Back to Journals » Journal of Pain Research » Volume 16
Bibliometric Analysis on Global Analgesia in Labor from 2002 to 2021
Authors Yu K, Ding Z, Yang J ![]() , Han X
, Han X ![]() , Li T, Miao H
, Li T, Miao H ![]()
Received 6 April 2023
Accepted for publication 10 June 2023
Published 14 June 2023 Volume 2023:16 Pages 1999—2013
DOI https://doi.org/10.2147/JPR.S416142
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Robert B. Raffa
Kang Yu,* Zhigang Ding,* Jiaojiao Yang, Xue Han, Tianzuo Li, Huihui Miao
Department of Anesthesiology, Beijing Shijitan Hospital, Capital Medical University, Beijing, 100038, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Huihui Miao, Department of Anesthesiology, Beijing Shijitan Hospital, Capital Medical University, 10th Tieyi Road, Haidian District, Beijing, 100038, People’s Republic of China, Email [email protected]
Background: Maternal pain during labor is one of the most important factors contributing to increased cesarean delivery rates and poor pregnancy outcomes, and this pain can be managed by labor analgesia. Many studies exist on labor analgesia, and the quantity and quality of these studies have not been reported. Therefore, we aimed to perform a bibliometric analysis of studies from 2002 to 2021.
Methods: We used the Web of Science database to obtain publications related to labor analgesia from January 2002 to December 2021. Various bibliographic information was collected, including country; author; journal; grant; discipline; institution and research hotspot. A total of 4536 papers were included.
Results: A total of 4536 articles were included in the study. The country with the most published articles on labor analgesia and the country of the funding agency was the United States. Most articles were published in the disciplines Anesthesiology and Obstetrics & Gynecology. The journal that published the most articles in this category was International Journal of Obstetric Anesthesia. In addition, we found different research hotspots for labor analgesia in the United States, Japan, and China.
Conclusion: This paper provides a bibliometric analysis of research on labor analgesia and highlights the differences in research hotspots for labor analgesia between countries.
Keywords: labor analgesia, bibliometric analysis, hotspots
Introduction
Women in labor suffer prolonged bouts of severe pain during delivery, leading to an increased risk of complications such as postpartum hemorrhage and postpartum depression.1 Labor analgesia, both pharmacologic and non-pharmacologic, can promote, support, and protect natural labor and improve the labor experience.2 Different modes of labor analgesia may also alter the outcome of labor, maternal expectations and preferences for analgesia should be fully respected and supported, and the decision-making model for labor analgesia is often dominated by a healthcare-led paternalistic or informed consent model.2
For a long time, labor analgesia has been performed by a single epidural injection of a large dose of local anesthesia, which produces analgesia and a short operative time after injection.3 Since then, researchers have diverged in their views on labor analgesia techniques and the emergence of epidural catheters, which solved the problem of repeated epidural puncture operations and reduced maternal postoperative complications.
The concept of drugs for epidural blocks has also often changed, and the addition of opioids to the drugs can reduce the concentration of bupivacaine to 0.065%, which can improve the adverse effects on the maternal lower limbs after delivery. In recent years, new levorotatory isomers of local anesthetics, levoropivacaine and levobupivacaine, have been introduced, which may be less cardiotoxic than bupivacaine.4
Remifentanil is a potent, ultra-short-acting opioid with a rapid onset of action and a rapid drug elimination half-life, able to be metabolized 3–5 minutes after discontinuation of the drug.5 Remifentanil has been shown to cause fewer maternal and neonatal postoperative complications than other opioid analgesics.6 Remifentanil can cross the placenta, but some countries believe that it can still be used in obstetric anesthesia because it can be rapidly metabolized in the fetus.
With social concerns, labor analgesia should be taken seriously, and labor pains have been developed in various countries and research findings have been reported. However, few of these articles are currently reported for statistical analysis and generalization of research trends. Bibliometric analysis refers to the quantitative and qualitative analysis of literature using theories and methods of metrology and informatics, and reflects the quantity, quality and influence of literature more systematically by quantifying and analyzing the time of publication, authors, citations, institutions and other factors. A previous bibliometric analysis by Zheng et al analyzed the bibliometric analysis on labor analgesia over the last 30 years,7 and the innovation of our study was to analyze the hotspots of research in three countries, the United States, Japan, and China, and to draw clusters by year for comparison, which was not found in previous studies. We used a bibliometric approach to evaluate 4536 forest articles on labor analgesia published from 2002 to 2021, analyzing the nature of these articles, their content, and their changes with respect to time.
Materials and Methods
Search Strategy
We searched the Web of Science database for all publications on labor analgesia from 2002 to 2021, using the subject term “labor analgesia” and the article type “article review the article type was “article review”. A total of 4536 articles were collected, including their country, author, journal of publication, grant, discipline, and institution. We did not have any exclusion criteria. Two reviewers reviewed the literature for relevant articles independently. We limited the type of paper as article and review which include ‘basic research, clinical trials and case report’, but excluded publications as follows: letter (n = 481), meeting abstract (n = 536), proceeding paper (n = 241), editorial material (n = 239), note (n = 36), correction (n = 19), early access (n = 6), correction, addition (n = 3), retracted publication (n = 2), Biographical-item (n = 1), new item (n =1) and reprint (n =1). We filter the retrieved articles by the process shown in Figure 1.
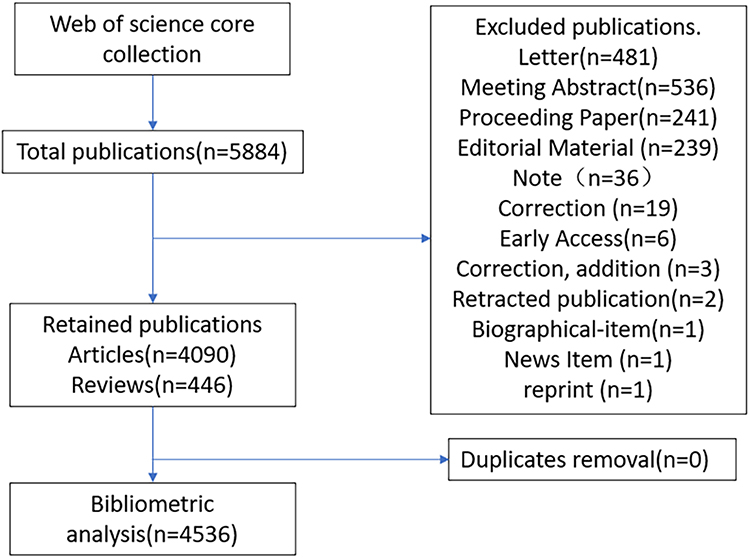 |
Figure 1 Search Flow Chart. |
Statistical Analysis
We used SPSS software (version 22.0; IBM Corporation, Armonk, NY, USA) for statistical analysis. The data were expressed as the mean (range) or number (%). We analyzed categorical variables using aχ2 test and continuous variables with an independent-sample t test. We calculated correlation coefficients (r) and P values using Spearman’s test. A P value of less than 0.05 was considered statistically significant.
Results
Year and Country of Publication
The country with the most published articles on labor analgesia was the United States (n=1375), much higher than the United Kingdom (n=515), which had the second highest number of publications, and Canada (n=296), the third, but the United Kingdom had the highest average citations per article of these three countries, with an average of 30.2 citations per article. The country with the highest average number of citations per article of all countries was Ireland, with an average of 40.94 citations per article, despite only 70 articles being published between 2002 and 2021. See Table 1.
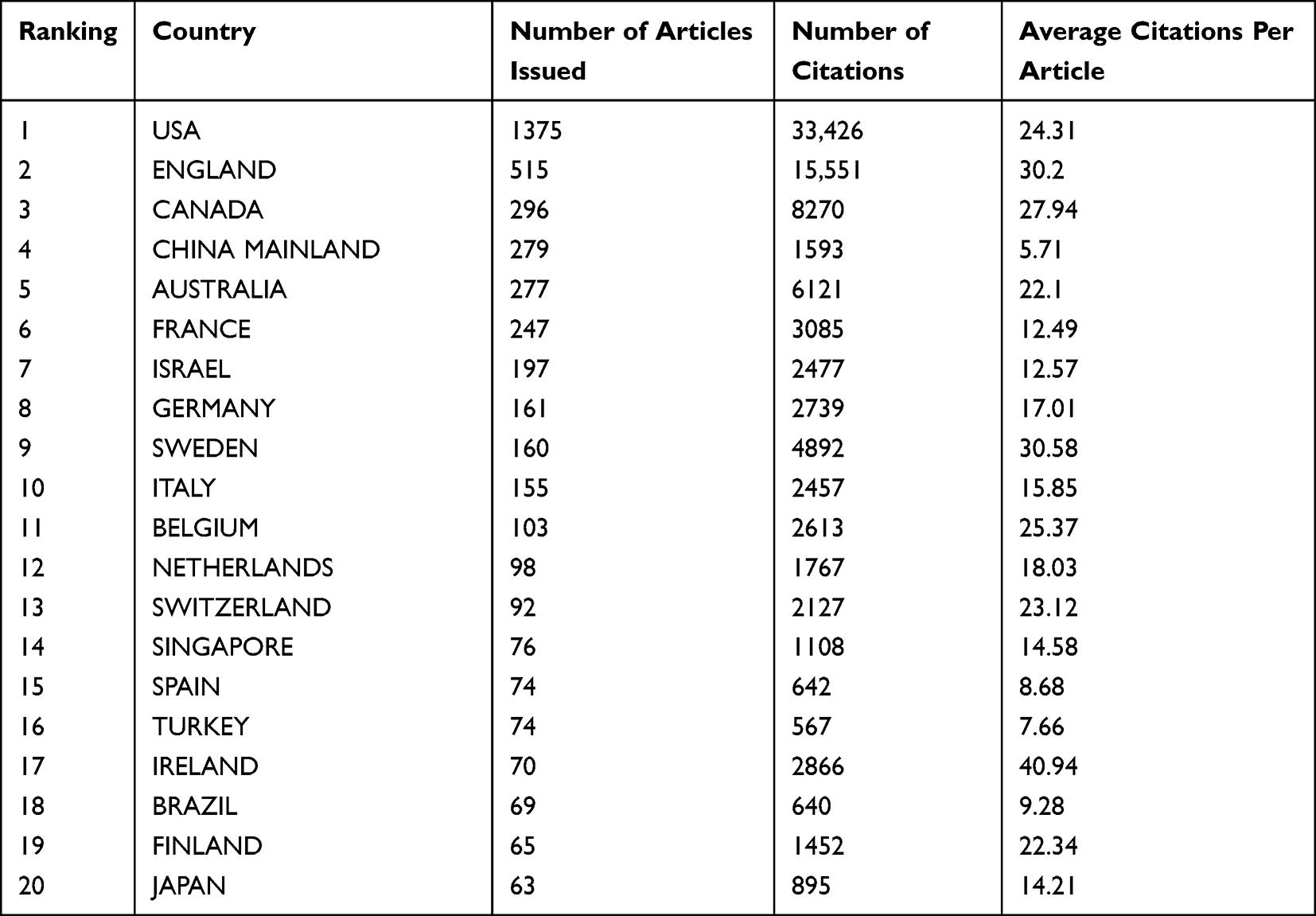 |
Table 1 Ranking of the Number of Articles Issued by Different Countries |
Among these 20 years 2021 had the highest number of publications (n=171), followed by 2017 (n=168) and 2019 (n=165). As shown in Figure 2A, the country with the highest number of publications per year continues to be the United States. In addition, we summarized the collaborative relationship between different countries in Figure 2B, and it was found that there were more collaborative treatises with USA; Canada and UK, followed by countries with more publications such as Australia and France. The United States leads the way in terms of volume of publications, annual publications and partnerships.
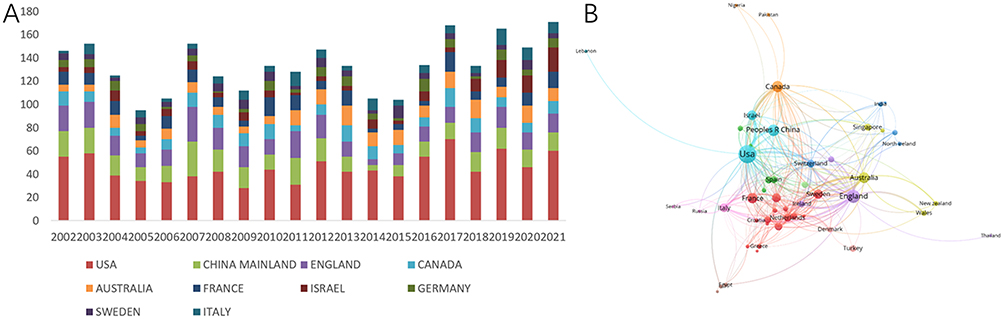 |
Figure 2 Statistical chart of the top 20 countries in terms of number of articles published on analgesia in childbirth. Notes: (A) Shows the number of articles issued by each country in different years. (B) shows the partnership of articles issued by each country, the larger the area of the dot means more partnership. |
Authors and Institutions
We also counted the corresponding authors of these articles and recorded their H-index to better assess the number and level of academic output of the researchers, with the most frequent corresponding author being Sng, Ban Leong of KK Women’s & Children’s Hospital (n=21; H-index=8). The next highest number of corresponding authors was Carvalho, Berta, B Braun Avitum Portugal (n=14; H-index=8) and Orbach-Zinger, S, Sackler Faculty of Medicine (n=10; H-index=5). The highest H-indexes among the top 20 authors counted were also Sng, Ban Leong and Carvalho, Berta.
We counted the number of articles published by different institutions and found that the two most published institutions were Harvard University (n=154; H-index=39) and Brigham & Women’s Hospital (n=115; H-index=37) in the United States, followed by the French institution UDICE-French Research Universities (n=115; H-index=23). We also summarized the graph of collaborative relationships between different institutions, as shown in Figure 3, with more collaborative institutions in Australia and more articles collaborated by institutions in the United States. See Table 2.
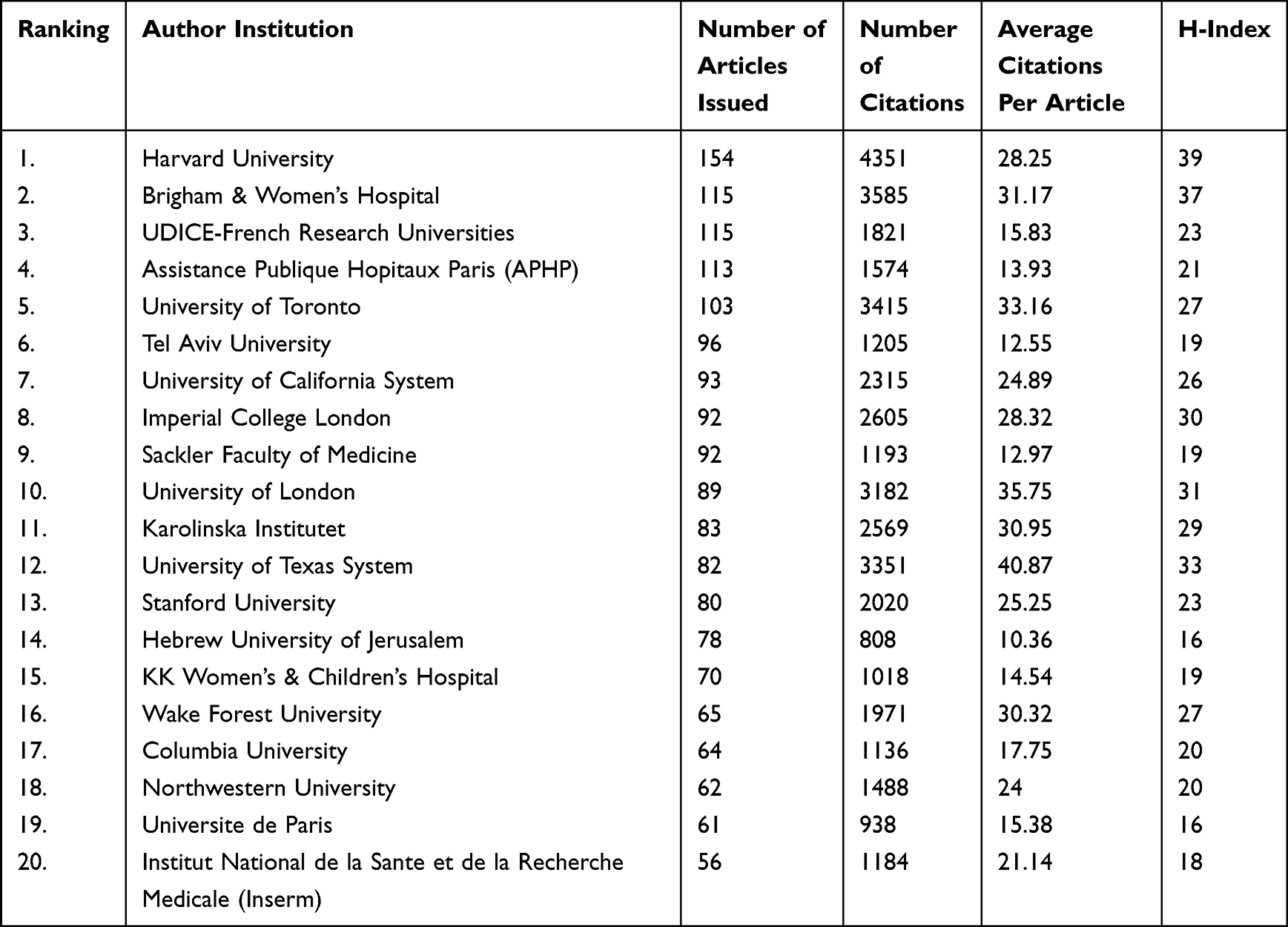 |
Table 2 Ranking of the 20 Institutions with the Highest Number of Publications |
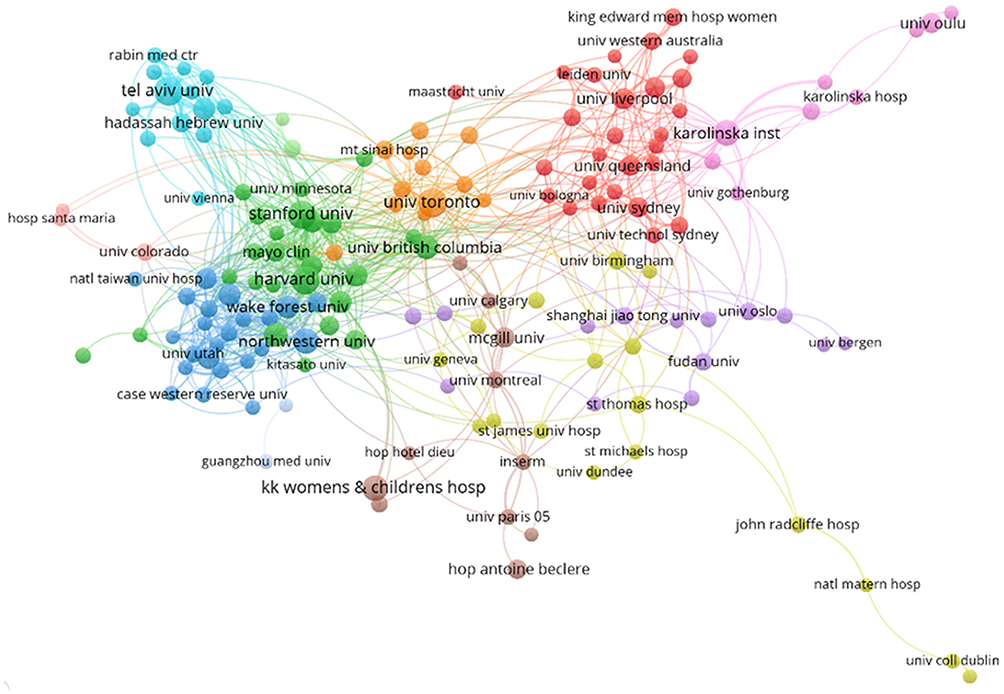 |
Figure 3 For labor analgesia without using the partnership map between institutions. Note: Larger dots indicate more collaborations. |
Subjects and Funds
We analyzed all included article disciplines and funds and categorized them statistically. The most predominant disciplines issuing articles were anesthesiology (39%) and obstetrics and gynecology (35%), accounting for more than half of all articles. Other disciplines included NURSING (6%) and PEDIATRICS (4). More detailed data are presented in Figure 4.
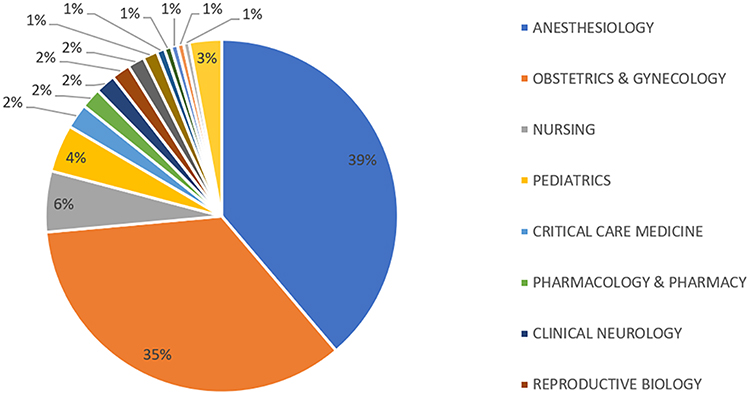 |
Figure 4 Distribution of articles published on labor analgesia in different disciplines. |
We also summarized the 10 funders that funded the most birth analgesia postings, as shown in Table 3. The United States Department of Health Human Services funded the largest number of publications with 167. This was followed by the Nih Eunice Kennedy Shriver National Institute Of Child Health Human Development Nichd (n=67) and the European Commission (n=42).
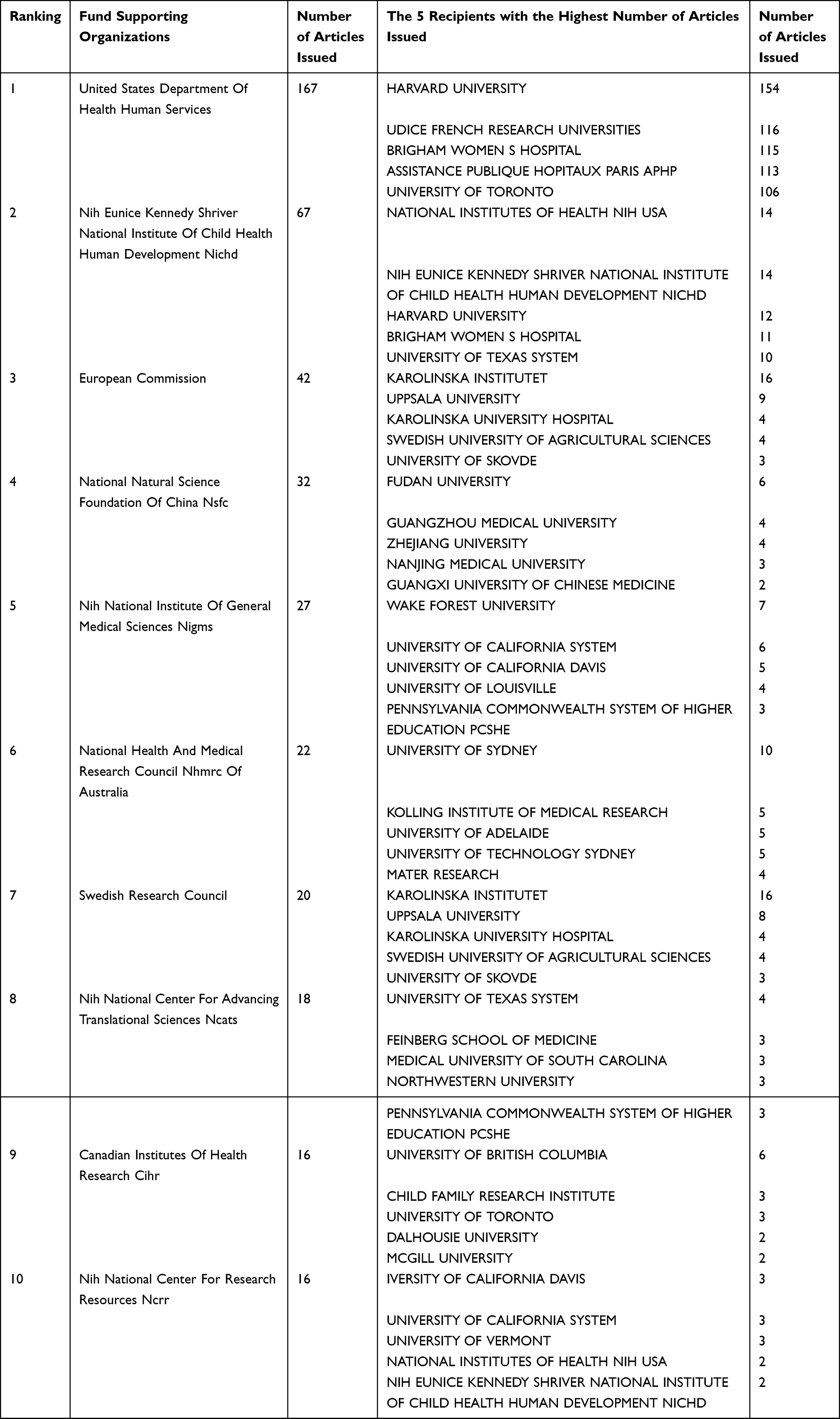 |
Table 3 The 10 Most Funded Funds and Recipient Institutions for Articles on Labor Analgesia |
In all these articles, most of the disciplines are anesthesiology and obstetrics and gynecology. The United States Department of Health and Human Services funded the most articles.
Journal Analysis
Secondly, we collected and counted the journals in which all articles were published, and we found that the journal that published the most articles in this category was International Journal of Obstetric Anesthesia, with 357 articles and 12.36 citations per article. In second place is Anesthesia and Analgesia, with 323 articles, by the highest number of citations two 9182, with an average of 28.43 citations per article. The third is Anesthesiology, with 160 publications, 6659 citations, and the highest average of 41.62 citations per article. More specific information is presented in Table 4. We also summarized the number of publications in each journal by year, and the number of publications in these journals has decreased significantly in recent years compared to the previous decade, but the proportion of publications in each journal has not changed significantly. More specific values are shown in Figure 5.
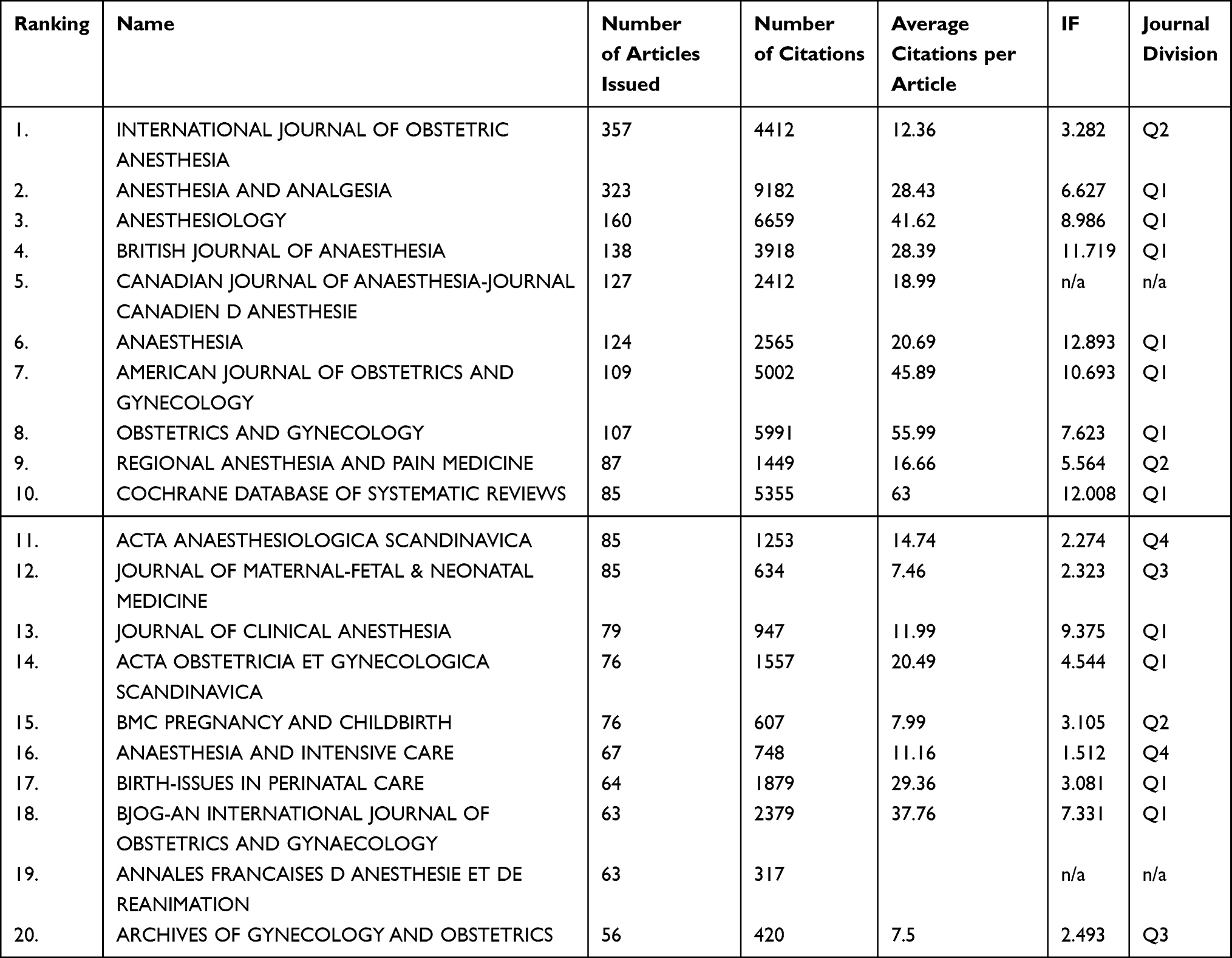 |
Table 4 Names of the Top 20 Journals in Terms of Number of Articles Published and Their Number of Articles Published |
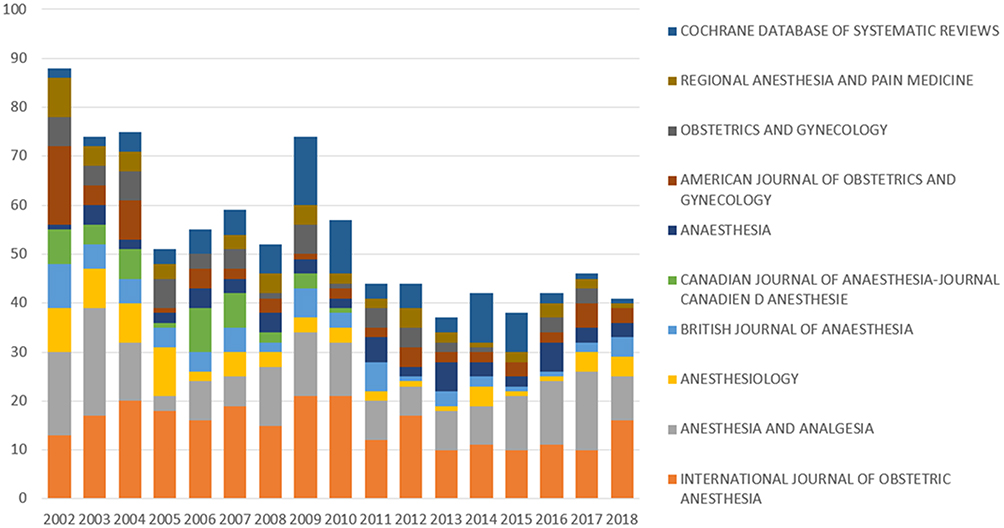 |
Figure 5 Annual distribution of articles on labor analgesia published in different journals. |
Citation
We summarized the citations of the included articles, and the 20 most cited articles are shown in Table 5. The most cited article was Clinical pharmacology of tramadol by Grond, S,8 which was cited 755 times. This was followed by Pain and women’s satisfaction with the experience of childbirth: A systematic review by Hodnett, ED9 (cited 586 times) and Midwife-led by Sandall, J continuity models versus other models of care for childbearing women10 (cited 530 times). The 20 publications included one basic medical study; nine retrospective clinical studies; two review articles and eight systematic reviews. More detailed information is shown in Figure 6 and Table 5.
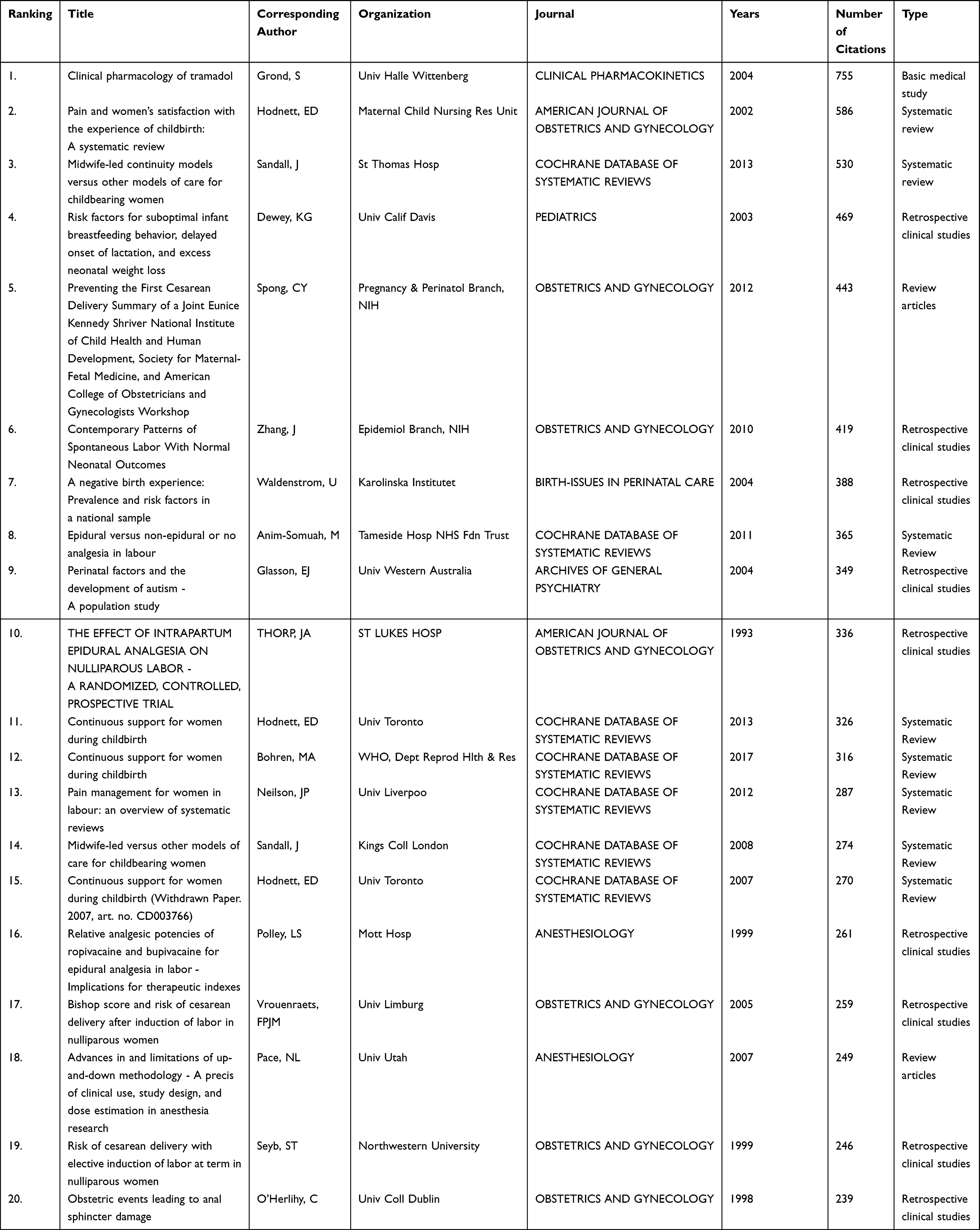 |
Table 5 Information on the Top 20 Cited Articles |
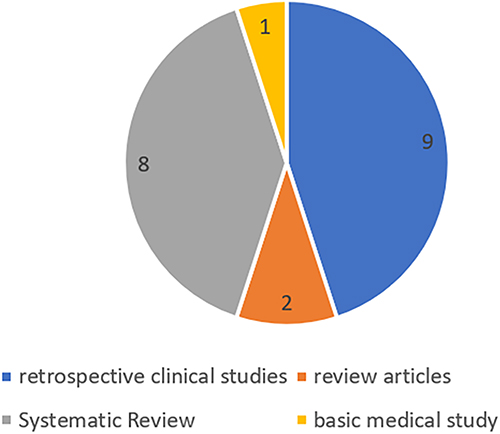 |
Figure 6 Types of articles with the top 20 citations for labor analgesia. |
Theme Analysis
We summarize the hot topics of recent research on labor analgesia in the United States and Asian countries. For the US research hotspots, bupivacaine; infusion anesthesia, etc. were mostly studied until 2010, after which epidural analgesia became the main research hotspot until around 2015, when perioperative management and possible risks became the main content of researchers’ thesis. We selected Japan and China as the Asian countries to analyze. The research hotspots in Japan before 2010 were like those in the United States, including bupivacaine and infusion anesthesia, with the difference that fentanyl also occupied a large part of the publications. There are significantly fewer articles on labor analgesia in Japan than in China and the United States. However, in the limited research found around 2015 there were many studies on nulliparous women in labor pain, which is a more unique point among the three countries. Compared with Japan, the number of publications in China appears to be more numerous and the research directions are richer. The research hotspot for labor analgesia in China remained focused on epidural anesthesia after 2015. Unlike the first two, China has recently started to study the effects of psychiatric factors, such as anxiety and depression, on labor analgesia, as well as the effects of different anesthetic drugs on labor analgesia, such as ropivacaine, bupivacaine, and dexmedetomidine. More specific results are shown in Figure 7.
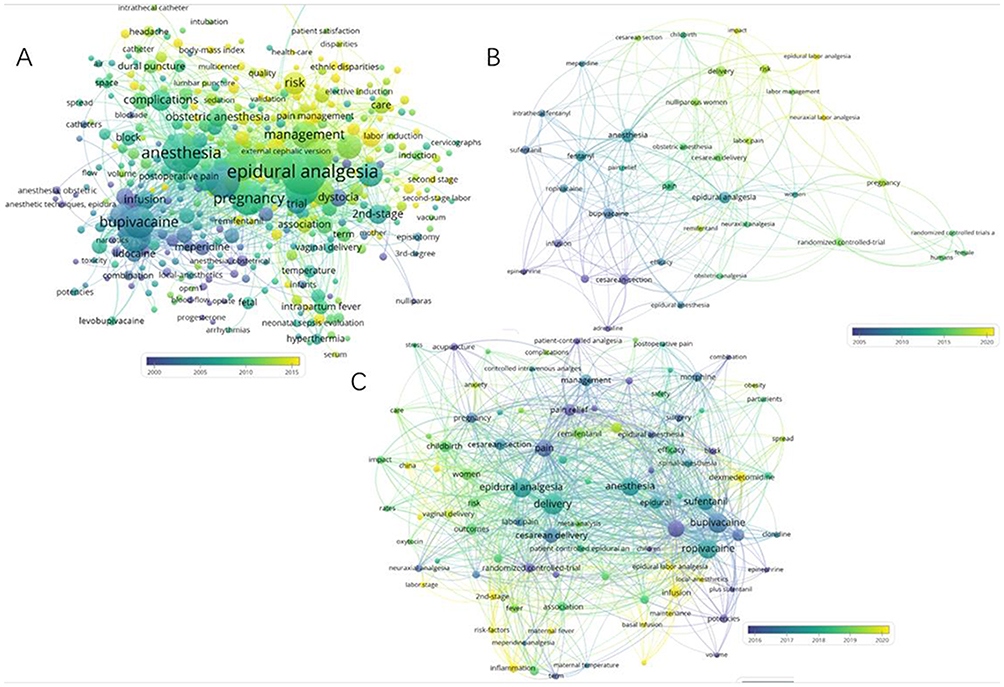 |
Figure 7 Hotspots of research on labor analgesia in the United States, Japan and China in recent years. Notes: Larger circles represent a greater number of publications. Different colors indicate different years of publication. (A) shows the clustering map of research hotspots in the United States; (B) shows the clustering map of research hotspots in Japan; (C) shows the clustering map of research hotspots in China. |
Discussion
Labor pain is a complex physiological and psychological phenomenon that occurs during labor and delivery and is related to the body’s own biochemical and physical basis, as well as having an individual emotional component. Labor pains are long-lasting and of high pain level. The main causes of labor pain include contraction of the smooth muscles of the uterus and dilatation of the cervix during labor, compression and dilatation of the rectum, pelvic floor, and soft tissues of the perineum by the fetus. Labor pain can cause maternal respiratory alkalosis, maternal and fetal hypoxia, and induce adverse events such as eclampsia and cardiac arrhythmias.
When analyzing the countries where these articles were published, we found that the United States is still the country with the most articles published in this area, with the highest number of citations. We found that the two highest H-index researchers were not from the United States, probably because there are more researchers on labor analgesia in the United States and the resources are more fragmented, and the resources are not concentrated on one researcher, but on the research institution such as Harvard University (H-index 39).
Compared to some of the world’s leading countries, China has a high number of publications but a large gap in total citations, average citations per item and H-index. With economic growth, government investment in the healthcare sector and a growing population base, a favorable environment for research is provided. Based on these advantages, China may provide a strong support to the world in the future.
In our study, we also summarized all high-citation articles from 2002 to 2021 and summarized recent research hotspots on labor analgesia in the United States, Japan, and China. We mapped the research hotspots by year and tried to relate them to the highly cited literature. We found that around 2010, epidural analgesia became a common research hotspot in all three countries, with many clinical studies on the use of epidural anesthesia for labor analgesia. Intradural labor analgesia is currently recognized as the most effective and widely used method of labor analgesia in clinical practice. Modern obstetric anesthesiology emphasizes the effective improvement of labor pain using minimal doses of intralesional anesthetics,11 thus maximizing analgesic effects and minimizing adverse effects on mother and child. Currently, there are three types of intralesional anesthesia for labor analgesia: epidural, combined lumbar-epidural, and continuous lumbar anesthesia. Epidural anesthesia has a high dosage of drugs, slow onset of pain, and may block movement. The epidural anesthesia has many drugs, a slow onset of effect, and may block the motor nerve, but it lasts for a long time and can achieve continuous analgesia during labor. The epidural can be used to provide continuous analgesia during labor. To complement the advantages of lumbar and epidural analgesia. During labor, lumbar anesthesia is used first for rapid onset of analgesia, and then continuous epidural anesthesia is used for maintenance. In the early part of the first stage of labor, lumbar anesthesia and analgesia can be used alone with opioids, and the analgesic effect is satisfactory without motor blockade. However, analgesia is insufficient in the late stage of labor. The use of local anesthetics plus opioids for lumbar anesthesia analgesia has better analgesic effect and longer maintenance time than local anesthetics or opioids alone. Low concentration of local anesthetics plus opioids for epidural analgesia can reduce the concentration of local anesthetics and reduce the number of local anesthetics. In conclusion, intradural anesthesia for labor analgesia is currently considered safe and effective, but there are still many issues that need to be studied, and the adverse effects of the drugs used need continued attention. Intradural anesthesia and epidural analgesia are still hot spots in the world of research, and we expect larger cohort studies.
The research hotspots also vary greatly between countries, and for the United States, in recent years, the research hotspots have begun to shift towards the perioperative management of maternity and possible risks. We then analyzed some of the articles that were highly cited in the text, the study by Kathryn G et al12 that described risk factors for feeding behavior in the perioperative and postpartum period, which is the same research hotspot as in the United States in recent years and could be the reason for the fourth highest number of citations in this article. In this article it was elaborated that early lactation and infant weight loss were associated with fetal gestation, number of deliveries, and no other factors such as mode of delivery and analgesic medications. The group with the lowest postpartum risk factors was multiple births and drug-free deliveries. In another highly cited literature9 a systematic evaluation of pain and women’s satisfaction with childbirth was conducted. This article included 137 reports containing more than 14,000 women from 9 countries. For the aspect of labor analgesia, the researchers illustrated that for women with prenatal anxiety usually had low satisfaction after the procedure, while the highest satisfaction was among those women who did not use pain medication. In another study included in13 it was illustrated14 that when women have enough said in their own decision making, the probability of satisfaction is higher than the effect of surgical analgesia on them. So, it is easy to see that studies on labor analgesia in the United States tend to consider pain relief and medical interventions during labor as having much less impact on maternal satisfaction than perioperative care for maternal management and emotional aspects.
In contrast to the US, recent research in China has focused on the effects of anxiety and depression on childbirth. During pregnancy, delivery, and the puerperium, women are under great physical and mental stress. The process of childbirth is a persistent and intense source of stress for the mother, and the interaction between her poor mental state and labor pain creates a vicious cycle that induces a stress response that may threaten the health of the mother and child during delivery. Some Chinese scholars have reported that many factors contribute to the failure of epidural anesthesia, including the choice of drug dosage, type and mode of delivery, and timing. Among them, maternal psychological factors are important influencing factors. Not only that, anxious and depressed emotional state can have a great impact on postpartum hemorrhage.15,16 The Japanese study on nulliparous women focused on the effect of continuous background infusion (CBI) on Patient-controlled epidural analgesia (PCRA).A study by T Okutomi et al17 concluded that when nulliparous women use background infusion, it reduces the amount of PCEA used, but does not reduce the total amount of ropivacaine and fentanyl used per hour after the start of the procedure. However, at the same time, other studies concluded that PCEA combined with CBI produced better analgesia while reducing the number of doses administered by the anesthesiologist.18,19
For labor analgesia drugs have also been the focus of research in various countries. The most cited article is the use of tramadol,8 in which it is mentioned that when tramadol is used for labor analgesia, there is no significant difference in pain relief, labor interval, etc., compared to pethidine, but pethidine shows more and more severe adverse effects.20 In some other studies tramadol was found to have no respiratory depressant effect on the mother and newborn unlike pethidine,21–24 therefore tramadol is recommended for obstetric analgesia. Dexmedetomidine has various pharmacological effects such as sedation, analgesia, and anti-sympathetic.25 Some studies have shown that intravertebral application of dexmedetomidine can enhance the analgesic and sedative effects of intravertebral anesthesia, which brings new opportunities for the use of dexmedetomidine for epidural labor analgesia.26 It is also a new research hotspot for labor analgesia in China.
Our study has some limitations; first, the articles included in the high-frequency citations, many excellent articles were published in recent years but were not included due to their short publication time and low total citation frequency. This may lead to the fact that research hotspots that are happening in recent years are not counted by us. Second, we know that the impact factors of journals are related to the citation frequencies of articles, and when they are included in the analysis at the same time, it may bias the article results.
Conclusion
We searched the database for all articles on labor analgesia published from 2002 to 2021. Despite the limitations of this article, we found differences in the hotspots of research on labor analgesia in the United States, China, and Japan, and these differences exist in medication use, paroxysm modes, and perioperative management. These differences may suggest future research directions and communications among different countries.
Author Contributions
Kang Yu and Zhigang Ding sre co-first authors. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
All the authors declare no financial support.
Disclosure
The authors declare that they have no conflict of interests.
References
1. Lim G, LaSorda KR, Farrell LM, et al. Obstetric pain correlates with postpartum depression symptoms: a pilot prospective observational study. BMC Pregnancy Childbirth. 2020;20(1). doi:10.1186/s12884-020-02943-7
2. Thomson G, Tajvar M, Pourreza A, et al. Women’s experiences of pharmacological and non-pharmacological pain relief methods for labour and childbirth: a qualitative systematic review. Reprod Health. 2019;16:16. doi:10.1186/s12978-019-0676-y
3. Albright GA. Cardiac arrest following regional anesthesia with etidocaine or bupivacaine. Anesthesiology. 1979;51(4):285–287. doi:10.1097/00000542-197910000-00001
4. Ranasinghe JS, Birnbach DJ. Progress in analgesia for labor: focus on neuraxial blocks. Int j Women’s Health. 2010;1:31–43. doi:10.2147/ijwh.s4552
5. Kan RE, Hughes S, Rosen M, et al. Intravenous remifentanil - Placental transfer, maternal and neonatal effects. Anesthesiology. 1998;88(6):1467–1474. doi:10.1097/00000542-199806000-00008
6. Thurlow JA, Waterhouse P. Patient-controlled analgesia in labour using remifentanil in two parturients with platelet abnormalities. Br J Anaesth. 2000;84(3):411–413. doi:10.1093/oxfordjournals.bja.a013452
7. Zheng H, Zheng B-X, Lin X-M, The Trend of Labor Analgesia in the World and China: a Bibliometric Analysis of Publications in Recent 30 Years. J Pain Res. 2021;14:2111. doi:10.2147/JPR.S328515
8. Grond S, Sablotzki A. Clinical pharmacology of tramadol. Clin Pharmacokinet. 2004;43(13):879–923. doi:10.2165/00003088-200443130-00004
9. Hodnett ED. Pain and women’s satisfaction with the experience of childbirth: a systematic review. Am J Obstet Gynecol. 2002;186(5):S160–S172. doi:10.1016/S0002-9378(02)70189-0
10. Sandall J, Soltani H, Gates S, et al. Midwife-led continuity models versus other models of care for childbearing women. Cochrane Database Sys Rev. 2016;2016(4). doi:10.1002/14651858.CD004667.pub5
11. Xu J, Langenbach BP, Gianotti LRR, et al. A Systematic Review and Meta-Analysis Comparing Programmed Intermittent Bolus and Continuous Infusion as the Background Infusion for Parturient-Controlled Epidural Analgesia. Sci Rep. 2019;9:9. doi:10.1038/s41598-018-36956-2
12. Dewey KG, Nommsen-Rivers LA, Heinig MJ, et al. Risk factors for suboptimal infant breastfeeding behavior, delayed onset of lactation, and excess neonatal weight loss. Pediatrics. 2003;112(3):607–619. doi:10.1542/peds.112.3.607
13. Green JM. EXPECTATIONS AND EXPERIENCES OF PAIN IN LABOR - FINDINGS FROM A LARGE PROSPECTIVE-STUDY. Birth Issues Perinatal Care. 1993;20(2):65–72. doi:10.1111/j.1523-536X.1993.tb00419.x
14. Brown S, Lumley J. Changing childbirth: lessons from an Australian survey of 1336 women. Br J Obstet Gynaecol. 1998;105(2):143–155. doi:10.1111/j.1471-0528.1998.tb10044.x
15. Lee NK, Kim S, Lee JW, et al. Postpartum hemorrhage: clinical and radiologic aspects. Eur J Radiol. 2010;74(1):50–59. doi:10.1016/j.ejrad.2009.04.062
16. Jaleel R, Khan A. Post-partum haemorrhage--a risk factor analysis. Mymensingh Med J. 2010;19(2):282–289.
17. Okutomi T, Saito M, Mochizuki J, et al. A double-blind randomized controlled trial of patient-controlled epidural analgesia with or without a background infusion following initial spinal analgesia for labor pain. Int J Obstet Anesth. 2009;18(1):28–32. doi:10.1016/j.ijoa.2008.06.006
18. Missant C, Teunkens A, Vandermeersch E, et al. Patient-controlled epidural analgesia following combined spinal-epidural analgesia in labour: the effects of adding a continuous epidural infusion. Anaesth Intensive Care. 2005;33(4):452–456. doi:10.1177/0310057X0503300405
19. Bremerich DH, Waibel HJ, Mierdl S, et al. Comparison of continuous background infusion plus demand dose and demand-only parturient-controlled epidural analgesia (PCEA) using ropivacaine combined with sufentanil for labor and delivery. Int J Obstet Anesth. 2005;14(2):114–120. doi:10.1016/j.ijoa.2004.12.005
20. Elbourne D, Wiseman RA. Types of intra-muscular opioids for maternal pain relief in labour. Cochrane Database Sys Rev. 2000;2:CD001237–CD001237.
21. Fieni S, Angeri F, Kaihura CT, et al. Evaluation of the peripartum effects of 2 analgesics: meperidine and tramadol, used in labor. Acta bio med de L’Ateneo parmense. 2000;71 Suppl 1:397–400.
22. Li E, Weng L. Influence of dihydroetorphine hydrochloride and tramadol on labor pain and umbilical blood gas. Zhonghua Fu Chan Ke Za Zhi. 1995;30(6):345–348.
23. Dinges H-C, Otto S, Stay DK, et al. Side Effect Rates of Opioids in Equianalgesic Doses via Intravenous Patient-Controlled Analgesia: a Systematic Review and Network Meta-analysis. Anesth Analg. 2019;129(4):1153–1162. doi:10.1213/ANE.0000000000003887
24. Bitsch M, Emmrich J, Hary J, et al. Obstetrical analgesia with tramadol. Fortschr Med. 1980;98(16):632–634.
25. Weerink MAS, Struys MMRF, Hannivoort LN, et al. Clinical Pharmacokinetics and Pharmacodynamics of Dexmedetomidine. Clin Pharmacokinet. 2017;56(8):893–913. doi:10.1007/s40262-017-0507-7
26. Zhao Y, Xin Y, Liu Y, et al. Effect of Epidural Dexmedetomidine Combined With Ropivacaine in Labor Analgesia. Clin J Pain. 2017;33(4):319–324. doi:10.1097/AJP.0000000000000411
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.