Back to Journals » Advances in Medical Education and Practice » Volume 17
BLEED TIME Simulation Study – Bleeding Limb, Effectiveness and Efficiency in Determining Time to Intervene on Mangled Extremity
Authors Bikman TJ ![]() , Selde WF, Belk WB
, Selde WF, Belk WB ![]() , Pathak M, Palm CE
, Pathak M, Palm CE ![]() , Thompson SJ
, Thompson SJ ![]()
Received 3 September 2025
Accepted for publication 19 December 2025
Published 8 January 2026 Volume 2026:17 560800
DOI https://doi.org/10.2147/AMEP.S560800
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sateesh Arja
Timothy J Bikman,1,2 William F Selde,1 William B Belk,3 Manoj Pathak,4 Craig E Palm,5 Simon J Thompson6
1Emergency Department, Billings Clinic, Billings, MT, USA; 2Simulation Experiential Learning Laboratory, Billings Clinic, Billings, MT, USA; 3Medical Simulation & Innovative Education, Air Methods Corporation, Greenwood Village, CO, USA; 4Department of Mathematics & Statistics, Murray State University, Murray, KY, USA; 5Trauma Services, Billings Clinic, Billings, MT, USA; 6Collaborative Science & Innovation, Billings Clinic, Billings, MT, USA
Correspondence: Simon J Thompson, Collaborative Science & Innovation, Billings Clinic, Billings, MT, USA, Tel +1 503 267 7314, Fax +1 406 435 1586, Email [email protected]
Purpose: Simulation-based education plays a pivotal role in preparing healthcare providers for rare, high-acuity emergencies such as hemorrhagic extremity trauma. Advances in simulation fidelity, including hemorrhagic pumping systems (HPS), may enhance realism, urgency, and clinical decision-making. However, evidence on how such enhancements affect provider performance remains limited.
Patients and Methods: In this randomized case-control study at a rural Level I trauma center simulation learning laboratory, emergency care providers (n = 146) managed a simulated extremity trauma scenario using either standard moulage (Group A; No HPS) or an active HPS (Group B). Participants were stratified by profession/licensure prior to recruitment. Within each professional stratum participants were randomized to ensure balanced representation, into the two groups and the timed endpoints included (i) First Intervention, (ii) Tourniquet-only Application, and (iii) Scenario Completion. Subgroup analyses were conducted by healthcare license (Emergency Medical Technician (EMT), Registered Nurse (RN), Others (neither EMT or RN licensure)) and years of licensure (< 5 vs ≥ 5 years).
Results: Participants using the HPS performed the first intervention significantly faster (mean = 54.9s) than those with No HPS (mean = 71.9s; p=0.002). EMTs and “Others” showed significant time improvements with HPS use, while RN performance did not differ. Tourniquet-only and Scenario Completion times were unaffected by HPS presence. Among RNs, those with < 5 years of experience performed significantly faster in the first intervention than their more experienced peers (p=0.039); no other timing differences reached statistical significance based on licensure length.
Conclusion: Enhanced realism within simulation-based education incorporating dynamic bleeding systems improves response time in initial trauma interventions, particularly among EMTs and less-experienced providers. While total scenario times and tourniquet application did not differ, early engagement appears positively influenced by simulation fidelity. Integrating high-fidelity elements like HPS into trauma training may strengthen learner urgency, decision-making, and improve real-world provider readiness.
Plain Language Summary: This study explored how realistic bleeding simulations affect emergency care providers’ response times to a serious leg or arm injury. The goal was to see if adding a system that mimics real bleeding (called a hemorrhagic pumping system, or HPS) could improve how quickly and effectively providers react in a training scenario.
Researchers tested 146 emergency workers at a rural trauma center. About half of them used a standard setup with no active bleeding (Group A), while the rest used a more realistic system that included simulated bleeding (Group B). They measured how long it took participants to start treating the injury, apply a tourniquet, and complete the full scenario.
The study found that those who used the bleeding system started treatment faster, about 17 seconds quicker on average. This improvement was especially true for Emergency Medical Technicians (EMTs) and providers without specific nursing or EMT licenses. Nurses did not show a difference overall, but newer nurses (with less than five years of experience) responded faster than more experienced ones.
Adding realistic bleeding did not change how fast tourniquets were applied or how long the entire scenario took to complete. However, it did make a difference in how quickly providers reacted at the start.
In summary, using more realistic bleeding in trauma simulations helps improve early response times, especially for newer or non-nurse providers. This suggests that adding lifelike features such as active bleeding to training could better prepare emergency workers for real-world trauma situations.
Keywords: medical simulation training, emergency medical services, clinical decision-making, dynamic bleeding models, high fidelity simulation training, trauma education
Introduction
Simulation-based education has become a critical component of medical training, particularly in the preparation for low-frequency, high-acuity events1 such as life-threatening traumatic limb injuries.2 It provides a controlled and risk-free environment in which healthcare professionals can systematically identify and address potential challenges in clinical practice.3 Timely intervention in hemorrhagic extremity trauma is well established as a critical determinant of patient outcomes, with much of the foundational evidence originating from military medicine.4,5 While such injuries are rare, approximately 1% of all extremity traumatic injuries in civilian practice,6 they carry substantial morbidity and mortality when they do occur,7 and are largely preventable.8 This led the American College of Surgeons to develop civilian strategies to improve victim survival with input from medical, law enforcement, fire/ rescue, emergency medical service first responders, and military experts,9 which steered the “Stop the Bleed” initiative.10
The degree to which moulage is used in the simulated environment is varied; that is, there is no guide for how authentic it is required to be.11 Given the combination of low incidence and high risk, simulation provides a unique opportunity to bridge the educational gap12 and prepare providers for rare but life-saving interventions. Advances in simulation technology have opened the door to more realistic and immersive training modalities. Among these is the use of dynamic bleeding systems, which simulate active bleeding, potentially increasing learner engagement and altering clinical decision-making behavior.13
Repetition and deliberate practice in realistic environments has been shown to improve both individual performance and patient outcomes.14 However, there remains a relative paucity of research exploring how differing simulation approaches, particularly those involving bleeding control, impact learner behavior and training effectiveness. One related study15 informed this project development and underscores the emerging interest in the area.
This study explores whether enhanced realism through the use of an active bleeding pump system influences emergency care providers’ response times in a simulated extremity trauma scenario. We hypothesized that participants exposed to active bleeding would demonstrate a shorter time to intervention compared to those using traditional moulage. Moreover, experienced medical practitioners assess patient status in distinct ways compared to novices, potentially impacting the effectiveness of simulated bleeding control interventions.16
This study compares traditional moulage with a high-fidelity bleeding system in trauma simulation. Our objectives are: (A) to evaluate learner performance using time-based measures, time to first intervention, time to tourniquet application, and total scenario time, across the two simulation methods; and (B) to examine differences in learner behavior and decision-making among emergency care professionals to guide the effective use of bleeding simulators in medical training. By integrating objective performance data with behavioral insights, this study aims to apprise the strategic use of bleeding simulators in emergency medical education.
Materials and Methods
Study Design
This randomized case-control study (Figure 1) was conducted at a simulation learning laboratory in a rural Northwestern US Level I trauma center.
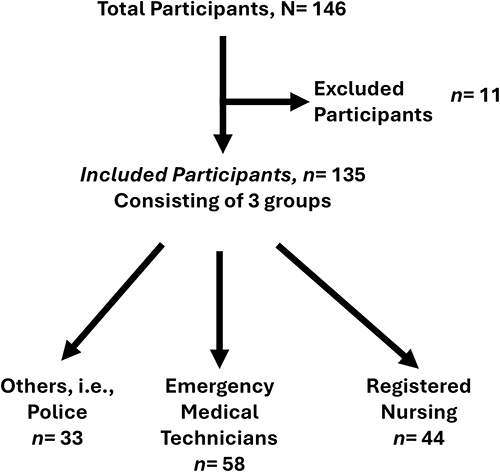 |
Figure 1 Diagrammatic representation of the Study Participants. |
This study was reviewed and deemed exempt by the Billings Clinic Institutional Review Board Privacy & Exemption Committee (Protocol #23.003). Verbal informed consent was obtained from all participants following a thorough explanation of the study’s purpose, procedures, potential risks, and benefits, prior to participation. Consent was documented by the research team at the time of the interview, confirming participants’ understanding and voluntary agreement to participate, in accordance with the Declaration of Helsinki, with confirmation recorded in study logs. To protect participant privacy, written consent was waived due to the use of digital recordings and the associated risk to confidentiality.
Participants were randomized into two task groups (Figure 2):
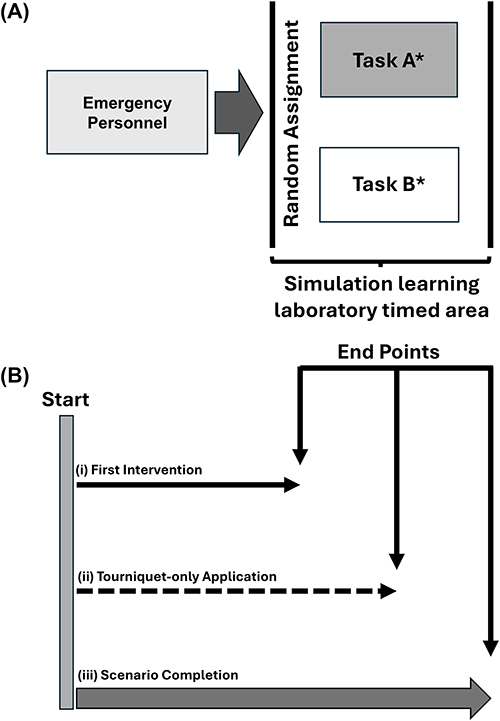 |
Figure 2 Diagrammatic Representation of the Study and Outcome Time Points. (A) Representation of the Training Simulation. Emergency personnel ie, EMS, Fire, Emergency Nurses & Police. Task completion recorded, observed and timed within the simulation learning laboratory, by independent observers. *Task A and B differ in presentation to the participants, ie Task A is more abstract classical mannequin simulation scenario. Task B is more “life-like”, with a Hemorrhagic Pumping System (HPS). (B) Timing End Point Diagrammatic Representation. First intervention refers to Finger, knee or tourniquet applied to wound. |
Group A: Managed a standard moulage mannequin. A silicone wound (Supplemental Materials Figure S1) was affixed to the right thigh, with simulated blood manually applied.
Group B: Managed the same mannequin, but the silicone wound was connected to an active hemorrhagic pump system (HPS; Stops Medical, San Diego, Ca) (Supplemental Materials Figure S2), producing continuous simulated bleeding.
Upon entering the simulation room, each participant received a standardized scenario prompt (Supplemental Materials Box S1) from a facilitator, describing a young male patient who sustained a traumatic limb injury during an industrial accident. No additional verbal cues or feedback were provided after the initial prompt. This moment marked the start of the scenario and the initiation of the intervention timer (“time zero”).
Participants had access only to visual cues, including the wound, simulated blood, and a single set of vital signs placed next to the patient (tachycardic, hypotensive, GCS 14) (Supplemental Materials Figure S3). The simulation concluded either at the 5-minute mark or once the participant verbally indicated completion of assessment and intervention.
All scenarios were video and audio recorded to allow for blinded post-hoc performance analysis. Metrics included time to first intervention, time to tourniquet placement, and total scenario duration. Interventions were defined as any action to control bleeding, including direct pressure, wound packing, or tourniquet placement.
Setting
This study was conducted at a simulation learning laboratory (SLL) in a rural Northwestern US Level I trauma center that consists of multiple simulation rooms equipped with audio/ visual recording systems, a control room, and a conference space for debriefing. This center supports training for a wide range of learners, including healthcare professionals, emergency responders, and community members across a broad rural area.
Participant Confidentiality
The SLL was specifically designed with the intent of participant confidentiality: Encrypted visual recordings are stored within the control room on isolated servers without network or internet integration. Participants’ names were not stored in records, only a subject number. Thus, visual recordings were not accessible outside of the physical entity of the simulation lab, and study observers who timed the individuals during the scenarios had to be physically within the control room to review. Visual recordings were deleted after the evaluation review.
Participants
A total of 146 individuals voluntarily participated in the study without compensation (Figure 1). All participants filled in the questionnaire (Figure 3) and had prior formal training in emergency wound care and tourniquet application. Participants represented a diverse group of emergency care professionals, including (Table 1):
- Police officers and Special Weapons and Tactics (SWAT) personnel
- Firefighters
- Paramedics and Emergency Medical Technicians (EMTs)
- Emergency department Registered Nurses (RNs)
- Medical students
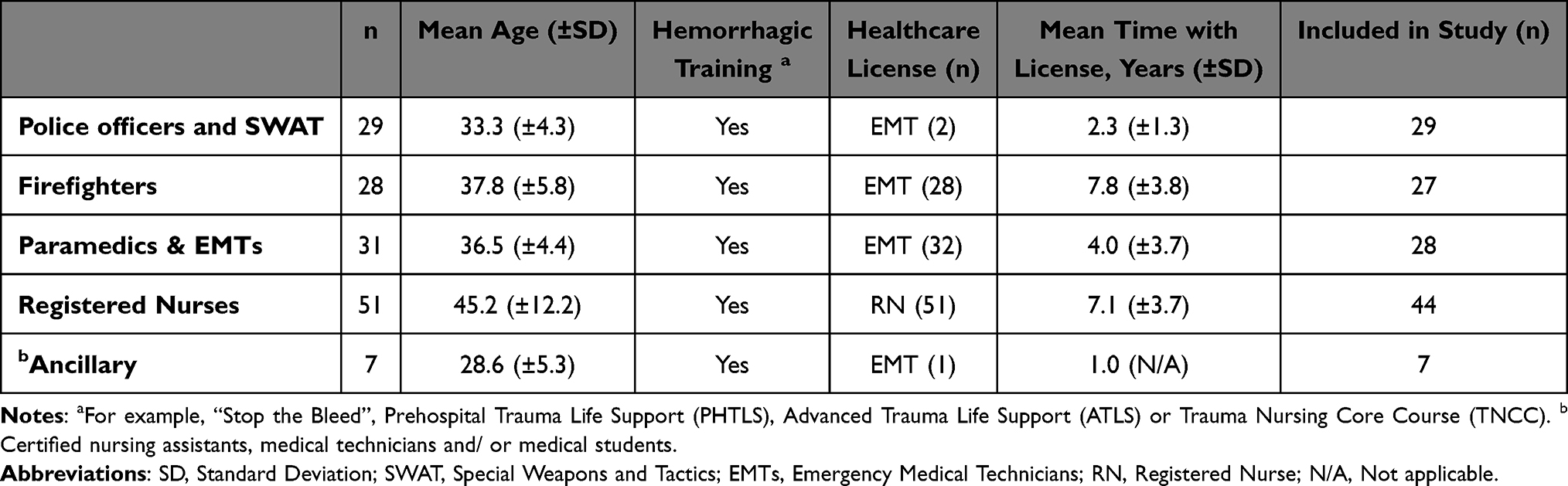 |
Table 1 Participant Demographics |
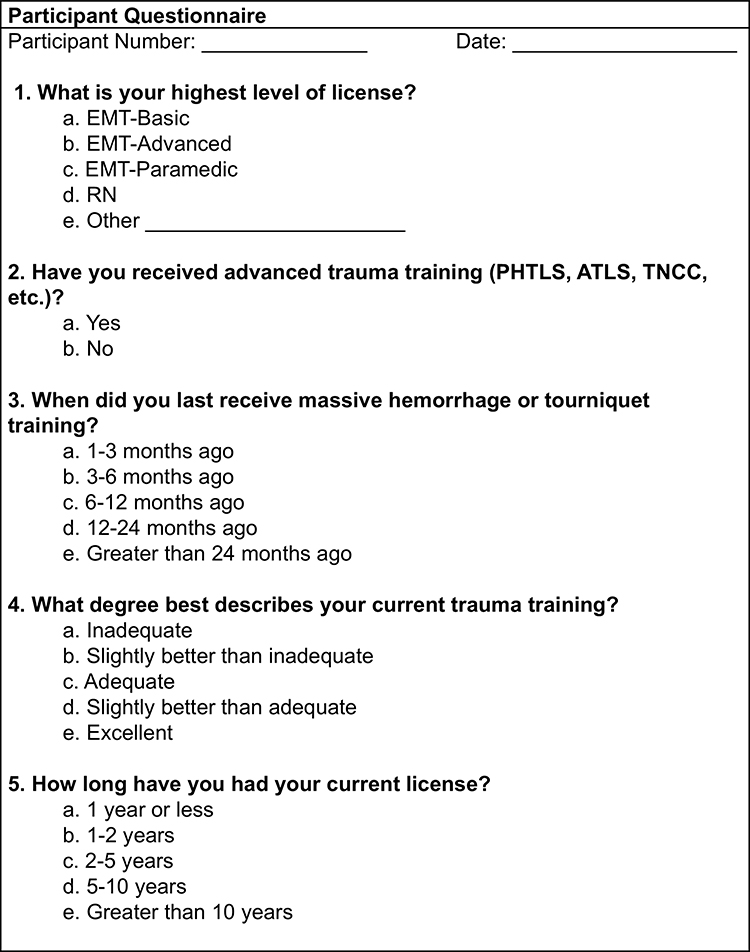 |
Figure 3 Participant Questionnaire. Abbreviations: EMT, Emergency Medical Technician; RN, Registered Nurse; PHTLS, Prehospital Trauma Life Support; ATLS, Advanced Trauma Life Support; TNCC, Trauma Nursing Core Course. |
Irrespective of specific job/role, the participants were divided into three specific groups dependent upon their personal healthcare license.
Others: Any participant without either an EMT or RN healthcare license.
EMTs: Participants with a current EMT license.
RNs: Participants with a current RN license.
The majority of individuals in the “Others” group had training in tactical medicine with some individuals trained in basic first aid. For the purposes of this project, all levels of EMT certification, including paramedics, are grouped under the general classification of “EMT” to streamline analysis and reflect their shared role in pre-hospital emergency care. In addition, it should be noted that EMT licensure is not exclusive to medical personnel, as it is a prerequisite for certain pre-hospital roles.
Recruitment occurred via Email invitations and peer-to-peer recruitment (Supplemental Materials Box S2), leveraging the lab’s longstanding relationships with local institutions and emergency services. Participants were stratified by profession/licensure prior to recruitment due to logistical considerations. Each professional group was engaged during pre-scheduled training periods specific to their discipline: RNs were recruited during hospital training days, fire service personnel during multiple departmental training sessions, EMT providers during their regular training days, and law enforcement officers over several allocated days corresponding with shift downtime. Randomization was conducted within each professional stratum to ensure balanced representation and to accommodate scheduling constraints inherent to each discipline. Enrollment was completed over a few months due to strong interest from the community.
Outcome Measures
Three primary outcome measures were evaluated and detailed in Figure 2:
(i) First Intervention - time to initial intervention, defined as the first hemorrhagic control maneuver (eg, direct pressure, wound packing, or tourniquet placement).
(ii) Tourniquet-only Application - time measured from scenario start to the application of a tourniquet.
(iii) Scenario Completion - total scenario duration, measured from the start of the scenario to its conclusion, either at five minutes or at participant-declared completion.
Participants’ actions were assessed using standardized criteria during blinded video review. Not every participant could be timed on each of the three measures, eg, some felt they had completed the exercise without applying the tourniquet thus were not timed for that intervention.
The majority of participants had completed hemorrhagic control training in the form of foundational education, tactical medicine training, or “Stop the Bleed” courses which emphasizes a stepwise approach: pressure, packing, and ultimately tourniquet application.17
Exclusion Criteria: (a) Received inappropriate feedback from “bystander”; (b) verbalized intervention, as opposed to physical placement; or (c) failed to apply adjuncts in a manner consistent with real-world practice.
Statistics
The statistical analysis was conducted using R statistical software version 4.5.1 (R Foundation for Statistical Computing, Vienna, Austria). Descriptive statistics were calculated for all variables. Continuous variables were summarized using means with 95% confidence intervals (CIs). A two-tailed Student’s t-test was used for continuous variables. Interaction between licensure duration and HPS was examined using two-way Analysis of Variance (ANOVA). Statistical significance was established at p <0.05.
Results
Of the enrolled participants (N=146), a total of 135 participants were included in this study.
Utilization of a Hemorrhagic Pumping System in a Simulation Environment
Initially, time to interventions (Figure 2) compared those scenarios using simple moulage and those using the HPS. In Table 2, results are presented in seconds. For the first intervention, participants using the HPS completed the task significantly faster (mean = 54.9 seconds; 95% CI [46.8, 63.0]) compared to those without the system (mean = 71.9 seconds; 95% CI [65.3, 78.5]), with the difference reaching statistical significance (p = 0.002). For both the tourniquet-only intervention and scenario completion, there was no statistically significant difference between groups.
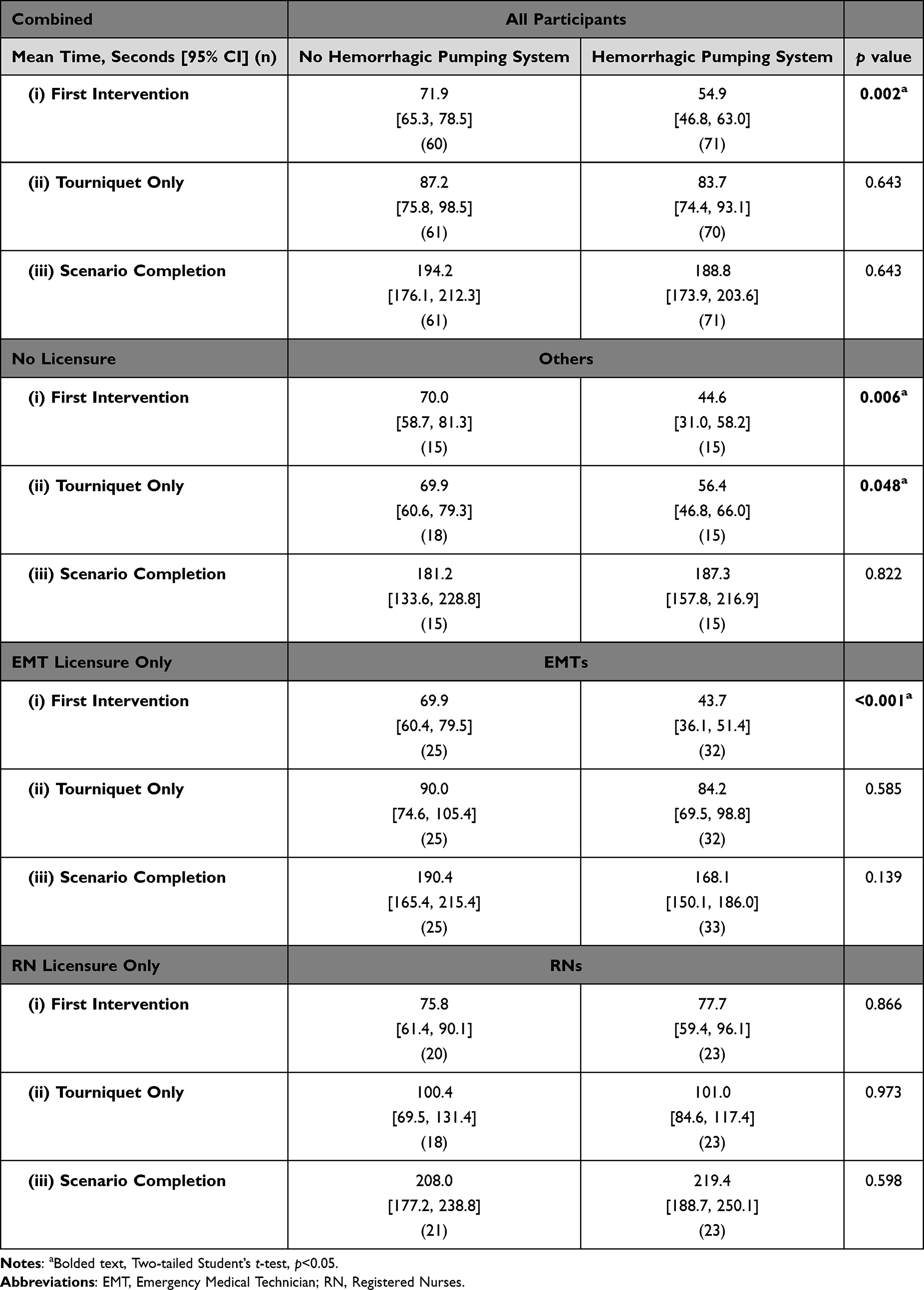 |
Table 2 Performance Differences Using a Hemorrhagic Pumping System Among All Participants and Grouped by Healthcare Licensure |
Performance Differences Among Participants Grouped by Healthcare Licensure
A subgroup analysis was conducted to evaluate performance differences among participants grouped by role (Table 2): Others, EMTs, and RNs. Mean times (in seconds) with 95% confidence intervals (CI) and sample sizes (n) are reported for each group, comparing those using the HPS versus those without (No HPS). First Intervention: in the Others group, participants using the HPS completed the first intervention significantly faster (mean = 44.6 seconds; 95% CI [31.0, 58.2]) than those without HPS (mean = 70.0 seconds; 95% CI [58.7, 81.3]), (p = 0.006). Similarly, among EMTs, HPS use resulted in a significantly faster completion time (mean = 43.7 seconds; 95% CI [36.1, 51.4]) compared to No HPS (mean = 69.9 seconds; 95% CI [60.4, 79.5]), (p <0.001). In contrast, RNs showed no significant difference between groups. Tourniquet-Only Intervention: in the Others group, HPS use was associated with a significantly faster application time (mean = 56.4 seconds; 95% CI [46.8, 66.0]) versus No HPS (mean = 69.9 seconds; 95% CI [60.6, 79.3]), (p = 0.048). Among either EMT or RNs, there was no statistically significant difference between groups. Scenario Completion: there were no statistically significant differences in times across all three (Others, EMTs, or RNs) groups.
Analysis by Length of Healthcare Licensure
Performance times were compared based on years of healthcare licensure, grouped into less than 5 years (<5 years) and 5 years or more (≥5 years). Analyses were conducted for combined EMT and RN groups, and separately within EMTs and RNs (Table 3).
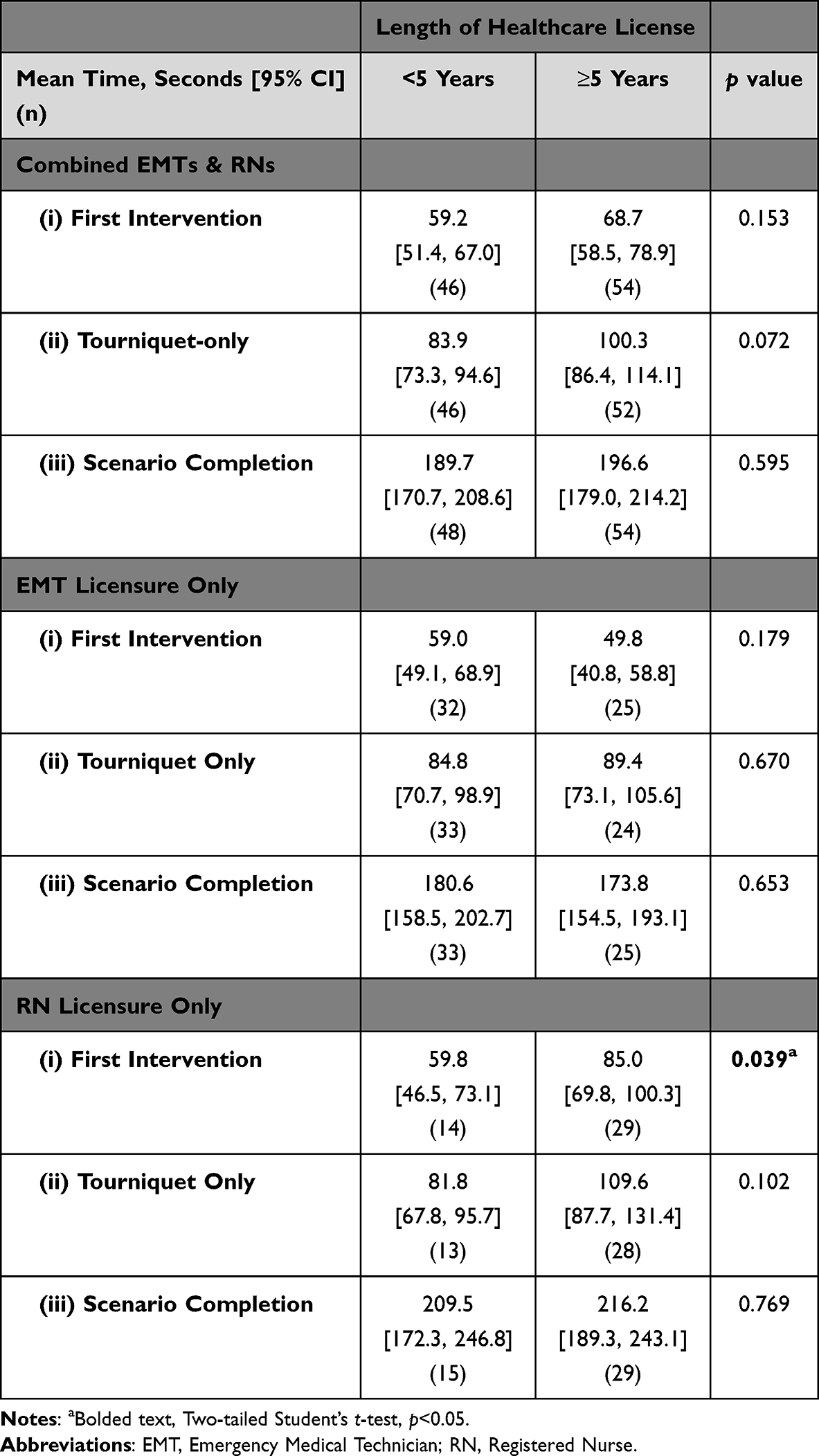 |
Table 3 Timing Analysis by Length of Healthcare Licensure |
Combining EMTs and RNs participants with <5 years of licensure demonstrated slightly faster times across all interventions, though none reached statistical significance compared to ≥5 years licensure, in any of the three intervention endpoints.
Among EMTs only, differences between license duration groups were not statistically significant at any of the timed end points.
For RNs only, a significant difference was observed in the first intervention. At First Intervention: RNs with <5 years of licensure performed significantly faster (mean = 59.8 seconds; 95% CI [46.5, 73.1]) than those with ≥5 years (mean = 85.0 seconds; 95% CI [69.8, 100.3]), (p = 0.039). No significant differences were found in the subsequent measures.
Interaction Between Years of Licensure and Hemorrhagic Pumping System Use
A two-way ANOVA was also conducted to evaluate whether years of licensure (<5 years vs ≥5 years) influenced the effectiveness of the HPS vs no HPS, resulting in four groups to be compared (Table 4).
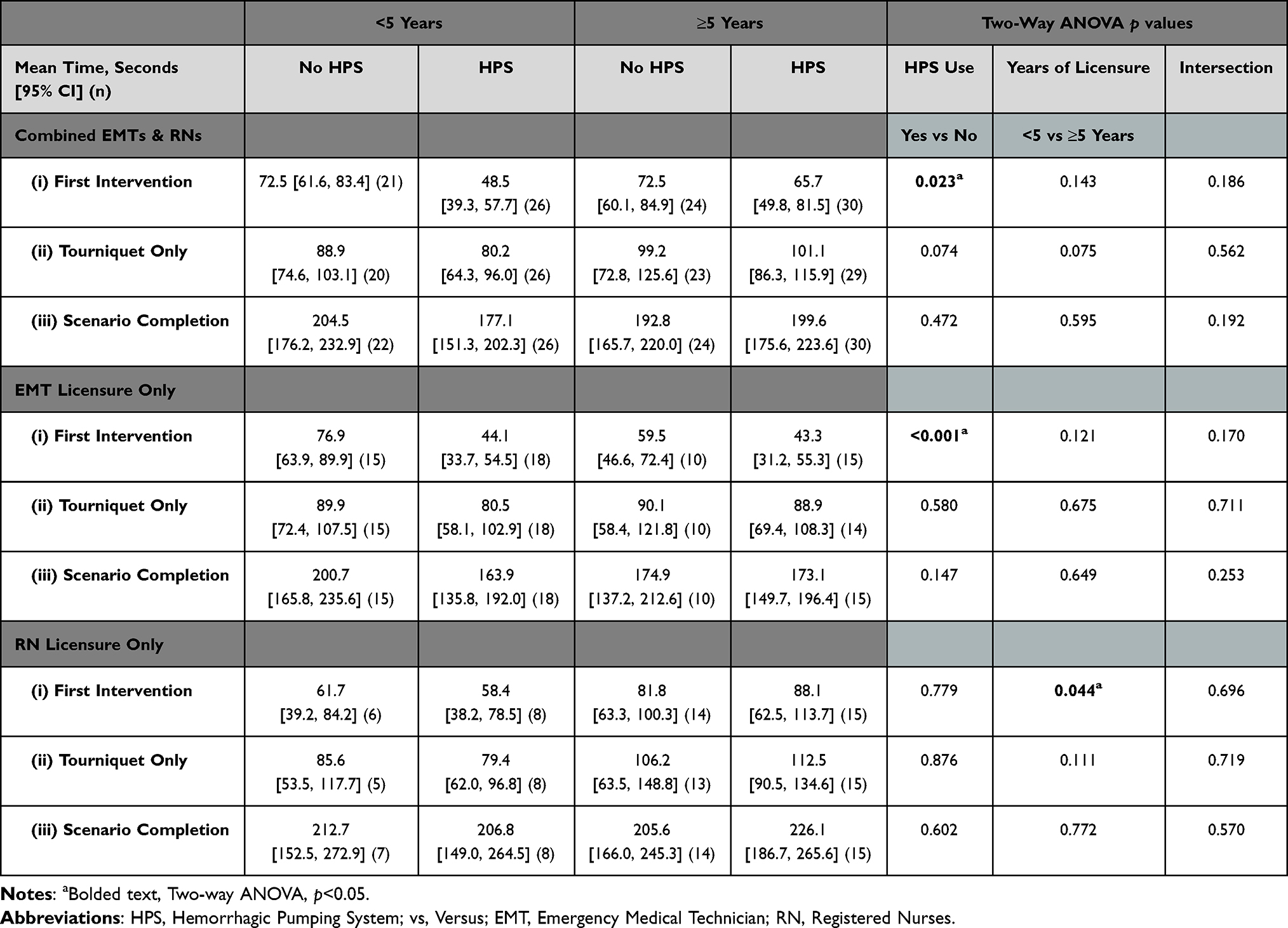 |
Table 4 Interaction Between Years of Licensure and Hemorrhagic Pumping System Use Mean Values and 95% CI Including Two-Way ANOVA p values |
Combining EMT and RN Participants, there was no significant interaction between years of licensure and HPS use (p = 0.186; Table 4). However, HPS use significantly improved performance when measured by time to the first intervention (p = 0.023; 95% CI for No HPS vs HPS [2.05, 27.62]). Among the four groups being compared, the fastest performance occurred in participants with <5 years of licensure using HPS (mean = 48.5 seconds, 95% CI [39.3, 57.7]), compared to those without HPS (mean = 72.5 seconds, 95% CI [61.6, 83.4]). For participants with ≥5 years, the time difference was statistically the same (HPS: 65.7 seconds, 95% CI [49.8, 81.5]) vs No HPS: 72.5 seconds, 95% CI [60.1, 84.9]). No significant interactions and effects of either HPS or years of Licensure were found for tourniquet-only (p = 0.562) or scenario completion measures (p = 0.192); Table 4).
Likewise, among the EMTs Only group, HPS use significantly improved first intervention times (p <0.001; 95% CI for No HPA vs HPS [13.93, 37.45]), though no significant interaction with licensure years of licensure was found (p = 0.170). The fastest performance was among EMTs with ≥5 years of licensure using HPS (mean = 43.3 seconds, 95% CI [31.2, 55.3]). No significant main effects or interactions were observed for tourniquet-only or scenario completion times.
Among registered nurses only there was no significant interaction between years of licensure and HPS use (p = 0.696), and HPS alone did not significantly impact performance (p = 0.779) either. However, years of licensure did significantly affect the first intervention time (p = 0.044; 95% CI for RNs with ≥5 vs <5 [0.78, 49.17]), with a trend toward longer times among more experienced nurses. RNs with <5 years had similar times regardless of HPS (HPS: 58.4 seconds, 95% CI [38.2, 78.5]; vs No HPS: 61.7 seconds, 95% CI [39.2, 84.2]). RNs with ≥5 years took longer (HPS: 88.1 seconds vs No HPS: 81.8 seconds), though these differences were not statistically significant. Further, no significant interactions between years of licensure and HPS use were found for tourniquet-only (p = 0.719) or scenario completion outcomes (0.570). Likewise, for both tourniquet-only and scenario completion outcomes, main effects were also not significant for both years of licensure and HPS use.
Discussion
Classical clinical experience with informal teaching is insufficient for developing skilled healthcare professionals, making standardized, structured practice with outcomes-based evaluation essential.18 Repeated immersive simulation, with feedback, improves learners’ knowledge and self-efficacy regardless of method,19 and higher-fidelity mannequins further enhance immediate post-training performance in knowledge and psychomotor skills.20 Thus, simulation-based education has become an essential element of medical training, particularly for rare but critical situations1 such as life-threatening traumatic limb injuries.2 It offers a unique and safe environment, a “sandbox”, where healthcare providers can identify and address potential challenges without risk to patients.3
Few studies to date have explored the impact of dynamic bleeding models in trauma simulation. Our study builds on foundational work such as the pilot study by Mills et al (2018).15 While that study focused primarily on paramedic students and the effects of realistic moulage, our study extended the concept by involving a broader group of emergency and prehospital providers and by directly integrating a dynamic bleeding control system into the simulation. That allowed for not only a comparison of learner experience, but also an assessment of objective clinical performance metrics, such as time to intervention and tourniquet placement.
This study explored the effect of incorporating an active bleeding pump system into trauma simulations and its influence on provider response and possible clinical decision-making.
As shown in Table 2, when considering all participants the HPS implementation significantly reduced time to first intervention, corroborating previous high-fidelity simulation literature.21
However, the majority of the existing literature in this realm focuses solely upon discrete participant’ roles, most specifically EMT15 or RN21 healthcare students. As opposed to real-world active law enforcement, fire service and healthcare professionals where each have separate but collaborative roles focusing on scene safety, initial medical stabilization, transport and advanced life support. In Table 2 HPS is shown to reduce time to intervention for both Others and EMTs. In addition, time to tourniquet was also reduced for the Others group. Interestingly however, there was no apparent impact on time with or without HPS with RNs, this was unexpected and contrary to the literature utilizing RN students.21
Thus, this RN observation was further explored in Table 3, which examined varying levels of experience (defined by licensure duration). RNs with 5 or more years’ experience demonstrated statistically longer times to first intervention compared to those with less than five years. This finding, although initially unexpected, is likely attributable to the more measured and strategic clinical reasoning of experienced providers and is corroborated in the literature.16 These individuals may be less reactive to an obvious injury and more inclined to assess for other potential life threats, indicating a higher-level cognitive approach that may ultimately improve overall patient care.22
To better understand this observation within the RN group, an additional subgroup analysis was conducted to jointly evaluate the effects of years of licensure and the impact of the HPS. Overall, though no significant interaction was observed between the years of licensure and HPS use (Table 4), participants with <5 years of experience combined with HPS consistently resulted in faster times to the first intervention (Table 4). Combining EMTs and RNs with less than <5 years licensure, HPS reduced time to first intervention. When further delineated, this was also shown in the EMTs only group. With the RN focused group, in contrast, no significant impact of HPS use was observed. However, what can be discerned is the more experienced RNs took a relatively longer time to complete the task with the HPS than those RNs with less than five years’ experience.
This recurring theme with experience may also be due to historical teaching of the trauma ABCs (airway, breathing, circulation) that guide trauma care in provider courses like Advanced Trauma Life Support (ATLS) and Trauma Nursing Core Course (TNCC). This standard has recently been reassessed with more recent combat casualty data, prioritizing massive hemorrhage control, shifting the classical trauma dogma to CABs (circulation, airway, breathing; exsanguination-first (x-ABC) model).23 This move has influenced civilian trauma care, progressing from public education initiatives like “Stop the Bleed”,10 to in-hospital protocols.24 Ultimately leading to a hypothesis for a future study, that the possible juxtaposition where nurses with 5 or more years’ experience intrinsically follow ABCs, and newer nurses with less than 5 years following the x-ABC model, thus reducing time to intervention in exsanguination simulations compared to their more experienced brethren.
Our findings suggest that active bleeding cues significantly increase perceived urgency, leading to earlier intervention when compared to traditional moulage-only simulations. Importantly, this difference in urgency did not translate into faster tourniquet placement, likely due to more complex real-world behaviors, such as donning personal protective equipment (PPE), applying direct pressure, or pausing for broader assessment.
Limitations
Despite its strengths, the study had several limitations:
(a) Lack of Dynamic Feedback: Participants noted frustration due to the absence of dynamic scenario feedback, particularly in the moulage-only group. This decision was intentional to limit confounding variables, but it may have influenced engagement and perceived realism.
(b) PPE and Scenario Consistency: Early participants varied in their use of gloves, which impacted time metrics. This was mitigated partway through the study by standardizing glove use prior to room entry; however, early variability may have influenced outcomes.
(c) Volunteer Bias: All participants were volunteers. The absence of incentives may have led to variable levels of motivation, potentially affecting performance. Some participants may have approached the simulation more casually than they would a real clinical situation.
(d) No Post-Simulation Self-Evaluation: We did not assess participants’ self-perceived competence before or after the simulation. Future studies could evaluate the impact of dynamic simulation on learner confidence, retention, and real-world performance over time.
(e) Although all analyses met appropriate statistical assumptions, the relatively limited sample size may have reduced the power to detect significant differences. Future studies with larger cohorts to jointly evaluate the effects of years of licensure and the impact of the HPS may clarify whether the observed trends reach statistical significance.
Participant Feedback
A notable theme emerged in participant feedback, many expressed frustrations with the lack of dynamic, scenario feedback. Participants were accustomed to high-fidelity simulation experiences involving facilitator interaction, changing vital signs, and responsive mannequins. In contrast, this study design intentionally limited variability by providing only a single set of vital signs at the beginning of the scenario and relying solely on static or visual cues. This constraint was necessary to preserve study validity but led to dissatisfaction, especially in the static moulage group, where there was no visual cue to indicate treatment effectiveness.
Interestingly, this frustration was far less common in the active bleeding group, where successful application of a tourniquet resulted in visible cessation of bleeding. This immediate visual feedback reinforced the value of dynamic simulation tools in learner engagement and perceived training effectiveness.
Future Directions
These findings suggest several avenues for future investigation. One possible study could involve crossover design, allowing participants to engage in both simulation arms and self-report, to measure which experience was more valuable for their learning. Additionally, longitudinal follow-up assessing retention and confidence in hemorrhagic control skills (eg, at 3- or 6-month intervals) could help determine whether dynamic realism enhances long-term training outcomes. We hypothesize that high-fidelity simulation will produce a more durable educational impact.
Conclusion
Simulation-based education remains essential for preparing providers to manage high-stakes, low-frequency emergencies. This study demonstrates that dynamic bleeding models enhance clinical urgency and engagement in extremity trauma scenarios. From our first objective, time-based measures showed differences with the use of the HPS. HPS significantly reduced time to first intervention, particularly among EMTs and providers with less than five years of experience, although it did not significantly impact tourniquet application or overall scenario completion times. To the second objective, longer response times among experienced RNs may reflect more deliberate clinical reasoning shaped by traditional trauma paradigms. However, future studies will be needed to examine these nuanced results about this objective. As trauma care shifts toward exsanguination-first approaches, simulation fidelity must evolve accordingly. High-fidelity tools like dynamic bleeding models can reinforce current trauma protocols, may enhance clinical decision-making, and potentially improve long-term skill retention and patient outcomes.
Acknowledgments
Thank you to Lanny Orr, Trauma Services, for guidance and support. Special thanks to Chris Sauter and Lori Martinez at the Simulation Center for their integral contributions to the study; their support and involvement were essential for the success of this project.
We specifically want to thank our local law enforcement, fire service, paramedics, EMTs and nursing staff colleagues who graciously volunteered their time for this study.
Disclosure
All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. All the authors declare that there is no conflict of interest in this work.
References
1. Elendu C, Amaechi DC, Okatta AU, et al. The impact of simulation-based training in medical education: a review. Medicine. 2024;103(27):e38813. doi:10.1097/md.0000000000038813
2. Quick JA. Simulation training in trauma. Mo Med. 2018;115(5):447–14.
3. Rider A, Schertzer K. Quality Improvement in Medical Simulation. In: StatPearls. StatPearls Publishing LLC; 2025. StatPearls Publishing Copyright © 2025.
4. Bixio M, Carenzo L, Accurso G, et al. Management of critically ill patients in austere environments: good clinical practice by the Italian Society of Anesthesia, Analgesia, Resuscitation and Intensive Care (SIAARTI). J Anesth Analg Crit Care. 2024;4(1):74. doi:10.1186/s44158-024-00209-8
5. Bonanno FG. Management of hemorrhagic shock: physiology approach, timing and strategies. J Clin Med. 2022;12(1). doi:10.3390/jcm12010260
6. Huber GH, Manna B. Vascular Extremity Trauma. In: StatPearls. StatPearls Publishing Copyright © 2025, StatPearls Publishing LLC; 2025.
7. Dorlac WC, DeBakey ME, Holcomb JB, et al. Mortality from isolated civilian penetrating extremity injury. J Trauma. 2005;59(1):217–222. doi:10.1097/01.ta.0000173699.71652.ba
8. Rocko JM, Tischler C, Swan KG. EXSANGUINATION IN PUBLIC - A PREVENTABLE DEATH. J Trauma Acute Care Surg. 1982;22(7):635.
9. Jacobs LM, McSwain NE Jr, Rotondo MF, et al. Improving survival from active shooter events: the Hartford Consensus. J Trauma Acute Care Surg. 2013;74(6):1399–1400. doi:10.1097/TA.0b013e318296b237
10. Levy MJ, Krohmer J, Goralnick E, et al. A framework for the design and implementation of Stop the Bleed and public access trauma equipment programs. J Am Coll Emerg Physicians Open. 2022;3(5):e12833. doi:10.1002/emp2.12833
11. Stokes-Parish J, Duvivier R, Jolly B. Expert opinions on the authenticity of moulage in simulation: a Delphi study. Adv Simul. 2019;4:16. doi:10.1186/s41077-019-0103-z
12. Gushing J, Blair SG, Albrecht RM, et al. Prehospital tourniquet placement in extremity trauma. Am J Surg. 2023;226(6):901–907. doi:10.1016/j.amjsurg.2023.08.007
13. McLauchlan NR, Frasier LL, Fisher L, et al. High-fidelity bleeding control simulation scenario during medical student orientation improves students’ self-reported ability to identify and treat life-threatening bleeding with 3-year follow-up. J Surg Educ. 2024;81(10):1484–1490. doi:10.1016/j.jsurg.2024.07.007
14. Mitchell SA, Boyer TJ. Deliberate Practice in Medical Simulation. In: StatPearls. StatPearls Publishing Copyright © 2025, StatPearls Publishing LLC; 2025.
15. Mills BW, Miles AK, Phan T, et al. Investigating the extent realistic moulage impacts on immersion and performance among undergraduate paramedicine students in a simulation-based trauma scenario: a pilot study. Simul Healthc. 2018;13(5):331–340. doi:10.1097/sih.0000000000000318
16. Hoffman KA, Aitken LM, Duffield C. A comparison of novice and expert nurses’ cue collection during clinical decision-making: verbal protocol analysis. Int J Nurs Stud. 2009;46(10):1335–1344. doi:10.1016/j.ijnurstu.2009.04.001
17. Tang X, Nie Y, Wu S, DiNenna MA, He J. Effectiveness of “Stop the Bleed” courses: a systematic review and meta-analysis. J Surg Educ. 2023;80(3):407–419. doi:10.1016/j.jsurg.2022.10.007
18. Motola I, Devine LA, Chung HS, Sullivan JE, Issenberg SB. Simulation in healthcare education: a best evidence practical guide. AMEE Guide No 82 Medical Teacher. 2013;35(10):e1511–e1530. doi:10.3109/0142159X.2013.818632
19. Platt A, Allan J, Leader C, Prescott-Clements L, McMeekin P. Preparing for practice, the effects of repeated immersive simulation on the knowledge and self-efficacy of undergraduate nursing students: a mixed methods study. Nurse Educ Pract. 2024;74:103866. doi:10.1016/j.nepr.2023.103866
20. Sherwood RJ, Francis G. The effect of mannequin fidelity on the achievement of learning outcomes for nursing, midwifery and allied healthcare practitioners: systematic review and meta-analysis. Nurse Education Today. 2018;69:81–94. doi:10.1016/j.nedt.2018.06.025
21. Bertini-Pérez D, Martin-Ibañez L, Gómez Chica P, et al. Effectiveness of a haemorrhage-control task simulator for training nursing students: a quasi-experimental before-after study. J Nurs Manag. 2024;2024:9730765. doi:10.1155/2024/9730765
22. Aldamiri KT, Alhusain FA, Almoamary A, Alshehri K, Al Jerian N. Clinical decision-making among emergency physicians: experiential or rational? J Epidemiol Glob Health. 2018;8(1–2):65–68. doi:10.2991/j.jegh.2018.04.102
23. Brito AM, Schreiber M. x-ABC versus ABC: shifting paradigms in early trauma resuscitation. Trauma Surg Acute Care Open. 2025;10(Suppl 1):e001773. doi:10.1136/tsaco-2025-001773
24. Breeding T, Martinez B, Katz J, et al. CAB versus ABC approach for resuscitation of patients following traumatic injury: toward improving patient safety and survival. Am J Emergency Med. 2023;68:28–32. doi:10.1016/j.ajem.2023.02.034
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.