")
Back to Journals » Journal of Hepatocellular Carcinoma » Volume 11
Biochemical Safety of SBRT to Multiple Intrahepatic Lesions for Hepatocellular Carcinoma
Authors Hall JT, Moon AM, Young M, Tan X, Darawsheh R , Danquah F, Tepper JE, Yanagihara TK
Received 28 October 2023
Accepted for publication 6 February 2024
Published 5 March 2024 Volume 2024:11 Pages 443—454
DOI https://doi.org/10.2147/JHC.S447025
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David Gerber
Jacob T Hall,1 Andrew M Moon,2,3 Michael Young,1 Xianming Tan,3,4 Rami Darawsheh,5 Flora Danquah,3 Joel E Tepper,1,3 Ted K Yanagihara1,3
1Department of Radiation Oncology, University of North Carolina Hospitals, Chapel Hill, NC, USA; 2Division of Gastroenterology and Hepatology, Department of Medicine, University of North Carolina, Chapel Hill, NC, USA; 3Lineberger Comprehensive Cancer Center, University of North Carolina Hospitals, Chapel Hill, NC, USA; 4Gillings School of Global Public Health, University of North Carolina, Chapel Hill, NC, USA; 5University of North Carolina School of Medicine, Chapel Hill, NC, USA
Correspondence: Ted K Yanagihara, Department of Radiation Oncology, 101 Manning Drive CB #7512, Chapel Hill, NC, 27514, USA, Tel +1-984-974-0400, Email [email protected]
Background: We aim to better characterize stereotactic body radiation therapy (SBRT)-related hepatic biochemical toxicity in patients with multiple intrahepatic lesions from hepatocellular carcinoma (HCC).
Methods: We conducted a retrospective analysis of patients with HCC who underwent SBRT for 2 or more synchronous or metachronous liver lesions. We collected patient characteristics and dosimetric data (mean liver dose [MLD], cumulative effective volume [Veff], cumulative volume of liver receiving 15 Gy [V15Gy], and cumulative planning target volume [PTV]) along with liver-related toxicity (measured by albumin-bilirubin [ALBI] and Child–Pugh [CP] scores). A linear mixed-effects model was used to assess the effect of multi-target SBRT on changes in ALBI.
Results: There were 25 patients and 56 lesions with median follow-up of 29 months. Eleven patients had synchronous lesions, and 14 had recurrent lesions treated with separate SBRT courses. Among those receiving multiple SBRT courses, there were 7 lesions with overlap of V15Gy (median V15Gy overlap: 35 mL, range: 0.5– 388 mL). There was no association between cumulative MLD, Veff, V15Gy, or PTV and change in ALBI. Four of 25 patients experienced non-classic radiation-induced liver disease (RILD), due to an increase of CP score by ≥ 2 points 3 to 6 months after SBRT. Sixteen of 25 patients experienced an increase in ALBI grade by 1 or more points 3 to 6 months after SBRT. Comparing the groups that received SBRT in a single course versus multiple courses revealed no statistically significant differences in liver toxicity.
Conclusion: Liver SBRT for multiple lesions in a single or in separate courses is feasible and with acceptable risk of hepatotoxicity. Prospective studies with a larger cohort are needed to better characterize safety in this population.
Keywords: HCC, SBRT, reirradiation, multi-site, toxicity
Introduction
The incidence of HCC has steadily increased over the last 20 years or more.1 Radiation therapy was initially used for palliation and has historically had a limited role in the management of HCC, largely because early experience using older radiation techniques resulted in excessive normal tissue toxicity, and prospective data are sparse.2–4 Over the last several decades, rigorous studies have investigated liver tolerance to irradiation and defined safe treatment parameters.5,6 This body of work, along with improvements in radiotherapy delivery techniques, such as SBRT, have led to numerous retrospective and prospective series demonstrating excellent disease control with a favorable toxicity profile.
Despite excellent local control (LC) in the range of 75–90% beyond two years,7–11 patients with localized HCC treated with SBRT, or other focal therapies, will often have recurrence within the liver, and many present with multiple lesions over time.12–14 Additionally, 80–90% of patients with HCC have clinically significant underlying liver disease,15 and functional liver reserve is an important consideration when selecting the optimal locoregional therapy for recurrent HCC. Furthermore, radiation tolerance of the liver is known to be worse in patients with underlying cirrhosis compared to those without cirrhosis.16,17 Re-irradiation poses unique challenges, primarily due to a poor radiobiological understanding of how the liver recovers from prior radiation dose and how volumetric constraints may need to be modified based on prior treatment.18 Data evaluating the efficacy and safety of SBRT in cirrhotic patients who have been previously irradiated or have multiple sites within the liver being irradiated simultaneously are very limited.19–26 To our knowledge, only two studies19,20 have evaluated hepatotoxicity in the setting of re-irradiation using the albumin-bilirubin (ALBI) score, which is more objective than the CP score.27,28 Our goal is to better characterize SBRT-related hepatic toxicity in patients with HCC and underlying cirrhosis who were treated with SBRT to multiple synchronous or metachronous targets.
Materials and Methods
Patient Characteristics
This study was reviewed and approved by the University of North Carolina institutional review board (UNC IRB 23–1226), and all research was conducted in compliance with the Declaration of Helsinki. All data were deidentified, and patient confidentiality was upheld. Informed consent was waived due to the retrospective nature of this study. All patients with primary HCC liver lesions that received SBRT at our institution from January 2010 to December 2022 were reviewed. We included patients treated with SBRT (5 or fewer fractions) and 2 or more liver targets, which could include two or more lesions treated in one course of radiation, a locally recurrent tumor, or intrahepatic recurrence distant from a previously treated site. Patients that received prior liver-directed therapies, which could include transarterial chemoembolization (TACE), transarterial radioembolization (TARE), surgical resection, and/or radiofrequency ablation (RFA), were also included. No performance status criteria were used for inclusion or exclusion in this study, but this was a factor considered by the multi-disciplinary tumor board and treating physician when deciding to treat the patient. HCC was diagnosed radiographically using LiRads criteria or pathologically. Relevant patient characteristics and data were recorded retrospectively.
Radiation Planning and Techniques
The decision to treat a lesion with SBRT versus other local-regional modalities was made during a multi-disciplinary tumor board. All patients received SBRT using either the CyberKnife (Accuray, Inc., Sunnyvale, CA) radiotherapy system or a standard linear accelerator with a treatment protocol that was derived from a prospective institutional trial.29 The CyberKnife system utilized Synchrony motion management, and all patients treated using CyberKnife required percutaneous intrahepatic placement of fiducial markers near the target(s), typically with three or more markers adjacent to the lesion (and no more than 6 cm away). Four-dimensional 3-mm and free-breathing 1-mm computed tomography (CT) images were obtained at the time of simulation. The simulation CT image set was fused with the most recent magnetic resonance imaging (MRI) image set (T1 sequence with gadolinium contrast) for contouring target visualization. Other MRI sequences, including delayed phase and b800 diffusion-weighted images, were also fused when it was thought they would aid in target delineation. The planning target volume (PTV) typically included a 5-mm radial and 8-mm craniocaudal volumetric expansion from the GTV depending on the tumor size, location, and radiotherapy system used. For the initial SBRT course, at least 700 cc of liver minus PTV was planned to receive 15 Gy or less in 3–5 fractions. In cases of repeat SBRT, liver dose constraints were modified at the physician’s discretion, although the same dose constraint was often used. Liver dosimetry was described using cumulative values of the following: mean liver dose (MLD), volume of liver receiving 15 Gy (V15Gy), and the effective volume (Veff). Cumulative values were defined as the sum of each for each SBRT course/plan. For example, if a patient was treated with a single SBRT course/plan but multiple targets were included, the MLD for that plan represented the cumulative value.
Prior liver radiation dose was accounted for by assuming the V15Gy from the prior SBRT course, if there was one, was non-functioning liver. In cases where lesions were treated during a second or third course of SBRT, dose was allowed to cover the area that previously received 15 Gy, but the liver volume that previously received 15 Gy was not included in the calculation of “spared liver” in the new plan. Meaning, the prior V15Gy was subtracted from the liver volume when ensuring the second or third SBRT plan would satisfy dose constraints. Dose constraints for other organs-at-risk (OARs) are listed in Table 1. The majority of patients were treated with 3 fractions, administered every other day (prescription dose and number of fractions listed in Table 2).
 |
Table 1 3-Fraction Liver SBRT Dose Constraints |
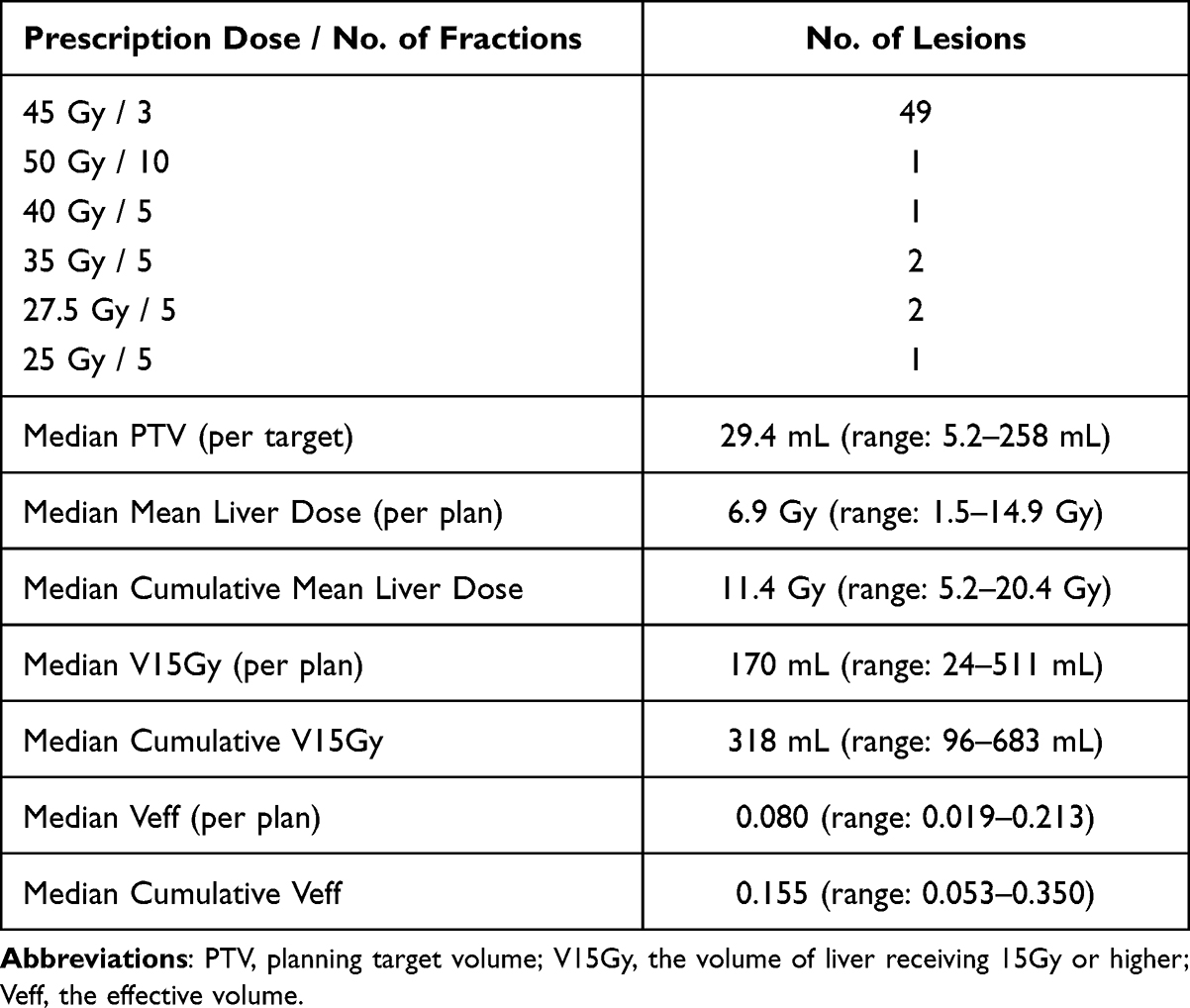 |
Table 2 Dosimetric Characteristics for the Entire Cohort |
Calculation of the Effective Liver Volume (Veff)
Veff, represented as a fraction of total liver volume, was calculated using a previously established procedure known as the Kutcher–Burman Veff DVH reduction scheme.30,31 The calculation of Veff requires the selection of a constant volume effect parameter (n), used in the calculation for all patients. The volume effect parameter is unique for a given organ and complication of interest when applying the NTCP model.31 The volume effect (n) for the purposes of this study was 0.97 and selected based on a previously published analysis of 203 patients.32 The rationale for selecting 0.97 is further described in the Discussion.
Calculation of Predicted Functional Liver Volume
Predicted functional liver volume (pFLV) is a tool initially used in surgical literature to estimate the optimal size of liver grafts needed for transplantation.33 In summary, the underlying concept is that there exists a correlation between body surface area (BSA) and volume of functioning liver needed for normal physiologic function. The calculation for pFLV was completed using a previously established technique.33
Follow-Up and Outcomes
Patients were evaluated by a radiation oncologist before and during SBRT and generally seen every 3–6 months following radiation for the first 5 years. The following tests were ordered at each follow-up visit per the treating physician’s discretion: abdominal MRI with and without contrast, CBC, CMP, and INR. Classic RILD was defined as elevated alkaline phosphatase to more than 2 times the upper limit of normal or baseline value, anicteric hepatomegaly, and ascites typically 2 weeks to 3 months following radiation.34,35 Non-classic RILD was defined as elevated liver transaminases more than 5 times the upper limit of normal or a worsening of CP by ≥2 points, typically occurring within 3 months of radiation.34,35 CP and ALBI scores were calculated at each follow-up visit. Disease progression, using LiRads criteria, was defined based on multi-phasic imaging, almost entirely by MRI, by board-certified radiologists with experience interpreting post-SBRT imaging along with multidisciplinary review. Local progression was defined on post-SBRT MRI, typically in the presence of any new nodular arterial phase hyperenhancement with washout or growth on sequential scans. The time point of local progression used was the date of the imaging study used to first detect the recurrent disease. We compared outcomes (detailed below) for those treated with a single course of SBRT to those treated with a second or third course of SBRT for intrahepatic recurrence.
Statistical Analysis
Patients were categorized into two groups: single course (N=11) and re-irradiation (N=14). Numerical variables, such as prescription dose and ALBI score, were summarized by their median and range (min, max) for each group. Categorical variables, such as sex and etiology, were described using frequencies. For assessing the effect of multiple-course SBRT on changes in the ALBI score from baseline to both 3-month and 6-month timepoints, we employed a linear mixed-effects model. The change in ALBI score served as the dependent variable, with the group label (single vs multiple rounds of SBRT) as the primary covariate. We adjusted for cumulative MLD, cumulative Veff, cumulative V15Gy, and cumulative PTV. Additionally, a random effect for subjects was introduced to accommodate the dependence of repeated measurements within patients in the re-irradiation group. An effect was deemed statistically significant if the p-value (obtained using the Wald-type test) for its associated regression coefficient was below 0.05.
This study was presented at the American Society of Clinical Oncology Gastrointestinal Cancers Symposium, San Francisco, January 18, 2024.36
Results
Patient and Dosimetric Characteristics
There were 25 patients and 56 lesions. All patients had primary HCC, and 24/25 patients were diagnosed with cirrhosis prior to the first course of SBRT. For the entire cohort, median follow-up from time of initial SBRT until last follow-up or death was 29 months (range: 3–55 months). The median age was 67 years (range: 52–84). Median liver volume and pFLV at time of initial SBRT were 1469 mL (range: 1019–3172 mL) and 1708 mL (range: 1198–2340 mL), respectively. The median tumor size for the entire cohort was 2.0 cm (range: 1–5.2 cm). Eight of 25 patients were Barcelona Clinic Liver Cancer (BCLC) A while the remaining 17/25 were BCLC C. Additional patient characteristics are displayed in Table 3.
 |
Table 3 Baseline Characteristics Comparison for Those That Received SBRT in a Single Course versus Multiple Courses |
There were 11 patients with multiple radiation targets treated during the same course of SBRT and 14 separate patients with multiple radiation targets treated in separate courses of SBRT. The median number of lesions treated per patient was 2 (range: 2–4). Of the 14 patients who underwent SBRT in multiple courses, the median interval between courses was 15 months (range: 6–40 months). Thirteen of these 14 patients received 2 courses of SBRT, and 1 received 3. Among those who received more than 1 SBRT course, there were 7 lesions with overlap of V15Gy from prior SBRT (median V15Gy overlap: 35 mL, range: 0.5–388 mL). One patient of 25 was treated using a standard linear accelerator, while the remaining 24 were treated using the CyberKnife radiotherapy system. Additional comparison of dosimetric variables between groups is displayed in Table 4.
 |
Table 4 Dosimetric Characteristics and Pre-SBRT ALBI Compared for Patients That Received Single and Multiple Courses of SBRT |
Toxicity, Survival, and Local Failure
Of 56 lesions, there were 8 local failures at a median of 8 months (range: 4–25 months) after SBRT. The median overall survival (OS) was 25 months. By multivariate linear mixed effects model, there was no association between cumulative MLD, Veff, V15Gy, or PTV and change in ALBI at 3 or 6 months following SBRT. Sixteen of 25 patients experienced a change in ALBI grade by 1 or more points at 3 and/or 6 months following SBRT. Thirteen of 25 and 4/25 patients experienced worsening of CP score of ≥1 or ≥2 points at 3 or 6 months following SBRT, respectively. Of the 4 patients with worsening CP, 3/4 patients experienced corresponding worsening of ALBI grade. Of the 16 patients that experienced worsening of ALBI grade of 1 or more points, 11 also experienced a worsening of CP by 1 or more points. The only patients with non-classic RILD were those with an increase of CP score of ≥2 points. No patients experienced liver transaminase elevation meeting criteria for RILD. One patient met criteria for classic RILD by experiencing worsening of alkaline phosphatase to more than twice the upper limit of normal 3 months after SBRT. The same patient experienced a worsening of CP score by 1 point at this time but never a worsening of CP score by 2 points or more. Of patients who received radiation to multiple lesions in a single course, the rate of worsening CP score by ≥1 and ≥2 points was 45% (5/11 patients) and 18% (2/11 patients), respectively. Of patients who received radiation in multiple courses, the rate of worsening CP score by ≥1 and ≥2 points was 57% (8/14 patients) and 14% (2/14 patients), respectively (CP ≥1: p=0.86; CP ≥2: p=1). The following paragraphs detail the 4 patients who experienced worsening of CP score of ≥2 points following SBRT (denoted as patients 1–4). Table 5 displays relevant dosimetric characteristics and ALBI and CP scores of these four patients.
 |
Table 5 Dosimetric Characteristics for the 4 Patients Experiencing an Increase in CP of ≥2 Points |
Discussion
Patients with primary HCC will often present with multiple synchronous lesions or experience recurrent/new intra-hepatic lesions following the initial diagnosis.12–14 Furthermore, SBRT is increasingly used in this population, raising the need to better characterize liver toxicity for patients with multiple targets.37 This paper reports outcomes for 25 patients with multiple primary or recurrent HCC liver tumors treated with SBRT. Four of 25 patients (16%) experienced non-classic RILD by worsening of CP score by 2 points or more following SBRT (3/4 patients at 3 months and 1 patient at 6 months). Three of these 4 patients experienced corresponding worsening in ALBI grade as defined by Johnson et al.38 Sixteen of 25 patients experienced worsening of ALBI grade by 1 or more points at 3 or 6 months following SBRT. Neither cumulative MLD, Veff, V15Gy, nor PTV was associated with worsening liver function as measured by ALBI. Treating multiple lesions in the same course compared to multiple courses separated by time did not appear to lead to higher risk of liver dysfunction.
Rates of worsening liver function following SBRT to multiple targets in this study are similar to other published studies.19–24 However, many of these studies prescribed doses in 5 fractions and to a biologically effective dose lower than the most commonly prescribed dose in this study, 45 Gy in 3 fractions. Additionally, many patients in other studies had liver metastases without cirrhosis. As measured by ALBI, Kimura et al reported rates of rates of liver dysfunction following liver SBRT in a series of 81 patients treated with 4–5 fraction courses of SBRT. They found no statistically significant difference in ALBI following the first versus second course of liver SBRT.20 McDuff et al reported a series in a Western population of 49 patients with 64 tumors that received repeat liver irradiation, with 27 of these patients receiving repeat irradiation with SBRT in 5–6 fractions (others received IMRT or 3DCRT).22 Nineteen of the 49 patients had primary HCC. They reported 2 patients who met criteria for non-classic RILD.22 The study by Eriguchi et al is a retrospective review of toxicity following repeat SBRT for recurrent primary HCC in 52 patients with 148 liver lesions.19 Approximately half their patients were prescribed 54 Gy in 3 fractions (for lesions ≤3 cm). Although they did not report significant worsening of CP scores following the second SBRT course, they did find a significant decline in liver function as measured by modified ALBI at 6, 12, and 24 months.19
There are many confounders to account for when comparing retrospective toxicity rates across studies in this population, but the rate of non-classic RILD in this study appears similar to those previously reported. Three of the 4 patients with worsening CP score by 2 or more points at 3 or 6 months following SBRT in this study had CP scores of B7 prior to the SBRT course. Prior studies have reported higher rates of liver dysfunction following liver SBRT for patients with baseline CP-B liver function, suggesting these patients have a lower tolerance of radiation to the liver.39,40 Of these 4 patients, there were also 2 with significantly higher pFLVs compared to their actual measured liver volume, suggesting there was little reserve. Cirrhosis of the liver may cause both enlargement and decrease in liver size, with the latter typically occurring during later stages of disease which may have further predisposed these patients to liver dysfunction following SBRT.41 Patient 1, who experienced a worsening of CP by 2 points, was prescribed 27.5 Gy in 5 fractions, which is a biologically effective dose that is much lower than what most patients in this study or others received.7–11,19–24 This, in combination with the opinion of the hepatologist, suggests that the liver function decline was due to intrahepatic progression rather than SBRT.
Re-irradiation and Recovery
Several dose constraints for liver SBRT have been published, but to our knowledge there are no standard dose constraints for liver re-irradiation.17,37,42,43 Overlapping V15Gy is an important consideration when comparing toxicity rates in patients who received SBRT in multiple courses. The overlapping V15Gy, often used as the threshold dose in 3 fractions to cause normal liver parenchyma dysfunction, between SBRT courses was quite small relative to the size of the liver for patients in our study.42–44 This suggests that much of the hepatic parenchyma receiving meaningful radiation doses (defined as 15 Gy or higher) in the second course of SBRT was not previously irradiated (received less than 15 Gy during the initial SBRT course) and should represent functional tissue. Our institutional dose constraints (Table 1) were often not modified for patients treated with a second or third course of SBRT, but prior radiation volumes were accounted for. This was accomplished by subtracting V15Gy from the initial SBRT course from the liver volume when planning the second SBRT course (further described in the Materials and Methods section). However, we acknowledge that the best way to account for prior liver SBRT is an open question. Although there was a relatively small number of patients, there was no statistically significant difference between cumulative V15Gy, Veff, or PTV between the groups in the study that received a single course of SBRT versus multiple courses. This suggests the total volume of liver irradiated was similar between the group that received SBRT to multiple targets in a single course versus SBRT to multiple targets in multiple courses.
Several studies, including the study presented here, have shown no increased risk of RILD following repeat SBRT using standard initial SBRT dose constraints suggesting regenerative capacity of the liver. However, in many studies it is unclear how close the patients were to violating the initial dose constraints with the initial course of SBRT. In our study, the median cumulative V15Gy was 318 mL, and median cumulative Veff was 0.16, with median liver volume of 1458 mL, suggesting it would have been possible to treat additional liver volume without violating liver dose constraints.
Dosimetric Variables, Veff, and the Selection of the Volume Parameter
We selected Veff, among other variables, to compare radiation plans between the subgroups that received SBRT in a single course versus multiple courses. MLD and V15Gy were also reported and used in comparison, but we acknowledge their limitations. MLD does not account for the heterogeneity of dose distribution within the liver and may be misleading for volumes of liver receiving high and low doses. Fifteen Gy in 3 fractions is believed to cause liver dysfunction in the irradiated volume and is a dose parameter used in published dose constraints.42,44,45 Therefore, V15Gy may be a useful surrogate to estimate the effect of different radiation plans on normal liver tissue. However, this excludes the liver exposed to a dose lower than 15 Gy which may also be affected to some degree.39 For the purposes of our study, we felt a variable that also captures volumes treated to doses lower than 15 Gy, such as Veff, would allow for a better comparison.
Initially, Veff was created to compare normal tissue complication probability (NTCP) between three-dimensional treatment plans prior to modern treatment-planning software.30,31 It reduces the dose volume histogram for a radiation plan to a single number which allows for more practical numeric and statistical comparison. Involved in the calculation of Veff is the selection of the volume effect (n), which is unique for a given organ and complication of interest.31 The relationship between radiation dose and risk of RILD has been studied extensively by several groups, with seminal work being performed at the University of Michigan and Princess Margaret Hospital.16 From this and including more contemporary studies, we found value estimates of n that range between 0.23 and 1.1.32,46,47 Of the available, large, contemporary databases identified that provide estimates for these values, we elected to use values drawn from patients where Hep B is not endemic because this most closely represents the Western population in our cohort. Therefore, we estimated n for patients with primary liver cancer to be 0.97.32
When using dosimetric variables to compare liver radiation dose across plans, we may also consider the functional liver requirement for each patient. That is, the volume of functional liver required to sustain an individual’s liver function. These data and estimates were originally drawn from surgical transplantation literature, and the correlation is a function of BSA.33 The necessary size of a patient’s liver relative to BSA is further complicated in our cohort by cirrhosis and prior local-regional therapy, but it is worth noting that the median liver volume prior to SBRT was lower than the median pFLV for patients in this study.
Limitations
As with any study investigating the effects of radiation on normal liver tissue, there are many confounding factors and comorbidities in this population, and this study is no exception, also limited by its relatively low power. Coincidental occurrence of acute decompensation of cirrhosis during one of the standard follow-up visits could affect the results in this small study, especially with few patients experiencing RILD. Patients with cirrhosis or without HCC can develop worsening of liver function due to natural progression of liver disease. The rate of decline is driven by many factors including the extent of baseline fibrosis, ongoing liver injury due to untreated viral hepatitis or alcohol use, or systemic inflammation or infections. Conversely, abstinence from alcohol, improvements in diet and exercise, and treatment of viral hepatitis can lead to improvement in liver function. Prior evidence suggests that patients with compensated cirrhosis have a 5% per year risk of decompensation (defined as bleeding due to esophageal varices, ascites, jaundice, or encephalopathy), excluding additional risk due to SBRT.48 Patients with worse baseline liver function (CP-B) may be at higher risk of worsening liver function due to liver SBRT,5 and this should be better studied considering the relatively low proportion of CP-B patients included in this study. We would also like to acknowledge that this study focuses on liver toxicity of liver SBRT and does not report toxicities that may be related to incidental radiation of other surrounding organs, such as the lungs and bowel. Additionally, this was a well-selected population in that patients that the treating radiation oncologist and multi-disciplinary tumor board thought would tolerate SBRT well were selected to receive SBRT. Although we have compared the proportions of patients that received local-regional therapies prior to SBRT between the groups that received a single versus multiple courses of SBRT, we acknowledge the variability of local-regional therapies that is not accounted for. For example, the range of the volumes treated with transarterial therapies can be large.
Conclusions
SBRT to multiple lesions is feasible and does not appear to lead to unacceptable risk of classic or non-classic RILD. The risk when treating multiple synchronous lesions does not appear to be elevated compared to treating multiple lesions in multiple SBRT courses when controlling for treatment volume. We acknowledge the limitations of this study, including the small sample size, and the need for larger studies to better understand the effects of SBRT to multiple liver targets in this population.
Abbreviations
ALBI, albumin-bilirubin; BSA, body surface area; CP, Child–Pugh; CT, computed tomography; Veff, effective volume, Gy, gray; HCC, hepatocellular carcinoma; LC, local control; MRI, magnetic resonance imaging; MLD, mean liver dose; NAFLD, nonalcoholic fatty liver disease; NTCP, normal tissue complication probability; OARs, organs at risk; OS, overall survival; PTV, planning target volume; pFLV, predicted functional liver volume; RILD, radiation-induced liver disease, SBRT, stereotactic body radiation therapy; RFA, radiofrequency ablation; TACE, transarterial chemoembolization; n, volume effect; V15Gy, volume of liver receiving 15 Gy.
Acknowledgments
This study was presented at the American Society of Clinical Oncology Gastrointestinal Cancers Symposium, San Francisco, January 18, 2024.
Funding
There is no funding to report.
Disclosure
AMM reports grants or contracts from the American Association for the Study of Liver Diseases, the American College of Gastroenterology, and the National Institutes of Health; and consulting fees from Target RWE; and serves on the American Association for the Study of Liver Diseases Practice Guidelines Committee. TKY reports grants or contracts from the Radiation Oncology Institute and Lineberger Comprehensive Cancer Center. The authors report no other conflicts of interest in this work.
References
1. Kulik L, El-Serag HB. Epidemiology and management of hepatocellular carcinoma. Gastroenterology. 2019;156(2):477–491.e1. doi:10.1053/j.gastro.2018.08.065
2. Chamseddine I, Kim Y, De B, et al. Predictive model of liver toxicity to aid the personalized selection of proton vs photon therapy in hepatocellular carcinoma. Int J Radiat Oncol Biol Phys. 2023:S0360301623001049. doi:10.1016/j.ijrobp.2023.01.055
3. Russell AH, Clyde C, Wasserman TH, Turner SS, Rotman M. Accelerated hyperfractionated hepatic irradiation in the management of patients with liver metastases: results of the rtog dose escalating protocol. Int J Radiat Oncol Biol Phys. 1993;27(1):117–123. doi:10.1016/0360-3016(93)90428-X
4. Blomgren H, Lax I, Näslund I, Svanström R. Stereotactic high dose fraction radiation therapy of extracranial tumors using an accelerator: clinical experience of the first thirty-one patients. Acta Oncologica. 1995;34(6):861–870. doi:10.3109/02841869509127197
5. Velec M, Haddad CR, Craig T, et al. Predictors of liver toxicity following stereotactic body radiation therapy for hepatocellular carcinoma. Int J Radiat Oncol Biol Phys. 2017;97(5):939–946. doi:10.1016/j.ijrobp.2017.01.221
6. Guha C, Kavanagh BD. Hepatic radiation toxicity: avoidance and amelioration. Sem rad Oncol. 2011;21(4):256–263. doi:10.1016/j.semradonc.2011.05.003
7. Andolino DL, Johnson CS, Maluccio M, et al. Stereotactic Body Radiotherapy for Primary Hepatocellular Carcinoma. Int J Radiat Oncol Biol Phys. 2011;81(4):e447–e453. doi:10.1016/j.ijrobp.2011.04.011
8. Wahl DR, Stenmark MH, Tao Y, et al. Outcomes after stereotactic body radiotherapy or radiofrequency ablation for hepatocellular carcinoma. J Clin Oncol. 2016;34(5):452–459. doi:10.1200/JCO.2015.61.4925
9. Dewas S, Bibault JE, Mirabel X, et al. Prognostic factors affecting local control of hepatic tumors treated by stereotactic body radiation therapy. Radiat Oncol. 2012;7:166. doi:10.1186/1748-717X-7-166
10. Ohri N, Tomé WA, Romero AM, et al. Local control after stereotactic body radiation therapy for liver tumors. Int J Radiat Oncol Biol Phys. 2018;S0360–3016(17):34525–X. doi:10.1016/j.ijrobp.2017.12.288
11. Rim CH, Kim HJ, Seong J. Clinical feasibility and efficacy of stereotactic body radiotherapy for hepatocellular carcinoma: a systematic review and meta-analysis of observational studies. Radiother Oncol. 2019;131:135–144. doi:10.1016/j.radonc.2018.12.005
12. Portolani N, Coniglio A, Ghidoni S, et al. Early and late recurrence after liver resection for hepatocellular carcinoma. Ann Surg. 2006;243(2):229–235. doi:10.1097/01.sla.0000197706.21803.a1
13. N’Kontchou G, Mahamoudi A, Aout M, et al. Radiofrequency ablation of hepatocellular carcinoma: long-term results and prognostic factors in 235 Western patients with cirrhosis. Hepatology. 2009;50(5):1475–1483. doi:10.1002/hep.23181
14. Scorsetti M, Comito T, Cozzi L, et al. The challenge of inoperable hepatocellular carcinoma (HCC): results of a single-institutional experience on stereotactic body radiation therapy (SBRT). J Cancer Res Clin Oncol. 2015;141(7):1301–1309. doi:10.1007/s00432-015-1929-y
15. Fattovich G, Stroffolini T, Zagni I, Donato F. Hepatocellular carcinoma in cirrhosis: incidence and risk factors. Gastroenterology. 2004;127(5):S35–S50. doi:10.1053/j.gastro.2004.09.014
16. Dawson LA, Ten Haken RK. Partial volume tolerance of the liver to radiation. Sem Rad Oncol. 2005;15(4):279–283. doi:10.1016/j.semradonc.2005.04.005
17. Miften M, Vinogradskiy Y, Moiseenko V, et al. Radiation dose-volume effects for liver SBRT. Int J Radiat Oncol Biol Phys. 2018;S0360–3016(17):34527. doi:10.1016/j.ijrobp.2017.12.290
18. Owen D, Lukovic J, Hosni A, et al. Challenges in reirradiation of intrahepatic tumors. Sem Rad Oncol. 2020;30(3):242–252. doi:10.1016/j.semradonc.2020.02.004
19. Eriguchi T, Tsukamoto N, Kuroiwa N, et al. Repeated stereotactic body radiation therapy for hepatocellular carcinoma. Pract Radiat Oncol. 2021;11(1):44–52. doi:10.1016/j.prro.2020.08.002
20. Kimura T, Takeda A, Tsurugai Y, et al. A multi-institutional retrospective study of repeated stereotactic body radiation therapy for intrahepatic recurrent hepatocellular carcinoma. Int J Radiat Oncol Biol Phys. 2020;108(5):1265–1275. doi:10.1016/j.ijrobp.2020.07.034
21. Sun J, Ouyang C, Chang X, et al. Repeated CyberKnife stereotactic body radiation therapy in hepatocellular carcinoma. Radiat Oncol. 2020;15(1):10. doi:10.1186/s13014-020-1457-z
22. McDuff SGR, Remillard KA, Zheng H, et al. Liver reirradiation for patients with hepatocellular carcinoma and liver metastasis. Pract Radiat Oncol. 2018;8(6):414–421. doi:10.1016/j.prro.2018.04.012
23. Gkika E, Strouthos I, Kirste S, et al. Repeated SBRT for in- and out-of-field recurrences in the liver. Strahlenther Onkol. 2019;195(3):246–253. doi:10.1007/s00066-018-1385-0
24. Lo CH, Huang WY, Lin KT, Lin MJ, Lin TP, Jen YM. Repeated stereotactic ablative radiotherapy using CyberKnife for patients with hepatocellular carcinoma. J Gastroenterol Hepatol. 2014;29(11):1919–1925. doi:10.1111/jgh.12659
25. Oshiro Y, Mizumoto M, Okumura T, et al. Analysis of repeated proton beam therapy for patients with hepatocellular carcinoma. Radiother Oncol. 2017;123(2):240–245. doi:10.1016/j.radonc.2017.03.004
26. Hashimoto T, Tokuuye K, Fukumitsu N, et al. Repeated proton beam therapy for hepatocellular carcinoma. Internat J Radiat Oncol Biol Phys. 2006;65(1):196–202. doi:10.1016/j.ijrobp.2005.11.043
27. Hasan S, Abel S, Jan I, Uemura T, Thai N, Kirichenko AV. The albumin-bilirubin (ALBI) model in hepatocellular carcinoma (HCC) may better predict hepatic failure in patients with traditionally low-risk cirrhosis following definitive stereotactic body radiotherapy (SBRT). J Radiat Oncol. 2018;7(3):247–253. doi:10.1007/s13566-018-0354-7
28. Su TS, Yang HM, Zhou Y, et al. Albumin - bilirubin (ALBI) versus Child-Turcotte-Pugh (CTP) in prognosis of HCC after stereotactic body radiation therapy. Radiat Oncol. 2019;14(1):50. doi:10.1186/s13014-019-1251-y
29. Moon DH, Wang AZ, Tepper JE. A prospective study of the safety and efficacy of liver stereotactic body radiotherapy in patients with and without prior liver-directed therapy. Radiother Oncol. 2018;126(3):527–533. doi:10.1016/j.radonc.2018.01.004
30. Kutcher GJ, Burman C. Calculation of complication probability factors for non-uniform normal tissue irradiation: the effective volume method. Int J Radiat Oncol Biol Phys. 1989;16(6):1623–1630. doi:10.1016/0360-3016(89)90972-3
31. Kutcher GJ, Burman C, Brewster L, Goitein M, Mohan R. Histogram reduction method for calculating complication probabilities for three-dimensional treatment planning evaluations. Internat J Radia Oncol Biol Phys. 1991;21(1):137–146. doi:10.1016/0360-3016(91)90173-2
32. Dawson LA, Normolle D, Balter JM, McGinn CJ, Lawrence TS, Ten Haken RK. Analysis of radiation-induced liver disease using the Lyman NTCP model. Internat J Radia Oncol Biol Phys. 2002;53(4):810–821. doi:10.1016/S0360-3016(02)02846-8
33. Urata K, Kawasaki S, Matsunami H, et al. Calculation of child and adult standard liver volume for liver transplantation. Hepatology. 1995;21(5):1317–1321. doi:10.1016/0270-9139(95)90053-5
34. Pan CC, Kavanagh BD, Dawson LA, et al. Radiation-Associated Liver Injury. Internat J Radia Oncol Biol Phys. 2010;76(3):S94–S100. doi:10.1016/j.ijrobp.2009.06.092
35. Cheng JCH, Wu JK, Huang CM, et al. Radiation-induced liver disease after three-dimensional conformal radiotherapy for patients with hepatocellular carcinoma: dosimetric analysis and implication. Internat J Radia Oncol Biol Phys. 2002;54(1):156–162. doi:10.1016/S0360-3016(02)02915-2
36. Hall J, Moon AM, Young M, et al. Liver toxicity following reirradiation and multiple-target SBRT for primary hepatocellular carcinoma. JCO. 2024;42(3_suppl):514. doi:10.1200/JCO.2024.42.3_suppl.514
37. Apisarnthanarax S, Barry A, Cao M, et al. External beam radiation therapy for primary liver cancers: an ASTRO clinical practice guideline. Pract Radiat Oncol. 2022;12(1):28–51. doi:10.1016/j.prro.2021.09.004
38. Johnson PJ, Berhane S, Kagebayashi C, et al. Assessment of liver function in patients with hepatocellular carcinoma: a new evidence-based approach—the ALBI grade. JCO. 2015;33(6):550–558. doi:10.1200/JCO.2014.57.9151
39. Lasley FD, Mannina EM, Johnson CS, et al. Treatment variables related to liver toxicity in patients with hepatocellular carcinoma, Child-Pugh class A and B enrolled in a Phase 1–2 trial of stereotactic body radiation therapy. Pract Radiat Oncol. 2015;5(5):e443–e449. doi:10.1016/j.prro.2015.02.007
40. Culleton S, Jiang H, Haddad CR, et al. Outcomes following definitive stereotactic body radiotherapy for patients with Child-Pugh B or C hepatocellular carcinoma. Radiother Oncol. 2014;111(3):412–417. doi:10.1016/j.radonc.2014.05.002
41. Wolf DC. Evaluation of the Size, Shape, and Consistency of the Liver. Walker HK, Hall WD, Hurst JW, editors. Clinical Methods: The History, Physical, and Laboratory Examinations.
42. Pollom EL, Chin AL, Diehn M, Loo BW, Chang DT. Normal tissue constraints for abdominal and thoracic stereotactic body radiotherapy. Sem rad Oncol. 2017;27(3):197–208. doi:10.1016/j.semradonc.2017.02.001
43. Hanna GG, Murray L, Patel R, et al. UK Consensus on Normal Tissue Dose Constraints for Stereotactic Radiotherapy. Clin Oncol. 2018;30(1):5–14. doi:10.1016/j.clon.2017.09.007
44. Cárdenes HR, Price TR, Perkins SM, et al. Phase I feasibility trial of stereotactic body radiation therapy for primary hepatocellular carcinoma. Clin Transl Oncol. 2010;12(3):218–225. doi:10.1007/s12094-010-0492-x
45. Diez P, Hanna GG, Aitken KL, et al. UK 2022 consensus on normal tissue dose-volume constraints for oligometastatic, primary lung and hepatocellular carcinoma stereotactic ablative radiotherapy. Clin Oncol. 2022;34(5):288–300. doi:10.1016/j.clon.2022.02.010
46. Cheng JCH, Wu JK, Lee PCT, et al. Biologic susceptibility of hepatocellular carcinoma patients treated with radiotherapy to radiation-induced liver disease. Int J Radiat Oncol Biol Phys. 2004;60(5):1502–1509. doi:10.1016/j.ijrobp.2004.05.048
47. Xu ZY, Liang SX, Zhu J, et al. Prediction of radiation-induced liver disease by Lyman normal-tissue complication probability model in three-dimensional conformal radiation therapy for primary liver carcinoma. Int J Radiat Oncol Biol Phys. 2006;65(1):189–195. doi:10.1016/j.ijrobp.2005.11.034
48. D’Amico G, Morabito A, D’Amico M, et al. Clinical states of cirrhosis and competing risks. J Hepatol. 2018;68(3):563–576. doi:10.1016/j.jhep.2017.10.020
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.