Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 18
Beyond Efficacy: The Access, Delivery Systems, Acceptability, Persistence, and Transition Management “ADAPT” Framework for Long-Acting Injectable PrEP in Sub-Saharan Africa
Authors Ikoona EN ![]() , Namulemo L, Kaluya R, Ikoona R, Sahr F
, Namulemo L, Kaluya R, Ikoona R, Sahr F
Received 13 April 2026
Accepted for publication 25 June 2026
Published 15 July 2026 Volume 2026:18 616392
DOI https://doi.org/10.2147/HIV.S616392
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Video abstract of “The ADAPT framework for long-acting injectable PrEP” [616392].
Views: 10
Eric Nzirakaindi Ikoona,1 Lucy Namulemo,2 Ronald Kaluya,3 Rebecca Ikoona,4 Foday Sahr5
1Department of Evaluation and Research, National Public Health Agency, Freetown, Sierra Leone; 2Department of Treatment Services, Foothills Community-Based Interventions, Monticello, KY, USA; 3Department of Counselling and Support Services, Uganda Counselling and Support Services, Kampala, Uganda; 4Pharmacy Department, Makerere University-Johns Hopkins University Research Collaboration, Kampala, Uganda; 5National Public Health Agency, Freetown, Sierra Leone
Correspondence: Eric Nzirakaindi Ikoona, Department of Evaluation and Research, National Public Health Agency, 42A Main Motor Road, Wilberforce, Freetown, Western Area, Sierra Leone, Tel +232 76 680085, Email [email protected]
Introduction: Long-acting injectable pre-exposure prophylaxis (LA-PrEP) is a major biomedical advance for HIV prevention, but efficacy alone does not deliver population-level impact. Oral PrEP performed well in trials yet persisted poorly in practice, including among young women in KwaZulu-Natal, South Africa. LA-PrEP reduces daily pill burden and improves discretion, but introduces implementation demands that oral PrEP did not: appointment-based adherence, product-specific delivery needs, workforce and task-shifting limits, financing vulnerability, HIV testing requirements and pharmacokinetic-tail management.
Purpose: This paper develops the Access, Delivery Systems, Acceptability, Persistence and Transition Management (ADAPT) framework as a conceptual, practice-oriented model for LA-PrEP implementation in sub-Saharan Africa.
Approach: ADAPT was developed through structured narrative synthesis of peer-reviewed and grey literature on oral PrEP scale-up, cabotegravir long-acting (CAB-LA) and lenacapavir (LEN) efficacy, HIV service delivery, task shifting and implementation frameworks, combined with non-research program experience from facility-facing implementation support in Uganda and Sierra Leone. The model is not empirically validated and should be tested through Delphi consensus, stakeholder consultation, prospective implementation studies and program evaluation.
Discussion: ADAPT complements CFIR, RE-AIM, BLUPrInt and WHO guidance. Its contribution is product awareness, planner orientation and explicit recognition of Transition Management as a safety domain. It asks planners to align regulatory access, procurement and affordability; product-specific delivery systems; choice-based acceptability; appointment persistence; and protocols for stopping, switching and restarting.
Conclusion: For sub-Saharan Africa, safer and more equitable LA-PrEP rollout requires deliberate design across financing, service delivery, community governance, persistence systems and transition protocols. ADAPT offers a testable organizing model for this work.
Keywords: long-acting injectable PrEP, cabotegravir, lenacapavir, implementation science, HIV prevention, Sub-Saharan Africa
Introduction
In 2024, about 1.3 million people acquired HIV worldwide, a reminder of how far prevention still falls short after decades of investment.1 Sub-Saharan Africa carries much of that burden and faces the implementation challenge most directly. The task is to turn effective biomedical products into protection that is durable, equitable and safe for people whose risk is shaped by poverty, gendered vulnerability, stigma, criminalization, weak health systems and donor-dependent financing.
Long-acting injectable PrEP is one of the most important prevention advances of the past decade. Cabotegravir long-acting (CAB-LA), administered by intramuscular injection every eight weeks, showed an 88% lower risk of HIV infection than daily oral tenofovir disoproxil fumarate/emtricitabine (TDF/FTC) in HPTN 084 among cisgender women in sub-Saharan Africa (hazard ratio 0.12; 95% CI 0.05 to 0.31).2 PURPOSE 1 showed no HIV infections among the 2134 cisgender women who received twice-yearly subcutaneous lenacapavir (LEN) in South Africa and Uganda.3 WHO now recommends CAB-LA and LEN as additional HIV prevention options for people at substantial risk of HIV.4,5
The implementation lesson from oral PrEP is sobering. Oral TDF/FTC showed high efficacy in pivotal trials, especially when adherence was high,6,7 yet trial efficacy did not produce sustained population coverage. In KwaZulu-Natal, South Africa, approximately half of young women who initiated oral PrEP discontinued within 12 months.8 Among female sex workers in eThekwini, Durban, Rao et al reported persistence of 53% at one month and 9% after one year.9 Across sub-Saharan Africa, policy adoption, commodity access, provider behavior, stigma, service design and retention support shaped program outcomes as much as biomedical efficacy.10 The central problem was not the absence of an effective drug. It was the failure to build implementation systems capable of sustaining prevention.
LA-PrEP reduces some barriers that constrained oral PrEP. It removes daily pill-taking, improves discretion for clients who fear visible medication, and may suit people who prefer episodic contact with services rather than daily adherence. Qualitative data from HPTN 084 participants found that the desire for privacy and ease of use favored injectable PrEP, with freedom from daily pill-taking outweighing injection-related concerns.11
At the same time, LA-PrEP makes protection a function of the health system, and it does so differently for each product. The adherence unit shifts from the daily pill to the scheduled injection visit, so a client is protected by returning on time, not by remembering a dose. The two products then diverge in how that visit must be delivered. CAB-LA is given by intramuscular gluteal injection, may begin with an optional oral lead-in or proceed directly to injection, and is then repeated every eight weeks, which loads the burden onto injection capacity, privacy and frequent clinic contact.12 LEN is given by subcutaneous injection every 26 weeks after an oral loading dose, which lowers visit frequency but adds an oral phase and still depends on regulatory authorization, HIV testing, trained personnel, pharmacovigilance and national guidance. The route also decides who may deliver each product, because community health workers are authorized for subcutaneous but not intramuscular injection in many settings.
The products diverge most sharply at discontinuation. Each leaves a long pharmacokinetic (PK) tail, during which declining drug concentrations can be too low to prevent infection yet high enough to select resistance in a client who acquires HIV.13 The resistance differs by product, and the difference reaches into treatment. Because CAB-LA is an integrase strand transfer inhibitor (INSTI), breakthrough infection during recent or ongoing drug exposure, especially with delayed diagnosis, can select INSTI resistance and may complicate dolutegravir-based first-line therapy. In HPTN 083, rare infections during or soon after CAB-LA exposure were associated with delayed diagnosis and INSTI resistance; in HPTN 084, no INSTI resistance mutations were detected in CAB-LA-group participants with HIV infection.14,15 LEN is a first-in-class capsid inhibitor, so its tail risk is capsid-inhibitor resistance, which does not compromise current first-line therapy but warrants surveillance as capsid inhibitors move toward treatment use. These are not generic adherence problems. They are product-specific requirements, and they are why a framework for LA-PrEP must be aware of which product it is planning for. Without that awareness, LA-PrEP risks repeating the implementation failures of oral PrEP, now with the added consequence of population-level resistance that unmanaged tails can generate at scale.
This article proposes the Access, Delivery Systems, Acceptability, Persistence and Transition Management (ADAPT) framework for long-acting injectable PrEP implementation in sub-Saharan Africa. The purpose is not to replace existing implementation science frameworks. It is to provide a product-aware and planner-oriented model that helps policy-makers, HIV program managers, implementing partners, clinicians and community actors identify the operational conditions that must align for LA-PrEP to move from efficacy to population-level prevention impact. Its intended beneficiaries are the populations at highest HIV risk who stand to gain from well-implemented LA-PrEP.
Sub-Saharan African Service-Delivery Context
LA-PrEP will be introduced into health systems that typically combine vertical HIV programs, primary care, reproductive health services, community health worker networks and externally financed commodity supplies. Where physicians are scarce, many countries already rely on task sharing, and this matters for LA-PrEP: nurses, midwives and community health workers routinely deliver HIV testing, antiretroviral therapy follow-up, contraception, immunization and community-based prevention.16,17
Provision is uneven, however. Urban and high-volume clinics tend to have trained staff, laboratory access and working commodity systems, but may offer little privacy or sit behind high transport costs. Peripheral facilities are often trusted locally yet lack secure storage, reliable stock management or staff authorized to give intramuscular injections. For adolescent girls and young women, sex workers, men who have sex with men, transgender people and people who inject drugs, services are further shaped by stigma, confidentiality concerns and legal risk.10,18 These are not background details. They decide whether any LA-PrEP framework can work in practice, so a useful framework must engage them rather than assume them away.
Approach and Framework Development
This article is a commentary and conceptual framework paper. It reports no empirical study, recruitment, sample-size calculation, primary data or statistical analysis, so reporting standards for empirical research do not apply. ADAPT was developed through a structured narrative synthesis designed to identify the implementation determinants that are specific to, or especially consequential for, long-acting injectable PrEP in sub-Saharan Africa.
The synthesis drew on four evidence streams. The first was peer-reviewed evidence on oral PrEP implementation, persistence and prevention choice in African settings. The second was clinical and pharmacokinetic evidence for CAB-LA and LEN, including pivotal trial data and the literature on the pharmacokinetic tail and resistance risk. The third was the implementation science frameworks and program tools used in HIV prevention, including CFIR, RE-AIM, BLUPrInt and WHO guidance. The fourth was non-research program experience from facility-facing implementation support in Uganda and Sierra Leone, covering storage and stock management, workforce scope of practice, privacy for injection, service integration and the feasibility of community delivery.
Sources were identified through PubMed/MEDLINE and Google Scholar, together with normative and technical guidance from WHO, program materials from AVAC and PrEPWatch, UNAIDS reports, Medicines Patent Pool information and public regulatory or access statements from product developers and global health agencies. Search concepts included long-acting injectable PrEP, cabotegravir, lenacapavir, oral PrEP persistence, PrEP choice, HIV prevention implementation, task shifting, sub-Saharan Africa, pharmacokinetic tail, integrase inhibitor resistance, product storage conditions, family planning integration and implementation science frameworks.
A domain was retained when it met three criteria: it represented a plausible bottleneck between clinical efficacy and population-level impact; it carried operational decisions that planners could act on before or during rollout; and it addressed a feature that existing frameworks treated generically or did not operationalize for LA-PrEP. ADAPT should therefore be read as a practice-oriented, hypothesis-generating model. It requires validation through Delphi consensus, stakeholder consultation, prospective implementation studies, comparative program evaluation and real-time learning across diverse settings.
Why Existing Frameworks are Useful but Insufficient for LA-PrEP Planning
Existing frameworks remain valuable. CFIR offers a broad taxonomy of implementation determinants across intervention characteristics, inner and outer setting, individuals and process.19 RE-AIM helps programs evaluate reach, effectiveness, adoption, implementation and maintenance.20 BLUPrInt is a practical PrEP program builder, and WHO guidance gives the essential clinical and programmatic recommendations for CAB-LA and LEN.4,5,21 These tools should continue to guide planning, and ADAPT is meant to complement them.
The gap is specific. CFIR does not distinguish intramuscular from subcutaneous delivery, nor say which determinants are rate-limiting for a modality-specific product. RE-AIM is built to evaluate performance, not to guide design. BLUPrInt does not differentiate product-specific delivery requirements and does not address the PK tail. WHO guidance is essential but product-specific and treats transition only briefly. A program manager choosing between district hospitals, family planning clinics and outreach sites needs a framework that separates intramuscular from subcutaneous products, links infrastructure to persistence, treats the appointment as the adherence unit, and makes discontinuation a core safety function. A national prevention lead choosing between CAB-LA, LEN or both needs to weigh storage, initiation options, visit schedules, task-shifting feasibility, affordability, switching pathways and resistance implications side by side.
ADAPT adds three things. It is product-aware, asking how CAB-LA and LEN differ across access, route, workforce, visit burden and transition risk. It is planner-oriented, turning determinants into early decisions and measurable indicators. And it makes Transition Management a distinct domain, because discontinuation, missed injections, switching and re-initiation carry pharmacological and population-level risks that do not fit standard retention or maintenance constructs. The added value is therefore not a new taxonomy but a planning lens that makes three things visible at the point of decision: that binding constraints differ by product, that persistence is a property of the delivery system rather than of the individual, and that the post-discontinuation period is a discrete safety domain with population-level consequences. Table 1 positions ADAPT against these tools and notes their validation status.
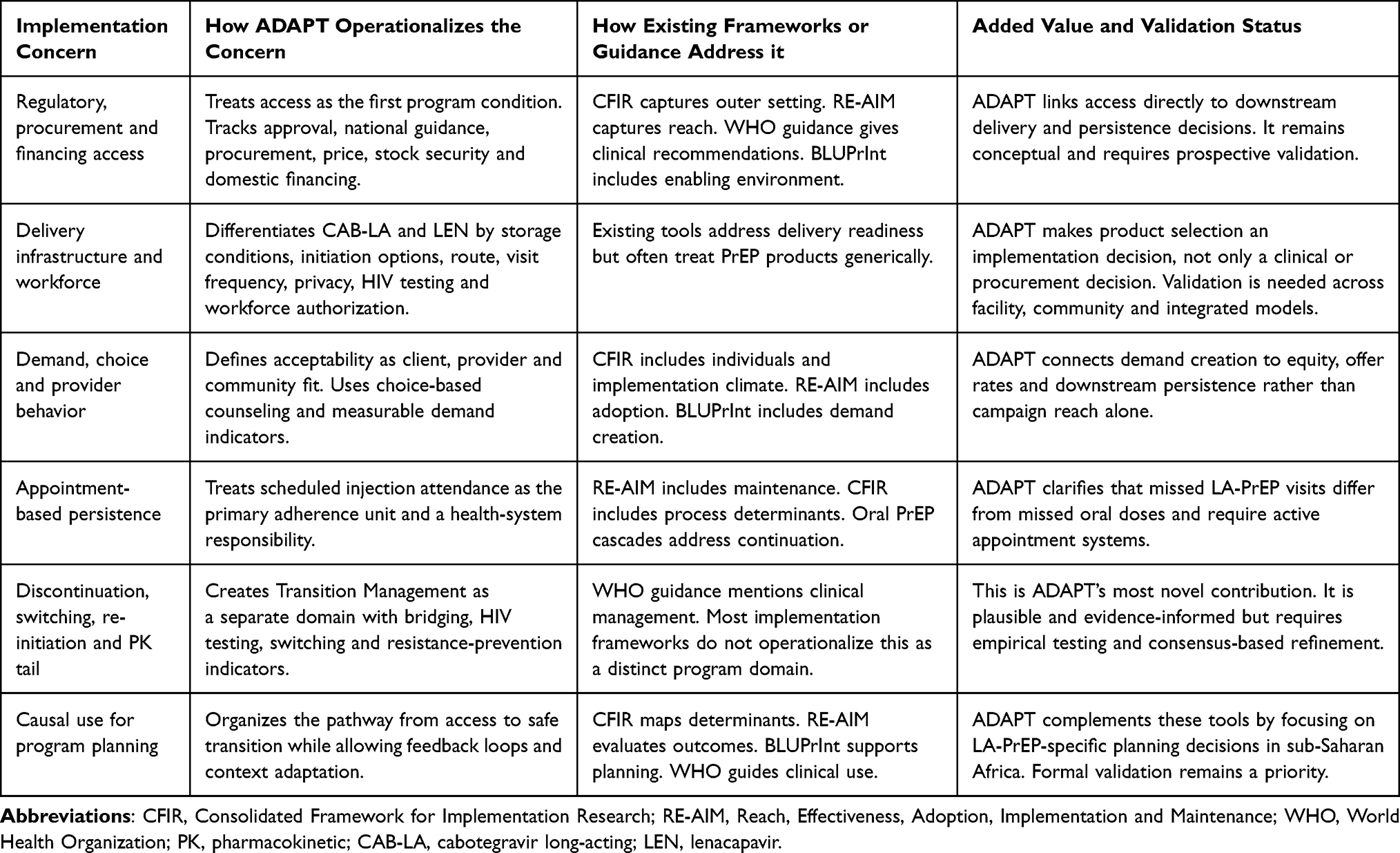 |
Table 1 Positioning ADAPT Against Existing Implementation Science Frameworks and Tools for PrEP |
The ADAPT Framework
ADAPT comprises five interlinked domains: Access, Delivery Systems, Acceptability, Persistence and Transition Management. They describe a dominant implementation pathway, not a rigid sequence, and feedback between them is expected. Poor acceptability can weaken political demand and so narrow access. Delivery failures undermine persistence. Weak transition protocols erode provider confidence and community trust. The framework is best read as a heuristic that shows where implementation tends to succeed or fail, not as a deterministic chain. Monitoring and evaluation, implementation research and community engagement cut across all five domains (Figure 1).
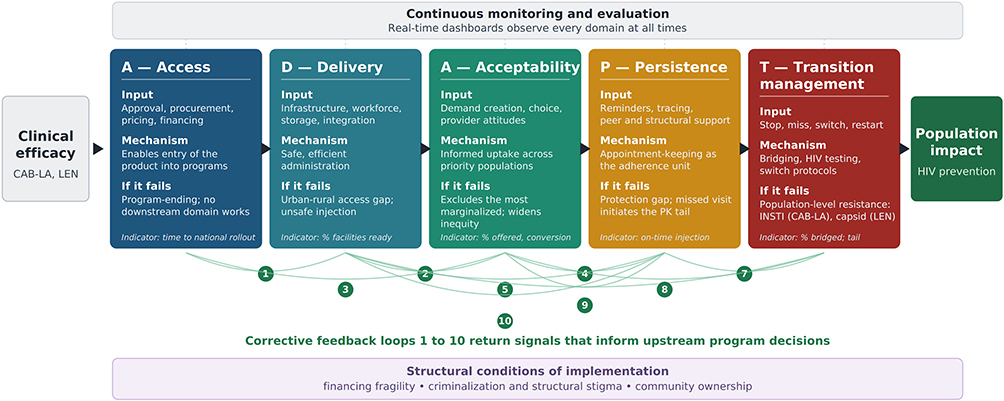 |
Figure 1 Access, Delivery Systems, Acceptability, Persistence and Transition Management (ADAPT) framework for long-acting injectable PrEP implementation in sub-Saharan Africa. The framework presents five interlinked implementation domains through which long-acting injectable PrEP may translate from clinical efficacy into population-level HIV prevention impact. Each domain carries an input, a mechanism, an outcome and a failure consequence, together with measurable program indicators. The figure should be read as a practical, product-aware heuristic rather than a strictly linear or deterministic sequence, and feedback loops are expected across domains, so that, for example, persistence data inform delivery-system and acceptability redesign. Transition Management is a distinctive contribution of ADAPT and is not explicitly operationalized as a discrete programmatic domain in existing PrEP implementation frameworks. Community engagement, monitoring and evaluation, implementation research and real-time dashboards cut across all domains. Abbreviations: CAB-LA, cabotegravir long-acting; INSTI, integrase strand transfer inhibitor; LEN, lenacapavir; PK, pharmacokinetic. |
ADAPT’s central claim is that LA-PrEP turns adherence from an individual behavior into a health-system function. With oral PrEP, a missed dose is an individual failure with individual consequences. With LA-PrEP, a missed appointment is at once a protection failure and a potential population pharmacovigilance event, because it starts a PK tail. Responsibility for protection therefore shifts from the individual to the delivery system, which must secure timely injections and safe transitions, and implementation should be built for that shift from the outset.
Because CAB-LA and LEN impose different delivery, workforce, visit-schedule and tail-management requirements, Table 2 summarizes the product-specific implementation features that planners need to consider before choosing one product or introducing both.
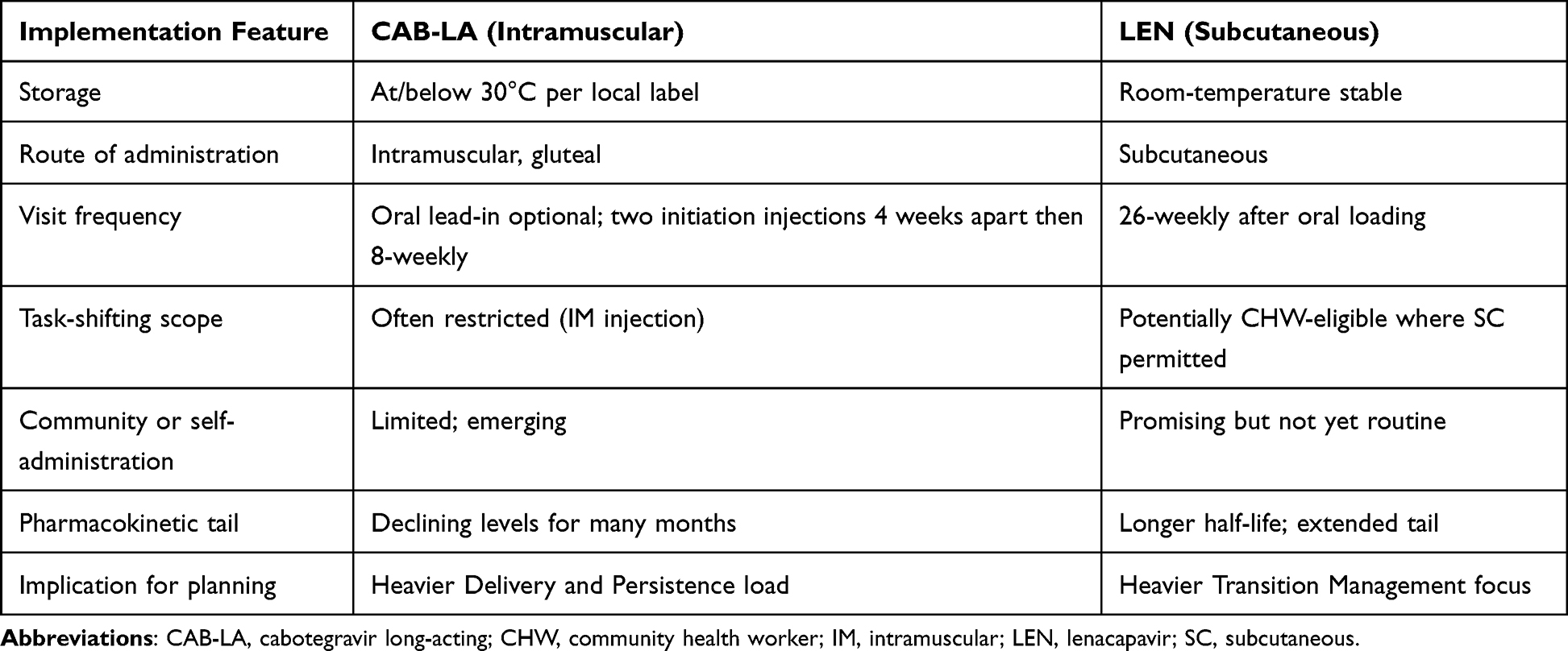 |
Table 2 Product-Aware Implementation Comparison Between Cabotegravir Long-Acting (CAB-LA) and Lenacapavir (LEN) |
Access
Access refers to the policy, regulatory, procurement and financing conditions that determine whether anyone can start LA-PrEP. For CAB-LA and LEN it begins with national regulatory approval, inclusion in guidelines, procurement pathways, commodity forecasting, essential medicines listing, price negotiation and financing. WHO recommendations confer legitimacy, but rollout depends on national budgets, supply chains and country-level decisions.4,5 Medicines Patent Pool licensing for CAB-LA and royalty-free licensing for lenacapavir in high-incidence countries open routes toward generic affordability.22,23
Access is not solved by involving funders alone. Financing matters, but cost-effectiveness turns on product price, negotiated procurement, generic availability, wastage, delivery cost, visit frequency, incidence in the target population, competing options and the cost of missed opportunities. CAB-LA is not cost-effective at current low-income-country prices,24 and modeling for Eastern and Southern Africa suggests the annual per-person cost must fall well below present levels to meet conventional value benchmarks, with thresholds of roughly one to two hundred US dollars per person-year in higher-incidence settings and far less where incidence is lower.25 The binding constraints are therefore price and delivery cost, not willingness to pay. Donor money can speed introduction, but dependence on external procurement is fragile: recent United States funding disruptions hit prevention, treatment and care across parts of East and Southern Africa and showed how fast platforms weaken when financing shifts.26 ADAPT therefore treats access as a structural, quantitative condition, with affordability as a design parameter rather than a matter of donor goodwill.
Priority indicators include time from WHO recommendation or regulatory approval to national guidance, proportion of target districts with product availability, cost per protected person-year, stock-out frequency, domestic co-financing share, and whether oral PrEP remains available at every LA-PrEP delivery site.
Delivery Systems
Delivery Systems are the infrastructure, workforce, integration and safety processes needed to administer LA-PrEP, and this is where the products differ most. CAB-LA requires intramuscular gluteal injection by trained providers, private injection space and a schedule of two initiation doses four weeks apart followed by an injection every eight weeks. Its storage is undemanding where local product information permits room temperature, so refrigeration is not the binding requirement; oral lead-in may be used to check tolerability, or programs may proceed directly to injection.12 LEN needs an oral loading dose and then a subcutaneous injection every 26 weeks, which means fewer visits, but its rollout still requires trained staff, HIV testing at initiation and continuation, pharmacovigilance, commodity management and national protocols.4,5
Facility-facing work in Uganda and Sierra Leone showed wide heterogeneity. Busy urban sites may have reliable storage and stock-management systems but no private injection space, while rural centers may offer privacy but lack reliable stock management, secure storage or authorized staff. Because CAB-LA does not depend on refrigeration, the real bottleneck moves to injection capacity, product accountability, the HIV testing workflow, privacy and appointment systems. The distinction is practical: programs that wrongly assume CAB-LA needs a cold chain may over-centralize it and add avoidable travel barriers. Lenacapavir’s subcutaneous route and twice-yearly schedule cut visit and workforce burden, though not the need for trained staff, testing and pharmacovigilance. Product awareness extends to drug interactions at the point of care. LEN undergoes only minor metabolism, but moderate and strong CYP3A inducers, including rifamycins used for tuberculosis and some anticonvulsants, can reduce LEN concentrations enough to compromise protection. Where tuberculosis and HIV often coincide, screening for these co-medications belongs in routine initiation and continuation counseling, not only in specialist review.
HIV testing is part of the delivery system, not a precondition standing outside it. Every visit, at initiation and continuation, depends on confirming HIV-negative status, and the choice of test decides whether that step is feasible at the point of care. Rapid diagnostic tests can be done by lower-cadre staff, return a result within the visit and need no laboratory, which makes same-day initiation possible even at peripheral sites. Laboratory-based tests, including nucleic acid tests, detect infection earlier but require sample transport, equipment and turnaround that most decentralized settings cannot sustain, and the delay is both an access barrier and a missed-injection risk. A rapid-test algorithm is therefore the realistic default across most of sub-Saharan Africa, with more complex testing kept for resolving uncertain results rather than gating access. The detailed algorithms lie beyond this article; the principle is that testing should match the delivery setting, not constrain it.
Task shifting is central to delivery design. Across the region, task sharing has let nurses and non-physician cadres extend HIV testing, antiretroviral therapy follow-up and maternal health services under national protocols,16,17 and subcutaneous DMPA self-injection (DMPA-SC) has been delivered acceptably by lower-cadre providers and by clients themselves.27 The same logic may help LA-PrEP, but it cannot be assumed across products, because intramuscular and subcutaneous injection can fall under different scope-of-practice rules. Where community health workers may give subcutaneous but not intramuscular injections, that rule alone favors lenacapavir for community-level delivery. Planning should separate established delivery requirements from future possibilities such as broader community delivery or self-administration, which are promising but still emerging and need specific evidence, regulatory approval and safety monitoring before routine use.
Family planning integration is promising but needs care. It suits adolescent girls and young women, women seeking reproductive health care and clients already using injectable contraception, because the service rhythm, counseling and privacy needs partly overlap.18 It should not be the only model. For sex workers, men who have sex with men, transgender people and people who inject drugs, such settings may be irrelevant, stigmatizing or unsafe. Integration should therefore be opt-in and confidential, and paired with peer-led, community-based or discreet facility and telehealth options for those who avoid mainstream reproductive health services.
Priority indicators include the proportion of facilities meeting product-specific readiness standards, the number of trained and supervised cadres by product route, temperature-storage and stock-management readiness, HIV testing availability before injection visits, privacy readiness, median client travel time, and the proportion of services integrated with client-preferred platforms.
Acceptability
Acceptability is whether communities, clients, providers and policy actors see LA-PrEP as appropriate, safe, desirable and feasible. It spans demand creation, prevention choice, provider behavior, counseling quality, privacy, stigma and community trust, and it cannot be inferred from efficacy. A product can work biologically yet fail socially if people distrust injections, fear stigma, cannot attend discreetly or meet judgmental providers. Provider bias documented during oral PrEP rollout restricted access for adolescents and young women, and will do the same for LA-PrEP unless training addresses it directly.
Choice is the foundation of acceptability. LA-PrEP should be offered within a prevention menu that may include daily oral PrEP, event-driven PrEP where appropriate, the dapivirine vaginal ring, condoms, harm reduction, and testing and treatment for partners. Evidence from the CATALYST and DREAMS PrEP Choice studies suggests that genuine choice improves both uptake and continuation, because people can pick the method that fits their lives.28,29 Demand creation should be tailored by population: peer-led for adolescent girls and young women, peer-educator networks for sex workers, and discreet facility or telehealth models for men who have sex with men where same-sex relations are criminalized.
Demand creation needs measurable benchmarks, not generic social media activity. Programs can track awareness, accurate recall of injection schedules, referral completion, eligibility screening, offer rate, uptake among eligible clients, reasons for refusal, misinformation, satisfaction, and differences by age, sex, location and key-population status. Reach without uptake or attendance is not enough. Acceptability failure does not fall evenly; it excludes the most marginalized and widens existing inequities, so ADAPT ties acceptability metrics to downstream persistence and equity. Priority indicators include the share of eligible clients offered LA-PrEP, the share choosing each option after counseling, satisfaction scores, the proportion of providers completing stigma-reduction and product-specific training, and uptake among priority populations.
Persistence
Persistence is sustained engagement with LA-PrEP over time, and it is the central implementation challenge, because LA-PrEP makes adherence a health-system function. With oral PrEP the adherence unit is the daily pill, and a missed dose can be taken the next day. With LA-PrEP the unit is the scheduled injection, and a missed one opens an immediate protection gap and starts the PK tail. Each missed appointment is therefore at once an adherence failure and a pharmacovigilance event.
The difference between CAB-LA and LEN matters. CAB-LA’s more frequent visits raise cumulative exposure to transport costs, waiting time, stigma, lost wages and missed appointments. LEN’s twice-yearly subcutaneous schedule, after the oral loading dose, lowers that burden, but its visits can still be missed where reminders, tracking and re-engagement are weak. Lower visit frequency is not automatic persistence. Early program experience suggests that structural design, rather than individual motivation alone, may be a main driver of retention, although this remains unevaluated and should be tested prospectively. The oral PrEP record points the same way: persistence among female sex workers fell to 53% at one month and 9% at twelve months, confirming that initiation without structural retention support does not yield durable coverage.9
Persistence support should be designed before rollout. Strategies proven in antiretroviral therapy retention include client-preferred reminders, appointment windows, active tracing of missed visits, peer navigators, injection-buddy models, differentiated service delivery, transport support for high-barrier clients, extended hours, removal of structural barriers and non-judgmental care.30 Co-locating injections within existing healthcare-seeking patterns helps further. Priority indicators include on-time injection coverage at 6 and 12 months, median delay after a missed injection, the share of missed clients contacted within a defined period, the share re-engaged, reasons for discontinuation, and persistence broken down by product, age, sex, district, delivery model and population group.
Transition Management
Transition Management is the most distinctive ADAPT domain. It covers the protocols and systems that protect clients and programs when LA-PrEP is stopped, interrupted, switched or restarted. It earns separate status because it links individual discontinuation to population-level pharmacovigilance and resistance prevention, and because no existing PrEP framework operationalizes it as a discrete domain.
After discontinuation, cabotegravir falls away over many months, and lenacapavir’s longer half-life leaves an even longer tail.13 Across that window, drug levels can be too low to prevent infection yet high enough to select resistance if HIV is acquired, and the resistance differs by product. Breakthrough infection during recent or ongoing CAB-LA exposure, especially with delayed diagnosis, can select INSTI resistance, as documented in HPTN 083; no INSTI resistance mutations were detected in HPTN 084;14,15 LEN’s corresponding risk is capsid-inhibitor resistance. The number of observed INSTI resistance events was small, but the programmatic stakes at scale are important. A low per-person probability of INSTI resistance, multiplied across large numbers of users, could complicate the dolutegravir-based regimens that anchor first-line therapy, so CAB-LA scale-up can have implications beyond prevention. Capsid-inhibitor resistance does not yet compromise standard therapy, but it warrants surveillance as capsid inhibitors enter the treatment pipeline. Either way, the post-discontinuation period is a program-level safety domain, not an individual footnote.
Transition Management spans four practical scenarios. Clients who choose to stop need counseling, HIV testing and oral PrEP bridging with TDF/FTC or TDF/3TC while exposure risk continues. Clients who miss an injection need rapid tracing, testing and clear criteria for delayed dosing or re-initiation. Clients switching between CAB-LA, LEN, oral PrEP or the dapivirine ring need product-specific overlap guidance as the toolkit expands. And clients returning after a long gap need testing strategies that avoid starting LA-PrEP during undetected infection.
Testing strategy is itself part of safe transition. The same long tail that creates resistance risk can blunt or delay the serological response to a new infection, so a reactive or inconclusive result after recent LA-PrEP calls for repeat testing and confirmation rather than reassurance, and a returning client needs an approach designed to rule out infection acquired during the tail. The trick is to do this without making complex laboratory testing a routine gate, which would rebuild the access barriers rapid testing removes.
In every scenario, oral PrEP must be available at each LA-PrEP site, because managing stopping and switching safely is population pharmacovigilance, not operational detail. The line from persistence is precise: retention asks whether a client stays in care, transition asks whether stopping, switching or restarting happens safely. It requires written national protocols, provider training, oral PrEP on hand, pharmacovigilance reporting, laboratory pathways where indicated and routine indicators. The landscape will keep moving; longer-acting products, including the once-yearly lenacapavir now in early study, would shift the balance between domains further and make transition management more important, not less.31 Priority indicators include the share of discontinuers assessed for ongoing risk, the share given oral PrEP bridging when indicated, time from missed injection to contact, the tail-period seroconversion rate, resistance-testing completion where available, and the share of re-initiations that follow national protocol.
How ADAPT Can Operate in Practice
ADAPT is built for several actor groups. National policy-makers can use it to decide which products to introduce, where to start, how to finance them and what protocols must exist before scale-up. Program managers can use it to assess facility readiness, workforce, appointment systems, demand creation, transition protocols and equity risk. Facility teams can use it to organize service flow, counseling, HIV testing, injection, reminders and missed-visit tracking. Community organizations can use it to co-design demand creation, monitor stigma, support clients and hold programs accountable for confidentiality and respectful care.
A practical ADAPT planning cycle has five steps. First, assess access and readiness: regulatory status, price, procurement, facility readiness, workforce authorization, oral PrEP availability and HIV testing capacity. Second, choose delivery models by population and geography rather than imposing one model nationally. Third, co-design counseling and demand creation with affected communities. Fourth, build persistence systems before the first injection, including reminder preferences and missed-visit escalation. Fifth, approve transition protocols, including oral PrEP bridging and switching procedures, before scale-up. The cycle guards against the common error of judging success by initiation alone. ADAPT treats success as a chain of linked outcomes: equitable access, safe delivery, informed choice, sustained protection and safe transition. Table 3 maps each domain to its decisions, actors, indicators and immediate actions.
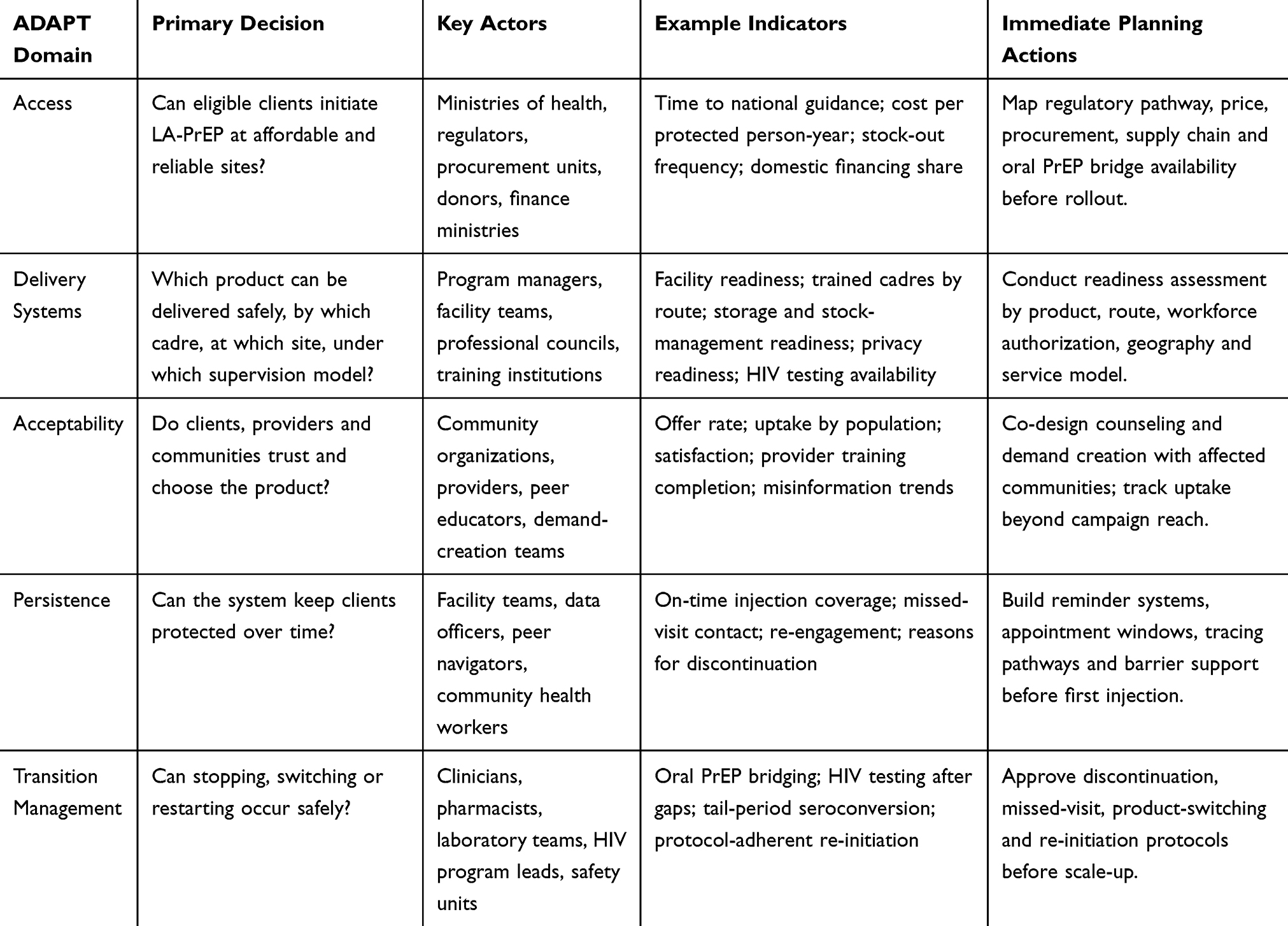 |
Table 3 Practical Use of ADAPT Domains During LA-PrEP Planning and Monitoring |
Monitoring, Evaluation and Implementation Research
Monitoring and evaluation should run across all five domains. Programs should not wait for end-line evaluations to learn that stock systems failed, that providers withheld LA-PrEP from adolescents, that clients missed injections because transport cost too much, or that discontinuers went without oral PrEP bridging. Real-time dashboards can link facility readiness, commodity status, client flow, appointment adherence, missed-visit tracing and transition outcomes, so managers act early rather than in hindsight. Community engagement is not only demand creation; it is the basis of implementation legitimacy. Community advisory boards, peer-led quality monitoring and participatory feedback strengthen every domain.29
Implementation research should test whether ADAPT predicts outcomes and improves planning beyond generic approaches. Five questions follow from the framework. First, which domains most strongly predict persistence failure, and how do delivery-system design and persistence infrastructure interact to shape retention across settings? Second, which pre-injection HIV-testing strategy best balances resistance prevention against access, especially for lenacapavir’s twice-yearly schedule? Third, how do outcomes differ across facility-based, community-based and family-planning-integrated models, and which configurations best close the urban-rural gap? Fourth, what are the real-world rates of product-specific tail resistance under programmatic conditions, INSTI for cabotegravir and capsid-inhibitor for lenacapavir, and which discontinuation protocols best minimize population-level risk? Fifth, how do CAB-LA, LEN and oral PrEP compare on cost-effectiveness once realistic persistence replaces trial-level efficacy? Validation should be prospective and participatory: Delphi consensus to refine domains and indicators, stakeholder consultation to test the framework against lived realities, and hybrid effectiveness-implementation studies embedded in existing programs as the most efficient design.
Limitations
ADAPT is a conceptual framework, not an empirically validated tool. Its domains come from narrative synthesis, existing frameworks, product characteristics, oral PrEP experience and non-research program experience, and that experience was drawn from facility-facing implementation support in only two countries, which limits generalizability. The model should be read as a testable, hypothesis-generating structure, not a proven causal instrument.
Product evidence and regulatory pathways are also moving quickly. Lenacapavir experience is still early in many African settings, and some delivery propositions, including broader community delivery and future self-administration, remain implementation hypotheses until authorized and evaluated. Sub-Saharan Africa is not one setting; legal environments, workforce rules, donor dependence, epidemiology, community trust and infrastructure vary across and within countries. Finally, ADAPT complements rather than replaces CFIR, RE-AIM, BLUPrInt and WHO guidance. Its value is practical organization around LA-PrEP-specific decisions, and it should be used alongside broader implementation tools, clinical guidance and community-led accountability.
Conclusion
Long-acting injectable PrEP offers exceptional prevention potential, but efficacy alone does not deliver population-level impact. Oral PrEP in sub-Saharan Africa showed that initiation without sustained support yields partial protection and unequal reach. LA-PrEP adds complexity, because appointment-based adherence, product-specific delivery, financing fragility and pharmacokinetic tail management make the health system the primary agent of prevention, with the further risk that unmanaged residual drug exposure may contribute to antiretroviral resistance at scale, including CAB-LA-associated INSTI resistance with implications for first-line treatment.
ADAPT answers this by organizing LA-PrEP planning around Access, Delivery Systems, Acceptability, Persistence and Transition Management. Its specific contribution is to tie product choice to delivery realities, to treat appointment persistence as a system function, and to make safe discontinuation and switching central to prevention programming. It complements, rather than replaces, the established frameworks that guide rigorous evaluation. The model is conceptual and requires validation, but it gives planners a practical structure for asking the right questions before scale-up. For sub-Saharan Africa, the aim is not only to introduce LA-PrEP, but to introduce it in ways that are affordable, trusted, safe, equitable and durable. ADAPT offers a way to test whether implementation can match the promise of the science.
Abbreviations
ADAPT, Access, Delivery Systems, Acceptability, Persistence and Transition Management; CAB-LA, cabotegravir long-acting; CFIR, Consolidated Framework for Implementation Research; DMPA-SC, subcutaneous depot medroxyprogesterone acetate; HIV, human immunodeficiency virus; HPTN, HIV Prevention Trials Network; INSTI, integrase strand transfer inhibitor; LA-PrEP, long-acting injectable pre-exposure prophylaxis; LEN, lenacapavir; PK, pharmacokinetic; PrEP, pre-exposure prophylaxis; RE-AIM, Reach, Effectiveness, Adoption, Implementation and Maintenance; TDF/FTC, tenofovir disoproxil fumarate/emtricitabine; TDF/3TC, tenofovir disoproxil fumarate/lamivudine; WHO, World Health Organization.
Data Sharing Statement
Data sharing is not applicable to this article because no datasets were generated or analyzed.
Acknowledgments
The authors are grateful to the communities, health workers and program managers across Uganda and Sierra Leone whose operational experiences informed the development of this framework. The populations most affected by HIV, including adolescent girls and young women, sex workers, men who have sex with men, transgender people and people who inject drugs, must be central to how the ADAPT framework is operationalized in their contexts.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No specific funding was received for this work. No funder or sponsor had any role in the conception, development, writing, review, approval or decision to submit this manuscript.
Disclosure
The authors report no financial or non-financial competing interests in this work.
References
1. UNAIDS. AIDS, crisis and the power to transform: UNAIDS global AIDS update 2025. Geneva: Joint United Nations Programme on HIV/AIDS; 2025. Available from: https://www.unaids.org/en/resources/documents/2025/2025-global-aids-update.
2. Delany-Moretlwe S, Hughes JP, Bock P, et al. Cabotegravir for the prevention of HIV-1 in women: results from HPTN 084, a phase 3, randomised clinical trial. Lancet. 2022;399(10337):1779–12. doi:10.1016/S0140-6736(22)00538-4
3. Bekker LG, Das M, Abdool Karim Q, et al. Twice-yearly lenacapavir or daily F/TAF for HIV prevention in cisgender women. N Engl J Med. 2024;391(13):1179–1192. doi:10.1056/NEJMoa2407001
4. World Health Organization. Guidelines on long-acting injectable cabotegravir for HIV prevention. Geneva: World Health Organization; 2022. Available from: https://www.who.int/publications/i/item/9789240054097.
5. World Health Organization. Guidelines on lenacapavir for HIV prevention and testing strategies for long-acting injectable pre-exposure prophylaxis (PrEP). Geneva: World Health Organization; 2025. Available from: https://www.who.int/publications/i/item/9789240111608.
6. Grant RM, Lama JR, Anderson PL, et al. Preexposure chemoprophylaxis for HIV prevention in men who have sex with men. N Engl J Med. 2010;363(27):2587–2599. doi:10.1056/NEJMoa1011205
7. Baeten JM, Donnell D, Ndase P, et al. Antiretroviral prophylaxis for HIV prevention in heterosexual men and women. N Engl J Med. 2012;367(5):399–410. doi:10.1056/NEJMoa1108524
8. Mansoor LE, Lewis L, Naicker CL, et al. Prospective study of oral pre-exposure prophylaxis initiation and adherence among young women in KwaZulu-Natal, South Africa. J Int AIDS Soc. 2022;25(7):e25957. doi:10.1002/jia2.25957
9. Rao A, Mhlophe H, Comins C, et al. Persistence on oral pre-exposure prophylaxis (PrEP) among female sex workers in eThekwini, South Africa, 2016–2020. PLoS One. 2022;17(3):e0265434. doi:10.1371/journal.pone.0265434
10. Irungu EM, Baeten JM. PrEP rollout in Africa: status and opportunity. Nat Med. 2020;26(5):655–664. doi:10.1038/s41591-020-0872-x
11. Tolley EE, Bula A, Chitukuta M, et al. Preferences for oral and injectable PrEP among qualitative sub-study participants in HPTN 084. PLoS One. 2024;19(10):e0309811. doi:10.1371/journal.pone.0309811
12. ViiV Healthcare. APRETUDE cabotegravir pre-exposure prophylaxis (PrEP): international product information. Version GDS06/IPI06. Bryanston, South Africa: GlaxoSmithKline South Africa (Pty) Ltd; 2024. Available from: https://assets.gskstatic.com/pharma/PM-PI_portal/Uganda/apretude_suspension_for_injection_ug.pdf.
13. Landovitz RJ, Li S, Grinsztejn B, et al. Safety, tolerability, and pharmacokinetics of long-acting injectable cabotegravir in low-risk HIV-uninfected individuals: HPTN 077, a phase 2a randomized controlled trial. PLoS Med. 2018;15(11):e1002690. doi:10.1371/journal.pmed.1002690
14. Eshleman SH, Fogel JM, Piwowar-Manning E, et al. Characterization of human immunodeficiency virus (HIV) infections in women who received injectable cabotegravir or tenofovir disoproxil fumarate/emtricitabine for HIV prevention: HPTN 084. J Infect Dis. 2022;225(10):1741–1749. doi:10.1093/infdis/jiab576
15. Marzinke MA, Grinsztejn B, Fogel JM, et al. Characterization of human immunodeficiency virus (HIV) infection in cisgender men and transgender women who have sex with men receiving injectable cabotegravir for HIV prevention: HPTN 083. J Infect Dis. 2021;224(9):1581–1592. doi:10.1093/infdis/jiab152
16. World Health Organization. Optimizing health worker roles to improve access to key maternal and newborn health interventions through task shifting. WHO recommendations. Geneva: World Health Organization; 2012. Available from: https://www.who.int/publications/i/item/9789241504843.
17. Kredo T, Adeniyi FB, Bateganya M, Pienaar ED. Task shifting from doctors to non-doctors for initiation and maintenance of antiretroviral therapy. Cochrane Database Syst Rev. 2014;2014(7):CD007331. doi:10.1002/14651858.CD007331.pub3
18. Celum CL, Delany-Moretlwe S, Baeten JM, et al. HIV pre-exposure prophylaxis for adolescent girls and young women in Africa: from efficacy trials to delivery. J Int AIDS Soc. 2019;22(Suppl 4):e25298. doi:10.1002/jia2.25298
19. Damschroder LJ, Reardon CM, Widerquist MAO, Lowery J. The updated consolidated framework for implementation research based on user feedback. Implement Sci. 2022;17(1):75. doi:10.1186/s13012-022-01245-0
20. Glasgow RE, Vogt TM, Boles SM. Evaluating the public health impact of health promotion interventions: the RE-AIM framework. Am J Public Health. 1999;89(9):1322–1327. doi:10.2105/AJPH.89.9.1322
21. PrEPWatch. BLUPrInt PrEP program builder. 2025. Available from: https://www.prepwatch.org/resources/bluprint-prep-program-builder/.
22. Medicines Patent Pool. Cabotegravir long-acting (LA) for HIV pre-exposure prophylaxis (PrEP) licence. Geneva: Medicines Patent Pool; 2025. Available from: https://medicinespatentpool.org/licence-post/cabotegravir-long-acting-la-for-hiv-pre-exposure-prophylaxis-prep.
23. Gilead Sciences. Gilead signs royalty-free voluntary licensing agreements with six generic manufacturers to increase access to lenacapavir for HIV prevention in high-incidence, resource-limited countries. Foster City, CA: Gilead Sciences; 2024. Available from: https://www.gilead.com/news/news-details/2024/gilead-signs-royalty-free-voluntary-licensing-agreements-with-six-generic-manufacturers-to-increase-access-to-lenacapavir-for-hiv-prevention-in-high-incidence-resource-limited-countries.
24. Jamieson L, Johnson LF, Nichols BE, et al. Relative cost-effectiveness of long-acting injectable cabotegravir versus oral pre-exposure prophylaxis in South Africa based on the HPTN 083 and HPTN 084 trials: a modelled economic evaluation and threshold analysis. Lancet HIV. 2022;9(12):e857–e867. doi:10.1016/S2352-3018(22)00251-X
25. Kaftan D, Sharma M, Resar D, et al. Cost thresholds for anticipated long-acting HIV pre-exposure prophylaxis products in Eastern and Southern Africa: a mathematical modelling study. J Int AIDS Soc. 2025;28(2):e26427. doi:10.1002/jia2.26427
26. UNAIDS. Impact of US funding cuts on HIV programmes in East and Southern Africa. Geneva: Joint United Nations Programme on HIV/AIDS; 2025. Available from: https://www.unaids.org/en/resources/presscentre/featurestories/2025/march/20250331_ESA-region_fs.
27. Cover J, Lim J, Namagembe A, Tumusiime J, Drake JK, Cox CM. Acceptability of contraceptive self-injection with DMPA-SC among adolescents in Gulu District, Uganda. Int Perspect Sex Reprod Health. 2017;43(4):153–162. doi:10.1363/43e5117
28. Fonner VA, Irungu E, Conlon M, et al. PrEP choice in the real world: results of a prospective cohort study describing uptake and use patterns of oral PrEP and the dapivirine vaginal ring among women in sub-Saharan Africa. J Int AIDS Soc. 2025;28(Suppl 2):e26457. doi:10.1002/jia2.26457
29. Naidoo NP, Mthimkulu N, Jama N, et al. Community PrEP delivery for adolescent girls and young women: insights from the DREAMS PrEP choice study in Johannesburg, South Africa. Front Reprod Health. 2025;7:1474067. doi:10.3389/frph.2025.1474067
30. Haberer JE, Sabin L, Amico KR, et al. Improving antiretroviral therapy adherence in resource-limited settings at scale: a discussion of interventions and recommendations. J Int AIDS Soc. 2017;20(1):21371. doi:10.7448/IAS.20.1.21371
31. Jogiraju V, Pawar P, Yager J, et al. Pharmacokinetics and safety of once-yearly lenacapavir: a Phase 1, open-label study. Lancet. 2025;405(10485):1147–1154. doi:10.1016/S0140-6736(25)00405-2
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
An Evaluation a PrEP-Focused HIV Prevention Intervention Tailored for Individuals with Opioid Use Disorder and Cognitive Dysfunction
Mistler CB, Huedo-Medina TB, Shrestha R, Gunstad J, Zelenev A, Copenhaver MM
Neuropsychiatric Disease and Treatment 2025, 21:1235-1248
Published Date: 24 June 2025