Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Bibliometric Analysis of Exercise and Chronic Obstructive Pulmonary Disease
Authors Chen M, Zhang Y, Mao Y, Lian Y, Ye P, Liu C, Zhang Z, Fu X
Received 2 February 2023
Accepted for publication 30 April 2023
Published 8 June 2023 Volume 2023:18 Pages 1115—1133
DOI https://doi.org/10.2147/COPD.S406955
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Mengtong Chen,1,2,* Yuting Zhang,1,2,* Yuqiao Mao,1 Yunwen Lian,1 Peng Ye,1 Chunlong Liu,2 Zhijie Zhang,3 Xihua Fu1
1Department of Infectious Diseases Unit, Panyu Central Hospital, Guangzhou, People’s Republic of China; 2College of Acupuncture Moxibustion and Rehabilitation, Guangzhou University of Chinese Medicine, Guangzhou, People’s Republic of China; 3Department of Rehabilitation, Luoyang Orthopedics Hospital of Henan Province, Luoyang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xihua Fu, Email [email protected]
Background: Chronic Obstructive Pulmonary Disease (COPD) is the leading cause of death in the world. Pulmonary rehabilitation includes, but is not limited to, exercise training and education, which aim to improve the physical and psychological conditions of patients with chronic respiratory diseases through self-management interventions.
Objective: The aim of this study was to perform a bibliometric analysis of studies on exercise and COPD published from 2000 to 2021 using VOSviewer and CiteSpace.
Methods: All included literature was obtained from the Web of Science core collection. VOSviewer was used to analyze country or region, institution, major co-cited journals, and keywords. CiteSpace was used to analyze centrality, author and co-cited authors, journals, the strongest citation bursts of references, and keywords.
Results: A total of 1889 articles meeting the criteria were obtained. The United States has the largest number of publications. The American Journal of Respiratory and Critical Care Medicine is the most influential in this field, and the most published research institution is Queen’s University. Denis E. O’Donnell has made significant contributions to exercise and COPD research. Association, impact, and statement are hot spots of research in this field.
Conclusion: A bibliometric analysis of exercise interventions for COPD over the past 22 years provides direction for future research.
Keywords: bibliometrics, visualization, exercise, COPD, research hotspots
Introduction
Chronic obstructive pulmonary disease (COPD) is a common, preventable, and treatable global health problem characterized by persistent airflow limitation and respiratory symptoms, the most common of which include dyspnea, cough, or sputum. According to the World Health Organization (WHO), COPD is the third leading cause of death worldwide,1 with more than 80% of deaths occurring in low- and middle-income countries.2,3 According to the Burden of Obstructive Lung Disease (BOLD) program and other large-scale epidemiological studies, the prevalence of COPD is expected to increase over the next 40 years as smoking rates increase in developing countries and populations in high-income countries age. As a result, more than 5.4 million people may die annually from COPD and related diseases by 2060.4,5 COPD poses a significant economic and social burden to the public health sector, and therefore effective therapeutic interventions for COPD are currently a research hotspot in the medical field.
It has been found that COPD patients have significantly lower than normal exercise levels in daily life for long periods of time, with a corresponding decrease in muscle mass and strength and associated disuse atrophy,6 leading to a decrease in exercise capacity and quality of life. On March 12, 2020, the World Health Organization (WHO) declared the COVID-19 outbreak a global pandemic.7 The coronavirus attacks the human respiratory system and causes severe respiratory syndrome.8 The pandemic raises questions about the management and treatment of patients with COPD. There is no clear evidence of an increased risk of novel coronavirus infection in COPD patients, and more clinical trials are needed.9 To reduce the virus’s transmission risks, hospital visits for pulmonary rehabilitation for COPD patients are suspended, and COPD patients should be encouraged to stay at home and engage in moderate exercise under professional guidance. Therefore, we believe that in the context of the COVID-19 pandemic, more resources will be devoted to exercise and COPD in the future.
In addition to pharmacological treatments, non-pharmacological treatments can be used as a complement to manage the health of COPD patients. Globally, it is estimated that one in three people currently have a health condition that could benefit from rehabilitation,10 and pulmonary rehabilitation is an important component of non-pharmacological treatment, and pulmonary rehabilitation has been shown to be the most effective treatment strategy for improving shortness of breath, health, and exercise tolerance.11 Exercise is a core component of pulmonary rehabilitation and the most appropriate option for patients in their home conditions. Exercises include endurance training, resistance training, interval training, and flexibility training.12 Multiple lines of evidence suggest that long-term exercise-based pulmonary rehabilitation is better at improving dyspnea, muscle strength, exercise capacity, and quality of life in COPD patients compared to non-exercise programs,13 while reducing the psychological impact of COPD. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) recommends that people with COPD participate in supervised exercise training at least three times a week for 20–30 minutes per exercise session, with a combination of moderate-intensity constant-load or interval training and strength training.14 Moderate-intensity exercise can produce a wide range of health benefits, including reduced inflammation, improved immunity, and reduced respiratory viral infections.15 Therefore, active exercise interventions should be considered a treatment priority for this population.
Bibliometric analysis is a method of statistical analysis of research results from the perspectives of authors, institutions, keywords, countries, cited authors, journals, and references using analysis software, which helps researchers have a clear understanding of the research field and grasp the research basis, hot issues, and frontier trends in the field.16 In recent years, bibliometrics has been widely used in medical fields such as acupuncture, pain, and regenerative medicine.17–19 Although there have been many publications on exercise interventions and COPD, to the best of our knowledge, these publications have not been analyzed bibliometrically with a visual approach to exercise interventions in COPD. Therefore, this study aims to help researchers understand the research progress and emerging research hotspots in this field by surveying the important collaborative forces, classic conferences, key conferences, and research hotspots in the field of exercise interventions for COPD in the past 22 years, in order to provide better exercise guidance and recommendations for COPD patients.
Materials and Methods
Search Strategy
All publication papers were searched from the Web of Science core collection database. We also used the Science Citation Index Expanded (SCI-Expanded) database of Web of Science (WOS) as the source of available databases. We set the period of publication paper retrieval from January 1, 2000, to December 31, 2021. The data search strategy was “TI = (exercise* OR kinesitherapy OR training OR “physical activity*” OR sport* OR fitness OR walk* OR run* OR swim* OR jog* OR cycling OR pilates* OR yoga OR qigong OR “tai chi”)20 AND TI = (“Pulmonary Disease, Chronic Obstructive” OR “Chronic Obstructive Lung Disease” OR “Chronic Obstructive Pulmonary Diseases” OR “COAD” OR “COPD” OR “Chronic Obstructive Airway Disease” OR “Chronic Obstructive Pulmonary Disease” OR “Airflow Obstruction*Chronic” OR “Chronic Airflow Obstruction*”) AND Language = English”. The publication types were restricted to “article” or “review”, letters, meeting abstracts, published editorials, materials, book reviews, conference presentations, news items, and corrections were excluded.
Analytical Tools
The data was cleaned up before the analysis, including removing duplicate documents and merging similar words. Graphs of the annual number of publications, the annual cumulative number of publications, and the annual total number of citations were produced by Microsoft Excel 2019 to analyze the global outputs and trend of articles related to COPD and exercise. VOSviewer (1.6.17) (Leiden University, Leiden, Netherlands)21 was used to identify productive countries or regions, institutions, the main co-cited journals, co-occurring keywords, and related visual networks. The network map was produced by VOSviewer; the size of nodes reflected the number of articles or the frequency of co-occurrence; the different colors of nodes represented different categories of research topics; the link between nodes represented the co-occurrence relationship, and the size of the link represented the co-occurrence frequency of two nodes. CiteSpace (5.8.R3) (Drexel University, Philadelphia, PA, USA)22 was used to analyze authors and co-cited authors, journals, the strongest citation bursts of references, and keywords. The strongest citation bursts show the growing interest of researchers in potential research at a given time and are a key indicator for identifying emerging hot trends.23 To obtain key clusters, three specialized measures were used: latent semantic indexing (LSI), logarithmic likelihood test (LLR), and the mutual information test (MI). Modular Q values > 0.3 mean that the delineated clustering structure is significant, average silhouettes > 0.5 are considered reasonable for clustering, and average silhouettes > 0.7 indicate that the clustering results are convincing. CiteSpace can help researchers understand the development trend of a field and find research hotspots. CiteSpace was also used to identify centrality, high centrality is often considered a pivotal point in a field.
Results
Annual Publication Outputs and Growth Trend
From 2000 to 2021, a total of 1889 publications met the inclusion criteria, including 1714 articles and 175 reviews (Figure 1), with an average annual production of 85. Graphs of the number of articles and frequency of citations were obtained using Microsoft Excel (Figure 2). Although there were fluctuations during the period, there was an overall upward trend in the annual volume of publications on exercise and COPD. We fitted a polynomial to the annual cumulative volume of publications in Figure 2A, with a growth trend model R² = 0.9991, predicting that more articles on COPD and exercise will be published in the future. Figure 2B shows that 1889 articles were cited 57,747 times (H-index 106), with an average annual citation frequency of 2624 and an all-time high of 5906 citations in 2021. These results suggest that interest in exercise and COPD continues to grow, and the intensity of research will continue to increase.
 |
Figure 1 The flow chart of study screening process. |
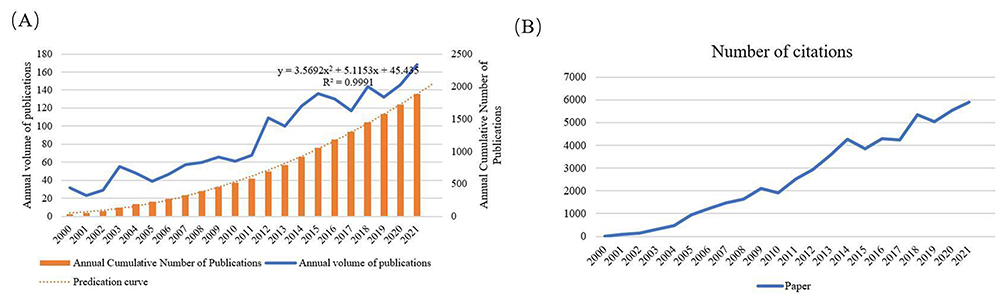 |
Figure 2 Number of publications and citations. Notes: (A) The number of publication outputs and growth trend from 2000 to 2021. (B) The number of annual citations from 2000 to 2021. |
Analysis of Country
The 1889 articles were published in 69 countries. For better visualization, we only selected 38 countries with more than 5 articles via VOSviewer (Figure 3). Each node represents a country, and the size of the node represents the number of posts in that country. The larger the node, the greater the number of articles published in this field in that country. In addition, the lines between the nodes represent the connections between countries, and the closer the connections, the thicker the lines. The countries or regions are presented on the world map in Figure 4.
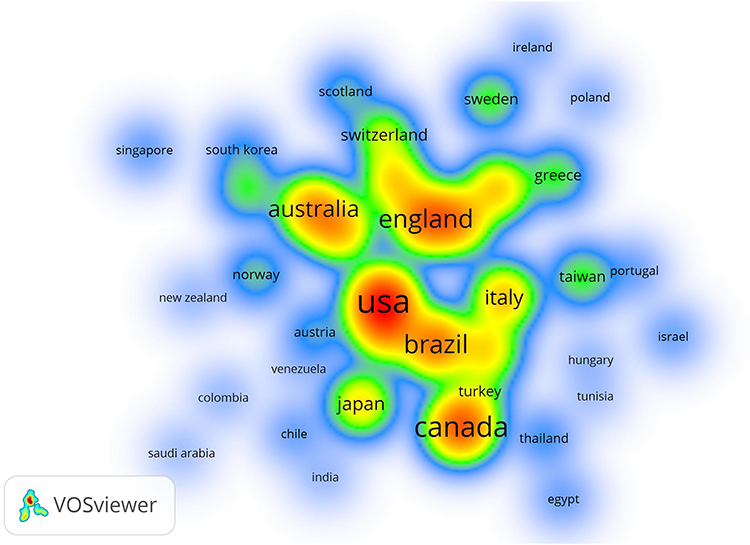 |
Figure 3 The item density visualization of active countries. Notes: The higher the density, the closer it is to red. Conversely, the lower the density, the closer it is to blue. |
 |
Figure 4 World Map of active countries. |
The list of the top 5 countries is presented in Table 1. The USA ranked first with 333 publications, followed by Canada and the United Kingdom, followed by Brazil, and finally Australia. The top five countries in terms of centrality were the USA, followed by the United Kingdom, Canada, Brazil, and Australia.
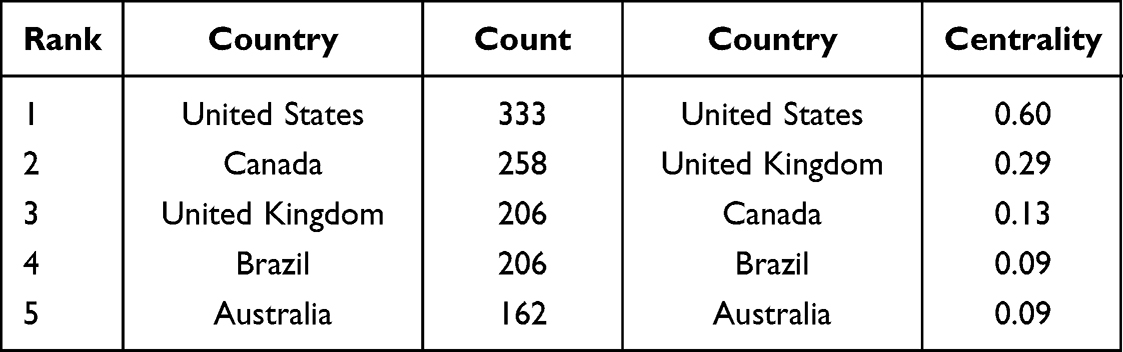 |
Table 1 Top 5 Active Countries with Count and Centrality |
Analysis of Institution
Overall, 1889 publications on exercise and COPD were coauthored by 2289 institutions. To obtain a better visualization, we only included institutions with at least 20 publications (Figure 5).
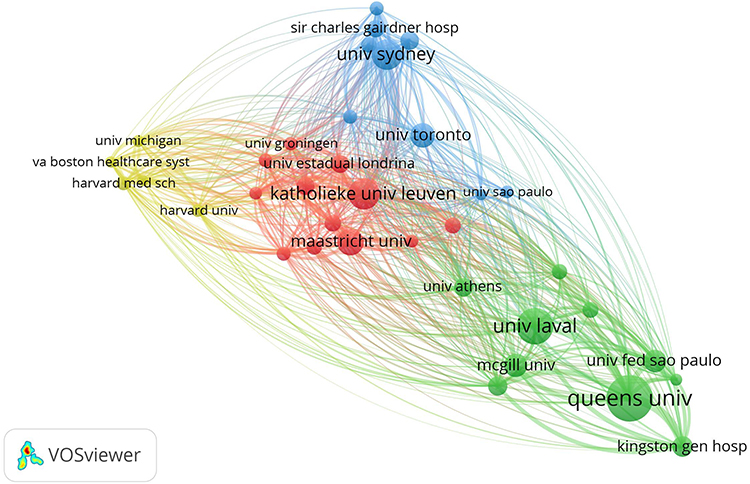 |
Figure 5 Map of active institutions. |
The list of the top 5 institutions was presented in Table 2. Queens University has published the largest number of publications (80), followed by the University of Laval (63), the Katholieke University Leuven (54), the University of Sydney (53), and the Maastricht University (46). The University of Laval showed the highest centrality (0.18). From the timeline of articles published by the institution using VOSviewer, the Hasselt University and the Harvard medical school pay more attention to exercise and COPD around 2016.
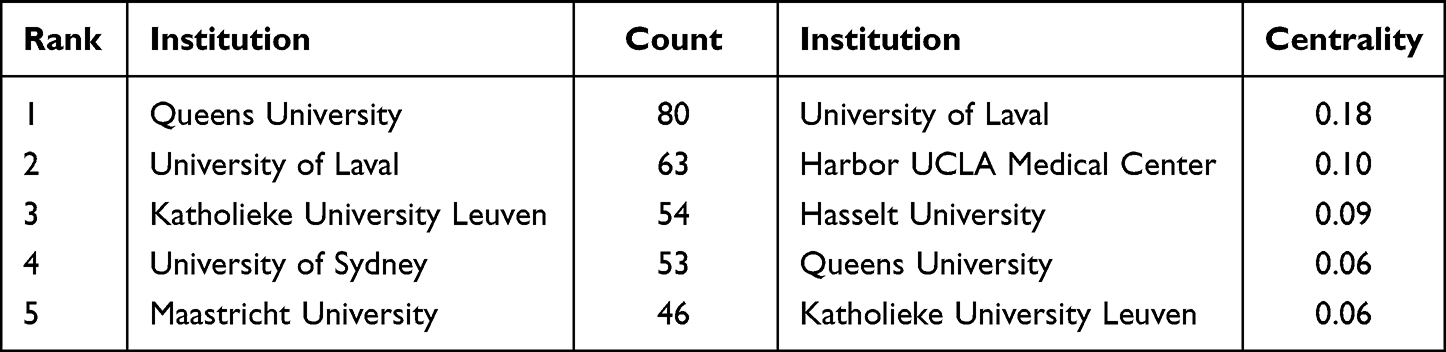 |
Table 2 Top 5 Active Institutions with Count and Centrality |
Distribution of Journals and Co-Cited Journals
A total of 310 journals published papers on exercise and COPD. Figure 6 shows a dual-map of journals. Citing journals were represented on the left, and cited journals were represented on the right. A line connects the reference logs on the left and the right. In a double-map overlay, the labels are labeled according to the subject discipline. The dual map shows that most journals are from the fields of medicine, medical and clinical. At the same time, most of the journals are cited in the fields of health, nursing, and medicine. Table 3 shows the top 10 academic journals publishing articles related to exercise and COPD research. Respiratory Medicine led the way with 149, followed by the International Journal of Chronic Obstructive Pulmonary Disease with 137, followed by CHEST with 105, European Respiratory Journal with 95, and finally the Journal of Chronic Obstructive Pulmonary Disease with 80. The average impact factor of the top 10 journals by the number of publications was 7.67, with the highest impact factor being the Sixth Ranked American Journal of Respiratory and Critical Care Medicine (IF=21.405). We only included 50 co-cited journals with at least 150 times via using VOSviewer (Figure 7). Ranked by co-citations, the American Journal of Respiratory and Critical Care Medicine ranked first with 1722, followed by the European Respiratory Journal with 1693, CHEST with 1622, THORAX with 1345, and Respiratory Medicine with 1157 (Table 4). The centrality was calculated by CiteSpace, and the journal with the highest centrality was JAMA-Journal of the American Medical Association (0.06).
 |
Table 3 Top 10 Academic Journals |
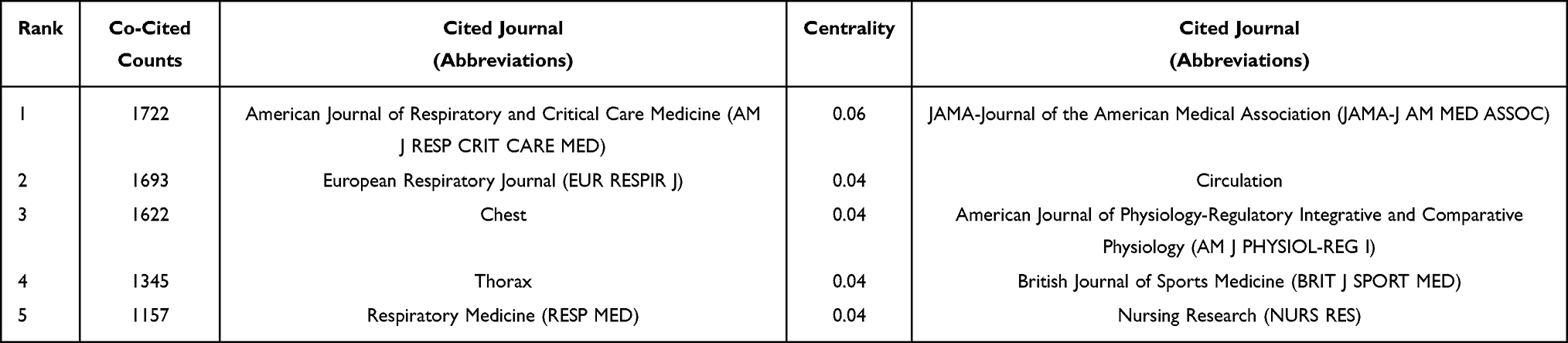 |
Table 4 Top 5 Co-Cited Journals and Centrality |
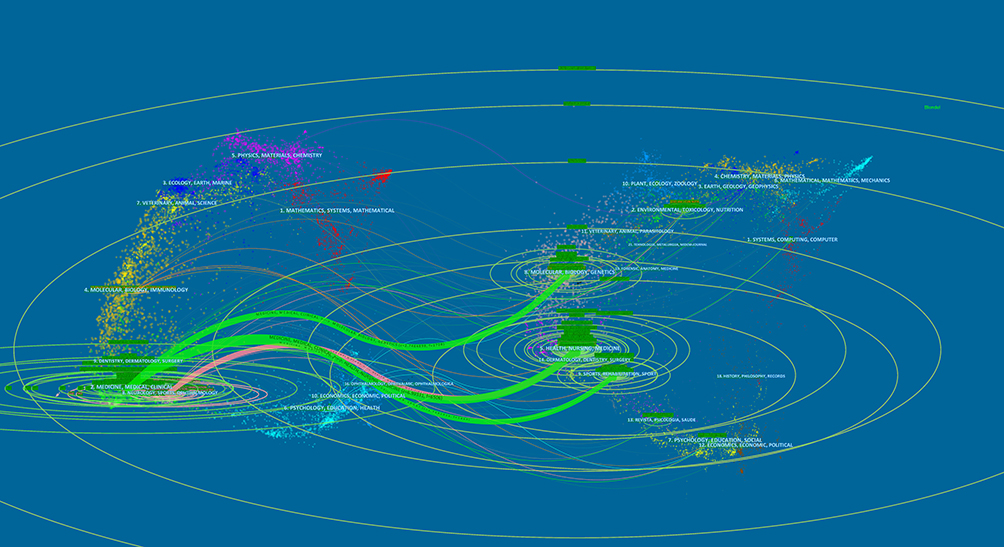 |
Figure 6 The dual-map overlay of journals with publications. |
 |
Figure 7 Map of co-cited journals with publications. |
Analysis of Authors and Co-Cited Authors
The authors’ map was generated using CiteSpace, and 1889 papers were published by 6805 study authors (Figure 8). Each node represents an author, and the larger the node, the more papers were published. The connections between nodes represent cooperation, and the more extensive the connections, the closer the cooperation. The authors’ cooperation map was generated by Cite Space with 770 nodes and 1212 links (Figure 8). The network density was 0.0041. Table 5 lists the top 10 authors who have published papers related to exercise and COPD. They are active professional writers from Canada, the Netherlands, the United Kingdom, Australia, and Spain. The collaboration between authors can be seen in Figure 8. Among the authors, O’Donnell DE, Maltais F, and Neder JA from Canada are closely related, as are Spruit MA and Wouters EFM from the Netherlands, which are mainly related to the region, but there is little connection between the authors from different countries. It indicates that scientific research exchanges and cooperation among countries should be strengthened.
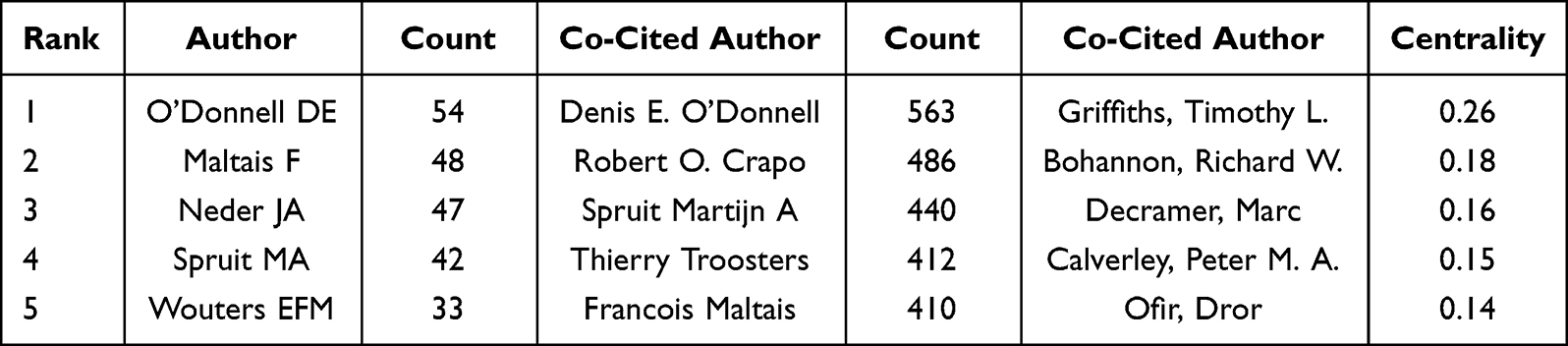 |
Table 5 Top 5 Active Authors and Co-Cited Authors |
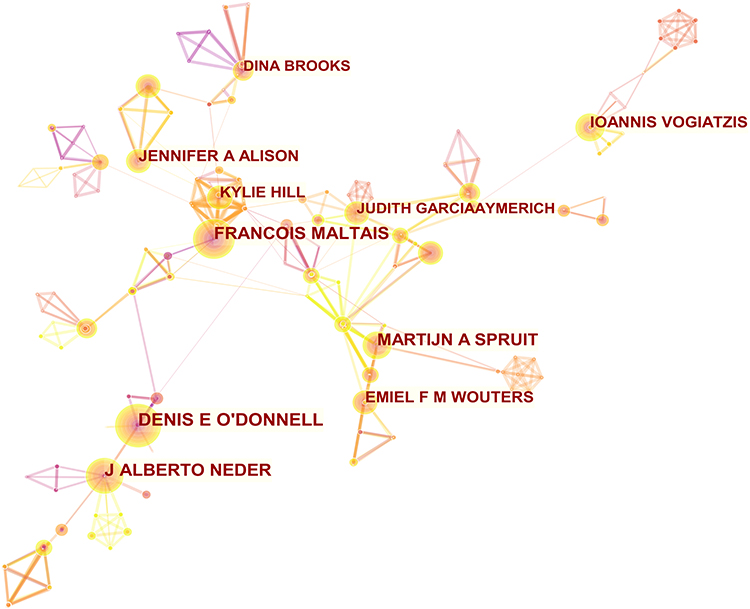 |
Figure 8 Map of authors with publications. |
A total of 852 authors had been cited. To get better visualization, we obtained a simplified network structure diagram (Figure 9, N = 852, E = 1246) by pruning the map through Pathfinder. Among all co-cited authors, anonymous authors had been cited 437 times. We would not discuss anonymously cited authors in this part. In addition, Denis E. O’Donnell ranked first, followed by Robert O. Crapo, Spruit Martijn A, Thierry Troosters, and Francois Maltais (Table 5).
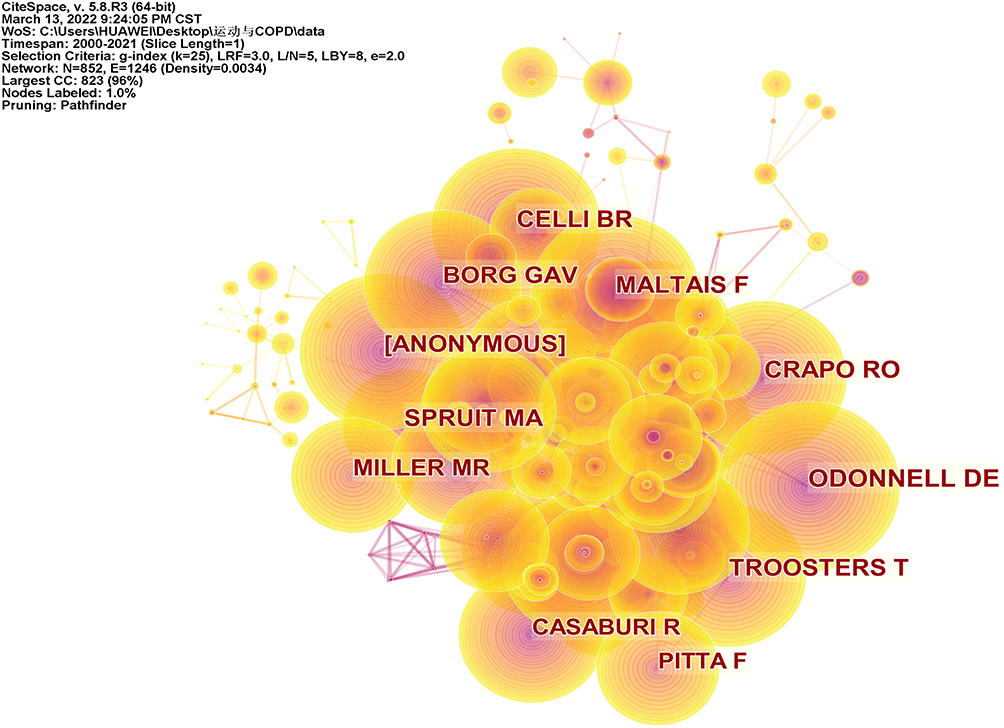 |
Figure 9 Map of co-cited authors with publications. |
In CiteSpace, the importance of nodes is highlighted through centrality. In other words, nodes with higher centrality play a greater role in the network. Griffiths, Timothy L, ranked first with the highest centrality (0.26), and he came from the University Hospitals of North Midlands.
Analysis of Co-Cited References
A total of 28,049 references were generated from 1889 records for the analysis of co-cited references. According to the period from 2000 to 2021, the time slice is 1, and the top 5 items with the most citations and the highest centrality during 2000–2021 are selected by CiteSpace.
As shown in Table 6, a key literature review jointly published by author Martijn A. Spruit and other experts in 2013 ranked first with 154 co-citations. This article presented a new definition of pulmonary rehabilitation and described the science and application of pulmonary rehabilitation, including its effectiveness in acutely ill individuals with chronic obstructive pulmonary disease.12 In the co-cited literature, the article with the highest centrality (0.16) was published by Henrik Watz et al in 2008 (Table 6). In a cross-sectional study, high values of systemic inflammation and left heart insufficiency in COPD patients were associated with reduced exercise.24 These cited studies are landmark publications in this field, laying the foundation for future research.
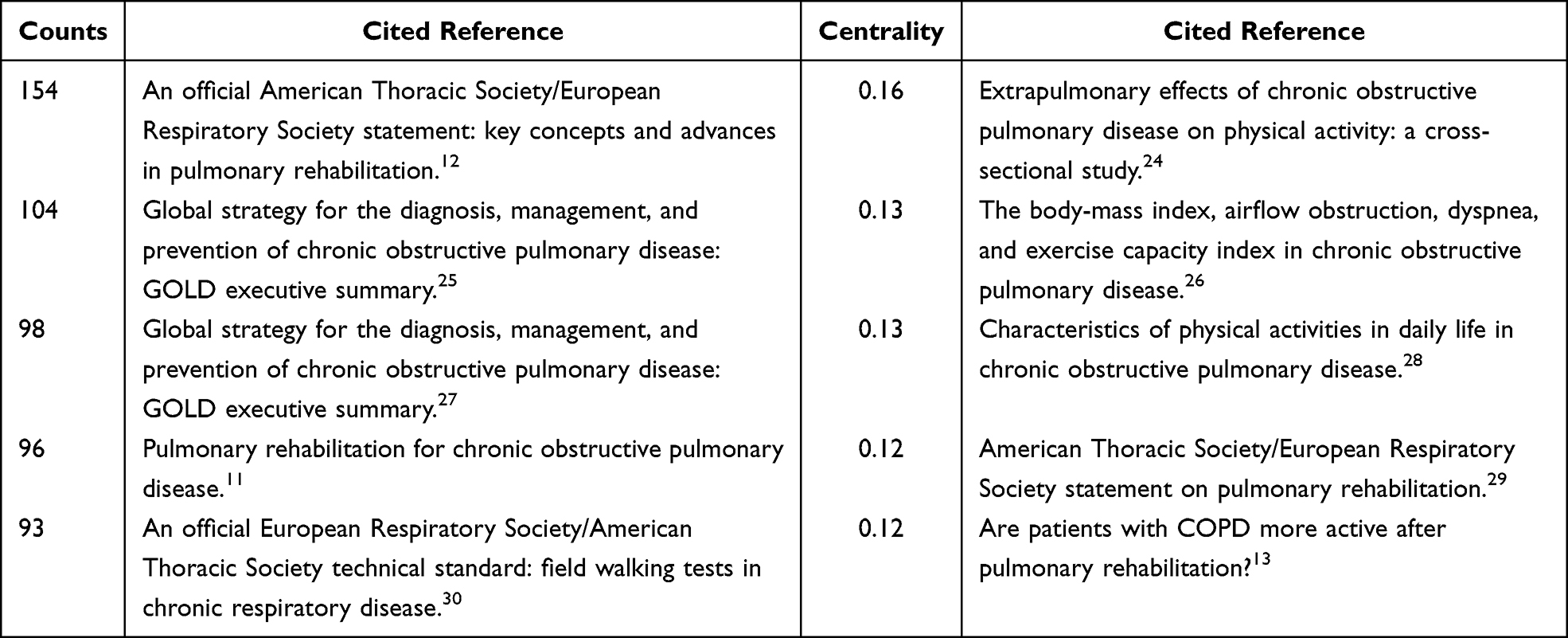 |
Table 6 Top 5 Co-Cited References in Terms of Counts and Centrality |
Analysis of Co-Occurring Keywords
From 2000 to 2021, a total of 4154 keywords appeared in the fields of exercise and COPD. In the VOSview software, we set the display co-occurrence frequency to at least 100 times (Figure 10). Therefore, a total of 23 keywords were frequently cited and grouped into three clusters. The green cluster represents the study of COPD disease manifestations and diagnostic evaluation measures; the blue cluster represents the study of exercise intensity, exercise type, and action site in COPD patients; and the red cluster represents the study of exercise ability, functional status, quality of life and disease prognosis in the process of COPD rehabilitation.
 |
Figure 10 Map of co-occurring keywords with publications. |
The centrality of each keyword was calculated using the CiteSpace software. Based on the analysis of co-occurrence frequency and centrality (Figure 10, Table 7), it was found that the maximum co-occurrence frequency was 901 times for “COPD”, followed by “obstructive pulmonary- disease” (673 times), “chronic obstructive pulmonary disease” (556 times), “exercise” (549 times), and “rehabilitation” (501 times). The highest centrality was for “lung disease” (0.07).
 |
Table 7 Top 10 Keywords |
Discussion
Research Trends for Exercise and COPD
Based on data collected from the Web of Science core collection database from 2000 to 2021, a total of 1889 articles on exercise and COPD were published in 310 journals. A total of 2289 institutions participated in the research and published papers, which were distributed in 69 countries around the world. From 2000 to 2021, the 1889 papers were cited 57,747 times. To the best of our knowledge, this is the first study using bibliometrics and visual analysis to evaluate trends in exercise and COPD, prospective outcomes, and research hotspots, which may provide directions for future research.
As shown in Figure 2, although the number of publications decreased in 2005, 2013, 2017, and 2019, the number of publications per year increased dramatically from 2019 to 2021, reaching 168 papers and 5906 citations in 2021. With the spread of the idea of “exercise as medicine”,31 appropriate exercise is essential to improving the daily living abilities of COPD patients. In addition, most COPD patients are elderly and have multiple comorbidities such as cardiovascular disease and diabetes, making them more vulnerable to serious complications of COVID-19.32 However, home isolation can delay COPD patients’ recovery. For COPD patients, in addition to regular medication, increased exercise at home for cardiopulmonary rehabilitation is necessary. For example, tai chi increases lung capacity by counteracting the formation of fibrotic scars, thus improving the quality of life and mental status of COPD patients,33 and it is also considered an effective rehabilitation tool for people affected by post-COVID-19. Many countries are gradually starting to focus on the field of exercise interventions for COPD research. The growing trend in the number of papers indicates that this research area has received increasing attention in recent years, and we predict great potential for growth in this research area.
Quality of Global Publications on Exercise and COPD
Countries
As shown in Table 2, the United States ranked first in the exercise and COPD topic studies with the highest number of publications (333) and the highest centrality (0.6). COPD poses a significant economic threat to the United States, and it is the second leading cause of disemployment-adjusted life years (DALY) loss in the United States34, after ischemic heart disease.
In item density visualization (Figure 3), each node on the graph fills in with the color based on the density of the elements surrounding that node. The higher the density, the closer it is to red. Conversely, the lower the density, the closer it is to blue. The density depends on the number of elements in the surrounding area and the importance of those elements. As can be seen from Figure 3, the countries with the most frequent cooperation with the United States include the United Kingdom, Brazil, Canada, Australia, Italy, and Japan, and the countries with the most close cooperation are all developed countries. A strong research culture underpinned by significant public and private funding no doubt supports this. In addition, the top five countries in terms of the number of publications also have high centrality, which indicates that these countries are more active in the international community and have closer cooperation with other countries. It can also be seen from Table 1 that, among the top five countries, only Brazil is a developing country, indicating that developed countries have invested a lot in this aspect.
Institutions
In Table 2, Queens University and Laval University, both from Canada, are ranked first in several publications and centrality respectively. As can be seen from Figure 5, Queens University has the closest connection with Kingston General Hospital, but it still needs to strengthen cooperation with other institutions. The University of Laval has the highest centrality, this shows that the University of Laval is active in this field and works closely with other institutions. Collaboration helps researchers who investigated exercise and COPD share resources and exchange knowledge and ideas, which is crucial for further development. Thus, stronger collaboration networks should be established among more institutions.
Journals and Co-Cited Journals
A total of 310 journals have published papers on exercise and COPD. From the dual map of the journals (Figure 6), most journals focus on the fields of medicine, medical, and clinical, while most of the co-cited journals focus on the fields of health, nursing, and medicine. Table 3 showed that Respiratory Medicine has published more exercise and COPD papers over the past 22 years, with 149 papers, and is the favorite journal of exercise and COPD researchers (IF = 3.415). However, from the perspective of publications, it is not enough to consider only the most influential journal on exercise and COPD. As shown in Figure 7 and Table 4, the most frequently cited journal is the American Journal of Respiratory and Critical Care Medicine, with 1722 co-citation counts and three of the top five citations. We found that the first paper cited in terms of counts was also from the American Journal of Respiratory and Critical Care Medicine. Therefore, we can say that the American Journal of Respiratory and Critical Care Medicine has the greatest influence in this field (IF = 21.405). In terms of centrality, the journal active in exercise and COPD is JAMA-Journal of the American Medical (Table 4), which works closely with other journals. Future scholars should pay more attention to these journals to obtain international information and the latest advances in exercise and COPD.
Authors and Co-Cited Authors
In this study, CiteSpace helped to identify the top authors in terms of numbers of publications and the number of citations (Figures 8 and 9), and the information about author citations in the field contributed to establishing potential co-authorships. As shown in Table 5, Denis E. O’Donnell has the highest number of publications (54) and co-citation counts (563). Griffiths Timothy L. is ranked as the first co-cited author in terms of centrality (0.26). Two authors have made outstanding contributions to this field. Denis E. O’Donnell comes from the department of Respiratory and Critical Care Medicine at Queen’s University and Kingston General Hospital. Robert O. Crapo is from the Division of Pulmonary and Critical Care Medicine at the University of Utah and LDS Hospital. Spruit Martijn A and Thierry Troosters are from the Katholieke Universiteit Leuven, specializing in respiratory rehabilitation and rehabilitation science. Francois Maltais is from the University of Laval.
Denis E. O’Donnell, was the most productive author, with 54 publications. Denis E. O’Donnell mainly studied the respiratory system, general internal medicine, and physiology, including exercise measurement, medical intervention, and improvement of exercise capacity (lung capacity, lung ventilation, etc.) in COPD patients with exercise intolerance.35–39 More attention to his research direction and results will help broaden our thinking and promote innovation. Griffiths Timothy L. is the co-cited author from University Hospitals of the North Midlands, ranking first in terms of centrality. His research direction is the respiratory system, focusing on effective measures to promote lung rehabilitation, such as encouraging outpatient rehabilitation programs for COPD patients, encouraging COPD patients to gradually carry out aerobic physical exercise and lung rehabilitation education to improve the respiratory and skeletal muscle function of COPD patients, and promoting the rehabilitation of lung function.40–42
Greater attention to the research findings of key authors in the field will help open up our thinking and encourage innovation in research.
Research Hotpot for Exercise and COPD
Co-Cited Reference and Reference with the Strongest Citation Bursts
In bibliometric studies, CiteSpace was used to identify landmark publications that are highly cited by scientists and that reflect active frontiers and developments in research.
The article with the highest co-citation counts (Table 6), published in 2013, was found by Spruit et al (154). The author introduced the pulmonary rehabilitation science to the latest data and applications, including various forms of exercise training for patients with chronic obstructive pulmonary disease (COPD), whose condition improved, was clinically safe and effective, and had a curative effect on individual random respiratory diseases, and stressed the importance of pulmonary rehabilitation in chronic disease management.12 The article with the highest centrality (Table 6) was published by Watz et al in 2008 (0.16). In this paper, a cross-sectional study has found that reduced exercise in patients with COPD is associated not only with clinical stages of COPD severity but also with left heart dysfunction and systemic inflammation. The authors advocate that COPD patients should increase exercise. Regular exercise can improve the decline of lung function and reduce mortality.24
The co-cited references in Table 6 showed that the daily exercise level of COPD patients will decrease due to pulmonary dysfunction. However, reduced exercise hurts lung function. Therefore, we should pay attention to the physical management of COPD patients and emphasize the important role of exercise training in pulmonary rehabilitation therapy in COPD management. Strengthening exercise rehabilitation to reduce the degree of lung function decline and speed up the recovery of physical function, the application of home lung rehabilitation training is also increasingly supported.
The significant increase in interest in exercise and COPD is highlighted in the literature with citation bursts. Figure 11 shows the top 20 references co-citations with the strongest citation bursts from 2000 to 2021. From the bursts of cited references, literature from 2001 to 2017 has opened up a hot spot in the study of exercise in COPD.
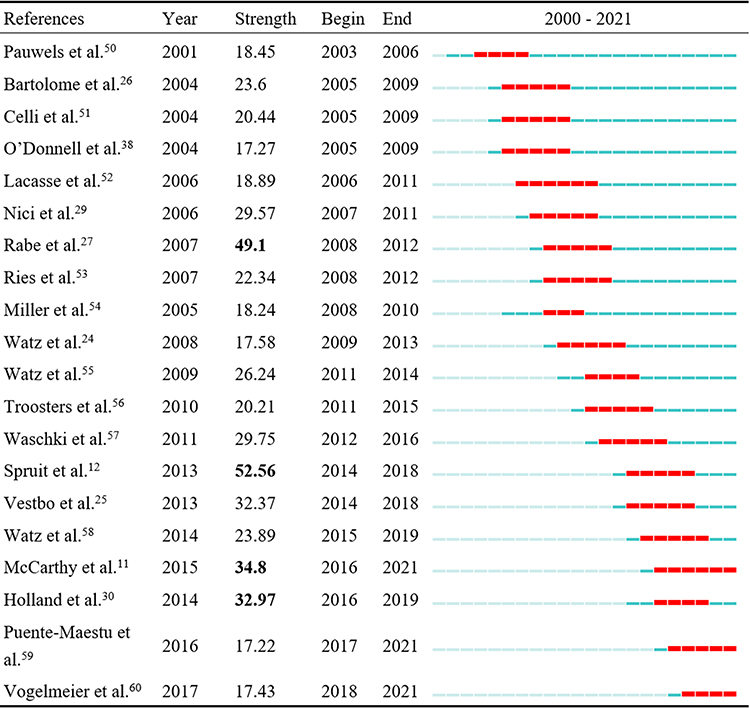 |
Figure 11 Top 20 references co-citation with the strongest citation bursts. Notes: Bold: citation burst strength >30. The light blue bar indicates that the reference has not yet appeared, the dark blue bar indicates that the reference has started to appear, and the red line represents the burst time. |
The co-cited references with bursts first occurred in 2003. Between 2003 and 2018, most references had citation bursts. The authors of the top four strongest burst references are Spruit MA, Rabe KF, McCarthy B, and Holland AE. Starting in 2013, the strongest burst came from Spruit MA and her team,12 who updated data on the scientific and applied aspects of pulmonary rehabilitation therapy and highlighted the important role of pulmonary rehabilitation therapy in the management of the chronic disease.
Labels chosen by the log-likelihood ratio test method (LLR) are used in the subsequent discussions.43 The modular Q is 0.6982, the average silhouette is 0.8839, and the map consists of 1196 nodes and 5932 links. The Modular Q values and average silhouettes obtained in the map suggest that the clusters are reasonable. I have compiled six clusters related to the theme (Table 8).
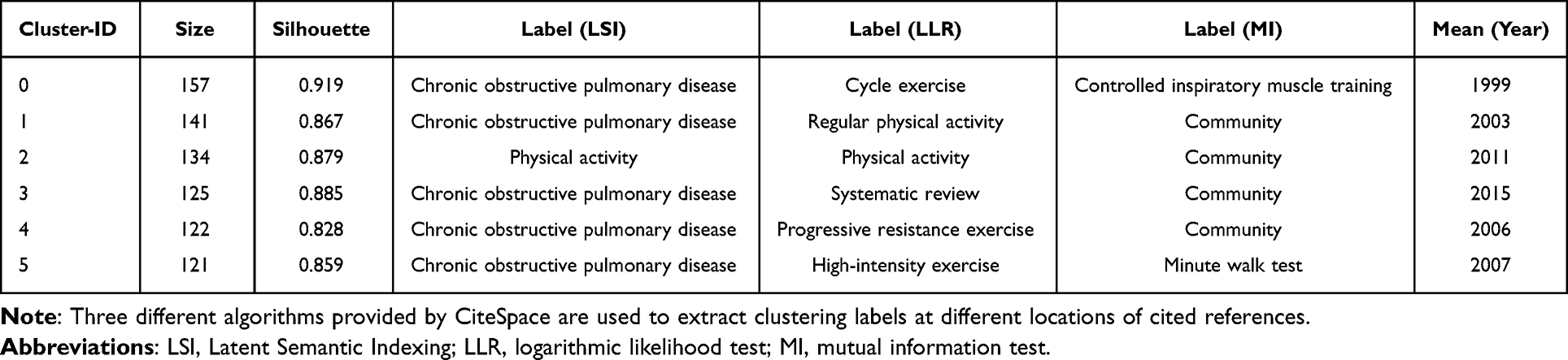 |
Table 8 Top-Ranked Clusters |
“Cycle exercise” is the largest cluster, with 157 references. The cluster has a silhouette of 0.919, indicating that the results make sense. The most active participant in this group is described in a paper published by Bernard et al. This study demonstrated that weakness in COPD was due to muscle atrophy. Periods of prolonged inactivity or lower than normal activity levels in COPD patients lead to a decrease in muscle mass and strength, resulting in peripheral skeletal muscle dysfunction.5
The second cluster is “regular physical activity”, with a silhouette of 0.867, which is one of 134 references. The most actively cited reference in the cluster is a paper published by Rabe et al. This study updated the definition of COPD, spirometry classification, and treatment, and provided new data on COPD morbidity and mortality based on the 2001 report. In addition to smoking as a risk factor, indoor air pollution from other risk factors such as biomass cooking and heating in poorly ventilated dwellings should be considered whenever possible. The study also suggested that emphasis should be placed on establishing good health care teams to ensure that COPD patients are diagnosed and receive timely and effective treatment.27
The third cluster was “physical activity”, with a silhouette of 0.879 and 125 references. The most active reference in this group is a paper published by Vestbo et al. The study revised the original recommendations and proposed three new recommendations: a change in treatment goals, a change in the COPD severity classification system, advocating for a new clinical management approach, and a new assessment system.25
Keywords with the Strongest Citation Bursts
Burst keywords are considered to be indicators of frontier topics or emerging trends. Keywords with citation bursts can reflect the development of a knowledge field. By using CiteSpace, we obtained the top 20 keywords with the strongest citation bursts (Figure 12). The keywords with earlier citation bursts could reflect the subjects that were of concern in the early stages. As can be seen from Figure 12, the words that were concerned in the early stage were lung disease (2000–2004), breathlessness (2000–2005), and randomized controlled trial (2000–2004). The emerging research keywords in recent years are association (2019–2021), impact (2017–2021), and statement (2018–2021). Figure 12 shows us that the early keywords with the strongest citation bursts included lung disease, breathlessness, and randomized controlled trial. We grouped this into three areas:
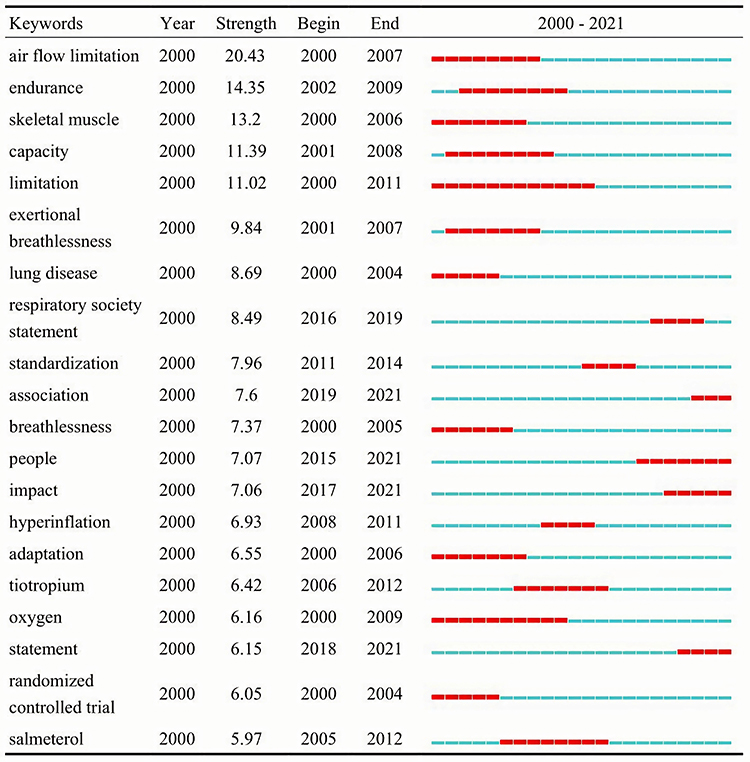 |
Figure 12 Top 20 Keywords with the Strongest Citation Bursts. Notes: The blue bars mean the reference was published; the red bars mean citation burstness. |
Disease
According to the statistics of the World Health Organization, respiratory disease is one of the three leading causes of death in the world. Chronic obstructive pulmonary diseases, as common and frequently-occurring diseases of the respiratory system, are common diseases characterized by continuous airflow restriction, with high disability and mortality rates worldwide.44
Clinical Symptoms
Common symptoms of COPD develop from mid-life on, including breathlessness or difficulty breathing, a chronic cough, often with phlegm, and tiredness.44
Intervention
To compare the effects of different interventions on lung function in COPD patients in randomized controlled trials.
The emerging research keywords are “association”, “impact”, and “statement”. Association is defined as the connection between objects. It enables one object to know the properties and methods of another object. Scholars continue to pay attention to the relationship between changes in exercise levels and COPD. According to a study in patients with and without COPD, a decline to a low exercise level was associated with the highest all-cause mortality risk in subjects with and without COPD. Moreover, it seems that being moderately physically active may already have important beneficial consequences in subjects with and without COPD.45 The Respiratory Society addressed various aspects of lung rehabilitation in its 2006, 2013, 2015, and 2018 statements.29 From emphasizing the importance of pulmonary rehabilitation to strengthening pulmonary rehabilitation education for COPD patients. Pulmonary rehabilitation should be included as a primary treatment for patients with COPD.46 An American Thoracic Society/European Respiratory Society statement on pulmonary rehabilitation noted that COPD patients accounted for the majority of the pulmonary rehabilitation treatment population.12 Pulmonary rehabilitation is clinically proven to be effective in improving the clinical outcomes of patients with COPD, such as increased exercise endurance, improved dyspnea, and ultimately improved overall quality of life for patients with COPD. Health care systems are encouraged to provide affordable rehabilitation for COPD patients, which can reduce health care resources and ultimately achieve long-term benefits.47–49 In addition, individualized treatment options, such as optimal exercise intensity and duration, should be provided for patients with COPD. Finally, patients with COPD should improve their compliance and actively participate in pulmonary rehabilitation.29 While there is a lack of evidence that education has a significant effect on the treatment of patients with COPD, self-managed educational activities have a positive impact on improving patients’ quality of life compared to routine care alone, according to the 2018 Respiratory Society statement.49,52 To improve the compliance of pulmonary rehabilitation in COPD patients, it is necessary to change the concept of patients’ education, so that they can actively participate in pulmonary rehabilitation treatment. We believed that a combination of strength and endurance training may be the best strategy for treating chronic respiratory diseases.
The change in focus reflects a trend in the field, with researchers now focusing more on the effects of the disease and providing better advice to patients with COPD.
Strengths and Limitations
This study describes the research status of exercise and COPD through countries, institutions, journals, authors and co-cited authors, keywords, co-occurrence, etc. This provides a great deal of information from different perspectives, showing current and future research trends in this field. As far as we know, this is the first time that VOSviewer and CiteSpace are used for literature analysis in this field. However, there are some limitations in the accuracy of our analysis. First, this study only included literature from the WOS core collection database, which may lead to insufficient data collection and have a certain impact on the outcome. Second, we limited the language to English and omitted non-English literature, which may lead to bias in the study of language-published literature. Furthermore, recently published research is likely to be underestimated, while existing publications with real impact will largely influence the citation indicators of journals, authors, institutions, and countries in the field more significantly over time.
Conclusion
This study analyzed trends and hot spots in exercise and COPD research from 2000 to 2021 using VOSviewer and CiteSpace. The study suggests that the number of papers published in this field will continue to increase in the future. The United States has made the largest contribution to exercise and COPD research, with Queens University and Laval University in Canada as the core institutions. Denis E. O’Donnell is an academic authority on the subject, both in terms of the number of publications and the most cited publications. The American Journal of Respiratory and Critical Care Medicine is the most frequently cited journal (IF = 21.405) and the most influential in the field. The main research interests include COPD manifestations and diagnostic evaluation methods, exercise prescription setting for COPD patients, and changes in exercise ability, functional status, quality of life, and disease prognosis after rehabilitation intervention in COPD. Emerging research focuses on the association between exercise level and COPD and the impact of pulmonary rehabilitation on clinical outcomes and quality of life in patients with COPD, according to COPD-related statements released by the Respiratory Society. Countries, institutions, and scholars should start with exercise and COPD research hotspots, strengthen academic cooperation, and improve the quality of research. The findings of this paper lay the framework for future development of research on exercise and COPD.
Research Ethics
All data used in this study were obtained from the Internet and no animal or human subjects were involved. Therefore, ethics committee approval is not required.
Acknowledgments
The authors show gratitude for Van Eck and Waltman, the inventor of the VOSviewer. The authors also would like to express their appreciation to Professor CM Chen, who invented CiteSpace, which is free to use.
Funding
This study was supported by Grant No.201904010065 from the science and technology program of Guangzhou.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. The top 10 causes of death. Available from: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death.
2. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2095–2128. doi:10.1016/S0140-6736(12)61728-0
3. Vos T, Flaxman AD, Naghavi M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2163–2196. doi:10.1016/S0140-6736(12)61729-2
4. Lopez AD, Shibuya K, Rao C, et al. Chronic obstructive pulmonary disease: current burden and future projections. Eur Respir J. 2006;27(2):397–412. doi:10.1183/09031936.06.00025805
5. Bernard S, Blanc PLE, Whittom F, et al. Peripheral muscle weakness in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1998;158:629–634. doi:10.1164/ajrccm.158.2.9711023
6. Buck D, Jacoby A, Massey A, Ford G. Evaluation of measures used to assess quality of life after stroke. Stroke. 2000;31(8):2004–2010. doi:10.1161/01.STR.31.8.2004
7. World Health Organization. World Health Organization announces COVID-19 outbreak a pandemic. Available from: https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/news/news/2020/3/who-announces-covid-19-outbreak-a-pandemic.
8. World Health Organization. Coronavirus disease (COVID-19). Available from: https://www.who.int/health-topics/coronavirus#tab=tab_1.
9. Gerayeli FV, Milne S, Cheung C, et al. COPD and the risk of poor outcomes in COVID-19: a systematic review and meta-analysis. EClinicalMedicine. 2021;33:100789. doi:10.1016/j.eclinm.2021.100789
10. World Health Organization. Rehabilitation. Available from: https://www.who.int/health-topics/rehabilitation#tab=tab_1.
11. McCarthy B, Casey D, Devane D, Murphy K, Murphy E, Lacasse Y. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2015;2:1–209.
12. Spruit MA, Singh SJ, Garvey C, et al. An official American Thoracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. 2013;188(8):e13–e64. doi:10.1164/rccm.201309-1634ST
13. Pitta F, Troosters T, Probst VS, Langer D, Decramer M, Gosselink R. Are patients with COPD more active after pulmonary rehabilitation? Chest. 2008;134(2):273–280. doi:10.1378/chest.07-2655
14. Ortega F, Toral J, Cejudo P, et al. Comparison of effects of strength and endurance training in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2002;166(5):669–674. doi:10.1164/rccm.2107081
15. Martin SA, Pence BD, Woods JA. Exercise and respiratory tract viral infections. Exerc Sport Sci Rev. 2009;37(4):157–164. doi:10.1097/JES.0b013e3181b7b57b
16. Bornmann L, Leydesdorff L. Scientometrics in a changing research landscape: bibliometrics has become an integral part of research quality evaluation and has been changing the practice of research. EMBO Rep. 2014;15(12):1228–1232. doi:10.15252/embr.201439608
17. Zhang J, Zhang Y, Hu L, et al. Global trends and performances of magnetic resonance imaging studies on acupuncture: a bibliometric analysis. Front Neurosci. 2020;14:620555. doi:10.3389/fnins.2020.620555
18. Wang YZ, Wu CC, Wang XQ, Kong Y. Bibliometric study of pain after spinal cord injury. Neural Plast. 2021;2021:6634644. doi:10.1155/2021/6634644
19. Chen C, Zhigang H, Liu S, Tseng H. Emerging trends in regenerative medicine: a scientometric analysis in CiteSpace. Expert Opin Biol Ther. 2012;12(5):593–608. doi:10.1517/14712598.2012.674507
20. Zhang Z, Zhu Y, Wang Q, et al. Global trends and research hotspots of exercise for intervening diabetes: a bibliometric analysis. Front Public Health. 2022;10:902825. doi:10.3389/fpubh.2022.902825
21. van Eck NJ, Waltman L. Software survey: vOSviewer, a computer program for bibliometric mapping. Scientometrics. 2010;84(2):523–538. doi:10.1007/s11192-009-0146-3
22. Chen C. CiteSpace II: detecting and visualizing emerging trends and transient patterns in scientific literature. J Am Soc Inform Sci Technol. 2006;57(3):359–377. doi:10.1002/asi.20317
23. Miao Y, Xu S-Y, Chen L-S, Liang G-Y, Pu Y-P, Yin L-H. Trends of long noncoding RNA research from 2007 to 2016: a bibliometric analysis. Oncotarget. 2017;8:83114–83127. doi:10.18632/oncotarget.20851
24. Watz H, Waschki B, Boehme C, et al. Extrapulmonary effects of chronic obstructive pulmonary disease on physical activity: a cross-sectional study. Am J Respir Crit Care Med. 2008;177(7):743–751.
25. Vestbo J, Hurd SS, Agusti AG, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187(4):347–365. doi:10.1164/rccm.201204-0596PP
26. Bartolome R, Celli MD, Claudia G, et al. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N Engl J Med. 2004;350:1005–1012. doi:10.1056/NEJMoa021322
27. Rabe KF, Hurd S, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2007;176(6):532–555. doi:10.1164/rccm.200703-456SO
28. Pitta F, Troosters T, Spruit MA, Probst VS, Decramer M, Gosselink R . Characteristics of physical activities in daily life in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005;171(9):972–977. doi:10.1164/rccm.200407-855OC
29. Nici L, Donner C, Wouters E, et al. American Thoracic Society/European Respiratory Society statement on pulmonary rehabilitation. Am J Respir Crit Care Med. 2006;173(12):1390–1413. doi:10.1164/rccm.200508-1211ST
30. Holland AE, Spruit MA, Troosters T. An official European Respiratory Society/American Thoracic Society technical standard: field walking tests in chronic respiratory disease. Eur Respir J. 2014;44(6):1428–1446. doi:10.1183/09031936.00150314
31. Sallis RE . Exercise is medicine and physicians need to prescribe it! Br J Sports Med. 2009;43(1)3–4. doi:10.1136/bjsm.2008.054825
32. Tsutsui M, Gerayeli F, Sin DD. Pulmonary rehabilitation in a Post-COVID-19 world: telerehabilitation as a new standard in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2021;16:379–391.doi:10.2147/COPD.S263031.
33. Castro JP, Kierkegaard M, Zeitelhofer M. A call to use the multicomponent exercise Tai Chi to improve recovery from COVID-19 and long COVID. Front Public Health. 2022;10:827645. doi:10.3389/fpubh.2022.827645
34. Tilert T, Dillon C, Paulose-Ram R, Hnizdo E, Doney B. Estimating the U.S. prevalence of chronic obstructive pulmonary disease using pre- and post-bronchodilator spirometry: the National Health and Nutrition Examination Survey (NHANES) 2007-2010. Respir Res. 2013;14:103. doi:10.1186/1465-9921-14-103
35. O‘donnell DE, Lam M, Webb KA. Measurement of symptoms, lung hyperinflation and endurance during exercise in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1998;158:1557–1565. doi:10.1164/ajrccm.158.5.9804004
36. O‘donnell DE, Lam M, Webb KA. Spirometric correlates of improvement in exercise performance after anticholinergic therapy in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1999;160:542–549. doi:10.1164/ajrccm.160.2.9901038
37. O‘donnell DE, Revill SM, Webb KA. Dynamic hyperinflation and exercise intolerance in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2001;164:770–777. doi:10.1164/ajrccm.164.5.2012122
38. O‘Donnell DE, Fluge T, Gerken F et al. Effects of tiotropium on lung hyperinflation, dyspnoea and exercise tolerance in COPD Eur Respir J. 2004;23(6):832–840. doi:10.1183/09031936.04.00116004
39. O‘Donnell DE, Fluge T, Gerken F. et al. Effects of tiotropium on lung hyperinflation, dyspnoea and exercise tolerance in COPD. Eur Respir J. 2004;23(6):832–840. doi:10.1183/09031936.04.00116004
40. Griffiths TL, Burr ML, Campbell IA, et al. Results at 1 year of outpatient multidisciplinary pilmonary rehabilitation: a randomised controlled trail. Lancet. 2000;355(9201)362–368. doi:10.1016/S0140-6736(99)07042-7
41. Griffiths TL, Clack TL, Roberts E, et al. Pulmonary rehabilitation. Thorax. 2001;56(11):827–834. doi:10.1136/thorax.56.11.827
42. Sabit R, Griffiths TL, Watkins, AJ, et al. Predictors of poor attendance at outpatient pulmonary rehabilitation programme. Respir Med.2008;102(6):819–824. doi:10.1016/j.rmed.2008.01.019
43. Polykandriotis E, Popescu LM, Horch RE. Regenerative medicine: then and now - an update of recent history into future possibilities. J cell Mol Med.2010;14(10):2350–2358. doi:10.1111/j.1582-4934.2010.01169.x
44. World Health Organization. Chronic respiratory diseases.Available from https://www.who.int/health-topics/chronic-respiratory-disease#tab=tab_3
45. Vaes AW, Garcia-Aymerich J, Marott JL. Changes in physical activity and all-cause mortality in COPD. Eur Respir J. 2014;44(5):1199–1209. doi:10.1183/09031936.00023214
46. Parshall MB, Schwartzstein RM, Adams L,et al. An official American Thoracic Society statement: update on the mechanisms, assessment, and management of dyspnea. Am J Respir Crit Care Med.2012;185(4):435–452. doi:10.1164/rccm.202222-2041ST
47. Maltais F, Decramer M, Casaburi R,\ et al. An official American Thoracic Society/European Respiratory Society statement: update on limb muscle dysfunction in chronic obstructive pulmonary disease. Am J Repir Crit Care Med. 2014;189(9):e15–e62. doi:10.1164/rccm.201402-0373ST
48. Rochester CL, Vogiatzis I, Holland AE et al, et al. An Official American Thoracic Society/European Respiratory Society Policy Statement: enhancing implementation, use, and delivery of pulmonary rehabilitation. Am J Respir Crit Care Med. 2015;192(11):1373–1386. doi:10.1164/rccm.201510-1966ST
49. Blackstock FC, Lareau SC, Nici, L, et al. Chronic obstructive pulmonary disease education in pulmonary rehabilitation. An Official American Thoracic Society/Thoracic Society of Australia and New Zealand/Canadian Thoracic Society/British Thoracic Society Workshop Report Ann Am Thorac Soc. 2018;15(7):69–784. doi:10.1513/AnnalsATS.201804-253WS
50. Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS, et al. Global strategy for the diagnosis, management, and the prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Innitiative for Chronic Obstructive Lung Disease (GOLD) Workshop Summary. Am J Respir Crit Care Med. 2001;163(5):1256–1276. doi:
51. Celli BR, MacNee W, Force AET, et al. Standrads for the diagnosis and treatment of patient with COPD: a summary of the ATS/ERS position paper. Eur Respir J. 2004;23(6):932–946. doi:10.1183/09031936.04.00014304
52. Lacasse Y, Goldstein R, Lasserson TJ, Martin S.Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cocharane Database Syst Rev. 2009;3:1–54
53. Ries AL, Bauldoff GS, Carlin BW, et al. Pulmonary rehabilitation: joint ACCP/AACVPR evidence based clinical practice guidelines. Chest. 2007;131(5Suppl):4S–42S. doi:10.1387/chest.10-252
54. Miller JD, Foster T, Boulanger H, et al. Direct costs of COPD in the U.S.: an analysis of Medical Expenditure Panel Survey (MEPS) data. OPD. 2005;2(3):311–318. doi:10.1080/15412550500218221
55. Watz H, Waschki B, Meyer T, Magnussen H, et al. Physical activity in patients with COPD. Eur Respir J. 2009;33(2):262–272. doi:10.1183/09031936.00024608
56. Troosters T, Sciurba F, Battaglia S, et al. Physical activity in patients with COPD, a controlled multi-center pilot-study. Respir Med. 2010;104(7):1005–1011. doi:10.1016/j.rmed.2010.01.012
57. Waschki B, Kirsten A, Holz O. Physical activity is the strongest predictor of all-cause mortality in patients with COPD: a prospective cohort study. Chest. 2011;140(2):331–342. doi:10.1378/chest.10-2521
58. Watz H, Pttta F, Rochester CL, et al. An official European Respiratory Society statement on physical activity in COPD. Eur Respir. 2014;44(6):1521–1537. doi:10.1183/09031936.00046814
59. Puente-Maestu L, Palange P, Casaburi R, et al. Use of exercise testing in the evaluation of interventional efficacy: an official ERS statement. Eur Respir J. 2016;47(2):429–460. doi:10.1183/13993003.00745-2015
60. Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. Am Thorac Soc. 2017;195(5):1–74.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Phenotyping COPD Patients with Emphysema Distribution Using Quantitative CT Measurement; More Severe Airway Involvement in Lower Dominant Emphysema
Park J, Kim EK, Lee SH, Kim MA, Kim JH, Lee SM, Lee JS, Oh YM, Lee SD, Lee JH
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2013-2025
Published Date: 31 August 2022
Chronic Obstructive Pulmonary Disease Prevalence and Associated Risk Factors in Adults Aged 40 Years and Older in Southeast China: A Cross-Sectional Study During 2019–2020
Chen J, Yin Y, Zhang Y, Lin X, Chen T, Yang Z, Wang D, Zhong W
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2317-2328
Published Date: 17 September 2022
Effects of High-Frequency Chest Wall Oscillation on Acute Exacerbation of Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Huang HP, Chen KH, Tsai CL, Chang WP, Chiu SYH, Lin SR, Lin YH
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2857-2869
Published Date: 10 November 2022
Prevalence of Chronic Obstructive Pulmonary Disease in England from 2000 to 2019
Stone PW, Osen M, Ellis A, Coaker R, Quint JK
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1565-1574
Published Date: 21 July 2023
A Long-Term Study of Adverse Outcomes Associated With Oral Corticosteroid Use in COPD

Tse G, Emmanuel B, Ariti C, Bafadhel M, Papi A, Carter V, Zhou J, Skinner D, Xu X, Müllerová H, Price D
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2565-2580
Published Date: 15 November 2023