")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Benefit of Prompt versus Delayed Use of Single-Inhaler Fluticasone Furoate/Umeclidinium/Vilanterol (FF/UMEC/VI) Following a COPD Exacerbation
Authors Mannino D , Bogart M, Germain G, Huang SP, Ismaila AS , Laliberté F, Jung Y, MacKnight SD, Stiegler MA , Duh MS
Received 25 September 2021
Accepted for publication 12 February 2022
Published 5 March 2022 Volume 2022:17 Pages 491—504
DOI https://doi.org/10.2147/COPD.S337668
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Min Zhang
David Mannino,1 Michael Bogart,2 Guillaume Germain,3 Shirley P Huang,2 Afisi S Ismaila,4,5 François Laliberté,3 Young Jung,3 Sean D MacKnight,3 Marjorie A Stiegler,6,7 Mei Sheng Duh8
1Department of Medicine, University of Kentucky, Lexington, KY, USA; 2GlaxoSmithKline, Value Evidence and Outcomes, Research Triangle Park, NC, USA; 3Groupe d’analyse, Ltée, Montréal, QC, Canada; 4GlaxoSmithKline, Value Evidence and Outcomes, Collegeville, PA, USA; 5Department of Health Research Methods, Evidence, and Impact, McMaster University, Hamilton, ON, Canada; 6GlaxoSmithKline, Medical Affairs, Research Triangle Park, NC, USA; 7Department of Anesthesiology and Critical Care, University of North Carolina, Chapel Hill, NC, USA; 8Analysis Group, Boston, MA, USA
Correspondence: Michael Bogart, GlaxoSmithKline, Value Evidence and Outcomes, 5 Moore Drive, PO Box 13398, Research Triangle Park, NC, 27709-3398, USA, Tel +1919-889-7413, Email [email protected]
Purpose: Triple therapy (TT; inhaled corticosteroid, long-acting muscarinic antagonist, and long-acting β2-agonist) is recommended for patients with chronic obstructive pulmonary disease (COPD) at risk of exacerbation, although the optimum timing of TT initiation remains unclear. This study evaluated the impact of prompt versus delayed initiation of single-inhaler TT (fluticasone furoate, umeclidinium, and vilanterol [FF/UMEC/VI]) following a COPD exacerbation.
Patients and Methods: This retrospective cohort study used data from the IQVIA PharMetrics® Plus database. Patients initiating FF/UMEC/VI following a COPD exacerbation between September 18, 2017 and September 30, 2019 (exacerbation = index date) were categorized as prompt (within 30 days of index) or delayed (31– 180 days after index) FF/UMEC/VI initiators. Patients were aged ≥ 40 years at index, had ≥ 12 months’ continuous health insurance coverage before index (baseline), and ≥ 6 months’ coverage after index (follow-up). Patients with a COPD exacerbation or claim for FF/UMEC/VI during baseline were excluded. Inverse probability weighting was used to adjust for differences in baseline characteristics between cohorts. Exacerbations (overall, moderate, and severe), healthcare costs, and readmissions were evaluated during follow-up.
Results: A total of 1904 patients (prompt: 529; delayed: 1375) were included. After weighting, baseline characteristics were well balanced between cohorts. Patients in the prompt cohort had significantly lower rates per person-year (PPY) of overall (0.98 vs 1.23; rate ratio [RR] [95% CI] = 0.79 [0.65– 0.94], p = 0.004), moderate (0.86 vs 1.03; RR [95% CI] = 0.84 [0.69– 0.99], p = 0.038), and severe (0.11 vs 0.20; RR [95% CI] = 0.57 [0.37– 0.79], p = 0.002) exacerbations, compared with delayed initiators. Mean all-cause and COPD-related healthcare costs were significantly lower among prompt initiators (all-cause: $26,107 vs $32,400 PPY, p = 0.014; COPD-related: $12,694 vs $17,640 PPY, p = 0.002).
Conclusion: Prompt initiation of FF/UMEC/VI following a moderate or severe COPD exacerbation was associated with significant reductions in exacerbations and healthcare costs relative to delayed initiation.
Keywords: chronic obstructive pulmonary disease, exacerbation, healthcare cost, single-inhaler triple therapy
Introduction
Chronic obstructive pulmonary disease (COPD) is a common respiratory disorder that represents a significant cause of morbidity and mortality worldwide, and is associated with a substantial economic burden.1 Episodes of acute worsening of respiratory symptoms, known as exacerbations of COPD, are a key driver of the clinical and economic burden of the disease.2–4 More specifically, hospitalization due to exacerbation of COPD is associated with high costs and readmission rates, along with an increased risk of death.3,5,6
Management options for COPD may include pharmacological treatments, pulmonary rehabilitation, and interventional therapies, such as lung volume reduction surgery.4 Pharmacological maintenance therapies include inhaled bronchodilators, such as long-acting muscarinic antagonists (LAMAs) and long-acting β2-agonists (LABAs), and inhaled corticosteroids (ICS; usually taken in combination with a LABA).4 Together, these therapies help to relieve COPD symptoms, reduce the frequency of exacerbations, and slow the progression of respiratory symptoms.7,8 The Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines recommend triple therapy with an ICS, LAMA, and LABA in patients whose symptoms are not adequately controlled with dual therapies (LABA+LAMA or ICS+LABA), or who are at risk of exacerbation (ie, severe airflow limitation, persistent breathlessness, and/or a history of frequent or severe exacerbations).4 However, the current guidelines do not provide recommendations on the optimum timing of triple therapy initiation.
Until recently, triple therapy was administered via multiple inhalers. In September 2017, the first once-daily single-inhaler triple therapy (SITT) comprising fluticasone furoate, umeclidinium, and vilanterol (FF/UMEC/VI) was approved for use in the US by the US Food and Drug Administration (FDA). FF/UMEC/VI was indicated for the long-term maintenance of COPD in patients who were previously receiving fixed dose combination ICS/LABA but required additional bronchodilation, or patients receiving LAMA + ICS/LABA (ie, multiple-inhaler triple therapy [MITT] to SITT switch). This indication was expanded in 2018 to include COPD patients who required improvement in airflow obstruction or who had a history of exacerbation, regardless of prior treatment, and in 2020 for the treatment of asthma in patients ≥18 years.9 Previous studies have demonstrated that COPD patients initiated on FF/UMEC/VI experience reduced rates of moderate or severe exacerbations compared with patients receiving dual therapy with ICS+LABA or LAMA+LABA.10 Patients receiving FF/UMEC/VI have also been shown to experience lower rates of COPD-related hospitalizations compared with patients receiving LAMA/LABA dual therapy.10 A second SITT, comprising budesonide, glycopyrrolate, and formoterol fumarate (BUD/GLY/FOR), was approved by the FDA in 2020 as a COPD maintenance therapy that requires twice-daily dosing.11
Previous real-world studies have demonstrated that adherence to COPD therapy is associated with improved health outcomes and reduced healthcare utilization.12–15 The use of multiple inhalers has been shown to negatively affect treatment adherence in patients with COPD.16,17 In addition, higher rates of COPD exacerbation have been reported among patients prescribed multiple devices requiring different inhalation techniques, compared with those prescribed devices with similar inhalation techniques.18 Taken together, these findings suggest that SITT is a viable option for patients with COPD who continue to experience exacerbations or have poorly controlled symptoms.
The administration of long-acting bronchodilators within 30 days of a hospital discharge due to an exacerbation of COPD is a quality-of-care measure in the US.19 However, there is currently limited real-world evidence to inform the optimal timing of triple-therapy initiation.4,20 A retrospective study in the US suggested that prompt initiation (≤30 days) of MITT following an exacerbation of COPD reduced the rate of future exacerbations and medical costs, compared with patients who had delayed (31–180 days) MITT initiation,20 but these clinical and economic outcomes have yet to be evaluated in patients who receive SITT following a COPD exacerbation. This study aimed to investigate the impact of prompt versus delayed initiation of FF/UMEC/VI on COPD exacerbations, healthcare costs, and hospital readmissions among a commercially insured COPD population using a large US claims database. As data for this analysis were collected prior to the recent approval of BUD/FOR/GLY, the results of this study are limited to FF/UMEC/VI.
Materials and Methods
Data Source
This analysis used data from the IQVIA PharMetrics Plus healthcare claims database, with data ranging from September 18, 2016 to September 30, 2019, which covers patients across all 50 states in the US with an average length of health plan enrollment of 36 months. Commercial insurance is the most frequent plan type captured (the database is generally representative of the <65 years of age, commercially insured population in the US), but other types can also be found including commercial Medicare, commercial Medicaid, self-insured employer groups (as managed by health plan), and pharmacy-only plans. The database contains information on patient demographics, health plan enrollment, and inpatient, outpatient, and pharmacy claims. The data are de-identified and compliant with the Health Insurance Portability and Accountability Act.
Study Design
This was a retrospective weighted cohort study of patients initiating single-inhaler FF/UMEC/VI, delivered using an ELLIPTA™ (GlaxoSmithKline, Brentford, Middlesex, UK) dry powder inhaler, following a COPD exacerbation. The index date was defined as the last day of the patients’ first moderate or severe COPD exacerbation (ie, the date of emergency room [ER] or outpatient visit for moderate exacerbations, or the hospitalization discharge date for severe exacerbations) on or after September 18, 2017 (approval date of FF/UMEC/VI in the US). Outpatient or ER visits with a COPD exacerbation diagnosis code in the primary position and at least one dispensing or administration of a systemic corticosteroid or guideline-recommended antibiotic within 5 days of the visit were defined as moderate exacerbations. A severe exacerbation was defined as a hospitalization with a primary COPD exacerbation diagnosis. Exacerbations occurring within 14 days of each other were considered a single exacerbation episode and were classified according to the highest severity.
Patients were classified into two mutually exclusive cohorts based on the time from the index date to the initiation of FF/UMEC/VI; patients who initiated FF/UMEC/VI within 30 days following the index date were categorized as prompt initiators and patients who initiated FF/UMEC/VI within 31–180 days following the index date were categorized as delayed initiators. The baseline period spanned 12 months prior to the index date, and the follow-up period (observation period) spanned from the index date to the earliest of either health plan disenrollment or end of data availability (September 30, 2019). The follow-up period was used to assess study outcomes: COPD exacerbations, all-cause and COPD-related healthcare costs, and hospital readmissions. Hospital readmissions were evaluated during the follow-up period at 30-, 60-, and 90-day time points among the subset of patients with a severe COPD exacerbation (ie, hospitalization) on the index date. A schematic of the study design is shown in Figure 1.
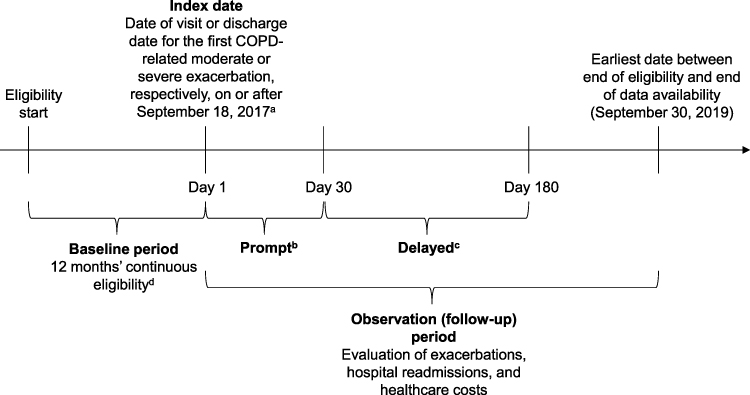 |
Figure 1 Study design. Abbreviations: COPD, chronic obstructive pulmonary disease; FF, fluticasone furoate; UMEC, umeclidinium; VI, vilanterol. Notes: a Approval date of FF/UMEC/VI. b Prompt: initiation of FF/UMEC/VI within 30 days after the index date. c Delayed: initiation of FF/UMEC/VI 31–180 days after the index date. d Patients with ≥1 moderate or severe exacerbation during baseline, or ≥1 pharmacy claim for FF/UMEC/VI prior to index were excluded. |
Study Population
Patients initiating single-inhaler FF/UMEC/VI were selected according to the following criteria: ≥1 moderate or severe COPD exacerbation on or after September 18, 2017, ≥12 months of continuous health insurance coverage prior to the index date (baseline period), ≥6 months of continuous coverage after the index date (follow-up), ≥1 pharmacy dispensing of FF/UMEC/VI within 6 months after the index date, and ≥40 years of age at the index date. For the hospital readmission analysis, patients were also required to have a severe COPD exacerbation on the index date. Patients were excluded from the study if they had ≥1 COPD exacerbation during the baseline period (excluding the index exacerbation) or ≥1 pharmacy dispensing of FF/UMEC/VI prior to the index date.
Study Outcomes
The primary outcome was the rate of COPD exacerbations (overall [moderate and severe combined], moderate only, and severe only), reported per person-year (PPY) of follow-up and calculated as the total number of exacerbations divided by the person-years of observation. Secondary outcomes included the time-to-first overall, moderate, and severe COPD exacerbation, evaluated during the follow-up period using Kaplan–Meier analysis at 3, 6, 9, and 12 months post-index. The median time to exacerbation (time point at which the proportion of patients with an exacerbation reaches 50%) was also reported when reached. Mean all-cause and COPD-related total healthcare costs (medical and pharmacy) were evaluated during the follow-up period. Costs were reported PPY, calculated by dividing the costs incurred during the follow-up period by the person-years of observation. Total healthcare costs were further broken down into hospitalization, ER visit, and outpatient visit cost components. COPD-related costs were identified as any claim with a primary or secondary diagnosis of COPD. All costs were inflation-adjusted to 2019 US dollars based on the medical care component of the Consumer Price Index.21 Time-to-first all-cause and COPD-related hospital readmissions were evaluated during the follow-up period at 30, 60, and 90 days post-index among the subset of patients who had a severe COPD exacerbation at index. COPD-related readmissions were identified as hospitalizations with a primary or secondary diagnosis of COPD.
Statistical Analysis
Inverse probability of treatment weighting (IPTW) based on the propensity score was used to account for differences in baseline patient characteristics between the prompt and delayed cohorts. The propensity score was derived from a logistic regression model conditional on baseline covariates, including age, sex, year of index, US region, insurance plan type, Quan-Charlson comorbidity index (Quan-CCI) score, diagnosis of asthma during baseline, Elixhauser and Diagnostic and Statistical Manual of Mental Disorders-5 (DSM-V) comorbidities (ie, those with ≥5% prevalence in either cohort), type of index COPD exacerbation (moderate or severe), baseline respiratory medication use, and all-cause and COPD-related healthcare resource utilization (HRU) and medical costs.
Patient demographics and clinical characteristics for the prompt and delayed cohorts were summarized using means and standard deviations (SDs) for continuous variables, and frequencies and proportions for categorical variables. Differences in characteristics between cohorts were assessed using standardized differences (std. diff.), with a threshold of <10% considered a negligible imbalance between cohorts.22
During follow-up, COPD exacerbations were compared between weighted cohorts using rate ratios (RRs) obtained from Poisson regression models, with 95% confidence intervals (CIs) and p-values generated from non-parametric bootstrap procedures. Time-to-first exacerbation was compared between weighted cohorts using hazard ratios (HRs) from Cox proportional hazards regression models. Mean cost differences between weighted cohorts were calculated, and 95% CIs and p-values were generated from non-parametric bootstrap procedures. Time to readmission was calculated using Kaplan–Meier analysis and compared between weighted cohorts using Cox proportional hazards regression models.
Results
Patient Characteristics
A total of 529 patients who initiated FF/UMEC/VI following a COPD exacerbation and met all selection criteria were included in the prompt cohort, and 1375 patients were included in the delayed cohort (Figure 2). After weighting, all demographics and clinical characteristics were well balanced between the two cohorts (std. diff. <10%; Table 1). Patients in the prompt and delayed cohorts were observed over an average of 358 days and 369 days, respectively. The type of COPD exacerbation on the index date was comparable between cohorts; 81.2% and 82.6% of patients in the prompt and delayed cohorts had a moderate exacerbation at index, respectively, and 18.8% and 17.4% of patients had a severe exacerbation at index. The mean age at index was 60 years for both prompt and delayed cohorts; the proportion of females was 52.4% and 50.1%, respectively. The mean Quan-CCI score was 1.5 in the prompt cohort and 1.6 in the delayed cohort, and asthma was present in 21.4% and 23.1% of patients during baseline, respectively. All-cause medical costs during the baseline period were also well balanced (prompt: $15,125; delayed: $16,102).
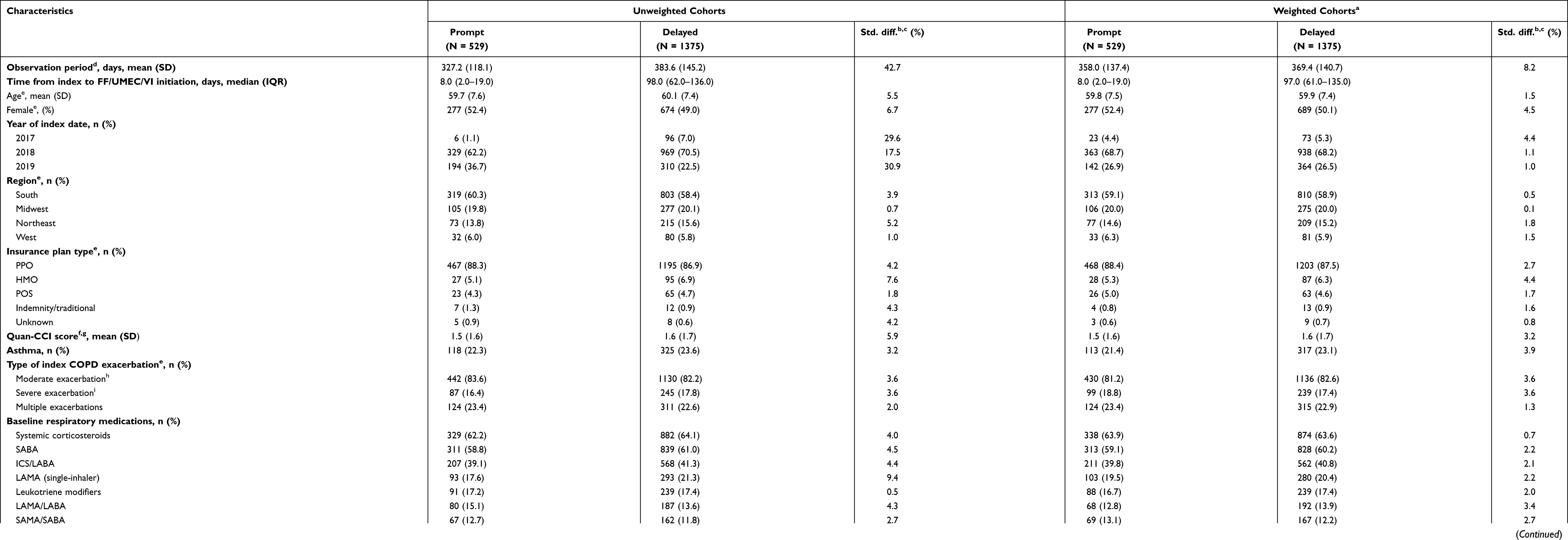 |
Table 1 Baseline Demographics and Clinical Characteristics of Unweighted and Propensity Score-Weighted Patient Cohorts |
 |
Figure 2 Patient attrition. Abbreviations: COPD, chronic obstructive pulmonary disease; ER, emergency room; FF/UMEC/VI, fluticasone furoate, umeclidinium, and vilanterol. Notes: a Moderate COPD exacerbations were defined as an outpatient or ER visit with a COPD exacerbation diagnosis code in the primary position and at least one dispensing/administration of a systemic corticosteroid or guideline-recommended antibiotic within 5 days following, or prior to, the visit. Severe COPD exacerbations were defined as an inpatient hospitalization with a diagnosis code for COPD exacerbation in the primary position. b Continuous eligibility was defined as continuous health plan enrollment with medical and pharmacy coverage. c FF/UMEC/VI was identified using National Drug Codes: 0173–0887-10, 0173–0887-14, and 0173–0887-61. d Initiation of single-inhaler FF/UMEC/VI within 30 days from the index date. e Initiation of single-inhaler FF/UMEC/VI between 31 and 180 days after the index date. |
The most prescribed rescue medications were systemic corticosteroids (prompt: 63.9%; delayed: 63.6%) and short-acting β2-agonists (prompt: 59.1%; delayed: 60.2%). The most prescribed maintenance medications were ICS/LABA (prompt: 39.8%; delayed: 40.8%), single-inhaler LAMA (prompt: 19.5%; delayed: 20.4%), and leukotriene modifiers (prompt: 16.7%; delayed: 17.4%).
The most common comorbidities (those with ≥20% frequency in either cohort) during the baseline period included hypertension (prompt: 58.0%; delayed: 57.7%), substance-related and addictive disorders (prompt: 34.8%; delayed: 33.0%), sleep-wake disorders (prompt: 24.6%; delayed: 23.9%), and anxiety disorders (prompt: 21.8%; delayed: 20.9%) (Supplementary Table S1).
Respiratory Medication Use During Follow-Up, Prior to Initiation of FF/UMEC/VI (Delayed Cohort)
The median duration from index to the initiation of FF/UMEC/VI for the delayed cohort was 97 days. During this time, the most prescribed maintenance medications were ICS/LABA (36.4%), leukotriene modifiers (19.6%), and single-inhaler LAMA (17.3%); 13.0% of patients received MITT prior to initiation of single-inhaler FF/UMEC/VI.
Rate of COPD Exacerbations
Patients in the prompt cohort had significantly lower rates of overall COPD exacerbations compared with those in the delayed cohort (0.98 vs 1.23 PPY; RR [95% CI]: 0.79 [0.65, 0.94], p=0.004), corresponding to a 21% lower rate of overall exacerbations (Table 2). Similarly, patients in the prompt cohort also had significantly lower rates of moderate exacerbations (0.86 vs 1.03 PPY; RR [95% CI]: 0.84 [0.69, 0.99], p=0.038) and severe exacerbations (0.11 vs 0.20 PPY; RR [95% CI]: 0.57 [0.37, 0.79], p=0.002). This corresponds to 16% and 43% lower rates of moderate and severe exacerbations, respectively, for the prompt cohort compared with the delayed cohort.
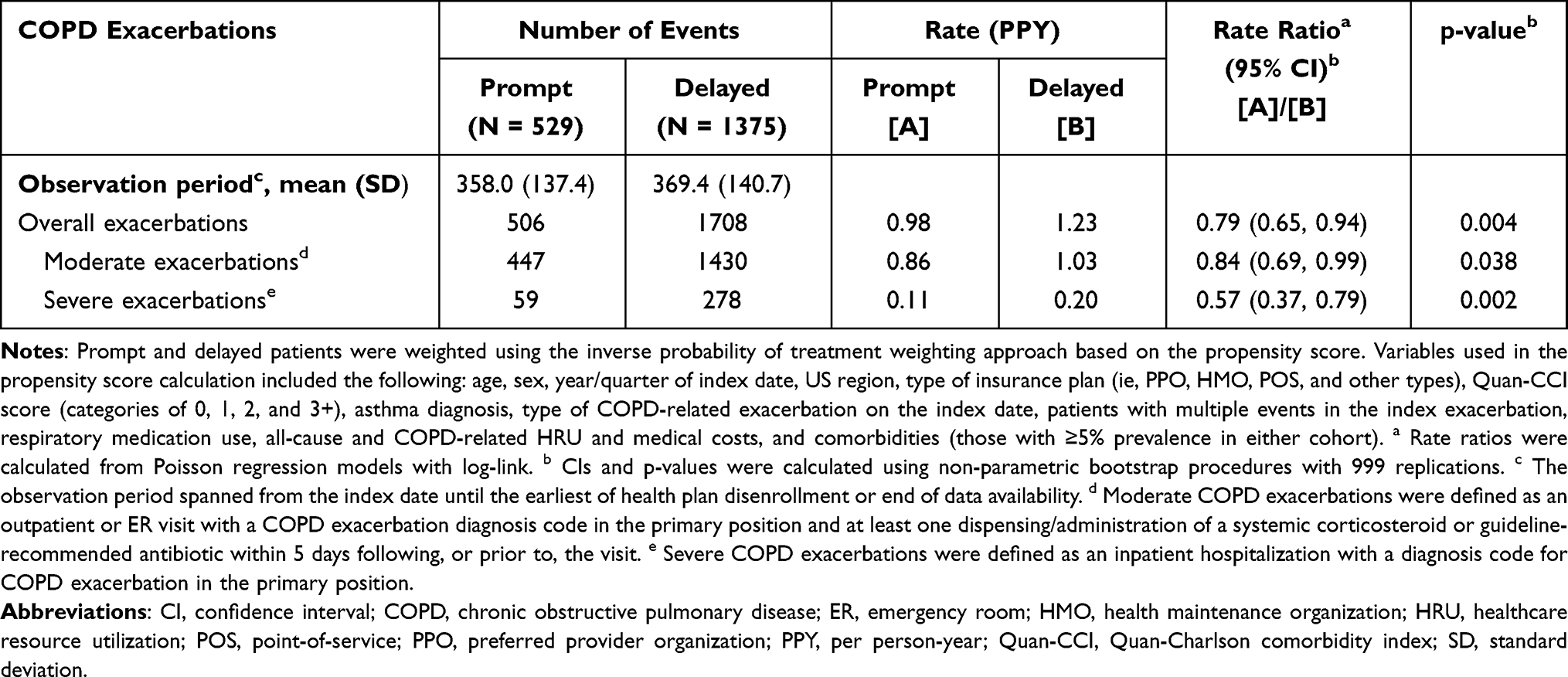 |
Table 2 Rates of COPD Exacerbations Among Weighted Prompt and Delayed Cohorts |
Time-to-First COPD Exacerbation
Kaplan–Meier rates of overall COPD exacerbation were significantly lower at 12 months of follow-up in the prompt compared with the delayed cohort (49.8% vs 59.4%; HR [95% CI]: 0.72 [0.62, 0.83], p<0.001; Figure 3A). Patients in the prompt cohort also had significantly lower Kaplan–Meier rates of moderate exacerbation (44.8% vs 54.3%; RR [95% CI]: 0.73 [0.63, 0.86], p<0.001; Figure 3B) and severe exacerbation (10.9% vs 15.5%; RR [95% CI]: 0.62 [0.45, 0.85], p=0.003; Figure 3C), compared with the delayed cohort. The median time-to-first COPD exacerbation was longer for patients in the prompt versus delayed cohort for overall (367 days vs 200 days) and moderate (435 days vs 292 days) exacerbations.
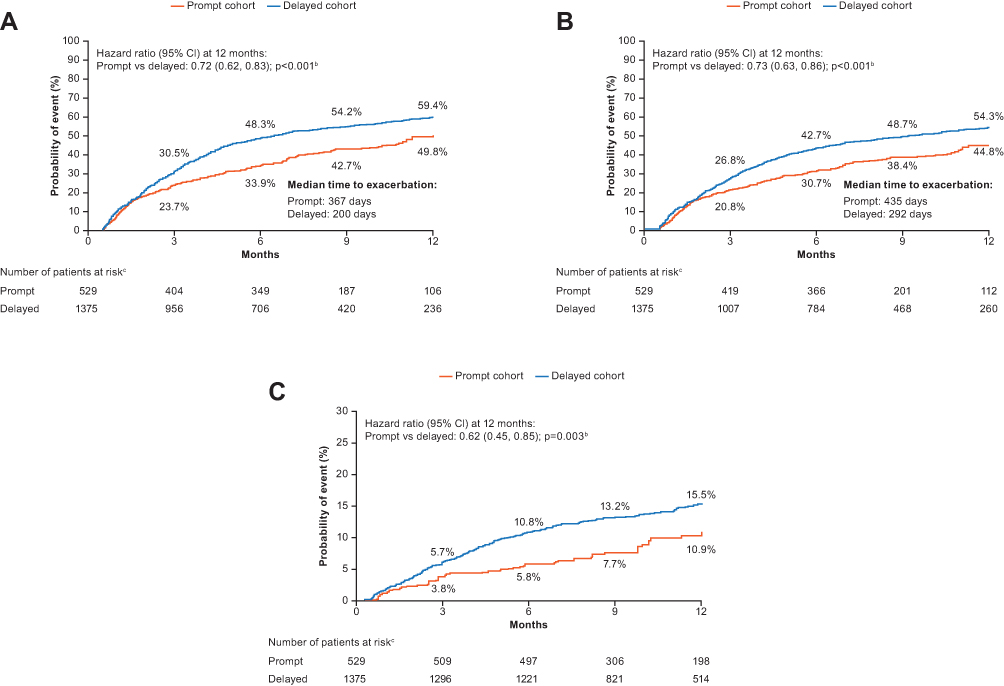 |
Figure 3 Time-to-first COPD exacerbation for (A) overall exacerbations, (B) moderate exacerbations, and (C) severe exacerbations (weighted analysis)a. Abbreviations: CI, confidence interval; COPD, chronic obstructive pulmonary disease; HMO, health maintenance organization; HRU, healthcare resource utilization; PPO, preferred provider organization; POS, point-of-service; Quan-CCI, Quan-Charlson comorbidity index. Notes: a Prompt and delayed patients were weighted using the inverse probability of treatment weighting approach based on the propensity score. Variables used in the propensity score calculation included the following: age, sex, year/quarter of index date, US region, type of insurance plan (ie, PPO, HMO, POS, and other types), Quan-CCI score (categories of 0, 1, 2, and 3+), asthma diagnosis, type of COPD-related exacerbation on the index date, patients with multiple events in the index exacerbation, respiratory medication use, all-cause and COPD-related HRU and medical costs, and comorbidities (those with ≥5% prevalence in either cohort). b Hazard ratios, including CIs and p-values, were calculated using Cox proportional hazards models. c The number of patients still observed at each timepoint. |
All-Cause and COPD-Related Medical Costs
Patients in the prompt cohort incurred significantly lower all-cause healthcare costs PPY compared with patients in the delayed cohort ($26,107 vs $32,400; cost difference: −$6293, p=0.014; Table 3). This was attributable to lower medical costs in the prompt cohort ($18,870 vs $24,360; cost difference: −$5489, p=0.026), which were largely driven by lower hospitalization costs ($6201 vs $9346; cost difference: −$3145, p=0.032).
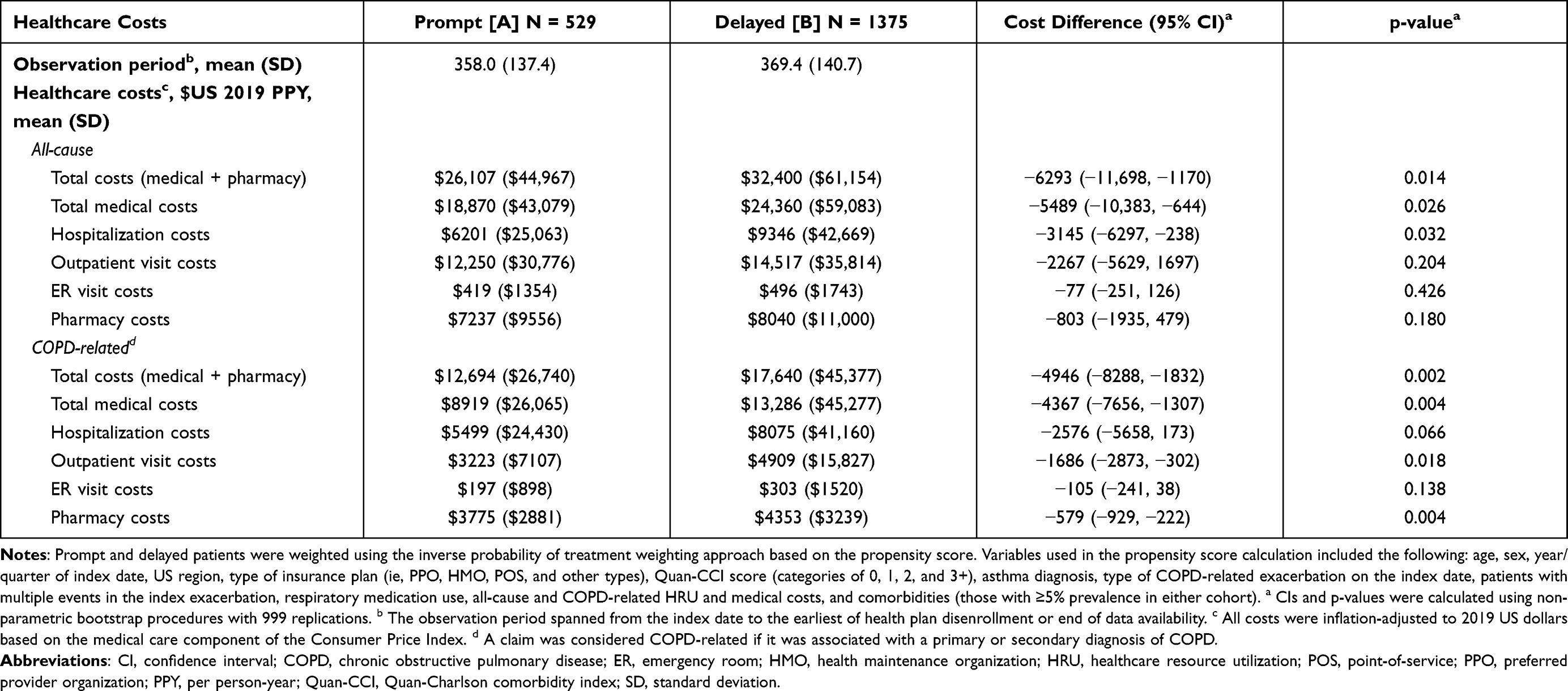 |
Table 3 Healthcare Costs Among Weighted Prompt and Delayed Cohorts |
Similar trends were observed for COPD-related healthcare costs, whereby prompt initiators incurred significantly lower total COPD-related costs PPY than delayed initiators ($12,694 vs $17,640; cost difference: −$4946, p=0.002; Table 3), driven by significantly lower medical costs ($8919 vs $13,286 PPY; cost difference: −$4367, p=0.004) and numerically lower hospitalization costs ($5499 vs $8075; cost difference: −$2576, p=0.066). COPD-related pharmacy costs were also significantly lower PPY in the prompt cohort versus the delayed cohort ($3775 vs $4353; cost difference: −$579, p=0.004).
Time-to-First Hospital Readmission
A total of 18.8% of patients in the prompt cohort and 17.4% in the delayed cohort experienced a severe exacerbation at index. Kaplan–Meier rates of all-cause and COPD-related readmissions were numerically lower in the prompt compared with the delayed cohort but did not reach statistical significance (Figure 4). At 90 days of follow-up, all-cause and COPD-related readmissions were trending lower in the prompt cohort compared with the delayed cohort (all-cause: 9.6% vs 12.5%; HR [95% CI]: 0.74 [0.36, 1.54], p=0.425; COPD-related: 8.6% vs 11.8%; RR [95% CI]: 0.70 [0.33, 1.51], p=0.365).
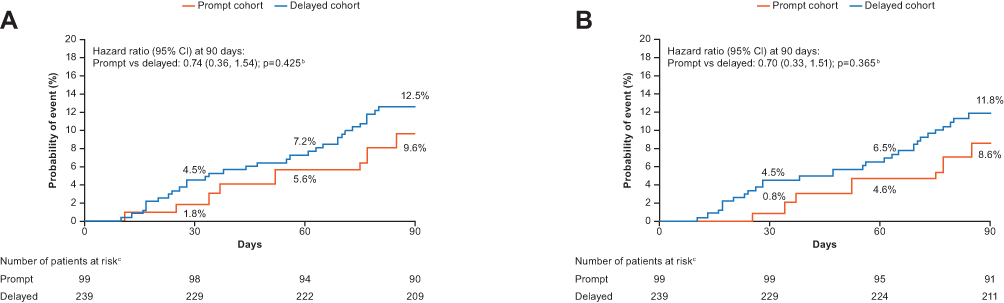 |
Figure 4 Time-to-first (A) all-cause and (B) COPD-related hospital readmission (weighted analysis)a. Abbreviations: CI, confidence interval; COPD, chronic obstructive pulmonary disease; HMO, health maintenance organization; HRU, healthcare resource utilization; PPO, preferred provider organization; POS, point-of-service; Quan-CCI, Quan-Charlson comorbidity index. Notes: a Prompt and delayed patients were weighted using the inverse probability of treatment weighting approach based on the propensity score. Variables used in the propensity score calculation included the following: age, sex, year/quarter of index date, US region, type of insurance plan (ie, PPO, HMO, POS, and other types), Quan-CCI score (categories of 0, 1, 2, and 3+), asthma diagnosis, type of COPD-related exacerbation on the index date, patients with multiple events in the index exacerbation, respiratory medication use, all-cause and COPD-related HRU and medical costs, and comorbidities (those with ≥5% prevalence in either cohort). b Hazard ratios, including CIs and p-values, were calculated using Cox proportional hazards models. c The number of patients still observed at each timepoint. |
Discussion
This study evaluated the rates of subsequent COPD exacerbations, time-to-first COPD exacerbation, healthcare costs, and hospital readmissions among patients with prompt compared with delayed initiation of single-inhaler FF/UMEC/VI following a COPD exacerbation. We observed that patients in the prompt cohort had significantly lower rates of overall, moderate, and severe COPD exacerbations in the follow-up period, and reduced Kaplan–Meier rates of exacerbation, compared with the delayed cohort. Patients in the prompt cohort also incurred significantly lower all-cause and COPD-related healthcare costs relative to those in the delayed cohort, primarily driven by lower hospitalization costs. Additionally, trends of lower hospital readmission rates during follow-up were observed in the prompt cohort.
In this study, 30 days was used as the cut-off between prompt and delayed initiation of triple therapy. This is in line with the Hospital Readmissions Reduction Program, which imposes penalties for hospitals with high 30-day readmission for specific conditions, including COPD. This initiative highlights the significance of the first 30 days post-exacerbation.23 Previous studies examining timing of therapy initiation following an exacerbation have also used this cut-off point.20,24
Previous reports have suggested that initiation of maintenance therapy earlier in the disease pathway reduces the risk of recurring COPD exacerbations.25,26 Recurrent exacerbations are associated with a greater and faster decline in lung function (measured by a decrease in forced expiratory volume in 1 second).27 Therefore, earlier intervention, particularly for patients with frequent exacerbations, is key to reducing the morbidity of the disease. Adequate control of COPD exacerbations is also critical for managing the substantial HRU and cost burden to COPD patients.28,29 The advantages of prompt compared with delayed initiation of MITT, following a COPD exacerbation or ER visit, have previously been reported.20 It was found that patients in the prompt cohort had 28% lower rates of overall exacerbations and significantly lower all-cause and COPD-related healthcare costs per patient per year (COPD-related: $8790 vs $13,100; cost difference: −$4330) compared with the delayed cohort.20
The results from our study are also consistent with another study of MITT initiation in a Spanish COPD population.24 In this study, patients in the prompt cohort had significantly lower rates of overall exacerbations and a longer time-to-first exacerbation during follow-up, compared with the delayed cohort. Patients in the prompt cohort also had lower COPD-related direct costs. While the study by Mainar et al reported that the lower COPD-related costs were offset by higher pharmacy costs, the present study observed significantly lower pharmacy costs among prompt versus delayed initiators. Taken together, our findings suggest that prompt initiation of single-inhaler FF/UMEC/VI following a COPD exacerbation leads to a reduction in future exacerbations, along with all-cause and COPD-related costs, which is in line with similar studies evaluating the timing of MITT initiation.
Previous studies have demonstrated that single inhaler use can lead to improved COPD treatment adherence and persistence compared with multiple inhalers, due to their ease of use and simplified treatment regimen.16,30 Indeed, it has recently been reported that COPD patients initiated on single-inhaler FF/UMEC/VI have improved adherence and persistence compared with those initiated on MITT.17 Although treatment adherence and persistence were not evaluated in the current study, these factors may have contributed to the lower rates of exacerbation and COPD-related healthcare costs observed in the prompt cohort, especially for patients in the delayed cohort who may have received several different medications prior to the initiation of FF/UMEC/VI; for example, 13.0% of these patients received MITT prior to initiating FF/UMEC/VI. The clinical and economic benefits of prompt initiation of SITT, combined with the observed improvements in adherence and persistence, indicate that future research on the proper timing of treatment in COPD may be warranted.
There are a few limitations to consider when interpreting the findings of this study. First, it should be noted that <1% of the total population of patients with a COPD exacerbation initiated FF/UMEC/VI within 6 months of the index exacerbation and met all selection criteria. Also, the study design may have resulted in a possible selection bias among the patients with delayed FF/UMEC/VI initiation. It is likely that the therapy of patients in the delayed cohort was escalated due to further exacerbations or uncontrolled symptoms; however, patients without further exacerbation or uncontrolled symptoms, who did not receive an escalation of therapy, would not have been included in the study. Further to this, this study primarily included commercially insured patients and therefore the results may have limited generalizability to the wider US population. In addition, missing data and coding inaccuracies are limitations that are common to all database studies. Furthermore, a dispensed medication does not confirm that a patient took the medication on that date, meaning that a patient’s true FF/UMEC/VI initiation date may have been after the dispensing day, potentially leading to cohort misclassification. Finally, while IPTW was used to account for observed differences between prompt and delayed cohorts, the possibility of unmeasured confounding by factors that were not captured in the claims database (eg, forced expiratory volume or smoking status) cannot be excluded.
Conclusions
Prompt initiation of triple therapy with FF/UMEC/VI following a moderate or severe COPD exacerbation resulted in a significant reduction in overall, moderate, and severe exacerbations, and lower all-cause and COPD-related healthcare costs, compared with patients with delayed FF/UMEC/VI initiation.
Abbreviations
BUD, budesonide; CI, confidence interval; COPD, chronic obstructive pulmonary disease; ER, emergency room; FDA, Food and Drug Administration; FF, fluticasone furoate; FOR, formoterol fumarate; GLY, glycopyrrolate; GOLD, Global Initiative for Chronic Obstructive Lung Disease; HMO, health maintenance organization; HR, hazard ratio; HRU, healthcare resource utilization; ICS, inhaled corticosteroid; IPTW, inverse probability of treatment weighting; IQR, interquartile range; LABA, long-acting β2-agonist; LAMA, long-acting muscarinic antagonist; MITT, multiple-inhaler triple therapy; PDE-4, phosphodiesterase-4; POS, point-of-service; PPO, preferred provider organization; PPY, per person-year; Quan-CCI, Quan-Charlson comorbidity index; RR, rate ratio; SABA, short-acting β2-agonist; SAMA, short-acting muscarinic antagonist; SD, standard deviation; SITT, single-inhaler triple therapy; Std. diff., standardized difference; TT, triple therapy; UMEC, umeclidinium; VI, vilanterol.
Data Sharing Statement
The data reported in this publication are contained in a database owned by IQVIA and contain proprietary elements. Therefore, it cannot be broadly disclosed or made publicly available at this time. The disclosure of this data to third-party clients assumes certain data security and privacy protocols are in place and that the third-party client has executed IQVIA’s standard license agreement, which includes restrictive covenants governing the use of the data.
Ethics Approval and Informed Consent
As this was an analysis of claims data, institutional review board (IRB) approval was not required. Per Title 45 of CFR, Part 46 (www.hhs.gov/ohrp/humansubjects/guidance/45cfr46.html#46.101), the administrative claims data analysis of our study was exempt from the IRB review as it was a retrospective analysis of existing data (hence no patient intervention or interaction), and no patient-identifiable information was included in the claims dataset.
Acknowledgments
Editorial support (in the form of writing assistance, including preparation of the draft manuscript under the direction and guidance of the authors, collating and incorporating authors’ comments for each draft, assembling tables and figures, grammatical editing, and referencing) was provided by Fiona Goodwin and Rebecca Cunningham of Aura, a division of Spirit Medical Communications Group Limited and was funded by GlaxoSmithKline. These data were previously presented in abstract/poster form at the American Thoracic Society 117th International Conference, 2021 (Michael Bogart, Guillaume Germain, Shirley Huang, Afisi Ismaila, Young Jung, François Laliberté, Sean MacKnight, Mei Sheng Duh. Benefit of prompt versus delayed initiation of single inhaler triple therapy on exacerbations and readmissions among patients with chronic obstructive pulmonary disease in the US. American Thoracic Society - 117th International Conference. 2021;203:A2252).
Author Contributions
All authors made a significant contribution to the work reported, whether that was in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the manuscript; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by GlaxoSmithKline (study number 209575 [HO-19-19552]). The sponsor was involved in study conception and design, data interpretation, and the decision to submit the article for publication. The sponsor was also given the opportunity to review the manuscript for medical and scientific accuracy as well as intellectual property considerations.
Disclosure
DM is a previous employee of GlaxoSmithKline and holds stocks/shares in GlaxoSmithKline, and reports personal fees from UptoDate, Inc., outside the submitted work. MB, SPH, ASI, and MAS are GlaxoSmithKline employees and hold stocks/shares in GlaxoSmithKline. ASI is also an unpaid part-time member of the McMaster University faculty. GG, FL, SDM, and MSD are employees of Analysis Group, a consulting company that has received research funds from GlaxoSmithKline. YJ was an employee of Analysis Group, a consulting company that has received research funds from GlaxoSmithKline, at the time of the study. The authors report no other conflicts of interest in this work.
References
1. López‐Campos JL, Tan W, Soriano JB. Global burden of COPD. Respirology. 2016;21(1):14–23. doi:10.1111/resp.12660
2. Blasi F, Cesana G, Conti S, et al. The clinical and economic impact of exacerbations of chronic obstructive pulmonary disease: a cohort of hospitalized patients. PLoS One. 2014;9(6):e101228. doi:10.1371/journal.pone.0101228
3. Dalal AA, Shah M, D’Souza AO, Rane P. Costs of COPD exacerbations in the emergency department and inpatient setting. Respir Med. 2011;105(3):454–460. doi:10.1016/j.rmed.2010.09.003
4. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease - 2021 report; 2020. Available from: https://goldcopd.org/wp-content/uploads/2020/11/GOLD-REPORT-2021-v1.1-25Nov20_WMV.pdf.
5. Dhamane AD, Moretz C, Zhou Y, et al. COPD exacerbation frequency and its association with health care resource utilization and costs. Int J Chron Obstruct Pulmon Dis. 2015;10:2609–2618. doi:10.2147/COPD.S90148
6. Cavailles A, Melloni B, Motola S, et al. Identification of patient profiles with high risk of hospital re-admissions for Acute COPD Exacerbations (AECOPD) in France using a machine learning model. Int J Chron Obstruct Pulmon Dis. 2020;15:949–962. doi:10.2147/COPD.S236787
7. Han MLK Patient education: chronic obstructive pulmonary disease (COPD) treatments (beyond the basics); 2019. Available from: https://www.uptodate.com/contents/chronic-obstructive-pulmonary-disease-copd-treatments-beyond-the-basics.
8. Rabe KF, Watz H. Chronic obstructive pulmonary disease. Lancet. 2017;389(10082):1931–1940. doi:10.1016/S0140-6736(17)31222-9
9. US Food and Drug Administration. Highlights of prescribing information - TRELEGY ELLIPTA; 2020. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/209482s010s011lbl.pdf.
10. Lipson DA, Barnhart F, Brealey N, et al. Once-daily single-inhaler triple versus dual therapy in patients with COPD. N Engl J Med. 2018;378(18):1671–1680. doi:10.1056/NEJMoa1713901
11. US Food and Drug Administration. Highlights of prescribing information - BREZTRI AEROSPHERE; 2020. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/212122s000lbl.pdf.
12. Chrystyn H, Small M, Milligan G, Higgins V, Gil EG, Estruch J. Impact of patients’ satisfaction with their inhalers on treatment compliance and health status in COPD. Respir Med. 2014;108(2):358–365. doi:10.1016/j.rmed.2013.09.021
13. Ismaila A, Corriveau D, Vaillancourt J, et al. Impact of adherence to treatment with tiotropium and fluticasone propionate/salmeterol in chronic obstructive pulmonary diseases patients. Curr Med Res Opin. 2014;30(7):1427–1436. doi:10.1185/03007995.2014.908828
14. Toy EL, Beaulieu NU, McHale JM, et al. Treatment of COPD: relationships between daily dosing frequency, adherence, resource use, and costs. Respir Med. 2011;105(3):435–441. doi:10.1016/j.rmed.2010.09.006
15. Vestbo J, Anderson JA, Calverley PMA, et al. Adherence to inhaled therapy, mortality and hospital admission in COPD. Thorax. 2009;64(11):939–943. doi:10.1136/thx.2009.113662
16. Bogart M, Stanford RH, Laliberté F, Germain G, Wu JW, Duh MS. Medication adherence and persistence in chronic obstructive pulmonary disease patients receiving triple therapy in a USA commercially insured population. Int J Chron Obstruct Pulmon Dis. 2019;14:343–352. doi:10.2147/COPD.S184653
17. Bogart M, Wu B, Germain G, et al. Real-world adherence to single-inhaler vs multiple-inhaler triple therapy among patients with COPD in a commercially insured US population. Chest. 2020;158(4):A1773–A1774. doi:10.1016/j.chest.2020.08.1548
18. Bosnic-Anticevich S, Chrystyn H, Costello RW, et al. The use of multiple respiratory inhalers requiring different inhalation techniques has an adverse effect on COPD outcomes. Int J Chron Obstruct Pulmon Dis. 2017;12:59–71. doi:10.2147/COPD.S117196
19. National Committee for Quality Assurance. Medicare Special Needs Plans performance results. HEDIS 2016; 2017. Available from: https://www.cms.gov/Medicare/Health-Plans/SpecialNeedsPlans/Downloads/2016-HEDIS-Report.pdf.
20. Bogart M, Glassberg MB, Reinsch T, Stanford RH. Impact of prompt versus delayed initiation of triple therapy post COPD exacerbation in a US-managed care setting. Respir Med. 2018;145:138–144. doi:10.1016/j.rmed.2018.10.013
21. US Bureau of Labor Statistics: Consumer Price Index - Medical Care; 2019. Available from: https://www.bls.gov/cpi/factsheets/medical-care.htm.
22. Austin PC. Goodness‐of‐fit diagnostics for the propensity score model when estimating treatment effects using covariate adjustment with the propensity score. Pharmacoepidemiol Drug Saf. 2008;17(12):1202–1217. doi:10.1002/pds.1673
23. Myers LC, Faridi MK, Hasegawa K, Hanania NA, Camargo CA. The Hospital Readmissions Reduction Program and readmissions for chronic obstructive pulmonary disease, 2006–2015. Ann Am Thorac Soc. 2020;17(4):450–456. doi:10.1513/AnnalsATS.201909-672OC
24. Mainar AS, Huerta A, Artieda RN, Monsó E, Landis SH, Ismaila AS. Economic impact of delaying initiation with multiple-inhaler maintenance triple therapy in Spanish patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2019;14:2121–2129. doi:10.2147/COPD.S211854
25. Hanania NA. Optimizing maintenance therapy for chronic obstructive pulmonary disease: strategies for improving patient-centered outcomes. Clin Ther. 2007;29(10):2121–2133. doi:10.1016/j.clinthera.2007.10.006
26. Mirza S, Clay RD, Koslow MA, Scanlon PD. COPD guidelines: a review of the 2018 GOLD report. Mayo Clin Proc. 2018;93(10):1488–1502. doi:10.1016/j.mayocp.2018.05.026
27. Donaldson GC, Seemungal TA, Bhowmik A, Wedzicha JA. Relationship between exacerbation frequency and lung function decline in chronic obstructive pulmonary disease. Thorax. 2002;57:847–852. doi:10.1136/thorax.57.10.847
28. Iheanacho I, Zhang S, King D, Rizzo M, Ismaila AS. Economic burden of chronic obstructive pulmonary disease (COPD): a systematic literature review. Int J Chron Obstruct Pulmon Dis. 2020;15:439–460. doi:10.2147/COPD.S234942
29. Jinjuvadia C, Jinjuvadia R, Mandapakala C, Durairajan N, Liangpunsakul S, Soubani AO. Trends in outcomes, financial burden, and mortality for acute exacerbation of chronic obstructive pulmonary disease (COPD) in the United States from 2002 to 2010. COPD. 2017;14(1):72–79. doi:10.1080/15412555.2016.1199669
30. Yu AP, Guérin A, Ponce de Leon D, et al. Therapy persistence and adherence in patients with chronic obstructive pulmonary disease: multiple versus single long-acting maintenance inhalers. J Med Econ. 2011;14(4):486–496. doi:10.3111/13696998.2011.594123
31. Quan H, Sundararajan V, Halfon P, et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med Care. 2005;43(11):1130–1139. doi:10.1097/01.mlr.0000182534.19832.83
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.