")
Back to Journals » International Journal of Women's Health » Volume 15
Beliefs and Utilization of Cervical Cancer Screening by Female Health Care Workers in Saudi Arabia Using the Health Belief Model: A Nationwide Study
Authors AlShamlan NA , AlOmar RS , AlAbdulKader AM , AlGhamdi FA , Aldakheel AA , Al Shehri SA , Felemban LA, Shafey MM , Al Shammari MA
Received 6 April 2023
Accepted for publication 29 July 2023
Published 7 August 2023 Volume 2023:15 Pages 1245—1259
DOI https://doi.org/10.2147/IJWH.S415924
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Nouf A AlShamlan,1 Reem S AlOmar,1 Assim M AlAbdulKader,1 Faisal A AlGhamdi,2 Abdullah A Aldakheel,2 Saud A Al Shehri,2 Lyana Atif Felemban,3 Marwa Mahmoud Shafey,1 Malak A Al Shammari1
1Department of Family and Community Medicine, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 2College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 3College of Medicine, Fakeeh College of Medical Sciences, Jeddah, Saudi Arabia
Correspondence: Nouf A AlShamlan, Department of Family and Community Medicine, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia, Tel +966 504901406, Email [email protected]
Purpose: Epidemiologically, cervical cancer is the fourth most commonly diagnosed cancer among females globally and the third most commonly diagnosed gynecological cancer in Saudi Arabia. Screening is an important measure to prevent it. The current study aimed to assess, epidemiologically, female healthcare workers’ (HCWs) utilization of cervical cancer screening services and its association with their beliefs about cervical cancer and the screening test, as well as their personal characteristics.
Methods: This cross-sectional study included female HCWs in Saudi Arabia. A predesigned, self-administered survey was used to collect data, and it included questions about sociodemographic and reproductive characteristics, self-utilization of cervical cancer screening services, and the Health Belief Model (HBM) scale. Regression analyses were conducted to identify predictors of cervical cancer screening service utilization.
Results: A total of 1857 females participated. The cervical cancer screening test uptake was 24.6% of ever-married females. However, 45% of the participants were willing to have the test. The odds of utilizing a screening were significantly higher among older participants, those with a higher level of education, and those with a higher number of pregnancies. Furthermore, HCWs with a history of HPV infection, cervical cancer in the family, hormonal contraception, or immunocompromised diseases were more likely to have the screening. An increase in the mean scores of the perceived benefits and motives subscales of HBM was associated with an increase in the uptake of screening. However, an increase in perceived barrier scores was significantly associated with a lower likelihood of cervical cancer screening uptake.
Conclusion: Low cervical screening uptake and slightly higher intentions to have the test exist among HCWs. Certain personal factors and health beliefs significantly affect the utilization of the screening test. Approaches that target perceived benefits, health motivation, and perceived barriers to improve the screening rates of cervical cancer among HCWs are recommended.
Keywords: cervical cancer screening, health belief model, Pap smear, healthcare worker, utilizations, Saudi Arabia
Introduction
Cervical cancer is the fourth most common female cancer and the fourth leading cause of female cancer deaths worldwide. According to the Global Cancer Statistics 2020 report, 604,000 new cases of cervical cancer and 342,000 deaths were expected globally in 2020.1 In the Gulf Cooperation Council (GCC) states, cervical cancer is the ninth most common malignancy among females.2 It is the third most common gynecological malignancy in females in Saudi Arabia, with an incidence rate of 1.9 cases per 100,000 female-years. Unfortunately, more than 40% of cases are diagnosed at a later stage, probably due to poor adherence to screening programs.3
The human papillomavirus (HPV) is a major contributor to the development of cervical cancer. However, other risk factors are also reported, such as smoking, sexual relations at a younger age, multiple sexual partners, a higher number of parities, HIV infection, and prolonged use of hormonal contraceptives.1,4 Cervical cancer can be a preventable cancer due to the availability of the HPV vaccine (primary prevention) and screening (secondary prevention).1 Several recommendations are issued by various guidelines to assist healthcare workers (HCWs) in screening for cervical cancer, e.g., the US Preventive Services Task Force recommends cervical cytology alone every 3 years for females aged 21–29 years. For females aged 30–65 years, different options can be offered; cervical cytology alone every 3 years, the high-risk human papillomavirus (hrHPV) test alone every 5 years, or a combination of cervical cytology and hrHPV tests (cotesting) every 5 years.5 In Saudi Arabia, cervical cancer screening has been an opportunistic service to date, provided free of charge in governmental health sectors, and is available also in the private sector. Every institution has its own unique patient communication strategies, policies, and procedures regarding cervical cancer screening.6
Reports from the GCC states revealed that the utilization of Pap smear tests among females aged 25–49 years was 28.0% in the United Arab Emirates, 17.7% in Kuwait, 10.6% in Oman, and 7.6% in Saudi Arabia.7 Personal decisions to uptake the screening programs can be influenced by many internal and external factors. The Health Belief Model (HBM) focuses on an individual’s health-associated behaviors to predict their future decisions. The following factors, according to this model, can influence the decision to participate in any disease detection or prevention program: perceived susceptibility to the disease, perceived severity of the disease on their health, perceived benefits of using the screening, and perceived barriers to the screening tests.4 Certain barriers that could affect the decision to uptake the cervical cancer screening services have been reported, such as knowledge, access to the services, a feeling of embarrassment or pain during the gynecological examination, fear of the results, and unawareness about the available services.8–10
HCWs can play a significant role in the perspective of their patients regarding cancer and its preventive measures. Moreover, HCWs were expected to be more knowledgeable and aware about cervical cancer and its screening than the general population.11 Usually, they are the first point of contact for their patients and even their relatives for health-related advice, regardless of their specialty. Their influence is evident by the significant decrease in the likelihood of testing among females who did not receive a recommendation from a HCW.12 Furthermore, females usually feel more comfortable discussing their health conditions, especially those related to gynecological issues, with their female physicians.13 Therefore, assessing the beliefs of female HCWs about cancer and screening in addition to their own self-utilization of the services that they can transmit to their relatives or patients is crucial. There have been no published studies using the HBM with regards to cervical cancer in female HCWs in Saudi Arabia, and there is limited data on self-utilization of cervical cancer screening programs. Hence, this study aimed to assess, epidemiologically, the personal utilization of cervical cancer screening by female HCWs in Saudi Arabia and its association with their beliefs towards cervical cancer and screening using the HBM, as well as their sociodemographic and reproductive characteristics.
Materials and Methods
Study Design and Participants
This nationwide cross-sectional study targeted all female HCWs in Saudi Arabia via self-administered questionnaires.
Sample Size Calculation
The minimum required sample size was calculated to be 825 through Epi Info 7.0. This assumed that 26.2% of female HCWs had cervical cancer screening according to the Heena et al study in Riyadh, Saudi Arabia, with a precision of 3.0%, and an alpha level of 0.05.14
Data Collection Process, Tool, and Study Variables
Using the non- probability sampling technique, an online survey was sent to female HCWs between July and October 2022 through their social media accounts and were encouraged to send the link to their connections in Saudi health institutions to include more participants. Moreover, leaders in the main hospitals and primary health care centers were also approached similarly. The questionnaire was developed by the researchers after a review of recent literature with similar objectives to the current study.4,11,14,15 The survey included questions on sociodemographic, occupational, and reproductive characteristics, the utilization of cervical cancer screening, and HBM components for cervical cancer and the Pap smear test (Tables 1–3).
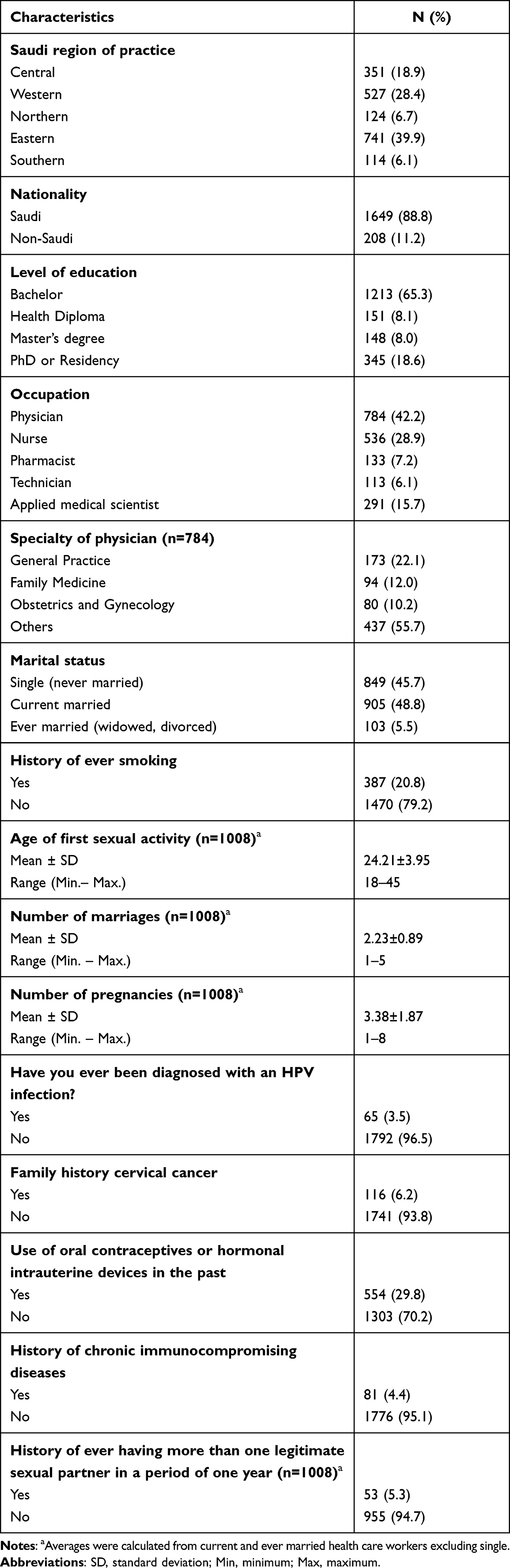 |
Table 1 Distribution of Female Health Care Workers According to Their Sociodemographic and Reproductive Characteristics, Saudi Arabia (N=1857) |
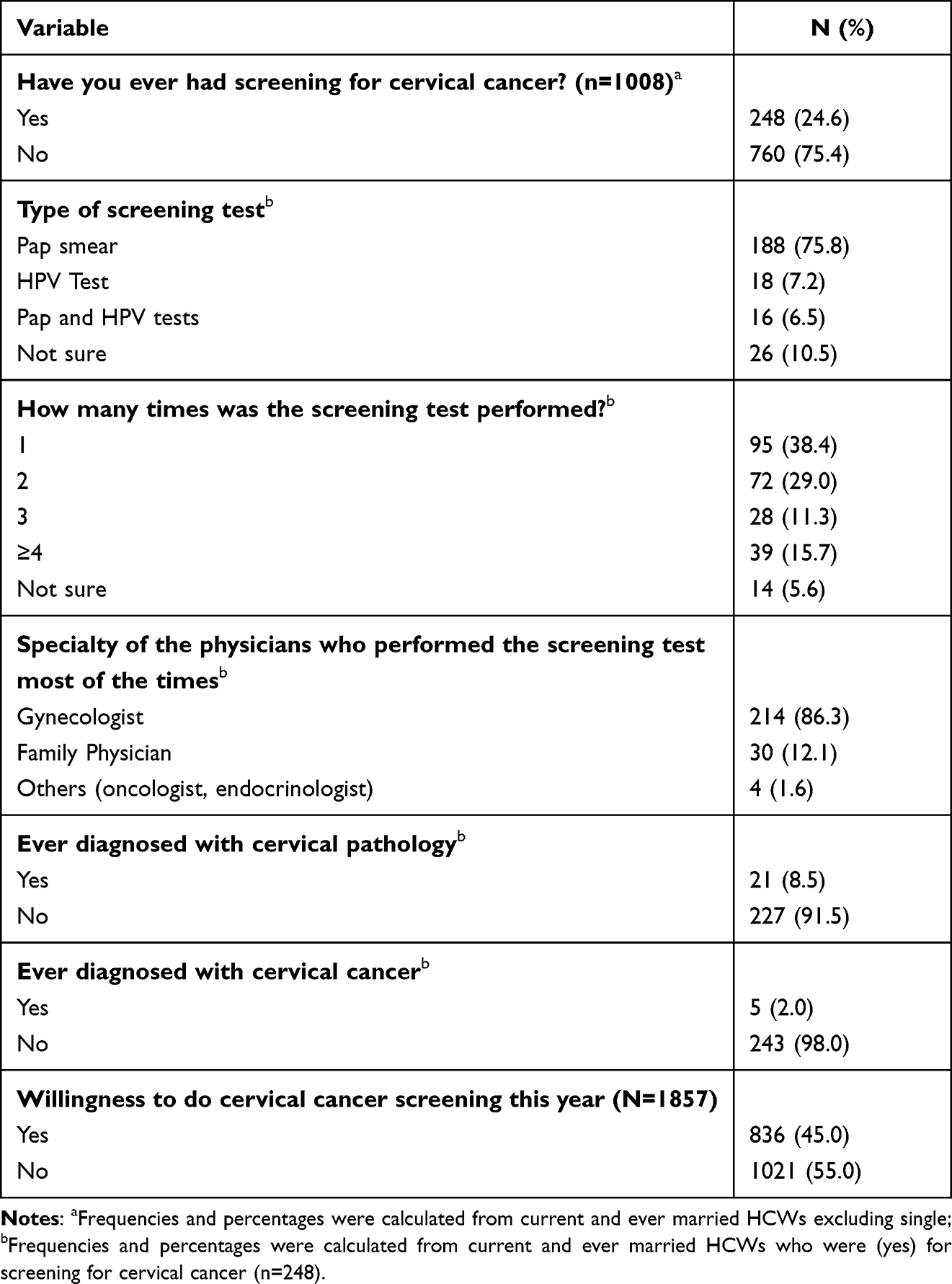 |
Table 2 Utilization of Cervical Cancer Screening by Female Health Care Workers, Saudi Arabia |
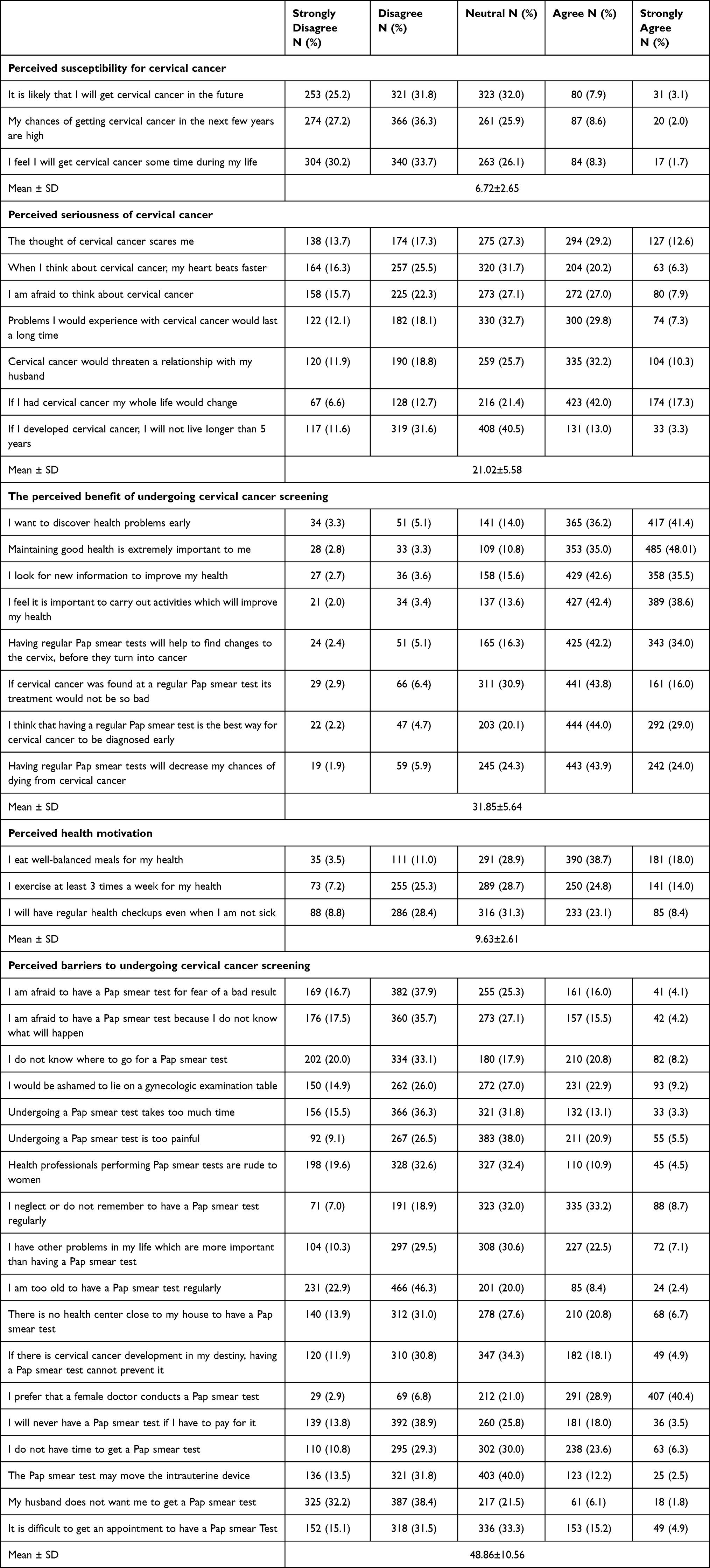 |
Table 3 Descriptive Distribution of the Components of Health Belief Model Among Females’ Health Care Workers, Saudi Arabia (Single Participants Excluded, n=1008) |
The HBM has been utilized among females from different cultures.4,15–21 The format of HBM items used in the current study was based on Victoria Champion’s CHBM scale that already was adapted, validated and applied by Aldohaian et al’s study among a sample of Saudi patients.4 Permission to use it in the current study was obtained from Victoria Champion.22–24
The HBM items are under five main subscales: perceived susceptibility to having cervical cancer; perceived seriousness of having cervical cancer; perceived benefits of undergoing a cervical cancer screening; perceived motivation towards enhancing their health; and perceived barriers to undergoing cervical cancer screening (Table 3). Each item of the subscales has a five-point Likert-scale response option ranging from strongly agree (5 points) to strongly disagree (1 point). A mean score was calculated for each of the subscales. A higher score reveals stronger feelings with regards to the related construct.4 In the current study, Cronbach’s alpha coefficients for the five subscales were observed to fall between 0.72 and 0.88.
The survey was in English, and three experts revised the tool to check the clarity and appropriateness of questions in the Saudi culture.
Data Processing and Analysis
The collected data was coded and analyzed using the Statistical Package for the Social Sciences (SPSS). For descriptive statistics, frequencies and percentages were used for categorical variables, and means with standard deviations for continuous variables. For the HBM, raw scores for each subscale were calculated with the mean and standard deviation; perceived susceptibility (3–15); perceived seriousness of having cervical cancer (7–35); perceived benefits of undergoing a cervical cancer screening (8–40); perceived motivation towards enhancing their health (3–15); and perceived barriers to undergoing a cervical cancer screening (18–90). A test of normality was performed, and accordingly, Chi-squared and t-tests were used to assess associations, followed by linear logistic regression analyses. An unadjusted linear regression model was performed with each independent variable and the uptake of screening for cervical cancer among HCWs, followed by 5 individual adjusted linear regression analyses of HBM subscales with the uptake of screening among HCWs. A P-value < 0.05 was set as the level of significance.
Ethical Approval
The institutional review board (IRB) committee at Imam Abdurrahman Bin Faisal University approved the study with IRB number IRB-2022-01-178. Anonymity and confidentiality of the data were assured. Participation in the study was voluntary. Consent to participate was obtained from all participants. The study complied with the principles of the Declaration of Helsinki.
Results
Characteristics of the Participants
The current study included 1857 female HCWs with a mean age of 32.07 (SD±8.45) and an age range of 24–65 years. Table 1 shows that about half of the participants were currently married, and 20.8% had ever smoked. Physicians constituted 42.2% of the sample, and 44.3% of them were family physicians, general practitioners, or gynecologists. Those are specialists who usually perform cervical cancer screening within their scope of service. Among non-single participants (ever and currently married), the mean age of first sexual activity was 24.21 (SD±3.95) years, the mean number of marriages was 2.23 (SD±0.89), and the mean number of pregnancies was 3.38 (SD±1.87). Only 3.5% of the respondents had been previously diagnosed with HPV infection, 6.2% had a positive family history of cervical cancer, and 29.8% had ever used oral contraceptive pills (OCPs) or hormonal intrauterine devices (IUDs). A small percentage (4.4%) had a previous history of immunocompromising diseases, and only 5.3% had more than one legitimate sexual partner in less than a year.
Utilization of Cervical Cancer Screening by the Participants
Table 2 shows that one quarter (24.6%) of ever-married and currently married HCWs have had screening for cervical cancer; mostly a Pap smear (75.8%), while only HPV testing was mentioned by 7.2%. Most participants reported performing only one test (38.4%). The majority of participants had the screening test with gynecologists (86.3%). Among those who performed cervical screening, 8.5% were diagnosed with cervical pathology and 2.0% with cervical cancer. HCWs who were willing to have cervical cancer screening accounted for 45.0% of the total respondents.
Health Belief Model Regarding Cervical Cancer Screening
Table 3 displays the distribution of different components of the HBM, where the mean scores for perceived susceptibility, seriousness, benefits, motives, and barriers were 6.72 (SD±2.65); 21.02 (SD±5.58); 31.85 (SD±5.64); 9.63 (SD±2.61) and 48.86 (SD±10.56). Most HCWs disagreed or strongly disagreed with statements regarding their personal chance to develop cervical cancer (perceived susceptibility). Less than half of participants were afraid of cervical cancer and its impact on their marital relationship, and 59.3% agreed that their lives would change after a cervical cancer diagnosis (perceived seriousness). Furthermore, the majority of respondents agreed with all statements measuring the perceived benefits of cervical cancer screening, such as more than three-quarters of females wanting to discover health problems early and agreeing that “having regular Pap smear tests will help to find changes to the cervix, before they turn into cancer.” Most participants were motivated to promote their health (perceived health motivation).
Regarding barriers to obtaining a Pap smear test, the highest percentage of HCWs agreed or strongly agreed that they prefer a female doctor to conduct a Pap smear test (69.3%), 41.9% neglect or do not remember to have a Pap smear test regularly, and nearly one third (32.1%) would be ashamed to lie on a gynecologic examination table. Having no time to get a Pap smear test has been reported by 29.9%, and having other problems in life that are more important than having a Pap smear test has been reported by 29.6%, and 29.0% of HCWs agreed that they do not know where to go for a Pap smear test. About 27.5% agreed that there was no nearby health center where they could get a Pap smear test. Reporting that undergoing a Pap smear test is too painful was agreed upon by 26.4% of HCWs. Around one fifth of HCWs agreed that they will never have a Pap smear test if they have to pay for it, that it is difficult to get an appointment to have a Pap smear test, and that they are afraid to have a Pap smear test for fear of a bad result. On the other hand, lower percentages of HCWs agreed that their husbands do not want them to get a Pap smear test (7.9%), they are too old to have a Pap smear (10.8%), health professionals performing Pap smear tests are rude to women (15.4%), and undergoing a Pap smear test takes too much time (16.4%).
Factors Associated with the Utilization of Cervical Cancer Screening
Uptake of cervical cancer screening was significantly higher among older HCWs (P-value < 0.001), those who are working in the central and eastern provinces of Saudi Arabia (P-value = 0.006), and those holding a Masters’ degree or higher (P-value < 0.001). Having cervical cancer screening was reported more by physicians (32.4%) and applied medical scientists (25.4%) than other HCWs. Obstetricians (56.5%), followed by family physicians (33.3%), had a higher uptake of cervical cancer screening (P-value < 0.001). Pregnancy rates were higher among HCWs who had cervical cancer screening (P-value < 0.001). Utilizing screening was more common among those who had previously been diagnosed with HPV infection (P-value = 0.002), those with a family history of cervical cancer (P-value = 0.001), those who used oral contraceptives or hormonal intrauterine devices in the past (P-value < 0.001), and those with a history of immunocompromising diseases (P-value < 0.001). A significantly higher mean score for perceived benefits and motivations was encountered among HCWs who had cervical cancer screening. Those who had never had cervical cancer screening, on the other hand, had a higher mean perceived barrier score (P-value < 0.001) (Table 4).
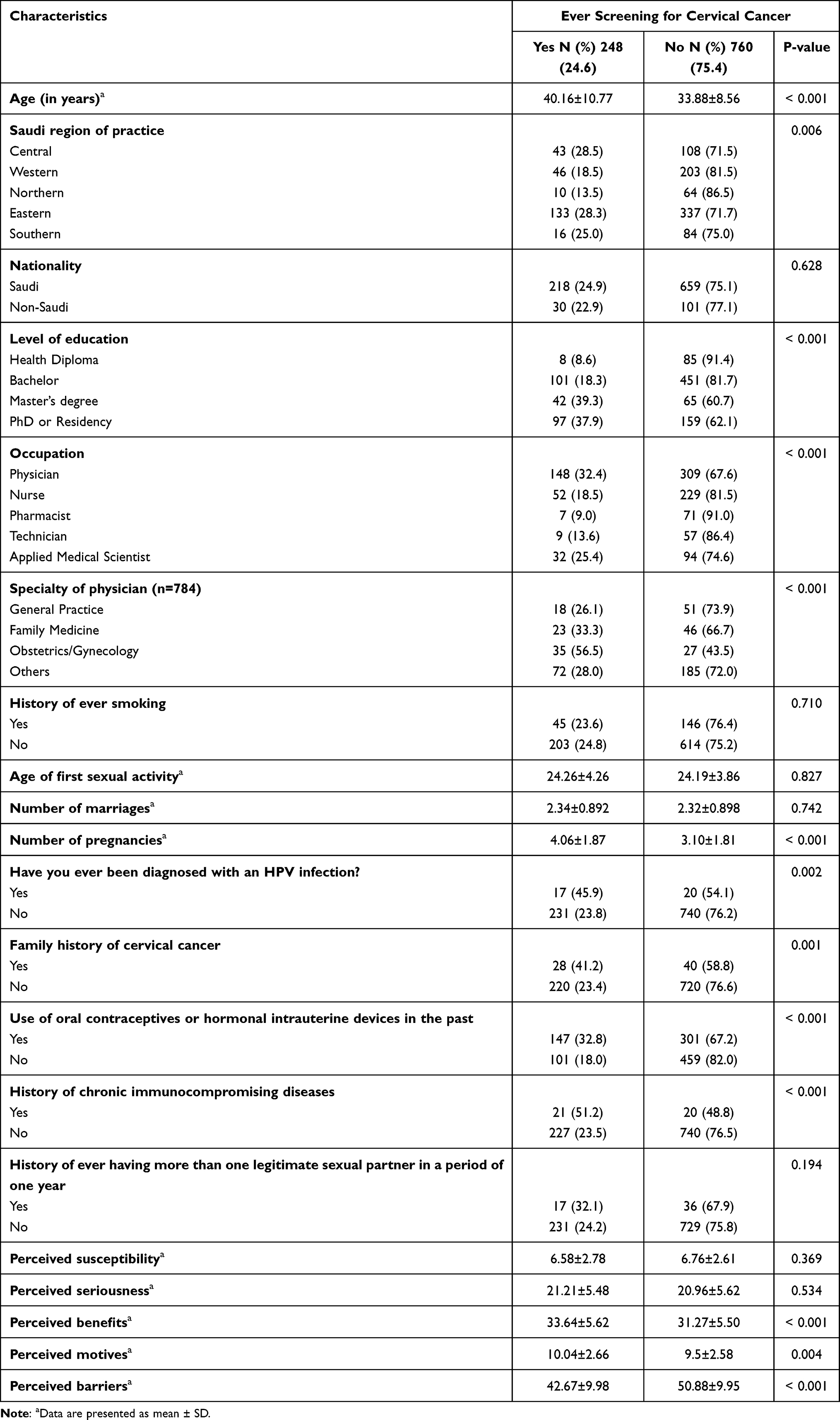 |
Table 4 Demographic and Reproductive Characteristics as Well as Health Belief Model According to the Uptake of Cervical Cancer Screening by Female Health Care Workers, Saudi Arabia (Single Participants Excluded, n=1008) |
Table 5 shows the logistic regression analyses of different variables (non-adjusted) with the uptake of screening among female HCWs. The odds of utilizing cervical cancer screening were significantly higher among older HCWs, those who had a master’s degree or higher, and those with a higher number of pregnancies than their counterparts. Furthermore, HCWs with a history of HPV infection were more likely to undergo cervical cancer screening (unadjusted OR = 6.159, 95% CI = 3.721–10.195). Uptake of cervical cancer screening was significantly higher among HCWs who had a family history of cervical cancer (unadjusted OR = 2.291, 95% CI = 1.381–3.800), those with a history of hormonal contraception (unadjusted OR = 2.219, 95% CI = 1.65–2.972), and HCWs who had a history of immunocompromised diseases (unadjusted OR = 3.423, 95% CI = 1.823–6.428). Nurses, pharmacists, and technicians, on the other hand, were significantly less likely than physicians to utilize cervical cancer screening (P-value < 0.05). Furthermore, HCWs working in the western and northern regions were significantly less likely than those working in the central region to utilize the screening (P-value < 0.05).
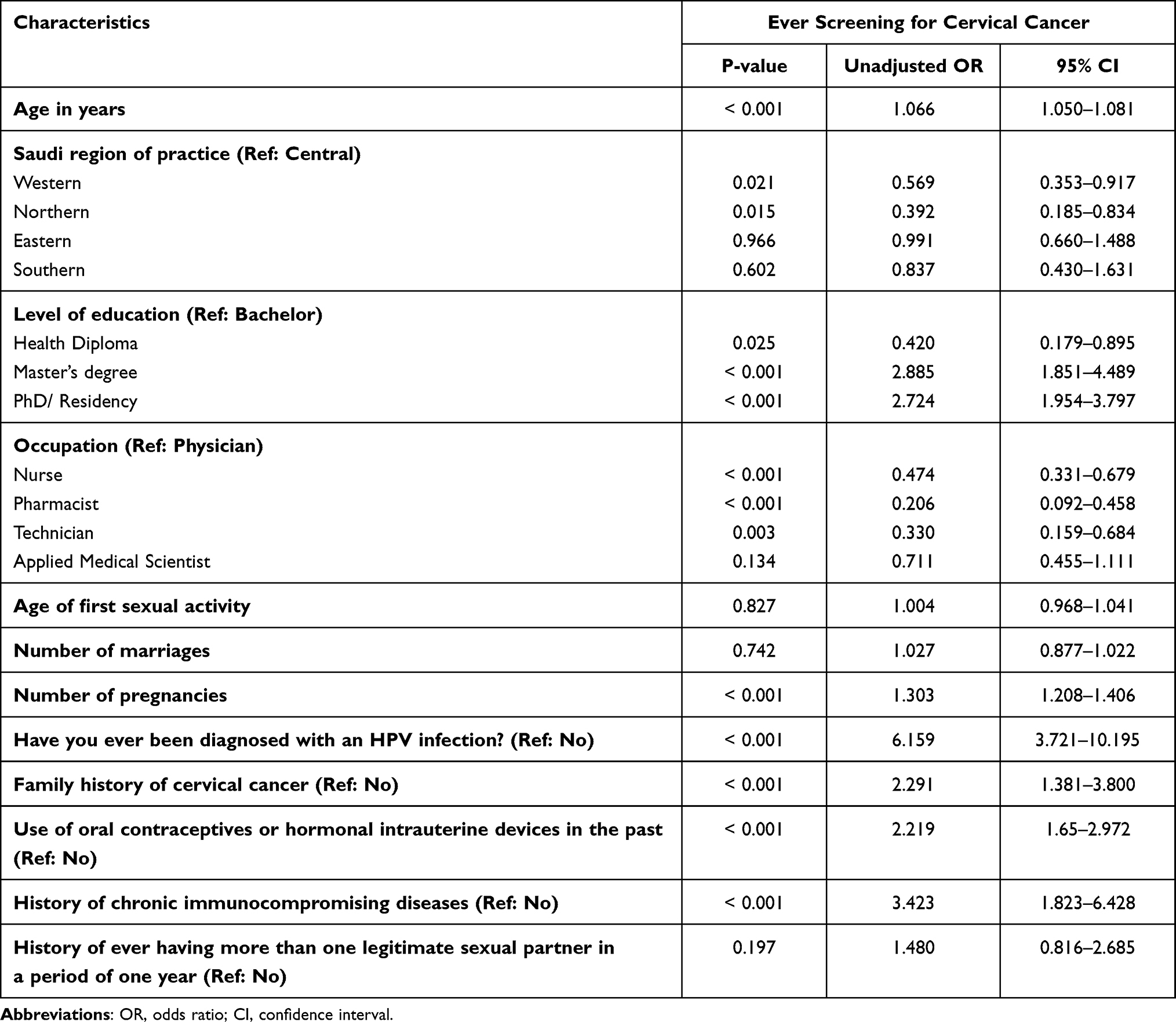 |
Table 5 Logistic Regression Analyses of Female Health Care Workers’ Characteristics (Non-Adjusted) with the Utilization of Cervical Cancer Screening, Saudi Arabia (Single Participants Excluded, n=1008) |
Table 6 demonstrates the regression analyses of HBM with the uptake of screening among female HCWs. After adjustment with the different variables listed in Table 5, an increase in mean scores of perceived benefits and motives was associated with an increase in the uptake of screening (adjusted OR = 1.074, 95% CI = 1.039–1.111, and adjusted OR = 1.078, 95% CI = 1.014–1.146, respectively). On the other hand, an increase in perceived barrier scores was significantly associated with a decreased likelihood of uptake of cervical cancer screening (adjusted OR = 0.921, 95% CI = 0.905–0.938).
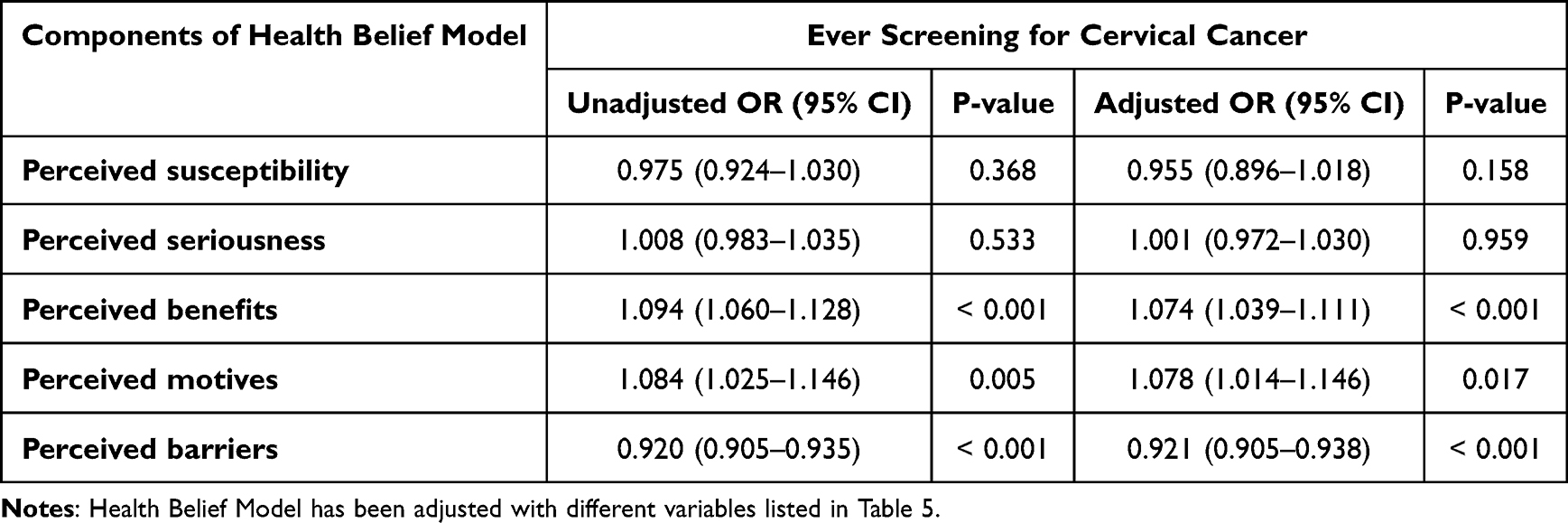 |
Table 6 Logistic Regression Analyses of Health Belief Model with the Uptake of Screening Among Female Health Care Workers, Saudi Arabia |
Discussion
The current study is assessed the utilization of cervical cancer screening by female HCWs in Saudi Arabia, their sociodemographic and reproductive characteristics, as well as their health beliefs regarding cervical cancer and its screening test. Results show that 24.6% of participating HCWs underwent a cervical cancer screening test. On the other hand, nearly half (45%) of HCWs in this study were willing to have the test. The frequency of cervical cancer screening uptake by HCWs varies among countries, eg, Pakistan (17.6%), Jordan (19.1%), Saudi Arabia (26.2%), Turkey (4.2–45.2%), Qatar (42.2%), and Taiwan (70.6%).14,25–31 Differences in cultural background and demographic characteristics of participants, the risk factor profile and epidemiology of cervical cancer, the healthcare system, and methodologies could contribute to these differences.
Based on the HBM constructs as a framework, our findings suggest that the majority of our study participants considered themselves to have a low susceptibility to cervical cancer. Besides, less than half of the participants expressed fear of cervical cancer and how it may impact their marital relationship, reflecting the low level of perceived seriousness. A systematic review has reported that the higher the scores of perceived susceptibility and seriousness of illness, the higher the likelihood of screening.32 Such an association could not be confirmed in the current study; a possible explanation is the deficiency of large epidemiological studies on the prevalence of cervical cancer and its risk profile in the country, which consequently affects the HCWs understanding of the magnitude of the problem.4 This study shows high scores for perceived benefits of undergoing cervical cancer screening among Saudi HCWs. Most participants believed that maintaining good health was essential to them. They wanted to discover health problems early and agreed that “having regular Pap smear tests will help to find changes to the cervix before they turn into cancer.” Similarly, the perceived health motivation scores were high among most study participants. In line with prior work, these observations have been associated with a higher likelihood of screening.15,18,32 Hence, we recommend focusing on the benefits of screening and health motivations in interventions aiming to promote cervical cancer screening. When asked about perceived barriers to cervical cancer screening, the majority of respondents strongly expressed a preference for a female doctor. Although this can be explained by the modesty of Muslim women and Arabic culture, as documented by a study among Arab Muslim women in the USA, studies among participants from other Western countries reported a similar preference for a female physician to perform the test.33,34 Most study participants did not perceive the reasons mentioned in the scale as significant barriers (eg, being afraid of the Pap test results, not knowing what will happen during the Pap test, the Pap test will take a long time, and the Pap test may move the IUD), which can be understandably explained by the fact that our study targeted HCWs who are more knowledgeable and familiar with the Pap test compared to the general population. Furthermore, paying for the Pap test was not cited as a significant barrier for most respondents, which the free access to universal healthcare in Saudi Arabia can explain. On the other hand, not prioritizing the screening, forgetting to do the test, fear of a painful procedure, and lack of access to a nearby health center appeared as potential barriers to undergoing cervical cancer screening. Therefore, interventions to improve the uptake of cervical cancer screening should include strong emphasis from the doctor on the importance of the screening, regular patient reminders, a proper explanation of the procedure to reduce apprehension, and improved access to healthcare facilities equipped with testing for cervical cancer screening.
Findings from the current study demonstrate that certain demographic and reproductive factors were associated with the uptake of the screening test. This study finds that older participants utilized the screening test more than younger participants. A study from Ethiopia confirmed this association, in which females aged 40–49 were more likely to have undergone screening than their younger counterparts.35
The present study demonstrates that participants with a higher level of education had higher utilization rates of screening, probably due to their knowledge and awareness regarding cancer and its preventive measures.16,19 Similar justifications can explain the findings of a higher uptake among physicians, specifically gynecologists. Moreover, accessibility to the service and the scope of their practice could also be additional reasons for this finding.
This study shows that the rates of cervical cancer screening utilization vary among different regions in Saudi Arabia, and the highest uptake was reported among HCWs who work in the central region. This could be attributed to numerous factors, such as differences in the distribution of primary healthcare centers (PHCs), population density, and acceptance of the test.36 Also, the geographical differences observed between regions within the country may be attributed to the socioeconomic differences between them. According to AlOmar’s socioeconomic indices of Saudi Arabia, the central and eastern regions were the highest in terms of education and affluency.37
This study demonstrates that a higher pregnancy rate, prior usage of oral contraceptives, and other factors that were present in a minority of participants, such as a history of HPV infection, immunocompromised conditions, or a family history of cervical cancer, were associated with a higher uptake of cervical cancer screening among HCWs. This might be attributed to their associations with the risk of cervical cancer, which could have an important motivational effect on the uptake of the screening test or be specifically targeted by their physicians due to their high-risk nature.5,38
Results of regression analyses of HBM and cervical cancer screening uptake among female HCWs in the present study show that, after adjusting for demographic and reproductive health variables, an increase in mean scores of perceived benefits of screening and health motives was associated with higher odds of undergoing cervical cancer screening. On the other hand, the odds of cervical cancer screening uptake decreased with an increase in the mean scores of perceived barriers to screening. This study supports evidence from previous observations that perceived benefits, motivations, and barriers are associated with the uptake of cervical cancer screening.15–17,19 With regards to the impact of self-utilization and beliefs about preventive measures on patient care, it was found in earlier studies that HCWs’ beliefs about such a preventive measure could affect their advice to their relatives and patients, not only their utilization.39 Therefore, our study suggests considering approaches that target perceived benefits, health motivation, and perceived barriers to improve the screening rates of cervical cancer among HCWs in Saudi Arabia.
We acknowledged some limitations in this study. Its design may affect the generalizability of the findings, and the self-reported data could potentiate the risk of recall bias. Moreover, because of the sensitivity of this question in Saudi culture, we tried to partially assess the history of having multiple sexual partners by asking about the history of having more than one legitimate sexual partner in a period of one year. Additionally, since sexual relations outside of marriage in Saudi Arabia are culturally and religiously unacceptable, the cervical cancer screening is approached by those who were previously or are currently married; therefore, single participants were excluded from some questions in the survey.
Conclusion
This study confirms the low utilization rates of cervical cancer screening services, with a slightly higher willingness to have the test among the female HCWs in Saudi Arabia. Demographic and reproductive predictors of screening utilization include age, a higher level of education, higher pregnancy rates, the use of hormonal contraception, a history of HPV infection or cervical cancer in the family, or immunocompromised diseases. Moreover, health beliefs about cervical cancer and its screening test are significantly affecting HCWs uptake of the services. The study also uncovered various barriers hindering HCWs’ utilization of the screening. To improve cervical cancer screening service uptake by female HCWs, acting on the perceived benefits of screening, perceived motivation toward enhancing health, and observed barriers to undergoing cervical cancer screening is crucial.
Acknowledgments
We wish to thank Victoria Champion, PhD, RN, FAAN, for permitting the use of the Health Belief Model Scale for Cervical Cancer and cervical cancer screening in the current study. Also, we want to acknowledge the efforts of Gulten Guvenc, PhD, RN, in developing this tool.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA. 2021;71(3):209–249.
2. Alkhalawi E, Al-Madouj A, Al-Zahrani A. Cervical cancer incidence and trends among nationals of the Gulf Cooperation Council States, 1998–2012. Gulf J Oncolog. 2019;1(31):7–13.
3. Al-Mandeel HM, Sagr E, Sait K, et al. Clinical practice guidelines on the screening and treatment of precancerous lesions for cervical cancer prevention in Saudi Arabia. Ann Saudi Med. 2016;36(5):313–320. doi:10.5144/0256-4947.2016.313
4. Aldohaian AI, Alshammari SA, Arafah DM. Using the health belief model to assess beliefs and behaviors regarding cervical cancer screening among Saudi women: a cross-sectional observational study. BMC Womens Health. 2019;19(1):6. doi:10.1186/s12905-018-0701-2
5. Curry SJ, Krist AH, Owens DK, et al. Screening for cervical cancer: US preventive services task force recommendation statement. JAMA. 2018;320(7):674–686. doi:10.1001/jama.2018.10897
6. Kingdom of Saudi Arabia, Ministry of Health, Agency of the Ministry of Public Health, Primary health care assistance agency, General administration of health programs and chronic diseases. Cancer prevention program. Cervical cancer guide. Available from: https://www.moh.gov.sa/Ministry/About/Health%20Policies/018.pdf.
7. Vht S, Channon AA, Ali MM, et al. Uptake of breast and cervical cancer screening in four Gulf Cooperation Council countries. Eur J Cancer Prev. 2019;28(5):451–456. doi:10.1097/CEJ.0000000000000466
8. Ndejjo R, Mukama T, Kiguli J, Musoke D. Knowledge, facilitators and barriers to cervical cancer screening among women in Uganda: a qualitative study. BMJ open. 2017;7(6):e016282. doi:10.1136/bmjopen-2017-016282
9. Chua B, Ma V, Asjes C, Lim A, Mohseni M, Wee HL. Barriers to and facilitators of cervical cancer screening among women in Southeast Asia: a systematic review. Int J Environ Res Public Health. 2021;18(9):4586. doi:10.3390/ijerph18094586
10. Black E, Hyslop F, Richmond R. Barriers and facilitators to uptake of cervical cancer screening among women in Uganda: a systematic review. BMC Womens Health. 2019;19(1):108. doi:10.1186/s12905-019-0809-z
11. Dulla D, Daka D, Wakgari N. Knowledge about cervical cancer screening and its practice among female health care workers in southern Ethiopia: a cross-sectional study. Int J Womens Health. 2017;9:365–372.
12. Ackerson K, Gretebeck K. Factors influencing cancer screening practices of underserved women. J Am Acad Nurse Pract. 2007;19(11):591–601. doi:10.1111/j.1745-7599.2007.00268.x
13. Heena H, Durrani S, Riaz M, et al. Knowledge, attitudes, and practices related to breast cancer screening among female health care professionals: a cross sectional study. BMC Womens Health. 2019;19(1):122. doi:10.1186/s12905-019-0819-x
14. Heena H, Durrani S, AlFayyad I, et al. Knowledge, attitudes, and practices towards cervical cancer and screening amongst female healthcare professionals: a cross-sectional study. J Oncol. 2019;2019:5423130. doi:10.1155/2019/5423130
15. Sumarmi S, Hsu YY, Cheng YM, Lee SH. Factors associated with the intention to undergo Pap smear testing in the rural areas of Indonesia: a health belief model. Reprod Health. 2021;18(1):138. doi:10.1186/s12978-021-01188-7
16. Nigussie T, Admassu B, Nigussie A. Cervical cancer screening service utilization and associated factors among age-eligible women in Jimma town using health belief model, South West Ethiopia. BMC Womens Health. 2019;19(1):127. doi:10.1186/s12905-019-0826-y
17. Chisale Mabotja M, Levin J, Kawonga M. Beliefs and perceptions regarding cervical cancer and screening associated with Pap smear uptake in Johannesburg: a cross-sectional study. PLoS One. 2021;16(2):e0246574. doi:10.1371/journal.pone.0246574
18. Maharjan M, Thapa N, Panthi D, Maharjan N, Petrini MA, Jiong Y. Health beliefs and practices regarding cervical cancer screening among women in Nepal: a descriptive cross-sectional study. Nurs Health Sci. 2020;22(4):1084–1093. doi:10.1111/nhs.12775
19. Ma GX, Gao W, Fang CY, et al. Health beliefs associated with cervical cancer screening among Vietnamese Americans. J Womens Health. 2013;22(3):276–288. doi:10.1089/jwh.2012.3587
20. Demirtas B, Acikgoz I. Promoting attendance at cervical cancer screening: understanding the relationship with Turkish womens’ health beliefs. Asian Pac J Cancer Prev. 2013;14(1):333–340. doi:10.7314/APJCP.2013.14.1.333
21. Guvenc G, Akyuz A, Açikel CH. Health belief model scale for cervical cancer and Pap smear test: psychometric testing. J Adv Nurs. 2011;67(2):428–437. doi:10.1111/j.1365-2648.2010.05450.x
22. Champion VL. Revised susceptibility, benefits, and barriers scale for mammography screening. Res Nurs Health. 1999;22(4):341–348. doi:10.1002/(SICI)1098-240X(199908)22:4<341::AID-NUR8>3.0.CO;2-P
23. Champion VL. Instrument development for health belief model constructs. ANS Adv Nurs Sci. 1984;6(3):73–85. doi:10.1097/00012272-198404000-00011
24. Champion VL. Instrument refinement for breast cancer screening behaviors. Nurs Res. 1993;42(3):139–143. doi:10.1097/00006199-199305000-00003
25. Alali A, Salem M, Elmahdi H, et al. Knowledge, attitudes and practices regarding cervical cancer screening among female health care workers in primary healthcare in Qatar. Middle East J Fam Med. 2016;14:4–15. doi:10.5742/MEWFM.2016.92809
26. Obeidat BR, Amarin ZO, Alzaghal L. Awareness, practice and attitude to cervical Papanicolaou smear among female health care workers in Jordan. Eur J Cancer Care. 2012;21(3):372–376. doi:10.1111/j.1365-2354.2011.01297.x
27. Yörük S, Açıkgöz A, Türkmen H, Ergör G. Risk factors and relationship between screening periodicity and risk of cervical cancer among nurses and midwives. A cross-sectional study. Sao Paulo Med J. 2019;137(2):119–125. doi:10.1590/1516-3180.2018.0244230119
28. Soylar P, Özer A, Doğan Yüksekol Ö, Ulucan M. Knowledge, attitude, and practice regarding cancer screening tests among health workers in a university hospital in Turkey. J Cancer Educ. 2020;35(4):718–723. doi:10.1007/s13187-019-01517-2
29. Chen SL, Tsai SF, Hsieh MM, Lee LL, Tzeng YL. Factors predicting nurse intent and status regarding Pap smear examination in Taiwan: a cross-sectional survey. Asian Pac J Cancer Prev. 2016;17(1):165–170.
30. Majid E, Shaikh MA, Qazi OA, Khan S, Majeed I, Bano K. Awareness, screening, practices and attitudes of cervical cancer among doctors and nursing staff working at a tertiary care centre. J Pak Med Assoc. 2022;72(6):1025–1030. doi:10.47391/JPMA.1443
31. Coskun S, Can H, Turan S. Knowledge about cervical cancer risk factors and Pap smear testing behavior among female primary health care workers: a study from south Turkey. Asian Pac J Cancer Prev. 2013;14(11):6389–6392. doi:10.7314/APJCP.2013.14.11.6389
32. Tanner-Smith EE, Brown TN. Evaluating the health belief model: a critical review of studies predicting mammographic and pap screening. Soc Theory Health. 2010;8(1):95–125. doi:10.1057/sth.2009.23
33. Salman KF. Health beliefs and practices related to cancer screening among Arab Muslim women in an urban community. Health Care Women Int. 2012;33(1):45–74. doi:10.1080/07399332.2011.610536
34. Nessler K, Chan SKF, Ball F, et al. Impact of family physicians on cervical cancer screening: cross-sectional questionnaire-based survey in a region of southern Poland. BMJ open. 2019;9(8):e031317. doi:10.1136/bmjopen-2019-031317
35. Woldetsadik AB, Amhare AF, Bitew ST, Pei L, Lei J, Han J. Socio-demographic characteristics and associated factors influencing cervical cancer screening among women attending in St. Paul’s teaching and referral hospital, Ethiopia. BMC Womens Health. 2020;20(1):70. doi:10.1186/s12905-020-00927-5
36. Al Saffer Q, Al-Ghaith T, Alshehri A, et al. The capacity of primary health care facilities in Saudi Arabia: infrastructure, services, drug availability, and human resources. BMC Health Serv Res. 2021;21(1):365. doi:10.1186/s12913-021-06355-x
37. AlOmar RS, Parslow RC, Law GR. Development of two socioeconomic indices for Saudi Arabia. BMC Public Health. 2018;18(1):791. doi:10.1186/s12889-018-5723-z
38. American Cancer Society. Cervical cancer. Causes, risk factors, and prevention. Available from: https://amp.cancer.org/cancer/cervical-cancer/causes-risks-prevention/risk-factors.html.
39. Karlsson LC, Lewandowsky S, Antfolk J, et al. The association between vaccination confidence, vaccination behavior, and willingness to recommend vaccines among Finnish healthcare workers. PLoS One. 2019;14(10):e0224330. doi:10.1371/journal.pone.0224330
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.