")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Benefits of Working from Home During the COVID-19 Pandemic for Undiagnosed Workers with Attention-Deficit/Hyperactivity Disorder Symptoms
Authors Ishimoto Y, Sotodate T, Namba Y, Uenishi T, Iwasaki K, Tomita H
Received 31 March 2023
Accepted for publication 5 July 2023
Published 15 July 2023 Volume 2023:19 Pages 1607—1621
DOI https://doi.org/10.2147/NDT.S414862
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Taro Kishi
Yoshikazu Ishimoto,1 Takuma Sotodate,2 Yuki Namba,3 Tatsuhiro Uenishi,4 Katsuhiko Iwasaki,4 Hiroaki Tomita5
1Medical Affairs Department, Shionogi & Co., Ltd., Osaka, Japan; 2Japan Medical Office, Takeda Pharmaceutical Company Limited, Tokyo, Japan; 3Medical Affairs Department, Shionogi & Co., Ltd., Tokyo, Japan; 4Data Science Department, Medilead, Inc., Tokyo, Japan; 5Department of Psychiatry, Tohoku University Graduate School of Medicine, Sendai, Japan
Correspondence: Yoshikazu Ishimoto, Medical Affairs Department, Shionogi & Co., Ltd, 1-8, Doshomachi 3-chome, Chuo-ku, Osaka, 541-0045, Japan, Tel +81-6-6209-7412, Fax +81-6-6202-2239, Email [email protected]
Purpose: Our previous study suggested that working conditions might impact work productivity amid the COVID-19 pandemic. This study aimed to investigate the association between working from home (WFH) and depressive symptoms, work productivity, and quality of life (QOL), in undiagnosed workers with attention-deficit/hyperactivity disorder (ADHD) symptoms during the COVID-19 pandemic.
Methods: During the pandemic, the survey was conducted among eligible workers with (N = 904) and without (N = 900) ADHD symptoms based on the Adult ADHD Self-Report Scale [ASRS]. Each group was further stratified by working conditions (full working on-site [FWOS], hybrid, full WFH [FWFH]). Two-way ANOVA was performed to investigate the impact of WFH on depressive symptoms (Patient Health Questionnaire [PHQ-9] score), work productivity (Work Productivity and Activity Impairment scale [WPAI] scores), and QOL (EuroQol 5-Dimensions 5-Levels [EQ-5D-5L] score). The Tukey–Kramer test was used to assess differences between the stratified subgroups. Poisson and multiple regression analyses were also performed to assess the factors associated with these outcomes.
Results: Other than PHQ-9 score between FWOS and hybrid work in workers with ADHD symptoms (p < 0.05), no significant differences were observed in outcomes among the working condition subgroups in both workers with and without ADHD symptoms. In workers with ADHD symptoms, hybrid work and FWFH were significantly associated with a lower PHQ-9 score (hybrid, p < 0.001; FWFH, p < 0.05) but neither were significantly associated with WPAI score nor EQ-5D-5L. Annual income and discretionary work were significantly associated with a lower PHQ-9 score and a higher EQ-5D-5L score in workers with ADHD symptoms. Job type (manufacture/construction) was significantly associated with a lower presenteeism score.
Conclusion: WFH (hybrid and FWFH) may be associated with lower depressive symptoms compared with FWOS in undiagnosed workers with ADHD symptoms. The findings may be useful when considering suitable working environments for workers especially with ADHD symptoms.
Keywords: depressive symptoms, hybrid work, quality of life, undiagnosed ADHD, work productivity, working condition
Introduction
Attention deficit hyperactivity disorder (ADHD) is a neurodevelopmental disorder affecting both children and adults.1 Previous studies have suggested that children with ADHD and who performed poorly at school were at risk of negative consequences such as school dropout,2 reduced future opportunities for education and employment, social difficulties, and lower self-esteem.3 ADHD symptoms are associated with poor academic performance, which is also influenced by depressive symptoms.4 Not only in childhood but also in adulthood, ADHD symptoms negatively impact daily life and activities, particularly academic achievement, and professional/working life.5 Health-related work impairment and decreased work productivity in adult workers with ADHD have been reported worldwide, in countries including Japan,6 the US,7,8 and the UK.9 Also, adult ADHD symptoms may impair work productivity, QOL, and mental well-being.10
Moreover, adult ADHD is commonly associated with comorbidities such as depression, anxiety,4 sleep difficulty, substance use, and personality disorders,5,11,12 which may limit educational and occupational options. Nevertheless, gaps remain in the diagnosis and treatment of ADHD among the adult population.11,12
Although adults with ADHD can pursue many careers, the suitability of specific jobs may depend on their symptoms, coping strategies, personal strengths, and environment.13 For example, symptoms of inattention may be a burden for certain types of jobs that required sustained concentration; however, other types of jobs, such as those requiring creative thinking, may be a better option for individuals who have combined (both inattention and hyperactivity) ADHD symptoms.14
The recent COVID-19 pandemic has affected peoples’ daily and work life owing to restrictions implemented for social distancing, including working from home (WFH). Lockdowns have negatively impacted the quality of life (QOL) and mental well-being of children, adolescents,15,16 and adults.17–20 It has been estimated that these countermeasures may increase unemployment and suicide rates in adults.21 Besides layoffs, bankruptcy/collapse in businesses, and reduced working hours, one of the most drastic changes in the work environment due to the COVID-19 pandemic is WFH, which has been rapidly and widely adopted in various work settings.
During COVID-19, adults with ADHD have shown emotional and sleeping difficulties, stress and anxiety, and lower physical and psychological QOL.22,23 Additionally, undiagnosed adults with ADHD symptoms have also experienced difficulties during the COVID-19 pandemic, such as increased mistakes and decreased productivity or missed deadlines.24 Identifying the difficulties faced by undiagnosed adults who have some ADHD symptoms may allow for early intervention and treatment to improve their situation amid the COVID-19 pandemic.
Previously, we reported that work productivity significantly improved during the pandemic in both adults with and without ADHD symptoms compared with that before the COVID-19 pandemic.25 This result suggests that certain factors might have affected work productivity. For example, working conditions, such as WFH may affect work productivity by providing benefits to some adults in dealing with their ADHD symptoms through fewer distractions and increased focus in optimal home settings. Identifying how work environment-related factors affect work productivity is important not only for the COVID-19 pandemic but also for similar situations that might occur in the future. This knowledge would be particularly useful for workers with ADHD symptoms and provide valuable insights to lead a better life.
To the best of our knowledge, there have been no studies that identify the factors influencing worker’s mental well-being, work productivity, and QOL during the COVID-19 pandemic period, with a focus on working conditions especially workers with ADHD symptoms. Therefore, in this study, we focused on working conditions, particularly WFH, during the pandemic and aimed to clarify whether working conditions are associated with mental well-being, work productivity, and QOL among adult workers with and without ADHD symptoms.
Materials and Methods
Study Design and Ethics
This is a post-hoc study of a previously published web-based survey.25 Survey 1 (demographics, work productivity, and QOL questionnaires) was conducted in Oct–Dec 2019 (before the COVID-19 pandemic), and Survey 2 (screening for ADHD symptoms, depressive symptoms, work productivity, and QOL questionnaires) was conducted in March 2021 (during the COVID-19 pandemic). Data from a Medilead Healthcare Panel (MHP; Medilead, Inc.) collected in Survey 2 were used for this post-hoc analysis. For Survey 2, the participants were asked to answer the questionnaires in relation to their status and condition during the emergency state in Japan between 16 April 2020 and 25 May 2020.
This surveillance was conducted in accordance with the principles of the Japanese Ethical Guidelines for Medical and Health Research Involving Human Subject, and the surveillance protocol was approved by the MINS Research Ethics Committee (MINS-REC-210210, approved March 4, 2021). Informed consent was obtained from all participants using a web form at the beginning of the survey and all responses were anonymized.
Study Participants
The study population was the same as the previously published study25 except for unemployed adults who were excluded from this post-hoc analysis. Briefly, eligible participants were employed adults aged ≥20 years who completed Survey 2. Participants who were diagnosed with ADHD or had received ADHD treatment within 1 year before the study were excluded. Medical professionals were also excluded because they were essential workers who likely had increased work demands and who have medical knowledge and may understand the purpose of the questionnaire.
As previously reported, 187,596 respondents were invited for the screening survey. Of 47,900 eligible participants who completed the Japanese version of the Adult ADHD Self-Report Scale-v1.1 (ASRS-V1.1) screener (Part A),26 1126 (2.35%) were identified as undiagnosed participants with ADHD symptoms, and 1116 participants without ADHD symptoms were selected as matched cohort by sex, age, and job type. Of 1891 participants who completed Survey 2, 87 (4.6%) unemployed participants were excluded. Therefore, 1804 employed participants were included in this post-hoc analysis (with ADHD symptoms, 904 [50.1%]; without ADHD symptoms, 900 [49.9%]). Hence, the participant demographics between these groups were generally similar in this study (Table 1).
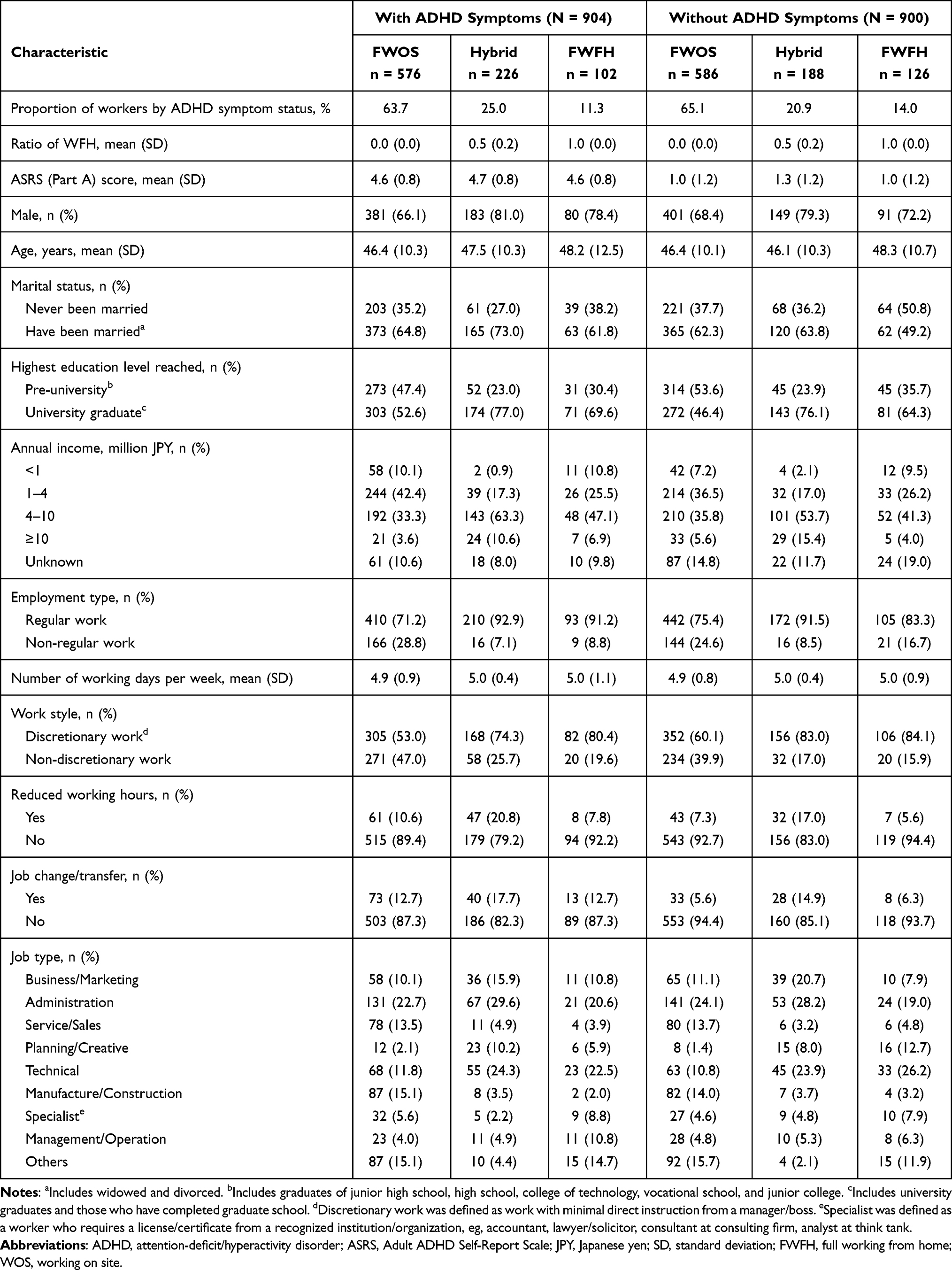 |
Table 1 Participant Demographics and Characteristics by Working Conditions |
Statistical Analysis
In this report, two statistical analyses were planned to assess primary clinical questions: 1) whether working conditions (ie, WFH) are associated with depressive symptoms, work productivity, and QOL levels in workers with and without ADHD symptoms (using 2-way ANOVA); 2) Poisson and multiple regression analyses were conducted to identify factors associated with these outcomes and for robustness of these results in light of covariates and potential confounding factors.
Measurement Scales
The Japanese version of the ASRS-V1.1 screener (Part A)26 was used to categorize participants having ADHD symptoms (ASRS-positive; ASRS Part A score ≥4) and those without ADHD symptoms (ASRS-negative; ASRS Part A score <4).26 The Japanese version of the Patient Health Questionnaire (PHQ-9)27 was used to assess depression levels, where a high score indicates more severe depression symptoms.28 A Japanese translation of the Work Productivity and Activity Impairment (WPAI) scale was used to assess work productivity as previously described.25 This scale consists of four categories: presenteeism, absenteeism, total work impairment (TWI) and total activity impairment (TAI), and denotes the percentage of time affected; therefore, a high score indicates low work productivity.29 The Japanese version of EuroQol 5-dimensions 5-levels (EQ-5D-5L) scale30 was used to assess QOL, where a higher score indicates better QOL. All measurement scales used in this study are well established and validated in English.28,29,31 The Japanese-language version of the PHQ-9 has been validated,27 and Japanese population norms have been established for the EQ-5D-5L.30
Variables
Working conditions were categorized as full working-on-site (FWOS, 0% WFH), hybrid work, full WFH (FWFH, 100% WFH) by calculating the ratio: days of WFH per week/weekly working days. Other information collected for analysis included ASRS Part A score, sex, age, marital status, highest education level, annual income, and other information related to participant work conditions (refer to covariates below and Table 1).
Analysis Methods and Modeling
Descriptive statistics are used for participant demographics and characteristics stratified by presence of ADHD symptoms and by working conditions. Continuous variables were summarized by the stratified group as means with standard deviations (SDs). Categorical variables were treated as frequencies and proportions.
Two-way ANOVA was used to assess the association of working conditions (FWOS, hybrid work, FWFH) with depression severity (PHQ-9), work productivity (presenteeism, absenteeism, TWI, TAI), and QOL (EQ-5D-5L) in workers with and without ADHD symptoms. The association between ADHD symptoms (ASRS positive or negative) and these outcomes were also assessed. Statistical significance between subgroups of working conditions in workers with/without ADHD symptoms was also assessed using the Tukey–Kramer test. Poisson regression was used to assess factors associated with depression severity, given that the PHQ-9 score is expressed as integers only. Multiple regression models were used to assess factors associated with work productivity and QOL.
For the regression analyses, all predictor variables were entered in the model first. The ASRS score and working conditions were forcibly remained in all models in principle as these variables are factors of interest. The model was selected by reducing the predictor variables and by comparing the goodness-of-fit for each test based on the Akaike Information Criterion (AIC). The variance of the inflation factor (VIF) was used to assess multicollinearity in the model.
Covariates used in the regression models were: working conditions (FWOS, hybrid work, FWFH), ASRS score, sex, age, marital status (have been married or never been married), highest education level reached (pre-university or university graduate), annual income (<1, 1–4, 4–10, ≥10 million JPY, or unknown), employment type (regular or non-regular work), number of working days per week, work style (discretionary work [ie, workers had choice/flexibility in their approach to work] or non-discretionary work [ie, follow instructions]), reduced working hours (yes or no), transferring/changing job (yes or no), and job type (business/marketing, administration, service/sales, planning/creative, technical, manufacture/construction, specialist, management/operation, or others) (Table 1). For the categorical variables, the references used for each predictor were: female, have been married, pre-university, annual income <1 million, non-regular work, FWOS, no discretionary work, no reduced working hours, no job change/transfer, and others for job type.
All analyses were performed using R statistical software (version 4.1.1, R Foundation, Vienna, Austria). Statistical significance was considered at a two-sided p-value of <0.05.
Results
Participant Demographics and Characteristics
Of the 1804 participants included in the post-hoc analysis, there were 904 workers with ADHD symptoms and 900 workers without ADHD symptoms (Table 1).
The proportions of working conditions were generally similar among the groups: FWOS, 63.7% (576/904); hybrid, 25.0% (226/904); FWFH, 11.3% (102/904) in workers with ADHD symptoms, and FWOS, 65.1% (586/900); hybrid, 20.9% (188/900); FWFH, 14.0% (126/900) in workers without ADHD symptoms. The mean scores of ASRS (Part A) were generally similar between the working condition subgroups: with ADHD symptoms, 4.6–4.7; without ADHD symptoms, 1.0–1.3. The proportions of males in the cohorts with ADHD symptoms were: FWOS, 66.1% (381/576); hybrid, 81.0% (183/226); FWFH, 78.4% (80/102) and without ADHD symptom were: FWOS, 68.4% (401/586); hybrid, 79.3% (149/188); FWFH, 72.2% (91/126). Mean age was generally similar among all working condition subgroups in both ADHD symptom cohorts: with ADHD symptoms, 46.4–48.2 years; without ADHD symptoms, 46.1–48.3 years (Table 1).
Impact of Working Conditions on Depressive Symptoms, Work Productivity, and QOL
Depressive Symptoms
The mean PHQ-9 score was significantly higher in workers with ADHD symptoms than in workers without ADHD symptoms (8.9 vs 3.5; p < 0.001; Supplementary Figure 1, Left). When the PHQ-9 scores were compared among working condition subgroups in each cohort, the mean PHQ-9 score was significantly lower in the hybrid work subgroup than in the FWOS subgroup in workers with ADHD symptoms when compared by the Tukey–Kramer test (7.9 vs 9.3; p = 0.033), and no significant differences were observed in these subgroups among workers without ADHD symptoms (Supplementary Figure 1, Right).
Work Productivity
All WPAI scores were significantly higher in workers with ADHD symptoms than in workers without ADHD symptoms (Supplementary Figure 2A–D, left). There were no significant differences in all WPAI scores among working condition subgroups when compared across the ADHD symptom cohorts (Supplementary Figure 2A–D, Right).
Quality of Life
EQ-5D-5L score was significantly lower in workers with ADHD symptoms than those without ADHD symptoms (Supplementary Figure 3 Left). No significant differences were identified among the three subgroups regarding working conditions in workers with and without ADHD symptoms (Supplementary Figure 3, Right).
Factors Associated with Depressive Symptoms, Work Productivity and QOL in Workers with ADHD Symptoms
Depressive Symptoms
Poisson regression analysis revealed that ASRS (Part A) score, being male, never been married, number of working days per week, reduced working hours during the COVID-19 pandemic, and job type (administration, technical) were significantly associated with a higher PHQ-9 score, whereas hybrid work, FWFH, age, annual income (1–4, 4–10, ≥10 million JPY, and unknown), discretionary work, and job type (manufacture/construction) were significantly associated with a lower PHQ-9 score (Table 2).
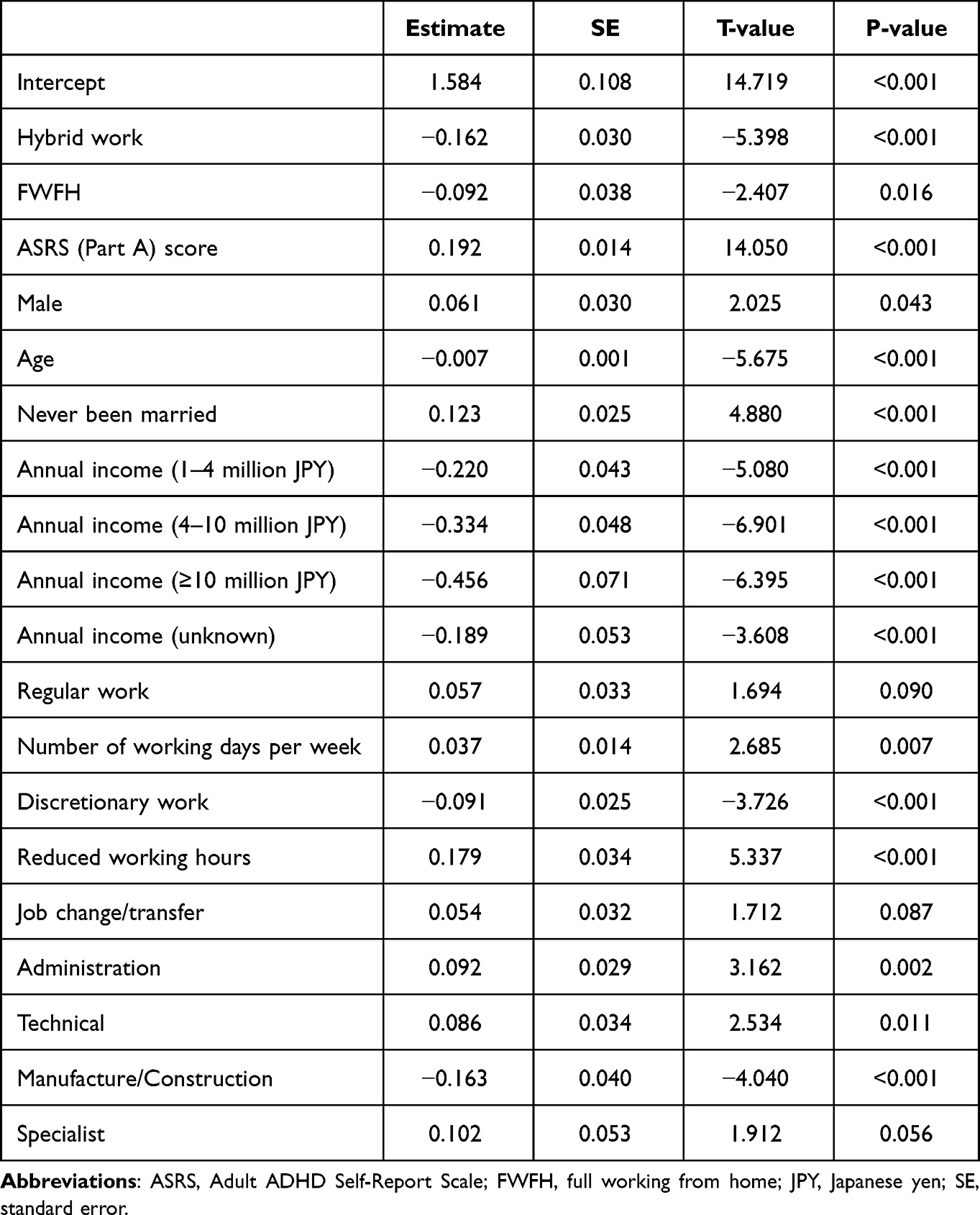 |
Table 2 Poisson Regression Analysis for Depressive Symptom (PHQ-9 Score) in Workers with ADHD Symptoms |
Work Productivity and QOL
Multiple regression analysis revealed that reduced working hours during the COVID-19 pandemic and job type (business/marketing) were significantly associated with a higher absenteeism score (Table 3A).
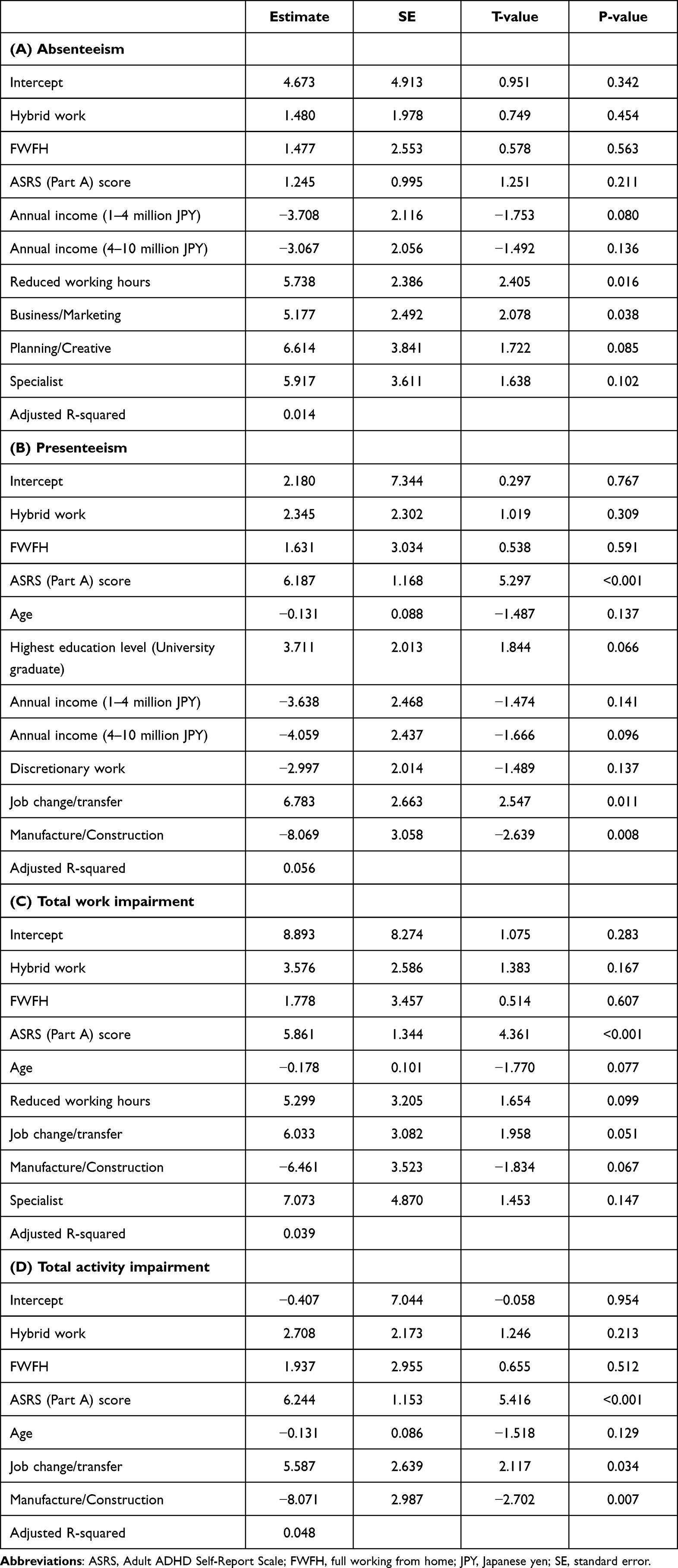 |
Table 3 Multiple Regression Analysis for Work Productivity (WPAI Scores) in Workers with ADHD Symptoms |
The ASRS score and job change/transfer were significantly associated with a higher presenteeism score, whereas job type (manufacture/construction) was associated with a lower presenteeism score (Table 3B). The ASRS score was significantly associated with a higher TWI score (Table 3C). The ASRS score and job change/transfer were significantly associated with a higher TAI score, whereas job type (manufacture/construction) was associated with a lower TAI score (Table 3D). Annual income (1–4, 4–10, and ≥10 million JPY), and discretionary work were significantly associated with a higher EQ-5D-5L score, whereas ASRS score and never been married were associated with a lower EQ-5D-5L score (Table 4).
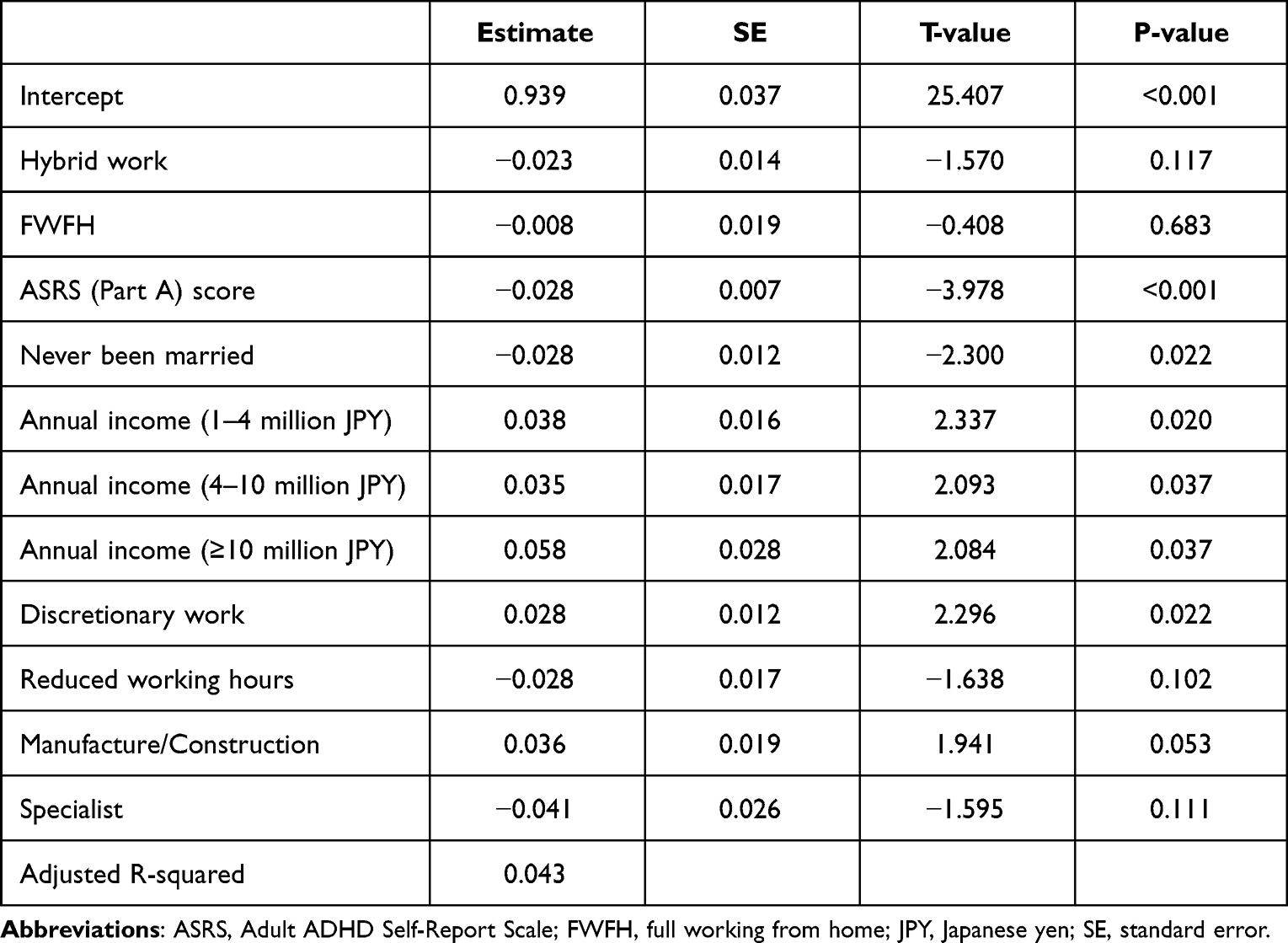 |
Table 4 Multiple Regression Analysis for QOL (EQ-5D-5L Score) in Workers with ADHD Symptoms |
Factors Associated with Depressive Symptoms, Work Productivity and QOL in Workers without ADHD Symptoms
Depressive Symptoms
Poisson regression analysis revealed that hybrid work and FWFH, ASRS score, never been married, regular work, and reduced working hours were significantly associated with a higher PHQ-9 score, whereas age, annual income (4–10, ≥10 million JPY and unknown), discretionary work and job type (business/marketing and technical) were associated with a lower PHQ-9 score (Supplementary Table 1).
Work Productivity and QOL
Multiple regression analysis revealed that regular work, reduced working hours and job type (manufacture/construction and specialist) were significantly associated with a higher absenteeism score, whereas annual income (≥10 million JPY) and number of working days per week were associated with a lower absenteeism score (Supplementary Table 2A).
Hybrid work, FWFH, ASRS score, reduced working hours, and job type (manufacture/construction) were significantly associated with a higher presenteeism score (Supplementary Table 2B). Hybrid work, FWFH, ASRS score, reduced working hours, and job type (manufacture/construction) were significantly associated with a higher TWI score, whereas annual income (≥10 million JPY) and number of working days per week were significantly associated with a lower TWI score (Supplementary Table 2C). FWFH, ASRS score, reduced working hours, and job type (administration) were significantly associated with a higher TAI score (Supplementary Table 2D). Hybrid work, reduced work hours and job change/transfer were significantly associated with a lower EQ-5D-5L score (Supplementary Table 3).
All VIF values used for the regression analyses were <2.2; therefore, significant multicollinearity was not observed in any of the models.
Discussion
This post-hoc analysis investigated associations of working conditions (FWOS, hybrid, FWFH) with depressive symptoms, work productivity, and QOL during the COVID-19 pandemic period. The results suggest that WFH (hybrid and FWFH) may be associated with lower severity of depressive symptoms but is not significantly associated with work productivity or QOL in workers with ADHD symptoms. In contrast, WFH may be associated with higher severity of depressive symptoms but also work productivity and QOL in workers without ADHD symptoms.
The current study confirmed the presence of significantly higher depressive symptoms, lower work productivity, and poorer QOL among adult workers with ADHD symptoms than those without ADHD symptoms, replicating results from previous studies, based on comparisons between adults with and without ADHD symptoms regardless of work conditions.25
Moreover, the results of the regression analyses indicated that having a higher ASRS score was associated with a higher PHQ-9 score, higher WPAI scores (except for absenteeism), and lower EQ-5D-5L score (with ADHD symptoms cohort only), suggesting that workers with more severe ADHD symptoms may experience a greater burden in terms of mental well-being, work productivity, and QOL.10,25
Workers with ADHD Symptoms
Impact of Working from Home
In workers with ADHD symptoms, the results of the Tukey–Kramer test, and Poisson and multiple regression analyses consistently indicated that WFH (hybrid and FWFH) was a significant predictor of lower severity of depressive symptoms, whereas WFH was not significantly associated with work productivity. This result differed from our hypothesis that WFH might be associated with improved work productivity and QOL, observed after, compared with before the COVID-19 pandemic.25
The effects of WFH during the pandemic on mental well-being in healthy workers have been controversial. An online survey of Canadian workers during the third wave of COVID-19 concluded that hybrid work was associated with more positive self-rated mental health compared with only WFH and in-person work.32 Another online survey conducted in Hong Kong reported that people who were more disturbed by not being able to WFH had poorer mental health status.33 In contrast, a US national survey reported that the workers who changed to WFH during the pandemic had higher distress than those who did not,34 which was in line with our results in workers without ADHD symptoms. The impact of WFH on mental well-being is most likely determined on a case-by-case basis and influenced by other factors, such as communication difficulties at work, workspace and setting at home, children at home, and distractions while working, which may also affect work productivity.35,36 Furthermore, family caregivers were at a higher risk of depressive symptoms during the pandemic compared with non-caregivers.37 In this study, data on participant’s family members and their home environment (having a child, being a caregiver for, and have support from another family member) were not collected. Because the home environment can affect work productivity,38 further studies examining the number of family members and this environment are warranted.
Recent studies have suggested that both adult workers with and without ADHD symptoms engaged in WFH may benefit from prior preparation and innovative practices to address factors such as communication with colleagues, workstation settings, and physical exercise, to improve work productivity and mental well-being while engaged in WFH.36,39 Therefore, improving the environment for WFH settings may positively impact mental well-being, work productivity, and QOL. Conversely, this study was conducted during the first state of emergency in Japan, which was declared for the whole country, few employers and employees had adapted to WFH settings or the new lifestyle to improve their work productivity and QOL. Nonetheless, WFH was significantly associated with lower depression symptoms in workers with ADHD symptoms, which was remarkable.
Other Factors Associated with Lower Severity of Depressive Symptoms, Higher Work Productivity and Better QOL
We found that other than working conditions, older age and discretionary work were associated with a lower severity of depressive symptoms, an annual income (1–4, 4–10, ≥10 million JPY, and unknown) and discretionary work were associated with better QOL, and the job type (manufacture/construction) was associated with lower depressive symptoms and higher productivity (presenteeism and TAI) in workers with ADHD symptoms.
The result that older age was associated with less severe depressive symptoms was in line with a web survey obtained during the COVID-19 pandemic in Canada that younger aged (<25 years) participants had poorer mental health (stress, anxiety, and depression) compared with participants of older age.40 Another data analysis of cohorts from three pandemic waves in the UK revealed that severity of depressive symptoms was highest in individuals aged 20 years, followed by those aged 30, 50, and 62 years across all waves.41
Notably, our study indicated that discretionary work was associated with lower severity of depressive symptoms and QOL in workers with ADHD symptoms. This result is in line with a systematic review and meta-analysis, which found that a lack of self-determination and job strain are associated with more severe depressive symptoms.42
In workers with ADHD symptoms, an annual income of >1–4, 4–10, ≥10 million JPY, and unknown was associated with lower severity of depressive symptoms and better QOL. This result was consistent with previous web-survey results from the US, where high-income workers reported increased productivity, which was possibly influenced by better mental and physical status.35 Additionally, in Austria workers with a high income had better QOL and fewer mental health problems than did those with a low income.43
Our results related to job type may simply reflect that workers with ADHD symptoms who engage in manufacture/construction type work were less affected by the burden of the COVID-19 pandemic and that this might be a more suitable type of work for adults with ADHD symptoms. Further research may also benefit to confirm more suitable type of work for adults with ADHD symptoms.
Other Factors Associated with Higher Severity of Depressive Symptoms, Lower Work Productivity and Poorer QOL
Being male and the number of working days per week were associated with a higher PHQ-9 score among workers with ADHD symptoms. Unmarried status was associated with a higher severity of depressive symptoms and QOL in workers with ADHD symptoms. Job change/transfer during the COVID-19 pandemic was associated with a lower work productivity (presenteeism and TAI) and reduced working hours during the pandemic were associated with lower work productivity (absenteeism) and higher severity of depressive symptoms.
Our study suggested being male was associated with higher depressive symptoms in workers with ADHD symptoms. The current study included a higher proportion of male than female workers with ADHD symptoms, and this result was not observed in the cohort without ADHD symptoms. Thus, the result suggests that higher depressive symptoms among male workers may be specific to those with ADHD symptoms. Nonetheless, several studies suggest that female workers tend to have more severe depressive symptoms, psychological distress, and anxiety than male workers,43–45 and a similar result has been reported in college students with ADHD symptoms.46 Therefore, further study is warranted to confirm gender differences in depressive symptoms among workers with ADHD symptoms, during the COVID-19 pandemic.
Unmarried status was associated with higher severity of depressive symptoms and poorer QOL in workers with ADHD symptoms. This is in line with a web survey in Canada that found PHQ-9 scores were higher in single (never been married) participants compared with those who were married/partnered.47 A web survey in China during the first wave of the pandemic found that being married was associated with better QOL compared with being single.48 Social isolation and loneliness, which single participants are most likely to feel, have been identified as major negative consequences of the COVID-19 pandemic and may be associated with higher levels of stress, anxiety, and depression.41,44,47
The number of working days per week was associated with higher severity of depressive symptoms in workers with ADHD symptoms. This suggests that workers with ADHD symptoms may have experienced greater distress, particularly when they had to work a greater number of days per week during COVID-19. This may be partially because workers with ADHD experienced psychological distress during the COVID-19 pandemic similar to those diagnosed adults with ADHD.38,49 Because the results of this study suggest that WFH (hybrid, FWFH) may be expected in reducing depressive symptoms, it may be necessary to consider providing options for WFH and support to provide suitable work settings for workers with ADHD symptoms, especially during the pandemic.
In workers with ADHD symptoms, job change/transfer during the COVID-19 pandemic may be a negative factor for work productivity (presenteeism and TAI) and reduced working hours during the pandemic may also be a negative factor for work productivity (absenteeism) and severity of depressive symptoms. This result may be partly because of the nature of WPAI scores, which ask for the time affected, which is strongly associated with reduced working hours (ie, hours missed from work for during a week owing to a health problem divided by total hours missed and hours worked during that week).
Our results suggest that job change/transfer and reduced working hours during the pandemic may influence lower work productivity and higher depressive symptoms. Although the models in this study did not show significant multicollinearity, younger workers and those having reduced working hours may be associated with low incomes, which may in turn place these workers at risk for more severe depressive symptoms. Nevertheless, reduced working hours, as in “flexibility”, may positively influence working life quality and stress,50 thus, this remains a topic for further investigation.
Our current study suggests that undiagnosed workers with ADHD symptoms may have higher depressive symptoms, lower work productivity, and poorer QOL amid the pandemic compared with workers without ADHD symptoms. Our results also suggest that some factors such as hybrid work, FWFH, discretionary work, and job type (manufacture/construction) may positively influence depressive symptoms. These results suggest that appropriate work arrangements may help workers with ADHD symptoms, particularly those who have depressive symptoms. A previous study has indicated that the symptom of inattention is strongly associated with work-related problems.51 Although the current study did not assess individual neuropsychological performances (inattention, hyperactivity and impulsivity), WFH might have helped in improving concentration and resolving issues the participants experienced in their workplace, eg, social interaction with colleagues, which also might have reflected the association between WFH and lower depressive symptoms.
Workers without ADHD Symptoms
The same analysis was applied to the cohorts without ADHD symptoms. The 2-way ANOVA and the Tukey–Kramer test indicated no significant differences in depressive symptoms, work productivity or QOL among the three subgroups of workers without ADHD symptoms; however, regression analyses indicated that WFH may be associated with higher severity of depressive symptoms as well as lower work productivity and poorer QOL in workers without ADHD symptoms. This difference in the results may be attributed to other factors considered in the regression analyses. Notably, in workers without ADHD symptoms, hybrid work conditions were significantly associated with poor QOL and reduced work productivity (presenteeism and TWI); FWFH was significantly associated with reduced work productivity (presenteeism, TWI and TAI); and both FWFH and hybrid work conditions were significantly associated with higher severity of depressive symptoms.
These results were consistent with previous studies, which have reported negative effects of WFH on productivity.39,52,53 According to survey results conducted at four manufacturing firms in Japan, workers who worked from home experienced greater productivity declines than those who did not.39 Another surveillance study conducted in Japan reported that productivity (comparable to presenteeism) in WFH workers decreased by 30–40% compared with that in FWOS workers. This productivity decline was even lower in employees and firms that introduced the WFH style after the pandemic than in those who introduced it before.52
In workers without ADHD symptoms, there were some positive factors for depressive symptoms, work productivity, and/or QOL: older age, annual income of >4 million JPY, and discretionary work were associated with lower severity of depressive symptoms whereas unmarried status (ie, never been married) was associated with higher severity of depressive symptoms; an annual income of ≥10 million JPY was a positive factor for work productivity (absenteeism and TWI); job change/transfer was a negative factor for QOL; reduced working hours was a negative factor for all outcomes (Supplementary Tables 1–3). These results were generally similar to those shown in workers with ADHD symptoms.
Whereas job type (manufacture/construction) was associated with lower depressive symptoms and higher work productivity (presenteeism and TAI) in workers with ADHD symptoms, this was associated with lower work productivity (absenteeism, presenteeism, and TWI) in workers without ADHD symptoms. The rationale for this difference is unclear, particularly in that the levels of these outcomes were significantly different between cohorts. The previous and our current study revealed that participants/workers with ADHD symptoms have higher severity of depressive symptoms, lower work productivity, and lower QOL than those without. Therefore, the contradictory factors affecting the outcomes in this study between cohorts with and without ADHD symptoms need to be cautiously interpreted. In any case, this is a limitation of this study, in which individual situations cannot be considered in detail.
Limitations
Besides the aforementioned limitations, others include that the participants who were registered in MHP (Medilead Healthcare Panel) may have more interest in health and self-care. Additionally, the participants of this survey were limited to those who were able to use computer and/or smartphone devices; therefore, the possibility of selection bias cannot be precluded. The answers relied on the participant’s retrospective perspective and were subjectively based in general. Also, the possibility of recall bias cannot be precluded; thus, not all answers may reflect the actual participants’ characteristics. This study is cross-sectional, thus a causal relationship between the factors and depressive symptoms, work productivity, and QOL cannot be concluded. Further investigation is necessary, including longitudinal analyses to affirm the causal linkages identified here. The analysis includes multiple comparisons without multiplicity adjustment, which may lead to type 1 errors. The adjusted R-squared values in all models were not high, indicating that there are other factors that may influence the outcomes. Particularly, individuals with ADHD commonly display several comorbidities,11,12 for which data were not collected in this study. These other factors need to be clarified in future research, and the results need to be cautiously interpreted. The detailed characteristics of ADHD symptoms were not considered in this study because the ASRS screener was used to screen participants’ ADHD symptoms. Nevertheless, ASRS Part A Score was significantly associated with most outcomes (except for the absenteeism scores) as a negative factor for both cohorts. Further research may be warranted to clarify whether particular ADHD symptoms (inattention, hyperactivity-impulsivity) would affect these outcomes.
Conclusion
In conclusion, WFH (hybrid and FWFH) may be associated with lower severity of depressive symptoms in undiagnosed workers with ADHD symptoms, while it may be associated with higher severity of depressive symptoms, lower work productivity, and poorer QOL in workers without ADHD symptoms. Moreover, WFH may not impact work productivity and QOL in workers with ADHD symptoms. Although ASRS score, reduced working hours and job change/transfer during the pandemic may be associated with lower work productivity, some positive factors were identified, including job type (manufacture/construction) for work productivity; and annual income (>1 million JPY) and discretionary work for both depressive symptoms and QOL, in workers with ADHD symptoms. These findings may help in considerations for constructing a suitable working environment for workers, particularly those with ADHD symptoms.
Abbreviations
ADHD, attention-deficit/hyperactivity disorder; ASRS, Adult ADHD Self-Report Scale; EQ-5D-5L, EuroQol 5-Dimensions 5-Levels; FWFH, full working from home; FWOS, full working on site; JPY, Japanese yen; MHP, Medilead Healthcare Panel; PHQ-9, Patient Health Questionnaire; QOL, quality of life; WFH, working from home; WPAI, Work Productivity and Activity Impairment.
Acknowledgments
Authors would like to thank all study participants. Medical writing assistance was provided by Mie Yamamoto, PhD, and Andrew Jackson, PhD, at MIMS Co. Ltd., in accordance with the Good Publications Practice guidelines (updated on 30 August 2022; https://www.ismpp.org/gpp-2022), and was funded by Shionogi & Co., Ltd. and Takeda Pharmaceutical Company Limited.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This study was sponsored by Shionogi & Co., Ltd. and Takeda Pharmaceutical Company Limited. Shionogi & Co., Ltd. Medilead, Inc. was involved in the study design, data collection and data analysis, which were funded by Shionogi & Co., Ltd.
Disclosure
YI and YN are employees of Shionogi & Co., Ltd. and own shares in the company. TS is an employee of Takeda Pharmaceutical Company Limited and own shares in the company. TU is an employee and KI was a former employee of Medilead, Inc, which received payment for study design and data analysis from Shionogi & Co., Ltd. HT reports grant funding (paid to Tohoku University) from Daiichi-Sankyo Company, Limited, Eisai Co., Ltd., Otsuka Pharmaceutical Co., Ltd., and Sumitomo Dainippon Pharma Co., Ltd.; and has also received honoraria from Daiichi-Sankyo Company, Limited, EA Pharma Co., Ltd., Eisai Co., Ltd., Janssen Pharmaceutical K.K., Lundbeck, Meiji Seika Pharma Co., Ltd., Mochida Pharmaceutical Co., Ltd., MSD K.K., Mylan EPD G.K., Otsuka Pharmaceutical Co., Ltd., Pfizer Japan Inc., Sumitomo Dainippon Pharma Co., Ltd., Takeda Pharmaceutical Company Limited, and Viatris Inc.
References
1. Posner J, Polanczyk GV, Sonuga-Barke E. Attention-deficit hyperactivity disorder. Lancet. 2020;395(10222):450–462. doi:10.1016/S0140-6736(19)33004-1
2. Mirza H, Roberts E, Al-Belushi M, et al. School dropout and associated factors among Omani children with attention-deficit hyperactivity disorder: a cross-sectional study. J Dev Behav Pediatr. 2018;39(2):109–115. doi:10.1097/DBP.0000000000000522
3. Usami M. Functional consequences of attention-deficit hyperactivity disorder on children and their families. Psychiatry Clin Neurosci. 2016;70(8):303–317. doi:10.1111/pcn.12393
4. Riboldi I, Crocamo C, Callovini T, et al. Testing the impact of depressive and anxiety features on the association between attention-deficit/hyperactivity disorder symptoms and academic performance among university students: a mediation analysis. Brain Sci. 2022;12(9):1155. doi:10.3390/brainsci12091155
5. Pitts M, Mangle L, Asherson P. Impairments, diagnosis and treatments associated with attention-deficit/hyperactivity disorder (ADHD) in UK adults: results from the lifetime impairment survey. Archives of Psychiatric Nursing. 2015;29(1):56–63. doi:10.1016/j.apnu.2014.10.001
6. Kirino E, Imagawa H, Goto T, Montgomery W. Sociodemographics, comorbidities, healthcare utilization and work productivity in Japanese patients with adult ADHD. PLoS One. 2015;10(7):e0132233. doi:10.1371/journal.pone.0132233
7. Pawaskar M, Fridman M, Grebla R, Madhoo M. Comparison of quality of life, productivity, functioning and self-esteem in adults diagnosed with ADHD and with symptomatic ADHD. J Atten Disord. 2020;24(1):136–144. doi:10.1177/1087054719841129
8. Murphy KR, Barkley RA. Occupational functioning in adults with ADHD. ADHD Rep. 2007;15(1):6–10. doi:10.1521/adhd.2007.15.1.6
9. Joseph A, Kosmas CE, Patel C, Doll H, Asherson P. Health-related quality of life and work productivity of adults with ADHD: a U.K. web-based cross-sectional survey. J Atten Disord. 2019;23(13):1610–1623. doi:10.1177/1087054718799367
10. Naya N, Tsuji T, Nishigaki N, et al. The burden of undiagnosed adults with attention-deficit/hyperactivity disorder symptoms in Japan: a cross-sectional study. Cureus. 2021;13(11):e19615. doi:10.7759/cureus.19615
11. Mirza H, Al-Huseini S, Al-Jamoodi S, et al. Socio-demographic and clinical profiles of adult attention deficit hyperactivity disorder patients in a university hospital in Oman. Sultan Qaboos Univ Med J. 2022;22(2):206–211. doi:10.18295/squmj.5.2021.104
12. Katzman MA, Bilkey TS, Chokka PR, Fallu A, Klassen LJ. Adult ADHD and comorbid disorders: clinical implications of a dimensional approach. BMC Psychiatry. 2017;17(1):302. doi:10.1186/s12888-017-1463-3
13. Adamou M, Arif M, Asherson P, et al. Occupational issues of adults with ADHD. BMC Psychiatry. 2013;13:59. doi:10.1186/1471-244X-13-59
14. Girard-Joyal O, Gauthier B. Creativity in the predominantly inattentive and combined presentations of ADHD in adults. J Atten Disord. 2022;26(9):1187–1198. doi:10.1177/10870547211060547
15. Samji H, Wu J, Ladak A, et al. Review: mental health impacts of the covid-19 pandemic on children and youth - a systematic review. Child Adolesc Ment Health. 2022;27(2):173–189. doi:10.1111/camh.12501
16. Seto M, Usukura H, Kunii Y, et al. Mental health problems among university students under the prolonged covid-19 pandemic in Japan: a repeated cross-sectional survey. Tohoku J Exp Med. 2023;260:1–11. doi:10.1620/tjem.2023.J012
17. Ahmed MZ, Ahmed O, Aibao Z, Hanbin S, Siyu L, Ahmad A. Epidemic of covid-19 in China and associated psychological problems. Asian J Psychiatr. 2020;51:102092. doi:10.1016/j.ajp.2020.102092
18. Amerio A, Lugo A, Stival C, et al. Covid-19 lockdown impact on mental health in a large representative sample of Italian adults. J Affect Disord. 2021;292:398–404. doi:10.1016/j.jad.2021.05.117
19. Lipskaya-Velikovsky L. Covid-19 isolation in healthy population in Israel: challenges in daily life, mental health, resilience, and quality of life. Int J Environ Res Public Health. 2021;18(3):999. doi:10.3390/ijerph18030999
20. Usukura H, Seto M, Kunii Y, Suzuki A, Osaka K, Tomita H. The mental health problems of public health center staff during the covid-19 pandemic in Japan. Asian J Psychiatr. 2021;61:102676. doi:10.1016/j.ajp.2021.102676
21. Kawohl W, Nordt C. Covid-19, unemployment, and suicide. Lancet Psychiatry. 2020;7(5):389–390. doi:10.1016/S2215-0366(20)30141-3
22. Hollingdale J, Adamo N, Tierney K. Impact of covid-19 for people living and working with ADHD: a brief review of the literature. AIMS Public Health. 2021;8(4):581–597. doi:10.3934/publichealth.2021047
23. Engel-Yeger B. Emotional status and quality of life in women with ADHD during covid-19. OTJR (Thorofare N J). 2022;42(3):219–227. doi:10.1177/15394492221076516
24. Rivas-Vazquez RA, Ramirez-Mejia C, Diaz S. Undiagnosed adult attention-deficit/hyperactivity disorder detected during the covid-19 pandemic. Prim Care Companion CNS Disord. 2022;24(5). doi:10.4088/PCC.22br03356
25. Nakai T, Tsuji T, Tsuda H, et al. Working conditions, work productivity, quality of life, and depressive symptoms in undiagnosed adults with and without attention-deficit/hyperactivity disorder (ADHD) symptoms during the covid-19 pandemic. Neuropsychiatr Dis Treat. 2022;18:1561–1572. doi:10.2147/NDT.S358085
26. Kessler RC, Adler L, Ames M, et al. The world health organization adult ADHD self-report scale (asrs): a short screening scale for use in the general population. Psychol Med. 2005;35(2):245–256. doi:10.1017/S0033291704002892
27. Muramatsu K, Miyaoka H, Kamijima K, et al. The patient health questionnaire, Japanese version: validity according to the mini-international neuropsychiatric interview-plus. Psychol Rep. 2007;101(3 Pt 1):952–960. doi:10.2466/pr0.101.3.952-960
28. Kroenke K, Spitzer RL, Williams JB. The phq-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
29. Reilly MC, Zbrozek AS, Dukes EM. The validity and reproducibility of a work productivity and activity impairment instrument. Pharmacoeconomics. 1993;4(5):353–365. doi:10.2165/00019053-199304050-00006
30. Shiroiwa T, Fukuda T, Ikeda S, et al. Japanese population norms for preference-based measures: eq-5d-3l, eq-5d-5l, and sf-6d. Qual Life Res. 2016;25(3):707–719. doi:10.1007/s11136-015-1108-2
31. Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new five-level version of eq-5d (eq-5d-5l). Qual Life Res. 2011;20(10):1727–1736. doi:10.1007/s11136-011-9903-x
32. Bodner A, Ruhl L, Barr E, Shridhar A, Skakoon-Sparling S, Card KG. The impact of working from home on mental health: a cross-sectional study of Canadian worker’s mental health during the third wave of the covid-19 pandemic. Int J Environ Res Public Health. 2022;19(18):11588. doi:10.3390/ijerph191811588
33. Choi EPH, Hui BPH, Wan EYF. Depression and anxiety in Hong Kong during covid-19. Int J Environ Res Public Health. 2020;17(10):87.
34. Matthews TA, Chen L, Omidakhsh N, et al. Gender difference in working from home and psychological distress - a national survey of u.S. Employees during the covid-19 pandemic. Ind Health. 2022;60(4):334–344. doi:10.2486/indhealth.2022-0077
35. Awada M, Lucas G, Becerik-Gerber B, Roll S. Working from home during the covid-19 pandemic: impact on office worker productivity and work experience. Work. 2021;69(4):1171–1189. doi:10.3233/WOR-210301
36. Xiao Y, Becerik-Gerber B, Lucas G, Roll SC. Impacts of working from home during covid-19 pandemic on physical and mental well-being of office workstation users. J Occup Environ Med. 2021;63(3):181–190. doi:10.1097/JOM.0000000000002097
37. Noguchi T, Hayashi T, Kubo Y, Tomiyama N, Ochi A, Hayashi H. Association between family caregivers and depressive symptoms among community-dwelling older adults in Japan: a cross-sectional study during the covid-19 pandemic. Arch Gerontol Geriatr. 2021;96:104468. doi:10.1016/j.archger.2021.104468
38. Ando M, Takeda T, Kumagai K. A qualitative study of impacts of the covid-19 pandemic on lives in adults with attention deficit hyperactive disorder in Japan. Int J Environ Res Public Health. 2021;18(4):2090. doi:10.3390/ijerph18042090
39. Kitagawa R, Kuroda S, Okudaira H, Owan H. Working from home and productivity under the covid-19 pandemic: using survey data of four manufacturing firms. PLoS One. 2021;16(12):e0261761. doi:10.1371/journal.pone.0261761
40. Nwachukwu I, Nkire N, Shalaby R, et al. Covid-19 pandemic: age-related differences in measures of stress, anxiety and depression in Canada. Int J Environ Res Public Health. 2020;17(17):6366. doi:10.3390/ijerph17176366
41. Rosa L, Godwin HJ, Cortese S, Brandt V. Predictors of longer-term depression trajectories during the covid-19 pandemic: a longitudinal study in four UK cohorts. Evid Based Ment Health. 2022;25(4):e3–e3. doi:10.1136/ebmental-2022-300461
42. Theorell T, Hammarström A, Aronsson G, et al. A systematic review including meta-analysis of work environment and depressive symptoms. BMC Public Health. 2015;15(1):738. doi:10.1186/s12889-015-1954-4
43. Pieh C, Budimir S, Probst T. The effect of age, gender, income, work, and physical activity on mental health during coronavirus disease (covid-19) lockdown in Austria. J Psychosom Res. 2020;136:110186. doi:10.1016/j.jpsychores.2020.110186
44. Matthews T, Danese A, Caspi A, et al. Lonely young adults in modern Britain: findings from an epidemiological cohort study. Psychol Med. 2019;49(2):268–277. doi:10.1017/S0033291718000788
45. Santomauro DF, Mantilla Herrera AM, Shadid J. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the covid-19 pandemic. Lancet. 2021;398(10312):1700–1712. doi:10.1016/S0140-6736(21)02143-7
46. Nelson JM, Liebel SW. Anxiety and depression among college students with attention-deficit/hyperactivity disorder (ADHD): cross-informant, sex, and subtype differences. J Am Coll Health. 2018;66(2):123–132. doi:10.1080/07448481.2017.1382499
47. Nkire N, Nwachukwu I, Shalaby R, et al. Covid-19 pandemic: influence of relationship status on stress, anxiety, and depression in Canada. Ir J Psychol Med. 2021;1–12. doi:10.1017/ipm.2021.54
48. Duan Y, Peiris DL, Yang M, et al. Lifestyle behaviors and quality of life among older adults after the first wave of the covid-19 pandemic in Hubei China. Front Public Health. 2021;9. doi:10.3389/fpubh.2021.744514
49. Adamou M, Fullen T, Galab N, et al. Psychological effects of the covid-19 imposed lockdown on adults with attention deficit/hyperactivity disorder: cross-sectional survey study. JMIR Form Res. 2020;4(12):e24430. doi:10.2196/24430
50. Voglino G, Savatteri A, Gualano MR, et al. How the reduction of working hours could influence health outcomes: a systematic review of published studies. BMJ Open. 2022;12(4):e051131.
51. Fuermaier ABM, Tucha L, Butzbach M, Weisbrod M, Aschenbrenner S, Tucha O. ADHD at the workplace: ADHD symptoms, diagnostic status, and work-related functioning. J Neural Transm. 2021;128(7):1021–1031. doi:10.1007/s00702-021-02309-z
52. Morikawa M. Work-from-home productivity during the covid-19 pandemic: evidence from Japan. Econ Inq. 2022;60(2):508–527. doi:10.1111/ecin.13056
53. Tejero LMS, Seva RR, Fadrilan-Camacho VFF. Factors associated with work-life balance and productivity before and during work from home. J Occup Environ Med. 2021;63(12):1065–1072. doi:10.1097/JOM.0000000000002377
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.