Back to Archived Journals » Adolescent Health, Medicine and Therapeutics » Volume 11
Birth Preparedness and Complication Readiness Practices Among Pregnant Adolescents in Bangkok, Thailand
Authors Teekhasaenee T, Kaewkiattikun K ![]()
Received 30 October 2019
Accepted for publication 21 January 2020
Published 31 January 2020 Volume 2020:11 Pages 1—8
DOI https://doi.org/10.2147/AHMT.S236703
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Alastair Sutcliffe
Tiradech Teekhasaenee, Kasemsis Kaewkiattikun
Department of Obstetrics and Gynecology, Faculty of Medicine, Vajira Hospital, Bangkok, Thailand
Correspondence: Kasemsis Kaewkiattikun
Department of Obstetrics & Gynecology, Faculty of Medicine, Vajira Hospital, Navamindradhiraj University, Bangkok 10300, Thailand
Tel +668 9536 6601
Email [email protected]
Background: Reducing the maternal mortality ratio is one of the United Nations Sustainable Development Goals. These maternal deaths are preventable with appropriate management and care. Birth preparedness and complication readiness (BPCR) is a strategy to make prompt decisions to seek care from skilled birth attendants, resulting in reduced maternal and neonatal mortality. Despite high global rates of adolescent pregnancy, there has not yet been a study of BPCR status and associated factors among pregnant adolescents.
Objective: To assess the proportion of, and associated factors for, good BPCR in adolescent pregnant women attending antenatal clinic in an urban tertiary care hospital.
Materials and Methods: This cross-sectional survey was conducted among adolescent pregnant women attending antenatal clinic at the Department of Obstetrics and Gynecology, Faculty of Medicine Vajira Hospital, Thailand, from September 1st, 2018 to March 31st, 2019. A total of 134 adolescent pregnant women were recruited. The participants and their parents or legal guardians were informed of the study process at the antenatal clinic before their parents or legal guardians, granted written consent on their behalf. The participants were interviewed using the BPCR index, which was adapted from the John Hopkins Program for International Education in Gynecology and Obstetrics.
Results: The proportion of good BPCR in adolescent pregnant women in an urban tertiary care hospital was 78.4%. The most mentioned aspect of BPCR was planning to give birth with a skilled provider (92.5%). The significant associated factor for good BPCR was the number of ANC ≥ 4 (odds ratio 3.2, 95% CI 1.13– 9.05, p=0.023).
Conclusion: This study demonstrated that the proportion of good BPCR among adolescent pregnant women attending an urban tertiary care hospital was high. The associated factor of good BPCR was the number of ANC ≥ 4.
Keywords: birth preparedness and complication readiness, BPCR, adolescent pregnancy, urban, Thailand
Introduction
Unexpected, and often life-threatening, events might occur at any stage of pregnancy, during the antepartum, intrapartum, and postpartum periods. Maternal death is a global issue of great concern. The World Health Organization (WHO) reported approximately 99% of them occur in developing regions, with Sub-Saharan Africa (66%) and Southern Asia (22%) accounting for 88% of the global burden of maternal death.1
Reducing the maternal mortality ratio is one of the United Nations Sustainable Development Goals. Most maternal deaths are preventable with appropriate management and care with the assistance of a skilled birth attendant.2 Birth preparedness and complication readiness (BPCR) is an important strategy in accomplishing these goals. There is clear evidence that BPCR interventions are effective in reducing maternal and neonatal mortality.3 Additionally, WHO has strongly recommended BPCR to increase the use of skilled care and the timely use of health-care facilities for obstetric and newborn complications.4
BPCR consists of understanding the process and complications of pregnancy, establishing a financial plan for delivery, and decision-making in emergency conditions. In addition, birth preparedness is also preparing for giving birth with a skilled provider, which minimizes maternal morbidities and mortality.5–7 The Maternal and Neonatal Health Program of the John Hopkins Program for International Education in Gynecology and Obstetrics (JHPIEGO) developed the BPCR matrix, which is a standard set of indicators that could be used across countries. The questionnaire for individual-level BPCR consisted of 9 indicators. The pregnant women who fulfilled at least four BPCR practices were defined as good BPCR.5,6
Many BPCR studies have been conducted in developing countries such as Sudan, Ethiopia, India, Nigeria, Tanzania and Ghana. Moreover, there have been few studies in urban areas; most of the earlier published investigations were conducted in rural or peri-urban areas where there are differences in health-care settings, socioeconomic status and cultural conditions compared to urban areas.3,8–20 Additionally, most previous studies focused on adult pregnancy. There has not yet been a study in adolescent pregnancy, which is highly prevalent worldwide.
Adolescence is the transitional stage from childhood to adulthood that occurs between ages 10 and 19. Adolescents are generally divided into sub-stage based on growth and development as early (10–13 years), middle (14–17 years), and late (18 years onwards). The majority of adolescents in low- and middle-income countries get married at the age of 18 or 19 years.21,22 About 15 million adolescents give birth each year, roughly 11% of all births worldwide.23 Adolescent pregnancy is known to be associated with maternal and neonatal risks. This can be explained by the fact that adolescents are usually not physically or psychologically developed enough for bearing a pregnancy. Consequently, health, social and economic problems occur.24,25 These may be the result of poor birth preparedness, leading to delays in seeking, reaching and obtaining proper and suitable care. Therefore, BPCR is an essential strategy for this group to diminish maternal and neonatal morbidities.
Despite the benefit of BPCR to adolescent pregnancy, no study has been conducted in this group. In Thailand, there is a high rate of adolescent pregnancy. According to Thailand Public Health Statistics, Thailand has the highest rate of adolescent births in Southeast Asia and the second highest in the world.26 A study was, therefore, necessary to determine BPCR among pregnant adolescents in Thailand. Additionally, there have been few reports of BPCR from urban areas. Therefore, questions of this study will fill the gap in research about BPCR status, and associated factors of good BPCR, among pregnant adolescents in an urban area. Aims of this study are to assess the BPCR status, and associated factors for good BPCR, among pregnant adolescents at a tertiary care hospital in urban Thailand. Furthermore, results of this study will contribute information for further management and study in designing a BPCR campaign or innovations to improve maternal and neonatal outcomes.
Materials and Methods
A cross-sectional study was conducted among adolescent pregnant women attending the antenatal clinic at the Department of Obstetrics and Gynecology, Faculty of Medicine Vajira Hospital, Navamindradhiraj University, Bangkok, Thailand, from September 1st, 2018 to March 31st, 2019. Reasons for choosing a university facility to study included more availability of antenatal educational programs, and timelier obstetric and neonatal care. Ethical clearance was approved by the Institutional Review Board (IRB) of the Faculty of Medicine Vajira Hospital, Navamindradhiraj University. Formal permission letters were secured from all respective local administrators. Additionally, this study was conducted in accordance with the Declaration of Helsinki.
The study population consisted entirely of antenatal adolescent pregnant women (age 10–19 years) who planned to give birth at the Department of Obstetrics & Gynecology, Faculty of Medicine Vajira Hospital. Inclusion criteria were low-risk pregnant adolescent Thai nationals who could read and communicate in Thai. Exclusion criteria were having maternal and fetal complications at the date of interview.
The sample size was calculated by using data from a pilot study which found that the prevalence of BPCR among pregnant adolescents was estimated at 73%. The level of confidence of 95% and permission margin of error of 7.5% were applied to determine the difference between groups. Adding 10% for incomplete data, a total of 134 participants were included in this study by computerized simple random sampling technique. A research assistant would interview the participant following randomization after obtaining written informed consent.
All the study subjects and their parents or legal guardians were informed about all the relevant aspects of the study, including its aim, interview procedures, anticipated benefits and potential hazards at an antenatal clinic by a research assistant. Confidentiality of the data was strictly maintained. Their right to refuse to participate in the study at any time was also assured. All participants and their parents or legal guardians had to assent to the study process. Parents or legal guardians provided permission and gave consent on their behalf since none of the participants could give consent because they were under the legal age of consent for research.
The eligible participants were interviewed by a well-trained research assistant at the first antenatal visit. They did not do the questionnaire themselves in order to avoid misunderstanding in questions. The next antenatal visit would be arranged according to standard recommendations. The interview process took about 15–20 mins for each participant, using a structured questionnaire which included demographic data, place of residence, average distance from the hospital, parity, gestational age at initial antenatal care, number of antenatal visits and individual level BPCR practices. The BPCR index was adapted from monitoring BPCR tools for maternal and newborn health, Johns Hopkins Program for International Education in Gynecology and Obstetrics (JHPIEGO).5,6 Most previous studies of BPCR used the BPCR tool of JHPIEGO.3 The BPCR questionnaire was translated into Thai by different experts to ensure consistency and back-translated to English. The individual-level BPCR index consisted of knowledge of danger signs during pregnancy, labor and childbirth, in the postpartum period, and in the newborn, plan to attend at least 4 antenatal care visits with a skilled provider, attend first antenatal care sessions with a skilled provider during first trimester, plan to give birth with a skilled provider, plan to save money for a childbirth, and plan to identify a mode of transport to the place of delivery. The participants who fulfilled at least four of the criteria on the BPCR index were considered as “well prepared” and the rest of them were “less prepared”.5,6,13
The primary outcome of this study was the proportion of good BPCR in adolescent pregnant women attending ANC clinic. The secondary outcomes were associated factors for good BPCR. The data were analyzed by statistician using SPSS version 22 (IBM Corp., Armonk, NY, USA).27 Chi-squared test was used for categorical data analysis to determine BPCR status and associated factor for BPCR. P-value of less than 0.05 was considered statistically significant.
Result
A total of 134 adolescent pregnant women were included in this study. Table 1 shows 105 (78.4%) adolescent pregnancies were well prepared by fulfilling at least four indicators of BPCR and the remaining 29 (21.6%) of them were less well prepared.
 |
Table 1 BPCR and BPCR Indexes Among Antenatal Adolescent Mothers |
For BPCR danger signs, 19.4% knew all danger signs during pregnancy, 29.1% knew all danger signs during labor and childbirth, 14.9% knew all danger signs during postpartum period, and 13.4% knew all danger signs in the newborn. The most mentioned danger sign was severe vaginal bleeding during the postpartum period (77.6%) and the least mentioned danger sign was convulsion and retained placenta during labor and childbirth (29.9%). The participants were able to mention neonatal danger signs more than obstetric danger signs. None of the participants knew ≥12 danger signs, 43.3% knew ≥8 danger signs, and 60.4% knew ≥4 danger signs.
Regarding birth preparedness, 85.1% of participants planned to attend at least four antenatal care sessions with a skilled provider, 57.5% attended first antenatal care visit with a skilled provider during the first trimester, 92.5% planned to give birth with a skilled provider, 42.5% planned to save money for a childbirth, and 91.0% planned to identify a mode of transport to the place of delivery. Therefore, the most mentioned BPCR indicator was planning to give birth with a skilled provider, and the least mentioned BPCR indicator was planning to save money for a childbirth (Table 1).
Socio-demographic characteristics of all 134 participants are shown in Table 2. The baseline characteristics revealed that the majority were 18–19 years old (51.5%), had normal BMI (71.6%), were married (52.2%), had an elementary and secondary school education (84.3%), had income <10,000 THB (64.9%), had a nuclear family (55.2%), lived in an urban area (88.8%), and average distance from the hospital was ≤2 hrs (59.7%). The obstetric characteristics showed that the majority were primipara (92.5%), had gestational age at first ANC > 12 weeks (63.4%) and number of ANC < 4 (64.9%). For those who were married, their husbands had mostly elementary or secondary school education (87.3%) and were employed (77.6%). The association between baseline characteristics with good BPCR status showed that only the number of ANC ≥ 4 was significantly associated with well-prepared BPCR (odds ratio 3.20, 95% CI 1.13–9.05, p = 0.023).
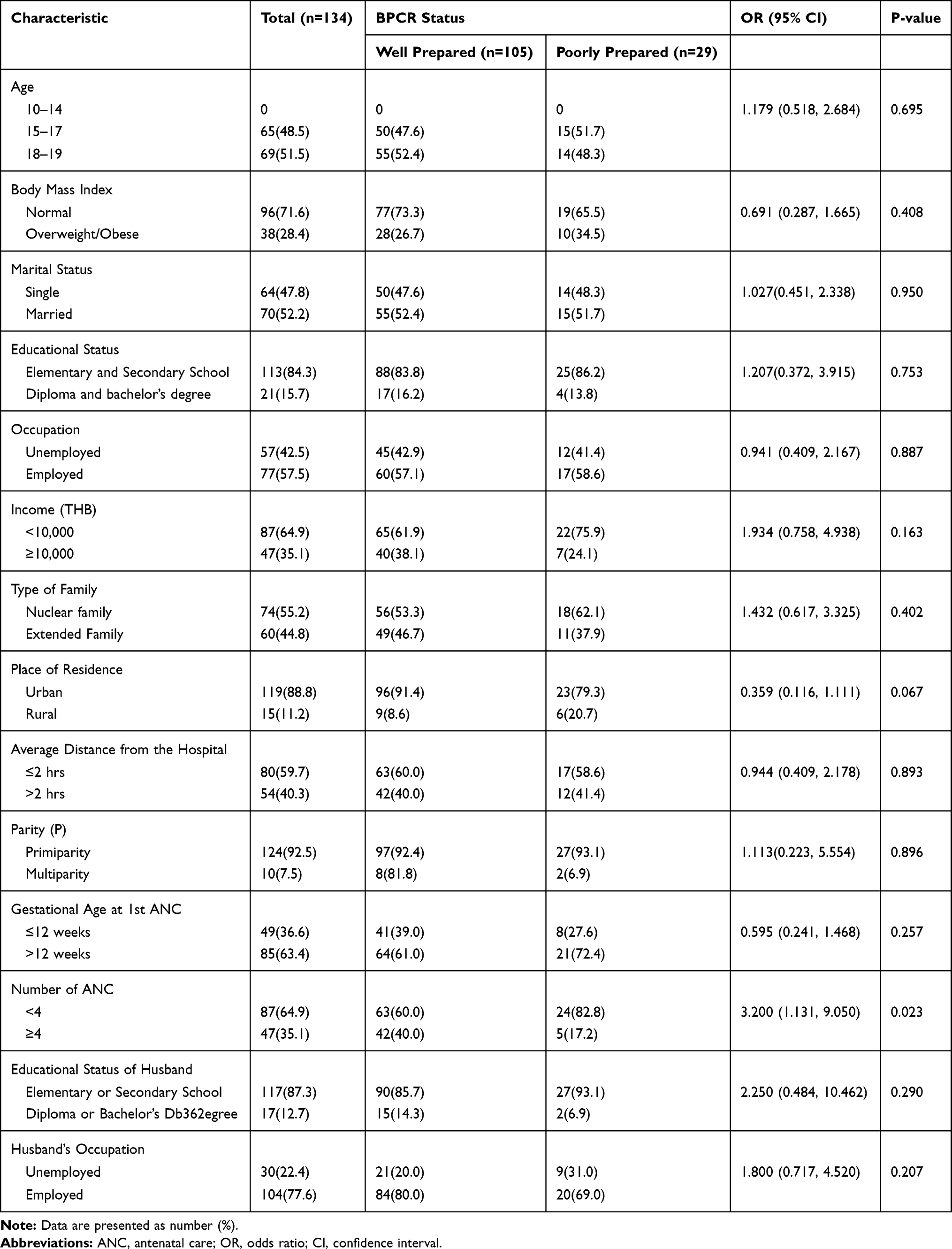 |
Table 2 Demographic Characteristics of Adolescent Mothers and Association with BPCR |
Discussion
This cross-sectional study in an urban tertiary care hospital revealed that there were many adolescent pregnant women with good BPCR (78.4%). This result is consistent with the same setting in India (71.5%)16 and Thailand (78.6%),17 in which most participants were adults. However, the level of BPCR in the present study is far higher compared with most previous reports in rural settings. They were 58.2% in Tanzania,10 17% in Southern Ethiopia,11 and 35.85% in India.13 Additionally, even a study from a tertiary care hospital in rural India found a low BPCR index (55.83%).28 This finding suggests that pregnant women who live in urban areas have better birth preparedness than those who live in rural areas. This confirms previous reports that well-prepared pregnant women tended to live in urban areas compared to those who were less prepared.9,11,29
When considering awareness of danger signs, this study found the percentage of adolescent pregnant women who mentioned all danger signs during pregnancy, labor, postpartum and in the newborn were 19.4%, 29.1%, 14.9%, and 13.4%, respectively. Similar findings were observed by most previous studies among adult pregnant women. Awareness of danger signs was 23.6% in Tanzania,10 4.7% in Kenya,12 28.03% in India,13 and 23.2% in Ethiopia.14 This indicates that most pregnant women have insufficient awareness to identify danger signs, despite the fact that recognition of danger signs has an effect on timely access to health-care facilities. Failure to recognize danger signs leads to delayed decisions to seek proper obstetric and newborn care. There is strong evidence that awareness of danger signs was significantly associated with good BPCR.15 Hence, providing danger signs knowledge for pregnant women should be included in the first health education program during the antenatal period. However, knowing the danger signs does not ensure that pregnant women will have the abilities to recognize and judge the severity of problems. Therefore, health-care personnel should also inform all pregnant women to be aware of the importance and progression of danger signs, along with going to the hospital as soon as problems occur.
Regarding other BPCR indicators, the most mentioned indicator was planning to give birth with a skilled provider (92.5%). This finding is consistent with most previous studies. It is 98.14–99.54% in India,13,28 86.8% in a prior report from Thailand,17 and 77.8% in Ethiopia.18 The high level of awareness about giving birth with a skilled provider could be due to increasingly widespread access to modern obstetric practice leading to awareness of safe births with skilled providers. The second most mentioned BPCR indicator in this study was planning to identify the mode of transport to the place of childbirth (91.0%). However, this is different from most prior reports from rural settings, in which arranging transport to the place of childbirth was much lower. It was 34.1% in Tanzania,10 10.8% in northwest Ethiopia,14 and 26.7% in Uganda.20 The high proportion of scheduling for transport in this study could be attributed to the traffic congestion in urban areas that results in long journey times even over short distances. Time spent on transportation is an important barrier for seeking and reaching a health-care facility. Therefore, early preparation for transport to a health-care facility in urban areas is essential in reducing the delay in reaching and obtaining suitable care.
It is interesting that a small percentage of adolescent pregnant women in this study were not concerned about saving money for childbirth (42.5%). This matches reports from southern Ethiopia (34.5%),11 northwest Ethiopia (37.5%),14 and Kenya (43.8%).12 Nevertheless, it is different from findings in Tanzania (84.1%),10 north Ethiopia (68.5%),18 and Uganda (67.2%).20 Money is necessary for seeking and reaching medical facilities for appropriate maternal and neonatal care. Individual money-saving plans may be determined by the cost of health-care services, pregnancy complications, transportation expenses, and cost of living.5 In adolescent pregnancy, the reasons that explain low financial preparation are probably low income and receiving financial support from the family.
After analyzing the association between demographic characteristics and BPCR status, this study revealed that only the number of antenatal care visits ≥4 was significantly associated with good BPCR. Adolescent pregnant women who attended ≥4 antenatal visits were 3.2 times better prepared than those who attended less antenatal visits. This finding is consistent with results from Tanzania and Northwest Ethiopia. They found that pregnant women who attended ≥4 antenatal visits were 1.73–76.91 times better prepared.10,14 Adequate antenatal care provides important and reliable information about pregnancy which leads to good BPCR and good pregnancy outcomes. However, there may be several barriers to attending optimal antenatal visits among adolescents which are different from adults, including low education, incomplete graduation, psychosocial unreadiness, unplanned pregnancy, late antenatal care, and family influences.
The results of this study have implications for institutions to improve BPCR programs for adolescent pregnant women, especially knowledge of danger signs. Moreover, eliminating various obstacles to maximize antenatal visits is also important for good BPCR, which requires cooperation from adolescents themselves, family, and health-care personnel. In addition, health-care personnel must develop specific BPCR programs that are different from those for adult pregnancy. This study may be generalizable to family and community to help adolescent mothers to better prepare. Further study in multiple centers with larger population would be valuable for exploring more associated factors for successful BPCR and developing specific BPCR programs for adolescent pregnant women. Suggestions for future research of BPCR should be extended to a comparative study in unmarried and married adolescents. Moreover, a comparative study of BPCR between adolescent and adult pregnancy would also be interesting.
Strengths and Limitations
This study is the first study BPCR status in adolescent mothers. The questionnaire was an adapted version of JHPIEGO and was used by a single skilled and well-trained research assistant. However, there were many limitations to this study. First, it was cross-sectional design, which could not prove the relationship between variables. Second, the answers were self-reported and might be influenced by their families, resulting in a bias. Finally, this was a single study, for which the results could not be generalized to other urban settings.
Conclusion
Adolescent pregnancy is highly prevalent and carries risks of adverse obstetric outcomes. BPCR is an essential strategy to reduce obstetric and neonatal morbidities and mortalities. Adolescent pregnant women in urban areas had mostly good BPCR. The number of antenatal care visits ≥4 was significantly associated with good BPCR.
Acknowledgment
The authors would like to express gratitude to all participants in the study. The authors also express their gratitude and thanks to Mr. Jason Cullen for proofreading the earlier drafts of the manuscript. Finally, this study was made possible through funding and support from the Faculty of Medicine, Vajira Hospital, Navamindradhiraj University. The funders had no role in the study design, data collection and analysis, decision to publish or preparation of the manuscript.
Disclosure
The authors report no conflicts of interest in this research.
References
1. World Health Organization. Trends in Maternal Mortality: 1990 to 2015: Estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division. Geneva, Switzerland: World Health Organization; 2015.
2. Department of Economic and Social Affairs (UNDESA). UN Sustainable Development Goals, SDGs. Available from: https://sustainabledevelopment.un.org/sdg3.
3. Soubeiga D, Gauvin L, Hatem MA, Johri M. Birth Preparedness and Complication Readiness (BPCR) interventions to reduce maternal and neonatal mortality in developing countries: systematic review and meta-analysis. BMC Pregnancy Childbirth. 2014;14(1):1–11. doi:10.1186/1471-2393-14-129
4. World Health Organization. WHO Recommendations on Health Promotion Interventions for Maternal and Newborn Health. Geneva, Switzerland: World Health Organization; 2015.
5. JHIPEGO. Maternal and Neonatal Program. Birth Preparedness and Complication Readiness: A Matrix of Shared Responsibilities. Baltimore, USA: JHPIEGO; 2001.
6. JHPIEGO. Monitoring Birth Preparedness and Complication Readiness, Tools and Indicators for Maternal and Newborn Health. Johns Hopkins, Bloomberg School of Public Health, Center for Communication Programs, Maryland, USA: JHPIEGO; 2004.
7. World Health Organization. Birth and Emergency Preparedness in Antenatal Care: Standards for Maternal and Neonatal Care. Geneva, Switzerland: World Health Organization; 2002.
8. Tura G, Afework MF, Yalew AW. The effect of birth preparedness and complication readiness on skilled care use: a prospective follow-up study in Southwest Ethiopia. Reprod Health. 2014;11(1):1–10. doi:10.1186/1742-4755-11-60
9. Debelew GT, Afework MF, Yalew AW. Factors affecting birth preparedness and complication readiness in Jimma Zone, Southwest Ethiopia: a multilevel analysis. Pan Afr Med J. 2014;19:272. doi:10.11604/pamj.2014.19.272.4244
10. Bintabara D, Mohamed MA, Mghamba J, Wasswa P, Mpembeni RNM. Birth preparedness and complication readiness among recently delivered women in chamwino district, central Tanzania: a cross sectional study. Reprod Health. 2015;12(1):1–8. doi:10.1186/s12978-015-0041-8
11. Hailu M, Gebremariam A, Alemseged F, Deribe K. Birth preparedness and complication readiness among pregnant women in Southern Ethiopia. PLoS One. 2011;6(6):e21432. doi:10.1371/journal.pone.0021432
12. Omari PK, Afrane YA, Ouma P. Birth preparedness and complication readiness among women attending antenatal care clinic in health facilities within Bureti Sub County of Kericho County, Kenya. Am JMMS. 2016;6(4):123–128.
13. Rajesh P, Swetha R, Rajanna M, Krishna Iyengar MS. A study to assess the birth preparedness and complication readiness among antenatal women attending district hospital in Tumkur, Karnataka, India. IJCMPH. 2016;3(4):919–924.
14. Bitew Y, Awoke W, Chekol S. Birth preparedness and complication readiness practice and associated factors among pregnant women, Northwest Ethiopia. Int Sch Res Notices. 2016;2016:1–8. doi:10.1155/2016/8727365
15. Zepre K, Kaba M. Birth preparedness and complication readiness among rural women of reproductive age in Abeshige district, Guraghe zone, SNNPR, Ethiopia. Int J Womens Health. 2017;9:11–21. doi:10.2147/IJWH.S111769
16. Kamineni V, Murki AD, Kota VL. Birth preparedness and complication readiness in pregnant women attending urban tertiary care hospital. J Family Med Prim Care. 2017;6(2):297–300. doi:10.4103/2249-4863.220006
17. Kiataphiwasu N, Kaewkiattikun K. Birth preparedness and complication readiness among pregnant women attending antenatal care at the Faculty of Medicine Vajira Hospital, Thailand. Int J Womens Health. 2018;10:797–804. doi:10.2147/IJWH
18. Hailemariam A, Nahusenay H, Hana EG, Abebe A, Getaneh B. Assessment of magnitude and factors associated with birth preparedness and complication readiness among pregnant women attending antenatal care services at public health facilities in Debrebirhan Town, Amhara, Ethiopia, 2015. GJMR (E) Gynecol Obstet. 2016;16(2):38–44.
19. Musa A, Amano A. Determinants of birth preparedness and complication readiness among pregnant woman attending antenatal care at Dilchora Referral Hospital, Dire Dawa City, East Ethiopia. Gynecol Obstet. 2016;06(02):1–5. doi:10.4172/2161-0932
20. Mbalinda SN, Nakimuli A, Kakaire O, Osinde MO, Kakande N, Kaye DK. Does knowledge of danger signs of pregnancy predict birth preparedness? A critique of the evidence from women admitted with pregnancy complications. Health Res Policy Syst. 2014;12(1):1–7. doi:10.1186/1478-4505-12-60
21. Steinberg L. Study Guide for Steinberg’s Development: Infancy Through Adolescence. Belmont: Wadsworth Publishing; 2011.
22. Curtis AC. Defining adolescence. J Adolesc Health. 2015;7(2):1–39.
23. Rosen JR. Position Paper on Mainstreaming Adolescent Pregnancy in Efforts to Make Pregnancy Safer. Department of Making Pregnancy Safer. Geneva: World Health Organization; 2010.
24. Ganchimeg T, Mori R, Ota E, et al. Maternal and perinatal outcomes among nulliparous adolescents in low- and middle-income countries: a multi-country study. BJOG. 2013;120(13):1622–1630. doi:10.1111/1471-0528.12391
25. World Health Organization. Adolescent pregnancy; Fact sheet. 2018 Available from: https://www.who.int/news-room/fact-sheets/detail/adolescent-pregnancy.
26. Sukrat B. Thailand adolescent birth rate: trend and related indicators. Thai J Obstet Gynaecol. 2014;22(1):15–21.
27. IBM Corp. IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp; 2013.
28. Patil MS, Vedpathak VL, Aswar NR, Deo DS, Dahire PL. Birth preparedness and complication readiness among primigravida women attending tertiary care hospital in a rural area. Int J Community Med Public Health. 2016;3(8):2297–2304.
29. Joyce C, Grace O, Waithira M. Factors affecting birth preparedness among pregnant women attending public antenatal clinics in Migori County, Kenya. Biomed J Sci Tech Res. 2018;3(4):3409–3415.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.