")
Back to Journals » Infection and Drug Resistance » Volume 16
Benefits and Safety of Empiric Antibiotic Treatment Active Against KPC-K. pneumoniae in Febrile Neutropenic Patients with Acute Leukemia Who are Colonized with KPC-K. pneumoniae. A 7-Years Retrospective Observational Cohort Study
Authors Micozzi A, Minotti C, Capria S, Cartoni C, Trisolini SM, Assanto GM, Barberi W , Moleti ML , Santilli S, Martelli M, Gentile G
Received 18 October 2022
Accepted for publication 23 December 2022
Published 31 January 2023 Volume 2023:16 Pages 695—704
DOI https://doi.org/10.2147/IDR.S393802
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Alessandra Micozzi,1 Clara Minotti,2 Saveria Capria,2 Claudio Cartoni,2 Silvia Maria Trisolini,2 Giovanni Manfredi Assanto,1 Walter Barberi,2 Maria Luisa Moleti,2 Stefania Santilli,3 Maurizio Martelli,1 Giuseppe Gentile1
1Haematology, Department of Translational and Precision Medicine, Sapienza University of Rome, Rome, Italy; 2Department of Haematology, Oncology and Dermatology, Azienda Policlinico Umberto I, Rome, Italy; 3Department of Diagnostics, Azienda Policlinico Umberto I, Rome, Italy
Correspondence: Alessandra Micozzi, Haematology, Department of Translational and Precision Medicine, Sapienza University of Rome, Via Benevento 6, Rome, 00161, Italy, Tel +39 6 857951, Fax +39 6 44241984, Email [email protected]
Purpose: To evaluate the benefits and safety of the empiric antibiotic treatment (EAT) active against KPC-K. pneumoniae in febrile neutropenic patients with acute leukaemia (AL) who are colonised by KPC-K. pneumoniae.
Patients and Methods: A 7-year (2013– 2019) retrospective observational cohort study was conducted at the Haematology, Sapienza Rome University (Italy) on 94 febrile neutropenia episodes (FNE) in AL patients KPC-K. pneumoniae carriers treated with active EAT.
Results: Eighty-two (87%) FNE were empirically treated with antibiotic combinations [38 colistin-based and 44 ceftazidime-avibactam (CAZAVI)-based], 12 with CAZAVI monotherapy. Successful outcomes were observed in 88/94 (94%) FNE, 46/49 (94%) microbiologically documented infections, and 24/27 (89%) gram-negative bloodstream infections (GNB-BSI). Mortality due to infective causes was 4.2% (2.1% within 1 week). KPC-K. pneumoniae infections caused 28/94 FNE (30%) and KPC-K. pneumoniae-BSI was documented in 22 FNE (23.4%) (85% of GNB-BSI), in all cases patients received active EAT, and 21 survived. KPC-K.pneumoniae-BSI mortality rate was 4.5%. CAZAVI-based EAT showed better results than colistin-based EAT (55/56 vs 33/38, p = 0.037), overall and without EAT modification (41/56 vs 20/38, p = 0.02). Empirical combinations including CAZAVI were successful in 98% of cases (43/44 vs 33/38 for colistin-based EAT, p = 0.01), without modifications in 82% (36/44 vs 20/28, p = 0.02). All deaths occurred in patients treated with colistin-based EAT (4/38 vs 0/56, p = 0.02). CAZAVI-containing EAT was the only independent factor for an overall successful response (HR 0.058, CI 0.013– 1.072, p = 0.058). Nephrotoxicity occurred in 3(8%) patients undergoing colistin-based EAT (none in those undergoing CAZAVI-based EAT, p = 0.02).
Conclusion: KPC-K. pneumoniae infections are frequent in colonised AL patients with FNE. EAT with active antibiotics, mainly CAZAVI-based combinations, was effective, safe, and associated with low overall and KPC-K. pneumoniae-BSI-related mortality.
Keywords: ceftazidime-avibactam, colistin, haematological malignancies, KPC-K. pneumoniae-BSI mortality rate
Plain Language Summary
Delayed adequate treatment is associated with very high KPC-K. pneumoniae bloodstream infection (BSI) mortality, reported to be up to 70% in patients with haematological malignancies who received initial inactive treatment. KPC-K. pneumoniae rectal carriage is a risk factor for developing BSI, particularly in acute leukemia patients undergoing intensive chemotherapy. We retrospectively analyzed the benefits of the use of antibiotics active against KPC-K. pneumoniae for the empirical treatment (EAT) of 94 febrile neutropenia episodes in patients with acute leukemia identified as KPC-K. pneumoniae carriers, at high risk of KPC-K. pneumoniae BSI. For this purpose, active EAT including ceftazidime-avibactam (CAZAVI) or colistin was used. Successful outcomes were observed in the 94% of febrile neutropenia episodes, and only 4 (4.2%) episodes were fatal due to infective causes. KPC-K. pneumoniae BSI caused a quarter of febrile neutropenia episodes and in all 22 cases patients received active treatment (active EAT) from the very onset, and 21 survived (KPC-K.pneumoniae-BSI mortality rate was 4.5%). Overall, EAT including CAZAVI showed better results than EAT including colistin (55/56 vs 33/38, p = 0.037), and it was the only independent factor for an overall successful response. All deaths occurred in patients who received colistin (p = 0.02), nephrotoxicity occurred in the 8% of patients receiving colistin and in none of those undergoing CAZAVI (p = 0.02).
In conclusion, KPC-K. pneumoniae BSI are frequent in colonised acute leukemia patients with febrile neutropenia. EAT with active antibiotics, mainly including CAZAVI, was effective, safe, and associated with low overall and KPC-K. pneumoniae-BSI-related mortality.
Introduction
In neutropenic patients with haematological malignancies (HM), inactive antibiotics and delayed adequate treatment are associated with KPC-K. pneumoniae bloodstream infection (KPC-KpBSI)-related mortality, reported to be up to 70%.1–5
In patients with febrile neutropenia, the susceptibility of gram-negative bacteria (GNB) to initial empiric antibiotic therapy (EAT) is key to successful treatment during HM, and the increase in GNB-BSI and multidrug-resistant GNB strains observed in the last few decades is associated with frequent rates of inappropriate EAT and BSI-associated mortality.6 Colonization by KPC-K. pneumoniae is a recognised risk factor for KPC-KpBSI, and colonised HM patients undergoing chemotherapeutic treatments are at high risk,4,7,8 particularly during neutropenia and severe gut mucositis.4,5 First-line anti-GNB antibiotics, cephalosporins, β-lactam–β-lactamase inhibitors, and carbapenems, recommended for EAT of febrile neutropenia episodes (FNE) in a different epidemiological context,9–11 are inactive against KPC-K. pneumoniae. Since 2013, the ECIL guidelines for EAT in febrile neutropenic patients in the era of growing resistance10 included prior colonization or infection with resistant pathogens - such as carbapenemase-producing Enterobacteriaceae (CPE) - among the major risk factors to be considered when choosing empirical therapy for infection with resistant bacteria. The 2020 ECIL guidelines12 for paediatric patients with cancer or post-HCT suggested that EAT should be adjusted for patients colonised or previously infected with resistant GNB or in centres with a high rate of resistant pathogens. Thus, the empirical treatment of FNE with active antibiotics in high-risk HM patients colonised with KPC-K. pneumoniae may guarantee prompt active therapy for KPC-KpBSI and protect patients from KPC-KpBSI-related deaths. In our experience,5 this pre-emptive strategy in colonised HM patients resulted in decreased KPC-KpBSI mortality from 50% to 6%, initial active treatment for all KPC-KpBSI, and prevention of KPC-KpBSI during inactive antibiotics. Currently, according to the guidelines,10,12 active EAT are broadly used in febrile neutropenic KPC-K. pneumoniae carriers, mostly in KPC-K. pneumoniae endemicity and high prevalence of hospitalised HM patients who are colonised, as in Italy.13 Few reports5,14,15 have analysed how efficient it is, compared to historical data. Literature data are focused on the treatment and outcome of KPC-KpBSI16–26 and not on the overall efficacy and safety of the empirical approach of FNE targeting the risk factor represented by KPC-K. pneumoniae colonisation. New combinations with β-lactamase inhibitors,21–29 such as ceftazidime-avibactam (CAZAVI), are increasingly used for the treatment of KPC-K. pneumoniae infections in HM patients5,25,26 and they represent effective therapeutic alternatives with increased efficacy and decreased toxicity compared with older agents.
The main questions related to the empirical approach are overtreatment and overuse of the few available drugs active against KPC-K. pneumoniae, and the potential to select for resistance.
We conducted a retrospective observational study to investigate the possible benefits and safety of antibiotics active against KPC-K. pneumoniae for the empirical treatment of FNE in patients with acute leukaemia (AL) colonised with KPC-K. pneumoniae. We also compared the empirical use of CAZAVI with colistin.
Materials and Methods
This retrospective observational study analysed FNE in patients with AL identified as KPC-K. pneumoniae carriers (including children older than 2 years, patients undergoing intensive chemotherapy, and allogeneic and autologous stem cell transplant recipients) and empirically treated with antibiotic regimens containing CAZAVI or colistin between January 2013 and June 2019 at the Haematology Department, Sapienza Rome University (Italy).
The study was approved by the institutional review board and the internal ethical committee of the Department of Translational and Precision Medicine. The ethical committee waived the need for consent. Patient data were obtained from the medical records of the patients stored at the institutional repository of the Haematology Department, each patient included in the study was given a code for the subsequent analysis and data were analysed using an anonymised database, and in compliance with the Declaration of Helsinki.
Data on the characteristics of AL, total duration of neutropenic episodes (<1000 neutrophils/mm3), profound neutropenia (<100 neutrophils/mm3), clinical presentation, EAT, microbiological documentation, clinical response to EAT, outcome, adverse events (AEs), and toxicity were recorded.
Study Objectives
The primary objective of this study was to evaluate successful response (the resolution of fever and clinical signs of infection, and eradication of the causative microorganisms at the end of the neutropenia episode) to the use of antibiotic regimens active against KPC-K. pneumoniae for the empirical treatment of FNE in AL patients KPC-K. pneumoniae carriers. “Failure” was defined as when the patient died from the primary infection, when KPC-KpBSI persisted beyond the first 48–72 hours of EAT or developed under EAT.
The secondary objective of the study was to compare CAZAVI-based and colistin-based EATs to evaluate differences in: A) mortality (early death between 1 week and crude 30-days mortality, B) successful response, overall and without EAT modification, C) clinical deterioration (shock, acute respiratory distress syndrome, or multiple organ failure), and D) toxicity that required treatment interruption (renal failure was defined as a serum creatinine level ≥2 mg/dL with or without renal replacement therapy).
Clinical Assessment and Follow-Up
KPC-K. pneumoniae colonised patients were identified through rectal swabs collected before admission, upon entry, weekly during hospitalisation, and from January 2018, twice weekly. The response was evaluated on day 4 after EAT (early evaluation), day 14, and at treatment completion (overall evaluation).
Empiric Antibiotic Treatments
The standard EAT used in high-risk febrile neutropenic AL patients in our Institution is piperacillin-tazobactam (4.5 g every 8 h) and tigecycline (100 mg loading dose then 50 mg every 12h) combination.11
From January 2013, the active EAT used was colistin [loading dose of 9 million international units (IU), then 4.5 million IU every 12h] combined with tigecycline (100 mg loading dose then 50 mg every 12h) with or without gentamicin (3 mg/kg/d once a day), with or without meropenem (2 g every 8h).
From August 2017, we started to use CAZAVI (2.5 g every 8h) monotherapy or in combination with tigecycline with or without gentamicin as active EAT. Between August 2017 and February 2018, CAZAVI was not available for routine clinical use in Italy. The patients had received CAZAVI therapy within the bounds of compassionate-use programs administered by the drug manufacturer (Pfizer) after obtaining ethical committee approval and informed written consent from each patient (the drug manufacturer had no influence on the study and on the analysis of the results).
Microbiology
Species identification was performed using MALDI-TOF, and susceptibility testing was performed using an automated VITEK2 system (bioMérieux, Marcy-l’Étoile, France). KPC genetic mechanism of K. pneumoniae blood-isolates was determined by in vitro real-time PCR assay Xpert Carba-R assay (Cepheid, Sunnyvale, CA). MICs of meropenem, colistin, ceftazidime-avibactam, tigecycline, and gentamicin for KPC-K. pneumoniae blood isolates were determined by broth microdilution (Sensititre Gram-Negative MICPlate, ThermoFisherScientific, CA) and interpreted following the European Committee on Antimicrobial Susceptibility Testing.30
Statistical Analysis
Continuous variables were compared using the Kruskal–Wallis test. Categorical variables were compared using the chi-square test corrected for continuity or Fisher’s exact test when indicated; 95% confidence intervals (CIs) for the differences in means and proportions were calculated. Odds ratio (OR) was calculated, when appropriate, based on the chi-square test to determine the protective effect of CAZAVI. Multivariate analysis was performed using the binomial regression logistic model on significant categories found in the univariate analysis that could influence the EAT failure (CAZAVI-based EAT, CAZAVI-based combination EAT) and acute myeloid leukaemia (AML) as underlying disease. Statistical calculations were performed using SPSS statistical package (SPSS for Windows, Release 15.0).
Results
Ninety-four FNE in 55 patients with AL colonised by KPC-K. pneumoniae were analysed. Thirty patients had a single FNE treated with active EAT, 25 patients received more than one active EAT for different FNE (mean 2.5/per patients, range 2–5).
Eighty-nine FNE (95%) occurred in patients identified as KPC-K. pneumoniae carriers within 6 months, notably 55 FNE (59%) developed in patients identified as carriers in the preceding 30 days, during hospitalization for intensive chemotherapy or stem-cell transplant in 48 cases.
The characteristics of the FNE are listed in Table 1. EAT comprised a combination of antibiotics in 87% of cases (38 colistin-based and 44 CAZAVI-based combinations), tigecycline was included in 96% of the combinations, associated with gentamicin in 84%. Empirical CAZAVI monotherapy was used in 12 (13%) FNE (Table 1).
 |
Table 1 Characteristics of 94 Febrile Neutropenia Episodes in 55 Patients with Acute Leukaemia Who are KPC-Klebsiella pneumoniae Carriers Treated with Active Empiric Antibiotic Treatment (EAT) |
Overall successful outcome was obtained in 94% of the FNE (93% of those treated with combinations and all those treated with CAZAVI monotherapy). The reasons for the six failures were death because of primary infection in four (4.2%) cases (one fatal KPC-KpBSI) and one case each of persistent KPC-KpBSI and KPC-KpBSI that developed under EAT (Table 2).
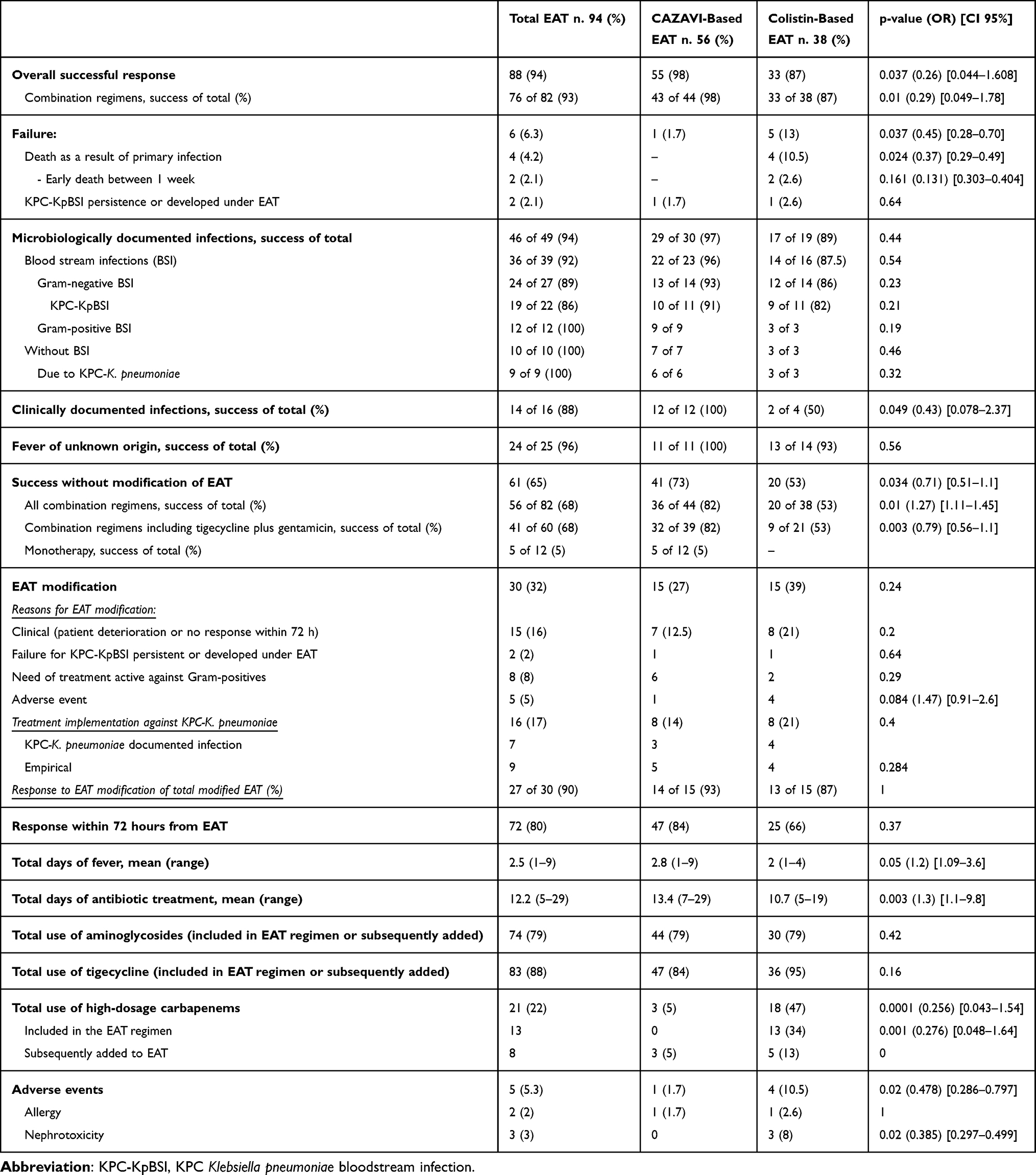 |
Table 2 Response to Empiric Antibiotic Treatment (EAT) |
Of 30 cases (32%), EAT was successfully modified in 27, after a mean of 3.8 days (range 1–8): in 16 cases, the treatment against KPC-K. pneumoniae was implemented for no response after 72h or clinical deterioration [KPC-K. pneumoniae infections (5 KPC-KpBSI) in 7 cases, and empirical modification in 8] (Table 2).
Microbiologically Documented Infections (MDI)
The 52% of FNE were microbiologically documented; 38 (75%) were BSI, 26 were due to GNB, and 22 were KPC-KpBSI (58% of BSI and 85% of GNB-BSI). Seventeen of the 22 (77%) KPC-KpBSI occurred in patients identified as carriers in the preceding 30 days. Nine of the 10 (90%) MDI without bacteraemia were due to KPC.K. pneumoniae (Table 2). Overall, KPC-K. pneumoniae infection was found in 34% of FNE. The susceptibilities of KPC-K. pneumoniae blood-isolates are shown in Table 3. Overall successful response was obtained in 94% of MDI and 89% of GNB-BSI. The 90% of KPC-K. pneumoniae infections, 86% of KPC-KpBSI (only one fatal case), and all KPC-K. pneumoniae MDI without bacteraemia had a successful outcome (Table 2).
 |
Table 3 Susceptibilities of 22 KPC-Klebsiella pneumoniae Blood Isolates |
Four of 12 methicillin-resistant coagulase-negative Staphylococcus BSI documented were PICC-related (two cases each of exit-site infection and thrombophlebitis), and the central line was removed in all cases.
Mortality
Four of the 94 (4.2%) FNE had fatal outcomes due to infective causes (Table 2). Two patients died within 5 days (2.1%), one due to KPC-KpBSI, and one due to septic shock with negative blood cultures. One patient with uncontrolled leukaemia developed acute abdomen and died due to surgical complications on day 12; one patient with interstitial pneumonia died of respiratory failure on day 15.
Overall, KPC-KpBSI mortality rate was 4.5% (Table 4). Death due to KPC-KpBSI occurred in 1.8% of 55 neutropenic AL patients, and 1% of 94 FNE.
 |
Table 4 Characteristics of KPC-Klebsiella pneumoniae BSI and Response to Empiric Antibiotic Treatment (EAT) |
Comparison Between CAZAVI-Based and Colistin-Based EAT
Overall, a successful outcome was observed in 55 of 56 (98%) and 33 of 38 (87%) FNE treated with CAZAVI-based and colistin-based regimens, respectively (p = 0.037), without EAT modification in 73% and 53% of cases, respectively (p = 0.049) (Table 2). All deaths occurred in the colistin-based EAT group, with a FNE mortality rate of 10.5% (p = 0.02) (Table 2).
CAZAVI-based combinations obtained a higher success rate of responses without EAT modification than colistin-based combinations [36/44 (82%) vs 20/38 (53%), p= 0.02]. Notably, tigecycline plus gentamicin combined with CAZAVI was successful without EAT modification in 82% of cases, combined with colistin in 53% (p = 0.003) (Table 2). The multivariable logistic regression model showed that only CAZAVI-containing EAT had a favourable impact on the overall successful response (HR 0.058, CI 0.013–1.072, p = 0.058).
The rates of MDI, BSI distribution, and type of isolated pathogens were similar between the CAZAVI and colistin groups (Table 2). Ten out of eleven (91%) KPC-KpBSI patients responded without modification to the CAZAVI-based EAT, and all patients survived. Eleven KPC-KpBSI patients received colistin-based EAT (including meropenem in 5 cases), the initial treatment was modified in five cases (45%, p = 0.032), and one KPC-KpBSI was fatal on day 5 (9%) (Table 4). When tigecycline and gentamicin were both included, CAZAVI-based empirical combinations were more successful without modification than those colistin-based (p = 0.007).
Toxicity
The incidence of AEs requiring EAT discontinuation was 5.3% (Table 2). Nephrotoxicity resulted in treatment discontinuation in three (8%) patients undergoing colistin (no patient receiving CAZAVI, p = 0.02), and the rate of treatment including aminoglycosides was similar between the two groups (Table 2).
Discussion
This retrospective observational cohort study addressed the overall benefits of the EAT active against KPC-K. pneumoniae, applied to FNE in patients with AL who were carriers of KPC-K. pneumoniae. Active EAT was successful in 94% of the FNE cases and 90% of the KPC-K. pneumoniae infections, and the KPC-KpBSI mortality rate was 4.5%.
EATs, a combination of antibiotics in the large majority of cases, obtained a high rate of successful response compared with historical data,11 remarkably in patients with AL, an independent risk factor for EAT failure,11 and during profound and persistent aplasia, a risk factor for a complicated clinical course.10 The overall mortality rates of 4.2% and 2.1% within one week, evaluated at the end of the febrile episode, were limited. Success without EAT modifications was obtained in 65% of FNE, confirming the overall efficacy of EAT regimens, and against KPC-K. pneumoniae infections. EAT was implemented against KPC-K. pneumoniae in a low number of cases, even empirically.
Active EAT was successful in 90% of KPC-K. pneumoniae infections and 86% of KPC-KpBSI. All KPC-KpBSI patients received active treatment from the very onset; the low related mortality of 4.5% confirmed the better outcome of KPC-KpBSI in patients who received prompt active treatment targeting gut colonization.5–15 Patients with AL are at the highest risk of KPC-KpBSI with unfavourable outcomes.4 AML is independently associated with high KPC-KpBSI related-mortality,4 and 64% of KPC-KpBSI reported in this series developed in AML carriers.
KPC-KpBSI-related mortality was lower than that in other reports.1–5,7,8,15,16,18–25 We previously described 88% of KPC-KpBSI-related mortality with inactive initial treatment chosen according to guidelines,9–11 all patients who died had AML, and 78% had received inactive EAT.4,5 Caston25 reported 45.2% of 30-days mortality in 31 HM patients with CPE bacteraemia who received appropriate EAT in 51% of cases; 79% of patients who died had AL, and 64% had received inactive EAT.
In this study, KPC-K. pneumoniae colonisation in AL patients is confirmed as a predictive factor for KPC-K. pneumoniae infections; during the study period, January 2013-June 2019, among 51 KPC- K. pneumoniae BSI observed in our population of HM patients, including patients with malignancies other than acute leukemia, 39 (76%) developed in KPC-K. pneumoniae colonized patients. Notably, the mortality rate of the 12 KPC-K. pneumoniae BSI in not colonized patients who did not receive initial active treatment, was 42% (unpublished data).
In this study, KPC-K. pneumoniae was involved in one-third of FNE developed AL patients, and KPC-KpBSI was documented in 23.4% of FNE. Furthermore, the KPC-KpBSI incidence of 85% among all GNB-BSI confirmed the higher risk of KPC-KpBSI in AL carriers compared with other haematological patients4 and an increase in endogenous infections, mainly bacteraemias, in AL patients KPC-K. pneumoniae carriers with chemotherapy-related prolonged neutropenia and intestinal toxicity.
CAZAVI represents a valuable option for treating patients with KPC-K.pneumoniae infections.21,28,29 Associated with lower mortality rates respect historical non-CAZAVI-based regimens.22–25 In our experience, the empirical use of CAZAVI, both combination therapy and monotherapy, for the treatment of FNE in AL patients who are KPC-K pneumoniae carriers resulted in better activity, lower toxicity, and a higher rate of successful outcome without EAT modification than colistin-based EAT, and independently associated with a significantly higher rate of overall successful response. Notably, even if observed in a small population of patients, no fatalities were observed with the CAZAVI-based EAT, and the mortality rate of FNE initially treated with colistin was 10.5%.
Data on the empirical use of CAZAVI combinations in neutropenic HM patients are scarce.5,14,15 In contrast, most studies have evaluated the efficacy of CAZAVI combinations for the treatment of CPE. Recently, the beneficial effect of CAZAVI combinations on KPC-KpBSI mortality compared with monotherapy has been questioned,24–29 however, in patients with high mortality scores, CAZAVI combinations resulted in lower KPC-KpBSI mortality than monotherapy.19 We believe that CAZAVI-based combinations should be preferred for active EAT in colonised febrile neutropenic AL patients at the highest risk of KPC-KpBSI, our results highlight better outcomes of FNE empirically treated with CAZAVI-based combinations and suggest a better clinical efficacy for the treatment of KPC-KpBSI. In contrast to the 25% mortality rate reported by Caston25 in eight HM patients with CPE-BSI undergoing CAZAVI combinations administered later as targeted therapy, all our patients with KPC-KpBSI who received initial CAZAVI-based combination survived without treatment modification in the majority of cases. Early discontinuation of combination partners should be the best strategy in appropriate clinical and microbiological conditions. This study analyzed EAT in high-risk acute leukemia patients KPC- K.pneumoniae carriers, with a long period of profound neutropenia, mean 12 days with less than 100 neutrophils/mm3. The de-escalation of antibiotics in the setting of still profoundly neutropenic high-risk patients is not supported by published experiences, and may be not appropriate.
The incidence of AEs was low, especially for CAZAVI-based regimens, and even if observed in a small population of patients, nephrotoxicity was only associated with colistin despite the comparable use of other nephrotoxic drugs.
CAZAVI proved active against our KPC-K. pneumoniae blood isolates. CAZAVI resistance in KPC-K. pneumoniae is described, more likely in CAZAVI monotherapy than in combination,28,29 but no decreased susceptibility or CAZAVI resistance emerged in prospective studies.23 Our prevalent use of CAZAVI in combination might have limited the selection of CAZAVI-resistant subpopulations.28
Prospective randomised studies on the management of CRE colonisation and infections in neutropenic HM patients are lacking. The major limitations of the study include its monocentric and retrospective design, however, the homogeneous population of high-risk AL patients, the high rate of microbiological documentation, and the >7-years observation period strengthen our results on the benefits of active EAT. Larger studies are needed to confirm our results on the better efficacy of CAZAVI-based EAT over colistin-based EAT, and to compare mono- versus combination EAT in the setting of high-risk patients hospitalized in countries characterized by widespread multidrug resistance.
Conclusion
Colonisation with KPC-K. pneumoniae, in high-risk neutropenic patients with AL was confirmed a major risk factor for infection, mainly KPC-KpBSI. As recently suggested by the ECIL guidelines,12 determination of KPC-K. pneumoniae colonisation may represent an adequate and efficacious tool for selecting HM patients with FN who require the adjustment of EAT, targeted to the potential MDR pathogen, to reduce the rate of inactive EAT and BSI-related mortality. Among febrile neutropenic patients with AL who are KPC-K pneumoniae carriers, empirical treatment with antibiotics active against KPC-K. pneumoniae, mainly CAZAVI-based combinations, was effective, safe, and associated with low overall and KPC-KpBSI-related mortality.
Ethical Approval
For this observational retrospective study has been obtained from the Institutional Review Board (IRB) and the Internal Ethical Committee of the Department of Translational and Precision Medicine, Sapienza University of Rome, Italy.
Funding
No external funding was received for this study.
Disclosure
Dr. A. Micozzi and Dr. G. Gentile report support for attending meetings and travelling from Pfizer and Gilead. The other authors report no conflicts of interest in this work.
References
1. Tofas P, Skiada A, Angelopoulou M, et al. Carbapenemase-producing Klebsiella pneumoniae bloodstream infections in neutropenic patients with haematological malignancies or aplastic anaemia: analysis of 50 cases. Int J Antimicrob Agents. 2016;47:335–339. doi:10.1016/j.ijantimicag.2016.01.011
2. Trecarichi EM, Pagano L, Martino B, et al. Bloodstream infections caused by Klebsiella pneumoniae in onco-hematological patients: clinical impact of carbapenem resistance in a multicentre prospective survey. Am J Hematol. 2016;91(11):1076–1081. doi:10.1002/ajh.24489
3. Poucha SM, Satlin MJ. Carbapenem-resistant Enterobacteriaceae in special populations: solid organ transplant recipients, stem cell transplant recipients, and patients with haematologic malignancies. Virulence. 2017;8:391–402. doi:10.1080/21505594.2016.1213472
4. Micozzi A, Gentile G, Minotti C, et al. Carbapenem-resistant Klebsiella pneumoniae in high-risk haematological patients: factors favouring spread, risk factors and outcome of carbapenem-resistant Klebsiella pneumoniae bacteraemias. BMC Infect Dis. 2017;17:203. doi:10.1186/s12879-017-2297-9
5. Micozzi A, Gentile G, Santilli S, et al. Reduced mortality from KPC-K. pneumoniae bloodstream infection in high-risk patients with haematological malignancies colonized by KPC-K. pneumoniae. BMC Infect Dis. 2021;21:1079. doi:10.1186/s12879-021-06747-8
6. Martinez-Nadal G, Puerta-Alcalde P, Gudiol C, et al. Inappropriate empiric antibiotic treatment in high-risk neutropenic patients with bacteraemia in the era of multidrug resistance. Clin Infect Dis. 2020;70:1068–1074. doi:10.1093/cid/ciz319
7. Amit S, Mishali H, Kotlovsky T, Schwaber MJ, Carmeli Y. Bloodstream infections among carriers of carbapenem-resistant Klebsiella pneumoniae: etiology, incidence and predictors. Clin Microbiol Infect. 2015;21:30–34. doi:10.1016/j.cmi.2014.08.001
8. Cattaneo C, Di Blasi R, Skert C, et al. Bloodstream infections in haematological cancer patients colonized by multidrug-resistant bacteria. Ann Hematol. 2018;97:1717–1726. doi:10.1007/s00277-018-3341-6
9. Freifeld AG, Bow EJ, Sepkowitz KA, et al. Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the infectious diseases society of America. Clin Infect Dis. 2011;52:e56–e93. doi:10.1093/cid/cir073
10. Averbuch D, Orasch C, Cordonnier C, et al. European guidelines for empirical antibacterial therapy for febrile neutropenic patients in the era of growing resistance: summary of the 2011 4th European conference on infections in leukaemia. Haematologica. 2013;98:1826–1835. doi:10.3324/haematol.2013.091025
11. Bucaneve G, Micozzi A, Picardi M, et al. Results of a multicentre, controlled, randomized clinical trial evaluating the combination of piperacillin/tazobactam and tigecycline in high-risk hematologic patients with cancer with febrile neutropenia. J Clin Oncol. 2014;32:1463–1471. doi:10.1200/JCO.2013.51.6963
12. Lehrnbecher T, Averbuch D, Castagnola E, et al. 8th European conference on infections in leukaemia: 2020 guidelines for the use of antibiotics in paediatric patients with cancer or post-haematopoietic cell transplantation. Lancet Oncol. 2021;22(6):e270–e280. doi:10.1016/S1470-2045(20)30725-7
13. Micozzi A, Assanto GM, Cesini L, et al. Reduced transmission of Klebsiella pneumoniae carbapenemase-producing K. pneumoniae (KPC-KP) in patients with haematological malignancies hospitalized in an Italian hospital during the COVID-19 pandemic. JAC Antimicrob Resist. 2021;3:dlab167. doi:10.1093/jacamr/dlab167
14. Micozzi A, Ansuinelli M, Minotti C, et al. Ceftazidime-avibactam as empirical therapy in febrile neutropenic high-risk haematological patients colonized with carbapenem-resistant Klebsiella pneumonia.
15. Forcina A, Baldan R, Marasco V, et al. Control of infectious mortality due to carbapenemase-producing Klebsiella pneumoniae in hematopoietic stem cell transplantation. Bone Marrow Transplant. 2017;52(1):114–119. doi:10.1038/bmt.2016.234
16. Daikos GL, Tsaousi S, Tzouvelekis LS, et al. Carbapenemase-producing Klebsiella pneumoniae bloodstream infections: lowering mortality by antibiotic combination schemes and the role of carbapenems. Antimicrob Agents Chemother. 2014;58(4):2322–2328. doi:10.1128/AAC.02166-13
17. Perez F, Chakhtoura NG, Papp-Wallace KM, Wilson BM, Bonomo RA. Treatment options for infections caused by carbapenem-resistant Enterobacteriaceae: can we apply “precision medicine” to antimicrobial chemotherapy? Expert Opin Pharmacother. 2016;17(6):761–781. doi:10.1517/14656566.2016.1145658
18. Bassetti M, Giacobbe DR, Giamarellou H, et al. Management of KPC-producing Klebsiella pneumoniae infections. Clin Microbiol Infect. 2018;24(2):133–144. doi:10.1016/j.cmi.2017.08.030
19. Gutiérrez-Gutiérrez B, Salamanca E, de Cueto M, et al. Effect of appropriate combination therapy on mortality of patients with bloodstream infections due to carbapenemase-producing Enterobacteriaceae (INCREMENT): a retrospective cohort study. Lancet Infect Dis. 2017;17(7):726–734. doi:10.1016/S1473-3099(17)30228-1
20. Rodríguez-Baño J, Gutiérrez-Gutiérrez B, Machuca I, Pascual A. Treatment of infections caused by extended-spectrum-beta-lactamase-, AmpC-, and carbapenemase-producing Enterobacteriaceae. Clin Microbiol Rev. 2018;4:e00079. doi:10.1128/CMR.00079-17
21. King M, Heil E, Kuriakos S, et al. Multicenter study of outcomes with ceftazidime-avibactam in patients with carbapenem-resistant Enterobacteriaceae infections. Antimicrob Agents Chemother. 2017;61(7):e00449–e00517. doi:10.1128/AAC.00449-17
22. Shields RK, Hong Nguyen M, Chen L, Press EG, Potoski BA, Marini RV. Ceftazidime-avibactam is superior to other treatment regimens against carbapenem-resistant Klebsiella pneumoniae bacteremia. Antimicrob Agents Chemother. 2017;61(8):e00883–e00917. doi:10.1128/AAC.00883-17
23. van Duin D, Lok JJ, Earley M, et al. Colistin versus ceftazidime-avibactam in the treatment of infections due to carbapenem-resistant Enterobacteriaceae. Clin Infect Dis. 2018;66(2):163–171. doi:10.1093/cid/cix783
24. Tumbarello M, Raffaelli F, Giannella M, et al. Ceftazidime-avibactam use for KPC-Klebsiella pneumoniae infections: a retrospective observational multicentre study. Clin Infect Dis. 2021;73:1664–1676. doi:10.1093/cid/ciab176
25. Castón JJ, Lacort-Peralta I, Martín-Dávila P, et al. Clinical efficacy of ceftazidime/avibactam versus other active agents for the treatment of bacteraemia due to carbapenemase-producing Enterobacteriaceae in hematologic patients. Int J Infect Dis. 2017;59:118–123. doi:10.1016/j.ijid.2017.03.021
26. Criscuolo M, Trecarichi EM. Ceftazidime/Avibactam and ceftolozane/Tazobactam for multidrug-resistant gram negatives in patients with haematological malignancies: current experiences. Antibiotics. 2020;9:58. doi:10.3390/antibiotics9020058
27. Zhanel GG, Lawrence CK, Adam H, et al. Imipenem-relebactam and meropenem-vaborbactam: two novel carbapenem-β-lactamase inhibitor combinations. Drugs. 2018;78:65–98. doi:10.1007/s40265-017-0851-9
28. Soriano A, Carmeli Y, Omrani AS, Moore LSP, Tawadrous M, Irani P. Ceftazidime-avibactam for the treatment of serious gram-negative infections with limited treatment options: a systematic literature review. Infect Dis Ther. 2021;10:1989–2034. doi:10.1007/s40121-021-00507-6
29. Li D, Fei F, Yu H, et al. Ceftazidime-avibactam therapy versus ceftazidime-avibactam-based combination therapy in patients with carbapenem-resistant gram-negative pathogens: a meta-analysis. Front Pharmacol. 2021;12:707499. doi:10.3389/fphar.2021.707499
30. The European Committee on Antimicrobial Susceptibility Testing. Breakpoint tables for interpretation of MICs and zone diameters. (EUCAST, Version 10.0, 2020-01-01). Available from: http://www.eucast.org/clinical_breakpoints/.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.