Back to Journals » International Journal of Women's Health » Volume 18
Bidirectional and Multivariable Mendelian Randomization Study of PCOS and VTE
Authors You L, Cui H, Zhao F, Huang H, Xu W
Received 2 December 2025
Accepted for publication 9 February 2026
Published 28 March 2026 Volume 2026:18 586045
DOI https://doi.org/10.2147/IJWH.S586045
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Lifang You,1,* Hongyin Cui,1,* Fen Zhao,1 Hairong Huang,2 Wenxuan Xu1
1Department of Gynecology and Obstetrics, First People’s Hospital of Linping District, Hangzhou, 311100, People’s Republic of China; 2Department of Gynecology, Yunhe Branch of the First People’s Hospital of Linping District, Hangzhou, 311102, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lifang You, Email [email protected]
Background: We used bidirectional and multivariable Mendelian randomization (MR) to test whether polycystic ovary syndrome (PCOS) is causally related to venous thromboembolism (VTE).
Methods: Using European-ancestry GWAS summary statistics, we performed bidirectional two-sample univariable MR and multivariable MR adjusting for diabetes, body mass index (BMI), hormone replacement therapy, and oral contraceptive use. Robustness was assessed with Cochran’s Q, MR-Egger intercept, MR-PRESSO, and leave-one-out analyses.
Results: Univariable MR showed no causal effect of PCOS on VTE (IVW OR 1.008, 95% CI 0.974– 1.042; p = 0.653), and reverse-direction MR provided no evidence that VTE causally influences PCOS. In multivariable MR, PCOS remained not associated with VTE (IVW OR 1.016, 95% CI 0.987– 1.045; p = 0.285), whereas BMI had a clear independent positive effect on VTE risk (IVW OR 1.358, 95% CI 1.262– 1.461; p < 0.001).
Conclusion: Genetic evidence does not support a causal relationship between PCOS and VTE. BMI is independently associated with VTE risk and appears to be a key determinant of VTE risk.
Keywords: polycystic ovary syndrome, venous thromboembolism, mendelian randomization, body mass index, genetic epidemiology, multivariable analysis
Background
Polycystic ovary syndrome (PCOS) is a common endocrine and metabolic disorder in women of reproductive age and is closely linked to obesity and insulin resistance.1–4 In European populations, prevalence estimates vary substantially across studies, largely reflecting differences in diagnostic criteria (eg, NIH vs Rotterdam/ESHRE ASRM) and ascertainment strategies.5,6 Venous thromboembolism (VTE) is a major, preventable vascular event.7 Observational studies have reported an association between PCOS and VTE,8,9 but interpretation is complicated by shared risk factors such as higher BMI and hormonal exposures, as well as residual confounding and potential reverse causation.8–13
Mendelian randomization (MR) uses genetic variants as instrumental variables to strengthen causal inference. Bidirectional and multivariable MR can further assess directionality and estimate direct effects while accounting for correlated risk factors.13–15 In this study, we used European ancestry genome-wide association summary statistics to conduct bidirectional two-sample and multivariable MR analyses to evaluate the causal relationship between PCOS and VTE and to determine whether any association persists after accounting for BMI, diabetes, and hormone related exposures.
Methods
Study Design
We conducted a bidirectional two-sample MR study to assess the causal relationship between PCOS and VTE. We performed univariable MR (UVMR) as the primary analysis and multivariable MR (MVMR) to estimate the independent effect of PCOS on VTE while jointly adjusting for major risk factors, including diabetes, body mass index (BMI), hormone replacement therapy (HRT) use, and oral contraceptive (OC) use. MR analyses relied on three core assumptions: (1) a robust association between exposure and the selected single nucleotide polymorphisms (SNPs); (2) independence of instrumental variables (IVs) from confounders; and (3) IVs influence outcomes solely via the exposure. Figure 1 presents the study workflow.
 |
Figure 1 Overview of the present Mendelian randomization study. (1) relevance, genetic variants are associated with the exposure; (2) Independence, genetic variants are not associated with confounders; (3) exclusion restriction, genetic variants affect the outcome only through the exposure, with no direct or pleiotropic pathway. The cross (×) denotes an assumed absent association or pathway, and the question mark (?) denotes the hypothesized and uncertain causal direction tested in the bidirectional analysis between PCOS and VTE. |
Data Sources
Data were extracted from publicly available GWAS datasets. PCOS data were sourced from the 2021 FinnGen project (finn-b-E4_PCOS; 642 cases, 118,228 controls). Diabetes data originated from the EBI database (ebi-a-GCST90038633; 24,659 cases, 459,939 controls, 2021). BMI, HRT, and oral contraceptive use data were drawn from the 2018 UK Biobank (ukb-b-19953, n=461,460; ukb-b-18541, 97,920 cases, 152,381 controls; ukb-b-9509, 205,516 cases, 44,924 controls, respectively). VTE summary statistics were also derived from FinnGen (finn-b-I9_VTE, 9,176 cases, 209,616 controls, 2021). All participants were of European descent. As all summary-level data were collected from previously published, open-access studies, neither additional ethical approval nor informed consent was required. Per China’s Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects (Feb 18, 2023), Article 32 (1)–(2), this study using publicly available, de-identified summary data is exempt from ethics review. The GWAS sources, IDs, ancestry, and sample sizes (cases/controls where applicable) are summarized in Table S1.
Instrumental Variable Selection
P-value thresholds. SNPs associated with PCOS, diabetes, BMI, and HRT were selected as instrumental variables at genome-wide significance (p < 5 × 10−8). For ever use of OCs, the threshold was relaxed to p < 5 × 10−7 due to the lack of genome-wide significant variants at p < 5 × 10−8.
LD clumping. To ensure independence, SNPs were clumped using linkage disequilibrium (LD) criteria of r2 < 0.001 within a 10,000-kb window, retaining the variant with the lowest p-value in each LD block.
Instrument strength. Instrument strength was assessed using F-statistics, and weak instruments were excluded (F < 10).
Harmonization
We harmonized exposure and outcome summary statistics to ensure consistent effect allele orientation. (1) Effect alleles were aligned across datasets. (2) SNPs requiring strand flipping were recoded so that the estimated effects corresponded to the same allele. (3) Palindromic SNPs (A/T or C/G) with ambiguous strand orientation were excluded to avoid misalignment. (4) SNPs with non-matching alleles or incomplete information were removed before downstream MR analyses.
Univariable Mendelian Randomization
A two-sample MR framework was implemented to assess the effect of PCOS on VTE. We applied five estimators: inverse-variance weighted (IVW, primary), MR-Egger, weighted median, simple mode, and weighted mode. The IVW estimator provides the most precise estimate when all instruments are valid (or when any horizontal pleiotropy is balanced). MR-Egger allows for directional pleiotropy under the InSIDE assumption, with a non-zero intercept indicating average pleiotropic effects. The weighted median estimator yields a consistent estimate if at least 50% of the total instrument weight comes from valid variants. Mode-based estimators (simple and weighted mode) are consistent when the largest cluster of SNP-specific causal estimates corresponds to valid instruments. Results were reported as odds ratios (ORs) with 95% confidence intervals (CIs), with p < 0.05 considered statistically significant.
Multivariable Mendelian Randomization
MVMR was performed with PCOS, diabetes, BMI, HRT use, and OC use entered jointly to estimate the direct effect of PCOS on VTE conditional on these covariates. These covariates were pre-specified a priori (Gariani et al).12 because they are established VTE-related factors and are also linked to PCOS, which may induce correlated exposures and alternative pathways affecting VTE.
Sensitivity Analyses
Heterogeneity was assessed using Cochran’s Q (IVW; MR-Egger where applicable). Directional pleiotropy was evaluated by the MR-Egger intercept test. MR-PRESSO was used to perform the global test, identify outliers, and re-estimate effects after outlier removal (including distortion testing). Leave-one-out analyses (IVW) were conducted to evaluate single-SNP influence. Collectively, these sensitivity analyses were used to support the consistency and robustness of causal estimates across MR methods.
Statistical Analysis
All analyses were conducted in R (version 4.3.3) using TwoSampleMR (v0.6.29), MendelianRandomization (v0.10.0), MVMR (v0.4.2), and MR-PRESSO (v1.0). Unless otherwise specified, functions were run with default settings. LD clumping and instrument-selection thresholds followed the prespecified criteria described above (r2 < 0.001, 10,000 kb window; p-value thresholds as stated). For MR-PRESSO, we enabled both the outlier and distortion components (OUTLIERtest = TRUE, DISTORTIONtest = TRUE) with SignifThreshold = 0.05 and NbDistribution = 1000 (default), and a fixed random seed when applicable to ensure reproducibility.
Statistical Power
Given the limited number of PCOS cases in the FinnGen GWAS, statistical power may be reduced for detecting modest causal effects, particularly in MVMR where instruments are partitioned across multiple exposures. Therefore, null findings should be interpreted cautiously as they may reflect limited power rather than absence of a causal effect.
Results
Genetic Variants as Instrumental Variables
Seven SNPs were selected as IVs for PCOS, all with F-statistics > 10 (range: 30.829–116.213). Detailed SNP information is provided in Tables S2 and S3. The GWAS sources and sample sizes for all exposures and outcomes are summarized in Table S1.
Bidirectional Two-Sample Mendelian Randomization Between PCOS and VTE
The comprehensive results of the MR analyses are presented in Table 1. Both fixed-effects and random-effects IVW analyses showed no evidence of a causal effect of PCOS on VTE risk (OR = 1.008, 95% CI: 0.974–1.042, p = 0.653; OR = 1.008, 95% CI: 0.962–1.056, p = 0.745, respectively). Consistent results were observed using MR-Egger, weighted median, simple mode, and weighted mode. Cochran’s Q provided no evidence of heterogeneity (MR-Egger: Q = 6.55, p = 0.256; IVW: Q = 11.360, p = 0.078) (Table 2 and Figure 2). The MR-Egger intercept did not indicate directional pleiotropy (intercept = −0.025, p = 0.113), and MR-PRESSO global test did not indicate horizontal pleiotropy (p = 0.091), and no outliers were identified (Table 2). Leave-one-out analyses suggested that no single SNP disproportionately influenced the IVW estimate. Overall, estimates were directionally consistent across MR methods and supported by sensitivity analyses indicating no material heterogeneity, directional pleiotropy, outliers, or single-variant influence.
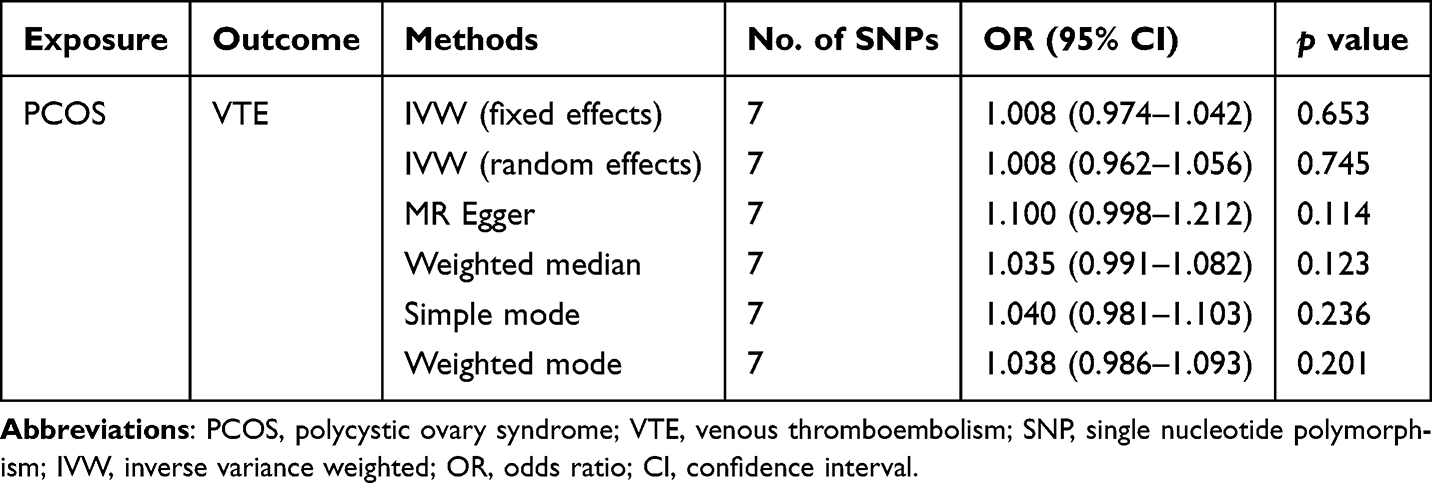 |
Table 1 Results of Mendelian Randomization Analyses Evaluating the Causal Effect of PCOS on VTE Risk |
 |
Table 2 Sensitivity Analyses for Heterogeneity and Pleiotropy in the Mendelian Randomization Study of PCOS and VTE |
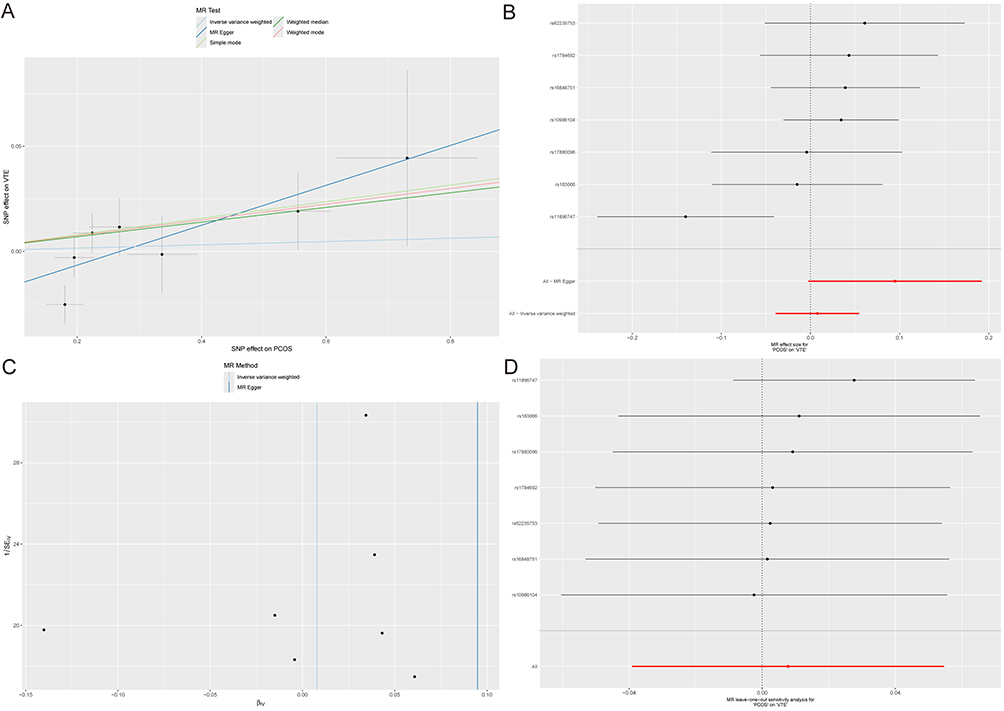 |
Figure 2 Results of Mendelian randomization analyses evaluating the effect of PCOS on VTE: (A) scatter plot, (B) forest plot, (C) funnel plot, and (D) leave-one-out sensitivity analysis. |
Reverse MR Analysis
For the reverse MR analysis assessing the impact of VTE on PCOS risk (excluding palindromic SNP rs2844543), IVW showed no evidence of a causal effect (fixed-effects OR = 0.998, 95% CI: 0.904–1.101, p = 0.962; Table S4 and Figure 3). Heterogeneity and pleiotropy assessments are detailed in Table S5.
 |
Figure 3 Results of Mendelian randomization analyses evaluating the effect of VTE on PCOS: (A) scatter plot, (B) forest plot, (C) funnel plot, and (D) leave-one-out sensitivity analysis. |
Multivariable MR Analysis
Figure 4 summarizes the results of the MVMR estimating associations between PCOS, diabetes, BMI, HRT, oral contraceptive use, and VTE. No significant causal effect of PCOS on VTE was found (IVW: OR = 1.016, 95% CI: 0.987–1.045, p = 0.285). However, a significant association was observed between BMI and VTE (IVW: OR = 1.358, 95% CI: 1.262–1.461, p < 0.001). No significant associations were found for diabetes, HRT, or oral contraceptive use with VTE, with consistent findings across MVMR-Egger, MVMR-Lasso, and MVMR-Median analyses.
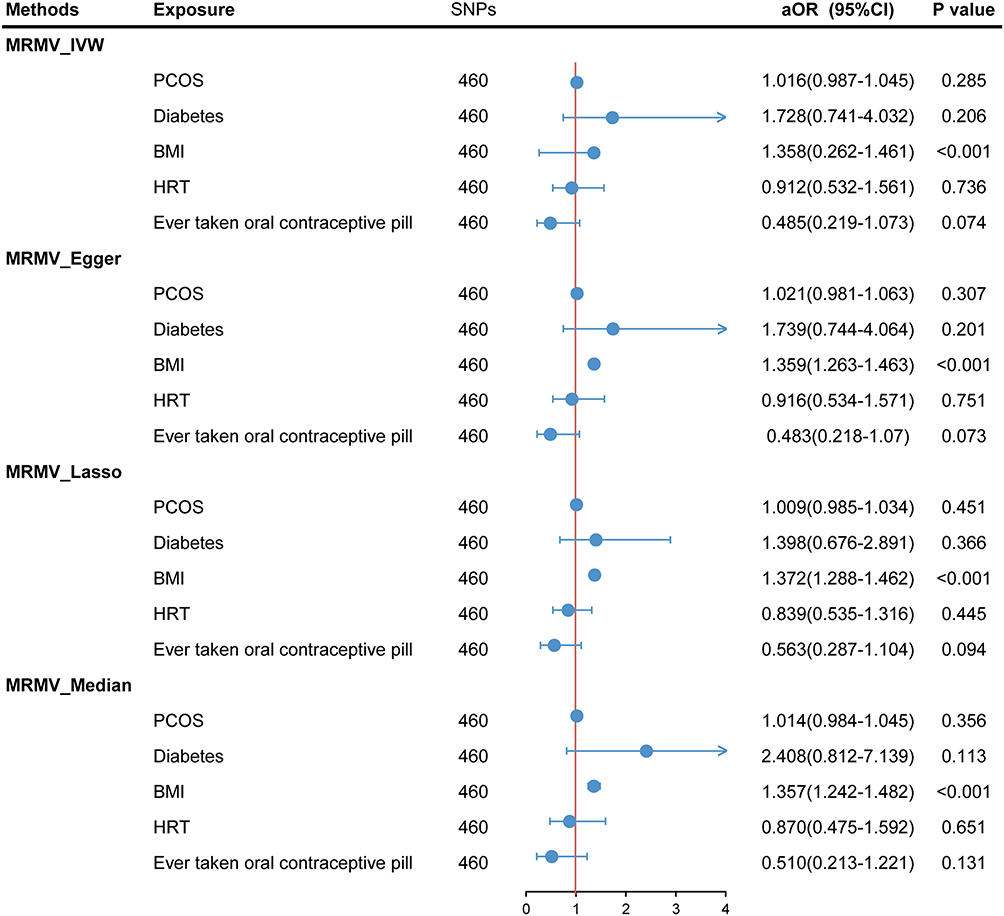 |
Figure 4 Multivariable Mendelian randomization. |
Discussion
In this bidirectional two-sample MR study, with additional multivariable MR analyses, we examined the potential causal relationship between PCOS and VTE. Across univariable MR, reverse-direction MR, and multivariable MR adjusted for major correlated risk factors (BMI, diabetes, HRT use, and OC use), we did not find evidence that genetically predicted PCOS has a direct causal effect on VTE. BMI, however, remained independently associated with higher VTE risk in MVMR.
Our findings differ from several observational studies reporting increased VTE risk among women with PCOS. This difference is plausible.8,9,16 Observational associations may be inflated by residual confounding and selection mechanisms that are difficult to fully address, particularly shared risk factors such as adiposity, insulin resistance or metabolic syndrome, and time-varying hormonal exposures (for example, OC use).10,17,18 Surveillance or diagnostic bias may also play a role, as women with PCOS often have more healthcare contact for reproductive and metabolic concerns, which could increase the likelihood of VTE detection.19 MR uses germline genetic variants as instruments for lifelong liability to the exposure, which helps reduce reverse causation and limits confounding relative to conventional observational designs.13
The association between BMI and VTE observed in our MVMR is consistent with epidemiologic evidence and prior MR studies supporting a causal role of adiposity in VTE.10,20,21 Taken together, the elevated VTE risk reported in PCOS cohorts may largely reflect co-occurring adiposity-related metabolic pathways and residual cardiometabolic confounding rather than a direct effect of PCOS itself. Evidence that modifiable metabolic factors can influence PCOS risk, along with the causal role of adiposity in VTE, is consistent with a model in which cardiometabolic burden contributes to vascular risk among women with PCOS.22–25 This also fits with clinical heterogeneity in insulin resistance across PCOS phenotypes.
From a clinical perspective, our results suggest a practical distinction. We found no evidence for a direct causal effect of PCOS on VTE, while BMI appears to be an independent causal risk factor. VTE prevention in women with PCOS may therefore benefit from focusing on modifiable cardiometabolic risk, particularly adiposity and related metabolic disturbances, rather than using PCOS diagnosis alone for thrombosis risk stratification.24,26 This approach may help identify women with higher adiposity or metabolic burden, in whom absolute VTE risk is more likely to be clinically meaningful.
Several limitations should be noted. First, the PCOS GWAS included a relatively limited number of cases, which may have reduced statistical power, especially for detecting modest effects in MVMR. Second, although sensitivity analyses did not indicate major violations of MR assumptions, horizontal pleiotropy cannot be completely excluded. Third, our analyses were restricted to European-ancestry datasets, which limits generalizability, as PCOS prevalence and metabolic manifestations can vary across populations and may be influenced by diagnostic criteria and ascertainment. Finally, the PCOS summary statistics were based on registry or ICD-defined case status. Detailed phenotyping (for example, Rotterdam A to D) was not available, so we could not conduct phenotype-stratified analyses.
Future work would benefit from larger, ancestry-diverse PCOS GWAS with improved phenotypic resolution, including Rotterdam subtypes and key medication exposures such as hormonal therapies. Pleiotropy-robust approaches, including colocalization and robust MR methods, as well as replication in independent cohorts, will also be important.
Conclusion
This bidirectional and multivariable MR study suggests that PCOS is unlikely to directly increase VTE risk, while higher BMI appears to be a robust independent causal risk factor. These findings support a clinical focus on reducing adiposity-related risk and managing cardiometabolic burden, rather than relying on PCOS diagnosis alone for VTE risk assessment.
Data Sharing Statement
Data analyzed in this study were publicly available from GWAS datasets. More details are shown in the main text.
Ethical Approval and Consent to Participate
As all summary-level data were collected from previously published, open-access studies, neither additional ethical approval nor informed consent was required.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Medical and health research Project of Yuhang District (Grant No.2019007).
Disclosure
Lifang You and Hongyin Cui are co-first authors for this study. The authors declared that they have no conflict of interest.
References
1. Galluzzo A, Amato MC, Giordano C. Insulin resistance and polycystic ovary syndrome. Nutr Metab Cardiovasc Dis. 2008;18(7):511–9. doi:10.1016/j.numecd.2008.05.004
2. Rojas J, Chávez M, Olivar L, et al. Polycystic ovary syndrome, insulin resistance, and obesity: navigating the pathophysiologic labyrinth. Int Reproductive Med. 2014;2014:719050. doi:10.1155/2014/719050
3. Zhao Y, Pang J, Fang X, et al. Causal relationships between modifiable risk factors and polycystic ovary syndrome: a comprehensive Mendelian randomization study. Front Endocrinol. 2024;15:1348368. doi:10.3389/fendo.2024.1348368
4. Gencer G, Serin AN, Gencer K. Analysis of the effect of hashimoto’s thyroiditis and insulin resistance on ovarian volume in patients with polycystic ovary syndrome. BMC Women’s Health. 2023;23(1):86. doi:10.1186/s12905-023-02200-x
5. Chiaffarino F, Cipriani S, Dalmartello M, et al. Prevalence of polycystic ovary syndrome in European countries and USA: a systematic review and meta-analysis. Eur J Obstet Gynecol Reprod Biol. 2022;279:159–170. doi:10.1016/j.ejogrb.2022.10.020
6. Bozdag G, Mumusoglu S, Zengin D, Karabulut E, Yildiz BO. The prevalence and phenotypic features of polycystic ovary syndrome: a systematic review and meta-analysis. Hum Reprod. 2016;31(12):2841–2855. doi:10.1093/humrep/dew218
7. Lancet Haematology T. The Lancet H. Thromboembolism: an under appreciated cause of death. Lancet Haematol. 2015;2(10):e393. doi:10.1016/S2352-3026(15)00202-1
8. Okoroh EM, Hooper WC, Atrash HK, Yusuf HR, Boulet SL. Is polycystic ovary syndrome another risk factor for venous thromboembolism? United States, 2003-2008. Am J Obstet Gynecol. 2012;207(5):377.e371–378. doi:10.1016/j.ajog.2012.08.007
9. Bird ST, Hartzema AG, Brophy JM, Etminan M, Delaney JA. Risk of venous thromboembolism in women with polycystic ovary syndrome: a population-based matched cohort analysis. CMAJ. 2013;185(2):E115–120. doi:10.1503/cmaj.120677
10. Rahmani J, Haghighian Roudsari A, Bawadi H, et al. Relationship between body mass index, risk of venous thromboembolism and pulmonary embolism: a systematic review and dose-response meta-analysis of cohort studies among four million participants. Thrombosis Research. 2020;192:64–72. doi:10.1016/j.thromres.2020.05.014
11. Pfeifer S, Butts S, Dumesic D. Combined hormonal contraception and the risk of venous thromboembolism: a guideline. Fertil Sterility. 2017;107(1):43–51. doi:10.1016/j.fertnstert.2016.09.027
12. Gariani K, Hugon-Rodin J, Philippe J, Righini M, Blondon M. Association between polycystic ovary syndrome and venous thromboembolism: a systematic review and meta-analysis. Thrombosis Research. 2020;185:102–108. doi:10.1016/j.thromres.2019.11.019
13. Davey Smith G, Hemani G. Mendelian randomization: genetic anchors for causal inference in epidemiological studies. Human Molecular Genetics. 2014;23(R1):R89–R98. doi:10.1093/hmg/ddu328
14. Lawlor DA, Harbord RM, Sterne JA, Timpson N, Davey Smith G. Mendelian randomization: using genes as instruments for making causal inferences in epidemiology. Stat Med. 2008;27(8):1133–1163. doi:10.1002/sim.3034
15. Davies NM, Holmes MV, Davey Smith G. Reading Mendelian randomisation studies: a guide, glossary, and checklist for clinicians. BMJ. 2018;362:k601. doi:10.1136/bmj.k601
16. Glintborg D, Ollila -M-M, Koskenkari N, et al. Increased prospective cardiovascular disease risk in 127 517 Nordic women with polycystic ovary syndrome: a national cohort study. European Journal of Endocrinology. 2025;194(1):58–68. doi:10.1093/ejendo/lvaf266
17. Ageno W, Di Minno MN, Ay C, et al. Association between the metabolic syndrome, its individual components, and unprovoked venous thromboembolism: results of a patient-level meta-analysis. Arteriosclerosis Thrombosis Vasc Biol. 2014;34(11):2478–2485. doi:10.1161/ATVBAHA.114.304085
18. Vinogradova Y, Coupland C, Hippisley-Cox J. Use of combined oral contraceptives and risk of venous thromboembolism: nested case-control studies using the QResearch and CPRD databases. BMJ. 2015;350:h2135. doi:10.1136/bmj.h2135
19. Berni TR, Morgan CL, Rees DA. Rising incidence, health resource utilization, and costs of polycystic ovary syndrome in the United Kingdom. J Clin Endocrinol Metab. 2025;110(5):e1580–e1589. doi:10.1210/clinem/dgae518
20. Hotoleanu C. Association between obesity and venous thromboembolism. Med Pharm Rep. 2020;93(2):162–168. doi:10.15386/mpr-1372
21. Ntinopoulou P, Ntinopoulou E, Papathanasiou IV, et al. Obesity as a risk factor for venous thromboembolism recurrence: a systematic review. Medicina. 2022;58(9):1290. doi:10.3390/medicina58091290
22. Day FR, Hinds DA, Tung JY, et al. Causal mechanisms and balancing selection inferred from genetic associations with polycystic ovary syndrome. Nat Commun. 2015;6:8464. doi:10.1038/ncomms9464
23. Brower MA, Hai Y, Jones MR, et al. Bidirectional Mendelian randomization to explore the causal relationships between body mass index and polycystic ovary syndrome. Hum Reprod. 2019;34(1):127–136. doi:10.1093/humrep/dey343
24. Lindström S, Germain M, Crous-Bou M, et al. Assessing the causal relationship between obesity and venous thromboembolism through a Mendelian Randomization study. Hum Genet. 2017;136(7):897–902. doi:10.1007/s00439-017-1811-x
25. Tay CT, Mousa A, Vyas A, Pattuwage L, Tehrani FR, Teede H. International evidence-based polycystic ovary syndrome guideline update: insights from a systematic review and meta-analysis on elevated clinical cardiovascular disease in polycystic ovary syndrome. J the Am Heart Association. 2024;13(16):e033572. doi:10.1161/JAHA.123.033572
26. Teede HJ, Tay CT, Laven JJE, et al. Recommendations from the 2023 international evidence-based guideline for the assessment and management of polycystic ovary syndrome. J Clin Endocrinol Metab. 2023;108(10):2447–2469. doi:10.1210/clinem/dgad463
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Causal Association Between Diabetes, Body Mass Index and Lichen Sclerosus: A Bidirectional Two-Sample Mendelian Randomization Analysis
Liu L, Zhang Q, Chang J, Yang K
Clinical, Cosmetic and Investigational Dermatology 2024, 17:931-940
Published Date: 26 April 2024
Causal Effects of Immune Cells on Reproductive Ill-Health, Including Abnormal Spermatozoa, Polycystic Ovary Syndrome and Spontaneous Abortion: Mendelian Randomization Analyses
Chen S, Sun S, Zhou Z, Zhou Z, Zhang R, Song W, Xin H, Yang Q, Dai S, Huang K, Niu W, Shi H, Guo Y
Journal of Multidisciplinary Healthcare 2025, 18:3219-3232
Published Date: 6 June 2025
Beyond BMI: A Mendelian Randomization Study of the Causal Effects and Mediating Pathways of Regional Adipose Tissue Depots on Polycystic Ovary Syndrome
Yang J, Zhang X, Zhang H, Guo X, Ren F, Dong C
International Journal of Women's Health 2025, 17:3279-3291
Published Date: 25 September 2025
Identification of the Shared Gene Signatures and Pathways Between Polycystic Ovary Syndrome and Endometrial Cancer Using Bioinformatics and Mendelian Randomization Analyses
Ye D, Yu Y, Xu C, Fu Z, Zhong F, Shen H
International Journal of Women's Health 2025, 17:5669-5687
Published Date: 26 December 2025
East Asian Mendelian-Randomization Evidence Linking PCOS to Gestational Diabetes Mellitus
Du J, Xing L, Chen Y, He Z, Zhong L, Zhao R
International Journal of Women's Health 2026, 18:559022
Published Date: 22 January 2026