Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Between Personality Traits and Postpartum Depression: The Mediated Role of Maternal Self-Efficacy
Authors Han L, Zhang J, Yang J, Yang X, Bai H
Received 26 October 2021
Accepted for publication 9 March 2022
Published 19 March 2022 Volume 2022:18 Pages 597—609
DOI https://doi.org/10.2147/NDT.S346327
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yu-Ping Ning
Lingli Han,1 Ji Zhang,2 Jingxuan Yang,1 Xiaoyu Yang,1 Hua Bai1
1The Third Affiliated Hospital, Zhengzhou University, Zhengzhou, Henan, People’s Republic of China; 2Zhengzhou Maternal and Child Health Hospital, Zhengzhou, Henan, People’s Republic of China
Correspondence: Hua Bai, The Third Affiliated Hospital, Zhengzhou University, Zhengzhou, Henan, 450000, People’s Republic of China, Tel +86 371 66903017, Email [email protected]
Purpose: Postpartum depression is related to many factors, which affect the health of mothers and infants. The purpose of this study is to test the mediated effect of self-efficacy in the relationship between vulnerable personality and postpartum depression.
Patients and Methods: A cross-sectional survey was conducted with pregnant women aged ≥ 20 years from February to April 2021 in Zhengzhou, China. We recruited 587 pregnant women, and 429 pieces of data were available. The demographic characteristics questionnaire, General Self efficacy Scale (GSES) and Vulnerable Personality Style Questionnaire (VPSQ) were distributed in the prenatal survey. The Edinburgh Postnatal Depression Scale (EPDS) was used to screen postpartum depression symptoms at one month through WeChat and telephone follow-up. A mediated model was constructed to explain the relationship of variables and test the mediated effect of self-efficacy.
Results: The valid questionnaires were 429 (effective response rate: 90.7%). The vulnerable personality and low self-efficacy were related to postpartum depression (all P< 0.01). The self-efficacy of pregnant women was inversely associated with vulnerable personality (β= − 0.415) and postpartum depression (β= − 0.216). The vulnerable personality and self-efficacy can explain 29.0% of the variation in postpartum depression. It was confirmed that a partial mediating effect of self-efficacy accounted for 18.0% (0.090/0.501) of the total effect.
Conclusion: Maternal self-efficacy partly mediates the relationship between vulnerable personality traits and postpartum depression. The study implies the importance of targeted interventions to improve self-efficacy for women with vulnerable personality traits to reduce the risk of postpartum depression.
Keywords: postpartum depression, vulnerable personality, self-efficacy, mediated effect
Introduction
Postpartum depression (PPD) is defined as “a major depressive episode with peripartum onset and onset of mood symptoms occurs during pregnancy or within 4 weeks following delivery” according to the Diagnostic and Statistical Manual of Mental Disorder (DSM-5).1–3 One of the main concerns of women’s mental health is postpartum depression.1,4,5 According to international research data, PPD was a global disease with a prevalence of 17.7%.6 Prevention of postpartum depression has become an urgent issue.
Multifarious variables have been identified as risk factors associated with PPD,7,8 including young age,7 overweight,9 multiple births,10 emergency caesarean section,11,12 lack of social support13 and immigration status,10 especially the vulnerable personality traits.14 Dennis and Boyce14 has reported that the vulnerable personality is positively associated with postpartum depression. In the past two decades, the role of personality traits has been gaining attention as a predictor for PPD.15–18 Vulnerable personality is not confined to one particular trait,17 mainly includes coping, nervy, timidity, sensitivity, worry, organisation, obsessive, expressive and volatility.17 However, the relationship between vulnerable personality and PPD, though widely demonstrated and reported in previous studies, is seldom investigated clearly in China.19,20
The direct relationship between vulnerable personality and postpartum depression has been identified in a previous study.14 However, their interrelationship cannot be well revealed by traditional analytical methods. Previous studies often used the methods of regression analysis to investigate the association between variables and PPD.9,21 Although several variables may have no direct effects on postpartum depression, there are possible intermediary variables to connect them. It is indicated that verifying the possible interrelations between variables and PPD could help us find potential risk factors for postpartum depression.7
Prior studies observe that the low self-efficacy of pregnant women is related to PPD, which is an individual’s ability to make meaningful, healthy choices and translate those choices into desired actions and outcomes.12,22–24 Notably, self-efficacy has been investigated as a mediated factor in previous researches.25–28 A cross-sectional study of 740 participants suggests that self-efficacy mediated the relationship between social support and dietary intake.26 Likewise, Cutrona et al28 note that infant temperamental difficulty and social support were strongly related to PPD directly and through the mediation of parenting self-efficacy. Identifying the underlying mediated factors could be helpful to explain the relationship between vulnerable personality and PPD clearly.
Therefore, this survey was conducted to explore the mediated effect of self-efficacy in the relationship between vulnerable personality and PPD by using structural equation modelling (SEM). The main variables of this study mentioned above were evaluated using self-report questionnaires or scales. Based on previous research, the most widely used cut-off scores were adopted to report the positive screening results of PPD and other variables. It was to demonstrate whether and how vulnerable personality influenced PPD through self-efficacy and, hopefully, help to prevent maternal from PPD.
Materials and Methods
Design
From February to April 2021, a cross-sectional study was conducted at two large tertiary general hospitals in Zhengzhou, China. After signing the Informed Consent Form, we recruited eligible pregnant women into the survey using convenience sampling.
The survey was composed of two sections. First, the prenatal survey was conducted by researchers and trained midwives at maternity wards and obstetric clinics. All recruited participants who were pregnant at least 37 weeks were required to finish the prepartum survey, including the General Self Efficacy Scale (GSES) and the Vulnerable Personality Style Questionnaire (VPSQ). Meanwhile, a demographic characteristics questionnaire was used to collect basic information about pregnant women during the prenatal survey. At the same time, we created two WeChat groups respectively in two hospitals to collect postpartum data online and keep good contact with pregnant women. WeChat is a widely used application in China that can help people communicate with two or more users by creating a chat group. Second, the postpartum survey consisted of the Edinburgh Postpartum Depression Scale (EPDS) and general obstetric information. Based on WeChat groups, we conducted a postpartum survey by the Wenjuanxing platform (https://www.wjx.cn/app/survey.aspx) one month after childbirth. Then we checked the postpartum data carefully to ensure that all informed participants had finished the postpartum survey. Furthermore, the unfinished one and those less than one month after childbirth would be notified again through telephone follow-up.
Finally, 587 pregnant women were recruited, among which 158 were invalid, thus there were 429 eligible samples.
Study Participants
Eligible participants were those who: 1) aged at least 20 years, 2) were pregnant at 37–41 weeks, 3) had no history of severe physical illness, 4) could understand Chinese and 5) agreed to participate in this survey and signed informed consent.
Exclusion criteria included the diagnosis of more than three pregnancy complications or other physical severe diseases during this pregnancy. Additionally, pregnant women who refused to participate in the research and exited halfway were also excluded.
Measurements
Sociodemographic and Obstetrical Characteristics Questionnaire
Based on previous reviews and researches,5,7,10,12 we designed the sociodemographic and obstetrical characteristics questionnaire to collect basic information of participants. It consisted of age, parity, gestational week, pregnancy complication, employment status, educational level, average monthly family income, marital status, residence, planning of pregnancy, planned mode of birth and primary caregiver in the prenatal survey. Postpartum data collection was conducted at the first month after delivery, including infant gender, breastfeeding behaviour and mode of birth.
The General Self Efficacy Scale (GSES)
The GSES, a unidimensional scale that included ten items, was constructed by Schwarzer and Renner.29 In this survey, we used the Chinese version of GSES that Wang et al30 translated in 2001 (Cronbach’s α = 0.87). It was used extensively to evaluate participants’ self-efficacy in China. Each item of GSES scored on a 4-point Likert scale (1 “definitely no” to 4 “definitely yes”). The sum scores of the scale ranged from 10 to 40. The higher the sum scores were, the better sense of self-efficacy. Internal consistency of GSES in this survey also showed excellent (Cronbach’s α = 0.852).
The Vulnerable Personality Style Questionnaire (VPSQ)
Dennis and Boyce initially developed the 9-item VPSQ in 2004.14 A localised version of VPSQ translated by Jin and Li20 was utilised widely in China, which consisted of 9 items. Each item represented a dimension, which scored on a 5-point Likert scale (1 “not at all” to 5 “very much so”). The sum scores of the questionnaire ranged from 9 to 45. There were two sub-scales, which consisted of the “vulnerability” (nervy, timidity, sensitivity, worrier, obsessive and volatility) and the “organised/responsive” (coping, organised and expressive). The sum scores of all the items revealed one’s personality tendency. Internal consistency of VPSQ was proved good in our survey (Cronbach’s α = 0.602), and Cronbach’s α of the sub-scales were 0.714 (“vulnerability”) and 0.671 (“organized/responsive”) respectively.
The Edinburgh Postnatal Depression Scale (EPDS)
The Edinburgh Postnatal Depression Scale (EPDS) was used globally to screen for symptoms of postpartum depression at one month. Cox and his team constructed EPDS initially,31 which was translated into Chinese by Lee and a cut-off score of 9/10 was recommended.32,33 The EPDS consisted of ten items scored from 0 to 3. The sum scores of the scale ranged from 0 to 30. Additionally, the women who scored over 9 were probably at risk of suffering from depression.32,33 The threshold score of 9/10 was used in this study. The internal consistency of EPDS was shown excellent in this research (Cronbach’s α = 0.805).
Data Collection
From February to April 2021, we conducted a cross-sectional survey among pregnant women by using convenient sampling. The survey was performed by researchers and trained midwives at maternity wards and obstetric clinics. At the beginning of the survey, all eligible participants were informed of the purpose of the study and required to provide informed consent. To ensure the authenticity and completeness of the data, researchers informed participants of the matters needing attention in filling in the questionnaire.
At first, 587 pregnant women were available, and 545 agreed to participate in this study. After the prenatal survey, including the GSES, VPSQ and demographic characteristics questionnaires, 72 women were excluded from 545 participants because of the following reasons: exit halfway (n=6), fail to meet the inclusion criteria (n=52), and incomplete questionnaires (n=14). In the first month after childbirth, we distributed electric questionnaires consisting of the EPDS and general obstetric information to mothers through the WeChat groups, and 159 completed questionnaires were finally returned. Then we continued to collect the rest data by telephone follow-up, and 44 participants could not be contacted. Finally, 429 pieces of data were analysed (response rate: 90.7%).
Data Analysis
The software of IBM SPSS Statistics 25.0 and AMOS Graphics 25.0 were employed to analyse data. Sociodemographic and obstetrical information and the scores of GSES, VPSQ and EPDS were examined by descriptive statistics of frequencies, percentages, means, standard deviations, and scores range. Pearson Correlation Coefficient was performed to explore the relationships among demographic characteristics, self-efficacy, vulnerable personality and postpartum depression. The internal consistencies of measurement tools were retested in this survey.
According to previous reviews,5,10,34 many sociodemographic characteristics such as age, parity, monthly income and educational level were associated with PPD. Therefore, the relationship between sociodemographic factors and PPD was first tested. And the predictors of self-efficacy and vulnerable personality were also explored, respectively. Then we investigated the direct relationship of self-efficacy, vulnerable personality and PPD.
After the fundamental data analysis, we made the structural equation modelling (SEM) consists of self-efficacy, vulnerable personality and postpartum depression. The bootstrap method (5,000 replicates)35,36 and product of coefficients test37,38 were used to verify the mediation effect of maternal self-efficacy on vulnerable personality and postpartum depression. The bootstrap method was more accurate and efficient in demonstrating the mediator effect than traditional statistical methods.37,39,40 Ninety-five percent confidence intervals were constructed by using a bootstrap resampling approach.39 The model’s fit with our data was tested using chi-square statistics (CMIN), degrees of freedom (df), goodness-of-fit index (GFI), adjusted goodness-of-fit index (AGFI), Tucker-Lewis index (TLI), comparative fit index (CFI), and root mean square error of approximation (RMSEA). A two-tailed significance level of 0.05 was used for statistical analysis.
Results
Participant Characteristics
There were 429 valid questionnaires in this survey. The age of pregnant women ranged from 20 to 43 years old, and the mean age was 31.15 (SD =4.0). Characteristics of all of the participants are shown in Table 1.
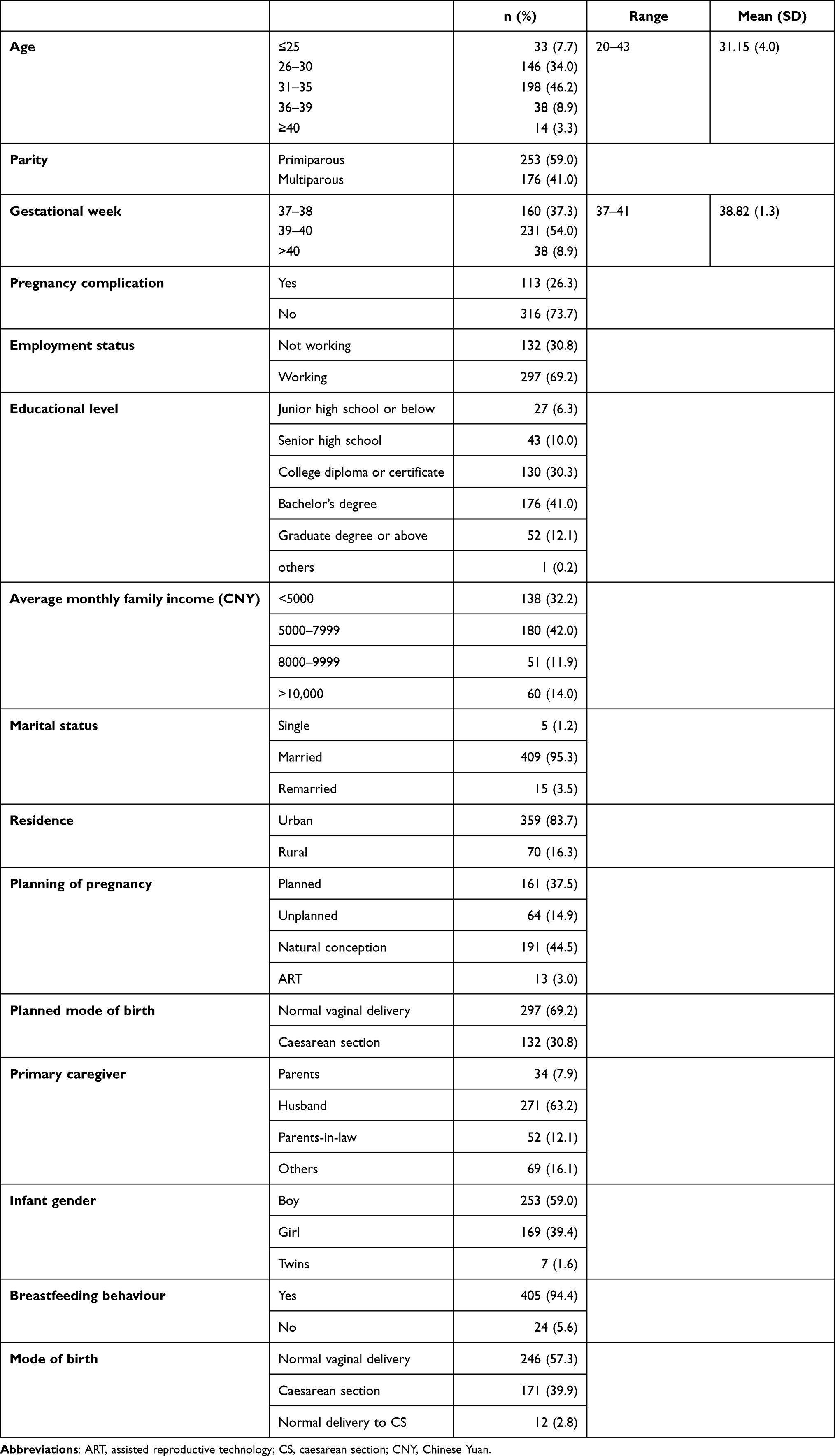 |
Table 1 Sociodemographic Characteristics of Participants (N=429) |
Descriptive Statistics of the Measurements
The score ranges, means and standard deviations of maternal self-efficacy, vulnerable personality and postpartum depression were performed in Table 2. We found that the average score of PPD was generally low (M=2.57, SD=3.3), and the rate of postpartum depression at one month determined by a score ≥10 on the EPDS was 3.3% (N=14).
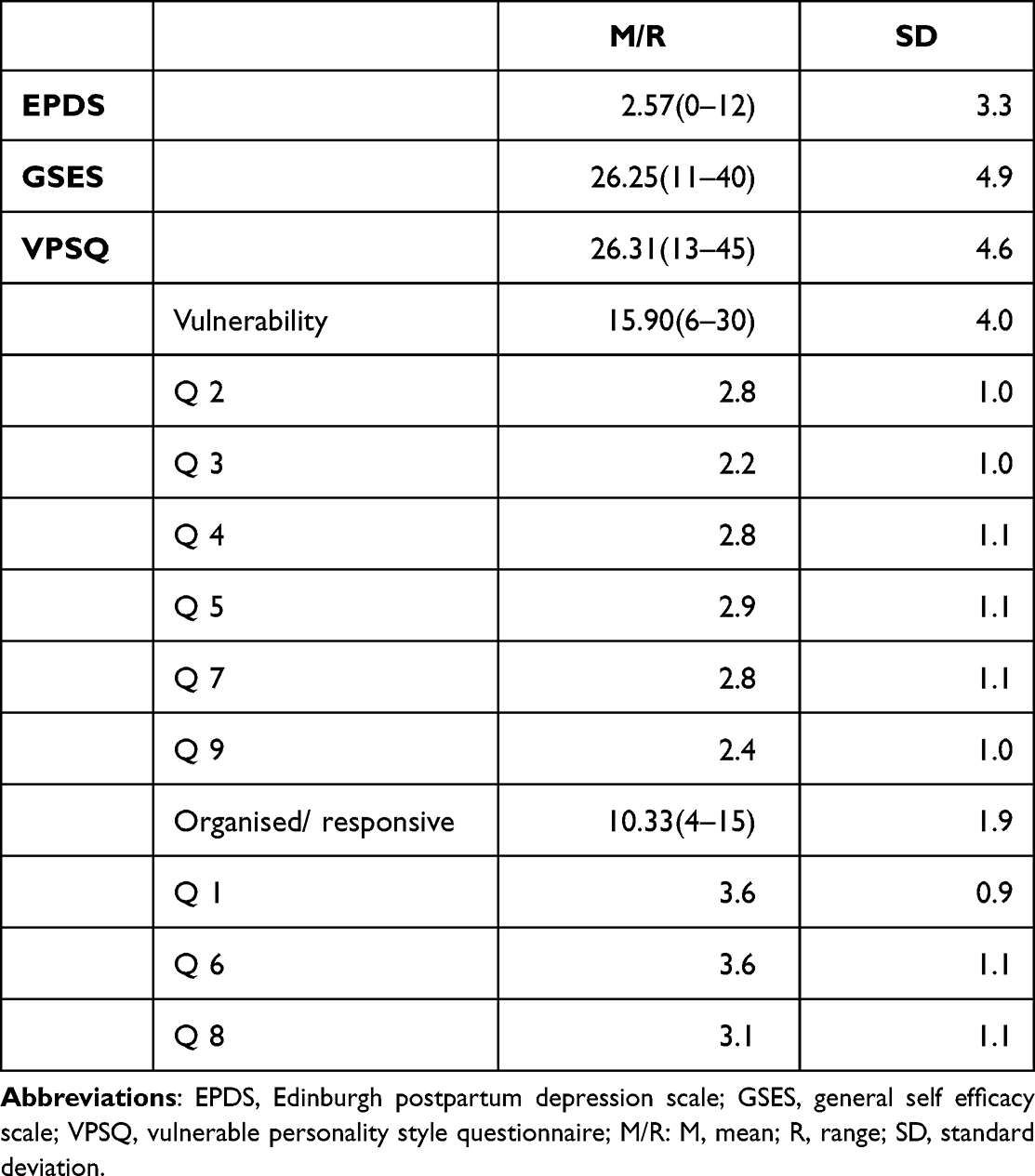 |
Table 2 Descriptive Statistics of Questionnaire Data (N=429) |
Correlations Analyses
The results of correlational analyses of sum scores of GSES, VPSQ and EPDS are shown in Table 3. As Table 3 described to us, postpartum depression is negatively correlated with self-efficacy (r= −0.382, P< 0.01), but positively correlated with vulnerable personality (r= 0.457, P<0.01). There is an inverse correlation between self-efficacy and vulnerable personality (r= −0.283, P< 0.01). Based on the significant correlation of three main variables, further analysis and exploration could be carried out to investigate the hypothesis.
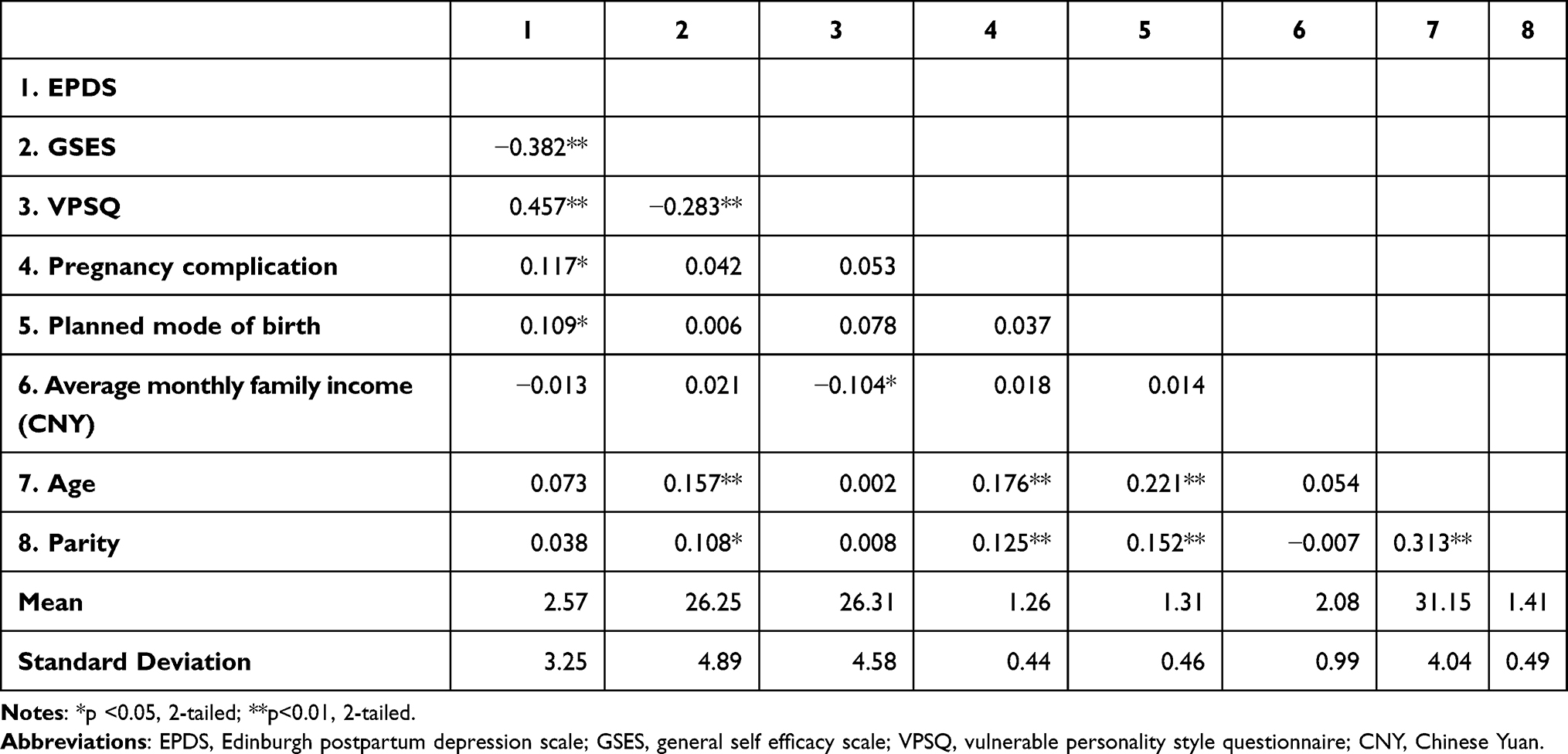 |
Table 3 Pearson Correlations for Risk Factors, VPSQ, GSES and EPDS (N=429) |
The Mediation Effect of Self-Efficacy Analysis
After basic statistical analyses, we constructed the structural equation modelling to test the hypothesis by using AMOS. The trimmed SEM is shown in Figure 1, and its model fit well with the data was: CMIN=43.485, df=32, X2/df=1.359, GFI=0.982, AGFI=0.963, TLI=0.974, CFI=0.985, RMSEA=0.029 and RMR=0.034. The SEM model demonstrated that vulnerable personality had a direct effect on postpartum depression (β= 0.411, P< 0.001). And self-efficacy negatively predicted PPD (β= −0.216, P< 0.001) as well vulnerable personality (β= −0.415, P< 0.001). Additionally, vulnerable personality was indirectly related to PPD through self-efficacy (β= 0.090, P< 0.001). Moreover, vulnerable personality and self-efficacy can explain 29.0% of the variation in PPD.
 |
Figure 1 Structural equation model of mediating role of self-efficacy in vulnerable personality and postpartum depression. Abbreviations: Vuln, vulnerability personality; PPD, postpartum depression; Self, self-efficacy. |
The standardised total, indirect, and direct effects of the model are depicted clearly in Table 4. It was revealed that maternal self-efficacy played a mediated role in the relationship between vulnerable personality and postpartum depression. A partial mediating effect of self-efficacy on PPD accounted for 18.0% (0.090/0.501) of the total effect. The bootstrapped 95% confidence interval of indirect effect between vulnerable personality and postpartum depression did not include zero (95% CI= [0.050, 0.136]), which indicated that the mediation effect of self-efficacy was significant.
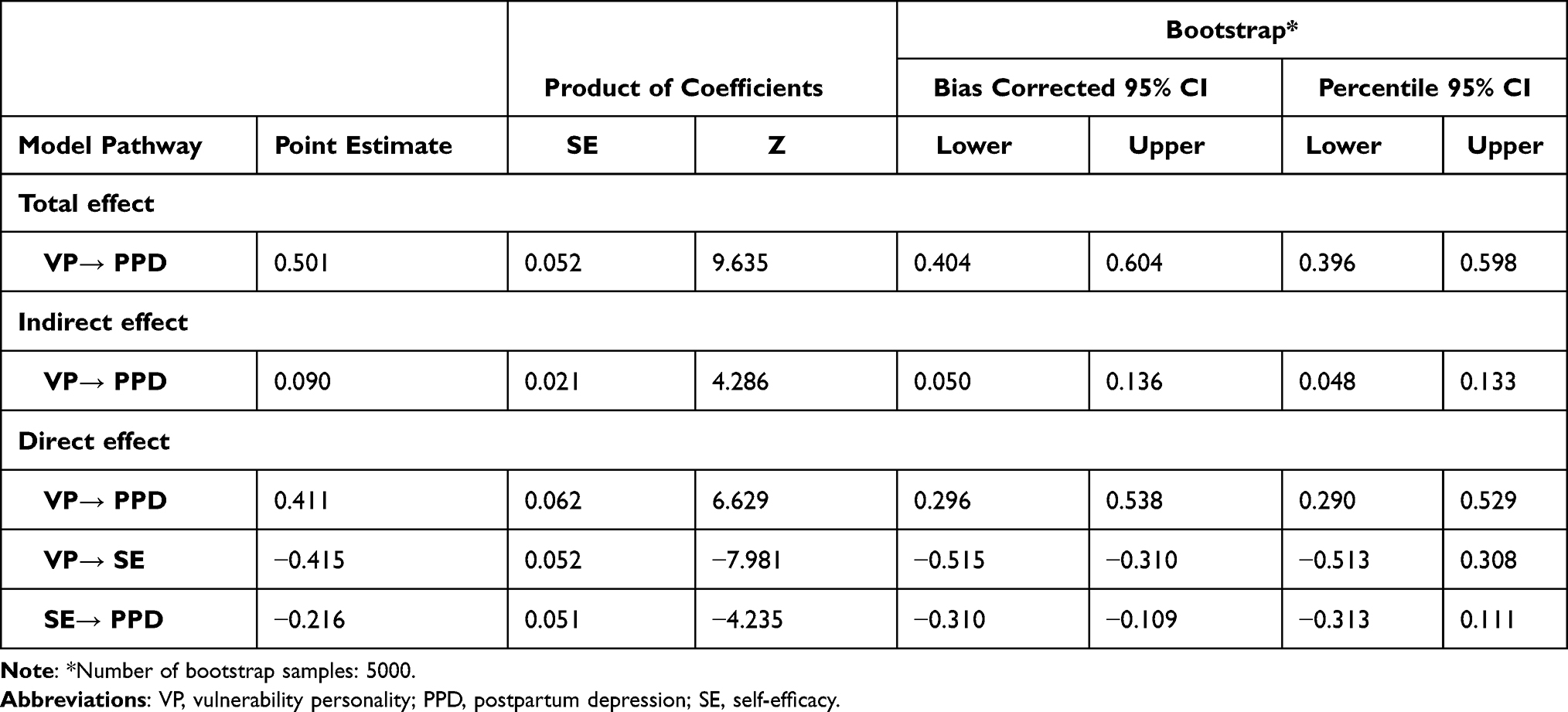 |
Table 4 The Standardised Total, Indirect, and Directs Effect of Mediation Model Among Self-Efficacy, Vulnerable Personality, and Postpartum Depression (N=429) |
Discussion
We found that self-efficacy played a mediated role in the relationship between vulnerable personality and postpartum depression. It is indicated that self-efficacy may be a key factor for pregnant women with personality traits of vulnerable to reduce the prevalence of PPD.
PPD is one of the most common complications after childbirth,41 which is negatively associated with mother-infant bonding and women’s mental health.3,8 Reports in various studies of the prevalence of PPD and associated predictive factors are inconsistent. The heterogeneity of measurement tools and the differences in cut-off scores of EPDS to define severe PPD might contribute to this inconsistency. The reported prevalence of postpartum depression ranges from 6.5 to 12.9% and is even higher in developing countries.3,42 With the EPDS threshold of 13, the incidence of postpartum depression is reported as 23.5% in Shanghai, China.43 However, a recent cross-sectional study shows a higher prevalence of postpartum depression (56.9%)44 in Hubei, China, which is probably a consequence of the COVID-19 pandemic.
In this survey, the prevalence of PPD was 3.3% (EPDS ≥10). The result is in line with the research in Changsha of China (5.0%)45 and a cross-sectional study from three continents (6.7%), including Denmark (6.4%), Vietnam (1.9%) and Tanzania (12.6%).46 The low prevalence of PPD in this study may be due to the data being collected cross-sectionally and certain methodological limitations or bias rendered by convenience sampling. For example, only 16.3% of participants with senior high school certificates or below in this survey. With reference to previous research, Wesselhoeft et al46 investigated those mothers with low education levels were prone to significant depressive symptoms. Further, according to statistics published by the National Bureau of Statistics of China in 2021 (http://www.stats.gov.cn/), Zhengzhou’s GDP ranks first in Henan Province, where the study was conducted. It seems that the city’s good economic status and health care system may partly contribute to the low sum scores of EPDS in this study. Taken together, the differences in sampling and data collection methods may be the main reasons for the low incidence of postpartum depression in this study. And further studies with larger sample sizes and more follow-up time points are needed to investigate the prevalence and risk factors of PPD in China. In terms of numerous factors related to PPD, it would be helpful to reduce the incidence of postpartum depression by controlling alterable risk factors.
Our study confirmed that pregnancy complications and preferred caesarean section are strong predictors of postpartum depression, which are consistent with previous studies.7,12,47 Meanwhile, Tobe48 notes that young age and primipara are risk factors for PPD in Japan. And a path model analysis suggests that younger maternal age led to a higher level of postpartum depression in the form of a direct pathway.7 Conversely, increasing age is proved to be an independent risk factor for the development of PPD in recent research.46 However, there was no significant correlation between women’s age as well as other demographic characteristics and PPD in our survey (Table 3). Vigod et al49 found that the prevalence of PPD was higher among women living in urban areas than in rural areas. However, according to the present survey, there is no significant correlation between the residence and the sum scores of EPDS. Additionally, the risk factors of PPD reported in previous studies include hormonal fluctuations,48 chronic pain caused by surgical wounds,50 difficulties in breastfeeding,23 poor quality sleep51 and lack of support from family.52 We were not able to compare all potential risk factors of PPD between our study and others due to different eligible samples. In addition, although several variables may have no direct effects on PPD, there are possible intermediary variables to connect them. Therefore, further research is needed to confirm and specify this association.
Our study identified that vulnerable personality was negatively related to high sum scores of EPDS. According to a series of studies,16,17,53,54 it is compelling that vulnerable personality predicts postpartum depression symptoms from personality and cognitive perspectives. A longitudinal study shows that our personality has a stable component across the life span,55 and the mechanism of personality change is still a cloud.56 Moreover, it is unclear whether indirect factors mediate the relationship between vulnerable personality and PPD.
Interestingly, in our present study, self-efficacy measured by GSES partly mediated the relationship between vulnerable personality and PPD. Furthermore, we found that self-efficacy negatively correlates with both vulnerable personality and postpartum depression. Many studies have also proved that self-efficacy is a mediator factor related to other variables.26,27,57 In addition, women over 35 years and multiparas obtained high GSES scores in this survey, which were in line with previous studies.58,59 However, a review points out that older adults may be less sensitive to self-efficacy interventions.60 According to an experimental randomised control study, psychological education can enhance general self-efficacy.61 Based on the SEM, strengthening pregnant women’s self-efficacy may be helpful to reduce the incidence of postpartum depression theoretically.
In light of the evidence about improving self-efficacy, the nurse-led intervention program,62 physical activity intervention,63 behaviour change techniques64 and interventions based on an empowering self-management model effectively improved the self-efficacy and health-promoting behaviours.65 To some extent, the present study may help improve our understanding of reducing the prevalence of PPD from a new perspective.
Additionally, a series of studies have pointed out that prenatal health care and behavioural intervention showed effectiveness in reducing the prevalence of PPD. Simhi et al66 investigated that cognitive-behavioural interventions reduced postpartum anxiety, distress, and depressive symptoms among postpartum women. Similarly, electronic nursing intervention,67 doula-home-visiting on postpartum maternal and infant,68 educational counselling program based on precede-proceed model69 also decrease the sum scores of EPDS of mothers. Despite the large number of interventions to prevent PPD, there are still no reported self-efficacy improvement programs for women with vulnerable personality traits to decrease the depressive symptoms. Theoretically, the implementation of interventions that enhance the self-efficacy of pregnant women may be helpful to decrease the risk of postpartum depression.
Of note, it is a cross-sectional study, which limits the possibility of establishing causal relationships among variables. Longitudinal and experimental studies are warranted to identify factors that increase or decrease PPD and construct effective targeted interventions of postpartum depressive symptoms among pregnant Chinese women.
Clinical Implication
The results of the study suggest that self-efficacy intervention may be helpful for pregnant women with vulnerable personality to reduce the incidence of postpartum depression. Due to China’s second-child policy, the number of women giving birth in hospitals is increasing rapidly.70 Compared with obstetricians, nurses and midwives are medical workers who accompany pregnant women more in China. General psychological screening for vulnerable personality conducted by midwives would help improve pregnant women’s mental health. Correspondingly, a series of train courses could be set up to improve maternal self-efficacy with the help of midwives.
Limitations
There are several limitations to our research. First, the sample selection bias may have occurred due to the investigation completed in only two hospitals in China. And the universality of the results was limited. Second, the variables of vulnerable personality and maternal self-efficacy explain less than 40% of the variance of the PPD. Third, all the main variables in this study are the sum scores of measurement tools, and they cannot be considered the diagnosis of psychopathology. Longitudinal and cohort studies are necessary to obtain a more conclusive causality inference. Finally, the mediation effect of self-efficacy is partial. Further research is required to confirm the results and construct efficient intervention programs to enhance maternal self-efficacy.
Conclusions
In summary, this study expanded the previous research by investigating the relationship that vulnerable personality and self-efficacy are significantly related to postpartum depression. To our knowledge, there is a dearth of studies to report the personality traits of pregnant women and explore the mediated role of self-efficacy between personality traits and PPD in China. Postpartum depression exacerbates maternal vulnerable mental health and impairs the mother-child bond.8 Therefore, the importance of effective and targeted antenatal health education against possible risk factors to reduce the prevalence of PPD cannot be overstated.
This study found that the prevalence of PPD was 3.3% and revealed that maternal self-efficacy partly mediated the relationship between vulnerable personality traits and postpartum depression. The finding underscores the importance of mental health interventions that target and improve self-efficacy in pregnant women with vulnerable personality to decrease the risk of postpartum depression. While we cannot infer causality from the present data, the vulnerable personality trait of pregnant women in this sample may have contributed to the tendency to postpartum depression. And further studies with larger sample sizes and more follow-up time points are needed to investigate the mediated model of self-efficacy and the relationship between vulnerable personality traits and PPD.
Ethics Approval and Informed Consent
The procedure was done in agreement with the Declaration of Helsinki. The study was supported by the Ethics Committee of the Third Affiliated Hospital of Zhengzhou University and the Chinese Health Department. Written consent was obtained from the participants, and they were utterly voluntary to participate in this survey.
Acknowledgments
We would like to express our appreciation for the great cooperation of the participants of this study and the staff at the two hospitals.
Author Contributions
All authors made significant contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This research is supported by the joint construction project of Henan Province’s medical science and technology research plan (no. SBGJ2018049).
Disclosure
The authors report no conflicts of interest for this work.
References
1. Stewart DE, Vigod SN. Postpartum depression: pathophysiology, treatment, and emerging therapeutics. Annu Rev Med. 2019;70(1):183–196. doi:10.1146/annurev-med-041217-011106
2. Wisner KL, Sit DK, McShea MC, et al. Onset timing, thoughts of self-harm, and diagnoses in postpartum women with screen-positive depression findings. JAMA Psychiatry. 2013;70(5):490–498. doi:10.1001/jamapsychiatry.2013.87
3. Stewart DE, Vigod S. Postpartum depression. N Engl J Med. 2016;375(22):2177–2186. doi:10.1056/NEJMcp1607649
4. Oztora S, Arslan A, Caylan A, et al. Postpartum depression and affecting factors in primary care. Niger J Clin Pract. 2019;22(1):85–91. doi:10.4103/njcp.njcp_193_17
5. Mu TY, Li YH, Pan HF, et al. Postpartum depressive mood (PDM) among Chinese women: a meta-analysis. Arch Womens Ment Health. 2019;22(2):279–287. doi:10.1007/s00737-018-0885-3
6. Hahn-Holbrook J, Cornwell-Hinrichs T, Anaya I. Economic and health predictors of national postpartum depression prevalence: a systematic review, meta-analysis, and meta-regression of 291 studies from 56 countries. Front Psychiatry. 2017;8:248. doi:10.3389/fpsyt.2017.00248
7. Liu S, Yan Y, Gao X, et al. Risk factors for postpartum depression among Chinese women: path model analysis. BMC Pregnancy Childbirth. 2017;17(1):133. doi:10.1186/s12884-017-1320-x
8. Motegi T, Watanabe Y, Fukui N, et al. Depression, anxiety and primiparity are negatively associated with mother-infant bonding in Japanese mothers. Neuropsychiatr Dis Treat. 2020;16:3117–3122. doi:10.2147/NDT.S287036
9. Johar H, Hoffmann J, Günther J, et al. Evaluation of antenatal risk factors for postpartum depression: a secondary cohort analysis of the cluster-randomised GeliS trial. BMC Med. 2020;18(1):227. doi:10.1186/s12916-020-01679-7
10. Zhao X-H, Zhang Z-H. Risk factors for postpartum depression: an evidence-based systematic review of systematic reviews and meta-analyses. Asian J Psychiatr. 2020;53:102353. doi:10.1016/j.ajp.2020.102353
11. Sun L, Wang S, Li XQ. Association between mode of delivery and postpartum depression: a systematic review and network meta-analysis. Aust N Z J Psychiatry. 2021;55(6):588–601. doi:10.1177/0004867420954284
12. Xu H, Ding Y, Ma Y, et al. Cesarean section and risk of postpartum depression: a meta-analysis. J Psychosom Res. 2017;97:118–126. doi:10.1016/j.jpsychores.2017.04.016
13. Ando H, Shen J, Morishige KI, et al. Association between postpartum depression and social support satisfaction levels at four months after childbirth. Arch Psychiatr Nurs. 2021;35(4):341–346. doi:10.1016/j.apnu.2021.03.010
14. Dennis CL, Boyce P. Further psychometric testing of a brief personality scale to measure vulnerability to postpartum depression. J Psychosom Obstet Gynaecol. 2004;25(3–4):305–311. doi:10.1080/01674820400017962
15. Josefsson A, Larsson C, Sydsjö G, et al. Temperament and character in women with postpartum depression. Arch Womens Ment Health. 2007;10(1):3–7. doi:10.1007/s00737-006-0159-3
16. Boyce P, Parker G, Barnett B, et al. Personality as a vulnerability factor to depression. Br J Psychiatry. 1991:106–114. doi:10.1192/bjp.159.1.106
17. Boyce P, Mason C. An overview of depression-prone personality traits and the role of interpersonal sensitivity. Aust N Z J Psychiatry. 1996;30(1):90–103. doi:10.3109/00048679609076076
18. Lotrich FE, Rabinovitz M, Gironda P, et al. Depression following pegylated interferon-alpha: characteristics and vulnerability. J Psychosom Res. 2007;63(2):131–135. doi:10.1016/j.jpsychores.2007.05.013
19. Xu H, Huang X, Chen C, et al. A pilot study on the Chinese vulnerable personality to depression. Chin J Clin Psychol. 2012;20(4):427–433.
20. Jin S, Li M. A study of the effectiveness of Vulnerable Personality Style Questionnaire to predict postpartum depression. Chin J Nurs. 2006;41(9):781–784.
21. Suhitharan T, Pham TP, Chen H, et al. Investigating analgesic and psychological factors associated with risk of postpartum depression development: a case-control study. Neuropsychiatr Dis Treat. 2016;12:1333–1339. doi:10.2147/NDT.S105918
22. van der Zee-vanden Berg AI, Boere-Boonekamp MM, Groothuis-Oudshoorn CGM, et al. Postpartum depression and anxiety: a community-based study on risk factors before, during and after pregnancy. J Affect Disord. 2021;286:158–165. doi:10.1016/j.jad.2021.02.062
23. Vieira ES, Caldeira NT, Eugênio DS, et al. Breastfeeding self-efficacy and postpartum depression: a cohort study. Rev Lat Am Enfermagem. 2018:e3035. doi:10.1590/1518-8345.2110.3035
24. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191–215. doi:10.1037/0033-295X.84.2.191
25. Volz M, Voelkle MC, Werheid K. General self-efficacy as a driving factor of post-stroke depression: a longitudinal study. Neuropsychol Rehabil. 2019;29(9):1426–1438. doi:10.1080/09602011.2017.1418392
26. Chang MW, Schaffir J, Brown R, et al. Mediation by self-efficacy in the relation between social support and dietary intake in low-income postpartum women who were overweight or obese. Appetite. 2019;140:248–254. doi:10.1016/j.appet.2019.05.031
27. Guo J, Yang J, Wiley J, et al. Perceived stress and self-efficacy are associated with diabetes self-management among adolescents with type 1 diabetes: a moderated mediation analysis. J Adv Nurs. 2019;75(12):3544–3553. doi:10.1111/jan.14179
28. Cutrona CE, Troutman BR. Social support, infant temperament, and parenting self-efficacy: a mediational model of postpartum depression. Child Dev. 1986;57(6):1507–1518. doi:10.2307/1130428
29. Schwarzer R, Renner B. Social-cognitive predictors of health behavior: action self-efficacy and coping self-efficacy. Health Psychol. 2000;19(5):487–495. doi:10.1037/0278-6133.19.5.487
30. Wang CK, Hu ZF, Liu Y. Research on the reliability and validity of general self-efficacy scale. Chin J Appl Psychol. 2001;7(1):37–40.
31. Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br J Psychiatry. 1987;150(6):782–786. doi:10.1192/bjp.150.6.782
32. Cox J. Thirty years with the Edinburgh Postnatal Depression Scale: voices from the past and recommendations for the future. Br J Psychiatry. 2019;214(3):127–129. doi:10.1192/bjp.2018.245
33. Lee DT, Yip SK, Chiu HF, et al. Detecting postnatal depression in Chinese women. Validation of the Chinese version of the Edinburgh Postnatal Depression Scale. Br J Psychiatry. 1998;172(5):433–437. doi:10.1192/bjp.172.5.433
34. Özcan NK, Boyacıoğlu NE, Dinç H. Postpartum depression prevalence and risk factors in Turkey: a systematic review and meta-analysis. Arch Psychiatr Nurs. 2017;31(4):420–428. doi:10.1016/j.apnu.2017.04.006
35. Fritz MS, Mackinnon DP. Required sample size to detect the mediated effect. Psychol Sci. 2007;18(3):233–239. doi:10.1111/j.1467-9280.2007.01882.x
36. Mackinnon DP, Lockwood CM, Williams J. Confidence limits for the indirect effect: distribution of the product and resampling methods. Multivariate Behav Res. 2004;39(1):99. doi:10.1207/s15327906mbr3901_4
37. Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986;51(6):1173–1182. doi:10.1037/0022-3514.51.6.1173
38. MacKinnon DP, Lockwood CM, Hoffman JM, et al. A comparison of methods to test mediation and other intervening variable effects. Psychol Methods. 2002;7(1):83–104. doi:10.1037/1082-989X.7.1.83
39. Hayes AF, Scharkow M. The relative trustworthiness of inferential tests of the indirect effect in statistical mediation analysis: does method really matter? Psychol Sci. 2013;24(10):1918–1927. doi:10.1177/0956797613480187
40. Sobel ME. Asymptotic confidence intervals for indirect effects in structural equation models. Sociol Methodol. 1982;13:290–312. doi:10.2307/270723
41. Payne JL, Maguire J. Pathophysiological mechanisms implicated in postpartum depression. Front Neuroendocrinol. 2019;52:165–180. doi:10.1016/j.yfrne.2018.12.001
42. Sword W, Landy CK, Thabane L, et al. Is mode of delivery associated with postpartum depression at 6 weeks: a prospective cohort study. BJOG. 2011;118(8):966–977. doi:10.1111/j.1471-0528.2011.02950.x
43. Liu Y, Zhang L, Guo N, et al. Postpartum depression and postpartum post-traumatic stress disorder: prevalence and associated factors. BMC Psychiatry. 2021;21(1):487. doi:10.1186/s12888-021-03432-7
44. An R, Chen X, Wu Y, et al. A survey of postpartum depression and health care needs among Chinese postpartum women during the pandemic of COVID-19. Arch Psychiatr Nurs. 2021;35(2):172–177. doi:10.1016/j.apnu.2021.02.001
45. Yu HY, Wang SY, Quan CX, et al. Dexmedetomidine alleviates postpartum depressive symptoms following cesarean section in Chinese women: a randomised placebo-controlled study. Pharmacotherapy. 2019;39(10):994–1004. doi:10.1002/phar.2320
46. Wesselhoeft R, Madsen FK, Lichtenstein MB, et al. Postnatal depressive symptoms display marked similarities across continents. J Affect Disord. 2020;261:
47. Tobe H, Kita S, Hayashi M, et al. Mediating effect of resilience during pregnancy on the association between maternal trait anger and postnatal depression. Compr Psychiatry. 2020;102:152190. doi:10.1016/j.comppsych.2020.152190
48. Brummelte S, Galea LA. Depression during pregnancy and postpartum: contribution of stress and ovarian hormones. Prog Neuropsychopharmacol Biol Psychiatry. 2010;34(5):766–776. doi:10.1016/j.pnpbp.2009.09.006
49. Vigod SN, Tarasoff LA, Bryja B, et al. Relation between place of residence and postpartum depression. Can Med Assoc J. 2013;185(13):1129–1135. doi:10.1503/cmaj.122028
50. Eisenach JC, Pan PH, Smiley R, et al. Severity of acute pain after childbirth, but not type of delivery, predicts persistent pain and postpartum depression. Pain. 2008;140(1):87–94. doi:10.1016/j.pain.2008.07.011
51. Huai-jie YA, Hong YA. Study on the sleep quality of perinatal women and the influencing factors of postpartum sleep. Chin J Dis Control Prev. 2021;25(02):176–179.
52. Dennis C-L, Ross LE. Depressive symptomatology in the immediate postnatal period: identifying maternal characteristics related to true- and false-positive screening scores. Can J Psychiatry. 2006;51(5):265–273. doi:10.1177/070674370605100501
53. Jones L, Scott J, Cooper C, et al. Cognitive style, personality and vulnerability to postnatal depression. Br J Psychiatry. 2010;196(3):200–205. doi:10.1192/bjp.bp.109.064683
54. Price L, Centifanti L, Slade P. Personality factors and vulnerability to post-traumatic stress responses after childbirth. Br J Clin Psychol. 2020;59(4):480–502. doi:10.1111/bjc.12262
55. Damian RI, Spengler M, Sutu A, et al. Sixteen going on sixty-six: a longitudinal study of personality stability and change across 50 years. J Pers Soc Psychol. 2019;117(3):674–695. doi:10.1037/pspp0000210
56. Oltmanns JR, Jackson JJ, Oltmanns TF. Personality change: longitudinal self-other agreement and convergence with retrospective-reports. J Pers Soc Psychol. 2020;118(5):1065–1079. doi:10.1037/pspp0000238
57. Lee BG, Lee TS, Kim SH. Mediation effect of self-efficacy on the relationship between perceived self-management support and health-related quality of life among cancer survivors. J Korean Acad Nurs. 2019;49(3):298–306. doi:10.4040/jkan.2019.49.3.298
58. Rottmann N, Dalton SO, Christensen J, et al. Self-efficacy, adjustment style and well-being in breast cancer patients: a longitudinal study. Qual Life Res. 2010;19(6):827–836. doi:10.1007/s11136-010-9653-1
59. Brunton R, Simpson N, Dryer R. Pregnancy-related Anxiety, perceived parental self-efficacy and the influence of parity and age. Int J Environ Res Public Health. 2020;17(18):6709. doi:10.3390/ijerph17186709
60. French DP, Olander EK, Chisholm A, et al. Which behaviour change techniques are most effective at increasing older adults’ self-efficacy and physical activity behaviour? A systematic review. Ann Behav Med. 2014;48(2):225–234. doi:10.1007/s12160-014-9593-z
61. Kılıç N, Şimşek N. The effects of psychological first aid training on disaster preparedness perception and self-efficacy. Nurse Educ Today. 2019;83:104203. doi:10.1016/j.nedt.2019.104203
62. Zheng X, Yu H, Qiu X, et al. The effects of a nurse-led lifestyle intervention program on cardiovascular risk, self-efficacy and health promoting behaviours among patients with metabolic syndrome: randomized controlled trial. Int J Nurs Stud. 2020;109:103638. doi:10.1016/j.ijnurstu.2020.103638
63. Blom V, Drake E, Kallings LV, et al. The effects on self-efficacy, motivation and perceived barriers of an intervention targeting physical activity and sedentary behaviours in office workers: a cluster randomised control trial. BMC Public Health. 2021;21(1):1048. doi:10.1186/s12889-021-11083-2
64. Olander EK, Fletcher H, Williams S, et al. What are the most effective techniques in changing obese individuals’ physical activity self-efficacy and behaviour: a systematic review and meta-analysis. Int J Behav Nutr Phys Act. 2013;10(1):29. doi:10.1186/1479-5868-10-29
65. Hourzad A, Pouladi S, Ostovar A, et al. The effects of an empowering self-management model on self-efficacy and sense of coherence among retired elderly with chronic diseases: a randomised controlled trial. Clin Interv Aging. 2018;13:2215–2224. doi:10.2147/CIA.S183276
66. Simhi M, Sarid O, Rowe H, et al. A cognitive-behavioral intervention for postpartum anxiety and depression: individual phone vs. group format. J Clin Med. 2021;10(24):5952. doi:10.3390/jcm10245952
67. McCarter D, Demidenko E, Sisco T, et al. Technology-assisted nursing for postpartum support: a randomised controlled trial. J Adv Nurs. 2019;75(10):2223–2235. doi:10.1111/jan.14114
68. Hans S, Edwards R, Zhang Y. Randomized controlled trial of doula-home-visiting services: impact on maternal and infant health. Maternal Child Health J. 2018;22(S1):105–113. doi:10.1007/s10995-018-2537-7
69. Beydokhti T, Dehnoalian A, Moshki M, et al. Effect of educational- counselling program based on precede-proceed model during Pregnancy on postpartum depression. Nurs Open. 2021;8(4):1578–1588. doi:10.1002/nop2.770
70. Guo XJ, Chen J, Ren JH, et al. Comparisons on perinatal depression between the first-child women and the second-child women in West China under the universal 2-child policy: a STROBE compliant prospective cohort study. Medicine. 2020;99(23):e20641. doi:10.1097/MD.0000000000020641
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.