")
Back to Journals » Infection and Drug Resistance » Volume 16
Bedaquiline, Delamanid, Linezolid, Clofazimine, and Capreomycin MIC Distributions for Drug Resistance Mycobacterium tuberculosis in Shanghai, China
Authors Guo Y, Yang J, Wang W, Wu X, Wan B, Wang H, Sha W, Yu F
Received 16 October 2023
Accepted for publication 28 November 2023
Published 11 December 2023 Volume 2023:16 Pages 7587—7595
DOI https://doi.org/10.2147/IDR.S440711
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Yinjuan Guo,1 Jinghui Yang,1 Weiping Wang,1 Xiaocui Wu,1 Baoshan Wan,1 Hongxiu Wang,1 Wei Sha,2 Fangyou Yu1
1Department of Clinical Laboratory, Shanghai Pulmonary Hospital, School of Medicine, Tongji University, Shanghai, People’s Republic of China; 2Tuberculosis Center for Diagnosis and Treatment, Shanghai Pulmonary Hospital, School of Medicine, Tongji University, Shanghai, People’s Republic of China
Correspondence: Wei Sha; Fangyou Yu, Email [email protected]; [email protected]
Background: New antituberculosis drugs have recently been approved for the treatment of multidrug-resistant tuberculosis TB (MDR-TB). We aimed to describe the distributions of bedaquiline, delamanid, linezolid, clofazimine, and capreomycin MIC values for M. tuberculosis.
Methods: M. tuberculosis clinical isolates were originally isolated from 2020 to 2021 from 1452 different pulmonary tuberculosis patients of the Shanghai Pulmonary Hospital in China. The drug susceptibility testing was performed using the Sensititre custom plates (SHTBMY) (TREK Diagnostic Systems, Thermo Fisher Scientific In., USA) consisting of a 96-well microtitre plate containing 4 (bedaquiline, delamanid, clofazimine, capreomycin) antimicrobial agents. MICs were determined for linezolid using a microdilution method.
Results: Based on the latest definitions, 156 (10.74%) were MDR-TB, 93 (6.40%) were pre-XDR-TB, and 27 (1.86%) were XDR-TB. The rate of BDQ resistance in cases of MDR-TB was 7.69%, while it was observed to be 10.75% in cases of pre-XDR-TB, and significantly higher at 37.04% in cases of XDR-TB. The lowest rate of drug resistance against M. tuberculosis was DLM (0.14%). For LZD, 11 (0.76%) clinical isolates were resistant, based on the CLSI breakpoint of 1μg/mL. The five strains with a MIC value of > 32 for LZD resistance were XDR-TB isolates. Among all MDR, pre-XDR, and XDR isolates tested, LZD’ MIC50 increased from 0.25 and 0.5 to 1μg/mL. The MIC90 value of LZD against XDR-TB isolates was 32μg/mL. For CFZ, six isolates with elevated MICs of ≥ 2μg/mL. CFZ’s MIC50 and MIC90 values in all isolates were 0.12μg/mL and 0.25μg/mL, respectively.
Conclusion: The study findings indicate that BDQ, DLM, CFZ, and LZD may exhibited excellent in vitro activity against MDR-TB isolates. Detection of resistance to BDQ and LZD was alarming for XDR-TB isolates. It is necessary to perform universal drug sensitivity testing for M. tuberculosis, especially MDR-TB and XDR-TB patients.
Keywords: Mycobacterium tuberculosis, MIC distributions, bedaquiline, delamanid, linezolid
Introduction
Between the years 2019 and 2021, there has been a notable global increase in the estimated mortality rate associated with tuberculosis (TB). According to estimates, the total number of deaths among individuals not infected with HIV amounted to approximately 1.4 million in the year 2021.1 Globally, latent tuberculosis infection has affected more than one-third of the population. Both forms of tuberculosis, namely multidrug-resistant TB (MDR-TB) and extensively drug-resistant TB (XDR-TB), which is defined as resistance to rifampicin and isoniazid, as well as resistance to rifampicin, any fluoroquinolone, and at least one of bedaquiline or linezolid, are challenging to manage and require significant financial resources. Furthermore, these forms of TB have a prolonged duration of treatment, are more prone to treatment failure, and can result in the fatality of the patient. XDR-TB, which accounts for approximately 6.0% of cases of MDR-TB, is even more lethal. According to the global tuberculosis (TB) report released by the World Health Organization (WHO) in 2022, the worldwide rate of successful treatment for diagnosed cases of MDR-TB stood at 60%. In contrast, there was an 85% success rate observed for all new and relapse cases.1 MDR-TB and XDR-TB remain significant obstacles to achieving effective global TB control. Therefore, there is an urgent requirement for novel anti-TB medications to address the issue of incipiently untreatable tuberculosis.
Bedaquiline (BDQ), an inhibitor of ATP synthase, obtained approval from the US Food and Drug Administration (FDA) and the European Medicines Agency (EMA) in the year 2012, and it was subsequently recommended by the World Health Organization (WHO) in 2013 for the treatment of MDR-TB.1,2 The present mechanisms identified for resistance towards BDQ encompass mutations occurring within the atpE, Rv0678, and pepQ genes.3 Delamanid, belonging to the nitro-dihydro-imidazooxazole class of compounds, hampers the production of essential mycolic acids.4 The medication was authorized by the EMA and endorsed by the WHO in 2014 for the treatment of patients with MDR-TB.5 Due to the distinct mechanisms of action possessed by each of the two drugs, which differ from those of other drugs currently accessible, one can anticipate a significant potential for effectiveness against extensively drug-resistant tuberculosis (XDR-TB).
Clofazimine (CFZ), an antibiotic derived from a fat-soluble riminophenazine dye, has exhibited substantial effectiveness and minimal toxicity in the treatment of drug-resistant tuberculosis.6 In accordance with the TB treatment guidelines revised by the WHO in 2016, CFZ, previously categorized as a group 5 drug, has been added to the core medications. This addition took place due to its reclassification as a group C drug within the second drug category.7 In accordance with various clinical studies, linezolid (LZD) is comparable to CFZ as it is an established and dated drug with antibacterial properties. It has demonstrated efficacy in successfully treating patients afflicted with MDR and XDR pulmonary tuberculosis.8,9
Nevertheless, the current presence of drug resistance towards BDQ, DLM, CFZ, and LZD poses a persistent and imminent danger.10–12 The resistance to BDQ may potentially arise spontaneously, even in situations where there is no presence of antimicrobial exposure.13 Therefore, it is necessary to assess susceptibility to these drugs to validate their clinical application. The minimum inhibitory concentration (MIC) value has been known for a very long time. For many years, it has been determined only occasionally but now it has been appearing increasingly frequently in the results of routine tests.14 The primary objective of this study was to examine the frequency of resistance to the four aforementioned drugs and the distribution characteristics of MIC values within a population that has not previously utilized these medications for tuberculosis treatment.
Materials and Methods
Clinical M. Tuberculosis Isolates and Culture Conditions
M. tuberculosis clinical isolates (n=1452) were originally isolated from December 2020 to June 2021 from 1452 different pulmonary tuberculosis patients of the Shanghai Pulmonary Hospital in China. Sputum and bronchoalveolar lavage fluid were digested with a 2% NaOH N-acetyl-l-cysteine and conducted utilizing conventional methodologies. Ziehl–Neelsen staining was utilized for smear microscopy on the concentrated pellet. Subsequently, a quantity of 0.5 mL of the resuspended pellet was introduced into BACTEC MGIT (Mycobacteria growth indicator tube) 960 culture (BD Biosciences, New Jersey, USA), while 0.2 mL was introduced onto Löwenstein–Jensen medium (L-J) medium at a temperature of 37°C.
Drug Susceptibility Testing
The utilization of the broth microdilution method for conducting the determination of minimal inhibitory concentration (MIC) for M. tuberculosis was established based on traditional drug susceptibility testing in accordance with the guidelines stipulated by the Clinical Laboratory Standards Institute M24-A2. MIC is the lowest concentration of an antibacterial agent expressed in mg/L (μg/mL) which, under strictly controlled in vitro conditions, completely prevents visible growth of the test strain of an organism. The MIC-related parameters geometric mean MIC (geometric mean of MIC values, GM MIC), MIC50 (MICs required to inhibit the growth of 50% of bacteria), and MIC90 (MICs required to inhibit the growth of 90% of bacteria) were evaluated. In brief, the bacterium was immersed in a sterile saline solution that included glass beads and subjected to a vortex for 30 seconds. After settling for 15 minutes, the supernatant was adjusted to McFarland 0.5 with turbidimetry, and the 1:10 diluted sample was subsequently mixed with Middlebrook 7H9 broth, and 100 µL of this mixture was employed as the inoculum. The 100 μL bacterial suspension that had been prepared was placed into each well of the MYCOTB plate. Subsequently, the plate was covered with an adhesive seal and subjected to incubation at a temperature of 37°C for a duration of 7 to 10 days. Additionally, growth controls that do not include antibiotics were incorporated, along with sterility controls that were not inoculated.
We used SENSITITRE CUSTOM PLATE (SHTBMY) (TREK Diagnostic Systems, Thermo Fisher Scientific In., USA) to perform DLM, BDQ, CFZ, and capreomycin (CPS) drug susceptibility testing as recommended by the manufacturer. The concentrations of antibiotics in the test panel ranged from 0.008 to 0.5 µg/mL for DLM, 0.06 to 8 µg/mL for BDQ, 0.06 to 4 µg/mL for CFZ, and 0.15 to 20 µg/mL for CPS, respectively. In addition, LZD (0.06 to 32 µg/mL) was used microbroth dilution method and only tests the susceptibility of MDR M. tuberculosis clinical isolates. The concentrations that defined the MIC breakpoints were as follows: 0.12 µg/mL for BDQ and DMD, 1.0 µg/mL for LZD and CFZ, and 5 µg/mL for CPS.
Quality Control
The Mtb H37Rv (ATCC 25618) was used as a reference strain. The control well exhibiting positive growth ought to be examined prior to further analysis, whereas any lack of growth would render the outcome invalid.
Statistical Analysis
The SPSS statistical software package (v20.0; SPSS) was used to perform all statistical analyses. A P-value of <0.05 was considered statistically significant.
Results
Demographic Data of M. Tuberculosis
Among 1452 patients infected M. tuberculosis, 959 (66.05%) were male and 493 (33.95%) were female. The mean age of patients was 43.7 years, ranging from 2 to 97 years. Most of the patients came from the eastern region.
Antimicrobial Susceptibility Profiles of M. Tuberculosis Isolates
Of the 1452 M. tuberculosis isolates, 1272 (87.60%) were collected from new cases, and 180 (12.40%) were collected from re-treated cases. Based on the latest definitions, 156 (10.74%) were MDR-TB, 93 (6.40%) were pre-XDR-TB, and 27 (1.86%) were XDR-TB. Table 1 shows the drug resistance profiles of all 1452 clinical isolates. Drug resistance rate of DLM was the lowest (0.14%), with only 2 isolates from new cases.
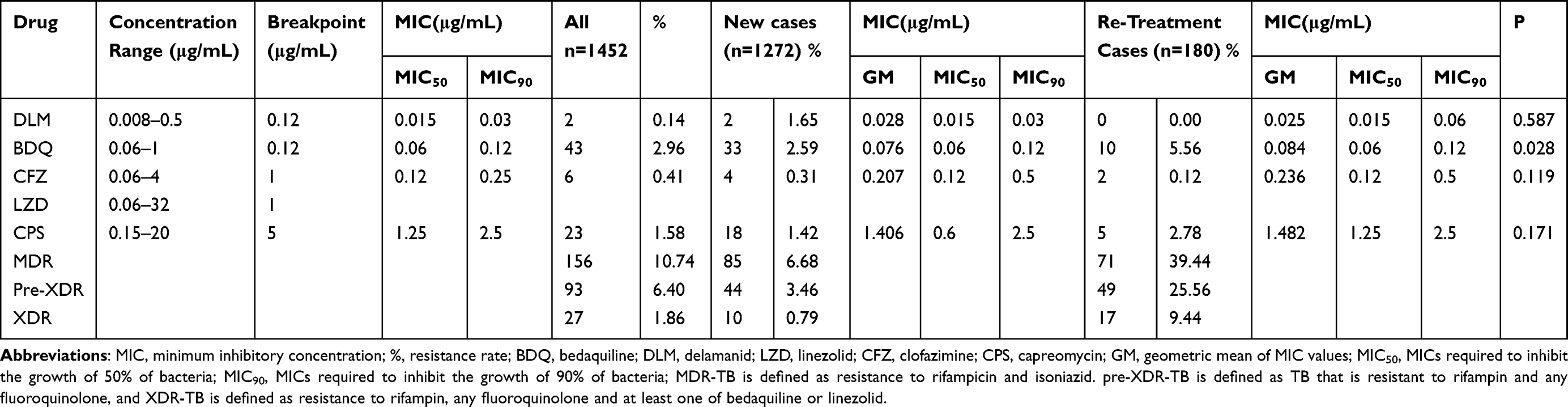 |
Table 1 Drug Resistance Profile of All Mycobacterium Tuberculosis Isolates (N=1452) |
The difference in resistance patterns between new cases (2.59%) and re-treated cases (5.56%) of BDQ was statistically significant (P<0.05). The resistance rates of re-treatment cases of CPS (2.78% V 1.42%) were approximately twice in new cases. Compared to re-treatment cases, resistance rate of DLM (1.65% V 0%) and CFZ (0.31% V 0.12%) were higher in new cases.
Drug Susceptibility Profiles of MDR- and XDR-TB Strains
The drug-resistant outcomes of MDR, Pre-XDR, and XDR groups are listed in Table 2. As shown in Table 2, among 156 MDR-TB and 27 XDR-TB isolates, the number of bacteria showing MIC > 1 μg/mL as determined by CFZ resistance was 2 isolates (1.28%) and 2 isolates (7.41%). The rate of BDQ resistance in cases of MDR-TB was 7.69%, while it was observed to be 10.75% in cases of pre-XDR-TB, and significantly higher at 37.04% in cases of XDR-TB. Notably, the BDQ resistance rate was found to be considerably higher in XDR-TB isolates compared to MDR-TB isolates (P < 0.001). Similarly, drug resistance rate of XDR-TB to LZD was as high as 25.93%.
 |
Table 2 Drug Resistance Profiles Among MDR-TB, Pre-XDR-TB, and XDR-TB Strains |
Of 27 XDR-TB strains, 2 (7.41%) were resistant to CFZ, which was also the two isolates resistant to BDQ. Moreover, only one isolate (11.11%) was resistant to both DLM and LZD. Out of a total of 27 isolates of extensively drug-resistant tuberculosis (XDR-TB), not a single isolate exhibited resistance to CPS. Nevertheless, the occurrence of concurrent resistance to BDQ and LZD was observed to be low, accounting for only 1.08% (1 out of 93) within the overall MDR-TB population and 3.70% (1 out of 27) within the pre-XDR-TB/XDR-TB subset. The quantities of drug-resistant strains to BDQ, DLM, LZD, and CFZ found in pre-XDR-TB and XDR-TB isolates were identical.
Delamanid, Bedaquiline, Clofazimine and Linezolid MIC Determination and Distribution
The MIC distributions for new and repurposed drugs are shown in Figure 1. We discovered that over 90% of isolates demonstrated a MIC of equal to or less than 0.12μg/mL for BDQ, 0.03μg/mL for DLM, 1μg/mL for LZD, 2.5μg/mL for CPS, and 0.5μg/mL for CFZ, correspondingly. Considering all 1452 M. tuberculosis, BDQ resistance was noted in 43 (2.96%) isolates. MICs for BDQ ranged from 0.06 to 0.1μg/mL, with an MIC50 of 0.06μg/mL and MIC90 of 0.12μg/mL. One isolate had BDQ MIC levels of 1μg/mL. For MDR-TB isolates, 13 (8.33%) showed BDQ’MICs 0.12μg/mL and 9 (5.77%) showed MICs 0.25μg/mL. Although the MIC50 and MIC90 of BDQ were the same for MDR, Pre-XDR, and XDR-TB isolates, GM gradually increased (0.088μg/mL, 0.092μg/mL, and 0.160μg/mL).
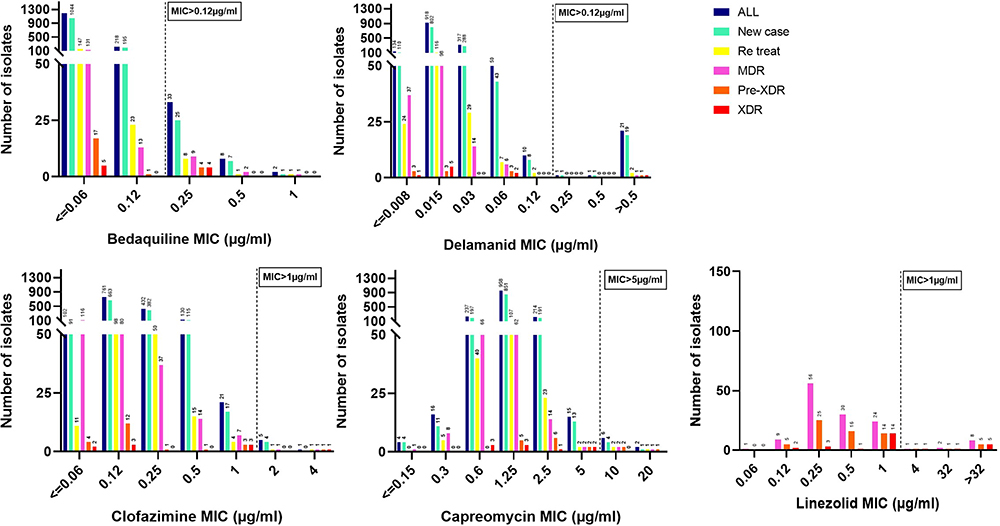 |
Figure 1 MIC distribution of M. tuberculosis isolates against bedaquiline, delamanid, linezolid, capreomycin, and clofazimine. |
The lowest rate of drug resistance against non-MDR M. tuberculosis was DLM (0.08%). MIC values of DLM ranged between 0.008 and 0.5μg/mL, with an MIC50 of 0.015μg/mL, and an MIC90 of 0.03μg/mL. DLM’MIC50 and MIC90 were the same between non-MDR-TB isolates and MDR, pre-XDR-TB isolates. DLM’MIC90 (0.06μg/mL) increased a gradient in XDR-TB isolates compared to MDR and pre-XDR-TB isolates.
For LZD, 11 (0.76%) clinical isolates were resistant, based on the CLSI breakpoint of 1μg/mL. The five strains with a MIC value of >32 for LZD resistance were XDR-TB isolates. Among all MDR, pre-XDR, and XDR isolates tested, LZD’ MIC50 increased from 0.25 and 0.5 to 1μg/mL. The MIC90 value of LZD against XDR-TB isolates was 32μg/mL. The GM value of LZD resistance to MDR, pre-XDR-TB, and XDR isolates gradually increases from 2.890% to 3.025% to 8.130%. For CFZ, six isolates with elevated MICs of ≥2μg/mL. CFZ’s MIC50 and MIC90 values in all isolates were 0.12μg/mL and 0.25μg/mL, respectively. The GM values of CFZ for MDR, pre-XDR TB, and XDR isolates also gradually increased.
Discussion
The compounds BDQ, DLM, CFZ, and LZD displayed remarkable in vitro efficacy against MDR-TB in over 90% of the tested isolates. BDQ was approved for MDR-TB treatment in 2012.15,16 Reports of resistance emerged shortly after the BDQ drug introduction.17 Nevertheless, the widespread utilization of BDQ was limited due to concerns regarding the prompt emergence of resistance. The WHO has issued a caution regarding the potential acceleration of resistance with the inappropriate utilization of BDQ. Recently, the European Committee on Antimicrobial Susceptibility Testing (EUCAST) formally approved a cutoff value of ≤0.25 μg/mL as the breakpoint for the application of BDQ. Consistent with the report Wang et al (7.16%),18 in this study, 7.69% of the MDR-TB isolates demonstrated resistance to BDQ. Conversely, He et al and Liu et al observed BDQ resistance in 1.0% and 2.2% of MDR-TB patients, respectively.19,20 The occurrence of co-resistance to both BDQ and LZD and to CFZ and LZD was also notably scarce in both the overall populations of MDR-TB and pre-XDR-TB/XDR-TB. The number of XDR-TB isolates that were resistant to BDQ and LZD overall was significant. The reason behind the inclination towards higher resistance in XDR-TB remains unexplained.
Hoffman et al documented a case wherein a patient exhibited multi-drug-resistant tuberculosis that displayed resistance to both BDQ and CFZ. Notably, this patient subsequently developed a rapid resistance to DLM.21 Findings from previous studies have revealed that the reason for cross-resistance between BDQ and CFZ was two drugs share MmpS5-MmpL5. Notwithstanding the presence of only two isolates (7.41%) displaying resistance to two drugs, prior administration of CFZ might engender a significant susceptibility of M. tuberculosis to BDQ, thus signifying the necessity for further surveillance investigations.
In the present study, 0.64% (1/156) of MDR-TB were resistant to DLM, which was much lower than the 4.5% (4/88) reported in southwest China,22 2.9% (3/102) reported in Beijing, China,19 and 8.8% (15/170) reported in Korea.13 Furthermore, it has been reported that over 25% of rifampicin-resistant tuberculosis isolates displayed resistance to DLM despite no prior exposure.23
As for CFZ, more than 90% of MDR-TB and XDR-TB isolates were susceptible in this study. The rate of resistance in the CFZ was comparatively higher in XDR isolates as compared to MDR isolates. In this study, it was found that the percentage of MDR-TB isolates exhibiting a CFZ resistance rate with MIC greater than 1 μg/mL, amounted to 1.28%. In contrast to the results we obtained, it was observed that 27.7% of the 195 MDR-TB isolates displayed resistance to CFZ, with MICs exceeding 2 μg/mL.24 Pang et al have reported the discovery of resistance to CFZ in 5 isolates, accounting for 5.6% of the XDR-TB strains. The MICs for these isolates were found to be greater than 1 μg/mL.12
A meta-analysis showed that the average resistance rate of MDR-TB to LZD in five studies from China was 5.8%.25 While resistance rate to LZD in the present study was 7.5%, which was higher than the five studies from China. According to the report, the prevalence rate of LZD resistance among the clinical isolates of MDR-TB in 14 distinct countries was found to be the highest in Spain, with a rate of 22.2%, while the United States had the lowest prevalence rate at 0.2%.25 The reason why the linezolid drug resistance rate varies so greatly may be due to the geographical diversity and the different methods used. Most studies used the method of microbroth dilution, while a study from Turkey used the method of agar dilution.
CPS plays a crucial role as an antimycobacterial drug in the management of XDR-TB. Among 56 MDR-TB isolates, 25% of isolates were resistant to CPS in Iran.26 The primary reason for this outcome was largely attributed to the continuous transmission of a highly resistant strain throughout the province, resulting in a significant number of fatalities. While 47/52 (90.4%) XDR-TB patients were CPS-resistant in South Africa.27 Likewise, a recent analysis conducted on patients diagnosed with XDR-TB in the Tugela Ferry region revealed a significantly elevated prevalence of resistance to CPS production (89.5%).28 A survey conducted in Europe has recognized CPS resistance as a distinct risk element contributing to unfavorable outcomes in patients diagnosed with MDR-TB.29 However, CPS-resistant XDR-TB isolate was not found in this study. Three isolates (1.92%) were resistant to CPS in MDR-TB patients. One of the possible reasons is that CPS, the first-line injection drug for anti-tuberculosis, was less used in China.
There were several limitations in this study. First, the isolates collected in this study were from one hospital in Shanghai. Second, the resistance mechanism was not clear. In our forthcoming research, we intend to prioritize the investigation of the susceptibility of MDR-TB isolates toward novel pharmaceuticals and thoroughly scrutinize the development of resistance to such drugs. The objective of this endeavor is to furnish clinical practitioners with a valuable resource to aid in their treatment decisions.
In conclusion, we presented the representative resistance profiles of new drugs for M. tuberculosis treatment in China. The study results demonstrate that BDQ, DLM, CFZ, and LZD displayed remarkable in vitro effectiveness against MDR-TB isolates. Detection of resistance to BDQ and LZD was alarming for XDR-TB isolates. It is necessary to perform universal drug sensitivity testing for M. tuberculosis, especially MDR-TB and XDR-TB patients.
Ethics Statement
The research plan received approval from the Ethics Committees of Shanghai Pulmonary Hospital, a subsidiary of Tongji University in Shanghai, China. The study adhered to the ethical principles set forth in the 1964 Declaration of Helsinki and its subsequent revisions. During the study, patients were granted written informed consent for the inclusion of their data. A parent or legal guardian of patients under 18 years of age provided informed consent.
Acknowledgments
We express our utmost gratitude to the Clinical Laboratory of Shanghai Pulmonary Hospital for their valuable support in the execution of this project. This project was supported by grants from the Shanghai Clinical Research Center for infectious diseases (tuberculosis) (19MC1910800 to W.S.) and Outstanding Medical Academic Leader (2019LJ13).
Disclosure
No potential conflict of interest was reported by the authors.
References
1. World Health Organization. Global Tuberculosis Report. World Health Organization; 2022.
2. Patel RV, Riyaz SD, Park SW. Bedaquiline: a new hope to treat multi-drug resistant tuberculosis. Curr Top Med Chem. 2014;14(16):1866–1874. doi:10.2174/1568026614666140929114822
3. Ismail N, Omar SV, Ismail NA, Peters RPH. Collated data of mutation frequencies and associated genetic variants of bedaquiline, clofazimine and linezolid resistance in Mycobacterium tuberculosis. Data Brief. 2018;20:1975–1983. doi:10.1016/j.dib.2018.09.057
4. Matsumoto M, Hashizume H, Tomishige T, et al. OPC-67683, a nitro-dihydro-imidazooxazole derivative with promising action against tuberculosis in vitro and in mice. PLoS Med. 2006;3(11):e466. doi:10.1371/journal.pmed.0030466
5. World Health Organization. Global Tuberculosis Report. World Health Organization; 2014.
6. Gopal M, Padayatchi N, Metcalfe JZ, O’Donnell MR. Systematic review of clofazimine for the treatment of drug-resistant tuberculosis. Int J Tuberc Lung Dis. 2013;17(8):1001–1007. doi:10.5588/ijtld.12.0144
7. World Health Organization. Global tuberculosis report. World Health Organization; 2016.
8. Villar M, Sotgiu G, D’Ambrosio L, et al. Linezolid safety, tolerability and efficacy to treat multidrug- and extensively drug-resistant tuberculosis. Eur Respir J. 2011;38(3):730–733. doi:10.1183/09031936.00195210
9. Koh WJ, Kang YR, Jeon K, et al. Daily 300 mg dose of linezolid for multidrug-resistant and extensively drug-resistant tuberculosis: updated analysis of 51 patients. J Antimicrob Chemother. 2012;67(6):1503–1507. doi:10.1093/jac/dks078
10. Bloemberg GV, Keller PM, Stucki D, et al. Acquired resistance to bedaquiline and delamanid in therapy for tuberculosis. N Engl J Med. 2015;373(20):1986–1988. doi:10.1056/NEJMc1505196
11. Polsfuss S, Hofmann-Thiel S, Merker M, et al. Emergence of low-level delamanid and bedaquiline resistance during extremely drug-resistant tuberculosis treatment. Clin Infect Dis. 2019;69(7):1229–1231. doi:10.1093/cid/ciz074
12. Pang Y, Zong Z, Huo F, et al. In vitro drug susceptibility of bedaquiline, delamanid, linezolid, clofazimine, moxifloxacin, and gatifloxacin against extensively drug-resistant tuberculosis in Beijing, China. Antimicrob Agents Chemother. 2017;61(10). doi:10.1128/AAC.00900-17
13. Yang JS, Kim KJ, Choi H, Lee SH. Delamanid, bedaquiline, and linezolid minimum inhibitory concentration distributions and resistance-related gene mutations in multidrug-resistant and extensively drug-resistant tuberculosis in Korea. Ann Lab Med. 2018;38(6):563–568. doi:10.3343/alm.2018.38.6.563
14. Kowalska-Krochmal B, Dudek-Wicher R. The minimum inhibitory concentration of antibiotics: methods, interpretation, clinical relevance. Pathogens. 2021;10(2):165. doi:10.3390/pathogens10020165
15. Diacon AH, Donald PR, Pym A, et al. Randomized pilot trial of eight weeks of bedaquiline (TMC207) treatment for multidrug-resistant tuberculosis: long-term outcome, tolerability, and effect on emergence of drug resistance. Antimicrob Agents Chemother. 2012;56(6):3271–3276. doi:10.1128/AAC.06126-11
16. Diacon AH, Pym A, Grobusch MP, et al. Multidrug-resistant tuberculosis and culture conversion with bedaquiline. N Engl J Med. 2014;371(8):723–732. doi:10.1056/NEJMoa1313865
17. Veziris N, Bernard C, Guglielmetti L, et al. Rapid emergence of Mycobacterium tuberculosis bedaquiline resistance: lessons to avoid repeating past errors. Eur Respir J. 2017;49(3):1601719. doi:10.1183/13993003.01719-2016
18. Wang G, Jiang G, Jing W, et al. Prevalence and molecular characterizations of seven additional drug resistance among multidrug-resistant tuberculosis in China: a subsequent study of a national survey. J Infect. 2021;82(3):371–377. doi:10.1016/j.jinf.2021.02.004
19. He W, Liu C, Liu D, et al. Prevalence of Mycobacterium tuberculosis resistant to bedaquiline and delamanid in China. J Glob Antimicrob Resist. 2021;26:241–248. doi:10.1016/j.jgar.2021.06.007
20. Liu Y, Gao M, Du J, et al. reduced susceptibility of mycobacterium tuberculosis to bedaquiline during antituberculosis treatment and its correlation with clinical outcomes in China. Clin Infect Dis. 2021;73(9):e3391–e3397. doi:10.1093/cid/ciaa1002
21. Hoffmann H, Kohl TA, Hofmann-Thiel S, et al. Delamanid and bedaquiline resistance in mycobacterium tuberculosis ancestral Beijing genotype causing extensively drug-resistant tuberculosis in a Tibetan refugee. Am J Respir Crit Care Med. 2016;193(3):337–340. doi:10.1164/rccm.201502-0372LE
22. Zheng H, He W, Jiao W, et al. Molecular characterization of multidrug-resistant tuberculosis against levofloxacin, moxifloxacin, bedaquiline, linezolid, clofazimine, and delamanid in southwest of China. BMC Infect Dis. 2021;21(1):330. doi:10.1186/s12879-021-06024-8
23. Kardan-Yamchi J, Kazemian H, Battaglia S, et al. Whole genome sequencing results associated with minimum inhibitory concentrations of 14 anti-tuberculosis drugs among rifampicin-resistant isolates of mycobacterium tuberculosis from Iran. J Clin Med. 2020;9(2):465. doi:10.3390/jcm9020465
24. Zhang Z, Li T, Qu G, Pang Y, Zhao Y. In vitro synergistic activity of clofazimine and other antituberculous drugs against multidrug-resistant Mycobacterium tuberculosis isolates. Int J Antimicrob Agents. 2015;45(1):71–75. doi:10.1016/j.ijantimicag.2014.09.012
25. Azimi T, Khoshnood S, Asadi A, et al. Linezolid resistance in multidrug-resistant mycobacterium tuberculosis: a systematic review and meta-analysis. Front Pharmacol. 2022;13:955050. doi:10.3389/fphar.2022.955050
26. Habibnia S, Karami-Zarandi M, Zaker S, et al. Molecular characterization of resistance to second-line anti-mycobacterial drugs among clinical isolates of multidrug-resistant mycobacterium tuberculosis. Clin Lab. 2023;69(1). doi:10.7754/Clin.Lab.2022.220211
27. O’Donnell MR, Pillay M, Pillay M, et al. Primary capreomycin resistance is common and associated with early mortality in patients with extensively drug-resistant tuberculosis in KwaZulu-Natal, South Africa. J Acquir Immune Defic Syndr. 2015;69(5):536–543. doi:10.1097/QAI.0000000000000650
28. Shah NS, Richardson J, Moodley P, et al. Increasing drug resistance in extensively drug-resistant tuberculosis, South Africa. Emerg Infect Dis. 2011;17(3):510–513. doi:10.3201/eid1703.101363
29. Migliori GB, Lange C, Centis R, et al. Resistance to second-line injectables and treatment outcomes in multidrug-resistant and extensively drug-resistant tuberculosis cases. Eur Respir J. 2008;31(6):1155–1159. doi:10.1183/09031936.00028708
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.