")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Bibliometric Analysis of Psychological Distress in Stroke: Research Trends, Hot Spots, and Prospects- An Emphasis on China
Received 6 August 2023
Accepted for publication 11 December 2023
Published 28 December 2023 Volume 2023:16 Pages 4279—4291
DOI https://doi.org/10.2147/JMDH.S434201
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Zhiguo Xu,1,2 Yi Zhu3,4
1Department of Pharmaceutical Engineering, School of Life and Health Sciences, Huzhou College, Huzhou, Zhejiang, People’s Republic of China; 2Xiehe Union East China Stem Cell & Gene Engineering Corp., Ltd, Zhejiang Umbilical Cord Blood Hematopoietic Stem Cell Bank, Huzhou, Zhejiang, People’s Republic of China; 3Department of Medicine and Health, Shaoxing University Yuanpei College, Shaoxing, Zhejiang, People’s Republic of China; 4Department of Nursing, Huzhou University, Huzhou, Zhejiang, People’s Republic of China
Correspondence: Yi Zhu, Shaoxing University Yuanpei College, 2799 Qunxian Middle Road, Yuecheng District, Shaoxing, 312000, People’s Republic of China, Fax +86-184 54518125, Email [email protected]
Background: Currently, the psychological problems of stroke patients are of great concern. It is a hot topic of clinical care research to analyze and discuss the current status and hot spots, frontiers and development trends of research on psychological distress of stroke patients, and to develop and implement psycho-social care programs to improve the quality of life of patients.However, there is an absence of visual overviews to assess the published literature systematically.
Methods: The Web of Science (WOS) database was used to search the relevant literature in this field, spanning the period 2009– 2023, and the countries, institutions, and research keywords in this field were visualized and analyzed by CiteSpace analysis software.
Results: An analysis of 416 papers found that the overall trend of psychological distress in stroke patients was increasing, and the research hotspots were mainly focusing on the relationship between different risk factors and psychological distress in stroke patients, psychological distress in stroke caregivers, positive psychology in stroke patients, and interventions on psychological distress in stroke patients. In the future, the research population may gradually shift to stroke caregivers, and the research focus will be on developing and studying scales.
Conclusion: Visual analysis of psychological distress studies in stroke patients can provide strategies for clinical interventions and broaden thinking about clinical care.
Keywords: stroke, psychological distress, emotional distress, visualization analysis, Citespace
Introduction
Stroke is a cerebrovascular disorder characterized by the disruption of blood flow in the brain due to the rupture or obstruction of blood vessels, leading to neurological damage.1 Ischemic strokes (IS) make for 80% of all strokes, with atherosclerotic and cardioembolic types being the predominant forms of IS.2,3 According to the Chinese National Stroke Registry, almost 45% of all IS cases are caused by massive atherosclerotic strokes. Cardioembolic stroke constitutes approximately 20% of all IS.4
Based on projections by the World Health Organization (WHO), the incidence of strokes in China is expected to increase from 1.8 million in 2010 to 5.4 million by 2030. At that juncture, the mortality rate would have surpassed that of cancer and cardiovascular diseases, emerging as the primary cause of death.5 The morbidity and mortality rates of stroke patients who are hospitalized are noteworthy. These rates are roughly 3.3% to 5.2% at 1 month after the stroke, 9% to 9.2% at 3 months, 34.5% to 37.1% for death or disability, and 11.4% to 15.4% after 1 year. The rates for death or disability range from 33.6% to 44.6%.6 In addition, the average medical expenses per person for stroke patients exceed 10,000 yuan, and the total direct medical expenses for hospitalized stroke patients amount to around 14.1 billion yuan.This imposes a substantial economic cost on society, families, and individuals.7,8
Psychological distress is defined as unpleasant emotional feelings caused by various reasons in the individual’s psychological (eg, behavioral style, cognitive level, or emotional state), social life, or spiritual aspects, which can progress from normal emotional changes such as sadness, tension, and fear to significant emotional challenges such as anxiety, depression, and personality changes.9 Psychological with issues of stroke are also collectively referred to abroad as psychological distress. Currently, the psychological problems of stroke patients are of great concern. The mechanisms of psychological distress and its risk factors in stroke patients, as well as the development and implementation of psycho-social care programs to enhance patients’ quality of life, are hot topics in clinical care research.
Bibliometrics is a method for analyzing a sizable body of literature in a particular research subject using mathematical and statistical approaches in order to quantitatively and qualitatively describe the literature and has grown to be a crucial part of study review.10 It can help academics evaluate the contributions of journals, institutions, and nations to a certain field of study as well as comprehend the development of that field of study. It can act as a basis for the formulation of clinical advice, especially in the field of medicine. Currently, there have been no scientometric studies conducted on the knowledge mapping of psychological distress study in stroke patients. This paper examines the current state and key areas of research on psychological distress in stroke patients. We analyze the relevant literature in the web of science database and use Citespace for cluster analysis. The aim is to identify the hot topics, frontiers, and trends in this field. The findings will offer insights for clinical interventions and suggestions for expanding clinical care.
Material and Methods
Data Sources
This study was conducted using data obtained from the Web of Science Core Collection (WOSCC), specifically the Science Citation Index Expanded, Social Sciences Citation Index, and Arts & Humanities Citation Index. The search was conducted in the restricted field “subject term” using an exact search method. The search criteria included the terms “Stroke”, “Psychological distress”, and “Emotional distress”. The language was set to English, and the document type was limited to Article and Review. The search was limited to the time period from 2009 to 2023, with a deadline of February 19, 2023. A total of 433 relevant documents were found. After excluding irrelevant research publications, a total of 416 documents were included in the analysis (Figure 1).
 |
Figure 1 Document search flow chart, selection and analysis process. |
Data Extraction and Collection
All information was collected, including number of publications and citations, title, year of publication, country of publication, institution, keywords, etc. Yi Zhu and Zhiguo-Xu, two authors, individually conducted searches in the WOSCC database to locate pertinent content. Subsequently, they retrieved the relevant data in TXT format.
Data Analysis
Citespace parameter settings: time span is 2009–2023, time slice is “1”, Term Source is “Title”, “Abstract”, “Author”, “keywords” and “keywords plus”; Node Types: Country, institution, keyword. g-index is set to 25, Top N value is set to 50, Top-N% is set to 10, using Pathfinder, Pruning sliced Pruning sliced networks clipping method was used to produce the maps.
The output analysis results mainly include annual publication volume and citation frequency analysis, country and institutional cooperation analysis, keyword co-occurrence and clustering analysis, and keyword explosion analysis. Relevant content is visualized as knowledge maps, and key nodes and links in different maps are explained and analyzed. Nodes indicate the analyzed research object, the higher the frequency of occurrence, the larger the range of nodes; the size of the outermost purple circle represents the intermediary centrality of the keyword, the value range is 0–1, the larger the node is the more important, > 0.1 indicates that it is a key node; the links between the nodes indicate the co-occurrence of the relationship, and the coarseness of the links indicates the strength of the co-occurrence.10 The more links, the stronger the relationship between nodes.
Based on the keyword co-occurrence, the keywords were clustered and analyzed, and the high-frequency keywords were clustered using log-likelihood ratio (LLR). The cluster label represents the main content of the research in the field, and the cluster ordinal number (#) is inversely proportional to the cluster size, ie, the smaller the number of clusters is, the larger the size of the literature research under the cluster, and the higher the research hotspot is. Meanwhile, CiteSpace provides modular values (Q-value) and average silhouette values (S-value) according to the network structure and clustering results. It is generally believed that Q value > 0.3 indicates a significant clustering structure, S value at 0.7 clustering has a certain degree of significance and credibility, and greater than 0.5 indicates that the clustering is generally reasonable.11
Results
Time Characteristics Analysis
The number of papers published in each period represents productivity, and the citation frequency represents influence, reflecting the development trend of research in this field. As shown in Figure 2, research in this field can be roughly divided into three stages.The first phase, from 2009 to 2012, was characterized by a constant publishing rate and a low level of citation frequency, showing that this field of study had a very early start but required further attention. The second phase, which lasted from 2013 to 2018, saw the field’s development generally continue to advance, but the average annual number of articles fell, reaching a modest peak of 37 articles in 2013. The third phase, from 2019 to 2022, showed an explosive increase in the cited frequency of research in this area. The investigation of psychological distress following a stroke was advancing.
 |
Figure 2 Trends in the number of articles and frequency of citations of studies on psychological distress in stroke. |
Distribublications Among Countries and Institutions
The number of countries and institutions that published studies on psychological distress in stroke was relatively broad, covering 36 countries and 366 institutions. Among the countries involved (Figure 3), the top 5 countries in terms of the number of publications were the United States (n=109), the United Kingdom (n=67), Australia (n=55), China (n=40), and Canada (n=28). Among the institutions (Figure 4), the top five institutions were City Univ London (n=11), University of Melbourne (n=10), Harvard University (n=9), Kings Coll London (n=9), UCL (n=8), and Columbia Univ (n=7).
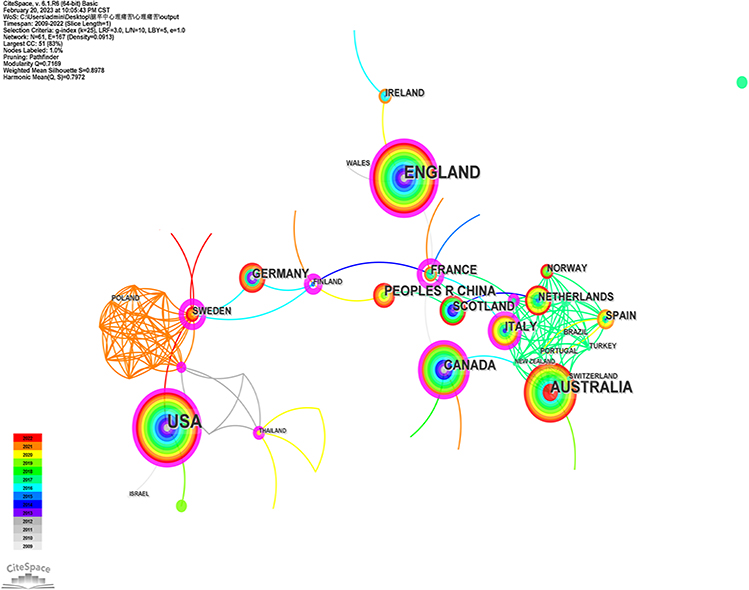 |
Figure 3 Distribution of national collaborations on psychological distress in stroke research. |
 |
Figure 4 Distribution of institution collaborations on psychological distress in stroke research. |
Research Hotspots and Frontier Analysis
Analysis of High-Frequency Keywords
High-frequency keywords are essential indicators of the research hotspots in the field. As shown in Figure 5, In addition to the keywords “psychological distress” and “stroke”, which were the most basic terms in this field of study, the top five high-frequency keywords were depression (n = 102), quality life (n=92), risk factor (n=49), mortality (n=35), anxiety (n=33). The top five keywords for high centrality were anxiety (centrality = 0.22), risk factor (centrality=0.17), coronary heart disease (centrality=0.15), family caregiver (centrality=0.08), cognitive impairment (centrality=0.06) (Table 1).
 |
Table 1 High-Frequency Keywords and Centrality of Stroke Psychological Distress Studies |
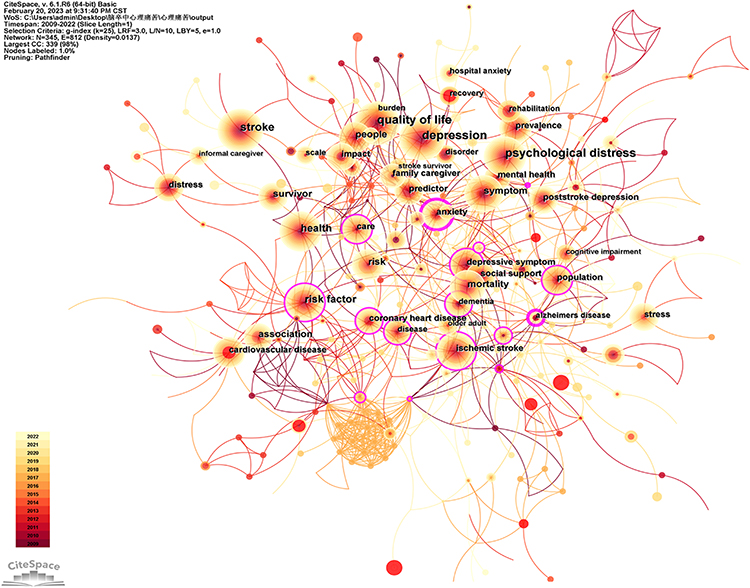 |
Figure 5 Co-occurrence of keywords in stroke psychological distress research. |
Analysis of Keyword Clustering
To reflect the research hotspots and directions more generally, this study used Citespace to cluster the keywords in the literature. As shown in Figure 6, A total of 14 thematic clusters were generated in this study, and the research directions mainly included #0 dementia, #1 quality of life, #2 mental health, #3 risk factors, #4 prospective study, # 5 carer, #6 acceptance and commitment therapy, #7 brain injury, #8 atrial fibrillation, #9 natural history, #10 blood pressure, #11 Pittsburgh sleep quality index, #12 disorder screener gad7, and #13 dyad.
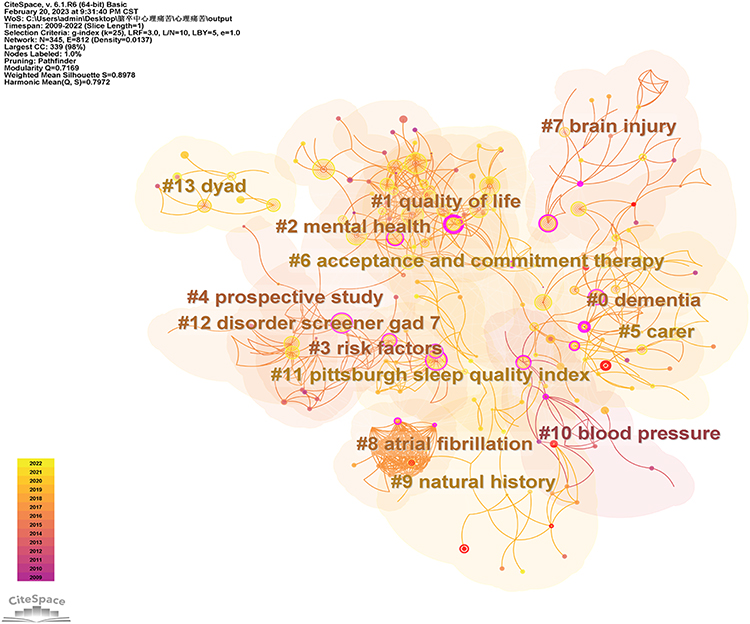 |
Figure 6 Clustering diagram of keywords for stroke psychological distress research. |
Analysis of Burst Words
The study used Citespace to explore keywords with high citation outbursts, from which subject terms with high-frequency change rates were detected to identify potential trends and research frontiers. According to Figure 7, strength denoted the degree of keyword emergence, begin denoted the year the keyword first appeared within the scope of the study, end denoted the year it stopped appearing, blue block denoted the intensity unit annual time slice, and red block indicated the time period corresponding to the keyword emergence. Between 2009 and 2022, the highest outbreak intensity was observed for the emergent word reliability (n=3.57), followed by cardiovascular disease (n=3.22) and myocardial infarction (n=2.98). It has been found that the scope of research on stroke psychological distress was relatively broad, with more focus on clinical research in the early and middle stages, on mechanisms and systems, the relationship between lesion location and stroke psychological distress, and risk factors for stroke patient psychological distress, such as coronary disease, myocardial infarction, and chronic illness. In recent years, the study population had focused on stroke survivors and increased the study of the informal caregiver. The keywords represented the research direction, such as scale, psychometric property, and reliability, suggesting that future research may shift to developing scales and research.
 |
Figure 7 Keyword emergence in stroke psychological distress research (top 25). |
Discussion
Overview of Research on Psychological Distress in Stroke
Regarding the number of publications and citations, Figure 2 shows that 2019 to date is a period of rapid development in the field of psychological distress in stroke. The reason for this is that, with the continuous improvement of the concept of excellent health in recent years, especially after 2019, the public has increasingly paid attention to the healthy development of its mental and spiritual aspects based on strengthening physical health. Problems such as mental emotions that deteriorate due to the occurrence of stressful events have received extensive. Before 2019, research on psychological suffering was first developed in the field of cancer diseases, and the research population mainly focused on cancer patients. In recent years, it gradually began to shift to patients with chronic diseases such as stroke, diabetes, coronary heart disease, and respiratory disease. Since then, the field of psychological distress in stroke has gradually stepped into the public’s view, and research fever has surged. In terms of issuing journals, the number of publications in journals of different disciplines, such as Clinical Neurology, Psychiatry, Rehabilitation, and Nursing, is also very high, indicating that research on stroke and psychological distress is not limited to a single discipline and can be published in journals with a wide range of readers.
From the perspective of issuing countries, developed countries such as the United States, the United Kingdom and Australia are the primary scientific research exporters in this field with their high volume of articles and wide distribution of issuing organizations. China has also made positive contributions in this research field, and international cooperation has been breaking through, delivering Chinese solutions and wisdom to the world. However, there are problems of lack of cross-regional cooperation and geographical limitations of research in China; therefore, different countries and institutions should strengthen cooperation and exchange further to improve the quality and influence of their research and promote the further diversified development of this research field.
Stroke Psychological Distress Research Hotspots and Future
The Relationship Between Different Risk Factors and Psychological Distress in Stroke
As shown in Table 1 and Figure 5, the high-frequency keyword risk factor (centrality = 0.17) represents the current research hotspot of psychological distress in stroke. Similarly, the high-frequency keyword coronary heart disease (centrality = 0.15) represents the related risk factors. Furthermore, the clusters labelled as #0 dementia, #8 atrial fibrillation, #10 blood pressure, and #11 Pittsburgh sleep quality index in Figure 6, as well as the emergent words myocardial infarction and chronic illness in Figure 7, were all found to be linked to risk factors for psychological distress in stroke patients.
Pittsburgh Sleep Quality Index
Cluster #11 of the Pittsburgh Sleep Quality Index clearly shows that the quality of sleep following a stroke is one-factor affecting psychological suffering. Research has indicated that insomnia affects as many as 56% of individuals who have experienced a stroke. A survey conducted among stroke patients revealed that those who reported fewer instances of insomnia demonstrated positive correlations with enhancements in physical well-being, energy levels, mobility, mood, personality, social functioning, cognitive abilities, and work performance. Conversely, an increase in the frequency of insomnia episodes was linked to decreased mobility, concentration, and memory.12 The adverse effects of post-stroke insomnia may continue throughout the stroke process, exacerbating physical disability, aggravating psychiatric conditions including dementia and anxiety, and raising the risk of suicide.13 It may also further exacerbate the symptoms of stroke complications such as hypertension, diabetes mellitus, and coronary artery disease, which may lead to secondary strokes in severe cases and affect the quality of life.14
Coronary Disease, Atrial Fibrillation, Dementia
The high-frequency keyword coronary heart disease (centrality = 0.15) was representative. Research has shown that psychological distress can have a negative impact on the heart, and a large sample (221,677 participants) prospective cohort study from Australia showed a strong positive association between the level of psychological distress and stroke and myocardial infarction.15 Clustering #0 dementia, #8 atrial fibrillation, #10 blood pressure and the emergent words myocardial infarction and cognitive impairment are instructive, and the study shows that myocardial infarction, stroke, and dementia are causally related to each other.15 Atrial fibrillation, a risk factor for stroke, causes hemodynamic disturbances, promotes thrombosis, and increases the risk of stroke 5-fold.16 At the same time, about 10% of patients develop dementia after their first stroke, and 1/3 develop dementia after a recurrent stroke. The prevalence of stroke in patients with cognitive impairment or dementia is up to six times higher than in cognitively normal patients. Severe strokes advance the onset of dementia by approximately 25 years, while mild strokes advance the onset of dementia by four years.17
With the increasing pace of life, psychological problems should not be underestimated, and the deterioration of health can be significantly exacerbated when mental illness coexists with chronic disease. When cardiovascular disease and mental illness co-occur, clinicians tend to diagnose and treat only cardiovascular disease. As a result, most co-morbidities are easily underdiagnosed and misdiagnosed, and more than 50% of depressed patients in general hospitals are underdiagnosed.18 Future research should, therefore, not only increase efforts to initially screen for mental health status in patients with cardiovascular disease but also better identify common risk factors for cardiovascular disease, thereby improving both primary and secondary prevention.
Sex
Meanwhile, the risk of developing stroke and myocardial infarction was found to increase with increasing levels of psychological distress, with high and very high psychological distress increasing the risk of stroke by 24% and 44% in men and women, respectively.15 However, within the field of stroke psychology, gender is the most widely studied and controversial factor associated with post-stroke depression.A prospective study conducted by Berg et al19 found that at 18 months post-stroke, males were more likely to develop depressive symptoms compared to females. Other studies have shown different results, Fuentes et al20 conducted a prospective, observational cohort study of patients with acute cerebral infarction and found that the risk of post-stroke depression at 3-month follow-up was not affected by age, gender, personal or family history.
However, the effect of gender on psychological distress after stroke is not known, and studies have found that women and men have different effects on risk factor distribution, stroke subtypes, stroke severity, and prognosis.2 The prevalence of diabetes mellitus, dyslipidemia, atrial fibrillation, and coronary heart disease was significantly higher in women than in men, but among the most common risk factors for stroke survivors, hypertension (88%), smoking (48%), and alcohol consumption (44%), alcohol consumption and smoking were significant in the prevalence in men.21 Some studies have shown that the clinical features and natural history of female acute stroke patients are more pronounced than those of males, with a poorer prognosis22 and that women surviving stroke have higher rates of mortality, disability, and dementia23 coupled with the fact that women are more emotional and sensitive to emotions, and are more susceptible to comorbid affective disorders, such as depression, as their endocrine levels change. This suggests that a fundamental line of our future research will be to accurately assess the impact of gender on psychological distress in stroke patients.
Psychological Distress in Stroke Caregivers
Figure 5 and Table 1 demonstrates that the high-frequency keyword “family caregiver” (centrality = 0.08) is currently the main focus of research on psychological distress in stroke. Additionally, Figure 6 clusters #5 “carer”, #13 “dyad”, and Figure 7 emergent word “informal caregiver” are all connected to the psychological distress experienced by stroke caregivers.
Informal or family caregivers are defined as “personal and medically oriented care provided by a relative, partner, friend, or neighbor”.24 Research indicates that over 80% of individuals who have experienced a stroke require assistance from their family members upon discharge from the hospital.25 After being released from the hospital, the majority of stroke patients in China have typically chosen home care. Out of the approximately 4.8 million stroke patients, almost 3.5 million rely on family caregivers.This responsibility often requires an extra allocation of time and effort and leads to significant psychological strain due to the sudden occurrence of a stroke, the lack of professional training among most family caregivers, and the constant need to adapt to the patient’s changing requirements. The health of caregivers becomes a topic of public health and health policy concern when they are impacted by a stroke patient.26 Reports indicate that primary caregivers of stroke patients have depression and anxiety symptoms at rates ranging from 30% to 45% and 20% to 50%, respectively.27
Future research should investigate the development of instruments that possess high sensitivity, specificity, and a comprehensive focus on all aspects of health, encompassing physical, mental, emotional, social, and spiritual dimensions, specifically tailored for stroke family caregivers. Measuring biological and physiological indicators like blood pressure, pulse, or cortisol levels can offer valuable insights into the health of stroke family caregivers. This allows researchers to assess changes in physical function in real-time.28 Therefore, future research clinicians should incorporate stroke caregivers into their care plans, particularly during the follow-up of stroke patients. They can also include objective indicators such as blood pressure and blood glucose in health measures for caregivers. Additionally, increasing opportunities for caregivers to engage with the healthcare system would be beneficial.
Furthermore, the variations in medical caregiving experiences among caregivers have yet to be investigated. Research has indicated that adult-child caregivers place a higher importance on receiving information and educational support, whereas spousal caregivers prioritize care experiences that involve effective communication and close interaction.29 Future research may shed light on variations in healthcare experiences depending on the type of caregiver (eg, spouse, adult child, sibling, or other).Comprehending the requirements of different caregivers and providing adequate assistance in diverse forms, such as knowledge, education, training, or family-centred care, can help alleviate the burden on caregivers and improve the quality of life for stroke patients.30
Positive Psychology
Figure 5 and Table 1 reveal that social support, with a centrality value of 0.05, is the primary focus of current research on psychological distress in stroke. Additionally, Figure 6 shows that cluster #2, which includes mental health, and cluster #6, which includes acceptance and commitment therapy, are connected to research on positive psychology in stroke.
Within the context of a thriving China, enhancing the well-being of individuals who have suffered from strokes, while also addressing and managing psychological distress, has become an imperative issue. From the standpoint of positive psychology, positive psychological coping resources play a crucial role in strengthening disease prognosis, fostering mental well-being, activating internal capabilities, boosting overall happiness, and improving quality of life.31 Currently, there have been studies on psychological distress and positive psychological variables such as self-acceptance, stigma, post-traumatic growth, and self-efficacy among stroke patients in China. However, the research on interventions is still in its early stages.
Searching for the keywords “stroke & Psychological distress & Emotional distress” on the Clinical Trials.gov website, different countries have made a big splash in clinical intervention research (see Table 2), and our country’s research on stroke patients’ psychological distress in China is still mainly limited to post-stroke anxiety and depression. Firstly, acupuncture therapy, which is characterized by traditional Chinese medicine (TCM), has gradually demonstrated new advantages in the treatment of post-stroke psychological problems, and many clinical studies have affirmed the effectiveness and safety of TCM treatments, including acupuncture; secondly, visual arts-based interventions based on Bandura’s theory of self-efficacy have come to the forefront of our attention; and lastly, in the case of Internet-based cognitive behavioral therapy (iCBT), we have developed a new approach to the treatment of post-stroke psychological problems. Finally, based on iCBT, Ecological momentary intervention (EMI) was pioneered to give psychological support to stroke caregivers, which shows great potential in mental health as an innovative and cost-effective intervention.
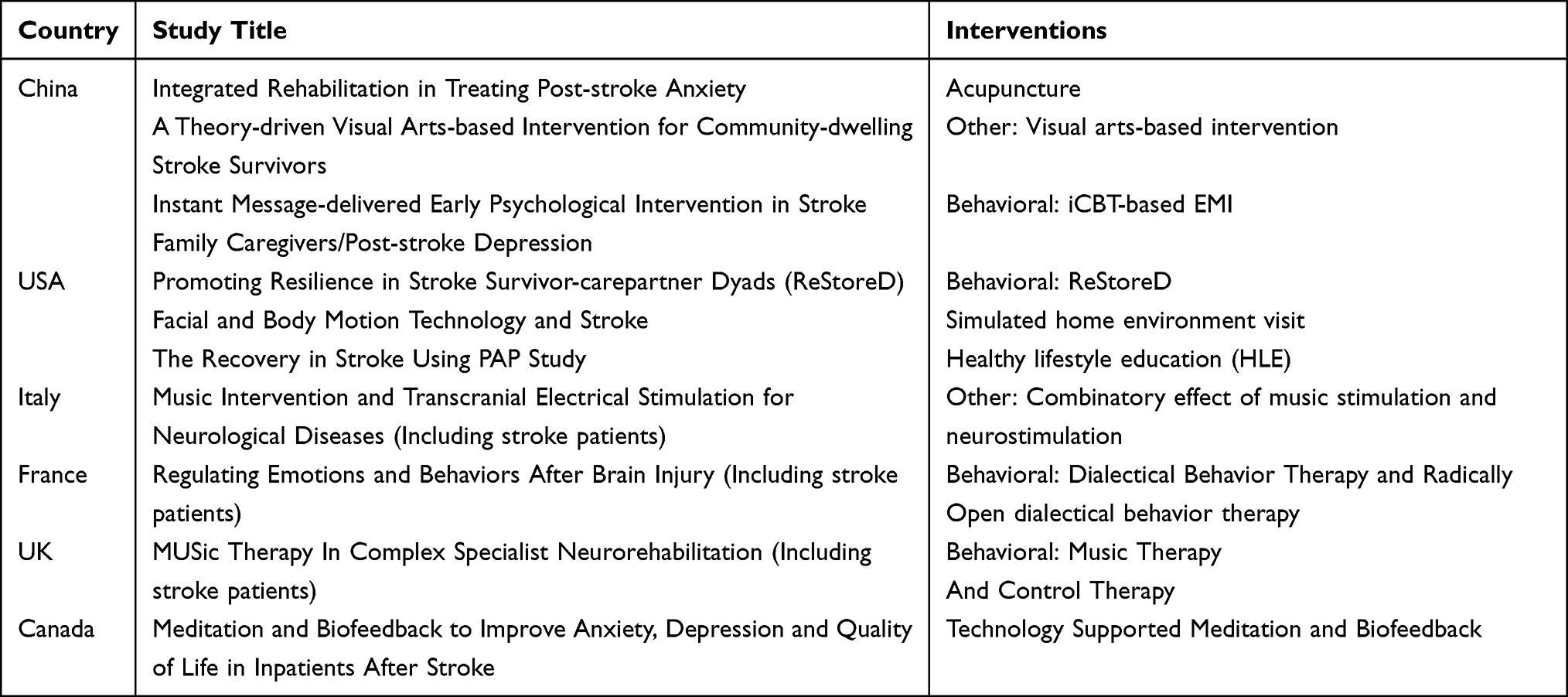 |
Table 2 Subject of Clinical Trials in the Field of Psychological Distress in Stroke |
In future clinical intervention research, two primary considerations arise. Firstly, how to effectively integrate the existing interventions (eg Chinese medicine) into the study of stroke patients’ psychological distress, and secondly, how to start from the practical point of view, and whether it is possible to take foreign countries as a reference, as far as possible, to consider the patient’s family economic situation, the strength of social support, and the existing national conditions of the health care resources and other influencing factors, to make interventions practical and feasible, and in line with the principles of the economy, and the current situation of China’s social and health care resources, which is worthy of further study.
Psychological Distress and Scale Development
As shown in Figure 5 and Table 1, among the high-frequency keywords depression, anxiety represent the current research hotspots of psychological distress in stroke, and the clustering Figure 6 #disorder screener gad7 are all related to the research of psychological distress scale in stroke. The emergent word scale, psychometric property, and reliability show the direction for future research (Figure 7).
Post Stroke Anxiety (PSA) and Post Stroke Depression (PSD) are prevalent psychiatric illnesses frequently linked to stroke. Schöttke et al32 reported that the prevalence of PSD was 31.1% and that of PSA was 20.4%. Given the high prevalence of PSD and PSA, and because of the generalizability of the anxiety and depression scales, research has focused on anxiety and depression among the forms of psychological distress. Other forms of psychological distress, such as fear, tension, sadness, worry, self-blame and loneliness have been neglected. Various types of psychological distress have varying effects on the prognostic outcomes of stroke patients. It is worth noting that the current research in the field of stroke psychology lacks a specific scale for measuring anxiety and depression. Consequently, other forms of psychological distress have not been extensively studied as research tools, and there is no agreement on the best assessment approach.33 Therefore, it is crucial for future research to conduct extensive, multicenter prospective studies in order to establish different scales specifically designed to measure psychological distress in stroke patients. This will enable a better understanding of the various manifestations of psychological distress in stroke patients and ultimately contribute to improving their mental well-being.
Conclusion
With the continuous development and maturation of stroke treatment technology, more and more patients will become part of the vast system of stroke survivors, and the pressure on caregivers will increase day by day, and psychological problems as one of the most representative problems of stroke patients and their caregivers, should not be underestimated. In the past five years, research on psychological distress in stroke has made significant progress. In future clinical research, it is necessary to continuously strengthen and update theoretical knowledge and practical skills, strengthen national and inter-institutional cooperation, improve the overall level of care, and promote the development of nursing disciplines.
Strength and Limitations
Compared with traditional reviews and systematic reviews, the advantage of this study lies in the use of bibliometrics to quantitatively analyze a large amount of literature in the field of stroke psychological distress research from 2009–2023, which more intuitively reflects the research content and research hotspots in the field.The results of the data analysis can predict the future research trends, thus focusing on and leading the future direction of research.
However, the following limitations exist in this study: (1) Only one database, WoSCC, was utilized in this investigation, resulting in limited information retrieval, potentially introducing bias. Nevertheless, it is important to acknowledge that WoSCC was the predominant database utilized in bibliometric study, and the data obtained from WoSCC could reasonably reflect the state of most publications within a specific subject to a certain degree. (2) The Citespace analysis software analyzes the key words instead of the full text, so the detection of the article as a whole may be omitted and needs to be further interpreted in the context of actual clinical work. (3) Due to the long time span of the included literature, the expression of keywords is inevitably inconsistent, similar, or written in multiple ways, leading to a certain bias in the analysis. (4) There is no international common or prescribed standard process for parameter setting in the software, and the results may be biased due to different algorithms.
Ethics Approval and Consent to Participate
An ethics statement is not applicable because this study is based exclusively on published literature.
Acknowledgments
We sincerely thank the three reviewers for their valuable comments to improve the quality of our article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the grants from Zhejiang key high-tech product development projects (No. 40, 290, [2017] Zhejiang Economic and Information Technology).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Johnson CO, Nguyen M, Roth GA.; Global. regional, and national burden of stroke, 1990–2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol. 2019;18(5):439–458. doi:10.1016/S1474-4422(19)30034-1
2. Arboix A, Oliveres M, Massons J, Pujades R, Garcia-Eroles L. Early differentiation of cardioembolic from atherothrombotic cerebral infarction: a multivariate analysis. Eur J Neurol. 1999;6(6):677–683. doi:10.1046/j.1468-1331.1999.660677.x
3. Adams HJ, Bendixen BH, Kappelle LJ, et al. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke. 1993;24(1):35–41. doi:10.1161/01.STR.24.1.35
4. Cao R, Lu Y, Qi P, et al. Collateral Circulation and BNP in predicting outcome of acute ischemic stroke patients with atherosclerotic versus cardioembolic cerebral large-vessel occlusion who underwent endovascular treatment. Brain Sci. 2023;13(4):539. doi:10.3390/brainsci13040539
5. Jiang B, Sun H, Ru X, et al. Prevalence, incidence, prognosis, early stroke risk, and stroke-related prognostic factors of definite or probable transient ischemic attacks in China, 2013. Front Neurol. 2017;8:309. doi:10.3389/fneur.2017.00309
6. Wang W, Jiang B, Sun H, et al. Prevalence, incidence, and mortality of stroke in China: results from a nationwide population-based survey of 480 687 Adults. Circulation. 2017;135(8):759–771. doi:10.1161/CIRCULATIONAHA.116.025250
7. Pellico-Lopez A, Fernandez-Feito A, Cantarero D, et al. Cost of stay and characteristics of patients with stroke and delayed discharge for non-clinical reasons. Sci Rep. 2022;12(1):10854. doi:10.1038/s41598-022-14502-5
8. Roth GA, Mensah GA, Johnson CO, et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: update From the GBD 2019 Study. J Am Coll Cardiol. 2020;76(25):2982–3021. doi:10.1016/j.jacc.2020.11.010
9. Riba MB, Donovan KA, Andersen B, et al. Distress Management, Version 3.2019, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2019;17(10):1229–1249. doi:10.6004/jnccn.2019.0048
10. Chen C. Searching for intellectual turning points: progressive knowledge domain visualization. Proc Natl Acad Sci U S A. 2004;1:5303–5310. doi:10.1073/pnas.0307513100
11. Synnestvedt MB, Chen C, Holmes JH. CiteSpace II: visualization and knowledge discovery in bibliographic databases. AMIA Annu Symp Proc. 2005;2005:724–728.
12. Helbig AK, Stockl D, Heier M, Ladwig KH, Meisinger C. Symptoms of Insomnia and sleep duration and their association with incident strokes: findings from the population-based MONICA/KORA Augsburg cohort study. PLoS One. 2015;10(7):e134480. doi:10.1371/journal.pone.0134480
13. Westerlund A, Bellocco R, Sundstrom J, Adami HO, Akerstedt T, Trolle LY. Sleep characteristics and cardiovascular events in a large Swedish cohort. Eur J Epidemiol. 2013;28(6):463–473. doi:10.1007/s10654-013-9802-2
14. Alimoradi Z, Jafari E, Brostrom A, et al. Effects of cognitive behavioral therapy for insomnia (CBT-I) on quality of life: a systematic review and meta-analysis. Sleep Med Rev. 2022;64:101646. doi:10.1016/j.smrv.2022.101646
15. Sundboll J. Depression, stroke, and dementia in patients with myocardial infarction. Dan Med J. 2018;65:4.
16. Mozaffarian D, Benjamin EJ, Go AS, et al. Heart disease and stroke statistics-2016 update: a report from the American heart association. Circulation. 2016;133(4):e38–e360. doi:10.1161/CIR.0000000000000350
17. Pendlebury ST, Rothwell PM. Incidence and prevalence of dementia associated with transient ischaemic attack and stroke: analysis of the population-based Oxford Vascular Study. Lancet Neurol. 2019;18(3):248–258. doi:10.1016/S1474-4422(18)30442-3
18. Tang T, Jiang J, Tang X. Psychological risk and protective factors associated with depression among older adults in mainland China: a systematic review and meta-analysis. Int J Geriatr Psychiatry. 2022;37(1). doi:10.1002/gps.5637
19. Berg A, Palomaki H, Lehtihalmes M, Lonnqvist J, Kaste M. Poststroke depression: an 18-month follow-up. Stroke. 2003;34(1):138–143. doi:10.1161/01.STR.0000048149.84268.07
20. Fuentes B, Ortiz X, Sanjose B, Frank A, Diez-Tejedor E. Post-stroke depression: can we predict its development from the acute stroke phase? Acta Neurol Scand. 2009;120(3):150–156. doi:10.1111/j.1600-0404.2008.01139.x
21. Traylor M, Rutten-Jacobs LCA, Holliday EG, et al. Differences in common genetic predisposition to ischemic stroke by age and sex. Stroke. 2015;46(11):3042–3047. doi:10.1161/STROKEAHA.115.009816
22. Arboix A, Oliveres M, Garcia-Eroles L, Maragall C, Massons J, Targa C. Acute cerebrovascular disease in women. Eur Neurol. 2001;45(4):199–205. doi:10.1159/000052130
23. Bousser MG. Stroke in women: the 1997 Paul Dudley White International Lecture. Circulation. 1999;99(4):463–467. doi:10.1161/01.CIR.99.4.463
24. Raanani P, Ledany R. Make family caregivers visible, valued, and supported: an interview with patients’ caregivers’ advocate. Acta Haematol. 2023;146(1):47–51. doi:10.1159/000527734
25. Teasell R, Salbach NM, Foley N, et al. Canadian stroke best practice recommendations: rehabilitation, recovery, and community participation following stroke. part one: rehabilitation and recovery following stroke; 6th edition update 2019. Int J Stroke. 2020;15(7):763–788. doi:10.1177/1747493019897843
26. Bucki B, Spitz E, Baumann M. Emotional and social repercussions of stroke on patient-family caregiver dyads: analysis of diverging attitudes and profiles of the differing dyads. PLoS One. 2019;14(4):e215425. doi:10.1371/journal.pone.0215425
27. Zhao J, Zeng Z, Yu J, et al. Effect of main family caregiver’s anxiety and depression on mortality of patients with moderate-severe stroke. Sci Rep. 2021;11(1):2747. doi:10.1038/s41598-021-81596-8
28. Byun E, Evans L, Sommers M, Tkacs N, Riegel B. Depressive symptoms in caregivers immediately after stroke. Top Stroke Rehabil. 2019;26(3):187–194. doi:10.1080/10749357.2019.1590950
29. Smith SD, Gignac MA, Richardson D, Cameron JI. Differences in the experiences and support needs of family caregivers to stroke survivors: does age matter? Top Stroke Rehabil. 2008;15(6):593–601. doi:10.1310/tsr1506-593
30. Pucciarelli G, Vellone E, Savini S, et al. Roles of changing physical function and caregiver burden on quality of life in stroke: a longitudinal dyadic analysis. Stroke. 2017;48(3):733–739. doi:10.1161/STROKEAHA.116.014989
31. Wang ZY, Liu L, Shi M, Wang L. Exploring correlations between positive psychological resources and symptoms of psychological distress among hematological cancer patients: a cross-sectional study. Psychol Health Med. 2016;21(5):571–582. doi:10.1080/13548506.2015.1127396
32. Schottke H, Giabbiconi CM. Post-stroke depression and post-stroke anxiety: prevalence and predictors. Int Psychogeriatr. 2015;27(11):1805–1812. doi:10.1017/S1041610215000988
33. Quinn TJ, Elliott E, Langhorne P. Cognitive and mood assessment tools for use in stroke. Stroke. 2018;49(2):483–490. doi:10.1161/STROKEAHA.117.016994
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.