Back to Journals » Infection and Drug Resistance » Volume 16
Bikunin: A Promising Prognostic Biomarker for Acute-on-Chronic Liver Failure in Patients with Viral Hepatitis B
Authors Qin G, Wang B ![]() , Zhang G, Wu L, Zhu P, Zhang Q
, Zhang G, Wu L, Zhu P, Zhang Q
Received 10 May 2023
Accepted for publication 1 August 2023
Published 31 August 2023 Volume 2023:16 Pages 5765—5775
DOI https://doi.org/10.2147/IDR.S417472
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Gang Qin,1 Bo Wang,2 Geng Zhang,2 Lili Wu,1 Peng Zhu,1 Qian Zhang2
1Department of Gastroenterology, Suining First People’s Hospital, Suining, People’s Republic of China; 2Department of Infectious Diseases, The Affiliated Hospital of Southwest Medical University, Luzhou, People’s Republic of China
Correspondence: Qian Zhang, Department of Infectious Diseases, The Affiliated Hospital of Southwest Medical University, Luzhou, Sichuan, People’s Republic of China, Email [email protected]
Purpose: To screen out potential prognostic biomarkers for HBV-related acute-on-chronic liver failure (HBV-ACLF).
Patients and Methods: Peripheral blood samples of HBV-ACLF patients (n=56) and normal controls (n=15) from the Affiliated Hospital of Southwest Medical University from January 2021 to April 2022 were collected, 5 normal patients and 10 patients with ACLF were randomly selected for Data independent acquisition (DIA) mass spectrometry analysis, and the potential core proteins were screened out via bioinformatics. All samples were validated by Enzyme linked immunosorbent assays (ELISA) technology, and the survival curve was constructed based on the patient’s 90-day survival time.
Results: A total of 247 differentially expressed proteins (DEPs) were screened, of which 148 were upregulated and 99 were down-regulated. The DEPs were mainly enriched in high-density lipoprotein particle remodeling, coagulation, and hemostasis and participated in signaling pathways such as cholesterol metabolism, coagulation cascades, and PPAR signaling pathway. Finally, bikunin was selected for further study and validated via the ELISA, compared with the normal group, bikunin was poorly expressed in the HBV-ACLF group, the difference was statistically significant (P < 0.0001), the area under the curve (AUC) for Receiver operating characteristic (ROC) analysis was 0.917. Furthermore, compared with the non-survival group, bikunin was highly expressed in the HBV-ACLF survival group, the difference was statistically significant (P=0.0015), and the survival curve showed a positive correlation with patient survival (P=0.0063).
Conclusion: The level of plasma bikunin in HBV-ACLF is down-regulated, which is positively correlated with the survival of the patients with HBV-ACLF, and is expected to become a new prognostic biomarker.
Keywords: HBV-ACLF, AMBP, bikunin, DIA
Introduction
Acute-on-chronic liver failure (ACLF) refers to a complex syndrome mainly manifested by acute jaundice and coagulation dysfunction caused by various triggers on the basis of chronic liver disease, which can be combined with complications such as hepatic encephalopathy, ascites, electrolyte imbalance, infection, hepatorenal syndrome, hepatopulmonary syndrome, and extrahepatic organ failure.1–3 Hepatitis B virus (HBV) infection is a major etiology of ACLF.4 Due to the complex and diverse etiology, course and complications of ACLF, the mixing of acute exacerbation and chronic liver damage, the liver itself failure and extrahepatic organ function affect each other, resulting in rapid progression and poor prognosis, even with strong comprehensive medical treatment, the 90-day mortality rate of ACLF patients is about 58%.5 Early warning and prognosis judgment are essential. Although there are many liver failure prognostic prediction models at home and abroad, such as Chinese Group on the Study of Severe Hepatitis B (COSSH) ACLF score,6 Chronic Liver Failure Consortium (CLIF-C) ACLF score,7 Asian Pacific Association for the Study of the Liver (APASL) ACLF research consortium (AARC) ACLF score,8 et al, they are mainly based on clinical manifestations and do not solve this problem well. With the development of high-throughput omics technology, through genomics, proteomics, metabolomics and other methods to process and analyze data, more specific prognostic markers can be found more efficiently, which is conducive to targeted individual prediction assessment and corresponding treatment. Proteomics primarily studies the composition of proteins and their dynamics and is in favor of the identification of candidate blood biomarkers by comparing the protein expression profiles between healthy individuals and patients.9 It is necessary to apply proteomics to find prognostic biomarkers for acute-on-chronic liver failure.
Here, we discuss the prognostic biomarker for HBV-ACLF. First, we used Data Independent Acquisition (DIA) mass spectrometry analysis to evaluate HBV-ACLF associated proteomic changes. Second, we validated the candidate biomarkers bikunin by ELISA.
Bikunin is a small circulating proteoglycan (PG) which is synthesized mainly by hepatocytes.
Bikunin is widely detectable in liver parenchyma, and tissues which is associated with pathophysiological conditions including cancer. It exerts to inhibit ovarian cancer cell invasion and metastasis.10 Moreover, bikunin is inversely associated with urokinase-type plasminogen activator (uPA) expression and is an independent survival predictor of ovarian cancer.11 In our study, bikunin was downregulated and positively correlated with survival in HBV-ACLF.
Material and Methods
Collection of Samples from Patients with HBV-ACLF
HBV-ACLF patients (n=56) from the Department of Infectious Diseases, the Southwest Medical University Hospital from January 2021 to April 2022 were collected. The diagnostic criteria for ACLF refer to the Chinese diagnostic criteria for liver failure.6 In brief, patients with chronic liver disease with hepatitis B virus infection, serum TBil ≥ 12 mg/dl and INR ≥ 1.5. All patients with HBV-ACLF were followed for 90 days or until death. The inclusion criteria for healthy volunteers (n = 15) were as follows: 1) age ≥18 years and ≤65 years, 2) no other acute and chronic diseases. The exclusion criteria were as follows: 1) patients who did not wish to enter the experiment, 2) patients with other viral infections, such as HIV, hepatitis A, hepatitis C, hepatitis E virus or liver cancer. Blood samples were collected within 24 hours of admission, and plasma was collected after peripheral blood centrifugation and stored in a −80°C freezer. This study was reviewed by the Ethics Committee of the Affiliated Hospital of Southwest Medical University (No. KY2021014). All patients or healthy volunteers included have the signature and consent of the patient himself or his family. The clinical study registration number is ChiCTR2100042896, which was registered at the Chinese Clinical Trial Registry (www.chictr.org.cn).
DIA Mass Spectrometry Analysis
Plasma from 10 HBV-ACLF patients and 5 healthy volunteers was randomly selected for Data independent acquisition (DIA, also called SWATH) mass spectrometry analysis. This project uses next-generation label-free quantitative proteomics techniques to complete the analysis. In DIA mode, it provides high proteome coverage while enabling precise, highly reproducible quantification of large amounts of protein per sample. The DIA analysis pipeline is based on three essential steps: 1) Spectral library construction: A spectral library collects all detectable non-redundant, high-quality peptide information (MS/MS spectra) of the sample that can be used as a peptide identification template for subsequent data analysis. It contains fragment ion intensity and retention time that characterize the peptide spectrum. The spectral library is constructed from samples of interest by using data-dependent acquisition (DDA) technique. 2) Large sample data acquisition in DIA mode utilizes the latest high-resolution mass spectrometer to simultaneously acquire peptide ion characteristics in mass and retention time space. Compared to traditional technique of extracting single ion for fragmentation analysis, in DIA mode, the mass spectrometer is set to a wide precursor ion window to collect product ions in turn. Thus, complete collection of all detectable protein peak information in the sample and high-reproducible analysis of large number of samples is achieved. 3) Data analysis: Identification and quantification of peptides and proteins were obtained from DDA spectral library by deconvolution of the DIA data. MSstats software package was used to perform differential analysis, followed by functional analysis of the differential proteins.
Differential Protein Screening
MSstats is an R package derived from the Bioconductor repository. It can be used to statistically evaluate the significant difference of proteins or peptides in different samples and is widely used in targeted proteomics MRM, non-standard quantification, and SWATH quantitative experiments, and its core algorithm is linear mixed-effects models. In this study, the data were logarithmically preprocessed according to a set comparison group, and then a significance test was performed based on the model. After that, differential protein screening was carried out according to the thresholds of a log2 (fold change) (log2FC) value ≥2 and P value <0.05 as the criteria for significant difference. Result visualization is done on an R-based online platform (https://www.xiantaozi.com/).
GO Enrichment Analysis
Gene Ontology (GO) systematically defines and explains the protein structure of genes by classifying and sorting out gene-related data around the world. The GO method is an effective method to completely dissect the structure of differential gene clusters, which is convenient for researchers to understand the classification of differential genes as a whole, and select the corresponding subdirection for in-depth analysis in the later stage. GO term is a basic unit, which divides the various functions of the genome into 3 aspects, namely Biological Process (BP), Cellular Component (CC) and Molecular Function (MF), thereby effectively reducing the complexity of analysis. In order to explore the functional enrichment of differential genes in more depth, GO analysis of differential proteins was performed, and P < 0.05 was statistically significant. Result visualization is done on an R-based online platform (https://www.xiantaozi.com/).
PPI Analysis
Protein–Protein Interaction Network (PPI) refers to the interaction between proteins or within them, which together affect all aspects of the organism, including information transmission, expression regulation, energy and nutrient metabolism, and body cycle regulation. In-depth study of the role of proteins in the ecosystem can provide insight into the mechanism by which proteins interact with each other, leading to a better understanding of pathological mechanisms. To further screen potential core proteins, we used STRING (https://cn.string-db.org/) to build a PPI network to facilitate the screening of genes located at the center of the network. Theoretically, the closer to the middle, the greater its functional role may be, and the more important it is to connect with the outside world.
ELISA Verification
To further validate the clinical relevance of potential biomarkers, the human bikunin ELISA kit (BOSTER, EK1598) was used to detect plasma samples from 56 HBV-ACLF patients and 15 healthy volunteers. The specific operation process is carried out in accordance with the company’s instructions. ROC analysis was used to evaluate the potential application value of this protein in the diagnosis of HBV-ACLF. AUC > 0.8 is defined as a good diagnostic value.
Survival Analysis
To further explore the relationship between the target protein and clinical prognosis, survival curves were used for prognostic assessment. All HBV-ACLF patients were followed for 90 days to count their survival or death status, if death, record the time of death (days). All patients were sorted by the concentration of the target protein from smallest to largest, with the first half being the low-expression group and the second half being the high-expression group. Log-rank was used for statistical analysis of survival curves, and P < 0.05 was defined as statistically significant.
Statistical Analysis
The data obtained from the ELISA and patients’ clinical information were analyzed with GraphPadPrism7 software. Continuous variables are presented as the mean ± standard deviation (SD), differences in continuous variables were analyzed with unpaired Student’s t-test. The chi-square test was used to carry out comparisons between categorical variables. The cutoff criterion was a P value <0.05.
Results
Description of Clinical Information
A total of 56 patients with HBV-ACLF and 15 healthy volunteers were included in this study. There were 44 male patients and 12 female patients in the HBV-ACLF group, 10 males and 5 females in healthy volunteers. The mean age of the HBV-ACLF group was 51.09±12.36 years, while the mean age of the normal group was 36.87±4.824 years (P < 0.0001). There was no statistically significant difference in creatinine (Crea) concentration between two groups. Compared with the normal group, the white blood cell (WBC) of the HBV-ACLF group was slightly higher and statistically significant (P=0.0438), the hemoglobin (HGB), platelet (PLT) and albumin (ALB) of the HBV-ACLF group decreased significantly, the liver function indexes such as alanine transaminase (ALT), aspartate transaminase (AST), and total bilirubin (TB) increased significantly in HBV-ACLF group, and the differences were statistically significant (Table 1). Based on the prognosis of 90 days of follow-up, HBV-ACLFs were divided into survival (n=30) and non-survival (n=26). Compared with the survival group, PLT (P=0.0062) and ALB (P=0.015) were reduced, while TB (P=0.0049), international normalized ratio (INR) (P=0.0006), Model for end-stage liver disease (MELD) (P=0.0005) and MELD-Na (P=0.0015) were increased in the non-survival group. However, there were no statistically significant differences in WBC, HGB, AST, ALT, Crea, alpha fetoprotein (AFP), and procalcitonin (PCT) between the two groups (Table 2).
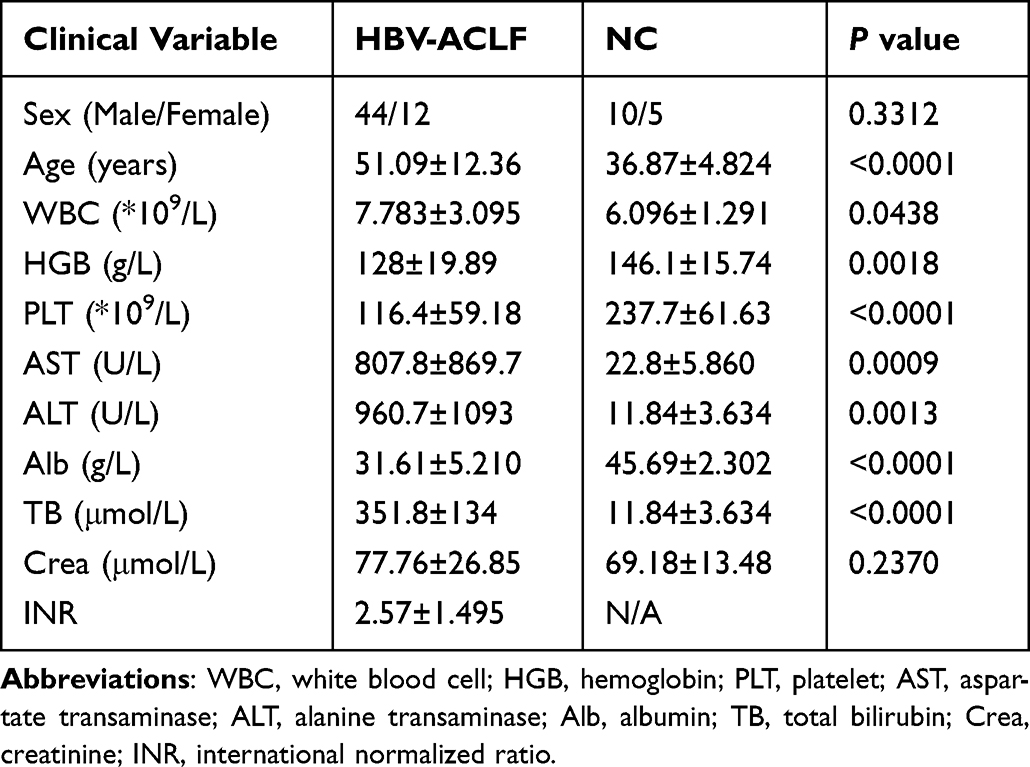 |
Table 1 Clinical Information of HBV-ACLF Group and Normal Group (NC) |
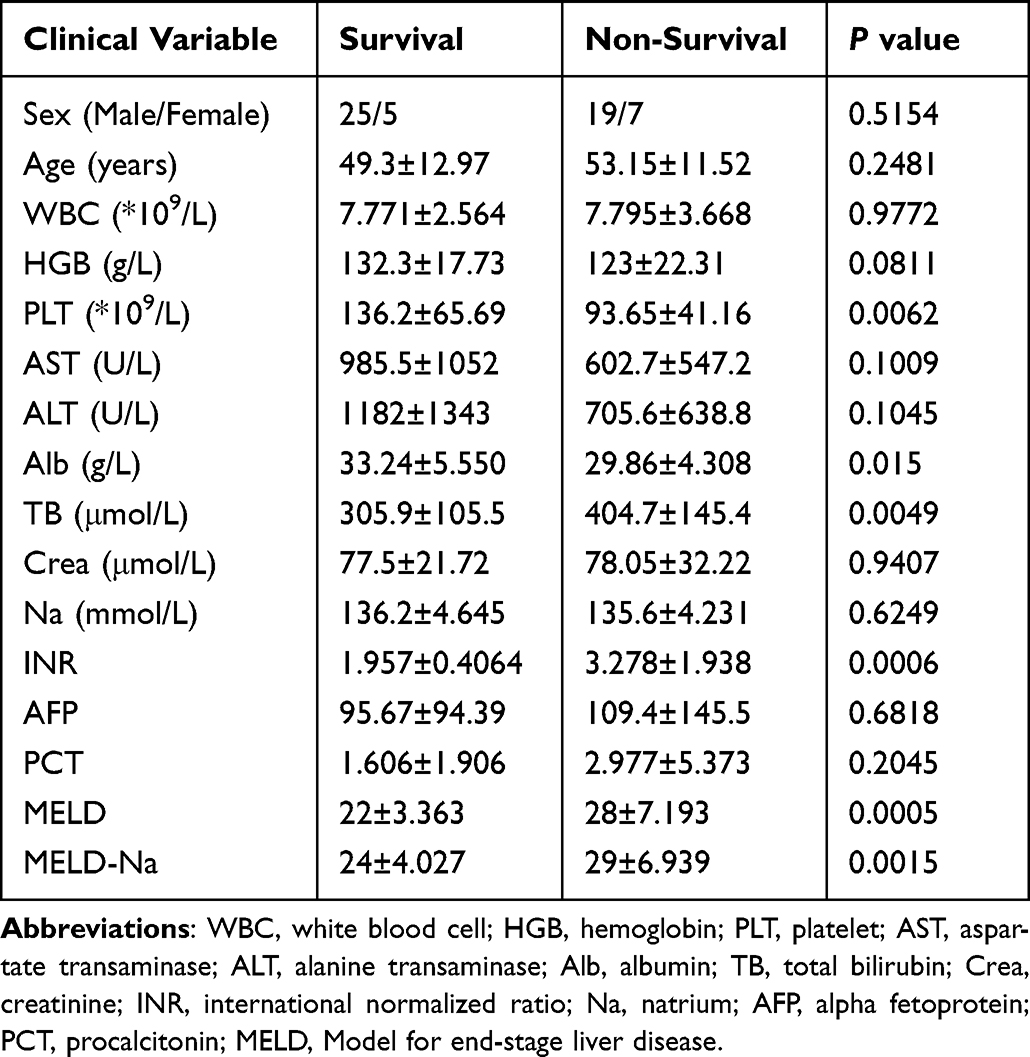 |
Table 2 Clinical Characteristic of HBV-ACLF Survival Group and Non-Survival Group |
Differential Protein Screening
In this project, Q-Exactive HF X (Thermo Fisher Scientific, San Jose, CA) was used to acquire mass spectrometry (MS) data for 15 samples in DIA mode, 14,581 peptide and 4155 protein were quantified, the data are available at the China National GeneBank DateBase Sequence Archive (CNSA) with the accession number CNP0002611. Quantification of peptides and proteins was performed using MSstats software packages. The Figures 1a and b were the basic statistics of the DDA identification results, which were unique peptide distribution and protein mass distribution. Through statistical analysis, 247 differential proteins were screened out, including 148 up-regulated proteins and 99 down-regulated proteins (Figure 1c and d).
 |
Figure 1 Protein identification and differential protein distribution diagram. (a) Unique peptide distribution. The X-axis is the number of unique peptides for each protein, and the Y-axis is the number of proteins. (b) Protein mass distribution. The X-axis is protein mass interval (Kilodalton), and the Y-axis is the number of proteins. (c) Differential proteins volcano map. The abscissa for log (FC), and the ordinate for -log10 (P value). The red dot are the up-regulated proteins, and the blue dot are the down-regulated proteins. (d) Differential proteins bar chart. A total of 247 differential proteins, of which 148 are up-regulated and 99 are down-regulated. |
GO Enrichment Analysis
Differential protein GO function enrichment analysis found that they were mainly enriched in high-density lipoprotein particle remodeling, blood coagulation, coagulation, hemostasis and negative regulation of hydrolase activity (TOP5) and other biological processes. These differential proteins were mainly distributed in high-density lipoprotein particle, plasma lipoprotein particle, lipoprotein particle, protein-lipid complex, collagen-containing extracellular matrix (TOP5) and mainly participates in lipoprotein particle receptor binding, enzyme inhibitor activity, lipoprotein particle binding, protein-lipid complex binding, peptidase regulator activity (TOP5). By constructing a functional-target gene network map (Figure 2a), we found that these functions have a strong association with differential proteins, which are mainly related to the coagulation system and lipoprotein regulation (Figure 2b). The results of the GO analysis are detailed in Appendix 1.
 |
Figure 2 Functional enrichment analysis of differential proteins. (a) Function-target protein network diagram. The red round type was the enrichment function, and the blue dot was the differential protein. The connection represents that the function includes the protein, and the size of the red circle represents the amount of protein contained. (b) Mapping of protein and GO function. |
Screening of Core Proteins
Building the PPI network through STRING, we found that α1-microglobulin/bikunin (AMBP) (Bikunin’s precursor protein), apolipoprotein A2 (APOA2), apolipoprotein A1 (APOA1), apolipoprotein C3 (APOC3), lecithin cholesterol acyltransferase (LCAT) and other proteins are located at the core of the network (Figure 3). We focused on differential proteins such as metabolic regulation, enzyme inhibitory activity, and inflammation regulation. The results suggest that multiple proteins such as Inter-alpha-trypsin inhibitor heavy chain family member 1 (ITIH1), AMBP and APOA1 have these functions, and these proteins are located in the extracellular region. AMBP was screened for further research. This gene encodes a complex glycoprotein secreted in plasma, and its precursor proteins can be broken down into functionally distinct proteins: α-1-microglobulin belongs to the lipoprotein transporter superfamily, and bikunin belongs to the family of Kunitz-type protease inhibitors of urinary trypsin inhibitors and plays an important role in many physiological and pathological processes.
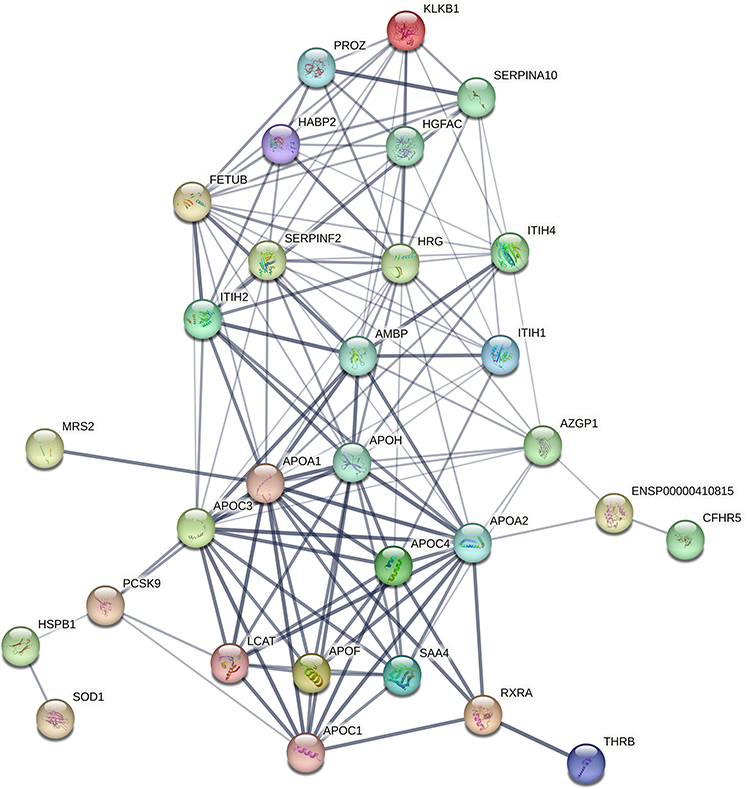 |
Figure 3 PPI diagram of critical proteins. The circle was the differentially expressed proteins, and the line were the interaction between proteins based on previous researches. The thicker the line, the higher the quality of evidence indicating the relationship between two proteins. In PPI network diagram, hub protein AMBP was located at the core of the network, indicating that its function was more important, which was our potential key research target. |
ELISA Verification
We speculate that bikunin may be related to the development of HBV-ACLF, so bikunin with protease inhibition was selected for ELISA verification. The results showed that the plasma concentration of bikunin in normal people was 16.66 ± 4.160μg/mL, and the plasma concentration in HBV-ACLF patients was 7.100 ± 4.281μg/mL (P<0.0001, Figure 4a). ROC analysis found that the two groups had AUC=0.917 and strong discrimination ability (Figure 4b).
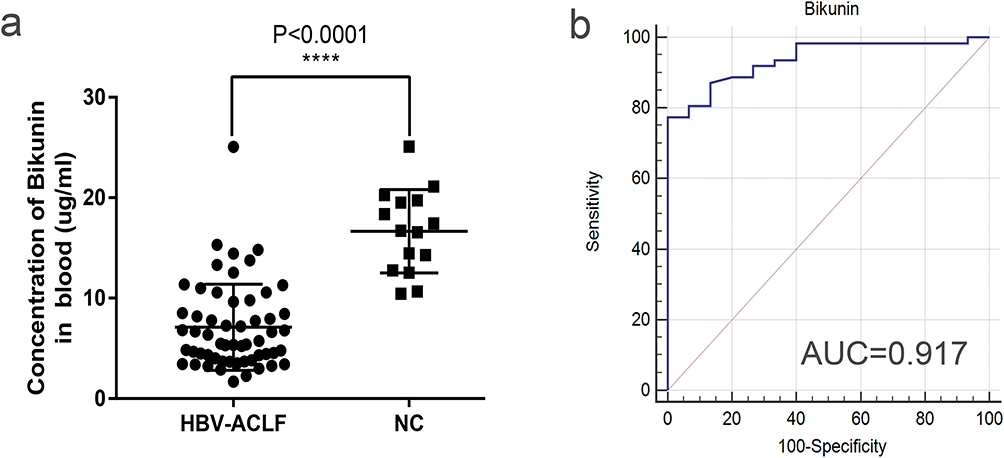 |
Figure 4 Analysis of ELISA results between HBV-ACLF and normal group. (a) Comparative analysis of plasma concentration for bikunin between HBV-ACLF and normal group, ****: p<0.0001. (b) ROC analysis of bikunin plasma concentration in normal group and HBV-ACLF group, AUC=0.917. |
Prognostic Assessment Ability
According to the 90-day survival outcome of HBV-ACLF patients, they were divided into survival group (n=30) and non-survival group (n=26). The plasma concentration in the non-survival group was 5.209 ± 2.653 μg/mL, and the concentration in the survival group was 8.739 ± 4.764μg/mL, and the difference between the two groups was statistically significant (P=0.0015) (Figure 5a). According to the log-rank statistical analysis results, compared with the non-survival group, the level of bikunin in the survival group was higher, and there was a statistical difference between the two groups (Figure 5b). These results suggest that bikunin is associated with prognosis in patients with HBV-ACLF and is also positively correlated with survival. It is reasonable to suggest that bikunin may be a potential prognostic biomarker in patients with HBV-ACLF.
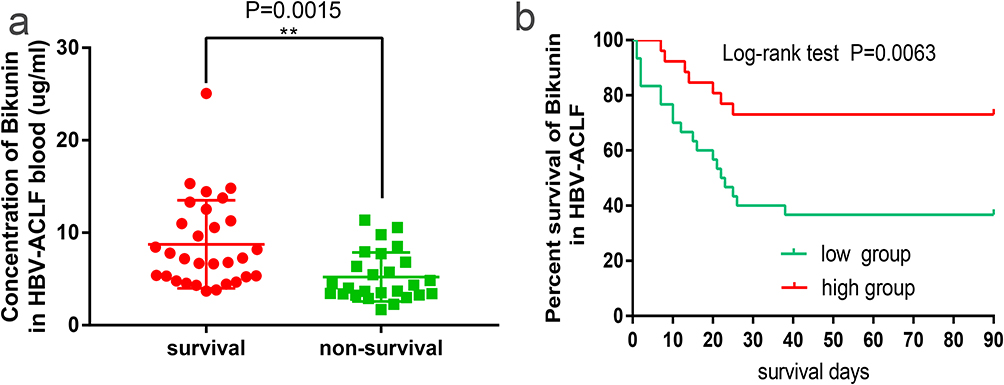 |
Figure 5 Analysis of ELISA results between survival group and non-survival group in HBV-ACLF. (a) Comparative analysis of plasma concentration for bikunin between survival group and non-survival group in ACLF, **: P=0.0015, (b) Survival analysis of bikunin protein. The red line represents the high concentration group (n=28), and the green line represents the low concentration group (n=28), with P=0.0063. |
Discussion
ACLF, initially described as a clinical entity in 2009,3 is characterized by the existence of organ failures and high in-hospital mortality.12 The definition of ACLF varies across countries and regions. The Asian Pacific Association for the Study of the Liver (APASL) defines ACLF as acute liver impairment on the basis of previously diagnosed or undiagnosed chronic liver disease, with jaundice (serum total bilirubin (TBil) ≥ 5 mg/dl) and coagulopathy (international normalized ratio [INR] ≥ 1.5 or prothrombin activity [PTA] <40%) are initially presented, and with peritoneal effusion or hepatic encephalopathy within 28 days.1 The European Association for the Study of the Liver (EASL) defines ACLF as acute hepatic decompensation on the basis of cirrhosis, characterized by multi-organ and systemic (liver, brain, kidney, coagulation, respiratory, circulatory) failure and short-term high mortality (28-day mortality >15%).7 The North American Consortium for the Study of End-Stage Liver Disease’s does not include liver failure and coagulopathy in the diagnostic criteria for ACLF in patients with alcohol- and HCV-related cirrhosis.13,14 The diagnostic criteria for ACLF in China were first proposed in 2006 and have undergone several revisions, and this project included patients in accordance with the latest criteria of the COSSH, which is more in line with the criteria for patients with ACLF in China.
Although a few studies utilized proteomic approaches to identify biomarkers for HBV-ACLF. Professor Li Lanjuan’s research has shown that plasminogen would be a prognostic biomarker for 30-day mortality of HBV-ACLF.15 Another study indicated that a prognostic model P8 which were integrated of GC, HRG, HPR, SERPINA6, age, NEU, INR and total protein was built to distinguish survivors from non-survivors in 28 and 90-days follow-up for HBV-ALCF.16 Ni Zhou et al revealed high diagnostic value of six candidates in HBV-ACLF by iTRAQ-based proteomic approach, including protein GP73, MMR, OPNA, TIII, HPX, APO-CII.17 The molecular signature of HBV-ACLF was still incomplete, further research and exploration are needed. Therefore, we performed this study with the aim of identifying effective biomarkers that reflect the survival of HBV-ACLF. In this study, 247 differential proteins were screened by DIA proteomics method, and for the GO function enrichment analysis and PPI network of differential proteins, we found that the top 5 functions enriched were related to coagulation system, lipoprotein regulation, and inflammation regulation, and we also found that AMBP (Bikunin’s precursor protein), APOA2, APOA1, APOC3, LCAT were located in the network core.
Endotoxemia plays an important role in the development and development of ACLF, ACLF is associated with systemic inflammation with high plasma levels of C-reactive protein12 and cytokines and chemokines,18 therefore, our main focus in the next step is AMBP (Bikunin precursor protein). The alpha-1-microglobulin/bikunin precursor (AMBP) is primarily synthesized in the liver, before being secreted from the cell, the precursor protein is cleaved in the Golgi and processed proteolytically into bikunin and alpha-1-microglobulin (A1M) separately. Bikunin, also known as the urinary trypsin inhibitor (UTI), is a glycoprotein in human plasma and urine, it has many biological functions and has been associated with many diseases, serum bikunin has been considered as the specific biomarkers of both congenital disorders of glycosylation and linkeropathies,19 and may represent a non-invasive marker for early diagnosis of some life-threatening pathological conditions of pregnancy,20 Lepedda et al analyzed bikunin expression in a variety of tumors by using UALCAN proteogenomic analysis portal, including ovarian cancer, breast cancer, colon cancer, lung adenocarcinoma, and so on, and discussed its inhibitory effects and mechanisms in cancer aggressiveness as well as its significance as cancer circulating biomarker.21 Bikunin is one of the main anti-inflammatory mediators. It is upregulated in response to heme, reactive oxygen species (ROS) and to the pro-inflammatory cytokines IL-6, TNF-α, and IL-1β.22 The bikunin core protein carries inhibitory activity towards inflammation-associated proteases and suppresses lipopolysaccharide-induced lethality through down-regulation of tumor necrosis factor-alpha and interleukin-1 beta in macrophages and lipopolysaccharide (LPS)-treated neutrophils.23,24 Bikunin also plays important antifibrotic and organ protective roles with important therapeutic implications in chronic kidney disease.25 Plasma UTI levels showed significant positive correlations with the levels of prothrombin time (PT), hepaplastin test, antithrombin III, a2-plasmin inhibitor, plasminogen (Plg) and fibrinogen.26 One retrospective study showed that Ulinastatin was protective against ischemia-reperfusion liver injury after partial liver resection,27 Ulinastatin could be a potential agent for prevention and treatment of acute liver injury induced by LPS/D-gal.28 Recent studies have shown that bikunin protects against acetaminophen-induced liver injury by alleviating ferroptosis via the SIRT1/NRF2/HO-1 pathway.29 Clinically, bikunin has been used to treat acute inflammatory diseases, such as septic shock, pancreatitis and disseminated intravascular coagulation. At present, there is a lack of research on the prognosis between bikunin and HBV-ACLF. In this study, through ELISA analysis, we found that bikunin expression decreased in HBV-ACLF and was positively correlated with prognosis. In summary, we believe that bikunin can not only judge the prognosis of HBV-ACLF well but also provide new treatment strategies.
This study has several limitations. First, this study was focused on bikunin mainly, but whether the other biomarkers could predict HBV-ACLF outcome has not been investigated. Second, only patients with HBV-ACLF were included in the study, and ACLF caused by other etiologies was not enrolled. Third, the sample of this study was small. Finally, the specific mechanism of bikunin in HBV-ACLF remains unclear. Therefore, this study needs to be validated by a larger sample size, comparative analysis of the other candidate markers and other etiologies for ACLF need to be investigated, and it is necessary to explore the mechanism of bikunin in HBV-ACLF through vivo and vitro experiments.
In conclusion, we investigated the proteomes of patients with HBV-ACLF using DIA mass spectrometry. Biomarker bikunin could distinguish the non-survivors from survivors for HBV-ACLF, it deserves to be investigated through further research and provides new strategies for clinical prognosis judgment and treatment.
Data Sharing Statement
The DIA data are available at the China National GeneBank DateBase Sequence Archive (CNSA) with the accession number CNP0002611. The clinical raw data of this article will be made available by the corresponding author.
Ethics Approval and Consent to Participate
The study protocol and informed consent were approved by the Clinical Experiment Ethics Committee of Affiliated Hospital of Southwest Medical University (No: KY2021014). The clinical trial registration No. was ChiCTR2100042896. Written informed consents were obtained from all study participants. This study was conducted in accordance with all the guidelines and principles described in the Declaration of Helsinki.
Funding
This study was supported by the Strategic Cooperation Project of Suining First People’s Hospital – Southwest Medical University (2020SNXNYD02); Department of Science and Technology of Sichuan Province (2022NSFSC1522).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sarin SK, Choudhury A, Sharma MK, et al. Acute-on-chronic liver failure: consensus recommendations of the Asian Pacific association for the study of the liver (APASL): an update. Hepatol Int. 2019;13(4):353–390. doi:10.1007/s12072-019-09946-3
2. Bernal W, Jalan R, Quaglia A, Simpson K, Wendon J, Burroughs A. Acute-on-chronic liver failure. Lancet. 2015;386(10003):1576–1587. doi:10.1016/S0140-6736(15)00309-8
3. Sarin SK, Kumar A, Almeida JA, et al. Acute-on-chronic liver failure: consensus recommendations of the Asian Pacific Association for the study of the liver (APASL). Hepatol Int. 2009;3(1):269–282. doi:10.1007/s12072-008-9106-x
4. Trepo C, Chan HL, Lok A. Hepatitis B virus infection. Lancet. 2014;384(9959):2053–2063. doi:10.1016/S0140-6736(14)60220-8
5. Mezzano G, Juanola A, Cardenas A, et al. Global burden of disease: acute-on-chronic liver failure, a systematic review and meta-analysis. Gut. 2022;71(1):148–155. doi:10.1136/gutjnl-2020-322161
6. Wu T, Li J, Shao L, et al. Development of diagnostic criteria and a prognostic score for hepatitis B virus-related acute-on-chronic liver failure. Gut. 2018;67(12):2181–2191. doi:10.1136/gutjnl-2017-314641
7. Jalan R, Saliba F, Pavesi M, et al. Development and validation of a prognostic score to predict mortality in patients with acute-on-chronic liver failure. J Hepatol. 2014;61(5):1038–1047. doi:10.1016/j.jhep.2014.06.012
8. Choudhury A, Jindal A, Maiwall R, et al. Liver failure determines the outcome in patients of acute-on-chronic liver failure (ACLF): comparison of APASL ACLF research consortium (AARC) and CLIF-SOFA models. Hepatol Int. 2017;11(5):461–471. doi:10.1007/s12072-017-9816-z
9. Li X, Wang W, Chen J. Recent progress in mass spectrometry proteomics for biomedical research. Sci China Life Sci. 2017;60(10):1093–1113. doi:10.1007/s11427-017-9175-2
10. Kobayashi H, Suzuki M, Kanayama N, Terao T. A soybean Kunitz trypsin inhibitor suppresses ovarian cancer cell invasion by blocking urokinase upregulation. Clin Exp Metastasis. 2004;21(2):159–166. doi:10.1023/b:clin.0000024751.73174.c2
11. Tanaka Y, Kobayashi H, Suzuki M, Kanayama N, Suzuki M, Terao T. Upregulation of bikunin in tumor-infiltrating macrophages as a factor of favorable prognosis in ovarian cancer. Gynecol Oncol. 2004;94(3):725–734. doi:10.1016/j.ygyno.2004.06.012
12. Arroyo V, Moreau R, Jalan R. Acute-on-chronic liver failure. N Engl J Med. 2020;382(22):2137–2145. doi:10.1056/NEJMra1914900
13. O’Leary JG, Reddy KR, Garcia-Tsao G, et al. NACSELD acute-on-chronic liver failure (NACSELD-ACLF) score predicts 30-day survival in hospitalized patients with cirrhosis. Hepatology. 2018;67(6):2367–2374. doi:10.1002/hep.29773
14. Rosenblatt R, Shen N, Tafesh Z, et al. The North American Consortium for the study of end-stage liver disease-acute-on-chronic liver failure score accurately predicts survival: an external validation using a national cohort. Liver Transpl. 2020;26(2):187–195. doi:10.1002/lt.25696
15. Wu D, Zhang S, Xie Z, et al. Plasminogen as a prognostic biomarker for HBV-related acute-on-chronic liver failure. J Clin Invest. 2020;130(4):2069–2080. doi:10.1172/JCI130197
16. Sun Z, Liu X, Wu D, et al. Circulating proteomic panels for diagnosis and risk stratification of acute-on-chronic liver failure in patients with viral hepatitis B. Theranostics. 2019;9(4):1200–1214. doi:10.7150/thno.31991
17. Zhou N, Wang K, Fang S, et al. Discovery of a potential plasma protein biomarker panel for acute-on-chronic liver failure induced by Hepatitis B virus. Front Physiol. 2017;8:1009. doi:10.3389/fphys.2017.01009
18. Claria J, Stauber RE, Coenraad MJ, et al. Systemic inflammation in decompensated cirrhosis: characterization and role in acute-on-chronic liver failure. Hepatology. 2016;64(4):1249–1264. doi:10.1002/hep.28740
19. Haouari W, Dubail J, Lounis-Ouaras S, et al. Serum bikunin isoforms in congenital disorders of glycosylation and linkeropathies. J Inherit Metab Dis. 2020;43(6):1349–1359. doi:10.1002/jimd.12291
20. Lepedda AJ, De Muro P, Capobianco G, Formato M. Role of the small proteoglycan bikunin in human reproduction. Hormones. 2020;19(2):123–133. doi:10.1007/s42000-019-00149-x
21. Lepedda AJ, Nieddu G, Cannas C, Formato M. Molecular and pathobiological insights of bikunin/UTI in cancer. Mol Biol Rep. 2023;50(2):1701–1711. doi:10.1007/s11033-022-08117-2
22. Lin SD, Takikawa Y, Endo R, Suzuki K. Proinflammatory cytokines up-regulate synthesis and secretion of urinary trypsin inhibitor in human hepatoma HepG2 cells. Hepatol Res. 2004;29(4):243–248. doi:10.1016/j.hepres.2004.04.003
23. Matsuzaki H, Kobayashi H, Yagyu T, et al. Bikunin inhibits lipopolysaccharide-induced tumor necrosis factor alpha induction in macrophages. Clin Diagn Lab Immunol. 2004;11(6):1140–1147. doi:10.1128/CDLI.11.6.1140-1147.2004
24. Kanayama S, Yamada Y, Onogi A, et al. Molecular structure and function analysis of bikunin on down-regulation of tumor necrosis factor-alpha expression in activated neutrophils. Cytokine. 2008;42(2):191–197. doi:10.1016/j.cyto.2007.12.011
25. Wei X, Zhu X, Jiang L, Long M, Du Y. Recent research progress on the role of ulinastatin in chronic kidney disease. Nephrology. 2021;26(9):708–714. doi:10.1111/nep.13906
26. Lin SD, Endo R, Sato A, Takikawa Y, Shirakawa K, Suzuki K. Plasma and urine levels of urinary trypsin inhibitor in patients with acute and fulminant hepatitis. J Gastroenterol Hepatol. 2002;17(2):140–147. doi:10.1046/j.1440-1746.2002.02676.x
27. Abu-Amara M, Gurusamy KS, Glantzounis G, Fuller B, Davidson BR. Pharmacological interventions for ischaemia reperfusion injury in liver resection surgery performed under vascular control. Cochrane Database Syst Rev. 2009;2009(4):CD008154. doi:10.1002/14651858.CD008154
28. Lu J, Chen YP, Wan R, Guo CY, Wang XP. Protective effects of ulinastatin on acute liver failure induced by lipopolysaccharide/D-galactosamine. Dig Dis Sci. 2012;57(2):399–404. doi:10.1007/s10620-011-1927-0
29. Wang C, Liu T, Tong Y, et al. Ulinastatin protects against Acetaminophen-induced liver injury by alleviating ferroptosis via the SIRT1/NRF2/HO-1 pathway. Am J Transl Res. 2021;13(6):6031–6042.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.