Back to Journals » Advances in Medical Education and Practice » Volume 13
Best Practices of the World Health Organization Collaborating Centres (WHOCCs) in the Eastern Mediterranean Region
Authors Shehata MH ![]() , Prabu Kumar A
, Prabu Kumar A ![]() , Al Ansari AM
, Al Ansari AM ![]() , Deifalla A
, Deifalla A ![]() , Atwa HS
, Atwa HS ![]()
Received 24 March 2022
Accepted for publication 27 June 2022
Published 30 September 2022 Volume 2022:13 Pages 1199—1205
DOI https://doi.org/10.2147/AMEP.S367834
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Mohamed Hany Shehata,1,2 Archana Prabu Kumar,3 Ahmed Mohammed Al Ansari,3 Abdelhalim Deifalla,4,5 Hani Salem Atwa3,5
1Department of Family and Community Medicine, College of Medicine and Medical Sciences, Arabian Gulf University, Manama, Bahrain; 2Helwan University Faculty of Medicine, Cairo, Egypt; 3Medical Education Unit, College of Medicine and Medical Sciences, Arabian Gulf University, Manama, Bahrain; 4Department of Anatomy, College of Medicine and Medical Sciences, Arabian Gulf University, Manama, Bahrain; 5Faculty of Medicine, Suez Canal, University, Ismailia, Egypt
Correspondence: Archana Prabu Kumar, Medical Education Unit, College of Medicine and Medical Sciences, Arabian Gulf University, Manama, Bahrain, Tel +973 33854782 ; +919962006869, Email [email protected]; [email protected]
Background: World Health Organization Collaborating Centres (WHOCCs) cooperate with the WHO on a range of strategic areas such as nursing, nutrition, mental health, chronic diseases, education, and health technologies, depending on their speciality areas. As of 2021, WHO has 47 CCs in the Eastern Mediterranean Region (EMR) collaborating on diverse areas. Four CCs in the EMR located in Egypt, Kingdom of Bahrain, Sudan, and Pakistan focus primarily on medical education (ME).
Objective: The objective of this review of the literature is to describe the best practices in ME based on published research from the four WHOCCs in EMR. The secondary objective is to classify them based on the level of Kirkpatrick’s model (KM) of educational outcomes.
Methods: The contributions of WHOCCs are categorised in to five domains namely “Curriculum Development and Course Design”, “Student Assessment”, “Quality, Accreditation, and Program Evaluation”, “Teaching and Learning” and “Innovation in Medical Education”. Initial extraction yielded 96 articles for review, while the second level of analysis reduced the number of publications to 37 based on the date of publication within the last 5 years. Numerous best practices in ME emerged from the recently published works of these WHOCCs in the areas of learning and teaching, curriculum development, innovations in medical education, quality, and assessments in medical education. Literature from the WHOCCs on assessment and curriculum design are limited, possibly indicating opportunities for additional research.
Conclusion: The researchers conclude that the WHOCCs in the EMR show transformational impact on all principal areas of research and at multiple levels.
Keywords: WHOCC, ME, EMR, best practice, research domains, educational outcomes
Introduction
The World Health Organization (WHO) engages in scientific or technical cooperation with selected institutions which are designated as collaborating centres (CC). A WHOCC is defined as
… an institution designated by the Director-General to form part of an international collaborative network carrying out activities in support of the Organization’s programme at all levels.1
WHOCCs facilitate implementation of WHO’s mandated work by cooperating on the organization’s strategic objectives at regional and global levels, and on institutional capacity building in various countries and regions.2
The collaboration brings benefits to both parties. The WHO gains institutional capacity to support its work and leadership of international health. Similarly, institutions designated as WHOCC gain enhanced recognition by national authorities, increased international visibility, and greater attention from the public for the health issues on which they work. As members of a global WHOCC network, the centres gain the opportunity to exchange information, gain important resources, and develop technical cooperation with WHOCC peers, particularly at international level.2 Four CCs in the EMR located in Egypt, Kingdom of Bahrain, Sudan, and Pakistan cooperate in the area of medical education (ME).2 Each of these CCs have their distinctive missions and objectives.
The Educational Development Centre (EDC) was established at the Faculty of Medicine, University of Gezira (FMUG) in 1978 in response to the growing demand in both Sudan and the region for qualified medical teachers. The purpose of the EDC was to provide effective teacher training programmes, consultation on curricula development, and innovative teaching and evaluation methods for the health professions. The EDC is
dedicated to the mission of educational development in medical and health training institutions with priority given to innovation, integration, relevance and excellence.3,4
The College of Medicine and Medical Sciences at the Arabian Gulf University (CMMS-AGU) was recognized as Centre for Health Professionals’ Educational Development (CHPED) in 2006, and was re-designated in 2019. The Centre’s terms of references include: (1) Support the implementation of the WHO global strategy on human resources for health and regional strategic framework on health workforce development. (2) Strengthen and build capacities of faculty at the regional level in health professions education (HPE). (3) Carry out studies to explore the ways of improving the contribution of WHOCC in the field of HPE.2,5
Centre for Research and Development (CRD) in ME and Health Services at the Faculty of Medicine Suez Canal University (FOM-SCU) in Ismailia, Egypt was established in 1986, and recognized as a WHOCC in 1988. The CRD offers consultations and training activities in the field of HPE and health services to faculty members from Egypt and the region.6 CRD’s diploma course, the only formal course in medical education (ME) in Egypt that is taught through distance learning, is endorsed by Medical Sector of the Supreme Council of Universities.7
The Centre for Research in Health Professional Education (CRHPE), Pakistan was established as a training centre in ME by the College of Physicians and Surgeons in Pakistan. It was designated as WHOCC in 1996 to support better understanding of the postgraduate ME practices in EMR and to assist WHO in reviewing the use of information and communication technologies in postgraduate ME in EMR. The core activities of the centre are mainly research, training, and education in the field of health care.2
Kirkpatrick’s model (KM) is a holistic and broad evaluation method for educational training programs. Under the model, educational outcomes are located in levels from 1 to 4, learners’ reaction (satisfaction/perception about the educational activity); learning (acquiring the intended learning outcomes); behaviour (application of acquired knowledge/skills) and results (improvement in key performance indicators, patient outcomes etc) respectively. The levels of outcomes are not necessarily hierarchical.8
The objective of this paper is to describe the best practices in ME based on published research from the four WHOCCs in EMR. The secondary objective is to classify them based on the level of KM educational outcomes.
Methodology
A task force of three educationists with Ph D in ME was formed for this project. A conceptual framework was developed by the taskforce as a guide for literature review. The following databases – PubMed, Google Scholar, EMBASE, ERIC, along with websites of WHOCCs, were chosen for the literature search. The search was conducted by the task force, using either relevant keywords such as “faculty development”, “assessment”, “medical education”, “mentoring”, “curriculum development”, “course design”, “accreditation”, “program evaluation”, “teaching methods”, “e-learning”, “blended learning”, “innovation in medical education” or names of authors who were faculty members at the WHOCCs (till May 2020). A structured search was carried out using suitable Boolean operators “AND”, “OR” and “NOT”, for all four WHOCCs at EMRO. The articles thus obtained were saved under “collections” in National Center for Biotechnology Information (NCBI) for easy storage and recovery. All the available articles related to ME from the four WHOCCs (from inception to May 2020) regardless of nature of study design, methodology or duration of implementation, were included while opinion papers, short communications, and conference presentations were excluded from this review. In-depth analysis of the articles was limited to those with full-text available in English. Directors of WHOCCs were also contacted via email and requested to share a list of published research done at their institutions in the field of ME.
The articles collected were screened and divided into five domains or principal areas of research namely: (1) Curriculum Development and Course Design (CDCD), (2) Student Assessment (SA), (3) Quality, Accreditation, and Program Evaluation (QAPE), (4) Teaching and Learning (TL) and (5) Innovation in ME (IME). All the articles were critically reviewed based on the agreed protocol and further classified based on the KM of educational outcomes (1: reaction/perception towards the program, 2: learning acquired at the end of the program, 3: behavioural changes after attending the program, 4: demonstratable results such as patient outcome, institutional growth, etc attributed to the program). Classification of all the articles based on major findings, study design, Kirkpatrick’s model of evaluation, WHOCCs and domains are presented in Table S1.
Results
A total of 96 articles representing published works from the four WHOCCs were selected for inclusion in this literature review. The date of publication spanned from 1998 to 2020. Scientific documentation of the scholarly work in ME in EMR started in EDC, Sudan, in 1998.9
A second level of analysis involved distillation of articles based on date of publication. For this second level of analysis, only recent articles published within the last five years (2017–2020) (n = 37) were selected for inclusion in the literature review. The rate of publication of articles increased in recent years in tandem with advances in technology and shifts in the variables that define modern society. Analysis focusing on recent articles would allow the researchers capture recent trends and contemporary thinking regarding best practices in ME based on principal research domains and Kirkpatrick model of educational outcomes. The highest rate of publication was from CRHPE, Pakistan at 54%, followed by CHPED, Bahrain at 18%, CRD, Egypt at 16%, and lastly, EDC Sudan at 8% (See “List of articles” in Tables S2 and S3).
Insert Table 1: (2017–2020) Research Domains and Kirkpatrick Outcomes.
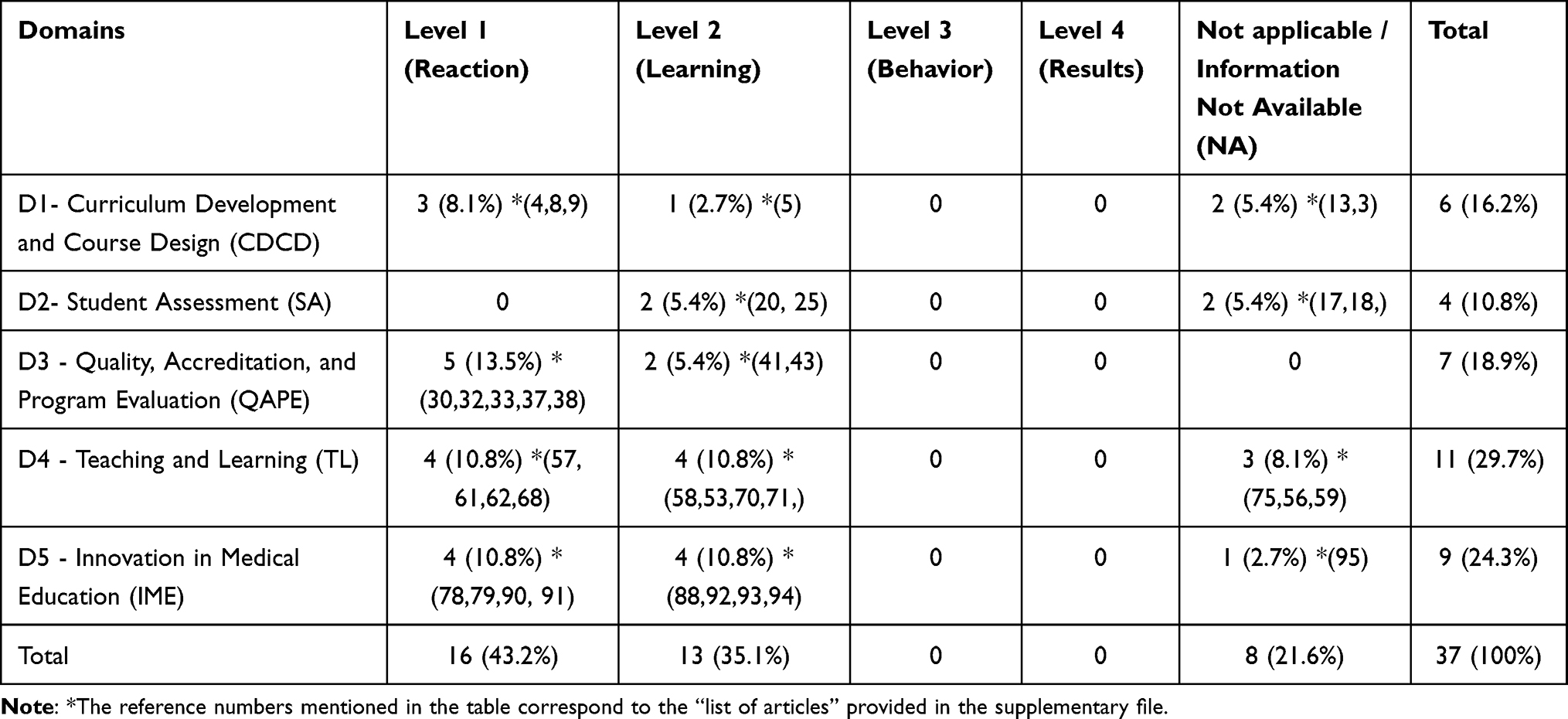 |
Table 1 (2017–2020) Articles Classified Based on Domains and Kirkpatrick’s Model of Evaluation |
Classification Based on Research Domains
As shown in Table 1, the results from classification of all WHOCC articles from the EMR region based on research domains revealed teaching and learning (TL) as the domain that received the highest publication focus at 29.7%, followed by innovation in medical education at 24%, quality, accreditation, and program evaluation (QAPE) at 18.9%, curriculum development and course design (CDCD) at 16%, and lastly, student assessment (SA) at 10.8%.
Classification Based on Kirkpatrick Model of Evaluation
Table 1 shows the result from classification of all articles based on Kirkpatrick model of evaluation. The largest proportion of publications fell under the reaction to training (level 1) category at 43%, followed by learning outcomes from training (level 2) at 25%, and “behavior” (level 3) at 1%. A large proportion of the publications (21%) fell under the “information not available or not applicable” category.
Cross-Tabulation: Research Domain and Kirkpatrick Outcomes
Comparing across both domain and Kirkpatrick outcomes, the highest publication rate was for reactions to training under the quality, accreditation, and program evaluation (QAPE) domain at 13.5%. The same publication rates were found for reaction to training (level 1) and learning outcomes from training (Level 2) (10.8%, respectively) for two domains, training and learning (TL) and innovations in medical education (IME). This result also mirrors the results for classification of recent ME WHOCC publications based on principal research domain.
Cross Tabulation: WHOCCS and Kirkpatrick Outcomes Classification of recent articles (2017–2020) was also done based on WHOCC and Kirkpatrick outcomes, yielding the following results (Table 2). As shown in Table 2, publications in ME best practices by the WHOCCs in EMR only focused on reactions to learning (level one) and learning outcomes from training (level 2). There were no results for behavior (level 3) and behavior (level 4). CRHPE, Pakistan, had the highest rate of publications for reaction to learning at 27%, while the other WHOCCS – CHPED, Bahrain, CRD, Egypt, and EDC, Sudan, had the same rate of publications for this outcome at 5.4%, respectively. CRHPE, Pakistan similarly had the highest publication rate for learning outcomes for training (level 2) at 24.3%, followed by CRD, Egypt at 8.1%, and CHPED, Bahrain at 2.7%. EDC, Sudan, had no publications (0%) on this training outcome.
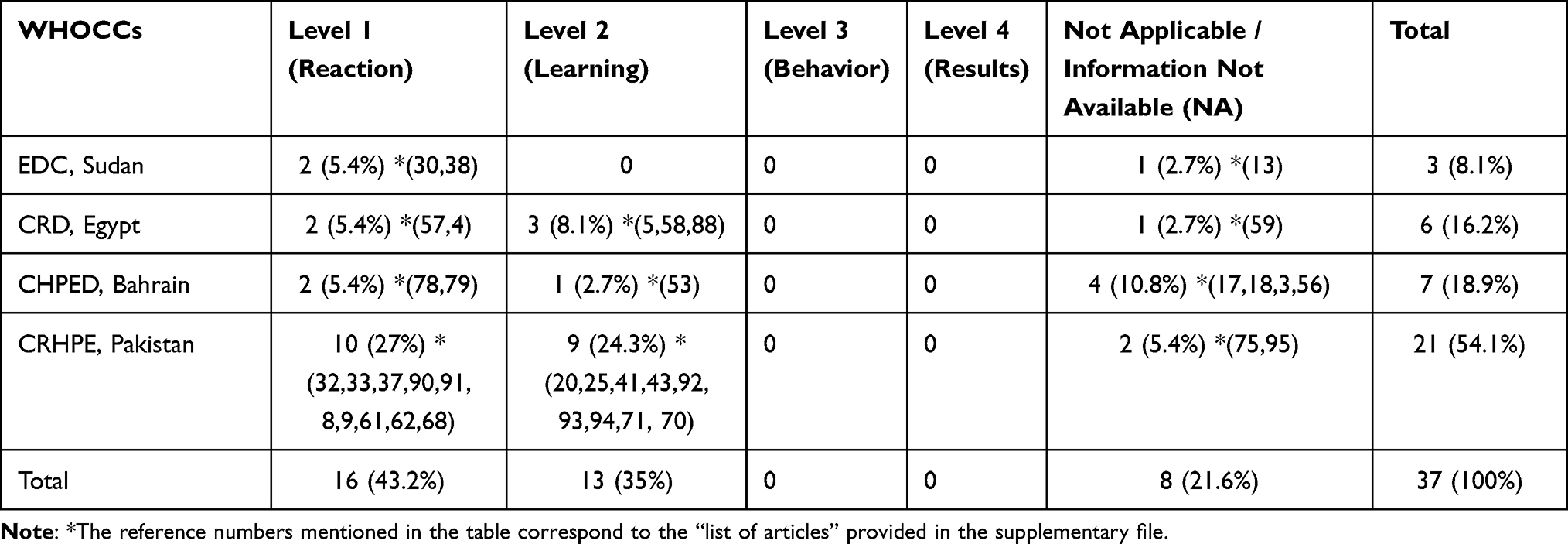 |
Table 2 (2017–2020) Articles Classified Based on WHOCCs and Kirkpatrick’s Model of Evaluation |
Discussion
The association between ME and evidence-based health delivery has been recognized globally. The establishment of four WHOCCs in EMR serve as nodal points for more collaboration in these two areas in the region and within the spheres of global influence created by cooperation with the WHO.
The best practices that emerged from this analysis of the literature are presented based on principal research domains to promote conceptual clarity.
Rapid changes and complexities in demography, lifestyle, community needs, emerging diseases, climate change and digital learning environments necessitate development, implementation and evaluation of new and innovative curricula.10 Sustainable health-care education depends on factors such as engaging teaching methods with evolved pedagogies.11 All the four WHOCCs in EMR have acted in recognition of these facts and have contributed immensely to the innovation and curriculum development domains as evidenced by the numbers and range of publications that have emerged from this EMR. Such contributions cover areas such as curriculum analysis,12 evidence-based learning (EBM),13 and curriculum review.14 Specific curriculum examples include specially designed courses such as patient safety course;15 EBM integration into undergraduate medical curriculum;13 integrated curriculum at undergraduate level16 and integrated-modular system in undergraduate medical education were identified as effective strategies for improving ME outcomes.
In addition to traditional assessment tool such as multiple-choice questions,17 new assessment techniques like competency-based E-assignments18 and use of a wide range of assessment methods12 have been tested by WHOCCs in EMR. Additional and rigorous research in this area remains essential.
Educational institutions all over the world are expected to formulate their own programs and protocols for quality assurance and accreditation.19 Strategies such as socially accountable health professional education (SAHPE) that facilitate an equally skilled but more socially competent workforce20 and utilization of student feedback21 emerge as promising strategies for improving quality in ME education. Implementation of evidence-based educational techniques that support learning such as Based Learning (PBL), clinical rotations, lectures, and integrated methods of teaching, are also important to quality.22
The highest rate of recent publications was on teaching and learning with equal representation across two Kirkpatrick outcomes only, reaction and learning. Numerous contributions to best practice literature emerged under this domain. Effective strategies studied include clinical simulation,23–25 and self-directed learning.26 Additional effective learning strategies include use of the mini-CEX;27,28 SPICES strategy, and a well-defined policy for curriculum management.12 Interactive lectures foster deep learning and critical thinking.14 Examples include training using a web-based simulated patient cases program “Diagnostic Clinical Reasoning Program (DxR)”23 and computer-based animations.29
Positive reaction to ME educational programs were supported by effective feedback mechanisms,21 and improved and non-threatening learning environments.30 Positive experiences were also created through motivative teaching techniques such as tutoring and coaching, and development of team work.16,25
Innovation in ME is a challenging task for any institution due to cultural inertia, faculty resistance, and lack of infrastructure.31 Most of the recommended innovations are habitually grounded on methods which are not supported by sufficient evidence.32 Numerous teaching and learning strategies that emerged from this review of the literature are based on innovative educational technologies and responsive approaches to the delivery of education.
Conclusion and Recommendations
Publications in ME best practices by WHOCCs in EMR reveal their commitment to the use of innovative approaches to improve learning and knowledge creation at their institutes. Wide dissemination of their published works supports the advancement of ME in the region and beyond. Proper documentation and publication of their institutes’ expertise allow CCs to share both their success stories and lessons learned with other institutes in the EMR. This review of the recent literature presents some of the best practice contributions that have emerged from these WHOCCs. The results reveal current best practices in ME adopted by the WHOCCs across principal research domains in ME. The findings indicate higher focus and contributions in the “quality, accreditation, and program evaluation”, “teaching and learning” and “innovation in medical education” domains. The results also reveal that the predominant educational outcomes in the region based on the Kirkpatrick model of evaluation are learners reactions and perception about the educational activity, and the acquisition of intended learning outcomes. Some priority areas for ME in the region based on these results might be improving best practice attention on “curriculum development and course design” and “student assessment” domains. It is also essential to improve educational outcome in the areas of application of acquired knowledge (level 3) and improvement in key performance indicators (level 4) based on the Kirkpatrick model of evaluation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization (WHO). Global network of WHO collaborating centres for occupational health: ways of working. WHO Press; 2016.
2. World Health Organization (WHO). Collaborating centres; 2021. Available from: https://wwwwhoint/about/partnerships/collaborating-centres.
3. Fahal AH. Medical education in the Sudan: its strengths and weaknesses. Med Teach. 2007;29(9–10):910–914. doi:10.1080/01421590701812991
4. University of Gezira (UofG). Administration; 2021. Available from: http://meduofgedusd/EN/Departmentaspx?Dep=3006.
5. Arabian Gulf University (AGU). http://www.arabian gulf university.com, Available from https://www.agu.edu.bh/en/search/pages/default.aspx?#k=World%20health%20organisation.
6. Hosny S, El Wazir Y, El Kalioby M, Farouk O, Ghaly M. Role of suez canal university, faculty of medicine in Egyptian medical education reform. Health Prof Educ. 2016;2(1):44–50. doi:10.1016/j.hpe.2016.01.007
7. Talaat W, Salem H. A new opportunity for Egyptian health professions educators. Med Educ. 2009;43(5):498–499. doi:10.1111/j.1365-2923.2009.03341.x
8. Kirkpatrick D, Kirkpatrick J. Evaluating Training Programs: The Four Levels. Berrett-Koehler Publishers; 2006.
9. Magzoub MEMA, Schmidt HG, Abdel‐Hameed AA, Dolmans D, Mustafa SE. Student assessment in community settings: a comprehensive approach. Med Educ. 1998;32(1):50–59. doi:10.1046/j.1365-2923.1998.00151.x
10. Schneiderhan J, Guetterman TC, Dobson ML. Curriculum development: a how to primer. Fam Med Commun Health. 2019;7(2):e000046. doi:10.1136/fmch-2018-000046
11. Tun MS. Fulfilling a new obligation: teaching and learning of sustainable healthcare in the medical education curriculum. Med Teach. 2019;41(10):1168–1177. doi:10.1080/0142159X.2019.1623870
12. Ahmed YA, Alneel S. Analyzing the curriculum of the faculty of medicine, University of Gezira using Harden’s 10 questions framework. J Adv Med Educ Prof. 2017;5(2):60.
13. Atwa H, Abdelaziz A. Evidence-based medicine (EBM) for undergraduate medical students: a six-step, integrative approach. Med Teach. 2017;39(sup1):S27–S32. doi:10.1080/0142159X.2016.1254750
14. Khalid K, Ahmad SA. Effectiveness of interactive lectures on knowledge retention and students motivation in undergraduate medical education-a mixed method study. Pak Armed Forces Med J. 2019;69(1):206–211.
15. Eltony SA, El-Sayed NH, El-Araby -SE-S, Kassab SE. Implementation and evaluation of a patient safety course in a problem-based learning program. Educ Health. 2017;30(1):44. doi:10.4103/1357-6283.210512
16. Asad M, Khaliq T. Faculty perception regarding integrated curriculum at undergraduate level: a qualitative study. Pak Armed Forces Med J. 2020;70(1):217–223.
17. Kheyami D, Jaradat A, Al-Shibani T, Ali FA. Item analysis of multiple choice questions at the department of paediatrics, Arabian Gulf University, Manama, Bahrain. Sultan Qaboos Univ Med J. 2018;18(1):e68. doi:10.18295/squmj.2018.18.01.011
18. Amin HA, Shehata MHK, Ahmed SA. Step-by-step guide to create competency-based assignments as an alternative for traditional summative assessment. MedEdPublish. 2020;9:120. doi:10.15694/mep.2020.000120.1
19. Blouin D, Tekian A. Accreditation of medical education programs: moving from student outcomes to continuous quality improvement measures. Acad Med. 2018;93(3):377–383. doi:10.1097/ACM.0000000000001835
20. Woolley T, Clithero-Eridon A, Elsanousi S, Othman A-B. Does a socially-accountable curriculum transform health professional students into competent, work-ready graduates? A cross-sectional study of three medical schools across three countries. Med Teach. 2019;41(12):1427–1433. doi:10.1080/0142159X.2019.1646417
21. Ansari T, Usmani A. Students perception towards feedback in clinical sciences in an outcome-based integrated curriculum. Pak J Med Sci. 2018;34(3):702. doi:10.12669/pjms.343.15021
22. Reza Z, Jadoon HK, Danish SH, Sa FK, Ahmed F. Student’s opinion regarding teaching methods: a survey amongst MBBS and BDS students of a private Medical University in Karachi-Short Communication. J Pak Med Assoc. 2018;68(8):1281–1284.
23. Hassan AB, Aziz Elamin A, Jaradat AAK. Impact of clinical simulation on the clinical competence of medical students clerkship training. Bahrain Med Bull. 2018;40(4):230–233.
24. Gaber DA, Shehata MH, Amin HAA. Online team‐based learning sessions as interactive methodologies during the pandemic. Med Educ. 2020;54(7):666–667. doi:10.1111/medu.14198
25. Farghaly A, Abdelaziz A. Coaching as a tool for personal and professional development in a Problem-Based Learning (PBL) medical curriculum: a qualitative study. Educ Med J. 2017;9(3):4.
26. Atwa HS. Assessment of medical students’ readiness for self-directed learning. Egypt J Commun Med. 2018;36(1):21.
27. Baqai S. Mini-Cex A reliable and doable workplace-based assessment tool. Pak Armed Forces Med J. 2018;68(6):1571–1575.
28. Sultana S. Mini-cex: feasibility, acceptability and effectiveness of its use in the learning of post graduate residents. Pak Armed Forces Med J. 2018;68(3):601–607.
29. Khan MA, Shukr I, Sabir S, Qamar K. Effect of computer based animations on learning of physiology. Pak Armed Forces Med J. 2017;67(2):271–275.
30. Ahmed Y, Taha MH, Al-Neel S, Gaffar AM. Students’ perception of the learning environment and its relation to their study year and performance in Sudan. Int J Med Educ. 2018;9:145. doi:10.5116/ijme.5af0.1fee
31. Rohlfsen CJ, Sayles H, Moore GF, et al. Innovation in early medical education, no bells or whistles required. BMC Med Educ. 2020;20(1):1. doi:10.1186/s12909-020-1947-6
32. Delgaty L, Fisher J, Thomson R. The ‘dark side’of technology in medical education. MedEdPublish. 2017;6:21.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.