Back to Journals » Clinical Ophthalmology » Volume 19
Biometric Factors in the VRF-G Formula for IOL Power Calculation
Authors Voytsekhivskyy OV ![]() , Biran A, Achiron A, Yahalomi T, Vega Y, Elbaz U, Levinger E
, Biran A, Achiron A, Yahalomi T, Vega Y, Elbaz U, Levinger E
Received 2 May 2025
Accepted for publication 22 July 2025
Published 31 July 2025 Volume 2025:19 Pages 2521—2528
DOI https://doi.org/10.2147/OPTH.S537931
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Oleksiy V Voytsekhivskyy,1 Amit Biran,2 Asaf Achiron,2 Tal Yahalomi,3 Yakov Vega,4 Uri Elbaz,5 Eliya Levinger2
1Department of Corneal Pathology, Ophthalmic Oncology and Oculoplasty, Kyiv Clinical Ophthalmology Hospital Eye Microsurgery Center, Kyiv, Ukraine; 2Department of Ophthalmology, Tel Aviv Sourasky Medical Center, Tel Aviv, Israel and Sackler School of Medicine, Tel Aviv University, Tel Aviv, Israel; 3Department of Ophthalmology, Samson Assuta Ashdod Hospital and the Faculty of Health Sciences, Ben-Gurion University of the Negev, Be’er Sheva, Israel; 4Department of Ophthalmology, Sheba Medical Center, Ramat-Gan and Sackler School of Medicine, Tel Aviv University, Tel Aviv, Israel; 5Department of Ophthalmology, Rabin Medical Center, Petach-Tikva and Sackler School of Medicine, Tel Aviv University, Tel Aviv, Israel
Correspondence: Oleksiy V Voytsekhivskyy, Department of Corneal Pathology, Ophthalmic Oncology and Oculoplasty, Kyiv Clinical Ophthalmology Hospital Eye Microsurgery Center, Komarov Ave. 3, Medical City, Kyiv, 03680, Ukraine, Tel +38067-584-28-11, Email [email protected]
Purpose: To assess the contribution of each optional parameter to the IOL power calculation and evaluate the effect of omitting biometric variables (ACD, LT, WTW) using the VRF-G formula.
Methods: A total of 501 eyes from 501 consecutive patients included in the study underwent cataract surgery with in-the-bag implantation of one-piece soft hydrophobic acrylic posterior chamber IOLs, AcrySof IQ SN60WF (Alcon Labs, Fort Worth, TX, USA). The primary calculation comprised five measured variables, and IOL power was recalculated for different combinations of omitting ACD, LT, and WTW. Outcome measurements included the difference in IOL power calculations between different omission combinations.
Results: Omitting any of the biometric variables resulted in a significant difference in the mean difference in IOL power calculation (ranging from 0.029 to 0.108 diopters), except for WTW omission alone (0.002 diopters). ACD proved to have the most impact, with its omission resulting in larger differences in power calculations (range: 0.177– 0.248 diopters) compared to combinations where ACD was not omitted (range: 0.057– 0.141 diopters). The shortest eyes were most affected by ACD omission.
Conclusion: The study highlights the importance of ACD in IOL power calculations, particularly for shorter eyes. WTW and LT were found to be less important when using the VRF-G formula for IOL power calculations.
Keywords: IOL power, formulas, VRF-formula, calculation, axial length
Introduction
Cataract surgery is one of the most common surgical procedures performed worldwide, in which the native opaque lens of the eye is replaced with a clear artificial intraocular lens (IOL). One of the most critical issues in attaining targeted refraction is predicting the IOL power in the eye following cataract surgery.1,2 There is no clinically relevant superiority among the latest generation formulas, and one formula may be slightly more accurate than another due to study design characteristics rather than the formula itself.3,4
The VRF (Voytsekhivskyy Regression Function) formula is empirical, and it estimates post-operative lens position using four predictors: axial length (AL), preoperative anterior chamber depth (corneal epithelium to anterior surface of the lens, ACD), corneal power (K), and horizontal corneal diameter (white to white (WTW)).5 The VRF-Gender (VRF-G) formula is a profound modification of the VRF formula, and it’s based on theoretical optics with regression and ray-tracing components. It includes VRF parameters (AL, ACD, K, WTW), as well as gender, preoperative refraction, lens thickness (LT), and central corneal thickness (CCT).6,7 The accuracy of this formula was proven by comparison to other traditional and recently developed intraocular lens formulas in general and short eyes in particular.6–10
Our previous report investigated the effect of different biometric data on the accuracy of IOL power calculation. Using the Barrett Universal II (hereafter, BUII) formula, a comparison of the results was achieved when all five relevant variables (AL, K’s reading, ACD, LT, and WTW values) were included in the calculation to the results achieved with different combinations of omission of one or more of these parameters.11,12 Our findings suggested that for the BUII, the omission of the investigated parameters from the calculation resulted in a clinically significant difference in IOL power calculation in short but not for the long or medium axial length ranges.
It remains unclear whether incorporating optional parameters yields a clinically significant difference in calculating the predicted IOL power using the VRF-G formula. To assess the contribution of each optional parameter to the IOL calculation, we evaluated the effect of the omission of three biometric variables (ACD, LT, and WTW) alone or in different combinations on the accuracy of IOL power calculation.
Materials and Methods
This retrospective study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of the Rabin Medical Center, Petah Tikva, Israel (Protocol N0775-18-RMC, date of approval 18/04/2019). Patients’ consent was waived due to retrospective data collection without identifying details.
The patients included in this study were patients from the daily practice. We analyzed 501 eyes of 501 consecutive patients undergoing uneventful phacoemulsification and in-the-bag implantation of one-piece soft hydrophobic acrylic posterior chamber IOLs AcrySof IQ SN60WF (501 eyes) (Alcon Labs, Fort Worth, TX, USA) between January 2019 and March 2020 at Rabin Medical Center, Petah Tikva, Israel. The cataract surgery with the phaco-chop technique was performed by the same surgeon (UE) with a temporal tunnel clear corneal incision of 2.5 mm. The study involved patients with a diagnosis of cataracts without comorbidity. The criteria for exclusion were any form of macular degeneration, any stage of glaucoma, corneal degenerative changes, corneal astigmatism greater than 2.0 diopter, any stage of keratoconus, and prior corneal refractive surgery. If patients had bilateral IOL surgery, a right eye was chosen for inclusion in the study.
Measurements were taken with the Swept-Source Optical Coherence Tomography (SS-OCT) biometry on IOLMaster 700, software version 1.70 (Carl Zeiss Meditec AG, Jena, Germany). Only measurements with good quality were included in the analysis since measurements with an exclamation (!) or asterisk (*) were eliminated. The BUII and SRK/T formulas were used as the actual IOL power formulas for preoperative calculation. Both formulas were accessible as a part of software V1.70 of the SS-OCT optical biometer.12,13 The Optimized A-constant of 119.0 and Lens Factor of 1.88 were used as recommended IOLCon platform (https://iolcon.org, accessed on January 30, 2020) for the SN60WF IOL.
Retrospectively, the IOL power targeting emmetropia was calculated using the VRF-G method. The VRF-G formula was previously described and showed promising results, especially in eyes with short axial lengths.7–9 It was programmed into Excel by the author (OVV). The optimized A-constant of 119.00 was used for the SN60WF IOL.
The primary calculation included only five measured variables (AL, K, ACD, LT, WTW) and was accepted as the reference measurement. Such variables as preoperative refraction, central corneal thickness, and gender were not included in this scrutiny. IOL power targeting emmetropia was recalculated for the seven combinations of omitting one or more of the ACD, LT & WTW values. Each result was compared to the reference measurement. After the operation, all patients underwent post-operative examinations by an experienced optometrist at 1 month. Post-operative examinations included uncorrected and best-corrected visual acuity, tonometry, automatic kerato-refractometry, and direct or indirect ophthalmoscopy. Patients who have post-operative corrected distance visual acuity of at least 20/40 were included in the study.
Statistical Analysis
Data were analyzed using SPSS software (SPSS for Windows, Version 22.0. IBMCorp, Armonk, NY, USA). The distribution normality of continuous variables was performed using the Kolmogorov–Smirnov test. The results indicated that the data were not normally distributed for the mean error and its absolute value (each P < 0.000). A non-parametric Friedman’s ANOVA test with Dunn’s post hoc test was used to compare the IOL dioptric power by the VRF-G formula. Correlation analyses were performed between the mean difference of the partial and complete VRF-G calculations and the AL, K, ACD, WTW, and LT readings (Spearman’s rho rank correlation). A value of p < 0.05 was considered statistically significant. Subgroup analysis was performed by AL: short (AL ≤ 22 mm), medium (22.01–25.99 mm), and long (AL ≥ 26 mm). A minimum sample size of 218 eyes was calculated using the PS program (version 3.0.12; Dupont WD, Plummer WD Jr. 2012).
Results
Demographics
In total, 501 right eyes of 501 patients were included in the present report. The mean age of patients was 65.2 ± 17.4 years, and the mean AL was 23.75 ± 1.88 mm. Of the 501 eyes in the study, 94 (18.8%) had short AL, 324 (64.7%) had medium AL, and 83 (16.6%) had long AL.
Whole Cohort Analysis
Table 1 presents the mean difference in IOL power results in different combinations of ACD, LT & WTW values omission compared to the result when all parameters are included in the calculation for the whole cohort. Every combination of omitted variables resulted in a meaningful difference in the mean difference in IOL power calculation (0.029–0.108 D), except for WTW omission alone (0.002 D).
 |
Table 1 Mean Difference in IOL Power Calculation Results Between Calculation Based on All Five Variables (AL, K, ACD, LT, WTW) and Calculation Conducted with the Omission of ACD, LT, and WTW Alone, in a Combination of Two of Them or Omitting All of Them |
Figure 1 presents the mean absolute difference in IOL power calculation for each omitting combination for the whole cohort. The most meaningful biometric value was the ACD – the four combinations included its omission, resulting in a larger difference in power calculations (range 0.177–0.248 D) compared to combinations in which ACD was not omitted (range 0.057–0.141 D). The least meaningful variable was WTW – its omission alone made a negligible impact on the calculation (0.057 D). Adding either WTW or LT to ACD omission resulted in a minor effect compared to the one observed for ACD alone (0.221 D and 0.196 D, respectively, compared to 0.248 D).
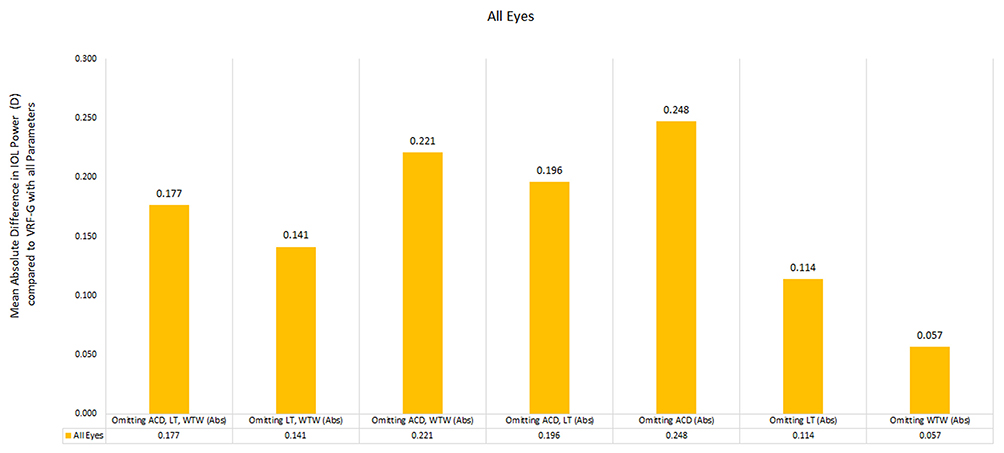 |
Figure 1 Bar presentation of the mean absolute difference in IOL power calculation results in the seven options of ACD, LT, WTW omission (alone or in combination) in the whole cohort. |
Analysis by AL
Figure 2 presents the mean difference in IOL power calculations for each of the omitting combinations stratified by the eye’s AL. In all omission combinations in which ACD is included, the eye’s axial length substantially affects the difference in IOL power calculation results – the shorter the eye, the larger the difference. When ACD has not been omitted, the effect of the omission is not affected by the AL.
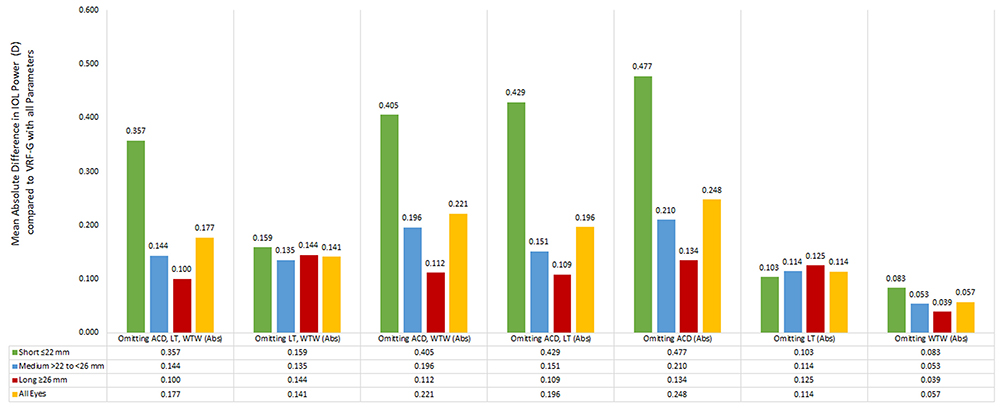 |
Figure 2 Bar presentation of the mean absolute difference in IOL power calculation results in the seven options of ACD, LT, and WTW omission stratified by eye length. |
Figure 3 further emphasizes this effect by analyzing the percentage of eyes with a mean absolute difference of 0.25 D or more for each of the omitting combinations and demonstrates that for longer eyes, the effect of ACD omission is smaller than the one observed for medium eyes and much smaller than the one observed for shorter eyes.
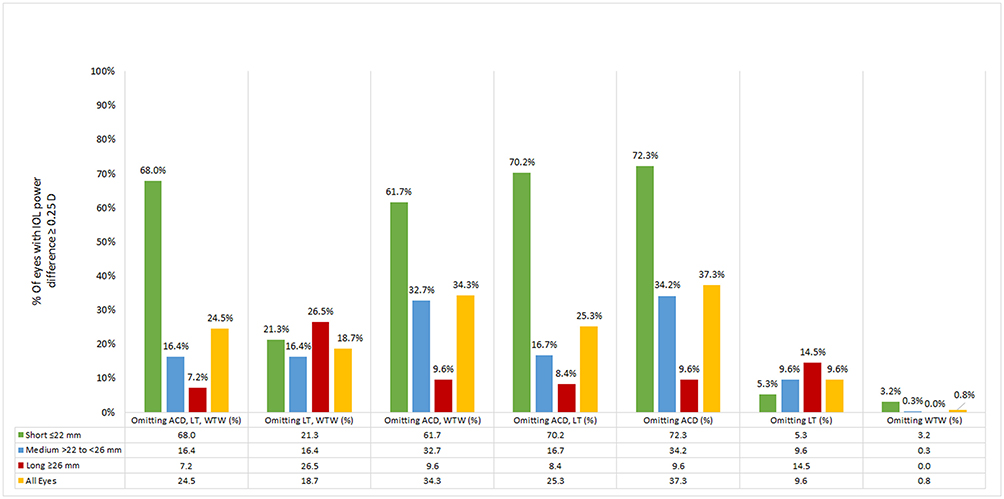 |
Figure 3 Bar presentation of the percentage of eyes in which the IOL power calculation resulted in a difference >0.25 diopter in the seven options of ACD, LT, and WTW omission stratified by eye length. |
Figure 4 presents a smooth line graph of the mean difference in IOL power calculation of the different omitting combinations in the whole cohort as a function of AL. While in short eyes, omitting ACD alone or in any combination causes a relatively more significant myopic difference, in longer eyes, the difference observed was much smaller and hyperopic. The differences for non-ACD omitting combinations are smaller, and their directions are opposite to the ACD omitting combinations (ie, hyperopic for short eyes and myopic for long eyes).
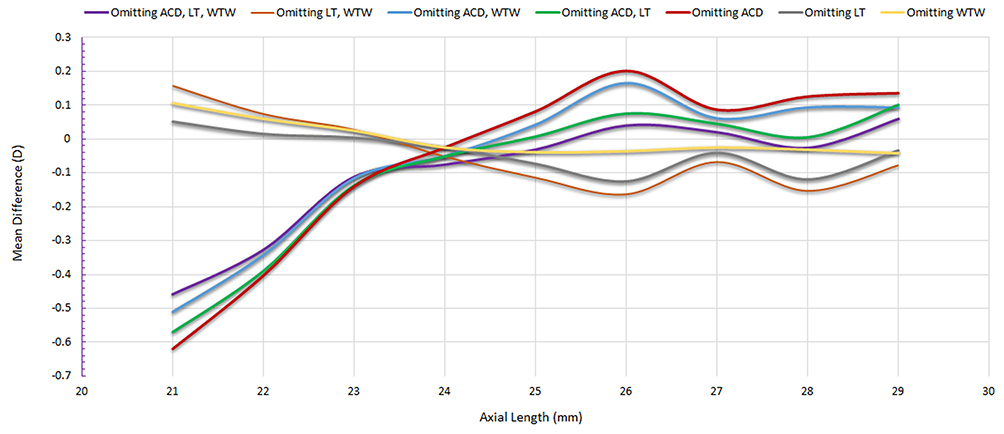 |
Figure 4 Smooth line presentation of mean difference in IOL power calculation results as a function of axial length in the seven options of ACD, LT, WTW omission combination. |
All omission options share the same point in which the difference changes from myopic to hyperopic at an AL of 24 mm. In eyes with AL of 23–25 mm, any omission of biometric value (ACD, LT, WTW) alone or in combination with the others has an insignificant effect on the IOL calculation results.
Discussion
To the best of our knowledge, this is the first study assessing the contribution of each optional parameter to the IOL calculation using the VRF-G formula. This study evaluated the effect of the omission of three biometric variables (ACD, LT, and WTW) alone or in different combinations on the accuracy of IOL power calculation. There is still no consensus on which traditional or modern intraocular power calculation methods are the most precise.3,6,7,10,14,15
We need to point out that although eyes with previous corneal refractive surgery were excluded, predicting IOL power in such eyes remains especially complex due to altered corneal parameters. In cases of corneal refractive surgery, there can be inaccurate measurements of anterior keratometry and variations in the keratometric index, making it necessary to use specific IOL power calculation methods.16
The VRF was created as a fourth-generation vergence formula that uses the CACD constant (similar to the ACD constant) and only four variables available on any partial coherence interferometry (PCI) biometer: AL, K, ACD, and WTW. This method was adopted for the parameters from the IOLMaster 500 (Carl Zeiss Meditec AG, Jena, Germany), and it does not, however, consider factors that can be obtained on other new-generation optical biometers, like lens thickness or central corneal thickness. The recently published results do not indicate that it is one of the most accurate algorithms.3,7,10
The VRF-G is a theoretical optics formula that incorporates regression and ray-tracing components, including AL, K, ACD, WTW, CCT, LT, preoperative refractive spherical equivalent, and gender. It utilizes an optical A-constant for the SRK/T formula.6,7,10 It is worth noting that although central corneal thickness (CCT) was not directly analyzed in the present study, its inclusion in the VRF-G formula highlights its wider clinical importance. It is also important to recognize that biometric parameters like CCT have implications beyond IOL power calculation, such as in tonometry, where it affects intraocular pressure measurement.17
This research supports results that were previously published in studies related to the accuracy of the VRF and VRF-G methods.3,5–10 Hipólito-Fernandes et al published an analysis of 828 patients with the same type of IOL AcrySof IQ SN60WF (Alcon Labs, Fort Worth, TX, USA). Comparing 13 IOL power calculation methods, the authors have found that the VRF-G formula had the lowest median absolute error (MedAE) over the entire axial length and the highest percentage of eyes within ±0.50D. Moreover, VRF-G had the lowest mean absolute error (MAE) in short eyes.7
Voytsekhivskyy et al6 studied nine IOL power formulas in 295 eyes. After optimization of the mean predicted error (PE) to zero, a statistically significant difference was found between the absolute errors of the Barrett, VRF, and VRF-G and other third-generation formulas (Hoffer Q, Holladay 1, and SRK/T, p < 0.006), but not Haigis, Holladay 2, and T2 formulas (p > 0.05). Notably, in terms of the standard deviation of the error (SD), the best results were shown by the VRF-G (0.464 D) and Haigis (0.466 D) formulas. In eyes with short axial lengths, the VRF and VRF-G were the most accurate methods (MedAE 0.243 and 0.258 D, respectively). Additionally, VRF-G achieved the highest value percentage of eyes with a PE within ±0.50 D (76.27%).
The findings of the present report show that the VRF-G intraocular lens power calculation formula agrees with the former report on the effect of biometric values omission on the BUII formula-based calculation of the IOL power.11 Both reports found that axial length is a significant factor influencing the extent of biometric value omission on IOL power calculation results. The difference in results is meaningful clinically for short eyes and much less meaningful for normal-length or long eyes.
Since the study includes eyes with long axial lengths (AL ≥ 26 mm), we should note that axial length correction factors can improve refractive accuracy in these cases.18 Cione et al19 demonstrated that group refractive index (GRI)-based biometers can cause systematic errors, especially in cataractous long eyes, and the advantages of AL adjustment in such eyes across traditional IOL formulas have been highly recommended.
The results of the present report demonstrated that omitting WTW and LT from the biometric values, regardless of the eye’s axial length, has little effect on IOL power calculation. In contrast, ACD omission has a significant effect on short eyes but not on long or average eyes. This finding implies the clinical significance of the ACD parameter in calculating IOL power, particularly in short eyes.
This could be explained by the significance of the ACD calculation on the effective lens position (ELP). Previous studies have shown that in short and normal eyes with an ACD < 2.5 mm, the calculation might affect the ELP.15
Jeong et al,20 studied Haigis, Hoffer Q, Holladay 1, and SRK/T formulas on 91 eyes of 91 patients with the same type of lens (Tecnis 1 ZCB00, Johnson & Johnson Vision, Jacksonville, FL, USA). They calculated the expected difference of each 3rd generation formula from the Haigis formula. Multiple regression analysis showed that preoperative ACD was the only significant factor for ELP prediction in all of the 3rd generation formulas. The authors revealed that for mean errors, axial length and post-operative change of ACD correlated significantly with the errors in all 3rd generation formulas, but not with errors of the Haigis formula. The preoperative ACD demonstrated the greatest influence concerning the expected difference between the third-generation and Haigis formulas. Thereby, post-operative change of ACD correlated significantly with errors of third-generation formulas according to simulated ACD. They supported our data that ACD is the most valuable predictor in the accuracy of modern formulas, especially in short axial length.
This study’s limitations include its retrospective design, which is common among studies evaluating IOL formulae. Conducting gender analysis with the same variables could be the next goal for future research. Furthermore, the sample size was relatively modest, and a larger-scale study should be done. Additionally, the optical biometry device type can affect the formula’s accuracy.21–23
Conclusion
In conclusion, applying our findings to a clinical setting suggests that when using the VRF-G formula for IOL power calculations, WTW and LT values are not essential, and omitting them does not affect the results of the IOL power calculation. In contrast, ACD values are significant for IOL power calculation in short eyes.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this work, the author did not use any artificial intelligence (AI) tool to write or prepare this manuscript or any of its parts.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
Dr Voytsekhivskyy is the inventor and sole owner of the VRF and VRF-G formulas and is the author and copyright holder of a computer program VRF Suite V1.7 (V/C/Systems, Kyiv, UA). The authors report no other conflicts of interest in this work.
References
1. Hoffer KJ, Savini G. Update on intraocular lens power calculation study protocols: the better way to design and report clinical trials. Ophthalmology. 2021;128(11):e115–e120. doi:10.1016/j.ophtha.2020.07.005
2. Wang L, Koch DD, Hill W, Abulafia A. Pursuing perfection in intraocular lens calculations: III. Criteria for analyzing outcomes. J Cataract Refract Surg. 2017;43(8):999–1002. doi:10.1016/j.jcrs.2017.08.003
3. Voytsekhivskyy OV, Hoffer KJ, Tutchenko L, Cooke DL, Savini G. Accuracy of 24 IOL power calculation methods. J Refract Surg. 2023;39(4):249–256. doi:10.3928/1081597X-20230131-01
4. Fernández J, Rodríguez-Vallejo M, Martínez J, Burguera N, Piñero D. Influence of the invariant refraction assumption in studies of formulas for monofocal and multifocal intraocular lens power calculation. Int Ophthalmol. 2022;42(8):2417–2424. doi:10.1007/s10792-022-02241
5. Voytsekhivskyy OV. Development and clinical accuracy of a new intraocular lens power formula (VRF) compared to other formulas. Am J Ophthalmol. 2018;185:56–67. doi:10.1016/j.ajo.2017.10.020
6. Voytsekhivskyy OV. Accuracy of the VRF and VRF-G intraocular lens power calculation formulas using swept-source optical coherence tomography biometry. Clin Ophthalmol. 2023;17:3663–3672. doi:10.2147/OPTH.S439287
7. Hipólito-Fernandes D, Elisa Luís M, Gil P, et al. VRF-G, a new intraocular lens power calculation formula: a 13-formulas comparison study. Clin Ophthalmol. 2020;14:4395–4402. doi:10.2147/OPTH.S290125
8. Voytsekhivskyy OV, Tutchenko L, Hipólito-Fernandes D. Comparison of the Barrett Universal II, Kane and VRF-G formulas with existing intraocular lens calculation formulas in eyes with short axial lengths. Eye. 2023;37(1):120–126. doi:10.1038/s41433-021-01890-7
9. Voytsekhivskyy OV, Hoffer KJ, Savini G, Tutchenko L, Hipólito-Fernandes D. Clinical accuracy of 18 IOL power formulas in 241 short eyes. Curr Eye Res. 2021;46(12):1832–1843. doi:10.1080/02713683.2021.1933056
10. Voytsekhivskyy OV, Hoffer KJ, Cooke DL, Savini G. IOL power calculation project: accuracy of 36 formulas. Am J Ophthalmol. 2025. doi:10.1016/j.ajo.2025.05.004
11. Vega Y, Gershoni A, Achiron A, et al. High agreement between Barrett Universal II calculations with and without utilization of optional biometry parameters. J Clin Med. 2021;10(3):1–7. doi:10.3390/jcm10030542
12. Barret GD. An improved universal theoretical formula for intraocular lens power prediction. J Cataract Refract Surg. 1993;19(6):713–720. doi:10.1016/s0886-3350(13)80339-2
13. Retzlaff JA, Sanders DR, Kraff MC. Development of the SRK/T intraocular lens implant power calculation formula. J Cataract Refract Surg. 1990;16(3):333–340. doi:10.1016/S0886-3350(13)80820-6
14. Melles RB, Kane JX, Olsen T, Chang WJ. Update on intraocular lens power calculation formulas. Ophthalmology. 2019;126(9):1334–1335. doi:10.1016/j.ophtha.2019.04.011
15. Yang S, Whang WJ, Joo CK. Effect of anterior chamber depth on the choice of intraocular lens calculation formula. PLOS ONE. 2017;12(12):e0189868. doi:10.1371/journal.pone.0189868
16. Cione F, De Bernardo M, Di Stasi M, De Luca M, Albano R, Rosa N. Lens factor choice in IOL power calculation after laser refractive surgery: the right constant for Advanced Lens Measurement Approach (ALMA). J Clin Med. 2024;13(17):5186. doi:10.3390/jcm13175186
17. De Bernardo M, Abbinante G, Borrelli M, Di Stasi M, Cione F, Rosa N. Intraocular pressure measurements in standing, sitting, and supine position: comparison between tono-pen avia and icare pro tonometers. J Clin Med. 2022;11(21):6234. doi:10.3390/jcm11216234
18. Voytsekhivskyy O, Tutchenko L. Comparison of the prediction accuracy of 13 formulas in long eyes. Graefes Arch Clin Exp Ophthalmol. 2023;261(9):2575–2583. doi:10.1007/s00417-023-06060-x
19. Cione F, De Bernardo M, Di Paola I, Caputo A, Graziano M, Rosa N. IOL power calculation in long eyes: selection of the best axial length adjustement factor using the most common formulas. Heliyon. 2024;10(17):e36609. doi:10.1016/j.heliyon.2024.e36609
20. Jeong J, Song H, Lee JK, Chuck RS, Kwon JW. The effect of ocular biometric factors on the accuracy of various IOL power calculation formulas. BMC Ophthalmol. 2017;17(1):62. doi:10.1186/s12886-017-0454-y
21. Pfaeffli OA, Weber A, Hoffer KJ, et al. Agreement of intraocular lens power calculation between 2 SS-OCT-based biometers. J Cataract Refract Surg. 2022;48(5):535–541. doi:10.1097/j.jcrs.0000000000000788
22. Galzignato A, Lupardi E, Hoffer KJ, Barboni P, Schiano-Lomoriello D, Savini G. Repeatability of new optical biometer and agreement with 2 validated optical biometers, all based on SS-OCT. J Cataract Refract Surg. 2023;49(1):5–10. doi:10.1097/j.jcrs.0000000000001023
23. Cooke DL, Cooke TL. Prediction accuracy of preinstalled formulas on 2 optical biometers. J Cataract Refract Surg. 2016;42(3):358–362. doi:10.1016/j.jcrs.2015.11.040
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Accuracy of the VRF and VRF-G Intraocular Lens Power Calculation Formulas Using Swept-Source Optical Coherence Tomography Biometry
Voytsekhivskyy OV
Clinical Ophthalmology 2023, 17:3663-3672
Published Date: 29 November 2023
Development and Clinical Accuracy of the New Paraxial Ray-Tracing IOL Power Formula (VRT) Based on the Thin Lens Assumption
Voytsekhivskyy OV
Clinical Ophthalmology 2026, 20:611115
Published Date: 29 May 2026