")
Back to Journals » International Journal of Women's Health » Volume 14
Behavioral Barriers to Stop Female Genital Mutilation/Cutting in South Ethiopia: An Exploratory Qualitative Study of the Perspective of Women
Authors Lejore Sibamo E , Bitew Workie S
Received 18 March 2022
Accepted for publication 3 August 2022
Published 10 August 2022 Volume 2022:14 Pages 1073—1081
DOI https://doi.org/10.2147/IJWH.S366961
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Ephrem Lejore Sibamo,1 Shimelash Bitew Workie2
1School of Public Health, College of Medicine and Health Sciences, Hawassa University, Hawassa, Ethiopia; 2School of Public Health, College of Medicine and Health Sciences, Wolaita Sodo University, Wolaita Sodo, South Ethiopia
Correspondence: Ephrem Lejore Sibamo, Email [email protected]
Background: Female genital mutilation or cutting (FGM/C) is an act that violates the rights of girls and women and causes serious medical complications. Approximately 200 million women have undergone circumcision in 31 countries. Ethiopia, in particular, has the largest number of women who undergone FGM/C. Unfortunately, there has been minimal research into the reasons for this high prevalence in the country. Hence, this study has been conducted to explore behavioral barriers to stopping FGM/C in Southern Ethiopia.
Methods: An exploratory qualitative study was employed from October to November 2021 in two purposively selected zones of Southern Ethiopia. A purposive sampling technique was used to select respondents from the two zones. A total of fourteen study participants were selected and interviewed in-depth to obtain responses from various perspectives. A thematic content analysis was conducted to analyze the data collected from the field.
Findings: The study revealed that FGM/C is widely practiced in the study area. Respondents were found to have poor awareness and positive attitude towards continuation of FGM/C. This is possibly due to the social and cultural acceptability of the practice and influences from peers, families, future marriage partners and the community. The study shows that women are more likely to be circumcised because they want to be respected by their community, to be considered eligible for marriage and to avoid stigma and discrimination.
Conclusion: The continued practice of FGM/C was in considerable state to require the development of intervention strategies in order to eliminate it by 2030. The study’s findings recommend stronger legal actions against those who perform FGM/C, alongside behavior change communication interventions, to improve awareness of its risks and encourage the community to stop FGM/C.
Keywords: female genital mutilation, female genital cutting, behavioral barriers, Southern Ethiopia
Introduction
Female genital mutilation or cutting (FGM/C) is recognized globally as a practice that violates the rights and physical integrity of girls and women.1 It constitutes an extreme form of discrimination against girls and women, which violates a girl’s rights to health, the right to be free from inhuman or degrading treatment, and the right to life when the procedure results in death.2 FGM/C is defined as a procedure that encompasses partial or total removal of the external female genitalia or other injury to the female genital organs for non-medical reasons.3 FGM/C has no health benefits.4 It is painful and traumatic procedure associated with a risk of adverse health consequences on several aspects of a girl’s or woman’s life, including her physical, mental and sexual health and her relationship with her husband or partner and other close family members.3
FGM/C is a global public health concern. According to the WHO report, more than 200 million girls and women have undergone circumcision in 30 countries in low- and middle-income countries including Africa, Middle East and Asia.2 Ethiopia is one of the high burden countries with the largest absolute number of women who have experienced FGM/C among Eastern and Southern Africa. It is estimated that 25 million girls and women have undergone FGM/C in Ethiopia.5 Similarly, evidences from the Ethiopian Demographic Health Survey6 and systematic review7 reports also confirmed that the practice is more common in Ethiopia and specifically in South region.
Drivers of FGM/C were multifaceted factors. FGM/C is a reflection of deep-rooted gender inequality and constitutes an extreme form of gendered harmful practice entrenched in social, political, economic, cultural, and religious structures of the community.2,4,8 Study findings revealed that FGM/C is associated with women’s socio-demographic aspects such as low female literacy rates; unequal status of women in the society, early marriage, place of residence, poor socio-economic status and weak political opportunity.9,10 Broadly speaking, FGM/C is strongly embedded in the sociocultural practice, which is performed as a rite of passage; for social acceptance; to promote marriageability; to prevent sexual activity; for aesthetic reasons; or under a perceived religious mandate.11 Due to this, girls and women will often fall under strong social pressure from their family, peers, and others in their social network to be circumcised.2
Regardless of who performs FGM/C, it is associated with a series of the health risks and adverse consequences to women.4,8 However, FGM/C performed by traditional practitioners holds more health risks with long-term implications compared to the one performed by health professionals.12 As nearly all FGM/C in Ethiopia is performed by traditional practitioners, it is greatly interfering girl’s or woman’s normal body functioning.5 Such increased risk and complications among traditional circumcisers are associated with the absence of antiseptic techniques or repeated use of a single instrument, nonuse of anesthetic agents, and unhygienic procedures.13,14
In general, all forms of FGM/C result in immediate and long-term complications, including physical, obstetric, gynecological, sexual and psychosocial complications that might have life-time impact on the victims.3 The women who undergone FGM/C can experience complications ranging from immediate problems like shock, bleeding and infection to long-term consequences such as chronic pain, miscarriage, stillbirth, primary infertility, and psychological suffering, like post-traumatic stress disorder.4 Moreover, the health impacts resulting from FGM/C in turn pose a great burden on health systems.15 In response to addressing these impacts, the idea of eliminating FGM/C has been recognized as the priority targets of the Sustainable Development Goals16 and the Government of Ethiopia.17
With these interventions, Ethiopia has achieved an average annual reduction rate of 1.7%.5 But this progress is far from achieving the national targets and needs to be accelerated eight times faster to eliminate the practice by 2030, and 13 times faster to eliminate the practice by 2025. Thus, for eliminating FGM/C, intervention strategies should be implemented with good understanding of behavioral and socio-cultural beliefs and perceptions related to the practice of FGM/C. Since the study area, South region, is one of the regions with the highest prevalence of FGM/C, exploring factors related with the practice is detrimental to design targeted interventions. However, there has been little evidence on the reasons associated with FGM/C in the region. Therefore, this study explores the behavioral barriers to stop female genital mutilation/cutting among reproductive age group women in south Ethiopia.
Method
To obtain an in-depth understanding on the behavioral barriers to stop FGM/C, an exploratory qualitative study, based on the assumptions of phenomenology was employed. The study was conducted between October and November 2021 in two purposively selected zones, Hadiya and Wolaita Zone of Southern Ethiopia. The region was selected because of the high burden of the practice of FGM/C.6 Similarly, the communities in Wolaita and Hadiya zone were also identified as hot spot areas with high rate of FGM/C.9,10
The study participants comprised women of reproductive age group. Women above the age of 18 years were included in the study as they are targets of the practice and willing to share their views, experiences and opinions regarding the practice of FGM/C. A purposive sampling technique was employed to select study participants from the two selected zones, aiming for maximum variation in terms of women’s age, marital status, educational level, and the experience of FGM/C. In this study, a total of 14 IDIs were conducted with women. The sample size was informed by thematic saturation of data during the interviews. A proportional number of IDIs were held in the two selected Zones.
Data were collected through face-to-face, semi-structured interviews. The interviews were guided by using interview guide, which consists open-ended questions on the behavioral barriers to stop FGM/C. The topic guide was prepared in a way that facilitates probing based on the responses of respondents and, thereby, allows to get adequate information regarding the subject matter of study. The interviews were held at comfortable sites preferred by the participants. Four female nurses who are familiar with the community norms and local languages were recruited and trained to conduct the interviews. Prior to the data collection, study participants were briefed on the objective of the study, their contribution and the expected duration of the interview. The interviews lasted on average for about 20 minutes and it was audio-taped using a digital voice recorder.
Digital audio recordings of the interviews were transcribed verbatim immediately after the interview by individuals fluent in local language and English. Transcripts were checked for accuracy and completeness by researchers. The analysis was conducted based on the principles of thematic content analysis through a three-pronged approach – noticing, collecting, and thinking. The researchers examined the transcripts carefully and independently coded into different categories by identifying common thematic areas. Then, the researchers merged the different codes generated from the transcripts and identified major thematic categories. The identified themes were compared across the transcripts to determine differences and similarities observed in the responses of the study participants on FGM/C and barriers they face to stop the practice. Accordingly, the researchers identified six thematic categories as barriers to stop FGM/C.
Results
Characteristics of Respondents
In this study, a total of fourteen women were included and interviewed to explore their perspectives regarding the practice of female genital mutilation. The mean age of study participants was 29 years, and half of them were between 21 and 34 years of age. The majority of the respondents were married and Orthodox Christians. Nearly two-thirds of the women interviewed respondents attended primary and secondary schools, and they reported that they undergone circumcision (Table 1).
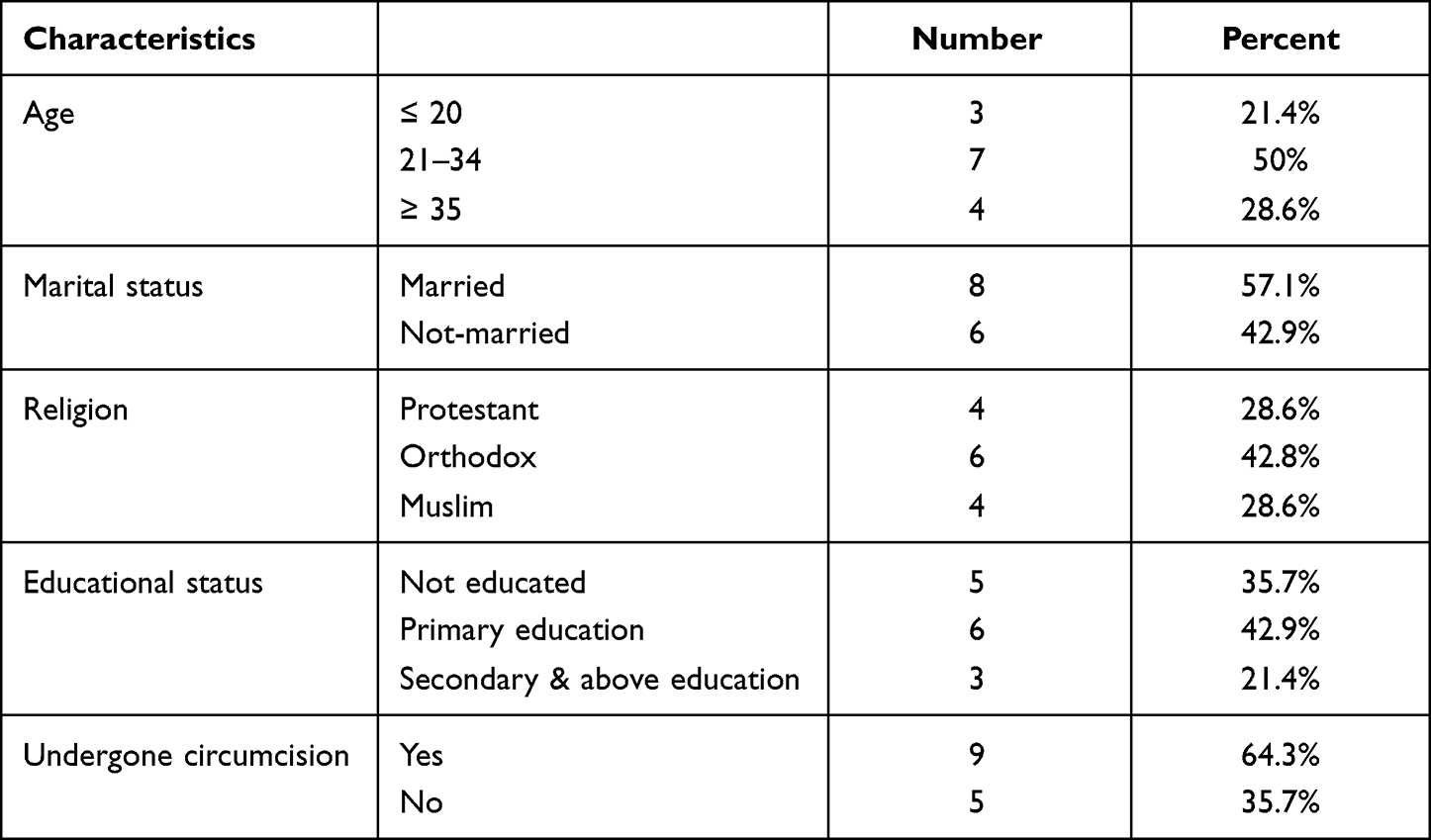 |
Table 1 Socio-Demographic Characteristics of Study Participants, South Ethiopia |
Current Situation of FGM/C Practice
The study participants revealed that the practice of FGM/C is a common practice throughout their community. The respondents who undergone FGM/C reported that they were circumcised between infancy and the age of 9 years without even telling them what is going on. It was carried out by locally known circumcisers like traditional birth attendants, elderly women in the village and some health professionals. A woman explained her experience as:
One day morning three women were showed up in our home while I was coming home back from river and my mother told me to be ready for circumcision and ordered me to wait in the hut behind the big house. I was 8 by the time. The only reason she gave me is that ‘You should be circumcised because all of your friends were circumcised.’ I can’t do any. Then, three women come to our home and told me to lay on the mattress on the floor. One woman sits on my chest and caught both of my hands down to the ground, my mom and another woman pulled my legs apart. Then … “don’ t ask me what happened to me? [she was laughing and nodding head]. (25 years old married woman)
In the same way, 21 years old women woman described the procedure as one of the tragic moments of her lifetime.
When I was circumcised, I thought I was dying. My blood was like a blood draining from a slaughtered animal. When I see my blood flows, I was in shock at the time.
Barriers to Stop FGM/C
The study participants raised a wide range of experiences and perceived behavioral barriers to stop female genital mutilation. Common themes regarding the barriers to stop FGM/C were perception about health risks of FGM/C, cultural value given to FGM/C, influences from peers, family and the society, FGM/C as a prerequisite for marriage, and weak efforts to stop FGMC practice.
Perception About Health Risks of FGM/C
The perception of women and other members of the community has a significant impact on attempts to end the practice of FGM/C. The study’s findings showed that participants’ perspectives on FGM/C practice varied widely. Participants in the study perceive the repercussions and effects of FGM/C on the rights and sexual and reproductive health of women and girls from one perspective. The respondents stated that the information received from different sources including healthcare providers, community leaders, and messages disseminated through mass media helped them to have good understanding about the health and social problems related to FGM/C. Among the health complications caused by FGM/C, respondents mentioned that the practice results in excessive bleeding, experience difficulty during labor and childbirth, and it may expose to HIV/AIDS.
Every time I heard about female genital mutilation, I become worried of going through pregnancy. Health care providers have told me that women who undergone FGM may have difficulty during labor. (28 years old women)
Similarly, another respondent reported the effect of FGM/C from tragic experience of her friend:
I see the practice of FGM as a bad practice, which causes health complication to the women and her fetus during labour. You see, … I lost my friend last year. She died during labour, while she is giving birth, but she didn’t survive the incident. Based on the information from the health care provider, the reason for her death is the scar from the circumcision began to tear and bleed. She lost too much blood and her baby died in her uterus. (23 years old female)
Contrary to the above perspective, the study participants perceived the FGM/C practice as an important traditional practice that every woman should undergo. The respondents believe that that woman should continue to practice FGM/C to earn community’s respect. Such traditionally influenced perception of the community has impacted them from realizing the risks of FGM/C. In addition to this, it was also seen as a major factor contributes for the continued practice of FGM/C. According to the explanation of a 32-year old respondent, the community perceives FGM/C as a normal procedure practiced for generations and makes the efforts of stopping FGM/C as a difficult process.
In our community, FGM is seen just as the removal of the tip of the clitoris, as having no risk to the women. The health risks related to FGM is not well understood by the community and they practiced it for a long period of time as an essential procedure. As a result of this, the community respect and continued to practice FGM for generations. So, I think it is difficult to simply stop FGM. (32 years old married woman)
Correspondingly, this assertion was also reinforced by a woman who undergone FGM/C. As she explained, the practice of FGM/C is an important practice that should be maintained and transferred to generations:
For me, circumcision is essential for women and it has its own importance. We inherited this practice from our mother’s and I believe that circumcision is a pride for women. For instance, … my mother was circumcised and no problem had happened to her. Still now, she is giving birth without any problem. In my opinion, we have to maintain the practice of circumcision and it should be transferred to next generation. (35 years old women)
In response to this, the study participants emphasized the need of strengthening awareness raising activities at the community level to improve understanding and awareness of the community about the health impacts of the FGM/C.
I understand that women who undergone circumcision will suffer a lot in their lifetime including at the time of childbirth. If the community have good knowledge about complications related to FGM, the current trend may change. Emphasis should be given to improve the awareness of the community, including women through trainings or other community-based health education activities. (39 years old women)
Cultural Value Given to FGM/C
The participants of the study stated that female circumcision is an important cultural procedure inherited from their parents and grandparents. A 35 years old married woman reiterates that
FGM is a mandatory cultural practice for every woman. As I inherited from my grandparents, I consider it as one of my cultural identities that I should have to maintain.
Respondents of the study also emphasized that the practice of FGM/C is viewed as a social obligation imposed against women and girls. They mentioned that the beliefs surrounding the practice as the one that prevents women from premarital sex were key to get approval from their friends, family, and the society in general. The community also perceives uncircumcised women as those who are out of social norms. A married woman explained:
In our culture, circumcision of female has given high value. For instance, if I let my daughter uncircumcised, the way the community sees her will be changed. Society sees as a violation of social norms. They think that we are not respecting norms of the society and nobody wants to marry her. So, I don’t want to see my daughter to be treated this way. (40 years old woman)
Moreover, a 21 years old young woman also revealed female circumcision as a source of pride for a woman.
I believe that a woman can be socially respected by undergoing circumcisions. Which inspires me and girls like me in our area, as eligible for marriage.
Influences from Peers, Family and the Society
The study participants reported that influences from the women’s social network including families, friends and elders in the community were also barriers for the continuation of FGM/C practice in the study area. The people in woman’s social network influence her to get circumcised in view of the value given to the practice. The study participants mentioned that the influence is related to the belief that circumcision is a source of pride to be respected by their peers, family, and others in the society and get married. As the 18 years old women explained:
I had circumcised due to my friends’ pressure. While I was playing with my friends during my uncles wedding ceremony, they know that I was uncircumcised and they laughed at me. At the moment, I was afraid of their act and feel ashamed. After that incident, I told to my parents that I want to be circumcised, not to be bullied by my friends.
The decision to get circumcised was not made by the woman. The participants explained that mothers were mainly involved in the decision to practice FGM/C. Despite males were involved in the discussion related to circumcision, mothers play a central role in female circumcisions.
I was kid when I get circumcised. Everything was decided by my parents. Especially my mother is the one who talked with the village women and bring her home to circumcise me. (18 years old unmarried girl)
FGM/C as a Prerequisite for Marriage
The study participants attribute the continuation of the FGM/C practice with the belief that circumcision of women is important to control women sexual desire and increase the chance of getting marriage. This means the community favors the practice as they believe that circumcision enables the woman to be protected from premarital sex and get approval from their future marriage partner. One respondent expressed what her mother believes about circumcision as:
I remember my mother told me the day I circumcised …. ‘An uncircumcised girl can’t control her sexual desire, which makes it difficult to maintain her virginity until she gets married compared to circumcised girls. And if she loses her virginity, she will lose her chance of marriage.’ So, I agree with circumcision thing. (23 years old married woman)
Weak Efforts to Stop FGM/C Practice
Although the practice of FGM/C is recognized as a criminal offence and punishable act under the Criminal Code of the Federal Democratic Republic of Ethiopia Proclamation No. 414/2004,18 the study participants revealed that the law is hardly implemented for protecting girls against the continued practice of FGM/C. Participants of this study reported that FGM/C practice is still prevalent in the area and negatively affecting the sexual and reproductive health of women and girls. In response to this, respondents stressed the need of taking legal actions as a means to stop FGM/C:
In my view, legal measures are the only ways to stop FGM practice in our community, because different activities were conducted in the last five years to improve awareness about the negative health effect of FGM and I heard this practice is legally prohibited by law. But communities are still performing this practice in their home and I didn’t see any legal measures taken to stop it. Therefore, in my view, legal actions should be applied on those who are willing to FGM and those who are performing according to the law. (27-year-old unmarried woman)
Whereas, another respondent argued that mere enforcement of laws may not be adequate to ensure the efforts of stopping the practice. This assertion was explained by a married woman who opposes the idea of taking only legal actions on perpetrators of FGM/C, because it might conflict with existing tradition and the laws may also be poorly understood by the community. In response to this, the respondent suggested the need of integrating legal actions with awareness raising activities as a suitable strategy to stop FGM/C:
…. FGM is a long existing traditional practice that is inherited from our grandparents and if the government ban all forms of circumcision through legal means it may leads to conflict with the community. Since the people think that the government is against their tradition and this may put all the initiatives and even the administration at risk. So, I believe that the government and other concerned bodies may better focus on improving awareness of the community by health education. (35-year-old unmarried woman)
Besides this, the lack of attention from the administrators to stop FGM/C and improve women’s, families, and community’s awareness about the risks associated with circumcision was also identified as one of the barriers to end FGM/C. As a woman explained:
I know women who undergone circumcision in their childhood suffer a lot during childbirth. I believe that concerned bodies should focus on improving the awareness of the community, including women. However, there is no opportunity for such trainings. I have never attended any trainings, workshops or other health education activities regarding FGM practice prevention and behavioral change sensitization programs. And my parents did not allow us to go such information sources including youth friendly services at the health center. (19 years old women)
Similarly, a 20 years old student mentioned that,
… As I am a member of female’s club at our school, we tried to communicate the health center regarding information on the health impacts of FGM. However, most of health staffs and other concerned bodies did not give emphasis to give us any information we wanted about FGM.
Discussion
This study has provided an insight into women’s perspectives regarding the behavioral barriers that impact the attempts to end the practice of FGM/C in South Ethiopia. Although the government of Ethiopia designed and implemented different intervention strategies for eliminating FGM/C by 2030, the study finding pinpointed that FGM/C is widely practiced in the study area. Women and girls who undergone FGM/C stated that the circumcision was done between the age of 5 and 9 years by traditional circumcisers. Such widespread practice of FGM/C was also reported by studies conducted in the study area.9,10,19 In this study, five major thematic categories of barriers to stop FGM/C were identified; perception about health risks of FGM/C, cultural value given to FGM/C, influences from peers, family and the society, FGM/C as a prerequisite for marriage, and weak efforts to stop FGMC practice.
The significant impact of the perception of women and other members of the community was identified as a major barrier to the attempts to end the practice of FGM/C. The study finding revealed that women had different perceptions towards the practice of FGM/C. Study participants perceive that the practice of FGM/C results in health and social problems due to its repercussions and effects on the rights and sexual and reproductive health of women and girls. This indicates that women do not perceive the practice of FGM/C as being beneficial to the female.20 The community’s understanding about the health consequences and impacts of FGM/C was found to be the major factor to prevent or undergo FGM/C practice.21 For this reason, the study participants emphasized the need of strengthening awareness raising activities to improve perception of the community about the health impacts of the FGM/C. Educating girls at a younger age can impact their perception and empower them to refuse FGM/C is of particular importance.22
Contrary to the above idea, some of the study participants perceive the practice of FGM/C as a traditional ritual that should be maintained and transferred to generations. The respondents believe that every woman should undergo FGM/C to earn community’s respect. The practice is viewed as a social obligation to prevent women and girls from becoming sexually promiscuous, if left uncircumcised.20 In fear of such views, women are more likely enforced to undergo circumcision.23 Somali women also continued to become circumcised in fear of stigmatization by the community.24 This is because of the fact that the community perceives FGM/C as a normal practice that does not have risk to the women and practiced for a long period of time as an essential procedure.
Similarly, the study finding outlines that the cultural and social value given to FGM/C by the community has been contributing for the continued practice of FGM/C. The participants mentioned that a woman gets approval from their friends, family, and the community, if she becomes circumcised. This is because of the belief that circumcised women were believed to be protected from premarital sex. For this reason, women were influenced to be circumcised to get acceptance from community, fear of discrimination, and become eligible for marriage.23–25 Particularly, influence of mothers greatly contributed for the continued practice of FGM/C.19,26
Many scholars argued that laws ratified globally and nationally should be cherished both as legitimate and enforceable by the public.27,28 Although the practice of FGM/C is prohibited by law and identified as a punishable act by the government of Ethiopia, the study participants revealed that the law is not actively implemented against those who perform and facilitate FGM/C. The anti-FGM/C laws of sub-Saharan countries fall short of offering adequate protection to potential victims.29 In response to this, the respondent suggested the need of integrating legal actions with awareness raising activities as a suitable strategy to stop FGM/C. Consistent with this, Shell-Duncan, Hernlund, Wander, Moreau27 suggested that legal reform must be complemented by other change initiatives that address the culturally mediated social, moral, and religious standards that may uphold the practice because law rarely changes behavior on its own. Thus, the participants stressed that taking legal actions on those who perform FGM/C along with other advocacy and other awareness raising activities has an essential role to the attempts to stop FGM/C.
Given the sensitive nature of the phenomena to be studied, the recruitment of research assistants who are familiar with the community norms and local languages has greatly helped to reduce potential barriers in interview. However, as the practice of FGM/C is driven by harmful gender, cultural, social, moral, and religious norms, such complex nature of the practice might have an impact on the participant response. This indicates that the findings of this research might be influenced by social desirability bias. To lessen the impact of this bias, participants were promised that their answers would remain anonymous.
Conclusion
Exploring the behavioral barriers to stopping FGM/C in areas with high prevalence of the practice allowed critical examination of women’s perspectives and experiences could be better heard and supported to refuse to FGM/C. Findings of the study revealed that female circumcision is widely practiced in the study area. The attempts made to stop FGM/C were shown to be influenced by women’s perception about the practice of FGM/C, cultural and social norms of the community. In addition to this, the study shows that the efforts made by government and stakeholders are challenged by the influences of peers, family and society to undergo circumcision as a prerequisite for marriage, and fear of stigma and discrimination. Moreover, weak efforts of the governing body to enforce laws enacted to stop FGMC practice were also reported as a barrier to eliminate FGM/C. It is suggested that emphasis should be given to integrate and strengthen enforcement of legal measures along with advocacy and awareness raising activities to the attempts to stop FGM/C.
Ethical Approval
Ethical clearance was obtained from the Institutional Review Board of the College of Medicine and Health Sciences, Hawassa University. The board also approved the verbal informed consent process. The participants were informed about the purpose, benefit, risk, confidentiality of the information, and the voluntary nature of participation. The study was conducted in accordance with the Declaration of Helsinki.
Consent
Data were collected only after full informed verbal consent was obtained, and confidentiality of the information was maintained throughout by excluding names as identification and keeping their privacy during the interview and reporting of the findings.
Acknowledgments
We would like to acknowledge South Regional health bureau and respective zones for providing support to the study. The authors are grateful to the respondents who offered their time to participate in this study.
Author Contributions
Both authors made a significant contribution to the work reported, including conception, study design, data collection, transcription and translation, data analysis and interpretation, drafting and critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest in relation to this work.
References
1. Khosla R, Banerjee J, Chou D, Say L, Fried ST. Gender equality and human rights approaches to female genital mutilation: a review of international human rights norms and standards. Reprod Health. 2017;14(1):1–9. doi:10.1186/s12978-017-0322-5
2. World Health Organization. Female genital mutilation: fact sheet; 2022. Available from: https://www.who.int/news-room/fact-sheets/detail/female-genital-mutilation.
3. World Health Organization. Care of Girls and Women Living with Female Genital Mutilation: A Clinical Handbook. Geneva: World Health Organization; 2018.
4. Williams-Breault BD. Eradicating female genital mutilation/cutting: human rights-based approaches of legislation, education, and community empowerment. Health Hum Rights. 2018;20(2):223.
5. UNICEF. A Profile of Female Genital Mutilation in Ethiopia. New York: United Nations Children’s Fund; 2020.
6. CSA, ICF. Ethiopia Demographic and Health Survey 2016. Addis Ababa, Ethiopia, and Rockville, Maryland, USA: Central Statistical Agency (CSA) [Ethiopia] and ICF; 2016.
7. Fite RO, Hanfore LK, Lake EA, Obsa MS. Prevalence of female genital mutilation among women in Ethiopia: a systematic review and meta-analysis. Heliyon. 2020;6(7):e04403. doi:10.1016/j.heliyon.2020.e04403
8. World Health Organization. Eliminating female genital mutilation: an interagency statement-OHCHR, UNAIDS, UNDP, UNECA, UNESCO, UNFPA, UNHCR, UNICEF, UNIFEM, WHO. World Health Organization; 2008. Available from: https://apps.who.int/iris/bitstream/handle/10665/43839/?sequence=3.
9. Setegn T, Lakew Y, Deribe K. Geographic variation and factors associated with female genital mutilation among reproductive age women in Ethiopia: a national population based survey. PLoS One. 2016;11(1):e0145329. doi:10.1371/journal.pone.0145329
10. Geremew TT, Azage M, Mengesha EW. Hotspots of female genital mutilation/cutting and associated factors among girls in Ethiopia: a spatial and multilevel analysis. BMC Public Health. 2021;21(1):1–18. doi:10.1186/s12889-021-10235-8
11. World Health Organization. Guidelines on the management of health complications from female genital mutilation: policy brief. Geneva: World Health Organization; 2016. Available from: https://www.who.int/reproductivehealth/topics/fgm/management-health-complications-fgm/en/.
12. Odukogbe A-TA, Afolabi BB, Bello OO, Adeyanju AS. Female genital mutilation/cutting in Africa. Transl Androl Urol. 2017;6(2):138. doi:10.21037/tau.2016.12.01
13. Wakabi W. Africa battles to make female genital mutilation history. Lancet. 2007;369(9567):1069–1070. doi:10.1016/S0140-6736(07)60508-X
14. Serour G. Medicalization of female genital mutilation/cutting. Afr J Urol. 2013;19(3):145–149. doi:10.1016/j.afju.2013.02.004
15. Kimani S, Muteshi-Strachan J, Njue C. Health impacts of female genital mutilation/cutting: a synthesis of the evidence; 2016.
16. UN. Transforming our world: the 2030 agenda for sustainable development; 2015.
17. Ministry of Women CaY. National costed roadmap for ending child marriage and FGM/C: 2020–2024; 2019.
18. Ethiopia FDRo. Criminal Code of the Federal Democratic Republic of Ethiopia. In. Proclamation No 414/2004. Addis Ababa: Berhanena Selam Printing Enterprise; 2005.
19. Tamire M, Molla M. Prevalence and belief in the continuation of female genital cutting among high school girls: a cross - sectional study in Hadiya zone, Southern Ethiopia. BMC Public Health. 2013;13(1):1–9. doi:10.1186/1471-2458-13-1120
20. Ahanonu E, Victor O. Mothers’ perceptions of female genital mutilation. Health Educ Res. 2014;29(4):683–689. doi:10.1093/her/cyt118
21. Gajaa M, Wakgari N, Kebede Y, Derseh L. Prevalence and associated factors of circumcision among daughters of reproductive aged women in the Hababo Guduru District, Western Ethiopia: a cross-sectional study. BMC Women Health. 2016;16(1):42. doi:10.1186/s12905-016-0322-6
22. Mohamud A, Qureshi Z, De Wildt G, Jones L. Exploring perceptions of female genital mutilation/cutting abandonment (FGM/C) in Kenyan health care professionals. Qual Health Res. 2021;31(11):1976–1989. doi:10.1177/10497323211015967
23. Gebremariam K, Assefa D, Weldegebreal F. Prevalence and associated factors of female genital cutting among young adult females in Jigjiga district, eastern Ethiopia: a cross-sectional mixed study. Int J Womens Health. 2016;8:357. doi:10.2147/IJWH.S111091
24. Abathun AD, Sundby J, Gele AA. Attitude toward female genital mutilation among Somali and Harari people, Eastern Ethiopia. Int J Womens Health. 2016;8:557. doi:10.2147/IJWH.S112226
25. Mohammed ES, Seedhom AE, Mahfouz EM. Female genital mutilation: current awareness, believes and future intention in rural Egypt. Reprod Health. 2018;15(1):175. doi:10.1186/s12978-018-0625-1
26. Bogale D, Markos D, Kaso M. Prevalence of female genital mutilation and its effect on women’s health in Bale zone, Ethiopia: a cross-sectional study. BMC Public Health. 2014;14(1):1076. doi:10.1186/1471-2458-14-1076
27. Shell-Duncan B, Hernlund Y, Wander K, Moreau A. Legislating change? Responses to criminalizing female genital cutting in Senegal. Law Soc Rev. 2013;47(4):803–835. doi:10.1111/lasr.12044
28. Adinew YM, Mekete BT. I knew how it feels but couldn’t save my daughter; testimony of an Ethiopian mother on female genital mutilation/cutting. Reprod Health. 2017;14(1):162. doi:10.1186/s12978-017-0434-y
29. Kandala N-B, Komba PN. Geographic variation of female genital mutilation and legal enforcement in sub-saharan Africa: a case study of Senegal. Am J Trop Med Hyg. 2015;92(4):838–847. doi:10.4269/ajtmh.14-0074
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.