")
Back to Journals » Drug Design, Development and Therapy » Volume 17
Bictegravir/Emtricitabine/Tenofovir Alafenamide Treatment: Efficacy and Tolerability in Clinical Practice
Authors Canetti D , Galli L , Lolatto R, Nozza S, Spagnuolo V , Muccini C, Trentacapilli B, Bruzzesi E, Ranzenigo M, Chiurlo M , Castagna A, Gianotti N
Received 18 September 2023
Accepted for publication 11 November 2023
Published 8 December 2023 Volume 2023:17 Pages 3697—3706
DOI https://doi.org/10.2147/DDDT.S437043
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Diana Canetti,1 Laura Galli,1 Riccardo Lolatto,1 Silvia Nozza,2 Vincenzo Spagnuolo,1 Camilla Muccini,1 Benedetta Trentacapilli,2 Elena Bruzzesi,2 Martina Ranzenigo,2 Matteo Chiurlo,2 Antonella Castagna,1,2 Nicola Gianotti1
1Infectious Diseases Unit, San Raffaele Scientific Institute, Milan, Italy; 2Infectious Diseases Unit, Vita Salute San Raffaele University, Milan, Italy
Correspondence: Diana Canetti, Infectious Diseases Unit San Raffaele Scientific Institute, Via Stamira D’Ancona 20, Milano, 20127, Italy, Tel +390226432461, Fax +390226437943, Email [email protected]
Objective: Analysis of bictegravir/emtricitabine/tenofovir alafenamide (BFTAF) efficacy and safety in virologically suppressed people living with HIV (PLWH) in clinical practice.
Patients and methods: The retrospective cohort study, which included adult treatment-experienced and virologically suppressed PLWH, switched to BFTAF from June 2019 to June 2021. Efficacy and safety were evaluated as virological failure (VF=2 consecutive HIV-RNA> 50 copies/mL or a single HIV-RNA> 400 copies/mL) and treatment failure (TF=VF or discontinuation for any reason) until data freezing (August 2022).
Results: Of the 1040 PLWH included, 67.8% switched from elvitegravir/cobicistat/FTAF. VF occurred in 4.2% (n=44), with incidence rate of 1.63 per 1000 person-months of follow-up (PMFU) and probability at 24– 30 months of 3.8%– 4.0%, respectively. Out of the 44 VF, in 75% virological re-suppression was achieved while maintaining BFTAF. Discontinuation occurred in 15% after a median time of 13.5 months of follow-up, with an incidence rate of 5.67 per 1000 PMFU, and a probability at 24– 30 months of 11.9%– 15.3%, respectively. Main discontinuation reasons were simplification (51.3%) and toxicity (21.8%, involving CNS in half of cases). TF occurred in 18.6% with an incidence rate of 7.01 per 1000 PMFU after a median time of 13.6 observation months; probability at 24– 30 months was 14.8%– 18.4%, respectively.
Conclusion: BFTAF has proven effective and well tolerated in clinical practice.
Plain Language Summary: In Clinical Randomized Trials, BFTAF proved to have a high genetic barrier regimen.
In this context of clinical practice:BFTAF proved effective and well toleratedIt showed a low rate of virological failureDiscontinuation was largely influenced by simplification with 2-drug regimens.
Keywords: bictegravir, people living with HIV, PLWH, efficacy, safety, clinical practice
Introduction
A fixed combination of bictegravir/emtricitabine/tenofovir alafenamide (BFTAF, Biktarvy®), an HIV integrase strand transfer inhibitor (InSTI) associated with two nucleoside reverse transcriptase inhibitors, has been available in Italy since June 2019 for the treatment of people living with HIV infection (PLWH).1
It represents a complete single-tablet antiretroviral therapy (ART) to be taken every 24 hr, both with food and on an empty stomach, which presents very few drug interactions and a high barrier to the selection of drug-resistant viral variants.2
BFTAF has proven to be very effective and well tolerated, both in antiretroviral-naive PLWH3–5 and in treatment-experienced ones,6–8 even in conditions of frailty due to co-morbidities.9
Based on these features, BFTAF appears as an attractive oral therapeutic regimen in terms of efficacy, tolerability, and ease of use.
Since its availability in our hospital pharmacy, it was planned to replace all regimens consisting of elvitegravir/cobicistat/emtricitabine/tenofovir alafenamide (ECFTAF) with BFTAF, depending upon several advantages in terms of safety, pharmacokinetics, antiviral activity, and pharmacoeconomics.10 In addition, BFTAF was prescribed according to a case-by-case clinical opinion, in other PLWH with a current regimen other than ECFTAF.
The aim of this study is to describe the efficacy and tolerability of BFTAF in PLWH virologically suppressed, while exposed to other antiretroviral regimens, in a context of clinical practice.
Methods
A retrospective cohort study was conducted in adult PLWH on antiretroviral therapy and HIV-RNA <50 copies/mL, who switched to BFTAF to replace the current regimen, from June 2019 to June 2021. To be included in the analysis, they had to have at least an HIV-RNA determination (PCR Cobas® HIV-1 test 6800 Systems, Roche Diagnostics) after the introduction of BFTAF. A validated in-house method was used to identify resistance-associated mutations (RAMs), as previously described by our group.11 GRT on plasma HIV-RNA and PBMC HIV-DNA was interpreted according to the Stanford University HIV Drug Resistance Database version 9.0 (hivdb.stanford.edu/hivdb/by-sequences/, last updated on 22 June 2023).
Virological failure (VF) was defined as two consecutive HIV-RNA values >50 copies/mL or a single HIV-RNA value >400 copies/mL. Treatment failure (TF) is defined as the occurrence of virological failure or discontinuation of BFTAF for any reason.
Follow-up accrued from the start of BFTAF (baseline) up to the stop of any drug in the regimen or lost to follow-up or data freezing (31 August 2022).
Data are reported as medians (first-third quartile). The incidence rate of VF or TF was calculated as number of VF or TF events per 1000 person-months of follow-up (PMFU). The cumulative probabilities (95% confidence interval, CI) of VF or TF were estimated using Kaplan–Meier curves; the Log rank test was used to compare survival curves. Univariate mixed linear models (MLM) with random slope and intercept for each patient were fitted to estimate mean changes in laboratory parameters (CD4+ lymphocytes, CD4+/CD8+ ratio, haemoglobin, neutrophil granulocytes, creatinine and estimated glomerular filtration rate, glucose, total cholesterol, HDL, LDL, FIB-4) since baseline. Slopes were reported with the corresponding 95% confidence interval. All analyses were conducted using SAS statistical software version 9.4 (Statistical Analyses System Inc, Cary, NC, USA).
Individuals provided written informed consent on the use of their data in scientific analyses and to be included in the Centro San Luigi (CSL) HIV Cohort. The CSL-HIV Cohort was approved by the Ethics Committee of the IRCCS San Raffaele Scientific Institute (Milan, Italy; date of approval 4 December 2017, protocol n. 34).
The authors declare that the procedures were followed according to the regulations established by the Clinical Research and Ethics Committee and to the Helsinki Declaration.
Results
Overall, 1040 patients who met the above-mentioned inclusion criteria were considered in the analysis (flowchart of data extraction in Figure 1).
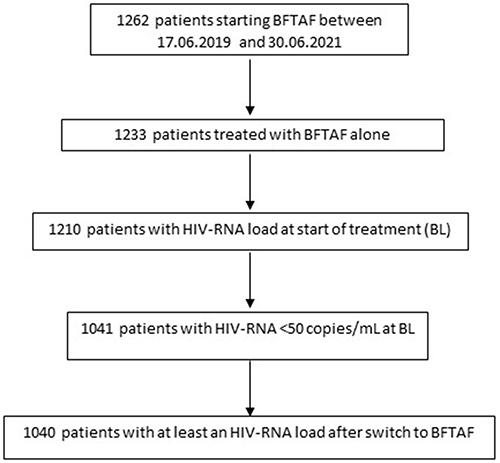 |
Figure 1 Flowchart of data extraction. |
Males represented 82.1% of the study population. At the beginning of BFTAF treatment, the median age (Q1-Q3) was 51.1 (42–57.1) years; patients had a known HIV infection lasting 13.8 (6.8–23.4) years and were on ART for 10.2 (5.1–19.7) years; nadir CD4+ lymphocyte count was 291 (166–447) cells/µL, while their current CD4+ count was 718 (535–941) cells/µL; an AIDS diagnosis was present in 181 subjects (17.4%) and a history of HCV co-infection in 212 (20.4%).
Of these 1040, 705 (67.8%) were taking ECFTAF, while 335 (32.2%) were on a different regimen. Of those on a regimen other than ECFTAF, 194 (59.9%) were on a three-drug integrase inhibitor-based regimen other than elvitegravir, 56 (16.7%) on a protease inhibitor-based regimen, 38 (11.7%) on a non-nucleoside reverse transcriptase inhibitor-based regimen, and 47 (14%) were taking a regimen that cannot be classified among the previous ones, including mono-and dual-therapies and study-protocol regimens. Among 335 patients not treated with ECFTAF, the switch to BFTAF was motivated by simplification (lower drug burden, lower pill burden, no food requirement, fewer potential adverse effects, and/or potential drug–drug interactions) in 236 cases (70.4%), toxicity in 26 (7.8%), and by a miscellany of different reasons in 73 cases (21.8%), such as presence of drug–drug interactions, concern of co-morbidities, exit from clinical studies, patient’s request.
Further details on the characteristics of the individuals included in the analysis are shown in Table 1.
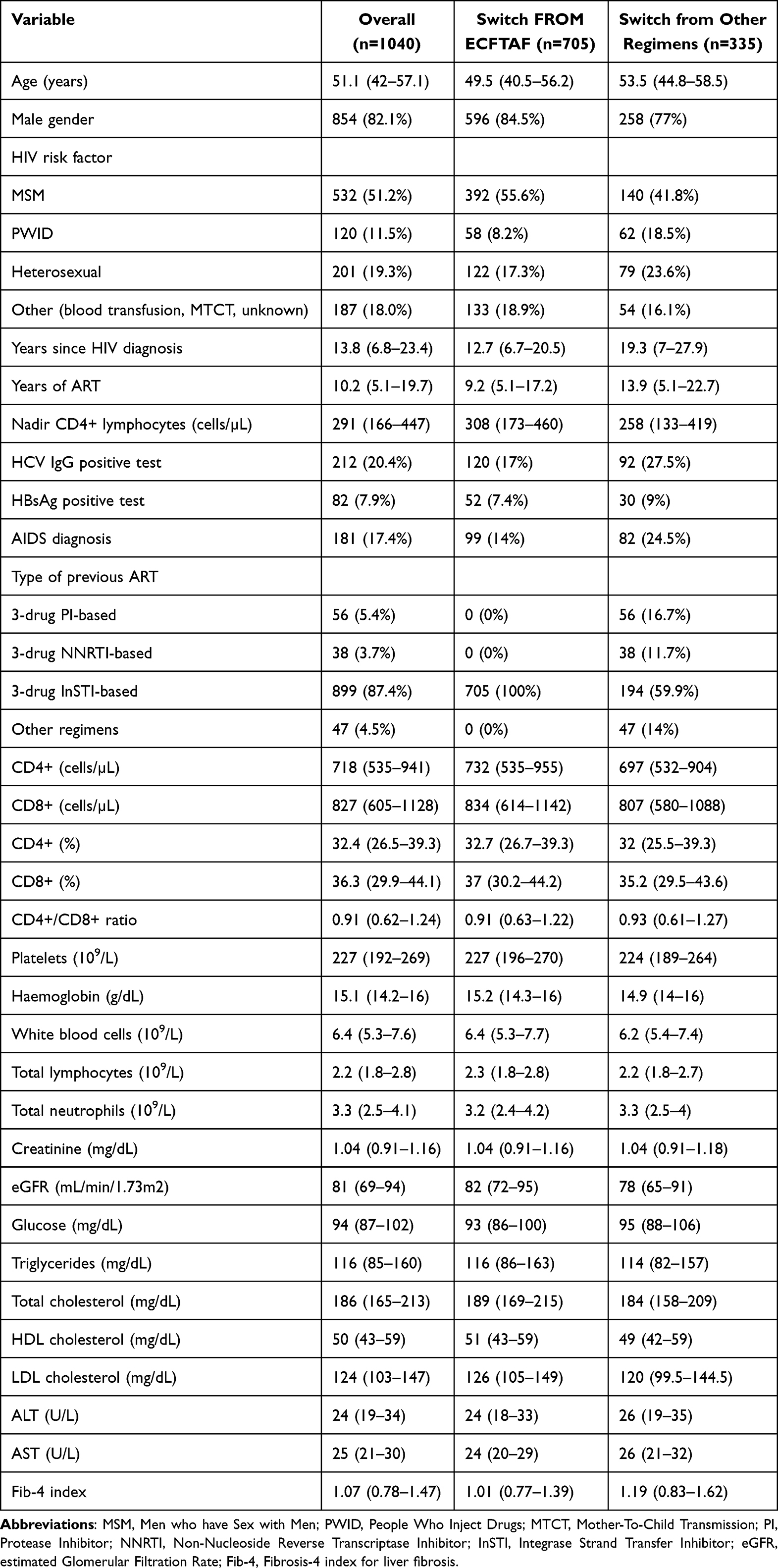 |
Table 1 Characteristics of Patients Included in the Analysis at the Time of BFTAF Treatment Initiation |
The overall median follow-up was of 29.7 (24.4–32.3) months, for a total of 27,536 PMFU. The median follow-up was of 30.5 (26.7–32.7) months with 19,352 PMFU among people who switched from an ECFTAF regimen and of 27.8 (19.1–30.8) months with 8,183 PMFU among people from another regimens.
Overall, VF occurred in 44 (4.2%) patients, with an incidence rate of 1.63 (95% CI 1.16–2.11) per 1000 PMFU; this event occurred after a median of 12.8 (5.8–22.8) months of observation. Median HIV-RNA values at failure were 246 (68–12,025) copies/mL, with 23 cases satisfying the finding of two consecutive HIV-RNA values >50 copies/mL, and 21 corresponding to the criterion of a single HIV-RNA value >400 copies/mL.
The probability of VF at 12, 24 and 30 months was 2.1% (95% CI 1.4–3.3%), 3.8% (95% CI 2.7–5.2%), and 4.0% (95% CI 2.9–5.5%), respectively. The estimate up to 30 months of the probability of VF is illustrated in Figure 2.
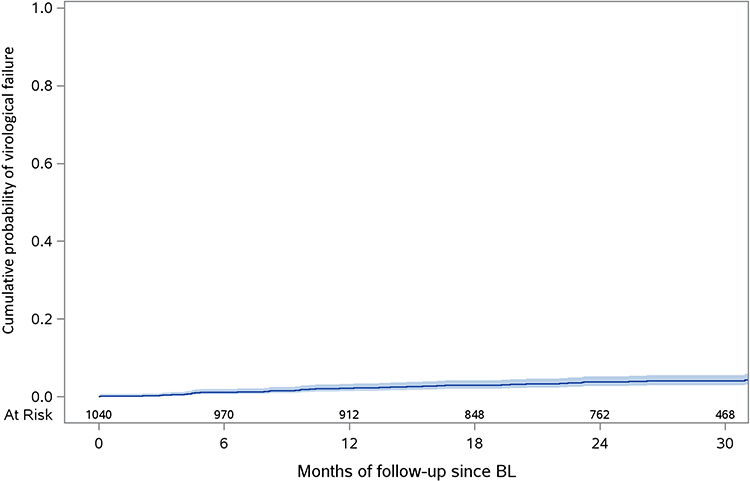 |
Figure 2 Probability of virological failure, Kaplan–Meier curve. |
No statistically significant differences were observed in the probability of VF between patients whose prior regimen was ECFTAF and those who were on a regimen other than ECFTAF at the time of initiating BFTAF.
Mainly due to the low values of viremia at VF, genotypic resistance tests (GRTs) were able to evaluate the drug resistance at VF only in five patients: none selected variants resistant to integrase inhibitors and no new mutations emerged in any case (Table 2).
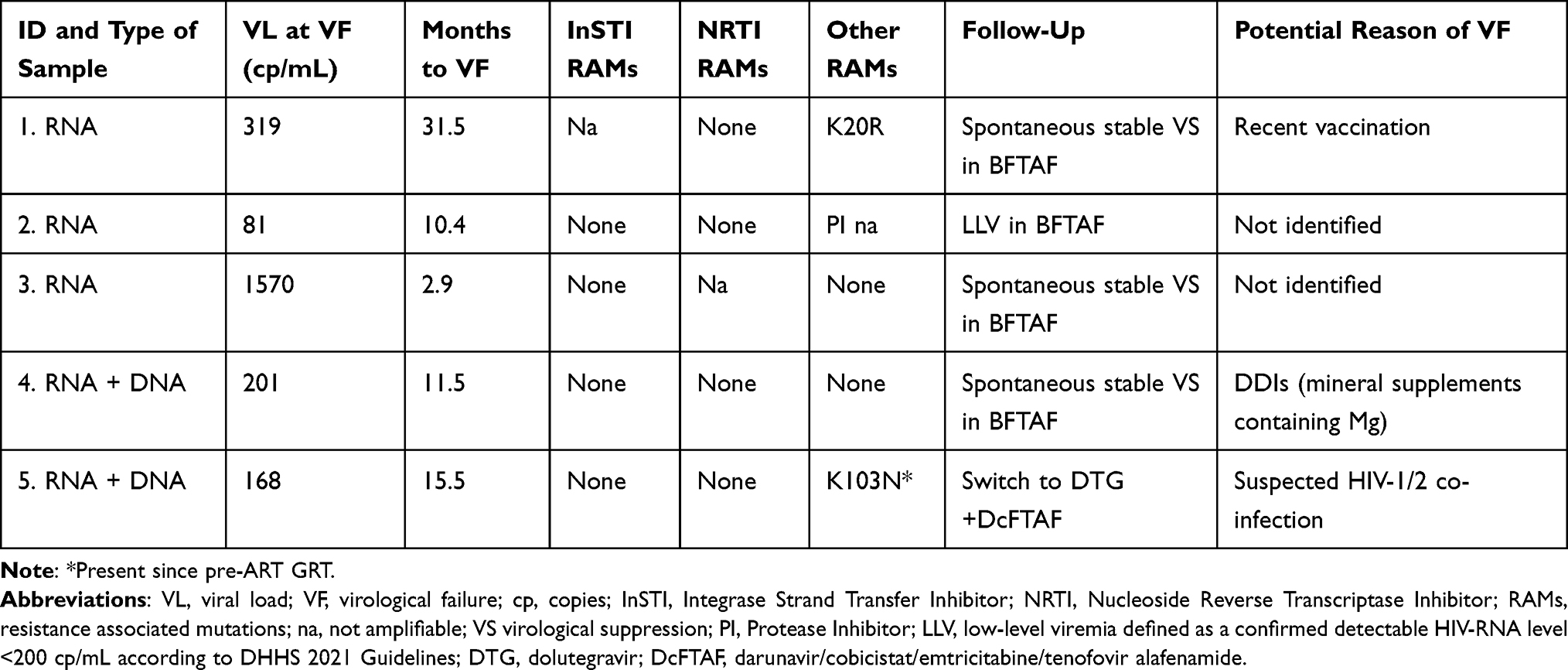 |
Table 2 Results of Genotypic Resistance Tests (GRTs) Available on Partially or Completely Amplifiable Samples |
Out of the 44 documented VF, in 33 cases (75%) BFTAF was successfully maintained with spontaneous virological re-suppression in at least two subsequent HIV-RNA determinations (data not shown). In a case-by-case revision, those HIV-RNA blips were attributable to self-reported transient non adherence (13/33 cases), intercurrent illnesses such as high or low respiratory tract infections, diarrhoea and vomiting, urinary tract infection and others (5/33 cases), drug–drug interactions (2/33 cases), recent vaccine administration (1/33 cases), and no evident explanation in the remaining 12 cases. Five patients who developed VF were switched to another regimen: darunavir/cobicistat/FTAF (DcFTAF) in two cases, dolutegravir (DTG) plus FTAF, DTG plus DcFTAF and rilpivirine (RPV)/FTAF in the other three cases, with virological suppression (3/5) or recurrent blips/low-level viremia (2/5). GRTs were fully amplifiable only in one case and resulted in susceptibility to all NRTIs, InSTIs, and PIs; in another case, switched to DcFTAF, GRTs were performed but analysis was feasible only for PIs, with full susceptibility. Finally, 6 PLWH with evidence of VF were lost at follow-up. Finally, 6 PLWH with evidence of VF were lost at follow-up.
BFTAF discontinuation occurred in 156 (15%) of patients after a median of 13.5 (6.8–23.4) months of follow-up; the incidence rate of regimen discontinuation was 5.67 (95% CI 4.78–6.55) per 1000 PMFU. The probability of discontinuation at 12, 24 and 30 months was 6.4% (95% CI 5.1–8.1%), 11.9% (95% CI 10–14%), and 15.3% (95% CI 13.2%-17.8), respectively. The estimate of the probability of discontinuation up to 30 months is illustrated in Figure 3.
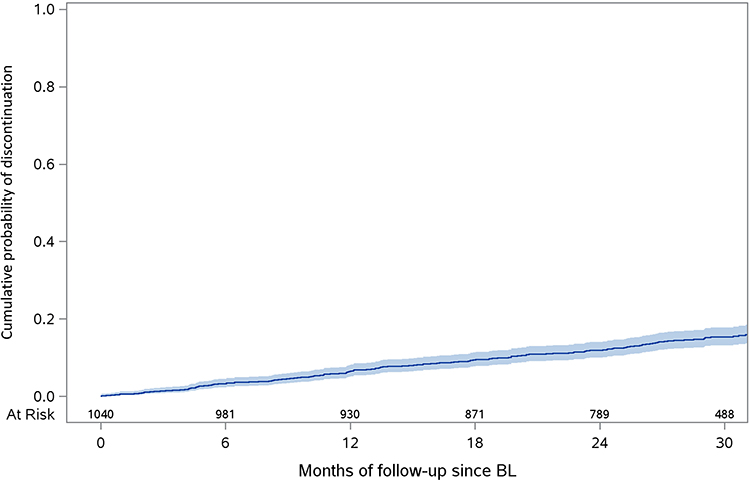 |
Figure 3 Probability of discontinuing BFTAF, Kaplan–Meier curve. |
No statistically significant differences were observed in the likelihood of discontinuing BFTAF between patients whose prior regimen was ECFTAF and those who were on a regimen other than ECFTAF at the time of initiating BFTAF.
The discontinuation of BFTAF occurred due to simplification to a regimen with a lower drug burden in 70 (44.9%) patients, due to simplification for other reasons in 10 patients (6.4%), due to central nervous system toxicity in 14 (9%) and due to other types of toxicity in 20 (12.8%), due to enrolment in clinical trials in 8 (5.1%), due to switch during pregnancy in 3 cases (1.9%), due to suspected weight gain in 2 (1.3%) and to drug–drug interactions in 2 cases (1.3%); then, as already mentioned, the reason for discontinuation was VF in 5 cases (3.2%), death in 8 cases (5.1%) and a miscellanea of other reasons including patient’s wish in 14 cases (9%).
TF occurred in 193 (18.6%) patients, with an incidence rate of 7.01 (95% CI 6.02–8) per 1000 PMFU, after a median of 13.6 (7.1–23.4) months of observation.
The probability of TF at 12, 24 and 30 months was 8.2% (95% CI 6.7–10.1%), 14.8% (95% CI 12.7–17.2%), and 18.4% (95% CI 16.0–21.0%), respectively. The estimate of the probability of outage up to 30 months is illustrated in Figure 4.
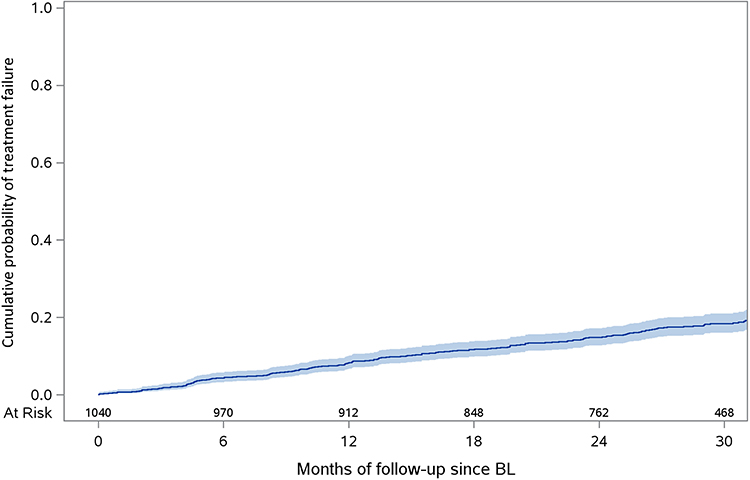 |
Figure 4 Probability of treatment failure, Kaplan–Meier curve. |
There were not statistically significant differences in the probability of TF between patients whose prior regimen was ECFTAF and those who were on a regimen other than ECFTAF at the time of initiating BFTAF. During the follow-up, statistically significant changes were found in CD4+ lymphocytes, CD4+/CD8+ ratio, haemoglobin, neutrophil granulocytes, creatinine and estimated glomerular filtration rate, glucose, total cholesterol, HDL, LDL, FIB-4. No significant changes were observed in CD8+ lymphocytes, nor in the total cholesterol/HDL ratio. Laboratory parameters with a significant monthly increase or decrease over the study period are shown in Table 3. During the observation period 11 (1.1%) patients developed diabetes.
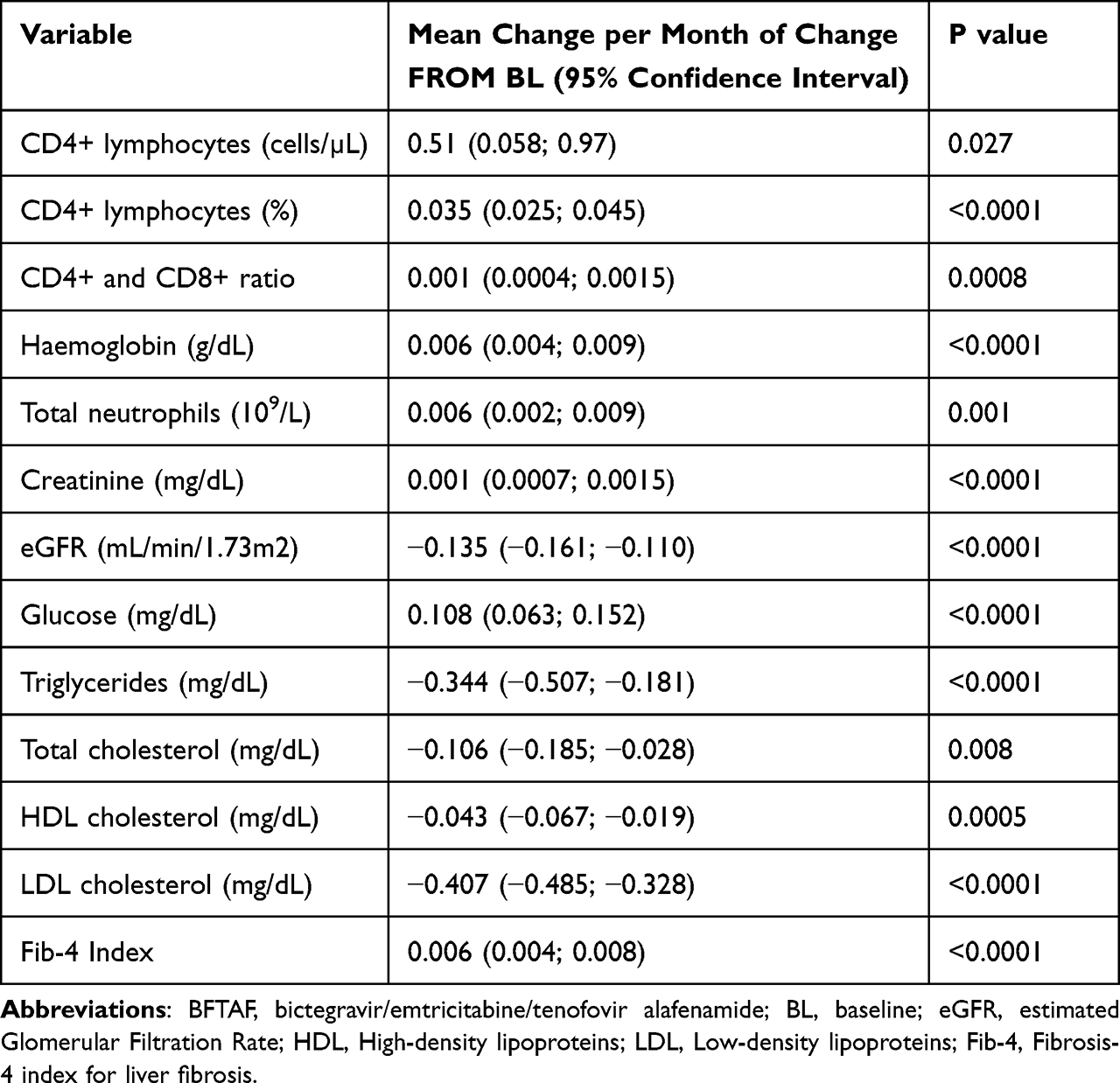 |
Table 3 Monthly Changes of Some Parameters of Interest After Starting BFTAF |
Discussion
After approximately 30 months of follow-up in a daily clinical practice setting, the probability of virological failure or discontinuation of BFTAF for any reason, although higher than those observed in the pivotal clinical trials,3–8 was small and consistent with those observed in observational studies in our country.12,13
Overall, the results of our analysis confirm that BFTAF is an effective and well-tolerated regimen.
Even in the cases of VF reported here, most patients (75%) developed a spontaneous virological control and, when genotypic resistance testing was feasible, there was no evidence of emerging resistance to integrase inhibitors, emtricitabine (or lamivudine), or tenofovir.
It should be emphasized that over half of interruptions occur due to simplification or enrolment in clinical trials, reasons that cannot be classified as clinical failure of the regimen.
In many cases, the suspension of BFTAF was justified by the will to reduce the drug burden, in the absence of signs or symptoms of toxicity. In this regard, it is necessary to highlight that, unlike the registration studies, the population described has a long history of HIV infection (about 14 years) and antiretroviral therapy exposure behind it, which may explain some treatment switches which should probably appear unjustified in patients on first or second-line therapy.
A similar study was recently conducted in Spain;14 performing an intention-to-treat analysis, Ambrosioni et al found that 78% of 1371 patients who switched to BFTAF from another regimen had HIV-RNA <50 copies/mL after 12 months of follow-up. Treatment discontinuation occurred in 3% of cases, and the main cause of discontinuation (69% of cases) was toxicity. Less than 1% of patients experienced virological failure during the 12-month follow-up.
Another real-world setting study was realized in Belgium between January 2019 and September 2020.15 It included 1593 treatment-experienced PLWH, 93.2% of whom maintained virological suppression after 48 weeks; 17 participants (1.1%) experienced viral blips and only a minority (0.7% of overall population including 363 naive-treatment subjects) met the criteria for loss of virological suppression (two consecutive HIV-RNA >200 copies/mL) by week 48. 6.1% (97/1593) discontinued the BFTAF regimen, mainly because of adverse events and then because of switching to dual therapies.
Despite the differences in design, in definition of success parameters and in length of observation period (16 months and 48 weeks, respectively, versus 30 months of our analysis), the three studies run in clinical practice reached similar conclusions with regard to the efficacy and tolerability of BFTAF.
The reported analysis revealed some statistically significant variations in immunological and metabolic parameters, although none of these variations can be considered clinically relevant: a slight increase in the mean change per month from BL of lymphocytes CD4+ percentage, CD4+ and CD8+ ratio, haemoglobin, total neutrophils, creatinine, glucose, and Fib-4 Index, as well as a slight decrease in EGFR, triglycerides, and total cholesterol, LDL, and HDL (Table 3). Pivotal studies in antiretroviral-naive patients have shown a modest worsening of the lipid profile during treatment with BFTAF [3–8]; on the contrary, analyses revealed a trend towards improvement. The difference is probably due to the fact that BFTAF was prescribed in PLWH who were largely already receiving TAF, cobicistat, and sometimes boosted protease inhibitors, differently from what happened in the pivotal studies.6–8
The trend towards a monthly increase in glycemia is quantitatively negligible in terms of clinical relevance. In our cohort, during the period of follow-up, 1% of patients developed diabetes, an incidence that seems to agree with data recently reported in similar groups of PLWH.16 Nevertheless, in an ageing population that is considered at higher risk of metabolic disorders regardless of ART type, it deserves to be kept under observation over time.17
The slight increase in creatinine (with a relatively slight decrease in eGFR) is likely related to the known effect of bictegravir on tubular creatine transport, which does not reflect an actual reduction in glomerular filtration rate.3–9
Only in rare cases, these changes led to precautional discontinuation of BFTAF, not justified by a current clinical condition but because of a concern of not already known long-term adverse events.
This study presents some limitations, such as retrospectivity, the absence of a standardized evaluation of adherence to treatment, and an amount of missing data for some variables. Nevertheless, the real-world setting and the long duration of follow-up, which largely took place during the problematic period of the coronavirus disease 2019 (COVID-19) pandemic, represent its main strength.
Conclusions
In this context of clinical practice, the treatment of HIV infection with a single daily tablet of BFTAF has proven to be effective and well tolerated, with a low rate of virological failure. The rate of discontinuation and of TF was largely influenced by treatment simplification with 2-drug regimens, rather than toxicity.
Funding
Funding for this publication was partially provided by an unconditional grant by Gilead Sciences (Medical Grant n. 15424).
Disclosure
DC has received research grants from Gilead Sciences and GlaxoSmithKline and received payment for educational events and support for attending meetings from Merck Sharp & Dohme and ViiV Healthcare. SN received fee for Advisory Boards and consultations from Gilead Sciences. VS reports grants and/or personal fees from GILEAD SCIENCES, ViiV Healthcare, and MSD, outside the submitted work. AC has received personal fees for advisory boards, speaker panels, and educational materials from Gilead Sciences, ViiV Healthcare, Janssen-Cilag, Merck Sharp & Dohme, and Theratechnologies. NG has been an advisor for Gilead Sciences, Janssen-Cilag, ViiV Healthcare, and Merck Sharp & Dohme and has received speakers’ honoraria from Gilead Sciences, ViiV Healthcare, Janssen-Cilag, and Merck Sharp & Dohme. All other authors declare no competing interests in this work.
References
1. Tsiang M, Jones GS, Goldsmith J, et al. Antiviral activity of bictegravir (GS-9883), a novel potent HIV-1 integrase strand transfer inhibitor with an improved resistance profile. Antimicrob Agents Chemother. 2016;60(12):7086–7097. PMID: 27645238; PMCID: PMC5118987. doi:10.1128/AAC.01474-16
2. Acosta RK, Willkom M, Martin R, et al. Resistance analysis of bictegravir-emtricitabine-tenofovir alafenamide in HIV-1 treatment-naive patients through 48 weeks. Antimicrob Agents Chemother. 2019;63(5):e02533–18. doi:10.1128/AAC.02533-18
3. Wohl DA, Yazdanpanah Y, Baumgarten A, et al. Bictegravir combined with emtricitabine and tenofovir alafenamide versus dolutegravir, Abacavir, and lamivudine for initial treatment of HIV-1 infection: week 96 results from a randomised, double-blind, multicentre, Phase 3, non-inferiority trial. Lancet HIV. 2019;6(6):e355–e363. doi:10.1016/S2352-3018(19)30077-3
4. Stellbrink HJ, Arribas JR, Stephens JL, et al. Co-formulated bictegravir, emtricitabine, and tenofovir alafenamide versus dolutegravir with emtricitabine and tenofovir alafenamide for initial treatment of HIV-1 infection: week 96 results from a randomised, double-blind, multicentre, phase 3, non-inferiority trial. Lancet HIV. 2019;6(6):e364–e372. doi:10.1016/S2352-3018(19)30080-3
5. Orkin C, DeJesus E, Sax PE, et al. Fixed-dose combination bictegravir, emtricitabine, and tenofovir alafenamide versus dolutegravir-containing regimens for initial treatment of HIV-1 infection: week 144 results from two randomised, double-blind, multicentre, phase 3, non-inferiority trials. Lancet HIV. 2020;7(6):e389–e400. doi:10.1016/S2352-3018(20)30099-0
6. Molina JM, Ward D, Brar I, et al. Switching to fixed-dose bictegravir, emtricitabine, and tenofovir alafenamide from dolutegravir plus Abacavir and lamivudine in virologically suppressed adults with HIV-1: 48 week results of a randomised, double-blind, multicentre, active-controlled, phase 3, non-inferiority trial. Lancet HIV. 2018;5(7):e357–e365. doi:10.1016/S2352-3018(18)30092-4
7. Daar ES, DeJesus E, Ruane P, et al. Efficacy and safety of switching to fixed-dose bictegravir, emtricitabine, and tenofovir alafenamide from boosted protease inhibitor-based regimens in virologically suppressed adults with HIV-1: 48 week results of a randomised, open-label, multicentre, phase 3, non-inferiority trial. Lancet HIV. 2018;5(7):e347–e356. doi:10.1016/S2352-3018(18)30091-2
8. Kityo C, Hagins D, Koenig E, et al. Switching to fixed-dose bictegravir, emtricitabine, and tenofovir alafenamide (B/F/TAF) in virologically suppressed HIV-1 infected women: a randomized, open-label, multicenter, active-controlled, phase 3, noninferiority trial. J Acquir Immune Defic Syndr. 2019;82(3):321–328. doi:10.1097/QAI.0000000000002137
9. Maggiolo F, Rizzardini G, Molina JM, et al. Bictegravir/emtricitabine/tenofovir alafenamide in older individuals with HIV: results of a 96-week, phase 3b, open-label, switch trial in virologically suppressed people ≥65 years of age. HIV Med. 2022;24(1):27–36. doi:10.1111/hiv.13319
10. Gallant JE, Thompson M, DeJesus E, et al. Antiviral activity, safety, and pharmacokinetics of bictegravir as 10-day monotherapy in HIV-1-infected adults. J Acquir Immune Defic Syndr. 2017;75(1):61–66. PMID: 28196003; PMCID: PMC5389589. doi:10.1097/QAI.0000000000001306
11. Canetti D, Muccini C, Spagnuolo V, et al. Achieving virological control in pan-resistant HIV-1 infection: a case series. EBioMedicine. 2022;77:103906. PMID: 35255457; PMCID: PMC8897623. doi:10.1016/j.ebiom.2022.103906
12. d’Arminio Monforte A, Cozzi-Lepri A, Di Biagio A, et al. Durability of first-line regimens including integrase strand transfer inhibitors (INSTIs): data from a real-life setting. J Antimicrob Chemother. 2019;74(5):1363–1367. doi:10.1093/jac/dky566
13. Mondi A, Cozzi-Lepri A, Tavelli A, et al. Effectiveness of dolutegravir-based regimens as either first-line or switch antiretroviral therapy: data from the Icona cohort. J Int AIDS Soc. 2019;22(1):e25227. doi:10.1002/jia2.25227
14. Ambrosioni J, Rojas Liévano J, Berrocal L, et al. Real-life experience with bictegravir/emtricitabine/tenofovir alafenamide in a large reference clinical centre. J Antimicrob Chemother. 2022;77(4):1133–1139. doi:10.1093/jac/dkab481
15. Nasreddine R, Florence E, Yombi JC, et al.; Belgian Research on AIDS and HIV Consortium (BREACH). Efficacy, durability, and tolerability of bictegravir/emtricitabine/tenofovir alafenamide for the treatment of HIV in a real-world setting in Belgium. HIV Med. 2023. PMID: 37038245. doi:10.1111/hiv.13493
16. Bratt G, Brännström J, Missalidis C, Nyström T, Andrei G. Development of type 2 diabetes and insulin resistance in people with HIV infection: prevalence, incidence and associated factors. PLoS One. 2021;16(6):e0254079. PMID: 34191847; PMCID: PMC8244855. doi:10.1371/journal.pone.0254079
17. Duncan AD, Goff LM, Peters BS, Remuzzi G. Type 2 diabetes prevalence and its risk factors in HIV: a cross-sectional study. PLoS One. 2018;13(3):e0194199. PMID: 29529066; PMCID: PMC5847234. doi:10.1371/journal.pone.0194199
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.