Back to Journals » Risk Management and Healthcare Policy » Volume 16
Big Data-Enabled Analysis of Factors Affecting Medical Expenditure in the Cerebral Infarction of a Developing City in Western China
Authors Zeng S, Zhang Y, Guo C, Zhou X, He X
Received 6 September 2023
Accepted for publication 3 December 2023
Published 13 December 2023 Volume 2023:16 Pages 2703—2714
DOI https://doi.org/10.2147/RMHP.S438869
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gulsum Kaya
Siyu Zeng,1 Ying Zhang,2 Chuijiang Guo,1 Xia Zhou,1 Xiaozhou He3
1School of Logistics, Chengdu University of Information Technology, Chengdu, Sichuan, People’s Republic of China; 2General Practice Ward, General Practice Medical Center, West China Hospital, Sichuan University, Chengdu, Sichuan, People’s Republic of China; 3Business School, Sichuan University, Chengdu, Sichuan, People’s Republic of China
Correspondence: Xiaozhou He, Business School, Sichuan University, No. 24 South Section 1, Yihuan Road, Chengdu, Sichuan, 610065, People’s Republic of China, Tel +86-18512811267, Email [email protected]
Purpose: Cerebral infarction (CI) has been one of the leading causes of death in China since 2017, and controlling the medical expenses of this disease is an urgent issue for the Chinese government. This study aims to explore the important factors that affect the hospitalization expenses of CI patients and to provide a scientific basis for establishing a reasonable reimbursement mechanism and hospitalization expense standard for CI patients.
Methods: Data from 109,314 inpatients from the Healthcare Security Administration of Chengdu in western China from January 2016 to December 2018 were utilized. Descriptive statistical analysis was used for variable characteristic analysis. The Mann–Whitney test and Kruskal–Wallis test were used for single-factor analysis, and multiple linear stepwise regression was used for single-factor analysis and multiple-factor analysis.
Results: This study found that the average direct economic burden of CI in Chengdu was approximately 10,569 Chinese yuan (CNY), about 1450 US dollars, the average length of stay (LOS) was 14.47 days, the indirect economic burden was approximately 2817 CNY, and the total economic burden was 13,386 CNY for a CI inpatient. Gender, insurance type, grade of medical institution, the level of payment type, age, LOS, and complications and comorbidities (CCs) are the most important factors affecting CI medical costs.
Conclusion: Citizens should improve their lifestyle habits to reduce disease risk to avoid the associated medical and economic burdens. Hospitals should improve their medical technology to decrease the LOS and reduce direct medical costs. The government should actively promote the hierarchical diagnosis and treatment policy to reduce the waste of medical resources caused by low-acuity patients going to high-level hospitals for treatment. The National Healthcare Security Administration should optimize the medical insurance payment method and establish a corresponding mechanism to reduce the occurrence of excessive medical treatments such as overuse.
Keywords: medical expenditure, cerebral infarction, influencing factors, reimbursement mechanism
Introduction
Stroke, a chronic noncommunicable disease, is a significant global public health issue and in 2017 became the leading cause of death in China.1–4 It reaching a total of 101 million prevalent cases and 6.55 million deaths globally, as well as 28.8 million prevalent cases and 2.19 million deaths, and 45.9 million in China in 2019.5–8 The burden of stroke is particularly severe in low- and middle-income countries (LMICs), where the morbidity and mortality rates from stroke are higher compared to that of high-income countries and any future increases in stroke rates will most likely be driven by LMICs.9,10 About 80% of all strokes are CI.11 In this study, a total of 297,757 patients with CI were hospitalized from 2011 to 2018. Among them were 149,376 males and 148,381 females, accounting for 50.16% and 49.84%, respectively. The incidence rate was calculated based on the number of insured people in Chengdu, and the incidence was increasing. Using 2018 as an example, the number of hospitalized people was 55,081, an increase of 14.91% compared with 2017. The incidence rate was 0.33%, which means that 33 people per 10,000 people may be hospitalized due to CI.
CI and its complications have resulted in a considerably increased risk of disability and death.12,13 Moreover, the cost of CI is much higher than most other diseases, bringing a huge economic burden on patients, their families, and basic medical insurance funds.8,14 The economic burden refers to the direct economic burden and indirect economic burden.15 Direct economic burden refers to the total medical cost, including the medication, examination, and bed costs, and any other costs incurred in the hospital.16 Indirect economic burden refers to the charge for lost working time, transportation costs, nutrition costs, and any other costs not paid to the hospital. The total health expenditure expressed continuous increase as share of GDP spending since 1995 in China.17 Studies show that the medical cost growth rate has exceeded the income growth of citizens,16 and more than 60% of CI disease costs are paid by basic medical insurance.18 The direct medical cost spent in hospitals reached 36.458 billion CNY, ranking first among all diseases and accounting for 17% of the total medical cost of treating disease, equivalent to 0.66% of GDP in 2017.18,19 Reducing the medical cost associated with CI is very important to reduce the economic burden on patients and basic medical insurance funds. Therefore, exploring the important factors that affect the hospitalization expenses of CI patients and providing a scientific basis for establishing a reasonable reimbursement mechanism and standard for the hospitalization expenses of CI patients have become urgent issues.
In this study, data was collected from 417 hospitals in a developing city, Chengdu, in western China between 2016 and 2018. Descriptive statistical analysis, single factor analysis, and multivariate linear regression analysis were utilized to identify the key factors affecting the medical costs of CI. We used this data to provide scientific and reasonable suggestions for reducing medical costs. The remainder of this paper is organized as follows. In Section 2, the materials and methods are introduced. In Section 3, our results are presented, including general information and inpatient medical expenditure, and single and multiple factor analysis of the factors influencing inpatient medical expenditure. In Section 4, the results are discussed. Section 5 concludes the study and provides a description of directions for future research.
Materials and Methods
Data Source
This study was supported by the Healthcare Security Administration of Chengdu in western China, which facilitated this health economics research to analyze the annual direct economic burden of CI. The data used in this research were collected from the Healthcare Security Administration of Chengdu between January 2016 and December 2018 and included medical records and cost information related to 111,025 inpatients with primary diagnoses of “cerebral infarction” (ICD-10 codes I63.1 to I63.9) from internal medicine departments of Chengdu. The original information about these patients included 58 variables, including gender, age, occupation, living place, LOS, hospitalization expenses, medical payment method, insurance type, insurance charge, CCs, level of medical institution, primary diagnosis, other diagnoses, and term of operation. This data was non-public, and all experimental protocols were approved by the Healthcare Security Administration of Chengdu.
Data Preprocessing
The data processing was conducted as follows.
First, considering the impact of the LOS on the cost of hospitalization, extreme cases with an LOS exceeding 60 days were excluded based on previous cases.19 According to the medical insurance policy of Chengdu, the reimbursement bill is capped at 150,000 CNY per year, excluding more than 150,000 cases. The basic medical insurance for urban employees and the basic medical insurance for urban residents were considered in this study. After removing cases with incomplete data, 109,314 cases remained.
Considering the impact of inflation on hospitalization costs, this paper uses the consumer price index (CPI) for 2016 to adjust hospitalization costs. To solve the problem of data bias, a logarithmic transformation of hospitalization costs was conducted.
Finally, for indicators of disease severity, we referred to the classification methods from the disease diagnosis related groups of China Healthcare Security (CHS-DRG) Technical Specifications and Grouping Protocols,20 and we used CCs as one of the indicators of disease acuity, and coded 1 as severe CCs, 2 as general CCs, and mild or no CCs were coded as 3. Males were coded as 1 and females as 2. The basic medical insurance of urban employees was coded as 1, and the basic medical insurance of urban resident was coded as 2. Age was divided into five categories: 0–45-year-olds as 1, 45–65 as 2, 65–75 as 3, 75–85 as 4, and older than 85 years as 5. The remaining codes are shown in Table 1.
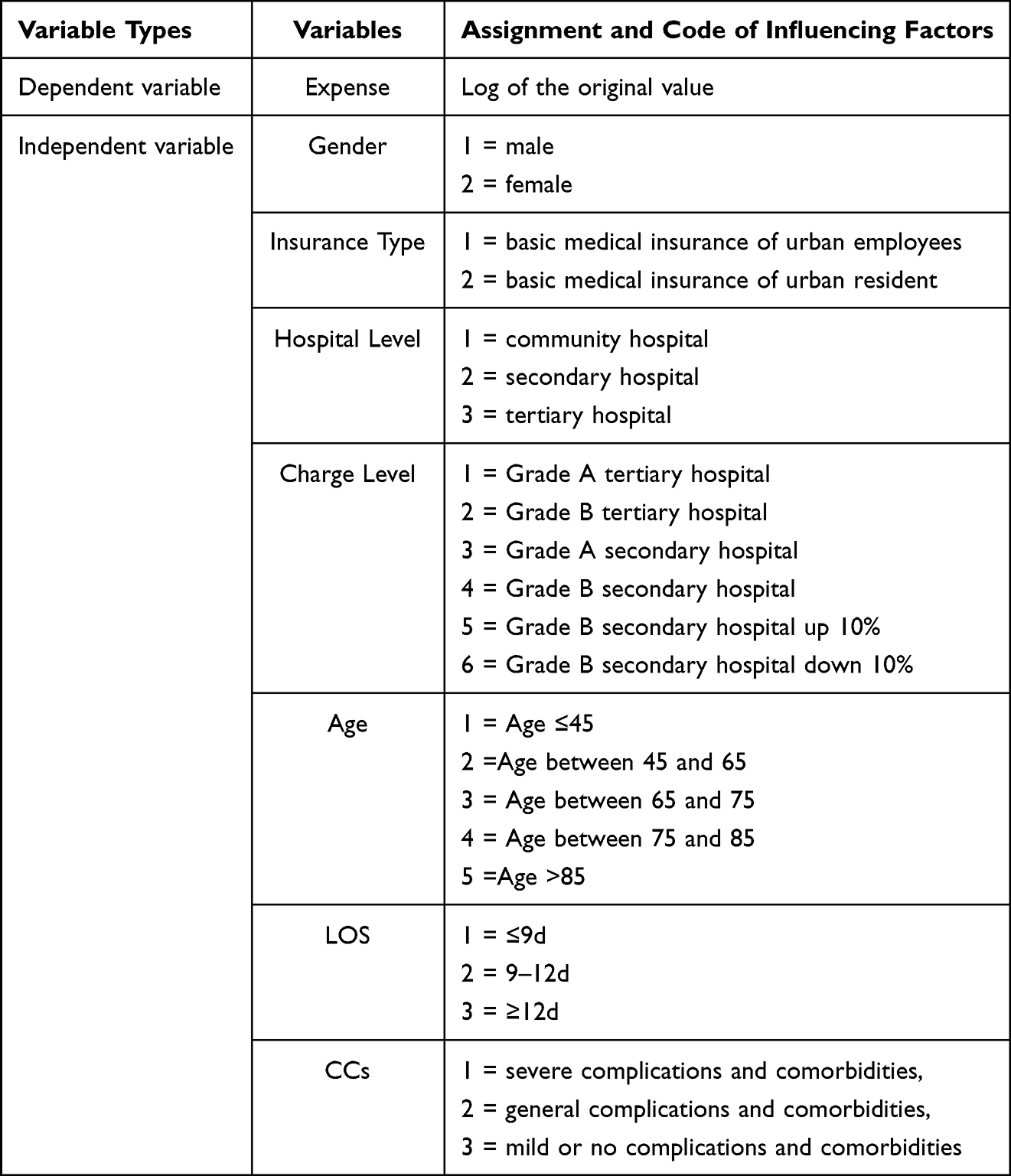 |
Table 1 Variable and Assignment Description |
Methods
R 4.0.2 software, an open source software, was used for data analysis, descriptive statistics analysis, single factor analysis, and multivariate linear regression analysis. Data were first summarized and described as mean, median ± interquartile range (IQR), and standard deviation, and the proportion of each variable was also calculated. Then, the Mann–Whitney test and the Kruskal–Wallis test were used for single-factor analysis, which allowed for the comparison of two and multiple groups of variables.21 A significance level of p <0.05 was set for all statistical tests, at an inspection level of α = 0.05. The statistically significant variables were considered as influence factors according to the single factor analysis. Finally, a stepwise multivariate linear regression model was constructed to explore the factors affecting the direct economic burden of CI. Significant influencing factors extracted from the single-factor analysis were imported into the multiple-factor model as independent variables. The selection criterion of the model was the lowest Akaike information criterion (AIC) value, and the multicollinearity was diagnosed by the Kappa value, with the multiple stepwise regression model fitted based on this.
Results
Descriptive Analysis
The total direct burden of 109,314 CI patients from 2016 to 2018 was 1.155 billion CNY, and the average annual direct burden per patient was 10,569.88 CNY. The demographic data of all patients in this study are listed in Table 2 and the sample information diagram of variables is shown in Figures 1–7.
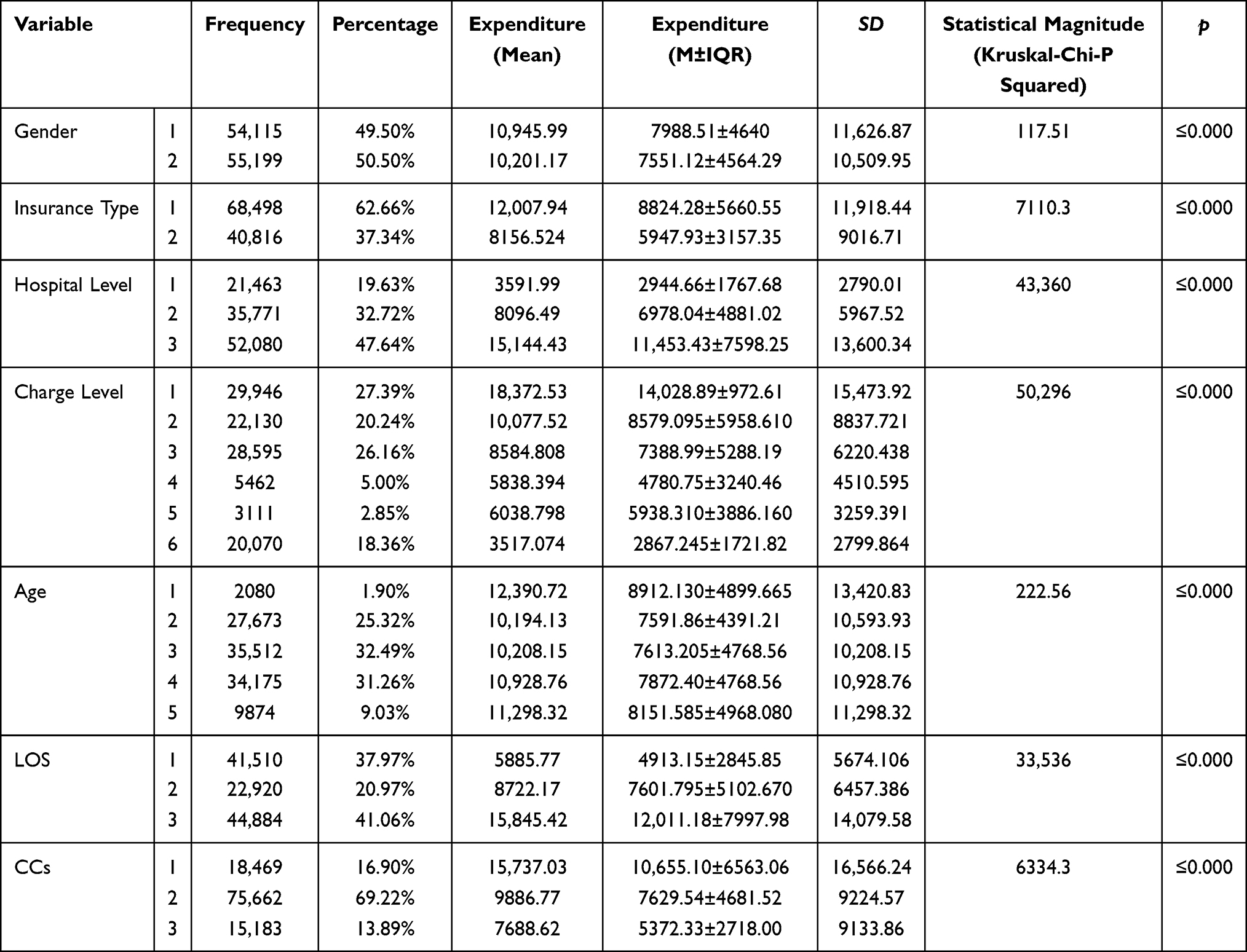 |
Table 2 Basic Characteristics and Results of Single Factor Analysis of the Factors Influencing Inpatient Medical Expenditure (n = 109,314) |
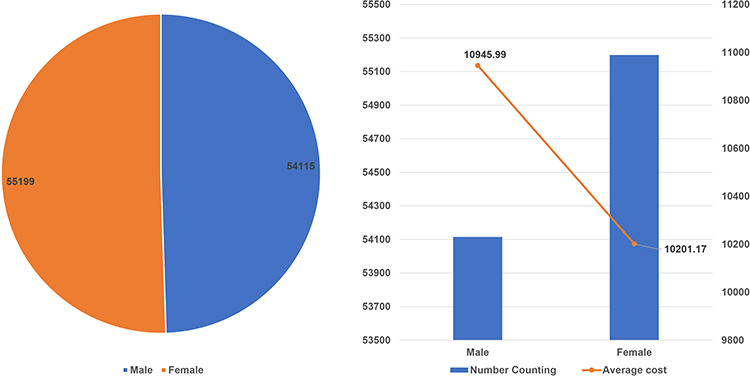 |
Figure 1 The effect of gender on hospitalization expenditure. |
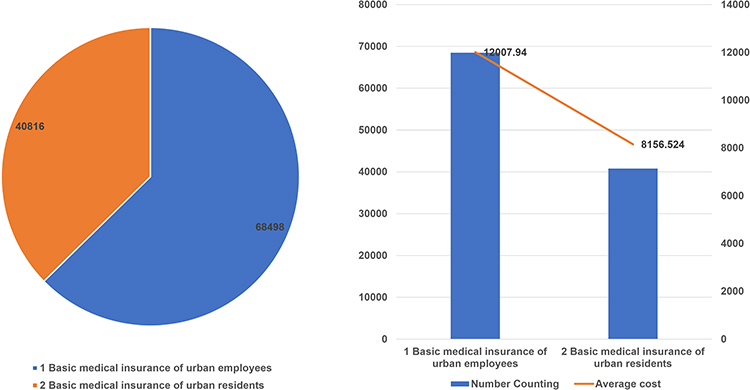 |
Figure 2 The effect of insurance type on hospitalization expenditure. |
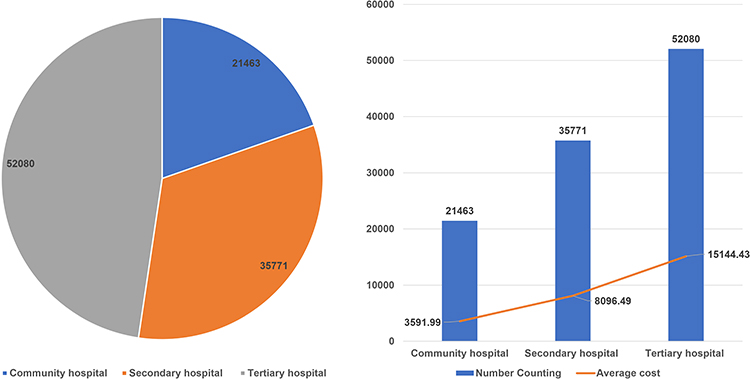 |
Figure 3 The effect of hospital level on hospitalization expenditure. |
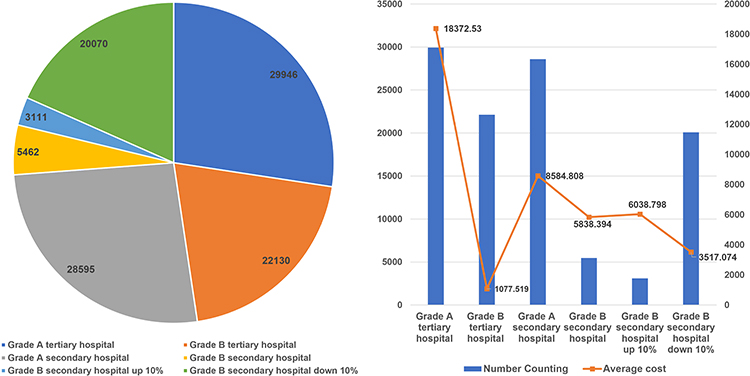 |
Figure 4 The effect of charge level on hospitalization expenditure. |
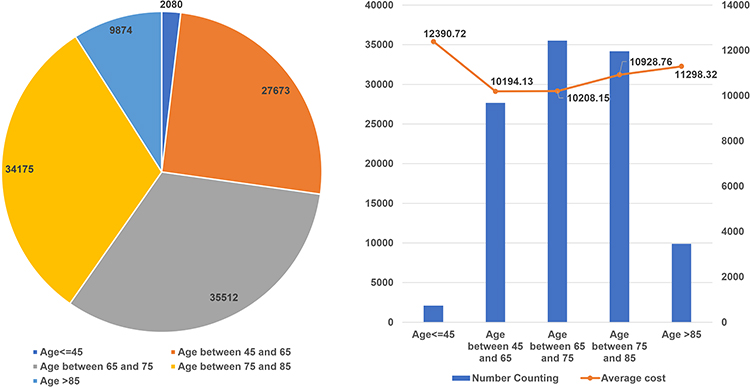 |
Figure 5 The effect of age on hospitalization expenditure. |
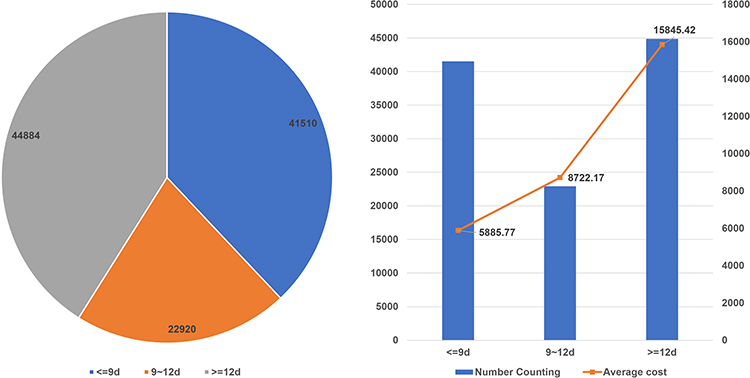 |
Figure 6 The effect of LOS on hospitalization expenditure. |
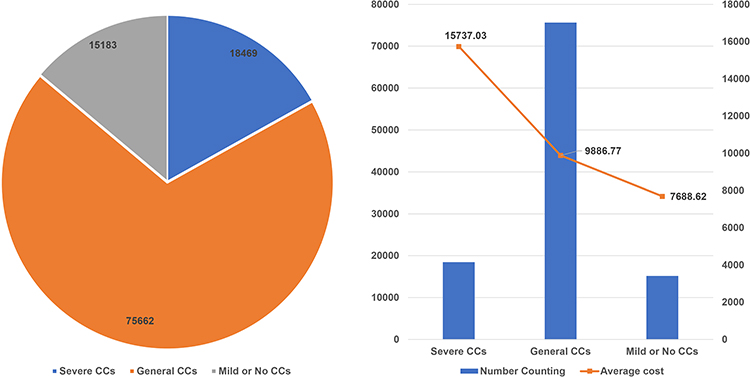 |
Figure 7 The effect of CCs on hospitalization expenditure. |
Figure 1 is the descriptive analysis diagram of the variable gender. There were 54,115 males with an average direct burden of 10,945 CNY, and 55,199 females with an average direct burden of 10,201 CNY, accounting for 49.50% and 50.50%, respectively.
Figure 2 is the descriptive analysis diagrams of the variable insurance type. There were 68,491 urban workers and 40,816 urban and rural residents, accounting for 62.66% and 37.34%, respectively. The average costs for urban workers and rural residents were 12,007 CNY and 8156 CNY.
Figure 3 is the descriptive analysis diagrams of the hospital level. Affected by the size of the hospital, tertiary hospitals received the largest number of patients, accounting for 47.64%. The higher the hospital level, the higher of the hospitalization cost. The average hospitalization costs of the three levels of hospitals were 3591, 8096, 15,144 respectively.
Figure 4 is the descriptive analysis diagrams of charge level. The number of patients in grade A tertiary hospital was the largest, accounting for 27.39%, with a per capita cost of 18,372 CNY. The number of patients in grade B secondary hospital up 10% was the smallest, only 3111, accounting for 2.85%, with a per capita cost of 3517 CNY, most hospital of this charge level are community hospital.
Figure 5 is the descriptive analysis diagrams of age. Considering that elderly people (over 65 years old) accounted for the majority of patients, this section further divides the elderly population into three subgroups: 65–75, 75–85, and over 85 years old. In Chengdu, from 2016 to 2018, there were 2080, 27,637, 35,512, 34,175, and 9874 patients of all ages, accounting for 1.9%, 25.32%, 32.49%, 31.26% and 9.03% respectively.
Figure 6 is the descriptive analysis diagrams of LOS. It can be seen that the majority of patients’ LOS are more than 12 days, and those patients have the highest cost, with an average of 15,845 CNY per person.
Figure 7 is the descriptive analysis diagrams of CCs. Patients with severe CCs had the highest medical costs, 18,469 CNY per person. 69.22% of the patients were general CCs, with the per capita cost 9886 CNY.
Univariate Analysis
The results indicate that the main influencing factors of the direct cost of inpatients were gender, insurance type, grade of medical institution, level of payment type, age, LOS, and CCs (p<0.05). Factors like occupation, living place, and marital status were not discussed here as the results indicate those lacked statistical difference (p >0.05). The direct cost associated with males was significantly higher than that of female inpatients with CI, and the average cost of males was 6.8% higher than that of females.
The cost of basic medical insurance for urban employees was significantly higher than the cost of basic medical insurance for urban residents. Additionally, the higher the grade of the medical institution and level of payment type, the higher the medical cost was found to be. Similarly, higher ages and longer hospital stays were associated with higher medical costs. Details are shown in Table 2.
Multivariate Linear Regression Analysis
Taking the natural logarithm of medical costs as the dependent variable, a stepwise regression model was utilized to filter the independent variables. The variables found to have a significant influence on medical expenses in the results of univariate analysis were considered as the independent variables of multivariate regression analysis. The selection criterion of the model was the lowest AIC, and the final multiple regression model was fitted. The model results are as follows.
The fitted model AIC was 161,092.6, and we used the coefficient of determination R-squared (R2) to measure the goodness of fit of the linear model. The R2 was 0.685, the adjusted R2 was 0.6849, and the residual standard error (SE) was 0.4786, which indicates that the regression line fits the observations well.
The multicollinearity test revealed that the Kappa value of the model was 1, (ie, less than 100) which indicates that there was no collinearity problem in the model. For the model, we utilized p <0.001, indicating that a test level of α = 0.05. Thus, the fit of the linear regression equation can be considered statistically significant.
To facilitate interpretation, age and LOS were treated as continuous variables, and the remaining variables were factor variables in the multivariate linear regression analysis. All the variables were statistically significant, and the charge grade and LOS were the main influencing factors of hospitalization cost according to the regression coefficient. Different hospitals accept patients with different illness acuities, so the impact of the charge level on the cost of hospitalization is significant. According to the coefficient, the cost of male patients is higher than that of female patients. Additionally, the hospitalization cost of urban workers was higher than that of urban and rural residents. Among hospital levels, the results of tertiary hospitals were not significant and were not discussed. The cost of a third-class hospital was higher than that of a second-class hospital, and the cost of a second-class hospital was higher than that of a first-class hospital. The older the patient’s age, the higher the hospitalization cost. Notably, for every year of age increase, hospitalization costs increase by 1.0012 times. Similarly, the longer the LOS, the higher the hospitalization cost, with each additional LOS day increasing the hospitalization cost by 1.0443 times. Furthermore, the hospitalization cost of patients with severe CCs was 1.18 times that of patients with general comorbidities and 0.84 times that of patients without CCs. Details are shown in Table 3.
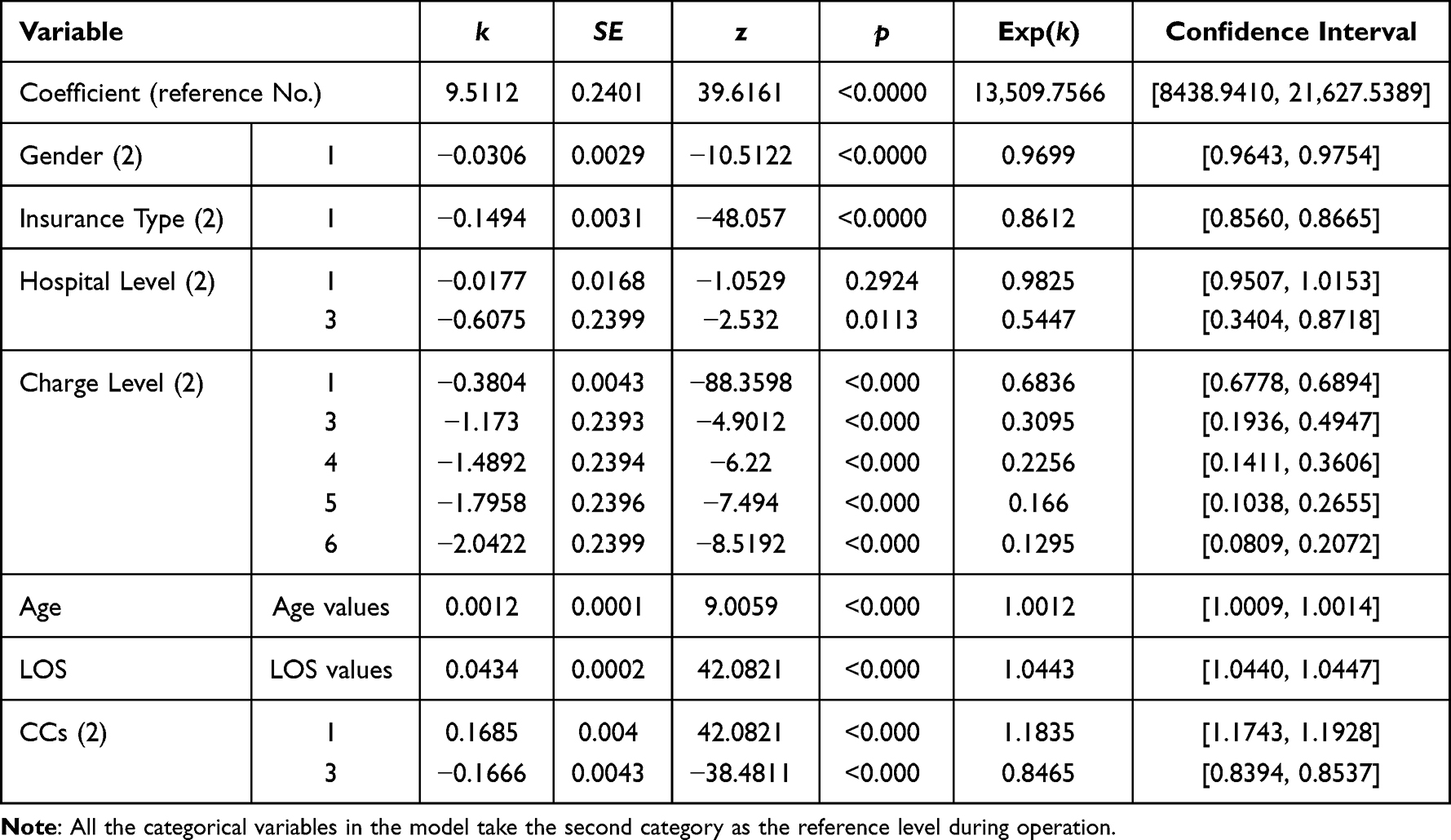 |
Table 3 Multiple Linear Stepwise Regression Results of Factors Influencing Hospitalization Expenditure in CI Disease Patients |
Discussion
Health spending in the BRICS countries (Brazil, Russia, India, China, and South Africa) has been increasing due to their economic prosperity. However, health security is still a distant dream in these countries due to low public health spending, lack of prepaid health coverage, and high out-of-pocket spending.22,23 The total health expenditure of China, one of the BRICS members, has continuously increased as a share of GDP spending since 1995 and controlling health expenditure is a big challenge for the Chinese government.17 In particular, CI, a disease with serious medical expenses, is more worthy of study. This study was based on data provided by the Healthcare Security Administration of an underdeveloped area in western China, which included 416 hospitals. Based on the theoretical findings presented in the results, interviews were conducted with hospital physicians and staff from the Healthcare Security Administration of Chengdu to learn more about the reasons behind the theoretical results.
The results of our study demonstrate that the average direct economic burden of CI in Chengdu was approximately 10,569 CNY. Taking into account that the average monthly salary in Chengdu in 2018 was 4600 CNY and the average LOS was 14.47 days, the indirect economic burden was approximately 2817 CNY, and the total economic burden was 13,386 CNY for a CI inpatient. Research found that the increase in medical cost is related to many factors, such as longevity, population aging, increased non-communicable diseases, growing patient expectations, gains in social welfare, and improvement in living standards.24–26 To control medical costs, in 2016, Chengdu canceled the drug markup, that is, hospitals no longer earned profits from drugs, which made medical costs lower in 2016 than in 2015. Even in this context, the medical cost of CI is still higher than that of other diseases. In 2018, the average LOS for all types of diseases was 10.14 days, compared to 13.1 days for CI, and the direct and indirect economic losses caused by CI to patients were greater than those of other diseases.
From the results of both univariate and multivariate linear regression analyses, it can be seen that the LOS and CCs are important factors affecting hospitalization expenses. Medical costs increased as the costs of medicine, examinations, and services increased during prolonged hospitalization.27 Table 3 shows that for each additional day of LOS, hospitalization expenses increased 1.04 times. Notably, the LOS is an important index to measure the quality of medical services. Reducing the LOS and accelerating the turnover rate of inpatient beds can effectively increase the efficient use of medical resources, and alleviate supply insufficiencies and uneven distribution of medical resources in China.28 According to Chengdu’s 2019 statistical yearbook, in 2018, there were 10,755 medical and health institutions in Chengdu, with 143,200 beds, increasing by 9.1% and 11.79% compared to 2016, respectively. From 2016 to 2018, the average LOS for CI patients in tertiary hospitals dropped from 19.35 days to 14.48 days, a cumulative decline of 25.16%. The promotion of new medical technologies such as minimally invasive surgery is one of the important reasons for the declining LOS. However, hospitals may extend the LOS to increase the revenue. To avoid out-of-hospital complications and reduce out-of-hospital medical costs, both doctors and patients may tend to stay longer than is required. Therefore, effective incentives are also needed to reduce the LOS and thus control medical costs. Medical costs were seen to have decreased when patients had mild CCs or no CCs and increased when patients had severe CCs.Previous studies have also demonstrated a strong correlation between medical costs and CC.29 Following interviews with doctors, we believe that prediction can control the emergence of CCs, thus reducing medical costs. Taking grade 3 hypertension as an example, if we can accurately predict in advance and intervene in advance, the average cost of each hospitalization can be reduced by more than 1000 CNY.
A large number of studies in the past decade have shown that CI and other neurological diseases have different effects on patients of different genders,30 and the risk of complications and mortality among female patients is higher than that of male patients.31 In 2018, for example, the male population of Chengdu was 7,322,452 and the female population was 7,438,028. The number of males hospitalized with CI was 27,578, and the number of females hospitalized with CI was 27,503. The hospitalization rate of CI was 0.38% and 0.37% respectively, with males slightly higher than females. Globally, 90.7% of strokes have been associated with ten correctable risk factors: hypertension, diabetes, dyslipidemia, heart disease, smoking, alcohol intake, unhealthy diet, abdominal obesity, physical inactivity, and psychological factors. The number of Chinese men who are considered obese and those who smoke is much higher than those of women, and the living habits of men and women are quite different, which may be the reason for the high medical costs associated with men. Therefore, men should be called upon to improve their lifestyles to reduce their disease risk.
China grades the qualifications of hospitals according to their scale and medical hardware-based capabilities, and different levels of medical institutions are responsible for the treatment of different diseases.32 The hierarchical and graded management system provides patients with different disease priorities for initial medical advice to allocate medical resources.33 Patients admitted to high-level hospitals are more seriously ill, which is the primary cause of the high cost of care in high-level hospitals.
These results demonstrate that the medical costs of CI patients when they have the basic medical insurance of urban employees are significantly higher compared to patients who have the basic medical insurance of urban residents. Medical insurance types are associated with increased medical costs.29,34 The reimbursement ratio of urban employees is higher than that of urban residents in China, and employees can also take time off work while in the hospital. All these factors lead to employees demanding more medical care, which significantly increases costs. Additionally, all of these factors further weaken the equitable use of medical resources.11 However, the government must also adjust the basic medical reimbursement project to reduce medical costs and improve the fairness of medical reimbursement while ensuring the quality of medical services. Social health insurance is not sufficient, and therefore the payment system must be improved to coincide with the increase in medical costs.35 Increasing transparency of medical progress may also help control the overuse of medical funds.36 The Chinese government has launched CHS-DRG and diagnosis-intervention packet pilot programs to solve this problem, and more incentives must be created to ensure that doctors, patients, and the Healthcare Security Administration of Chengdu are actively involved in controlling healthcare costs.
Conclusion
The real data from 416 medical institutions from a less developed region in China were used to identify the factors affecting hospitalization expenses, the first step in reducing medical costs. The results indicate that the average direct economic burden of CI in Chengdu was approximately 10,569 CNY and the indirect economic burden was approximately 2817 CNY, which is higher than most diseases. Gender, insurance type, grade of medical institution, level of payment type, age, LOS, and CCs are the most important factors affecting CI medical costs. The citizens themselves should improve their lifestyles to reduce disease risks and avoid associated medical and economic burdens. Hospitals should improve their medical technologies to decrease the LOS and reduce the associated direct medical costs. The Healthcare Security Administration of Chengdu should optimize the medical insurance payment method and establish a corresponding mechanism to reduce occurrences of excessive medical treatment including overuse. More research in this area is urgently needed. Here are a few limitations to this study. We only considered the personal total cost, and it is better to consider more details, such as treatment expenses, bed expenses, surgery expenses and drug expenses. Also, we only have data of one city, and it’s better to get more than 3 cities and make a comparison. Therefore, more research needs to be done.
Abbreviations
CI, cerebral infarction; CNY, Chinese yuan, the official currency of China; LOS, length of stay; CCs, complications and comorbidities; LMICs, low- and middle-income countries; CPI, consumer price index; CHS-DRG, the disease diagnosis related groups of China Healthcare Security; IQR, interquartile range; AIC, Akaike information criterion.
Data Sharing Statement
All the data were taken from the Medical Insurance Laboratory of the Healthcare Security Administration of Chengdu. They are not publicly available due to the restrictions of the administration.
Ethical Approval
The study does not involve human subjects and adheres to all current laws of China. The data accessed complied with relevant data protection and privacy regulations.
Funding
This project was sponsored by the National Natural Science Foundation of China (No. 72001153) and the Chengdu University of Information Technology talent introduction project (No. KYTZ2022123).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zhou M, Wang H, Zeng X, et al. Mortality, morbidity, and risk factors in China and its provinces, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2019;394(10204):1145–1158. doi:10.1016/S0140-6736(19)30427-1
2. Park SK, Jung JY, Kim MH, et al. The association between changes in proteinuria and the risk of cerebral infarction in the Korean population. Diabetes Res Clin Practice. 2022;192:110090. doi:10.1016/j.diabres.2022.110090
3. Cui R, Liao X, Robinson N, et al. Comparative efficacy of oral traditional Chinese patent medicines for acute cerebral infarction: a protocol for a systematic review and network meta-analysis. Eur J Integrative Med. 2019;32:100977. doi:10.1016/j.eujim.2019.100977
4. Feigin VL, Norrving B, Mensah GA. Global burden of stroke. Circulation Res. 2017;120(3):439–448. doi:10.1161/CIRCRESAHA.116.308413
5. Ma Q, Li R, Wang L, et al. Temporal trend and attributable risk factors of stroke burden in China, 1990–2019: an analysis for the Global Burden of Disease Study 2019. Lancet Public Health. 2021;6(12):e897–e906. doi:10.1016/S2468-2667(21)00228-0
6. Huang Q, Lan X, Chen H, et al. Association Between Genetic Predisposition and Disease Burden of Stroke in China: A Genetic Epidemiological Study. The Lancet Regional Health–Western Pacific; 2023.
7. Feigin VL, Stark BA, Johnson CO, et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021;20(10):795–820. doi:10.1016/S1474-4422(21)00252-0
8. Peng S, Liu X, Cao W, et al. Global, regional, and national time trends in mortality for stroke, 1990–2019: an age-period-cohort analysis for the global burden of disease 2019 study and implications for stroke prevention. Int J Cardiol. 2023;383:117–131. doi:10.1016/j.ijcard.2023.05.001
9. Pandian JD, Kalkonde Y, Sebastian IA, et al. Stroke systems of care in low-income and middle-income countries: challenges and opportunities. Lancet. 2020;396(10260):1443–1451. doi:10.1016/S0140-6736(20)31374-X
10. Khatib R, Arevalo YA, Berendsen MA, et al. Presentation, evaluation, management, and outcomes of acute stroke in low-and middle-income countries: a systematic review and meta-analysis. Neuroepidemiology. 2018;51(1–2):104–112. doi:10.1159/000491442
11. Zeng S, Luo L, Chen F, et al. Association of outdoor air pollution with the medical expense of ischemic stroke: the case study of an industrial city in western China. Int J Health Planning Management. 2021;36(3):715–728. doi:10.1002/hpm.3115
12. Chen CH, Chang YJ, Sy HN, et al. Risk assessment of the outcome for cerebral infarction in tuberculous meningitis. Revue Neurologique. 2014;170(8–9):512–519. doi:10.1016/j.neurol.2014.06.004
13. Kalita J, Misra UK, Nair PP. Predictors of stroke and its significance in the outcome of tuberculous meningitis. J Stroke Cerebrovascular Dis. 2009;18(4):251–258. doi:10.1016/j.jstrokecerebrovasdis.2008.11.007
14. Koester SW, Catapano JS, Rumalla K, et al. Health care expenditures associated with delayed cerebral ischemia following subarachnoid hemorrhage: a propensity-adjusted analysis. World Neurosurgery. 2022;167:e600–e606. doi:10.1016/j.wneu.2022.08.057
15. Movahed MS, Barghazan SH, Adel A, et al. Economic burden of stroke in Iran: a population-based study. Value Health Regional Issues. 2021;24:77–81. doi:10.1016/j.vhri.2020.04.004
16. Luo Y, Yang W, Qi M, et al. Annual direct economic burden and influencing factors of dry eye diseases in central China. Ophthalmic Epidemiol. 2023;30(2):121–128. doi:10.1080/09286586.2021.1959618
17. Jakovljevic M, Chang H, Pan J, et al. Successes and challenges of China’s health care reform: a four-decade perspective spanning 1985—2023. Cost Effectiveness Resource Allocation. 2023;21(1):59. doi:10.1186/s12962-023-00461-9
18. Zhang Y, Chai P, Zhai T, et al. Study on accounting and analysis of curative expenditure on cardio-cerebrovascular diseases in China. Chine Circulation J. 2020;35(9):859–865.
19. Zeng S, Luo L, Fang Y, et al. Cost control of treatment for cerebrovascular patients using a machine learning model in western China. J Healthcare Eng. 2021;2021:1–8. doi:10.1155/2021/6158961
20. The state council of China. Notice of the Office of the National Healthcare Security Administration on issuing the detailed grouping plan for the disease diagnosis related groups of China Healthcare Security (CHS-DRG) (Version 1.0), 2020. Available from: https://www.gov.cn/zhengce/zhengceku/2020-06/19/content_5520572.htm.
21. Hu Y, Zeng S, Li L, et al. Risk factors associated with postoperative complications after liver cancer resection surgery in western China. Cost Effectiveness Resource Allocation. 2021;19(1):1–10. doi:10.1186/s12962-021-00318-z
22. Sahoo PM, Rout HS, Jakovljevic M. Future health expenditure in the BRICS countries: a forecasting analysis for 2035. Globalization Health. 2023;19(1):49. doi:10.1186/s12992-023-00947-4
23. Jakovljevic M, Timofeyev Y, Ekkert NV, et al. The impact of health expenditures on public health in BRICS nations. J Sport Health Sci. 2019;8(6):516. doi:10.1016/j.jshs.2019.09.002
24. Kosaka M, Ozaki A, Kaneda Y, et al. Generic drug crisis in Japan and changes leading to the collapse of universal health insurance established in 1961: the case of Kobayashi Kako Co. Ltd. Cost Effectiveness Resource Allocation. 2023;21(1):1–3. doi:10.1186/s12962-023-00441-z
25. Jakovljevic M, Verhaeghe N, Souliotis K, et al. Challenges of pharmacoeconomics in global health arena—Contemporary momentum in the early 2020s. Front Public Health. 2023;11:1189671. doi:10.3389/fpubh.2023.1189671
26. Jakovljevic M, Chang H, Kumagai N. Global excellence in health economics: Asia and Australasia. Front Public Health. 2023;11:1172632. doi:10.3389/fpubh.2023.1172632
27. Chen C, Song J, Xu X, et al. Analysis of influencing factors of economic burden and medical service utilization of diabetic patients in China. PLoS One. 2020;15(10):e0239844. doi:10.1371/journal.pone.0239844
28. Yang X, Wu H, Liu S, et al. Blood Tests predict length of stay in patients with first-ever ischemic stroke. Modern Preventive Med. 2020;47(6):1133–1137.
29. Han J, Zhang X, Meng Y. Out-patient service and in-patient service: the impact of health insurance on the healthcare utilization of mid-aged and older residents in urban China. Risk Management Healthcare Policy. 2020;2199–2212. doi:10.2147/RMHP.S273098
30. Williams N. How Sex and Gender Impact Clinical Practice: an Evidence-Based Guide to Patient Care. Occupational Med. 2021;71(6–7):307. doi:10.1093/occmed/kqab056
31. Karunawan NH, Pinzon RT. The gender differences in risk factors and clinical outcomes of atherosclerotic cardiovascular disease: a hospital-based stroke registry in ASEAN country. Metabolism. 2021;116.
32. Li L, Du T. The different classification of hospitals impact on the equity of medical outcomes of patients in China[Preprint]. Available at Research Square; 2021.
33. Liu C, Zhou XH. Medical information spillovers and health care choice of Chinese residents in the Internet era: an empirical research based on CHNS (in Chinese). J Public Management. 2017;14(4):78–90.
34. Guindon GE, Fatima T, Garasia S, et al. A systematic umbrella review of the association of prescription drug insurance and cost-sharing with drug use, health services use, and health. BMC Health Services Res. 2022;22(1):1–33. doi:10.1186/s12913-022-07554-w
35. Jakovljevic M, Wang L, Adhikari C. Asian health sector growth in the next decade—Optimism despite challenges ahead. Front Public Health. 2023;11:1150917. doi:10.3389/fpubh.2023.1150917
36. Timofeyev Y, Dremova O, Jakovljevic M. The impact of transparency constraints on the efficiency of the Russian healthcare system: systematic literature review. J Med Economics. 2023;26(1):95–109. doi:10.1080/13696998.2022.2160608
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.