Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Biomarkers, Clinical Course, and Individual Needs in COPD Patients in Primary Care: The Study Protocol of the Stockholm COPD Inflammation Cohort (SCOPIC)
Authors Lundh L ![]() , Larsson K
, Larsson K ![]() , Lindén A
, Lindén A ![]() , Montgomery S
, Montgomery S ![]() , Palmberg L, Sandelowsky H
, Palmberg L, Sandelowsky H ![]()
Received 12 January 2022
Accepted for publication 11 April 2022
Published 2 May 2022 Volume 2022:17 Pages 993—1004
DOI https://doi.org/10.2147/COPD.S358056
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Prof. Dr. Richard Russell
Lena Lundh,1,2 Kjell Larsson,3 Anders Lindén,4,5 Scott Montgomery,6– 8 Lena Palmberg,3 Hanna Sandelowsky1,2,7
1Academic Primary Health Care Centre, Stockholm County Council, Stockholm, Sweden; 2Division of Family Medicine and Primary Care, Department of Neurobiology, Care Sciences and Society, Karolinska Institutet, Huddinge, Sweden; 3Division of Integrative Toxicology, Institute of Environmental Medicine, Karolinska Institutet, Stockholm, Sweden; 4Division for Lung and Airway Research, Institute of Environmental Medicine, Karolinska Institutet, Stockholm, Sweden; 5Karolinska Severe COPD Center, Department of Respiratory Medicine and Allergy, Karolinska University Hospital Solna, Stockholm, Sweden; 6Clinical Epidemiology and Biostatistics, School of Medical Sciences, Örebro University, Örebro, Sweden; 7Division of Clinical Epidemiology, Department of Medicine Solna, Karolinska Institutet, Stockholm, Sweden; 8Department of Epidemiology and Public Health, University College London, London, UK
Correspondence: Hanna Sandelowsky, Karolinska Institutet, Department of Medicine, Division of Clinical Epidemiology, Stockholm, SE-171 76, Sweden, Tel +46738902565, Email [email protected]
Background: To facilitate effective personalized medicine, primary health care needs better methods of assessing and monitoring chronic obstructive pulmonary disease (COPD).
Aim: This cohort study aims to investigate how biomarkers relate to clinical characteristics and COPD patients’ subjective needs over time.
Methods: Patients (n=750) in different COPD severity according to the GOLD criteria and age- and sex-matched controls (n=750) will be recruited over a period of 5 years from 15 primary health care centers in Region Stockholm, Sweden, and followed for 10 years in the first instance. Data on patients’ subjective needs will be collected via telephone/email, data on clinical/physiological variables (eg, symptoms, exacerbations, comorbidities, medications, smoking habits, lung function) from existing databases that are based on medical records, and data on biomarkers via repeated blood sampling. Quantitative and qualitative methods will be used. Initial results are expected after 2 years (feasibility test), and a larger body of evidence after 5 years.
Discussion: The study is expected to provide definitive and clinically useful scientific evidence about how biomarkers relate to clinical variables and patients’ subjective needs. This new evidence will facilitate accurate, and personalized COPD management by the use of valid biomarkers. It will provide useful tools for primary care professionals and may facilitate optimal self-management.
Keywords: airway inflammation, COPD, biomarkers, cohort, patients’ needs, personalized medicine, primary care
Introduction
Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disease that develops gradually and is due to exposure to noxious agents that are inhaled (eg, tobacco smoke, air pollution, work-related agents), being born prematurely, childhood respiratory infections, and alpha-1-antitrypsin deficiency.1,2 COPD is the third most common cause of disease-related mortality worldwide and is costly to society.3 An estimated 5% to 10% of the general population over 40 years of age have moderate or severe COPD, and as many as 50% of older smokers may have the disease.4,5 Diagnosis is based on the triage of harmful exposure, typical symptoms, and chronic airflow obstruction confirmed through spirometry. The recommended treatment is carried out inter-professionally; requires a long-term commitment from patients and professionals; and includes smoking cessation, pulmonary rehabilitation (physical activity and nutritional treatment), and pharmacological treatment with bronchodilators and anti-inflammatory drugs.6
Approximately 80% of patients with COPD have other co-existing chronic conditions, which is why primary care professionals are typically responsible for most COPD patients. Comorbidity tends to significantly worsen the prognosis of chronic conditions and complicate care.7,8 In Sweden, a combination of organizational problems (eg, heavy workload, staff shortages, time constraints), the complexity of managing multi-morbidity, and insufficient levels of COPD knowledge and management skills among clinicians has led to underdiagnosis and undermanagement of COPD.9,10 The situation is likely similar in other countries.
Given these circumstances, it is crucial to make the assessment of COPD as easy and reliable as possible. Guidelines currently recommend that clinicians use The Global Initiative for Chronic Lung Disease (GOLD) A-D classification system to assess COPD.3 This classification, based on information about COPD-related symptoms and exacerbation history, guides clinicians to recommended treatments.3 Some additional information on severity and prognosis can be obtained through spirometry measurements (GOLD severity stages 1–4) and the patient’s level of physical functioning. However, many primary care professionals regard current assessment methods as inaccurate, complex, time-consuming, and thus impractical. Misclassification may occur, which in turn can lead to nonoptimal care.11
Previous studies have found associations between COPD outcomes and each of the three aspects of COPD that we propose to study in The Stockholm COPD Inflammation Cohort (SCOPIC). However, a better understanding of patient’s subjective needs, clinical phenotyping, and endotyping—as well as the relationships between them—has the potential to make assessment of COPD status and prognosis more personalized and precise.
Patients’ Subjective Needs
In person-centered care, patients are partners in care and experts on their own experiences and subjective needs. Patients’ perspectives are integrated with the health care professionals’ evidence-based clinical assessments to make decisions about disease management. Person-centered care is thus an important complement to evidence-based care.
Core components of person-centered care include regarding each patient as a person with physical, emotional, and social needs.12 Meeting these needs promotes health. Education and support that are based on patient’s subjective experiences and needs can decrease anxiety and increase self-efficacy, health-related quality of life, and exercise capacity.13,14 It can also lead to fewer unscheduled physician visits, hospital admissions, and days in the hospital.15 Thus, it would be natural to assume that specialized COPD nurses have a thorough knowledge of patients’ needs, but this is not always the case. Time constraints and staffing shortages often force nurses to prioritize “mechanical” tasks, such as performing spirometry or demonstrating inhaler techniques, thus compromising person-centeredness and continuity of care.16 Additionally, conversations between professionals and patients may be challenging, as COPD is often lifestyle-related and can be stigmatized as a self-inflicted disease.17 Professionals can also find it frustrating if a patient is not motivated to make lifestyle changes.18
Many primary care patients with moderate to severe COPD have substantial needs for support in COPD self-management,19,20 and these needs can change over time (Sandelowsky, et al, in manuscript). To help busy primary care asthma/COPD nurses deliver optimal care, we need feasible and effective methods for assessing patients’ subjective COPD-related needs. The Lung Information Needs Questionnaire (LINQ) was developed to measure such needs.19 The LINQ is a brief review of patients’ subjective needs for information about disease knowledge, medication, self-management, smoking, diet, and exercise. However, it does not address a number of issues relevant to COPD nurses’ work. An example is multimorbidity. COPD patients with multi-morbidity may need particular support in self-management, use of healthcare, and understanding the ways that comorbid diseases affect each other.21 Other examples of issues not addressed by the LINQ include patients’ views on polypharmacy and patients’ social situations. Thus, to date, the LINQ has mainly been used by pulmonary rehabilitation professionals.19 Further investigation is required to determine whether the LINQ in its current form is an appropriate tool for primary care COPD nurses to use in assessing patients’ subjective needs.
Clinical Phenotyping
Identifying unique clinical COPD phenotypes might help individualize patient care. COPD phenotype refers to a disease attribute or combination of disease attributes that describe(s) differences between COPD patients based on clinically significant parameters, such as exacerbations, symptoms, treatment response, rate of disease progression, comorbidity, and mortality risk.22 Some investigators have defined clinical COPD phenotypes on the basis of exacerbation frequency, symptom patterns, inflammatory response, and dominant clinical manifestations (emphysema, chronic bronchitis, asthma-COPD overlap).23 More detailed models of clinical COPD phenotypes are needed to determine whether the proposed phenotypes are useful in clinical practice. For instance, the role of multi- and comorbidity in possible COPD phenotypes needs further investigation. Weighing the clinical relevance of co-existing diagnoses (eg, by disease categorizations according to Calderon-Larranaga, Charlson’s index, and Elixhauser’s index) may provide additional information about COPD prognosis.7,8,24
Biomarkers
Endotyping by quantifying alterations in biological markers (biomarkers) has the potential to facilitate personalized medicine. Endotyping improves characterization and classification of the disease and thus enables more accurate diagnosis and treatment.25 Thus, biomarkers could help with diagnosis, assessing prognosis, and monitoring treatment. However, despite previous attempts, there are no reliable, established laboratory tests to assess COPD characteristics among patients in clinical practice.
Inflammation can be detected by sampling the local airway (fraction of exhaled nitric oxide [FENO]), peripheral blood (C-reactive protein [CRP] or granulocytes), or urine (eicosanoids). However, a laboratory test for routine clinical use in primary care should meet all the following criteria: 1) sampling must be easy; 2) the result must be clear and precise; and 3) the result must provide decisive, clinically relevant information. Unfortunately, previously proposed biomarkers of systemic inflammation (eg, CRP, neutrophils, and eosinophils) or local inflammation (eg, FENO) do not fully meet these three criteria.
Evidence suggests that the inflammatory event behind COPD involves several inflammatory pathways. In these pathways, extracellular inflammatory mediators (cytokines and chemokines) affect the functions of a variety of structural and immune cells. Some of the currently known key components of these pathways are:
- Eosinophils. Eosinophil count in blood may help clinicians choose treatment and assess prognosis of COPD.3 It is a simple and inexpensive test that is already in use in routine care. Information about aspects of eosinophil mobilization can be used to support decisions about anti-inflammatory treatment and to prevent exacerbations in certain subtypes of COPD.26,27 Eosinophilic cationic protein (ECP) and eotaxin are biomarkers that are associated with changes in eosinophil levels in the blood of patients with COPD.28,29 Prospective studies are needed to confirm whether ECP and eotaxin measurements are superior to a simple eosinophil count for monitoring COPD progress.
- Neutrophils. Neutrophils are known mediators of inflammatory changes in COPD both at the local and the systemic level. Our research group has previously characterized systemic neutrophil mobilization, the CXC chemokine, the growth related oncogene-alpha (GRO-α) and interleukin(IL)-17A (formerly known as IL-17) in COPD during stable disease and exacerbations.30–32 At this systemic level, the average IL-17A concentration during stable disease is substantially lower in smokers with COPD than in controls, especially in the smokers with COPD whose lungs have been colonized by airway pathogens.30 The long-term alterations in IL-17 levels in COPD patients have not been studied.
- Lymphocytes. The number of CD8+ T lymphocytes is increased in the airways of patients with COPD. In advanced COPD, these cells are likely to contribute to disease pathogenesis and progression through inflammation, alveolar wall destruction, and small airway fibrosis.33,34 However, the association between clinical findings and levels of CD8+ T lymphocytes in peripheral blood is not yet clear.35,36
- Macrophages and epithelial cells. Inflammatory changes in COPD are also characterized by an imbalance of the proteolytic homeostasis between proteases (eg, matrix metalloproteinase-9 [MMP-9]) and antiproteases (such as tissue inhibitor of metalloprotease [TIMP]) and an increased degree of oxidative stress. This can lead to a higher number of goblet cells, increased mucus production, fibrosis development, and lung tissue destruction, which are characteristic changes in chronic bronchitis and COPD.37,38 Smoking induces an imbalance between oxidants and antioxidants, which leads to increased oxidative stress both locally in the lungs and systemically in the blood. The airway epithelium can produce secretory leukocyte protease inhibitor (SLPI) and 16-kDa club (Klara) cell secretory protein (CC16). SLPI is a serine protease inhibitor that can be produced by a number of cell types in the airways. SLPI has anti-inflammatory and antimicrobial properties and acts as an antiprotease.39 CC16, produced by Klara cells, may protect the airways from oxidative stress and inflammation,40 and reduced levels have been detected in smokers.41 Furthermore, studies have shown that decreased serum levels of CC16 are related to the severity of COPD.42 Measuring MMP-9, TIMP-1, and the ratio of these biomarkers, as well as SLPI, could help evaluate protease/antiprotease balance. CC16 analyzed in serum samples could be used to assess the presence of oxidative stress.
Most studies about COPD biomarkers have been conducted on patients who have had exacerbations and needed secondary care, often on fairly small numbers of patients. It is not clear whether and to what extent these biomarkers are useful in patients with mild to moderate disease. Typically, these patients visit only primary care. Further short- and long-term studies in clinical primary care contexts are needed, as are studies on the role of multimorbidity in inflammatory COPD processes.
SCOPIC aims to investigate how biomarkers relate to clinical characteristics and subjective needs of patients with COPD over the short and long term, including disease regression and progression. Our ultimate goal is to improve risk assessments and management of COPD.
Materials and Methods
SCOPIC is a prospective, observational cohort study that will include primary care patients with COPD (“study group”, n=750) and age- and sex matched controls who do not have COPD (“biomarker/clinical controls”, n=750) (Table 1). We intend to follow up the study patients and the biomarker/clinical controls individually for 10 years in the first instance via repeated measurements of clinical, physiological, and inflammatory (biomarker) variables. Additionally, the LINQ will be used to repeatedly assess patients’ subjective COPD-related needs and perspectives on COPD. We will recruit COPD patients who do not otherwise participate in SCOPIC to serve as controls for the LINQ subgroup (“LINQ controls”, n=300). Additionally, individual interviews will be conducted with approximately 15 to 20 participants in the study group to further explore patients’ subjective COPD-related needs.
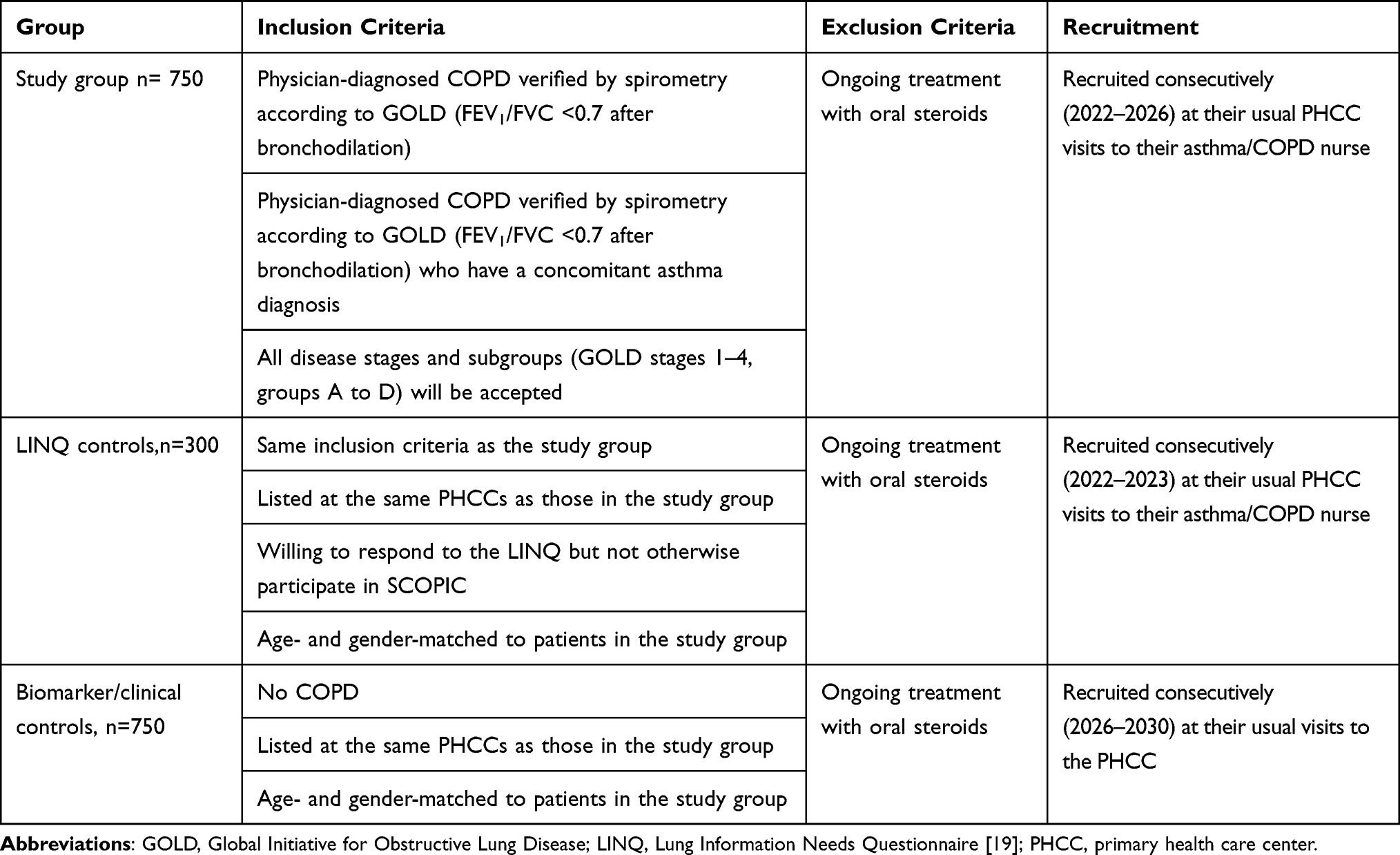 |
Table 1 SCOPIC Eligibility Criteria and Recruitment Procedure |
Participant Eligibility and Recruitment
Approximately half of the 210 primary healthcare centers (PHCCs) in the administrative area that constitutes the county of Stockholm (Region Stockholm) have a nurse-led asthma/COPD clinic. These PHCCs will be invited by email to participate in the study. At least 15 PHCCs will be included consecutively in the study.
Patient eligibility criteria and the SCOPIC recruitment procedure are summarized in Table 1. As we aim to study real-world COPD patients in primary care, all disease stages and subgroups (GOLD stages 1–4, groups A to D) will be accepted and patients will be recruited consecutively as they visit their physician or nurse at the PHCC. We plan to recruit the study group between 2022 and 2026, and the biomarker/clinical control group between 2025 and 2029. Clinical considerations make it necessary to recruit the study group and controls at separate times. Given the size of the project, it is necessary to test the feasibility of the study logistics (see description on page 13) prior to a full-scale study. This feasibility test will enable us to ensure that project resources are sufficient and that the project accommodates the realities of clinical primary care, particularly given the Covid-19 pandemic.
All patients will be recruited to the study consecutively by PHCC personnel at regular patient visits. A subset of the patients in the study group will participate in individual interviews. These patients will be recruited consecutively by the study nurse. The 300 LINQ controls will be recruited separately.
Patients are regularly treated with oral steroids will be excluded from the study, as oral steroid treatment may influence the biomarkers measured in the study.
Outcomes and Data Collection
Data collection (Table 2) will start in parallel with recruitment. Clinical and biomarker data will be collected via blood sampling taken at PHCC laboratories (sputum tests may later be performed in a subgroup of patients who provide specific written informed consent). Patients in the study group will contribute blood samples four times a year for 10 years, and the biomarker/clinical controls will do so twice a year. The samples will be transported by regular mail to and stored at the Karolinska Institutet Biobank. For the biomarker analyses, we will use methods based on the Enzyme-Linked Immunosorbent Assay (ELISA) technique. We will use the meso scale discovery (MSD) analysis in accordance with manufacturer instructions (https://www.mesoscale.com/). This method enables simultaneous analyses of several biomarkers in the same blood sample. Apart from the LINQ scores, all clinical data will be extracted retroactively from databases that are based on medical records and from Region Stockholm’s database that contains statistics on health care use and demographics. The dates of the blood samples will be matched with the dates of the clinical data, including the diagnoses registered at the visit, medications, and type of visit (urgent or regular). This information will enable us to determine the patient’s clinical COPD status when the blood sampling was taken (ie, stable COPD or acute exacerbation; see Table 1 for variable definitions). Data on patients’ subjective, COPD-related needs will be collected via the LINQ, which will be administered by the study nurse.
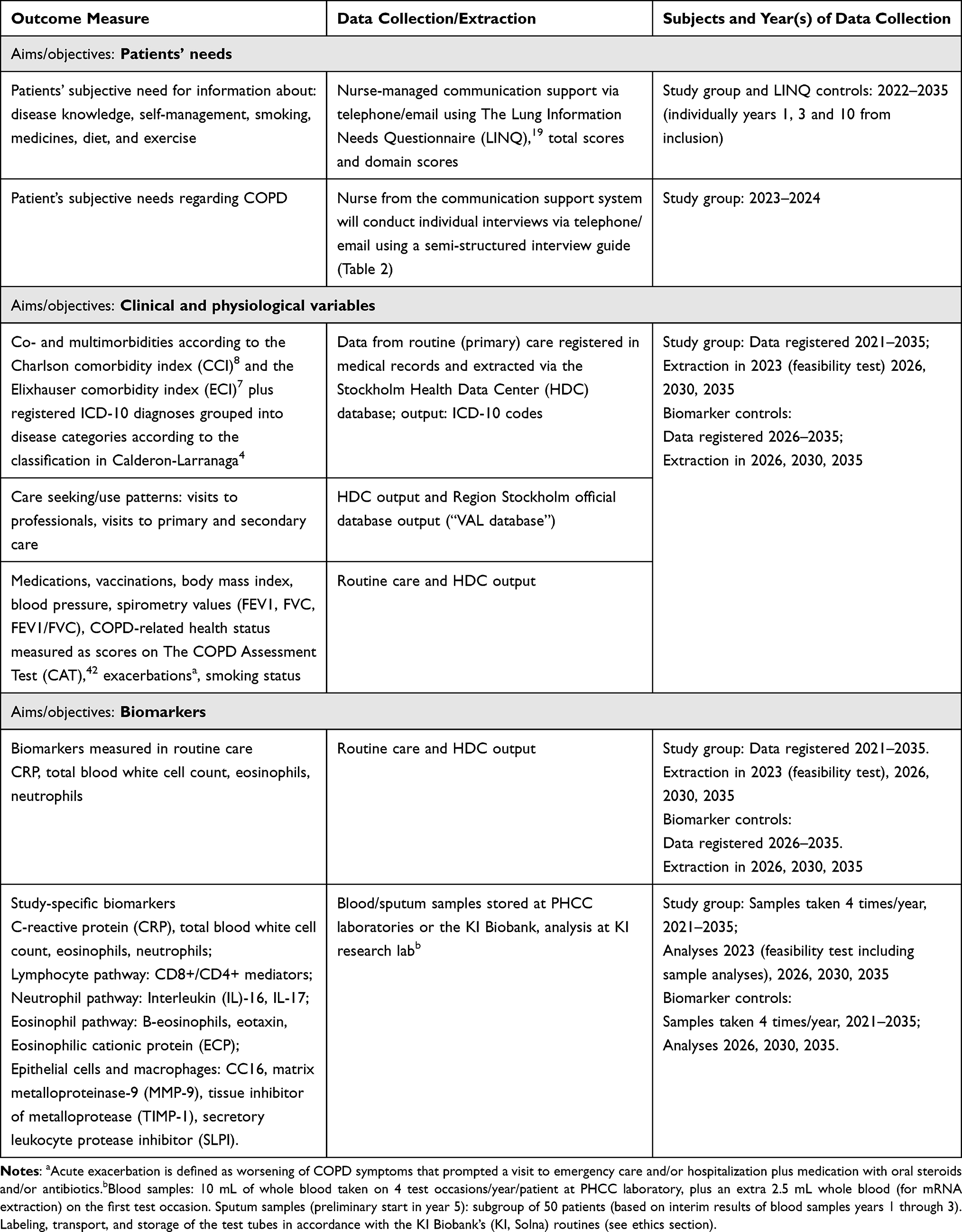 |
Table 2 Summary of Outcome Measures, Data Collection Methods and Years in SCOPIC |
Feasibility Test
As SCOPIC includes complicated procedures and study logistics, a feasibility test (pilot study) will be conducted. We will begin recruiting patients to the study group and the LINQ control group at three PHCCs in Region Stockholm in 2022. We have chosen these PHCCs because their catchment areas represent a variety of demographic and geographic locations (city, suburban, and rural) and ownership types (private and public). We will test the logistics at the PHCCs and the logistics of transporting samples between PHCCs and the biobank. Additionally, we will test the feasibility of the laboratory methods for biomarker analyses and the procedures for extracting clinical data from the databases, including matching the extracted data with the biomarkers. All data generated from the feasibility test in 2022 will be analyzed in 2023, and the results will be published in peer-reviewed scientific articles.
After making any needed adjustments to study logistics, we will continue with PHCC and study group recruitment for another 5 years by inviting PHCCs with nurse-led asthma/COPD clinics until at least 750 patients with COPD have been consecutively included in the study group. Recruitment of the 300 LINQ controls will continue until 2023.
The Study Nurse
To facilitate patient interest in participating throughout the initial 10-year study period, a study nurse will support participants by providing information and reminders (eg, about blood sampling) throughout the study period. This interaction between participants and the research group, which will primarily occur via telephone and email, will be used to collect data about patients’ subjective COPD-related needs (see Table 3) and to respond to patients’ questions. A study nurse who is specialized in asthma/COPD but has no other contact with the participants will manage this communication. The nurse-managed support will be available to patients in the study group and the biomarker/clinical control group but not to the LINQ controls. When needed, the study nurse will also facilitate contacts and communication between the researchers, PHCCs, local labs, and biobank.
 |
Table 3 The Semi-Structured Interview Guide Used in the Qualitative Study About COPD Patients’ Needs and Perspectives About Their Illness |
Statistics
Sample Size
Given the size of the population of primary care patients with COPD in Region Stockholm, we expect it to take approximately 5 years to recruit 750 patients. We have used two methods to estimate the minimum size of our cohort: one based on biomarkers and one based on clinical variables. Both methods indicate that 750 patients should provide sufficient power:
- The variability and reproducibility of COPD biomarkers remain uncertain. However, higher levels of CRP in blood are associated with higher levels of systemic inflammation. With a power calculation based on the assumption that in one year, approximately 25% of the patients in the study population will experience a COPD exacerbation, and a further assumption that these patients account for the highest 15% of CRP values in blood, we will need at least 260 patients in our study group.
- The score from the validated symptom assessment tool, the COPD Assessment Test (CAT)43 is a clinical variable associated with the progression of COPD.19 With a power calculation based on the minimum clinically important difference in CAT scores (= 2 points) and its standard deviation,44 and assuming a dropout rate of 30% and an intracluster coefficient (for PHCCs) of 0.04, we will need at least 325 patients in our study group.
However, loss to follow-up is usually substantial in long-term cohort studies. This may be particularly true of longitudinal studies of older patients with chronic diseases, who often have multimorbidity. Thus, we aim to include 750 patients, ie, 150 patients a year for five years. We estimate that each PHCC will have at least 150 registered patients with COPD and that approximately 85% of them visit the center at least once every 18 months.45 We will therefore need to recruit at least 15 centers (approximately 50 participants per center) to the study. For the studies on patients’ subjective COPD-related needs, a power calculation based on previous publications about LINQ scores (rather than CAT scores as described above) would have been preferable. However, this was not possible, as only an informal minimal clinically important difference (MCID) is currently available for the LINQ.19
Data Analyses
Quantitative analyses will use parametric and non-parametric methods, including logistic regression and Cox regression. P values of <0.05 will be considered statistically significant. All final data at the individual level will be adjusted after univariate significance tests have been performed. In addition, all final data at the PHCC level will be adjusted for clusters (= PHCCs), baseline data, and sociodemographic factors.
Qualitative research methods, eg, inductive content analysis by Elo and Kyngäs46 will be used for interview studies. A purposive sampling of participants, data collection through interviews with a semi-structured interview guide (Table 3), will be used. The analysis is based on systematically deriving concepts from the data.
Discussion
COPD is a complex clinical challenge. Early detection is crucial, and diagnosis is often difficult, as are monitoring the disease and predicting its different phases over time. Additionally, diverse aspects of multimorbidity, symptom adaptation, and questioning the patient’s lifestyle (smoking) complicate COPD management. We expect the present study to contribute scientific evidence, including biomarkers and a deeper understanding of patient needs, that will facilitate simpler, more accurate, and personalized management of COPD. This new evidence will be particularly useful to primary care professionals, as they are responsible for the vast majority of patients with COPD. The results will also have the potential to promote optimal self-management of COPD, which is central to managing and living with this life-long chronic condition.
Although patients who are on regular medication with oral corticosteroids will be excluded from the study, short-term oral steroid treatment against acute exacerbation of COPD will not lead to an exclusion. However, short-term steroid treatments will be taken into particular consideration when the results of the biomarker analyses are interpreted.
We anticipate a number of methodological challenges. The feasibility testing at the three PHCCs (see page 13 and Table 4) is a response to potential challenges such as recruiting PHCCs and patients, engaging PHCC staff in the study and the logistics of collecting samples and delivering them to the biobank. At the moment, this is particularly challenging in primary health care because of the heavy workload due to the Covid-19 pandemic. Another anticipated challenge is maintaining participating patients’ interest and engagement over the entire study period. The telephone and email support provided by the study nurse is designed in part to help us meet this challenge (eg, through reminders). It is possible that the support provided by the nurse will improve participants’ health, but these potential improvements will not bias the associations between biomarkers and clinical variables. Additionally, as most patients will be middle-aged or older and often suffer from other chronic diseases as well as COPD, the participation may be interrupted by death. Hence, we aim at doubling the number of participants that is determined by power calculation. Assessment of selection bias will be undertaken, especially where it might result in spurious associations. However, as the majority of COPD patients in primary care are in milder severity stages of COPD (GOLD 1–3 and/or A-C) at the time of the inclusion, we assess that most of them will be able to complete the 10-year follow-up period.
 |
Table 4 SCOPIC Time Plan |
Self-reported data (eg, questionnaire responses) and data extracted from databases and medical records have strengths and limitations. For example, data from the LINQ can be biased by problems with the responder’s recall and interpretation of the questions and replies. Register data may be biased by discrepancies between what has actually been done and what has been entered in the medical records, register, or database.
Abbreviations
CAT, the COPD Assessment Test; CC16, 16-kDa club cell secretory protein; COPD, chronic obstructive lung disease; CRP, C-reactive protein; ECP, eosinophilic cationic protein; FENO, Fraction of exhaled nitric oxide; GCP-2, granulocyte chemotactic factor; GOLD, The Global Initiative for Chronic Lung Disease; GRO-α, growth related oncogene-alpha; IL, Interleukin; LINQ, The Lung Information Needs Questionnaire; MMP-9, matrix metalloproteinase-9; MCID, minimal clinically important difference; PHCC, primary health care center; SCOPIC, The Stockholm COPD Inflammation Cohort study; SLPI, secretory leukocyte protease inhibitor; TIMP, tissue inhibitor of metalloprotease.
Data Sharing Statement
Data analyzed in this study will be available from the corresponding author in response to requests that comply with ethical principles of good research.
Ethics Approval and Consent to Participate
The present study complies with the Declaration of Helsinki. The study, including a model consent form and other related documentation for participants, has been approved by the Swedish Ethical Review Authority (ref 2021-00398). Prior to enrollment, all participants will provide written informed consent.
Acknowledgments
The authors would like to thank the Region Stockholm Study Unit and Karolinska Institutet Biobank for help with study logistics and biobank services and scientific editor Kimberly Kane for language improvement throughout the text.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception or study; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study will be funded by The Swedish Heart and Lung Association and Region Stockholm (formerly the Stockholm County Council), and more funding will be applied for in coming years to cover study costs. The funders will not play any role in study design; collection, management, analysis, and interpretation of data; writing manuscripts, posters, or other reports of study results; or the decision to submit descriptions of results for publication.
Disclosure
Lena Lundh has no conflicts of interests. Anders Lindén has, during the last five years, obtained research grants from and/or served as consultant in advisory boards organized by AstraZeneca, Boehringer-Ingelheim, Chiesi, GlaxoSmithKline and Novartis. Kjell Larsson has, during the last five years, on one or more occasion served in an advisory board and/or served as speaker and/or participated in education arranged by AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Orion, Novartis, Mylan, Sanofi and Teva. Scott Montgomery and Lena Palmberg have no conflicts of interests. Hanna Sandelowsky has, during the last five years, received honoraria for educational activities from Boehringer Ingelheim, Novartis, AstraZeneca, Chiesi, and TEVA. Hanna Sandelowsky reports personal fees from GlaxoSmithKline outside the submitted work.
References
1. Grahn K, Gustavsson P, Andersson T, et al. Occupational exposure to particles and increased risk of developing chronic obstructive pulmonary disease (COPD): a population-based cohort study in Stockholm, Sweden. Environ Res. 2021;200:111739. doi:10.1016/j.envres.2021.111739
2. World Health Organization. Chronic obstructive pulmonary disease (COPD) [homepage on the Internet]; 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-copd.
3. Global initiative for chronic obstructive lung disease [homepage on the Internet]; 2022. Available from: http://www.goldcopd.com/.
4. Lundback B, Lindberg A, Lindstrom M, et al. Not 15 but 50% of smokers develop COPD?–Report from the obstructive lung disease in Northern Sweden studies. Respir Med. 2003;97(2):115–122. doi:10.1053/rmed.2003.1446
5. Backman H, Vanfleteren L, Lindberg A, et al. Decreased COPD prevalence in Sweden after decades of decrease in smoking. Respir Res. 2020;21(1):283. doi:10.1186/s12931-020-01536-4
6. Läkemedelsverkets riktlinjer för behandling av kroniskt obstruktiv lungsjukdom [The Swedish Medical Products Agency’s guidelines for treatment of chronic obstructive pulmonary disease] [homepage on the Internet]; 2015. Available from: https://www.lakemedelsverket.se/sv/behandling-och-forskrivning/behandlingsrekommendationer/sok-behandlingsrekommendationer/lakemedel-vid-kroniskt-obstruktiv-lungsjukdom-kol–behandlingsrekommendation.
7. Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med Care. 1998;36(1):8–27. doi:10.1097/00005650-199801000-00004
8. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
9. PRAXIS-studien astma KOL [The PRAXIS study of asthma and COPD] [homepage on the Internet]; 2022. Available from: http://www.praxisstudien.se/.
10. OLIN-studierna [The OLIN studies] [homepage on the Internet]; 2021. Available from: https://www.norrbotten.se/olin.
11. Blonde L, Khunti K, Harris SB, Meizinger C, Skolnik NS. Interpretation and Impact of real-world clinical data for the practicing clinician. Adv Ther. 2018;35(11):1763–1774. doi:10.1007/s12325-018-0805-y
12. Fawcett J. The metaparadigm of nursing: present status and future refinements. Image J Nurs Sch. 1984;16(3):84–89. doi:10.1111/j.1547-5069.1984.tb01393.x
13. Zwerink M, Brusse-Keizer M, van der Valk PD, et al. Self management for patients with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2014;(3):CD002990. doi:10.1002/14651858.CD002990.pub3
14. Sjöstrand T, Sulaiman J. Living with COPD – Experiences from Daily Life. A Literature Review. [Degree Project in Nursing 15 Credit Points]. Accra: Malmö University; 2020.
15. Lisspers K, Johansson G, Jansson C, et al. Improvement in COPD management by access to asthma/COPD clinics in primary care: data from the observational PATHOS study. Respir Med. 2014;108:1345–1354. doi:10.1016/j.rmed.2014.06.002
16. Sundström JWM Distriktssköterskans erfarenheter av kroniskt obstruktiv lungsjukdom i primärvården - en kvalitativ intervjustudie [District nurse’s experiences of chronic obstructive pulmonary disease in primary care: a qualitative interview study] [thesis]. Accra: Högskolan i Dalarna; 2020. Available from: http://www.diva-portal.org/smash/get/diva2:1390121/FULLTEXT01.pdf.
17. Lundh L, Hylander I, Tornkvist L. The process of trying to quit smoking from the perspective of patients with chronic obstructive pulmonary disease. Scand J Caring Sci. 2012;26(3):485–493. doi:10.1111/j.1471-6712.2011.00953.x
18. van Eerd EA, van Rossem CR, Spigt MG, Wesseling G, van Schayck OC, Kotz D. Do we need tailored smoking cessation interventions for smokers with COPD? A comparative study of smokers with and without COPD regarding factors associated with tobacco smoking. Respiration. 2015;90(3):211–219. doi:10.1159/000398816
19. Jones RC, Wang X, Harding S, Bott J, Hyland M. Educational impact of pulmonary rehabilitation: lung information needs questionnaire. Respir Med. 2008;102(10):1439–1445. doi:10.1016/j.rmed.2008.04.015
20. Sandelowsky H, Krakau I, Modin S, Stallberg B, Nager A. COPD patients need more information about self-management: a cross-sectional study in Swedish primary care. Scand J Prim Health Care. 2019;37(4):459–467. doi:10.1080/02813432.2019.1684015
21. Ansari S, Hosseinzadeh H, Dennis S, Zwar N. Patients’ perspectives on the impact of a new COPD diagnosis in the face of multimorbidity: a qualitative study. NPJ Prim Care Respir Med. 2014;24:14036. doi:10.1038/npjpcrm.2014.36
22. Han MK, Agusti A, Calverley PM, et al. Chronic obstructive pulmonary disease phenotypes: the future of COPD. Am J Respir Crit Care Med. 2010;182(5):598–604. doi:10.1164/rccm.200912-1843CC
23. Miravitlles M, Calle M, Molina J, et al. Spanish COPD Guidelines (GesEPOC) 2021: updated Pharmacological treatment of stable COPD. Arch Bronconeumol. 2021;58:T69–T81. doi:10.1016/j.arbres.2021.03.026
24. Calderon-Larranaga A, Vetrano DL, Onder G, et al. Assessing and measuring chronic multimorbidity in the older population: a proposal for its operationalization. J Gerontol a Biol Sci Med Sci. 2017;72(10):1417–1423. doi:10.1093/gerona/glw233
25. Ciprandi G, Tosca MA, Silvestri M, Ricciardolo FLM. Inflammatory biomarkers for asthma endotyping and consequent personalized therapy. Expert Rev Clin Immunol. 2017;13(7):715–721. doi:10.1080/1744666X.2017.1313117
26. Ho J, He W, Chan MTV, et al. Eosinophilia and clinical outcome of chronic obstructive pulmonary disease: a meta-analysis. Sci Rep. 2017;7(1):13451. doi:10.1038/s41598-017-13745-x
27. Andelid K, Andersson A, Yoshihara S, et al. Systemic signs of neutrophil mobilization during clinically stable periods and during exacerbations in smokers with obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2015;10:1253–1263. doi:10.2147/COPD.S77274
28. Perng DW, Wu CC, Su KC, Lee YC, Perng RP, Tao CW. Inhaled fluticasone and salmeterol suppress eosinophilic airway inflammation in chronic obstructive pulmonary disease: relations with lung function and bronchodilator reversibility. Lung. 2006;184(4):217–222. doi:10.1007/s00408-005-2586-8
29. D’Armiento JM, Scharf SM, Roth MD, et al. Eosinophil and T cell markers predict functional decline in COPD patients. Respir Res. 2009;10:113. doi:10.1186/1465-9921-10-113
30. Andelid K, Tengvall S, Andersson A, et al. Systemic cytokine signaling via IL-17 in smokers with obstructive pulmonary disease: a link to bacterial colonization? Int J Chron Obstruct Pulmon Dis. 2015;10:689–702. doi:10.2147/COPD.S76273
31. Andersson A, Malmhall C, Houltz B, et al. Interleukin-16-producing NK cells and T-cells in the blood of tobacco smokers with and without COPD. Int J Chron Obstruct Pulmon Dis. 2016;11:2245–2258. doi:10.2147/COPD.S103758
32. Andersson A, Bossios A, Malmhall C, et al. Effects of tobacco smoke on IL-16 in CD8+ cells from human airways and blood: a key role for oxygen free radicals? Am J Physiol Lung Cell Mol Physiol. 2011;300(1):L43–55. doi:10.1152/ajplung.00387.2009
33. Gadgil A, Duncan SR. Role of T-lymphocytes and pro-inflammatory mediators in the pathogenesis of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2008;3(4):531–541. doi:10.2147/COPD.S1759
34. Williams M, Todd I, Fairclough LC. The role of CD8 + T lymphocytes in chronic obstructive pulmonary disease: a systematic review. Inflamm Res. 2021;70(1):11–18. doi:10.1007/s00011-020-01408-z
35. Forsslund H, Mikko M, Karimi R, et al. Distribution of T-cell subsets in BAL fluid of patients with mild to moderate COPD depends on current smoking status and not airway obstruction. Chest. 2014;145(4):711–722. doi:10.1378/chest.13-0873
36. Hodge G, Nairn J, Holmes M, Reynolds PN, Hodge S. Increased intracellular T helper 1 proinflammatory cytokine production in peripheral blood, bronchoalveolar lavage and intraepithelial T cells of COPD subjects. Clin Exp Immunol. 2007;150(1):22–29. doi:10.1111/j.1365-2249.2007.03451.x
37. Fischer BM, Pavlisko E, Voynow JA. Pathogenic triad in COPD: oxidative stress, protease-antiprotease imbalance, and inflammation. Int J Chron Obstruct Pulmon Dis. 2011;6:413–421. doi:10.2147/COPD.S10770
38. Padra M, Andersson A, Levanen B, et al. Increased MUC1 plus a larger quantity and complex size for MUC5AC in the peripheral airway lumen of long-term tobacco smokers. Clin Sci. 2020;134(10):1107–1125. doi:10.1042/CS20191085
39. Weldon S, McGarry N, Taggart CC, McElvaney NG. The role of secretory leucoprotease inhibitor in the resolution of inflammatory responses. Biochem Soc Trans. 2007;35(Pt 2):273–276. doi:10.1042/BST0350273
40. Broeckaert F, Bernard A. Clara cell secretory protein (CC16): characteristics and perspectives as lung peripheral biomarker. Clin Exp Allergy. 2000;30(4):469–475. doi:10.1046/j.1365-2222.2000.00760.x
41. Bernard A, Roels H, Buchet JP, Lauwerys R. Decrease of serum Clara cell protein in smokers. Lancet. 1992;339(8809):1620. doi:10.1016/0140-6736(92)91891-B
42. Rong B, Fu T, Gao W, et al. Reduced serum concentration of CC16 is associated with severity of chronic obstructive pulmonary disease and contributes to the diagnosis and assessment of the disease. Int J Chron Obstruct Pulmon Dis. 2020;15:461–470. doi:10.2147/COPD.S230323
43. Jones PW, Harding G, Berry P, Wiklund I, Chen WH, Kline Leidy N. Development and first validation of the COPD assessment test. Eur Respir J. 2009;34(3):648–654. doi:10.1183/09031936.00102509
44. Kon SS, Canavan JL, Jones SE, et al. Minimum clinically important difference for the COPD assessment test: a prospective analysis. Lancet Respir Med. 2014;2(3):195–203. doi:10.1016/S2213-2600(14)70001-3
45. Stockholms läns sjukvårdsområde bokslut 2018 [Stockholm County Council annual financial report 2018] [homepage on the Internet]; 2018. Available from: http://www.e-magin.se/paper/35ggrq8m/paper/1#/paper/35ggrq8m/42.
46. Elo S, Kyngas H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–115. doi:10.1111/j.1365-2648.2007.04569.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.