Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Barriers for the Functional Implementation of Community Health Volunteers in Health Developmental Army in Debre Libanos District, Oromia, Ethiopia: A Descriptive Qualitative Study
Authors Tareke KG ![]() , Solomon N
, Solomon N ![]() , Teshome F
, Teshome F ![]()
Received 4 October 2021
Accepted for publication 15 December 2021
Published 11 January 2022 Volume 2022:15 Pages 103—114
DOI https://doi.org/10.2147/JMDH.S342711
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Kasahun Girma Tareke,1 Nahom Solomon,2 Firanbon Teshome1
1Department of Health, Behavior and Society, Faculty of Public Health, Institute of Health, Jimma University, Jimma, Ethiopia; 2Department of Public Health, Mizan Tepi University, Mizan-Aman, Ethiopia
Correspondence: Kasahun Girma Tareke Email [email protected]
Background: Although the existing evidence suggests that the implementation of the health, developmental army (HDA) brought promising successes towards the delivery of Health Extension Programs (HEPs), pieces of evidence have shown that there are problems related to its functionality. Therefore, this study explored barriers to the functionality of HDAs.
Methods: A descriptive qualitative study was conducted from March 11 to April 7, 2019, in the Debre Libanos District, Oromia, Ethiopia. The study participants were purposively recruited from six kebeles. They were recently delivered mothers, pregnant women, other reproductive age group community members, health workers, kebele chairman, HDA team leaders, and religious leaders. Five in-depth interviews, seven key informant interviews, and four focus group discussions were conducted with a total of 52 participants. Data were audio-recorded, transcribed verbatim, and translated. The inductive thematic analysis approach was used and the data were coded, categorized, and themes were developed using Atlas ti.7.1. software package.
Results: The barriers to the functionality of HDAs were organized into four major themes. First, it was affected by structure, monitoring, or supervision-related challenges. Second, community-related barriers such as perceptions and attitudes towards HDAs, and the need for incentives or compensation from the HDAs affected the functionality. Third, it was affected by the lack of multi-sectoral collaboration to strengthen, monitor, or supervise the HDAs. Lastly, behavior, residence, or shortage of health extension workers affected its implementation. In addition, the study found that, as a result of poor functionality of HDAs, service utilization was decreased, especially antenatal care, postnatal care, sick newborn treatment, etc.
Conclusion: The functionality of HDAs was affected by a variety of barriers. Therefore, there is a need to develop different strategies and take action to address the explored barriers to improve their capacity and implementation status for increasing health care service utilization.
Keywords: Health Developmental Army, health extension worker, Health Extension Program, community health volunteers, barriers, Ethiopia
Background
Health Developmental Army (HDA) is a network comprising women who have adopted better health behavior through completing the packages of Health Extension Program (HEP) with five other women who have not yet completed so that they can influence the later to practice a healthy lifestyle.1,2 The HDA team leaders and members voluntarily (working without payment) conduct the activities, and in Ethiopia, it was established in 2011. It is organized under the facilitation of health centers, health extension workers (HEWs) and kebele administrations.1–3 Functional team leaders meet every 2 weeks.1,2 The network is established to support the HEWs for successful implementation of the 16 HEP packages, which focuses on basic promotive, preventive and curative health services.3,4 They are the most important frontiers, especially, for maternal, newborn and child health interventions, which include the provision of antenatal and postnatal counseling and service, promotion of institutional delivery, identification of maternal and newborn danger signs and referral, identification of sick newborn and referral.1,2,5
They play a role in being role models for others, monitoring the implementation of the one to five network plans, gathering and analyzing the data, identifying the bottlenecks and the way forward, and sharing the best experiences. They are also responsible for mobilizing communities to improve the community’s capacity to bring sustainable behavioral changes for improved health outcomes.1–3 Specific to maternal, neonatal and child health care services, they are responsible for identifying families who need services, developing the healthcare-seeking behavior of the community members, promoting the availability of services delivered at the community and health facility level, introducing new health cultures that significantly reduce mortality.2,5
Moreover, evidence from various countries in the world indicated that community volunteers are involved in health service intervention programs, and significantly contributed to improving community health, especially in developing countries where there is a shortage of health care providers.6–11 For instance, pieces of evidence from Ethiopia indicated that these volunteers brought a reduction in maternal and child morbidities and mortalities; improved maternal, neonatal and child health services such as immunization, skilled delivery, antenatal care visits by sharing information for mothers; notifying the presence of delivering women; improve health-seeking behaviors and facilitate early referral to reduce the delay of seeking care. They conduct these activities under close supervision of HEWs; who provide the health extension packages at the grassroots level (ie, health post and home-to-home to reach all mothers and newborns).9–14
Although several actions have been undertaken, the actions and requirements should be reviewed and put in place to make the network strong enough to play a role in reducing maternal and newborn morbidity and mortality through promoting health and enhancing health-seeking behavior and utilization. For instance, a study conducted in the current study setting indicates that the HDAs team leaders were not functional or did not conduct activities expected from them.15 Existing evidence indicated that the performance of community health workers was challenged from lack or irregularity of supportive supervision, high workload without monetary compensation, lack of family support, or lack of motivation or appreciation.9–11,16–20 However, little was known about the barriers affecting their functionality in the study setting or the context of our country, Ethiopia. Therefore, this study explored barriers to the functional implementation of HDA teams. Moreover, exploring and understanding its barriers is critical and useful for reorganizing and/or strengthening the network, and empowering them to play a substantial role in maternal and newborn health-seeking behavior and utilization. The findings of the study would be helpful for local and national program planners to develop strategies that address the barriers and enhance the delivery of HEP.
Methods
Study Design, Setting and Period
A descriptive qualitative study design was conducted from March 11 to April 7, 2019, in the Debre Libanos District. The district is located around 90 km away from Addis Ababa in the Northwest direction. The population of the district was estimated to be 64,305 (Debre Libanos district health office annual plan, 2018/2019, unpublished data). Nearly, 77.1% and 22.9% of the population lived in rural (ie, farmers) and urban, respectively. About 99.29% of the inhabitants practiced Ethiopian Orthodox Christianity. The majority of them were Oromo in ethnicity followed by Amhara.21 There were 2 health centers, 10 functional health posts (ie, 2 urban and 8 rural), 1 nonfunctional health post (ie, no health extension worker) and 3 private primary clinics. The district also had 4 health officers, 1 BSc nurse, 20 clinical nurses, 1 public nurse, 4 laboratory technicians, 2 druggists, 5 midwifery nurses, 14 rural and 5 urban HEWs (Debre Libanos district health office annual plan, 2018/2019, unpublished data).
Ethiopian Health Care System Structure
Currently, Ethiopia follows a three-tier health care system: Primary, Secondary and Tertiary levels of care. A primary health care system is found at the grassroots level that comprises primary hospitals (each serving 60,000–100,000 population), health centers (each serving 15,000–25,000 Population) and health posts (each serving 3000–5000 population). A primary hospital provides emergency, inpatient and ambulatory services, and referral sites for health centers. Also, it acts as a practical training center for nurses and other health professionals. In addition, the primary health care level has a primary health care unit structure in which a health center and five satellite health posts are linked together through referral and supervision. Health post is the lowest-level health system facility and the point where HEP is delivered near the community. Exceptionally, in an urban setting, the health care system is organized with a health center as a primary entry point (each serving about 40,000 populations). Therefore, this is a stage when community volunteers, HDAs, enter the health system to facilitate and play a role in delivering HEP.1,22–25 Accordingly, there were an estimated number of 45,414, 195864 (FMOH. Annual Performance report, 2020, unpublished data) and 223 (Debre Libanos district health office annual plan, 2018/2019, unpublished data) HDAs nationally, in Oromia regional state and Debre Libanos district, respectively. The secondary health care system includes a general hospital (each serving 1–1.5 million people) that act as a referral center for primary hospitals, and also a training center for health officers, nurses and emergency surgeons. A tertiary health care system includes a specialized hospital, a referral center for general hospitals (each serving 3.5–5 million people).1,22–25
Study Participants and Participant Recruitment
A total of five in-depth interviews, seven key informant interviews, and four focus group discussions were conducted with 52 diversified groups of individuals. The participants were purposively recruited participants from six kebeles (ie, the lowest level of administration in the Ethiopian government that consists of 3000–5000 catchment populations). The kebeles were selected considering the number of catchment kebeles per health center, diversity in distance from the health center, rural versus urban residence, and performance of the HEWs. The participants involved in an in-depth interview were HDA team leaders. The key informants were health workers, HEWs, religious leaders, and kebele chairman.
Twelve participants were recruited for each focus group discussion, but 7–12 individuals have participated. The participants were from women who gave birth within 2 months before data collection, families of women who gave birth, mother-in-law, fathers-in-law, pregnant mothers, and other reproductive age group people. Participants from health facilities were recruited based on their role in the implementation and monitoring or supervising of HDAs. At the kebele level, study participants were recruited based on having rich information on the organization, structure, and role of HDAs towards facilitating health care service utilization among community members.
Data Collection Instrument and Procedures
Data were collected through in-depth interviews, key informant interviews and focus group discussions using a semi-structured guide (Supplementary File). The guide was developed by the principal investigator in the English language in relation to the research questions considering local knowledge and cultural sensitivities. Then, the guides were translated into Afan Oromo and Amharic languages and back‐translated into English by an independent translator. The guides were developed to cover topics related to 1) community-related barriers to HDAs implementation; 2) health facility-related barriers to HDAs implementation; 3) HEWs-related barriers of HDAs’ implementation.
The principal investigator was the modulator throughout the in-depth interviews, key informant interviews and focus group discussions. Before starting the interview and discussion, the purpose of the study and the topic of discussion were explained well to study participants. Individual-based written informed consents were taken, and separate consents were obtained to record their voice. The moderator used a topic guide to conduct the interviews and modulate the focus group discussions aiming to cover all relevant topics. The in-depth interviews and focus group discussions were conducted in their natural settings; the in-depth interviews were conducted with women, religious, one to five and HDA leaders in their homes, focus group discussions at the community level, and interviews with health workers and kebele chairman at their office. The in-depth interviews were conducted on a one-on-one basis between the principal investigator and participant, but the focus group discussions were conducted by the principal investigator as a modulator and research assistant as a note-taker and audio-recorder. On average, the focus group discussions lasted from 1:15 to 1:41 hour and the interviews with community members lasted from 21:33 to 43:51 minutes and interviews with health workers lasted from 0:39:40 to 1:12 hour.
Data Analysis
Inductive thematic analysis was employed to analyze the data using Atlas.ti 7.1. software version. The analysis was started in the field debriefing the data with a research assistant. The audio-recorded material was transcribed verbatim. Field notes were incorporated within the transcription simultaneously. Then, the transcriptions were checked for completeness and consistency. Then, all focus group discussions and in-depth interview transcripts were translated from Afan Oromo and Amharic languages to English by the principal investigator and research assistant. The completeness and consistency of the translations were checked with the transcriptions.
Then, reading and re-reading the transcription were done to extract important points from the description. Line-by-line coding was done starting from the richest data on Atlas ti 7.1. Then, inter-coder consistency was checked and the codebook manual was developed. After that, the principal investigator coded the whole translations using the codebook manual as a guide to ensure code consistency and credibility. Again, the principal investigator repeated the coding system to check intra-coder consistency. Potential categories and themes were developed by clustering codes and categories, respectively, which answer the research questions. The principal investigator repeated the coding system four times after the first codebook was developed while refining the codebook, categories, and themes.
Trustworthiness (Rigor)
To ensure the trustworthiness of the study findings, different techniques were used.15,24,26,27 First, the guiding questions were developed concerning the research objectives and pretested at a neighboring district. Second, data were collected from diversified groups of participants recruited from six kebeles. Third, a daily-based data debriefing was done with a research assistant. Fourth, member checking was conducted by presenting the summary of major themes to study participants at the end of each interview and focus group discussion, conducting a discussion with them on the issues for checking consistency and understandability. Also, the transcriptions and translations, a summary of core points and some confusing ideas were shared with the study participants for clarity and to check the interpretations. Then, they provided their comments and critiques on the raised points and consensus was made on unclear ideas. Therefore, during subsequent interviews and focus group discussions, findings from emerging data were briefly presented to participants for confirmation and refutation.
Fifth, data were triangulated by collecting data through in-depth interviews and focus group discussions (method triangulation) from perspectives of different community members, key informants, clients and health care providers (data triangulation). Sixth, the principal investigator spent enough time on this study setting, interacting with study participants during the recruitment, data collection and analysis, and member checking (ie, prolonged engagement). During this time, he observed various aspects like the closure of health posts on working hours, time spent by HEWs in the health posts, their punctuality and traveling to and from town, presence or absence of arrangements such as pregnant women conferences, supervision and mentoring for the HEWs or HDAs, the decrease in the trend of maternal and newborn health service utilization from secondary data, etc. These observations enabled the researcher to confirm the findings of the interviews and FGDs. Seventh; the principal investigator created rapport by discussing the importance of this study with zonal health department staff, district health office staff, health center staff and study participants (ie, spoken with a range of people) and developed a trusting relationship with them. Eight, contradicting ideas or deviant cases that emerged in the data were analyzed by enquiring in-depth information from potential study participants on the consecutive data collection periods [Negative case analysis] and the analysis and interpretation were tested against audio tapped data and notes taken before producing the final document (inferential adequacy). Ninth, the whole research process, participants’ diverse perspectives and experiences, methodology, interpretation of results, and contributions of research assistants were explained (thick Description) to ensure transferability and dependability.
Tenth, the principal investigator is a public health officer in his educational background who had working experience of the health center and took training in areas related to HDAs issues. The investigator was also an expert in health promotion and health behavior and has research experience in conducting in-depth interviews and focus group discussions (Researcher self-reflectivity and bracketing). Eleventh, the whole research process, paradigm, and findings of this study were audited and verified by the research assistant, colleagues and another person who has experience in qualitative research (audit trial).
Result
Participants’ Socio-Demographics
The majority of study participants were married women with ages ranging from 31 to 40 years. The mean age of participants was 37.6 years (range: 21–73 years). Predominantly, they were from rural and all of the participants were Oromo in ethnicity and Orthodox in religion (Table 1).
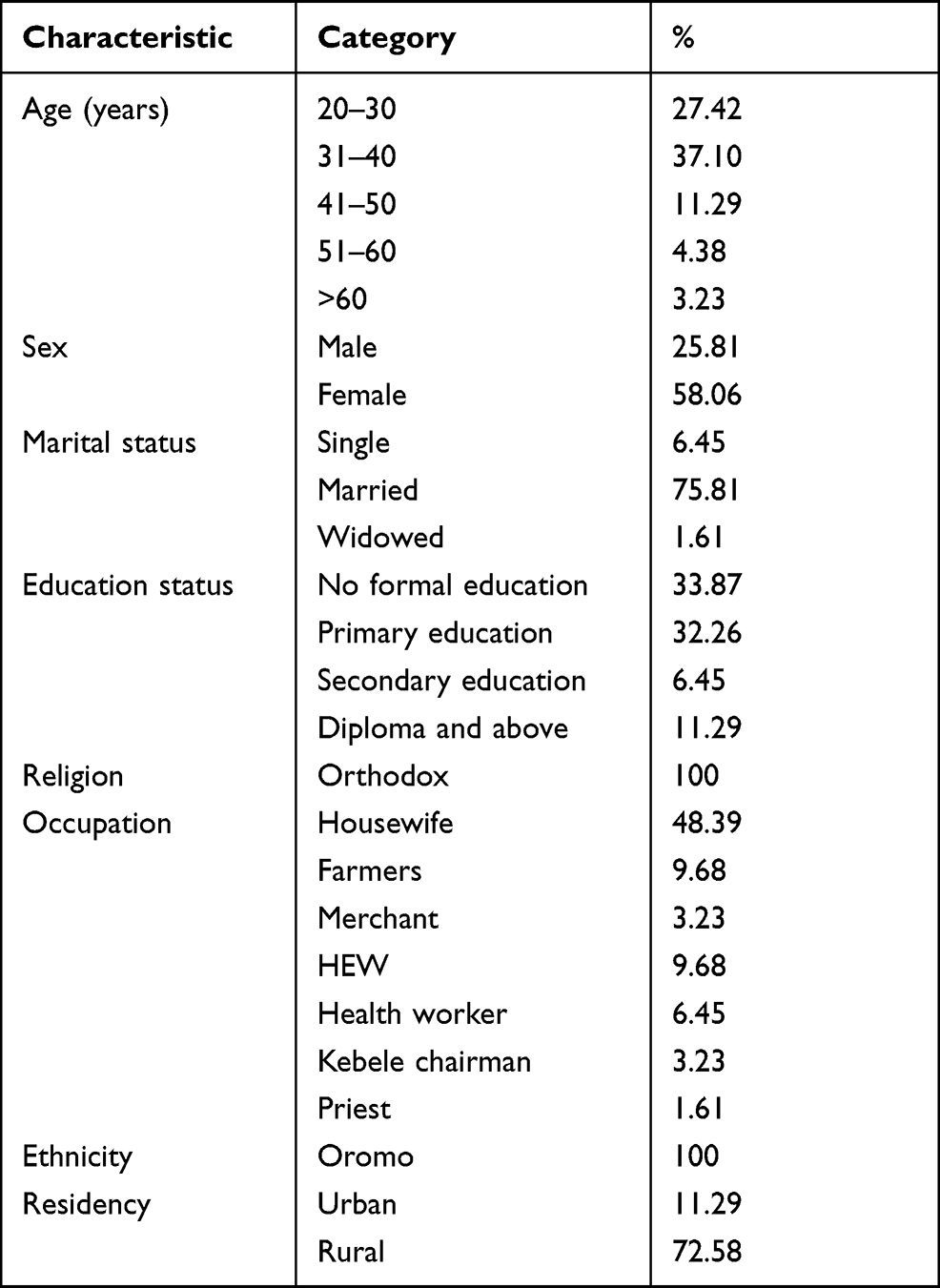 |
Table 1 Demographic Characteristics of Participants in Debre Libanos District, North Shoa, Oromia, Ethiopia, 2019 (n=62) |
The study found key barriers affected the implementation of HDA and was grouped into four major themes: structure, monitoring and supervision-related challenges; intersectoral collaboration-related challenges; HEWs-related challenges, and community-related challenges. In addition, the study also explored the study participants perceived negative health consequences or impacts of non-functional HDAs on health service utilization.
Barriers for the Functional Implementation of HDA
Barriers to HDA functional implementation, in the context of this study, imply any perceived or actual barriers that affected the implementation status of the HDAs and were mentioned by the study participants. Therefore, the study explored barriers that were organized into four major themes. There is a relationship between the explored themes and no demarcation was kept while presenting the barriers. For instance, the HEW-related barriers have a strong relationship with the structure, monitoring or supervision, and community-related barriers. This is because the residence, commitment and shortage of the HEWs resulted in not strengthening, supervising, or monitoring the HDAs, and changing the perception of the community members towards the HDAs. Additionally, poor intersectoral collaboration has a nearly similar effect on the structure, monitoring or supervision with that of the HEW-related barriers (Figure 1). Therefore, anyone who reads this work should have understood these concepts.
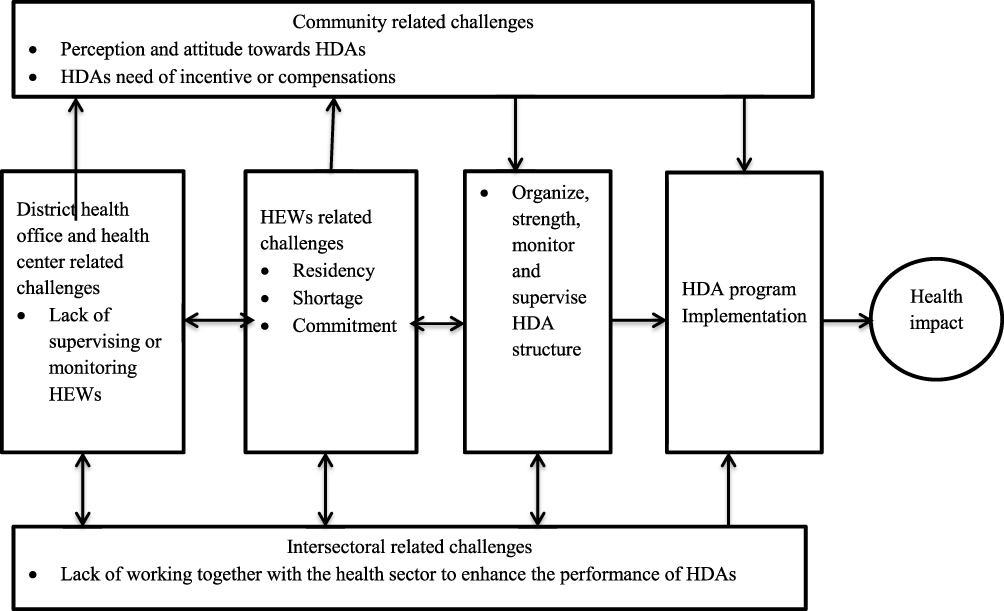 |
Figure 1 Schematic representation of the workflow of barriers affecting the functional implementation of Health Developmental Army in the Debre Libanos district, Oromia, Ethiopia, 2019. |
Structure, Monitoring or Supervision-Related Barriers
Study participants mentioned that, from the beginning, the HDAs were not organized to the level of playing a role and supporting HEWs in providing or delivering the health extension packages to the community members. In addition, it was also mentioned that the community members did not know their team members or the teams did not know each other. However, the HEWs report in a written document to the health center or district health office without its availability on the ground. This affected the implementation of the activities expected from the HDAs.
There is a problem with this issue. Previously, we were obtaining reports as the HDAs were organized well. However, when we look at the ground level, it is not well organized or functioning. (34 years old, in-depth interview participant, health worker)
The majority of the study participants indicated that the HEWs, kebele chairmen, health centers, district health offices and other sectors did not provide regular monitoring or supervision to HDAs. They mentioned that the supportive supervisions were discontinued in a meanwhile due to lack of attention and from poor commitment of the health, political and other sectors. This affected the implementation of activities conducted by HDAs in the study setting.
Previously, there were regular supportive supervisions provided to health developmental armies. However, currently, no one is providing it for them. (58 years old, focus group discussion participant, community member)
The health extension workers are responsible to provide supportive supervision to the health developmental armies. However, they only reach health post and return without accomplishing their duties. (30 years old, in-depth interview participant, health worker)
On the other hand, it was mentioned that the health workers from the health center did not provide supportive supervision of the HEWs weekly indicating weak health center and health posts linkage. This was happening from a poor commitment of the health workers or lack of transportation or accommodation expenses, especially for those health center staff. The health workers who participated in this study mentioned that they expense non-reimbursed pocket money while going to the health post for supervision. This created dissatisfaction among them, which in turn, affected the implementation of activities conducted by HDAs.
There is a weak linkage between the health center and health posts. We do not provide supportive supervision to the health extension workers or health developmental armies regularly as per the schedule. (30 years old, in-depth interview participant, health worker)
Intersectoral Collaboration-Related Barriers
The study also found that kebele command posts, women leagues, political administrations, agricultural and other sectors were expected to support the HEWs and involve in supporting, monitoring or supervising the HDAs. However, it was mentioned that there were no such activities conducted by these sectors. They perceived that it was a mandate of health sectors to supervise or monitor them.
The kebele command post is the major contributor to affect the implementation status of health developmental armies. This is because they did not support the health extension workers in monitoring or supervising the health developmental armies. Previously, other sectors like women and child office were also supporting them, but currently, they do not. (34 years old, in-depth interview participant, HEW)
Health Extension Workers (HEW)-Related Barriers
In the context of this study, these challenges include any problems reported by the study participants from the HEWs side that affected the implementation of HDAs. This theme is further categorized into three categories: shortage, residence and commitment/behavior of the HEWs.
Shortage of HEWs
In the study setting, two health posts had only one HEW and one health post had HEW. Due to this, it was mentioned that health posts were closed during working hours, and HDAs did not obtain adequate support, monitoring or supervision from HEWs.
… For example, for this broad kebele, we have only one health extension worker. How can one health extension workers reach all health, developmental armies within this kebele? (34 years old, focus group discussion participant, community member)
Residency of HEWs
Residency of the HEWs was also mentioned as a major challenge for the successful implementation of HDAs. They mentioned that except for two of them, the rest of rural HEWs lives in district town and work traveling from there due to lack of residence home within the kebele and at nearby the community. Due to this; they were not available at the health posts timely on working hours, on weekends and holidays to support, monitor or supervise the HDAs.
At the current time, the health developmental armies do not conduct activities due to problem-related to the health extension workers. They live and work traveling from the district town. Due to this problem, they do not supervise and conduct a meeting with health, developmental armies. (30 years old, in-depth interview participant, HDA team leader)
Commitment/Behavior
The study participants were mentioned that most of the time, health posts were closed during working hours. It was indicated that the HEWs were available at the health post for 3–4 hours per day for a maximum of 3 days per week. They did not take adequate time to plan, transfer knowledge and skill, or discuss issues with the HDAs; affecting the implementation of HDAs.
The health posts might be open once per week. The health posts are only open for the expanded program for immunization, but not for other activities. With this condition, we do not expect that the health developmental armies successfully implement their activities. (32 years old, male, in-depth-interview participant, health worker)
Community-Related Barriers
In the context of this study, community-related challenges imply that any problems reported by the study participants from the community member side affected the implementation of HDAs. This theme is further categorized into two categories: the community’s perception and attitude towards HDAs, and HDAs need for incentive or compensation.
Communities Perception and Attitude Towards HDA
Study participants also mentioned that community members had a negative attitude towards HDAs. They indicated that conflict was commonly occurring while discussing issues of interest within team members or broad community, and also taking action. Due to this, the community members perceived it as an enemy that affected their harmony, affecting the implementation of activities conducted by HDAs.
Some people perceive health developmental army as a source of conflict among the community members during their discussion and setting solution. (34 years old, in-depth interview participant, health extension worker)
HDA-Related Barriers: Need of Incentive or Compensation
Study participants mentioned that the HDAs voluntarily played a significant role to change the community’s health-seeking behavior. However, there was no recognition or compensation given to them from the concerned bodies (ie, the district health office, health center or other sectors). Therefore, they mentioned that for the sustainability of the program and better performance, there should be compensations in-kind or material for extra services they rendered to communities.
There is no support we receive from the District or the health center. I am doing this voluntarily, because, I would like to see the change in my community. It will be great if we receive recognition either from the District or the Health Center. (38 years old, female, HDA leader)
The Negative Consequences or Impacts of Non-Functional HDAs on Health Service Utilization
Study participants mentioned that due to the non-functionality of the HDAs, the community’s health-seeking behavior and utilization were decreased. Especially, the trend maternal, neonatal and child health care services such as antenatal care, pregnant women’s conference, skilled delivery, postnatal care, immunization, and community-based newborn care service utilization such as community-based management of newborn possible serious bacterial infection was decreased.
If HDA identifies pregnant women as early as possible, then pregnant women’s conference will be conducted. This increases service utilization. However, it is very low. Currently, due to a lack of functional the HDAs, home delivery becomes increased. (30 years old, in-depth interview participant, health worker)
Discussion
This study found structure, monitoring or supervision-related barriers; community-related barriers (community perception and attitude towards HDAs, and HDAs need of incentive or compensation), inter-sectorial collaboration-related barriers, and HEW-related barriers (shortage, residence and commitment) that affected the functional implementation of HDAs. This study also explored the communities’ and health care providers’ perspectives on the negative consequences that resulted in service utilization from the non-functionality of the HDAs.
The study found that there the HDAs were not monitored or supervised well due to a lack of commitment among HEWs, health workers, kebele chairman and other sectors. However, the establishment of HDA mandates that the health and other sectors are involved in organizing the HDAs, and the HEWs are expected to provide monitoring or supervision to the leaders every 2 weeks, aiming to empower their capacity in identifying local problems, prioritizing, implementing and evaluating activities related to Health Extension Programs.25 This implies there is a lack of putting into practice the principles or strategies endorsed by the Ministry of Health or higher health sectors. Therefore, importantly, this underscores the necessity of sticking to the implementation strategies, guidelines and principles to conduct to regularly monitor and supervise the HDAs. Similarly, this finding was supported by the other findings that indicated that poor or limited supervision and support was a factor that negatively affected barrier the implementation of HDAs.16,28
The study also found that there were problems with a health center or district health officials in monitoring or supervising the HEWs. As a result, they were not available at the health posts during working hours; affecting the implementation of HDAs. This happened from lack of commitment or burnout from expensing non-reimbursed pocket money for travel and accommodation. However, in the context of the Ethiopian health care system, through health center-health post linkage, the HEWs should be supervised every week by the health centers to improve their knowledge and skill, identify and solve challenges facing them, and support them in strengthening or developing the capacity of HDAs to enhance healthcare-seeking behavior of the community members.25 Therefore, this implies that there is a weak health center and post linkage that needs to strengthen the linkage for better HDAs’ implementation on HEP. Moreover, this underscores that the government should have to allocate accommodation and travel expenses or facilitate transportation. In addition, the government should restructure the health posts to a higher level and assign other health professionals like nurses at each health post for better service delivery and to closely monitor or supervise the HEWs and HDAs. Similarly, existing evidence support this finding that the community health workers did not get regular supportive supervision or monitoring the concerned bodies.16,19 Also, a study conducted in rural Zimbabwe emphasized the importance of supportive supervision and indicated the more community health workers get supportive supervision, the higher behavior change lesson scores would be achieved.9
The study also found that the shortage of HEWs was one of the challenges, which affected the implementation status of HDAs. This affected the supportive supervision or monitoring provided to the HDAs to improve their capacity to enhance the utilization of HEP among the community members. However, according to the Ethiopian HEP, two HEWs should have to be assigned to the health posts.25 Therefore, this underscores the need to fill the gap and assign the required number of HEWs per health post.
Also, health posts were not opened during working hours of the day over the course of a week from the living conditions of HEWs. Almost all of them lived in the district town due to a lack of residential houses. As a result, they were not regularly monitored or supported the HDAs, or the HDAs had no chance to get them as they want. However, accordingly, they should have to live in the village nearby the community.1,25 Therefore, this underscores that the kebele administrator along with the health and other sectors should have to mobilize resources and construct a residential home for them within the community. Also, they should have to live within the community by renting a residential house and keep going to provide the service and improve the capacity of the HDAs till the residence house is built. On the contrary, there was evidence which indicated that approximately 15% of health posts were open less than 5 days of the week and also a little over half of them serve the community weekends or holidays25 and from an observational time-motion study which showed that they open health posts for 21 days showing health extension workers were on duty for an average of 15.5 and they stayed on duty for about 6 hours per day.29 This difference might probably be due to differences in geographical location, availability of residential homes constructed for them, their commitment or due to lack of supportive supervision given to them from health or other sectors.
This study also found that, except for the health sector, there is a lack of different sector’s involvement in establishing, supervising and monitoring affected implementation of the HDAs. In contrast, inter-sectoral and multi-sectoral collaboration is promoted for the improvement of the health status of the population at large.30 This implies that there was a poor inter-sectoral collaboration in the district and which underscores the necessity of putting into practice the principles and strategies in supporting the health extension workers to reorganize, monitor and supervise HDAs for successful implementation of HEP. Similarly, the finding from other qualitative study conducted in Ethiopia supports this finding.28
The other challenge found in the study was that the community had a poor perception or attitude towards HDAs. The community members consider the HDA as an enemy, which affected their social interaction from the conflicts that occurred while discussing their competing interests or taking action. This might imply that the community members did not understand the purpose of the HDA or the way they had discussed or solved problems might have wrong directions. Therefore, this underscores the need to conduct a social and behavioral change communication to change the community member’s perception and develop positive attitudes towards HDAs and their importance for the health care service utilization. Similarly, this finding was supported by the finding of another qualitative study that showed the opposition from local community members was mentioned as a barrier to the success of HDAs’ initiatives.28
Lack of incentive or compensation provided to the HDA team leaders was also identified as a challenge for the successful implementation of the HDA. The study found that there were no compensation or incentives provided to the HDAs from the health or other sectors. This implies that the HDAs need material compensations for the extra services they rendered to communities. Therefore, there should be a provision of incentives like motivation and recognition for their performance, even though the program is established to involve the community members and take part voluntarily.1,2,5 On the other hand, the program will benefit if new HDA team leaders will be regularly replaced to avoid burnout. Similarly, this finding was supported by the finding of a study that indicated that a study conducted in lack of recognition and appreciation of accomplishments negatively affected their motivation.16 Also, evidence indicated that they were overloaded with different activities without incentive, promotion or compensation, and lack of support from the family from the perception that it has low economic value of the family leading them to be stressed and/or deprived.17,18
This study also found that the negative consequences resulted from the non-functionality of HDAs in the study setting. It was indicated there key health care service utilization, especially maternal and newborn health services like the antenatal care, postnatal care, and delivery services; health care seeking for sick newborns or maternal health conditions was decreased, and there was a progressive increase of home delivery. This implies the HDA was very important for enhancing the health care service utilization, which become decreased after the HDAs become non-functional. Therefore, there is a need to improve reorganizes the HDAs and make them functional by developing strategies to address the key challenges explored in this study. In contrast, the findings of studies conducted in different settings showed that there were achievements seen in health care service utilization from activities done by HDAs. For example, it was indicated that HDAs have been conducting early pregnant women identification, facilitating and provision of antenatal care and postnatal care service, identification of sick newborns, referring sick newborns and children to health facilities, carrying out social mobilization activities to increase the knowledge, develop an attitude and health-seeking behavior of mothers.12,14,25,31–33
Strengths and Limitations
This study has several strengths. To the best of authors’ knowledge, this is the first study conducted in Ethiopia that explored challenges for the successful implementation of the HDA. A diversified group of participants was involved in the study to generate ideas from different perspectives. The focused groups allowed frank discussion among attendees. The findings of this study significantly help local planners and managers to improve the implementation of HDAs. This study also has limitations. There might be a probability of social desirability bias. Literature relating to the challenges of successful implementation of the HDA was very limited.
Conclusions
From this study, it was understood that the functional implementation of community volunteers in HDAs was affected by both the community and health facility-related barriers. The communities had negative perceptions and unfavorable attitudes towards the network from the conflict arising while discussing issues. This might imply that the HDA leaders lack skill in facilitating discussions or criticize their members to a level of causing conflict. Therefore, there is a need to empower the leader’s skill to facilitate discussion, and social and behavioral change communication needs to be done addressing the whole community to change their perception and attitude towards the purpose of the network. Also, HEW’s commitment, residence and shortage affected its implementation. Therefore, there HEWs need to be committed and regularly monitor the volunteers to improve their capacity and implementation to enhance health care service utilization and reduce the negative health consequences. The health and other sectors are advised to give due emphasis to the implementation of HDA, solve the bottlenecks and reward those who successfully achieved their performance. The chain of monitoring and supportive supervision needs to be strengthened both at the local and national level. The researchers are also recommended to conduct studies on similar issues broadly as regional and national given that this study was only in one district.
Abbreviations
HAD, Health Developmental Army; HEP, Health Extension Program; HEW, health extension worker.
Data Sharing Statement
All study data were reported within the manuscript.
Ethics Approval and Consent to Participate
Ethical approval was obtained from the Jimma University Research Ethical Review Board, Ethiopia. The right of research participants was maintained by ensuring non-maleficence and underscoring the benefits of the study. Study participants were informed adequately about the purpose of the study, voluntary participation and right to participate or withdraw at any time. To ensure their privacy and autonomy, codes were given to participants and they were informed that the study uses the codes in place of their names in connection with the study findings or their answers on discussions or interviews. Time was given to them to reflect and provide a detailed explanation of the issue. Written informed consent was taken from all study participants for participation in the study and records their voice. Furthermore, the authors confirmed that there participant’s response was anonymized to ensure their confidentiality.
Acknowledgments
We acknowledge research assistants, and study participants for their voluntary participation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. The authors reviewed the manuscript and it is their original work.
Disclosure
The authors declared that they have no competing interests in this work.
References
1. Maternal and Child Health Directorate. Federal Ministry of Health. National newborn and child survival strategy 2015/16–2019/20. Addis Ababa: FMOH; 2015.
2. Federal Democratic Republic of Ethiopia Ministry of Health. HSTP health sector transformation plan 2015/16–2019/20 (2008‐2012 EFY); 2015.
3. Banteyerga H. Ethiopia’s health extension program: improving health through community involvement. MEDICC Rev. 2011;13(3):46–49.
4. Sebhatu A. The implementation of Ethiopia’s health extension program: an overview. Addis Ababa, Ethiopia; 2008.
5. Federal Ministry of Health [Ethiopia]. National newborn and child survival strategy document brief summary 2015/16–2019/20; 2015.
6. Glenton C, Scheel IB, Pradhan S, et al. The female community health volunteer programme in Nepal: decision makers’ perceptions of volunteerism, payment and other incentives. Soc Sci Med. 2010;70(12):1920–1927. doi:10.1016/j.socscimed.2010.02.034
7. Hadi A. Management of acute respiratory infections by community health volunteers: experience of Bangladesh Rural Advancement Committee (BRAC). Bull World Health Organ. 2003;81(3):183–189.
8. Chung MHL, Hazmi H, Cheah WL. Role performance of community health volunteers and its associated factors in Kuching District, Sarawak. J Environ Public Health. 2017;2017:1–9. doi:10.1155/2017/9610928
9. Kambarami RA, Mbuya MN, Pelletier D, Fundira D, Tavengwa NV, Stoltzfus RJ. Factors associated with community health worker performance differ by task in a multi-tasked setting in rural Zimbabwe. Glob Health Sci Pract. 2016;4(2):238–250.
10. Jobson G, Naidoo N, Matlakala N, et al. Contextual factors affecting the integration of community health workers into the health system in Limpopo Province, South Africa. Int Health. 2020;12(4):281–286.
11. World Health Organization. Community health workers: What do we know about them? Available from: https://www.who.int/hrh/documents/community_health_workers.pdf.
12. Berhanu D, Avan BI. Community Based Newborn Care: Quality of CBNC Programme Assessment-Midline Evaluation Report, March 2017. London: IDEAS, London School of Hygiene & Tropical Medicine; 2017.
13. Alam N, Hajizadeh M, Dumont A, Fournier P. Inequalities in maternal health care utilization in sub-Saharan African countries: a multiyear and multi-country analysis. PLoS One. 2015;10(4):e0120922.
14. Yitbarek K, Abraham G, Morankar S. Contribution of women’s development army to maternal and child health in Ethiopia: a systematic review of evidence. BMJ Open. 2019;9(5):e025937. doi:10.1136/bmjopen-2018-025937
15. Tareke KG, Lemu YK, Feyissa GT. Exploration of facilitators of and barriers to the community-based service utilization for newborn possible serious bacterial infection management in Debre Libanos District, Ethiopia: descriptive qualitative study. BMC Pediatr. 2020;20(1):1–4. doi:10.1186/s12887-020-02211-9
16. Jigssa HA, Desta BF, Tilahun HA, McCutcheon J, Berman P. Factors contributing to motivation of volunteer community health workers in Ethiopia: the case of four woredas (districts) in Oromia and Tigray regions. Hum Resour Health. 2018;16(1):57. doi:10.1186/s12960-018-0319-3
17. Maes K, Closser S, Tesfaye Y, Gilbert Y, Abesha R. Volunteers in Ethiopia’s women’s development army are more deprived and distressed than their neighbors: cross-sectional survey data from rural Ethiopia. BMC Public Health. 2018;18(1):1. doi:10.1186/s12889-018-5159-5
18. Steege R, Taegtmeyer M, McCollum R, et al. How do gender relations affect the working lives of close to community health service providers? Empirical research, a review and conceptual framework. Soc Sci Med. 2018;209:1–3. doi:10.1016/j.socscimed.2018.05.002
19. Kok MC, Kea AZ, Datiko DG, et al. A qualitative assessment of health extension workers’ relationships with the community and health sector in Ethiopia: opportunities for enhancing maternal health performance. Hum Resour Health. 2015;13(1):1–2. doi:10.1186/s12960-015-0077-4
20. Kawakatsu Y, Sugishita T, Tsutsui J, et al. Individual and contextual factors associated with community health workers’ performance in Nyanza Province, Kenya: a multilevel analysis. BMC Health Serv Res. 2015;15(1):1. doi:10.1186/s12913-015-1117-4
21. Population, E.O.o.t. and H.C. Commission. Summary and statistical report of the 2007 population and housing census: population size by age and sex. 2008: Federal Democratic Republic of Ethiopia, Population Census Commission. Available from: https://www.ethiopianreview.com/pdf/001/Cen2007_firstdraft(1).pdf. Accessed December 24, 2021.
22. Assefa Y, Gelaw YA, Hill PS, Taye BW, Van Damme W. Community health extension program of Ethiopia, 2003–2018: successes and challenges toward universal coverage for primary healthcare services. Global Health. 2019;15(1):1. doi:10.1186/s12992-019-0470-1
23. World Health Organization. Primary health care systems (PRIMASYS): case study from Ethiopia, abridged version. Geneva: World Health Organization; 2017. Licence: CC BY-NC-SA 3.0 IGO.
24. Gizaw AT, Zebre G, Tareke KG, Lemu YK. Implementation, experience, and challenges of urban health extension program in Addis Ababa: a case study from Ethiopia; 2021.
25. Wang H, Tesfaye R, Ramana GN, Chekagn CT. Ethiopia Health Extension Program: An Institutionalized Community Approach for Universal Health Coverage. The World Bank; 2016:25.
26. Tesfaye L, Lemu YK, Tareke KG, Chaka M, Feyissa GT. Exploration of barriers and facilitators to household contact tracing of index tuberculosis cases in Anlemo district, Hadiya zone, Southern Ethiopia: qualitative study. PLoS One. 2020;15(5):e0233358. doi:10.1371/journal.pone.0233358
27. Tareke KG, Lemu YK, Yidenekal SA, Feyissa GT. Community’s perception, experiences and health seeking behavior towards newborn illnesses in Debre Libanos District, North Shoa, Oromia, Ethiopia: qualitative study. PLoS One. 2020;15(1):e0227542. doi:10.1371/journal.pone.0227542
28. Tilahun H, Fekadu B, Abdisa H, et al. Ethiopia’s health extension workers use of work time on duty: time and motion study. Health Policy Plan. 2017;32(3):320–328. doi:10.1093/heapol/czw129
29. FMOH: Health service extension programme. Draft implementation guideline. Addis Ababa; January, 2005.
30. Betemariam W, Damtew Z, Tesfaye C, Fesseha N, Karim AM. Effect of Ethiopia’s health development army on maternal and newborn health care practices: a multi-level cross-sectional analysis. Ann Glob Health. 2017;83(1):24. doi:10.1016/j.aogh.2017.03.051
31. Damtew ZA, Karim AM, Chekagn CT, et al. Correlates of the Women’s Development Army strategy implementation strength with household reproductive, maternal, newborn and child healthcare practices: a cross-sectional study in four regions of Ethiopia. BMC Pregnancy Childbirth. 2018;18(1):373. doi:10.1186/s12884-018-1975-y
32. Rieger M, Wagner N, Mebratie A, Alemu G, Bedi A. The impact of the Ethiopian health extension program and health development army on maternal mortality: a synthetic control approach. Soc Sci Med. 2019;232:374–381. doi:10.1016/j.socscimed.2019.05.037
33. Woldie M, Feyissa G, Alaro T, et al. Community health volunteers as mediators of accessible, responsive and resilient community health systems: lessons from the Health Development Army in Ethiopia Development Army in Ethiopia; 2016.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.