Back to Journals » Patient Preference and Adherence » Volume 16
Barriers and Solutions to Improve Therapeutic Adherence from the Perspective of Primary Care and Hospital-Based Physicians
Authors Carratalá-Munuera C, Cortés-Castell E ![]() , Márquez-Contreras E
, Márquez-Contreras E ![]() , Castellano JM, Perez-Paramo M, López-Pineda A
, Castellano JM, Perez-Paramo M, López-Pineda A ![]() , Gil-Guillen VF
, Gil-Guillen VF
Received 20 May 2021
Accepted for publication 3 July 2021
Published 11 March 2022 Volume 2022:16 Pages 697—707
DOI https://doi.org/10.2147/PPA.S319084
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Concepción Carratalá-Munuera,1 Ernesto Cortés-Castell,2 Emilio Márquez-Contreras,3 José Maria Castellano,4,5 María Perez-Paramo,6 Adriana López-Pineda,1 Vicente F Gil-Guillen1
1Department of Clinical Medicine, Miguel Hernandez University, San Juan de Alicante, Spain; 2Department of Pharmacology, Pediatrics, and Organic Chemistry, Miguel Hernandez University, San Juan de Alicante, Spain; 3Primary Health Center of Molino de la Vega, Huelva, Spain; 4Centro Nacional de Investigaciones Cardiovasculares Carlos III (CNIC), Madrid, Spain; 5Centro Integral de Enfermedades Cardiovasculares (CIEC), Hospital Universitario Monteprincipe, Grupo HM Hospitales, Madrid, Spain; 6Medical Department, Pfizer GEP SLU, Madrid, Spain
Correspondence: Adriana López-Pineda, Miguel Hernandez University, Ctra. Nnal. 332 Alicante-Valencia s/n, San Juan de Alicante, 03550, Spain, Tel +1 34 965919309, Email [email protected]
Purpose: To identify the barriers affecting treatment adherence in patients with chronic disease and to determine solutions through the physician’s opinion of primary care and hospital settings.
Methods: An observational study using the nominal group technique was performed to reach a consensus from experts. A structured face-to-face group discussion was carried out with physicians with more than 10 years of experience in the subject of treatment adherence/compliance in either the primary care setting or the hospital setting. The experts individually rated a list of questions using the Likert scale and prioritized the top 10 questions to identify barriers and seek solutions afterward. The top 10 questions that obtained the maximum score for both groups of experts were prioritized. During the final discussion group, participating experts analyzed the prioritized items and debated on each problem to reach consensual solutions for improvement.
Results: A total of 17 professionals experts participated in the study, nine of them were from a primary care setting. In the expert group from the primary care setting, the proposed solution for the barrier identified as the highest priority was to simplify treatments, measure adherence and review medication. In the expert group from the hospital setting, the proposed solution for the barrier identified as the highest priority was training on motivational clinical interviews for healthcare workers undergraduate and postgraduate education. Finally, the expert participants proposed implementing an improvement plan with eight key ideas.
Conclusion: A consensual improvement plan to facilitate the control of therapeutic adherence in patients with chronic disease was developed, taking into account expert physicians’ opinions from primary care and hospital settings about barriers and solutions to address therapeutic adherence in patients with chronic disease.
Keywords: treatment adherence and compliance, chronic disease, general practitioners, family practice, hospital medicine, consensus
Introduction
The concept of therapeutic adherence1 refers to the degree to which a person’s behavior, in terms of taking medication, following a diet, and making lifestyle changes, corresponds to the agreed upon recommendations of a healthcare provider. Poor therapeutic adherence occurs when there is no congruence between the above mentioned behavior of the person and the recommendations prescribed by the healthcare professional.2–4 This new term moves away from the paternalistic view of the relationship between the healthcare professional and the patient, associated with the concept of adherence, and includes the responsibility of the healthcare provider.
Currently, poor therapeutic adherence5,6 is the cause for the failure of many treatments, and entails serious problems in terms of quality of life for patients with chronic diseases, as well as costs for the healthcare system, also contributing to the failure to achieve positive clinical results.7 That is why the World Health Organization (WHO)7 considers poor therapeutic adherence and its negative clinical and economic consequences a top-priority issue in public health.
It is estimated that, in developed countries, the adherence rate for long-term treatments is 40–50%, while for short-term treatment it is 70–80%. Moreover, regarding health-dietary measures, the adherence rate is only 20–30%.4,8 In developing countries, it is assumed that the magnitude and impact of poor adherence are even greater, given the scarcity of healthcare resources and inequities in access to healthcare.3
Poor therapeutic adherence is a multidimensional phenomenon that is determined by five factors: socioeconomic factors, healthcare-system related factors, patient-related factors, treatment-related factors and disease-related factors.9,10 Overall, simple forgetfulness on the part of the patient is the most frequent cause of poor therapeutic adherence.8,11,12
Patient adherence with therapeutic regimens may be influenced by subjective beliefs about chronic disease.13,14 One of the challenges for healthcare professionals in improving adherence is to take into account the perception and knowledge that patients have about their disease and how well they understand the disease, with regard to both health education and medical treatment.
Assessment of therapeutic adherence is necessary for planning effective and efficient treatments. Haynes and Sackett1 were the first to study the concept of therapeutic adherence and its measurement. This was the starting point of this concept, as well as the interest in studying methods to quantify it. Since then, numerous methods for measuring adherence have been described in scientific literature, which can be classified as direct and indirect.3,7,8 Despite this, no measurement strategy has been considered optimal on its own, therefore multiple strategies that combine reasonable objective measures and self-reporting are required.
Poor therapeutic adherence is a serious problem for properly approaching chronic patients in our healthcare system.15 This is due to the existence of a series of barriers that healthcare professionals encounter in their daily clinical practice that make it difficult to integrate protocols for therapeutic adherence for patients with low or no adherence. Although the identification of barriers and possible solutions to treatment adherence have been the focus of many previous research studies, the management of non-adherence has not still been consensually defined.16 Previous qualitative studies have been carried out considering a specific condition or a stakeholder, such as patients, physicians, nurses or pharmacists. However, to explore the therapeutic adherence from the joint perspective of primary care physicians and hospital-based physicians could help to implement improvement plans aimed at facilitating the integration of adherence protocols between medical professionals. The present study aimed to identify the barriers that affect adherence in patients with chronic disease and to determine solutions from primary care and hospital settings.
Methods
This was an observational study using the nominal group technique17 as a qualitative research tool. This is a consensus method used in research to solve problems, create ideas and set priorities, and consists in a structured face-to-face group discussion with experts. The criteria for selecting the participating experts was to have more than 10 years of experience in the subject of treatment adherence/compliance in either the primary care setting or the hospital setting. Two groups of participants were formed: one group of primary care physicians (PCP) and a second group of specialists in cardiology, pulmonology, internal medicine, geriatrics, psychiatry, pain unit and clinical pharmacology. All professionals received an invitation letter and provided written consent before participating. This study was reviewed by the responsible research office of Miguel Hernandez University. Ethical approval was not required because patient data was not included in this study.
One researcher was the facilitator for discussion groups, ie the person who guided the group and ensured that the objectives of nominal group technique were met effectively. This qualitative study consisted of three discussion sessions on different days between November 2019 and January 2020: a first session with the PCP group, a second session with only hospital-based physicians (HBP) and, a third session with both groups of participants. In the first and second sessions, expert participants were invited to respond individually to a series of questions or items established by the research team. Individually and silently, each expert wrote their ideas about each question. For this, they had a maximum of 10 minutes. Then, each participant presented their ideas to the rest of the group (maximum 15 minutes per presentation) and all the members of the discussion group debated solutions. Finally, each expert rated the priorities and ideas. Discussions were held in Spanish language and no translation was needed. All the group discussions were recorded and transcribed by the researchers.
A questionnaire for the discussion group was developed by the research team using the most recent literature and the experience of the researchers. The proposed questionnaire consisted of 29 questions, divided into seven topics: General, Training, Patient, Structure and Healthcare, Treatments, Disease and Socio-health Environment (Supplementary Data). The experts had to individually rate the proposed items and prioritize the top 10 questions to identify barriers and seek solutions afterward. In the event of a tie, the assessment was repeated. The highest rated proposals/ideas were selected in the end. The questions were rated using the Likert scale, with the participants giving each one a value ranging from “Not at all, disagree” = 1 point, to “Completely agree” = 5 points. The top 10 questions that obtained the maximum score for both groups of experts were prioritized.
In the third session, both PCPs and HBPs analyzed the items selected or prioritized by both groups of experts in the first two sessions, interacting in a structured debate on each individual problem that was prioritized, in order to reach consensual solutions or opportunities for improvement. Figure 1 shows how this nominal group session was conducted. This technique also took into account the minority positions. All the members of the groups participated, ensuring that the success of the ideas was not dependent on the overbearing presentation of a few members, thus promoting balance and seeking consensus.
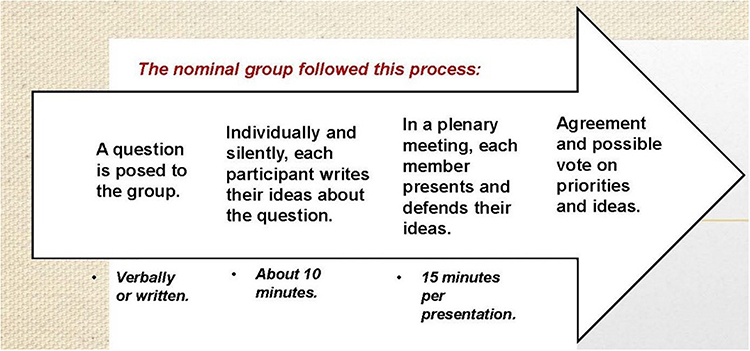 |
Figure 1 Nominal group process. |
Results
A total of 17 professionals participated in this study, of which nine were primary care physicians (PCP group) and eight were hospital-based physicians (HBP group). Tables 1 and 2 show the results of the prioritization of the 10 top-scoring questions out of the 29 questions raised (Annex 1) by the two groups of experts, in order to identify barriers. The maximum score that a question could receive for the PCP group was 45 points, since there were nine experts in the nominal group of primary care physicians; and the maximum score for the HBP group was 40, since this group had eight experts.
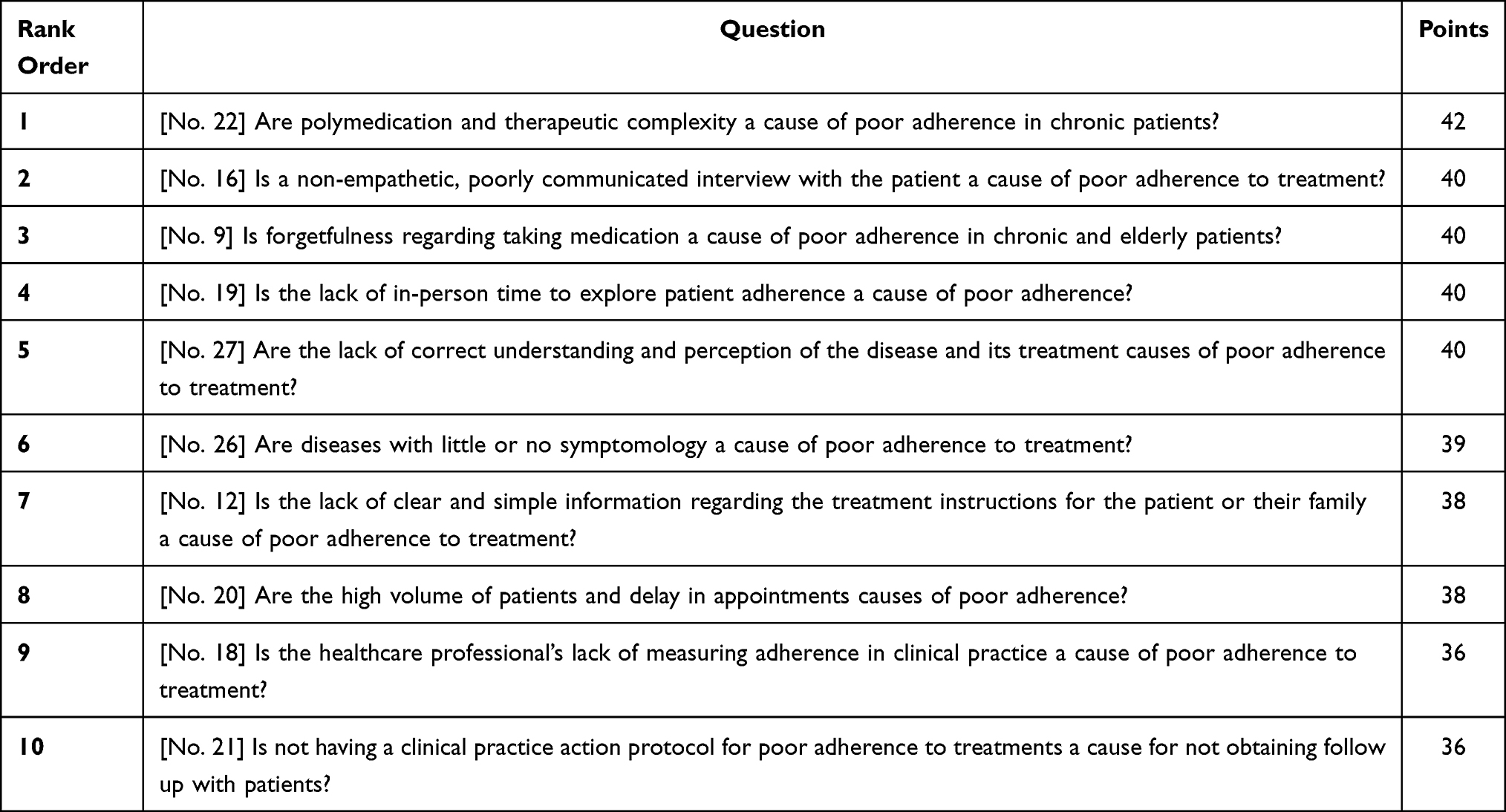 |
Table 1 Order of Priority of the Ten Highest Scoring Questions to Identify Barriers from the Primary Care Physician Group |
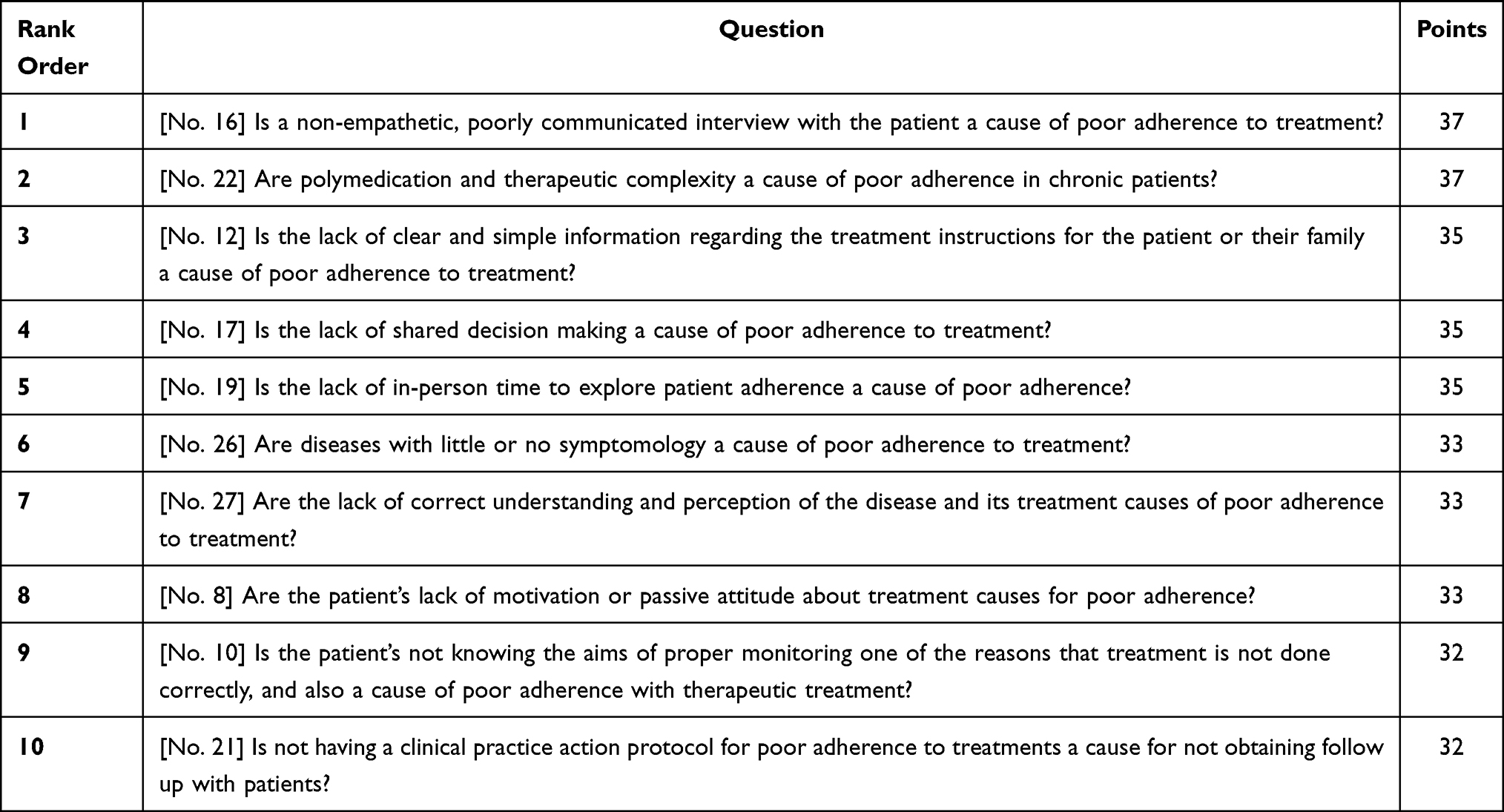 |
Table 2 Order of Priority of the Ten Highest Scoring Questions to Identify Barriers from the Hospital-Based Physician Group |
It is noteworthy that, in the PCP group, the highest score obtained was 42 points on question 22 (“Are polymedication and therapeutic complexity a cause of poor adherence in chronic patients?”) and the second place question was question 16 (“Is a non-empathetic, poorly communicated interview with the patient a cause of poor adherence to treatment?”) with 40 points; while in the HBP group, the first place question was question 16 with a score of 37 points, and second place was question 22, also with 37 points; although in the individual rating, the highest rated question was question 16. Three questions were identified as priority barriers only by the PCP group: question 9, from the Patient topic (“Is forgetfulness regarding taking medication a cause of poor adherence in chronic and elderly patients?”), and questions 20 (“Are the high volume of patients and delay in appointments causes of poor adherence?”) and 18 (“Is the healthcare professional’s lack of measuring adherence in clinical practice a cause of poor adherence to treatment?”), from the Healthcare Structure topic. Other three questions were identified as priority barriers only by the HBP group: questions 17 (“Is the lack of shared decision making a cause of poor adherence to treatment?”), 8 (“Are the patient’s lack of motivation or passive attitude about treatment causes for poor adherence?”) and 10
(Is the patient’s not knowing the aims of proper monitoring one of the reasons that treatment is not done correctly, and also a cause of poor adherence with therapeutic treatment?)
also from the Healthcare Structure and Patient topics (Tables 1 and 2). It is noteworthy that question 21 (“Is not having a clinical practice action protocol for poor adherence to treatments a cause for not obtaining follow up with patients?”), with 36 points in the PCP group and 32 points in the HBP group, was prioritized in last (tenth) place in both groups of experts.
The results obtained for identifying 10 barriers and 10 solutions prioritized by both groups of PCP and HBP experts are shown in Tables 3 and 4, in order starting with the highest score given on the questionnaire for identifying possible causes of poor therapeutic adherence. In the PCP group, the proposed solution for the barrier identified as the highest priority (question no. 22) was to simplify treatments, measure adherence and review medication (Table 3). In the HBP group, the proposed solution for the barrier identified as the highest priority (question no. 16) was training on motivational clinical interviews for healthcare workers undergraduate and postgraduate education (Table 4).
 |
Table 3 Items Identified as Barriers and Their Solutions, Prioritized by Primary Care Physicians |
 |
Table 4 Items Identified as Barriers and Their Solutions, Prioritized by Hospital-Based Physicians |
Finally, during the third session of nominal group, the expert participants proposed implementing an improvement plan with eight key ideas, in order to foster therapeutic adherence in patients with chronic diseases, from clinical practice. This plan was drawn up based on the barriers and solutions for better control of therapeutic adherence that were identified by the groups of primary care experts and hospital-based experts (Table 5).
 |
Table 5 Improvement Plan: Facilitating Control of Therapeutic Adherence in Patients with Chronic Disease |
Discussion
The present study allowed identifying barriers and solutions to address therapeutic adherence in patients with chronic disease from the perspective of primary care and hospital-based physicians. There were some differences between the results of the nominal group session with PCP and those of the session with only HBP. However, they managed to develop a consensual improvement plan to facilitate the control of therapeutic adherence in patients with chronic disease.
Regarding the obtained results, several issues were cause for great discussion in the meeting with both groups of experts. Question 9, “Is the healthcare professional’s lack of measuring adherence in clinical practice a cause of poor adherence to treatment?”, was in fourth place with 40 points in the PCP group, and was only identified by primary care professionals, possibly because hospital-based physicians have a different point of view of forgetfulness when it comes to taking medications. A systematic review published in 2018 by Zaugg et al,18 had the aim of evaluating the effects of providing doctors’ comments on adherence with medication to their patients to improve adherence, since it seems that, sometimes, hospital-based physicians tend to overestimate patients taking their medications as prescribed. This could lead to lost opportunities for changing medications, resolving side effects or proposing the use of reminders to improve adherence in patients. Therefore, doctors providing feedback on adherence with medications has the potential to bring about changes that improve patients’ adherence with prescribed medications. In general, primary care physicians have more feedback with their patients since they have longitudinal appointments over the life of the patient, taking into account their social environment, whether they live alone, whether the patient is socially fragile, etc., which means they have a more holistic point of view of the problem of poor adherence with long-term treatments.19,20
Forgetfulness is one of the largest causes for poor adherence, and there are many publications and clinical practice guides based on the evidence related to the topic of forgetfulness in poor adherence in chronic pathologies. Mahtani et al21 concluded that patients with chronic pathologies often do not take their medications properly due to forgetfulness, changes in the times at which the medication must be taken, or due to lifestyle. It is estimated that between 40% and 60% of people with chronic pathologies have at least some lack of adherence with their drug treatments, which can lead to worse health conditions.
The objective of the FOCUS22 study was to analyze the factors that interfere with correct adherence with cardiovascular treatments for secondary prevention after acute myocardial infarction. It concluded that the use of combination therapy (multiple medications in one pill) strategy fulfilled the principal evaluation criteria of adherence with secondary prevention after acute myocardial infarction.
The guide of the National Institute for Health and Clinical Excellence (NICE)23 recommends taking into account the patient’s wishes to take less medication, asking them about their concerns regarding the medication (side effects or risk of dependence), and talking to them about how to incorporate taking the medication into their daily lives.
Question 20, “Are the high volumes of patients and delay in appointments causes of poor adherence?”, was only prioritized by the PCP expert group, and the solution that they proposed is to teach healthcare professionals to properly manage and prioritize or limit appointments. They also suggested enhancing clinical management of appointments/clinical self-management in PCP and also creating agreements between different levels of doctors regarding standard care, based on patients with chronic pathologies. A study published in 2019 by Freixa-Pamias et al24 had the goal of analyzing a clinical management model which integrated cardiology and primary care in the clinical practice. In this new clinical management model with integrated attention, each cardiologist was assigned a primary care center and improved coordination was observed between the different levels of medical attention.
Question 18, “Is the healthcare professional’s lack of measuring adherence in clinical practice a cause of poor adherence to treatment?”, was only identified by the PCP group. The solution proposed by this group of experts is to include a tool for measuring adherence in electronic medical history charts. In a study conducted by Mabotuwana et al25 the objective of which was to analyze patterns in electronic prescriptions in electronic medical records and their capacity to detect cohorts of patients with significant adherence problems, it was observed that non-adherent patients, ie medication possession rate < 80% or lapse of > 30 days, are three times more likely to have poor control of their blood pressure goals. It was concluded that the development of a generic computerized framework of medical histories would be useful for formulating and consulting criteria based on long-term medication adherence issues. The levels of adherence observed indicated that a substantial proportion of patients classified with high blood pressure and diabetes had poor adherence associated with lower rates of blood pressure monitoring, which can be detected by an analysis of electronic prescriptions in computerized medical histories.
Question 17, “Is the lack of shared decision making a cause of poor adherence to treatment?”, was only identified by the HBP group. The solution they proposed is to negotiate the manner of taking the treatment with the patient, and follow up. They also suggested involving the family or caregiver, being empathetic with the patient and performing positive reinforcement regarding possible fears that their disease and treatment may cause (Table 4).
Question 21, “Is not having a clinical practice action protocol for poor adherence to treatments a cause for not obtaining follow up with patients?”, had 36 points in the PCP group and 32 points in the HBP group. Both groups selected this as a barrier. The solution proposed by the hospital experts is to identify non-compliant or non-adherent patients based on whether or not they picked up their medication from the pharmacy, and to perform a study to identify the causes and establish intervention strategies. This solution aligns with several articles published, such as one by Warren et al.26 This study looked at the effectiveness of follow up by primary care professionals guided by computerized medical history data to improve adherence medication. The results obtained were an improvement in adherence and good monitoring of patients that received the intervention, and that this is feasible, since it was well-received and well-accepted by the patients. Regarding the primary care expert group, the solution they proposed for this barrier was to create a protocol that integrates all the measures proposed at the meeting.
A study published in October 2019 by Carvalho et al27 reviewed literature on medication adherence in patients with high blood pressure and their relationship with the organizational factors of health standards. The authors concluded that non-adherence to medication treatment is a real problem today, and it depends on the interaction of factors related to the patient, providers, and the surrounding context. The role of the physician is not only to prescribe, but also to address all the aspects of the patient to comprehend the best strategy for each person individually. Promoting adherence is as important for the health of the population as the act of prescribing medication. This is explained by the fact that therapeutic adherence is a multi-faceted phenomenon that is determined by factors that go beyond the healthcare setting.3,5 Therefore, being aware of the factors that influence patient adherence to treatment is very important for overcoming therapeutic non-compliance.28,29
The study findings revealed that physicians from different settings have different opinion about the therapeutic adherence. The improvement plan that arose from the consensus between physicians from both settings might lead to the correct management of non-adherence in patients with chronic disease. The use of the nominal group technique as a consensus method allowed generating ideas related to problems and solutions of therapeutic adherence in chronic patients. However, as this method requires face-to-face meetings, some expert participants could have felt uncomfortable to contribute their views or discuss the opinion of another participant. This limitation was addressed through the facilitator who made easy the process by creating a comfortable environment. In addition, the study findings are only based on the perspective of physicians. A future study using the Delphi method and including different healthcare providers and patients will be conducted to develop strategic actions to improve therapeutic adherence in patients with chronic disease.
In conclusion, the polymedication and a poorly communicated interview with the patient were identified as possible causes of poor treatment adherence by both groups. PCP and HBP prioritized different causes and solutions of adherence. However, they achieved to develop an improvement plan to facilitate the control of therapeutic adherence in patients with chronic disease.
Acknowledgments
We thank to the collaborative working group: Carmen Valdés y Llorca, Centro de Salud de Fuencarral, Madrid. Jacinto Espinosa García, Centro de Salud Villanueva de la Serena-Norte, Badajoz. Carlos Brotons Cuixart, Equipo de Atención Primaria Sardenya, Barcelona. Mariano de la Figuera, Equipo de Atención Primaria Sardenya, Barcelona. Enrique Martín Rioboó, Centro de Salud Fuensanta, Córdoba. Juan Antonio Divisón Garrote, Centro de Salud Fuentealbilla, Albacete. Francisco Ponce Lorenzo – Hospital Virgen del Castillo, Yecla, Murcia. José Manuel Ribera Casado, Universidad Complutense de Madrid. Nieves Martell, Hospital Clínico San Carlos. Madrid. Pedro Zapater Hernández, Hospital San Juan. Alicante. Juan Manuel Arriero Marín, Hospital General Universitario de Alicante. Olga Brotons, Hospital General Universitario de Elche, Germán Cerdá Olmedo, Universidad Católica de Valencia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Haynes RB, Taylor DW, Sackett DL, Gibson ES, Bernholz CD, Mukherjee J. Can simple clinical measurements detect patient noncompliance? Hypertension. 1980;2(6):757–764. doi:10.1161/01.HYP.2.6.757
2. Laufs U, Rettig-Ewen V, Böhm M. Strategies to improve drug adherence. Eur Heart J. 2011;32(3):264–268. doi:10.1093/eurheartj/ehq297
3. World Health Organization. Adherence to long-term therapies: evidence for action. Washington D.C.: World Health Organization; 2003. Available from: https://www.who.int/chp/knowledge/publications/adherence_report/en/.
4. Jin J, Sklar GE, Min Sen Oh V, Chuen LS. Factors affecting therapeutic compliance: a review from the patient’s perspective. Ther Clin Risk Manag. 2008;4(1):269–286. doi:10.2147/TCRM.S1458
5. Nieuwlaat R, Wilczynski N, Navarro T, et al. Interventions for enhancing medication adherence. Cochrane Database Syst Rev. 2014;11:CD000011.
6. Conn VS, Ruppar TM, Chase JD. Blood pressure outcomes of medication adherence interventions: systematic review and meta-analysis. J Behav Med. 2016;39(6):
7. Rodríguez Chamorro MA, García Jiménez E, Amariles P, Rodríguez Chamorro A, Faus MJ. Revisión de tests de medición del cumplimiento terapéutico utilizados en la práctica clínica. [Review of the measurement tests for therapeutic compliance used in clinical practice]. Aten Primaria. 2008;40(8):413–417. doi:10.1157/13125407
8. Márquez Contreras E, Gil Guillén V, Casado Martínez JJ, et al. Analysis of studies published on hypertension treatment non-compliance in Spain between 1984 and 2005. Aten Primaria. 2006;38(6):325–332. doi:10.1157/13093369
9. Seng JJB, Tan JY, Yeam CT, Htay H, Foo WYM. Factors affecting medication adherence among pre-dialysis chronic kidney disease patients: a systematic review and meta-analysis of literature. Int Urol Nephrol. 2020;52(5):903–916. doi:10.1007/s11255-020-02452-8
10. Yeam CT, Chia S, Tan HCC, Kwan YH, Fong W, Seng JJB. A systematic review of factors affecting medication adherence among patients with osteoporosis. Osteoporos Int. 2018;29(12):2623–2637. doi:10.1007/s00198-018-4759-3
11. Conn VS, Ruppar TM. Medication adherence outcomes of 771 intervention trials: systematic review and meta-analysis. Prev Med. 2017;99:
12. Rafii F, Fatemi NS, Danielson E, Johansson CM, Modanloo M. Compliance to treatment in patients with chronic illness: a concept exploration. Iran J Nurs Midwifery Res. 2014;19(2):159–167.
13. Shahin W, Stupans I, Kennedy G. Health beliefs and chronic illnesses of refugees: a systematic review. Ethn Health. 2018;11:1–13. doi:10.1080/13557858.2018.1557118
14. Shahin W, Kennedy GA, Stupans I. The impact of personal and cultural beliefs on medication adherence of patients with chronic illnesses: a systematic review. Patient Prefer Adherence. 2019;13:
15. Simpson SH, Eurich DT, Majumdar SR, et al. A meta-analysis of the association between adherence to drug therapy and mortality. Br Med J. 2006;333(7557):15. doi:10.1136/bmj.38875.675486.55
16. Hameed MA, Dasgupta I. Medication adherence and treatment-resistant hypertension: a review. Drugs Context. 2019;8:212560. doi:10.7573/dic.212560
17. Miguel VS. Técnicas cualitativas de investigación social. Reflexión metodológica y práctica profesional. [Qualitative techniques of social research. Methodological reflection and professional practice].
18. Zaugg V, Korb‐Savoldelli V, Durieux P, Sabatier B. Providing physicians with feedback on medication adherence for people with chronic diseases taking long‐term medication. Cochrane Database Syst Rev. 2018;2018(1). doi:10.1002/14651858.CD012042.pub2
19. Carratalá-Munuera MC, Gil-Guillén VF, Orozco-Beltrán D, et al. Barriers associated with poor control in Spanish diabetic patients. A consensus study. Int J Clin Pract. 2013;67(9):888–894. doi:10.1111/ijcp.12160
20. Ladova K, Vlcek J, Vytrisalova M, Maly J. Healthy adherer effect - the pitfall in the interpretation of the effect of medication adherence on health outcomes. J Eval Clin Pract. 2014;20(2):111–116. doi:10.1111/jep.12095
21. Mahtani KR, Heneghan CJ, Glasziou PP, Perera R. Reminder packaging for improving adherence to self‐administered long‐term medications. Cochrane Database Syst Rev. 2011;9. doi:10.1002/14651858.CD005025.pub3
22. Castellano JM, Sanz G, Peñalvo JL, et al. A polypill strategy to improve adherence: results from the FOCUS project. J Am Coll Cardiol. 2014;64(20):2071–2082. doi:10.1016/j.jacc.2014.08.021
23. National Institute for Health and Clinical Excellence. Medicines adherence: involving patients in decisions about prescribed medicines and supporting adherence. Clinical guideline 76; 28 January 2009. Available from: https://www.nice.org.uk/guidance/cg76.
24. Freixa-Pamias R, Gràcia PB, Rodríguez Latre ML, et al. Impact of an integral assistance model between primary care and cardiology on the management of patients with ischemic heart disease or atrial fibrillation. J Comp Eff Res. 2019;8(2):
25. Mabotuwana T, Warren J, Kennelly J. A computational framework to identify patients with poor adherence to blood pressure lowering medication. Int J Med Inform. 2009;78(11):745–756. doi:10.1016/j.ijmedinf.2009.06.006
26. Warren J, Kennelly J, Warren D, et al. Using the general practice EMR for improving blood pressure medication adherence. Stud Health Technol Inform. 2012;178:228–234.
27. Carvalho AS, Santos P. medication adherence in patients with arterial hypertension: the relationship with healthcare systems’ organizational factors. Patient Prefer Adherence. 2019;13:1761–1774. doi:10.2147/PPA.S216091
28. Carratala-Munuera C, Gil-Guillen VF, Orozco-Beltran D, et al. Barriers to improved dyslipidemia control: delphi survey of a multidisciplinary panel. Fam Pract. 2015;32(6):672–680. doi:10.1093/fampra/cmv038
29. Ministerio de Sanidad, Servicios Sociales e Igualdad. Estrategia para el abordaje de la cronicidad en el Sistema Nacional de Salud. [Strategy for addressing chronicity in the National Health System]. Madrid: Ministerio de Sanidad, Servicios Sociales e Igualdad; 2012. Available from: https://www.mscbs.gob.es/organizacion/sns/planCalidadSNS/pdf/ESTRATEGIA_ABORDAJE_CRONICIDAD.pdf.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.