychological stress. This work seeks to apply validated psychological and menstrual inventories to detail interactions between COVID-associated stress and menstrual changes towards the goal of better understanding elements of these complex interactions. Although the reported correlation coefficients are generally characterized as “weak” our survey data provide evidence suggesting that these relationships are likely meaningful and non-trivial. We encourage future research to explore the complex and dynamic connections between stress, mental health, and menstrual health in greater depth. Additionally, future studies should attempt to look into the lived experiences of nonbinary and transgender individuals who menstruate in order to get clearer and more generalizable findings related to heavy bleeding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nicholson WK, Ellison SA, Grason H, Powe NR. Patterns of ambulatory care use for gynecologic conditions: a national study. Am J Obstet Gynecol. 2001;184(4):523–530. doi:10.1067/mob.2001.111795
2. Cw WMH, Borger J. Menorrhagia. StatPearls Publishing; 2024. https://www.ncbi.nlm.nih.gov/books/NBK536910/.
3. Division of Blood Disorders. National center on birth defects and developmental disabilities, centers for disease control and prevention. Heavy Menstrual Bleeding, Available from:, https://www.cdc.gov/ncbddd/blooddisorders/women/menorrhagia.html#:~:text=Menorrhagia%20is%20menstrual%20bleeding%20that,larger%2C%20that%20is%20heavy%20bleeding.
4. Mayo Clinic. Heavy menstrual bleeding. Available from:, https://www.mayoclinic.org/diseases-conditions/menorrhagia/symptoms-causes/syc-20352829.
5. Figà-Talamanca I. Occupational risk factors and reproductive health of women. Occupational Medicine. 2006;56(8):521–531. doi:10.1093/occmed/kql114
6. Kwak Y, Kim Y, Baek KA. Prevalence of irregular menstruation according to socioeconomic status: a population-based nationwide cross-sectional study. PLoS One. 2019;14(3):e0214071. doi:10.1371/journal.pone.0214071
7. Chrousos GP, Torpy DJ, Gold PW. Interactions between the hypothalamic-pituitary-adrenal axis and the female reproductive system: clinical implications. Ann Intern Med. 1998;129(3):229–240. doi:10.7326/0003-4819-129-3-199808010-00012
8. Mitra A, Verbakel JY, Kasaven LS, et al. The menstrual cycle and the COVID-19 pandemic. PLoS One. 2023;18(10):e0290413. doi:10.1371/journal.pone.0290413
9. Fisseha S, Sen G, Ghebreyesus TA, et al. COVID-19: the turning point for gender equality. Lancet. 2021;398(10299):471–474. doi:10.1016/s0140-6736(21)01651-2
10. Zamarro G, Prados MJ. Gender differences in couples’ division of childcare, work and mental health during COVID-19. Rev Econ Househ. 2021;19(1):11–40. doi:10.1007/s11150-020-09534-7
11. Mwenyango H. Impact of COVID-19 pandemic on women’s rights and wellbeing: analysis of the Ugandan response to the global virus. J Hum Rights Soc Work. 2023;8(1):105–113. doi:10.1007/s41134-022-00229-w
12. World Economic Forum. The pandemic has hurt women’s health. this is why that’s bad for everyone. Available from:, https://www.weforum.org/agenda/2021/09/lessons-must-be-learned-from-covid-19-s-impact-on-women-s-health-and-rights/.
13. United Nations Women. UN secretary-general’s policy brief: the impact of COVID-19 on women. Available from:, https://www.unwomen.org/en/digital-library/publications/2020/04/policy-brief-the-impact-of-covid-19-on-women.
14. Anto-Ocrah M, Valachovic T, Chen M, et al. Coronavirus Disease 2019 (COVID-19)-related stress and menstrual changes. Obstet Gynecol. 2023;141(1):176–187. doi:10.1097/aog.0000000000005010
15. Ozimek N, Velez K, Anvari H, Butler L, Goldman KN, Woitowich NC. Impact of stress on menstrual cyclicity during the coronavirus disease 2019 Pandemic: a Survey Study. J Women's Health. 2022;31(1):84–90. doi:10.1089/jwh.2021.0158
16. Phelan N, Behan LA, Owens L. the Impact of the COVID-19 pandemic on women’s reproductive health. Front Endocrinol. 2021;12:642755. doi:10.3389/fendo.2021.642755
17. Doğan E, Uncu B, Duman R. Comparison of menstrual cycle irregularities among young women based on coronavirus disease 2019 infection status: a cross-sectional study. Rev Assoc Med Bras. 2024;70(2):e20230801. doi:10.1590/1806-9282.20230801
18. Bell AJ, Afulani P, Compton S, et al. Understanding how COVID-19 affected black pregnant women early in the pandemic: a cross-sectional survey. Midwifery. 2024;130:103915. doi:10.1016/j.midw.2024.103915
19. Maher M, Owens L. SARS-CoV-2 infection and female reproductive health: a narrative review. Best Pract Res Clin Endocrinol Metab. 2023;37(4):101760. doi:10.1016/j.beem.2023.101760
20. Norris KG, Huang PA, Glantz JC, Kodam RS, Anto-Ocrah M. A cross-cultural analysis of the COVID-19 Pandemic’s impact on antenatal healthcare-seeking behaviors in Ghana and the United States. J Patient Exp. 2021;8:23743735211062392. doi:10.1177/23743735211062392
21. de Oliveira L, Carvalho J. Women’s Sexual Health During the Pandemic of COVID-19: declines in Sexual Function and Sexual Pleasure. Curr Sex Health Rep. 2021;13(3):76–88. doi:10.1007/s11930-021-00309-4
22. Diamond-Smith N, Logan R, Marshall C, et al. COVID-19’s impact on contraception experiences: exacerbation of structural inequities in women’s health. Contraception. 2021;104(6):600–605. doi:10.1016/j.contraception.2021.08.011
23. Latthe P, Latthe M, Say L, Gülmezoglu M, Khan KS. WHO systematic review of prevalence of chronic pelvic pain: a neglected reproductive health morbidity. BMC Public Health. 2006;6:177. doi:10.1186/1471-2458-6-177
24. National Center for Health Statistics, Centers for Disease Control and Prevention,. 2022. Available from:, https://www.cdc.gov/nchs/hus/sources-definitions/incidence.htm#:~:text=Incidence-,Incidence,Acknowledgments.
25. Ruta DA, Garratt AM, Chadha YC, Flett GM, Hall MH, Russell IT. Assessment of patients with menorrhagia: how valid is a structured clinical history as a measure of health status? Qual Life Res. 1995;4(1):33–40. doi:10.1007/bf00434381
26. Matteson KA, Boardman LA, Munro MG, Clark MA. Abnormal uterine bleeding: a review of patient-based outcome measures. Fertil Steril. 2009;92(1):205–216. doi:10.1016/j.fertnstert.2008.04.023
27. Piccardo A, Siri G, Ugolini M, et al. A three-domain scoring system to customize the risk of relapse of differentiated thyroid carcinoma. Cancers. 13(17). doi:10.3390/cancers13174335
28. Alharbi AH, AlSindi T, Ashoor AF, et al. The use of pain severity and its impact as a predictor for MRI findings: a cross-sectional study in Ta’if, Saudi Arabia. Cureus. 2023;15(9):e45463. doi:10.7759/cureus.45463
29. Streiner DL, Norman GR, Cairney J. Health measurement scales: a practical guide to their development and use.
30. Murray AL, Booth T. Item Response Theory. In: Zeigler-Hill V, Shackelford TK, editors. Encyclopedia of Personality and Individual Differences. Springer International Publishing; 2017:1–4.
31. P-CM C-A-A, Pedrozo-Pupo JC. pandemic-related perceived stress scale of COVID-19: an exploration of online psychometric performance.Rev Colomb Psiquiatr. 2020;49:229–230. doi:10.1016/j.rcp.2020.05.005
32. Corey LK. Mental health continuum short form (MHC-SF). Updated 06-28-2023. Available from:, https://www.psytoolkit.org/survey-library/mhc-sf.html.
33. Harris E. COVID-19 vaccine and health care visits for menstrual changes. JAMA. 2023;329(21):1817. doi:10.1001/jama.2023.8658
34. Nazir M, Asghar S, Rathore MA, et al. Menstrual abnormalities after COVID-19 vaccines: a systematic review. 10.1016/j.vacun.2022.07.001. Vacunas. 2022;23:S77–S87. doi:10.1016/j.vacun.2022.07.001
35. Gibson EA, Li H, Fruh V, et al. COVID-19 vaccination and menstrual cycle length in the apple women’s health study. medRxiv. 2022. doi:10.1101/2022.07.07.22277371
36. Ibrahim PM, Samwel EL. Prevalence of heavy menstrual bleeding and its associated factors among women attending kilimanjaro Christian medical centre in northern eastern, Tanzania: a cross-sectional study. East Afr Health Res J. 2023;7(1):1–6. doi:10.24248/eahrj.v7i1.702
37. Tayyaba Rehan S, Imran L, Mansoor H, et al. Effects of SARS-CoV-2 infection and COVID-19 pandemic on menstrual health of women: a systematic review. Health Sci Rep. 2022;5(6):e881. doi:10.1002/hsr2.881
38. Aolymat I, Khasawneh AI, Al-Tamimi M. COVID-19-associated mental health impact on menstrual function aspects: dysmenorrhea and premenstrual syndrome, and genitourinary tract health: a cross sectional study among Jordanian medical students. Int J Environ Res Public Health. 2022;19(3). doi:10.3390/ijerph19031439
39. Bofill Rodriguez M, Lethaby A, Farquhar C, Duffy JM. Interventions commonly available during pandemics for heavy menstrual bleeding: an overview of Cochrane Reviews. Cochrane Database Syst Rev. 2020;7(7):Cd013651. doi:10.1002/14651858.CD013651.pub2
40. Winters U, Ghosh M, Shelleh A. Heavy menstrual bleeding management during the Covid pandemic. Obstet Gynaecol Reprod Med. 2021;31(2):53–58. doi:10.1016/j.ogrm.2020.12.002
41. Demir O, Sal H, Comba C. Triangle of COVID, anxiety and menstrual cycle. J Obstet Gynaecol. 2021;41(8):1257–1261. doi:10.1080/01443615.2021.1907562
42. Serafini G, Parmigiani B, Amerio A, Aguglia A, Sher L, Amore M. The psychological impact of COVID-19 on the mental health in the general population. Qjm. 2020;113(8):531–537. doi:10.1093/qjmed/hcaa201
43. Zhu C, Zhang T, Li Q, Chen X, Wang K. Depression and anxiety during the COVID-19 pandemic: epidemiology, mechanism, and treatment. Neurosci Bull. 2023;39(4):675–684. doi:10.1007/s12264-022-00970-2
44. Chaudhary R, Rohilla M, Chauhan S, et al. The pandemic’s unseen wounds: COVID-19’s profound effects on mental health. Ann Med Surg. 2023;85(10):4954–4963. doi:10.1097/ms9.0000000000001223
45. Muharam R, Agiananda F, Budiman YF, et al. Menstrual cycle changes and mental health states of women hospitalized due to COVID-19. PLoS One. 2022;17(6):e0270658. doi:10.1371/journal.pone.0270658
46. Poitras M, Shearzad F, Qureshi AF, Blackburn C, Plamondon H. Bloody stressed! A systematic review of the associations between adulthood psychological stress and menstrual cycle irregularity. Neurosci Biobehav Rev. 2024;163:105784. doi:10.1016/j.neubiorev.2024.105784
47. Strine TW, Chapman DP, Ahluwalia IB. Menstrual-related problems and psychological distress among women in the United States. J Women's Health. 2005;14(4):316–323. doi:10.1089/jwh.2005.14.316
48. Aolymat I, Al-Tamimi M, Almomani H, et al. COVID-19-associated mental health impact on menstruation physiology: a survey study among medical students in Jordan. Women's Health. 2023;19:17455057221150099. doi:10.1177/17455057221150099
49. Ballard Brief. Period Poverty in the United States. https://ballardbrief.byu.edu/issue-briefs/period-poverty-in-the-united-states#:~:text=In%20the%2040%20years%20on,having%20their%20own%20sales%20tax.
50. Rohatgi A, Dash S. Period poverty and mental health of menstruators during COVID-19 pandemic: lessons and implications for the future. Front Glob Women's Health. 2023;4:1128169. doi:10.3389/fgwh.2023.1128169
51. Schmitt ML, Dimond K, Maroko AR, et al. “I stretch them out as long as possible:” U.S. women’s experiences of menstrual product insecurity during the COVID-19 pandemic. BMC Women's Health. 2023;23(1):179. doi:10.1186/s12905-023-02333-z
52. Gokyildiz S, Aslan E, Beji NK, Mecdi M. The Effects of menorrhagia on women’s quality of life: a case-control study. ISRN Obstet Gynecol. 2013;2013:918179. doi:10.1155/2013/918179
53. Hwang TJ, Rabheru K, Peisah C, Reichman W, Ikeda M. Loneliness and social isolation during the COVID-19 pandemic. Int Psychogeriatr. 2020;32(10):1217–1220. doi:10.1017/s1041610220000988
54. Ernst M, Niederer D, Werner AM, et al. Loneliness before and during the COVID-19 pandemic: a systematic review with meta-analysis. Am Psychol. 2022;77(5):660–677. doi:10.1037/amp0001005
55. Kern-Goldberger AR, Srinivas SK. Obstetrical telehealth and virtual care practices during the COVID-19 Pandemic. Clin Obstet Gynecol. 2022;65(1):148–160. doi:10.1097/grf.0000000000000671
56. How OBGYNs adapted provision of sexual and reproductive health Care during the COVID-19 Pandemic. Available from:, https://www.kff.org/womens-health-policy/issue-brief/how-obgyns-adapted-provision-of-sexual-and-reproductive-health-care-during-the-covid-19-pandemic/.
57. Critchley HOD, Babayev E, Bulun SE, et al. Menstruation: science and society. Am J Obstet Gynecol. 2020;223(5):624–664. doi:10.1016/j.ajog.2020.06.004
58. Quinn SD, Higham J. Outcome measures for heavy menstrual bleeding. Women's Health. 2016;12(1):21–26. doi:10.2217/whe.15.85
59. Harvard Medical School News and Research. Telemedicine can change care for the better — with the right rules. Available from:, https://hms.harvard.edu/news/telemedicine-can-change-care-better-right-rules?utm_source=AcousticMailing&utm_medium.
60. Janssen CA, Scholten PC, Heintz AP. A simple visual assessment technique to discriminate between menorrhagia and normal menstrual blood loss. Obstet Gynecol. 1995;85(6):977–982. doi:10.1016/0029-7844(95)00062-v
61. Mishra D, Sultan S. FIGO’s PALM–COEIN classification of abnormal uterine bleeding: a clinico-histopathological correlation in Indian setting. J Obstet Gynaecol India. 2017;67(2):119–125. doi:10.1007/s13224-016-0925-8
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Psychosocial Problems Among Primary School Children in Thailand During the COVID-19 Pandemic, 2022
Pudpong N, Julchoo S, Sinam P, Uansri S, Kunpeuk W, Suphanchaimat R
Pediatric Health, Medicine and Therapeutics 2023, 14:159-168
Published Date: 20 May 2023