Back to Journals » Clinical Ophthalmology » Volume 20
Binocular Occlu-tab Training in Patients with Ametropic Amblyopia: A Retrospective Study
Authors Zaynutdinov NN, Tatara S ![]() , Ishigaki Y
, Ishigaki Y ![]() , Handa T
, Handa T ![]()
Received 11 March 2026
Accepted for publication 12 May 2026
Published 19 May 2026 Volume 2026:20 606380
DOI https://doi.org/10.2147/OPTH.S606380
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sotiria Palioura
Nazim Nadirkhodjayevich Zaynutdinov,1,* Shunya Tatara,2,* Yo Ishigaki,3 Tomoya Handa4
1Department of Ophthalmology, NAZAR Eye Center, Tashkent, Uzbekistan; 2Department of Orthoptics and Visual Sciences, Faculty of Medical Technology, Niigata University of Health and Welfare, Niigata, Japan; 3Research Center for Realizing Sustainable Societies, The University of Electro-Communications, Chofu, Tokyo, Japan; 4Department of Rehabilitation, Orthoptics and Visual Science Course, School of Allied Health Sciences, Kitasato University, Sagamihara, Kanagawa, Japan
*These authors contributed equally to this work
Correspondence: Nazim Nadirkhodjayevich Zaynutdinov, Department of Ophthalmology, NAZAR Eye Center, Yangi Yunusabad Street, 40A. Yunusabad District, Tashkent, 100206, Uzbekistan, Tel + 9989012999045, Fax + 998555039199, Email [email protected]
Purpose: Although previous studies have reported favorable outcomes of Occlu-tab therapy for anisometropic and strabismic amblyopia, its effectiveness for bilateral ametropic amblyopia has not been well documented. This study evaluated the therapeutic effectiveness of Occlu-tab training applied to both eyes in children with bilateral ametropic amblyopia.
Patients and Methods: This retrospective study included 25 children with bilateral ametropic amblyopia (best-corrected visual acuity ≤ 0.8 in both eyes) treated at the NAZAR Eye Center (Tashkent, Uzbekistan) between September 2024 and February 2025. The eye with better visual acuity, as assessed at the initial visit, was defined as the better eye and the fellow eye as the worse eye. All patients received refractive correction and initiated Occlu-tab training at the first visit. Occlu-tab training was performed for 10 minutes per eye per day (20 minutes total for both eyes), 10 times per month, for 6 months. Visual acuity was assessed at baseline (0 months; 0 M) and at 1 M, 3 M, and 6 M. Changes in visual acuity over time were analyzed using repeated-measures analysis of variance.
Results: The mean patient age was 7.96 ± 1.30 years. In the worse eye, mean visual acuity (LogMAR) was 0.32 ± 0.17 at 0 M, 0.28 ± 0.15 at 1 M, 0.22 ± 0.12 at 3 M, and 0.19 ± 0.11 at 6 M (p < 0.001). In the better eye, mean visual acuity was 0.26 ± 0.15 at 0 M, 0.24 ± 0.14 at 1 M, 0.19 ± 0.13 at 3 M, and 0.15 ± 0.11 at 6 M (p < 0.001).
Conclusion: Over the 6-month treatment period, Occlu-tab training applied to both eyes was associated with significant visual acuity improvement in children with bilateral ametropic amblyopia. These findings suggest that Occlu-tab therapy may improve in visual acuity in patients with bilateral ametropic amblyopia.
Keywords: occlu-tab, occlu-pad, ametropic amblyopia, refractive error, occlusion
Introduction
Amblyopia is a condition in which visual acuity does not fully develop, even with appropriate refractive correction, in the absence of detectable ocular pathology. Major causes of amblyopia include strabismus, form vision deprivation, and refractive errors.1 If amblyopia is insufficiently treated during the critical period of visual development, visual acuity may remain incompletely developed. For this reason, early detection and timely intervention are essential for achieving optimal visual outcomes.1,2 Full correction of refractive error with spectacles is considered the standard first-line treatment for amblyopia.3 In cases where a greater therapeutic effect is required, occlusion of the fellow eye using an eye patch is commonly employed as an additional intervention.4 However, adherence to occlusion therapy is often poor because patching can impose physical discomfort, visual inconvenience, cosmetic concerns, and a substantial treatment burden over time.5
In recent years, a novel amblyopia treatment approach using an open-type binocular system has been developed based on a modified tablet device. This system, known as the Occlu-tab in Japan and internationally, enables controlled visual input to the amblyopic eye without complete occlusion of the fellow eye using polarization glasses.6 This approach allows targeted training of the amblyopic eye without complete occlusion of the fellow eye, reducing the risk of decreased visual acuity in the fellow eye and preserving binocular visual function. Binocular open-type game–based training using the Occlu-tab has been shown to produce greater improvements in visual acuity than conventional eye patch therapy when administered for equivalent treatment durations.7 Additionally, a binocular iPad game using red–green anaglyphic glasses has been shown to improve visual acuity in children with amblyopia and to be more effective than patching at the 2-week visit.8
As the tablet-based visual training is a relatively new therapeutic technology, there is limited evidence of its clinical effectiveness. Published studies to date have primarily reported its effects in anisometropic amblyopia6–12 and strabismic amblyopia,13 leaving the therapeutic efficacy of Occlu-tab for bilateral visual impairment unexplored. To address this research gap, this study evaluated the outcomes of Occlu-tab therapy applied to both eyes in patients with ametropic amblyopia presenting with bilateral visual impairment.
Materials and Methods
Participants and Inclusion Criteria
For this retrospective study, we analyzed the medical records of children treated at the NAZAR Eye Center (Tashkent, Uzbekistan) between September 2024 and February 2025. The inclusion criteria were a diagnosis of ametropic amblyopia, corrected visual acuity of ≤0.8 in both eyes, and having received amblyopia treatment using the Occlu-tab. Patients with eye diseases other than ocular deviation or refractive errors, as well as those who underwent conventional occlusion therapy using an eye patch or pharmacologic penalization in combination with Occlu-tab therapy, were excluded.
This study was approved by the Institutional Review Board of The University of Electro-Communications (No. H25083). The Institutional Review Board waived the need for patient consent. Appropriate measures were taken to protect the confidentiality of the study participants. This study was conducted in accordance with the Declaration of Helsinki.
Visual Assessment and Study Protocol
At the initial visit, all patients underwent measurements of uncorrected visual acuity, corrected visual acuity, axial length, and cycloplegic refraction with cyclopentolate. Visual acuity was measured using the Vision Chart C901 (Shanghai MediWorks Co. Ltd., China), which was converted to the logarithm of the minimum angle of resolution (LogMAR) units for statistical analysis. Based on baseline visual acuity, the eye with better visual acuity was defined as the better eye, while the eye with poorer visual acuity was defined as the worse eye. In cases where visual acuity was similar between both eyes, the right eye was defined as the better eye and the left eye as the worse eye. Refraction was measured using Auto-Kerato-Refractometer KR-800 (Topcon Inc., Japan) and axial length was measured using Pentacam AXL (Oculus Optikgeräte Gmbh, Germany). At this visit, spectacles were prescribed and Occlu-tab therapy was initiated. After receiving initial instruction at the clinic, the Occlu-tab device was lent to patients for home-based training. Corrected visual acuity was evaluated at 1, 3, and 6 months after the initiation of Occlu-tab therapy.
Occlu-tab Treatment
Occlu-tab is a tablet-based amblyopia training device used in combination with polarized glasses (Figure 1). A key feature of Occlu-tab is that it enables amblyopia training under binocular open-view conditions without occluding either eye. Images displayed on the Occlu-tab screen are not visible to the naked eye; however, when viewed through polarized glasses, the preselected training eye can perceive the images. The fellow eye cannot perceive the images even through the polarized glasses. As a result, only the designated training eye is stimulated during Occlu-tab use even though both eyes remain open.
 |
Figure 1 Image of the Occlu-tab device. The Occlu-tab enables visual stimulation of one eye when viewed through polarized glasses. The designated training eye can perceive the displayed images through the polarized glasses, whereas the fellow eye cannot. The images displayed on the liquid crystal screen are not visible to the naked eye. |
In the present study, patients performed Occlu-tab training for 10 minutes per eye per day (20 minutes total for both eyes), 10 times per month. This training protocol was continued for 6 months.
Statistical Analysis
Visual acuity, refractive error, keratometric values, and axial length were compared between the better and worse eyes using paired t-tests. Changes in visual acuity over time in the better and worse eyes were analyzed using one-way repeated-measures analysis of variance. In cases where the assumption of sphericity was violated, Greenhouse–Geisser correction was applied. In cases where a significant main effect was detected, post hoc pairwise comparisons were performed using Bonferroni correction. Effect sizes were calculated as generalized eta squared (η2). Results with a p value < 0.05 were considered statistically significant. Statistical analyses were performed using MedCalc (version 23.4.9; MedCalc Software Ltd) and R (version 4.3.1; R Foundation for Statistical Computing).
Results
A total of 25 children with amblyopia were enrolled in this study (mean age: 7.96 ± 1.30 years).
Table 1 presents the visual acuity (LogMAR), spherical power (D), cylindrical power (D), K1 (D), K2 (D), and axial length (mm) for the better and worse eyes at the initial visit. Because the eye with better visual acuity was defined as the better eye, visual acuity differed significantly between eyes (p < 0.001). No significant differences were observed between the two eyes for any other parameters.
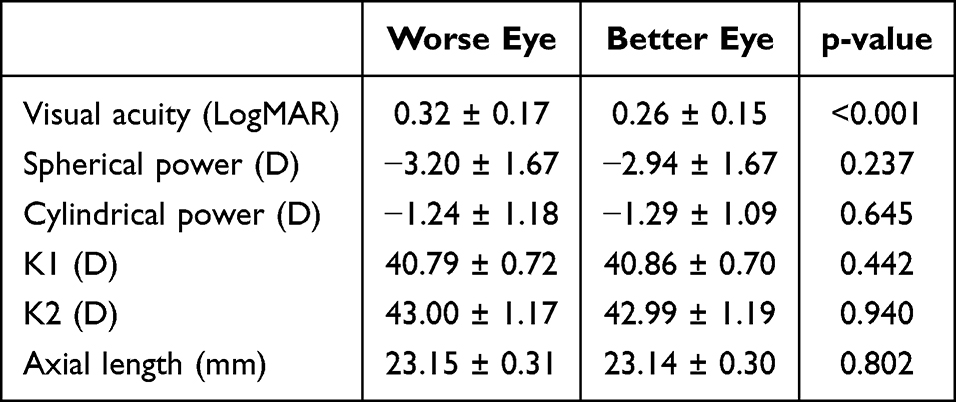 |
Table 1 Participant Characteristics |
Visual acuity was measured at baseline (0 M) and 1, 3, and 6 months after initiation of Occlu-tab treatment. Mean visual acuity (LogMAR) in the worse eye was 0.32 ± 0.17 at 0 M, 0.28 ± 0.15 at 1 M, 0.22 ± 0.12 at 3 M, and 0.19 ± 0.11 at 6 M, showing significant improvement over time (repeated-measures ANOVA, Greenhouse–Geisser corrected, F(1.65, 39.65) = 49.04, p < 0.001, generalized η2 = 0.13). All pairwise comparisons between time points were statistically significant (Bonferroni-adjusted p-values ranging from 0.0027 to <0.001). Mean visual acuity (LogMAR) in the better eye was 0.26 ± 0.15 at 0 M, 0.24 ± 0.14 at 1 M, 0.19 ± 0.13 at 3 M, and 0.15 ± 0.11 at 6 M, also showing significant improvement over time (repeated-measures ANOVA, Greenhouse–Geisser corrected, F(1.44, 34.51) = 56.13, p < 0.001, generalized η2 = 0.09). Again, all pairwise comparisons in visual acuity between time points were statistically significant (Bonferroni adjusted p-values ranging from 0.015 to <0.001). Figure 2 shows the time course of visual acuity changes, and Figure 3 shows the changes in visual acuity from baseline to 6 months for each individual patient. The mean change in visual acuity over the 6-month period was 0.14 ± 0.09 LogMAR in the worse eye and 0.11 ± 0.07 LogMAR in the better eye. In addition, 32% of patients achieved an improvement of ≥2 lines.
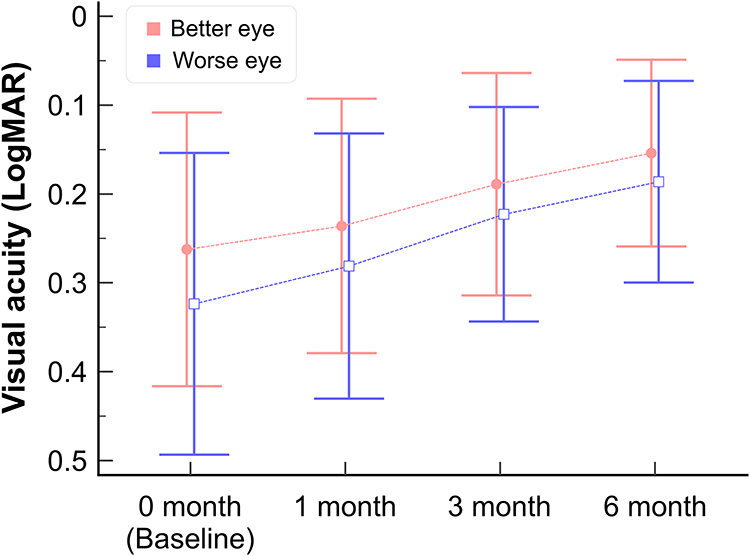 |
Figure 2 Time course of changes in visual acuity following Occlu-tab therapy. Visual acuity (LogMAR) was measured at baseline (0 M) and at 1, 3, and 6 M after initiation of Occlu-tab treatment. The blue line represents the worse eye, while the red line represents the better eye. Error bars indicate standard deviation. Significant visual improvements were observed for both the worse and better eyes over the 6-month treatment period. |
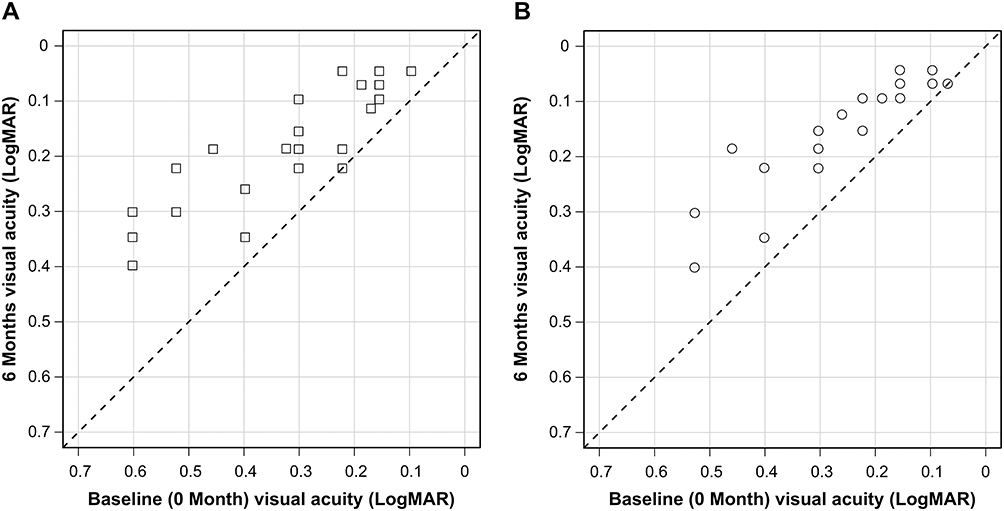 |
Figure 3 Individual changes in visual acuity from baseline to 6 months. Baseline (0 M) visual acuity (LogMAR) is shown on the x-axis, and visual acuity at 6 months is shown on the y-axis. Each point represents an individual patient, illustrating the magnitude of visual improvement over the 6-month period. (A) Scatterplot of visual acuity in the worse eye. (B) Scatterplot of visual acuity in the better eye. |
Discussion
This study evaluated the therapeutic effects of Occlu-tab training for children with bilateral ametropic amblyopia presenting with reduced visual acuity in both eyes. Amblyopia is generally considered less responsive to treatment beyond age 7 because of reduced neural plasticity and interindividual variability in treatment response.14 When treated within the sensitive period, visual outcomes of ametropic amblyopia are generally favorable. Although optical correction is regarded as the standard treatment for this condition, combining occlusion therapy with spectacle correction may accelerate visual improvement.15
Amblyopia was detected relatively late in our patient sample, with a mean age of 7.96 ± 1.30 years at diagnosis. As visual plasticity may already be declining at this age, it was necessary to select a therapeutic approach that could promote more rapid visual improvement. Previous reports suggest that Occlu-tab can achieve visual outcomes comparable to or better than conventional full-time occlusion therapy.7 As a result, refractive correction was combined with Occlu-tab training for our cohort.
Occlu-tab therapy is primarily used for cases of unilateral amblyopia, such as anisometropic amblyopia, due to its unique structure that allows visual stimulation of only the designated eye under binocular open conditions. Favorable therapeutic outcomes have been reported for such unilateral cases.6,7,9–13 In contrast, the present study focused on bilateral ametropic amblyopia. Because both eyes exhibited reduced visual acuity, Occlu-tab training was performed for each eye. Notably, significant visual improvement was observed in both the better and worse eyes over the 6-month treatment period. A meta-analysis examining the effect of age on treatment response in cases of strabismic or anisometropic amblyopia reported that response decreases with increasing age, particularly in children with more severe amblyopia. Given that ametropic amblyopia is often associated with relatively mild visual impairment, the patients in our study may have retained sufficient visual plasticity to achieve significant improvement despite their relatively older age at diagnosis.16 In the Pediatric Eye Disease Investigator Group randomized trial evaluating the treatment of amblyopia in children aged 7–12 years, approximately 25% of patients showed an improvement of ≥ 2 lines with optical correction alone.17 Although our study did not include an optical-correction–only control group, the magnitude of visual improvement observed in the present study, in which 32% of patients achieved improvement of ≥ 2 lines, appears greater than would be expected from optical correction alone, suggesting a potential additive effect of Occlu-tab training. These findings suggest that the observed improvements may be clinically meaningful.
Evidence supporting binocular open-type tablet-based amblyopia treatment has largely been derived from studies conducted in specific geographic regions. Data from the Intelligent Research in Sight Registry suggest that the effectiveness of amblyopia treatment in real-world practice varies substantially across populations and regions.18 Although standard amblyopia treatments are generally effective, residual visual acuity deficits remain common and treatment outcomes appear to be influenced by racial and socioeconomic factors. To support worldwide dissemination of this approach, Handa et al7 noted the need to analyze the effects of different types of games and consider potential cultural and religion-related factors. The current study provides evidence of favorable outcomes of Occlu-tab therapy conducted in Uzbekistan, a region with no previously published reports of its clinical use. To establish Occlu-tab as a standard therapeutic option, further evidence from diverse geographic regions—including developing countries—is warranted.
It should be acknowledged that this study was not a randomized controlled trial. Because we did not include a control group receiving refractive correction alone, we cannot exclude the possibility that visual improvement may have occurred with spectacle correction alone. Although this is a significant limitation of this study, there are currently no reports suggesting that the addition of Occlu-tab worsens outcomes. Given the availability of Occlu-tab as a therapeutic option in our clinical setting, it was considered ethically inappropriate to withhold its use. For this reason, causal inference is limited and the observed improvements should be interpreted with caution. Furthermore, adherence to Occlu-tab training was managed by parents. Although parents reported good compliance, adherence was not objectively verified and may have influenced the study outcomes. This represents a potential source of bias in the study outcomes. Future prospective, controlled studies will be required to further validate the clinical effectiveness of Occlu-tab therapy.
Conclusion
In this study, Occlu-tab training was performed for both eyes in 25 children with bilateral ametropic amblyopia. Visual acuity improved significantly in both eyes over the 6-month treatment period, suggesting that Occlu-tab training may be associated with visual improvement.
Data Sharing Statement
The datasets used and analyzed in the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Institutional Review Board of The University of Electro-Communications (No. H25083). This study was conducted in accordance with the Declaration of Helsinki. As this was a retrospective, non-interventional study using de-identified data extracted from existing medical records, the Institutional Review Board waived the requirement for written informed consent. Appropriate measures were taken to protect the confidentiality of the study participants.
Funding
This research was funded by JSPS KAKENHI, grant number JP24KK0191.
Disclosure
TH received equipment support from Hopnic Inc. and NAC Image Technology Inc. and served in a technical advisory role for NIDEK Co., Ltd. and JFC Co., Ltd. The authors report no other conflicts of interest in this work.
References
1. DeSantis D. Amblyopia. Pediatr Clin North Am. 2014;61(3):505–7. doi:10.1016/j.pcl.2014.03.006
2. Epelbaum M, Milleret C, Buisseret P, Dufier JL. The sensitive period for strabismic amblyopia in humans. Ophthalmology. 1993;100(3):323–327. doi:10.1016/S0161-6420(13)32170-8
3. Cotter SA, Edwards AR, et al. Treatment of anisometropic amblyopia in children with refractive correction. Ophthalmology. 2006;113(6):895–903. doi:10.1016/j.ophtha.2006.01.068
4. Pediatric Eye Disease Investigator Group. A randomized trial of atropine vs. patching for treatment of moderate amblyopia in children. Arch Ophthalmol. 2002;120(3):268–278. doi:10.1001/archopht.120.3.268
5. Wallace MP, Stewart CE, Moseley MJ, et al. Compliance with occlusion therapy for childhood amblyopia. Invest Ophthalmol Vis Sci. 2013;54(9):6158–6166. doi:10.1167/iovs.13-11861
6. Handa T, Ishikawa H, Shoji N, et al. Modified iPad for treatment of amblyopia: a preliminary study. J AAPOS. 2015;19(6):552–554. doi:10.1016/j.jaapos.2015.08.008
7. Handa T, Thakkar H, Ramakrishnan M, et al. Comparison of the effectiveness of amblyopia treatment with eye-patch and binocular Occlu-tab for the same treatment duration. Indian J Ophthalmol. 2022;70(5):1722–1726. doi:10.4103/ijo.IJO_1733_21
8. Kelly KR, Jost RM, Dao L, Beauchamp CL, Leffler JN, Birch EE. Binocular iPad game vs patching for treatment of amblyopia in children: a randomized clinical trial. JAMA Ophthalmol. 2016;134(12):1402–1408. doi:10.1001/jamaophthalmol.2016.4224
9. Jethani J, Kamat A, Shah K, Thakkar H, Sharma S. Efficacy of supplemental Occlu-pad therapy with partial occlusion in children with refractive anisometropic amblyopia. Indian J Ophthalmol. 2022;70(4):1318–1320. doi:10.4103/ijo.IJO_1322_21
10. Iwata Y, Handa T, Ishikawa H, Goseki T, Shoji N. Evaluation of the effects of the occlu-pad for the management of anisometropic amblyopia in children. Curr Eye Res. 2018;43(6):785–787. doi:10.1080/02713683.2018.1439066
11. Totsuka S, Handa T, Ishikawa H, Shoji N. Improvement of adherence with occlu-pad therapy for pediatric patients with amblyopia. Biomed Res Int. 2018;2018(1):2394562. doi:10.1155/2018/2394562
12. Iwata Y, Handa T, Ishikawa H, Goseki T, Shoji N. Comparison between amblyopia treatment with glasses only and combination of glasses and open-type binocular “occlu-pad” device. Biomed Res Int. 2018;2018(1):2459696. doi:10.1155/2018/2459696
13. Iwata Y, Kusayanagi Y. Three cases of amblyopia with fusion maldevelopment nystagmus successfully treated with dichoptic treatment. Cureus. 2024;16(12):e75496. doi:10.7759/cureus.75496
14. Holmes JM, Levi DM. Treatment of amblyopia as a function of age. Vis Neurosci. 2018;35:E015. doi:10.1017/S0952523817000220
15. Kaur S, Sharda S, Aggarwal H, Dadeya S. Comprehensive review of amblyopia: types and management. Indian J Ophthalmol. 2023;71(7):2677–2686. doi:10.4103/IJO.IJO_338_23
16. Holmes JM, Lazar EL, Melia BM, et al. Effect of age on response to amblyopia treatment in children. Arch Ophthalmol. 2011;129(11):1451–1457. doi:10.1001/archophthalmol.2011.179
17. Scheiman MM, Hertle RW, Beck RW, et al. Randomized trial of treatment of amblyopia in children aged 7 to 17 years. Arch Ophthalmol. 2005;123(4):437–447. doi:10.1001/archopht.123.4.437
18. Repka MX. Amblyopia outcomes through clinical trials and practice measurement: room for improvement: the LXXVII Edward Jackson memorial lecture. Am J Ophthalmol. 2020;219:A1–A26. doi:10.1016/j.ajo.2020.07.053
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.