Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Barriers and Facilitators for Smoking Cessation in Chinese Smokers with Chronic Obstructive Pulmonary Disease: A Qualitative Study
Authors Zhang YY, Tang WT, Zhang H, Wang J, Bai XX, Liao YH, Robinson N ![]() , Liu JP
, Liu JP ![]()
Received 11 January 2022
Accepted for publication 28 March 2022
Published 6 May 2022 Volume 2022:17 Pages 1107—1120
DOI https://doi.org/10.2147/COPD.S356935
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Ying-Ying Zhang,1 Wen-Tao Tang,2 Hong Zhang,3 Jing Wang,3 Xiao-Xu Bai,3 Yan-Hui Liao,4 Nicola Robinson,1,5 Jian-Ping Liu1
1Centre for Evidence-Based Chinese Medicine, Beijing University of Chinese Medicine, Beijing, 100029, People’s Republic of China; 2Pingyi Hospital of Traditional Chinese Medicine, Linyi, Shandong, People’s Republic of China; 3Fangshan Hospital of Traditional Chinese Medicine Affiliated to Beijing University of Chinese Medicine, Beijing, People’s Republic of China; 4Department of Psychiatry, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, 310016, People’s Republic of China; 5Institute of Health and Social Care, London South Bank University, London, UK
Correspondence: Jian-Ping Liu, Centre for Evidence-Based Chinese Medicine, Beijing University of Chinese Medicine, 11 Bei San Huan Dong Lu, Chaoyang District, Beijing, 100029, People’s Republic of China, Email [email protected]; [email protected]
Background: Smoking cessation is recommended as a key intervention for chronic obstructive pulmonary disease (COPD) smokers. However, in China, few COPD smokers quit successfully. The aim of this study was to explore in depth the barriers and facilitators for smoking cessation among smokers with COPD in China.
Methods: A purposive sample of 32 hospitalized smokers with COPD were included, 17 ex-smokers and 15 current smokers, participated in the semi-structured interviews. Interviews were analyzed thematically and using a deductive approach guided by Capability, Opportunity, Motivation-Behavior (COM-B) framework.
Results: Three inter-related themes were generated: smokers’ motivation was a prerequisite for quitting, maintaining capability to quit smoking, and opportunities that facilitated smokers to quit. Motivation to quit for most participants was activated by COPD-related symptoms, although they had a limited knowledge of COPD. Physical benefits from quitting and strong willpower were facilitators for maintaining quitting, while exposure to smoking environment and strong addiction to nicotine were frequent reasons for relapse. Most ex-smokers quit smoking by their own willpower rather than professionally delivered smoking cessation interventions. Smokers’ attitudes toward these interventions depended on their effectiveness and convenience. Very few participants had experienced pharmacotherapy or behavioral support from physicians. However, interviewees preferred auricular acupressure to pharmacotherapy.
Conclusion: Motivation to quit among smokers with COPD was usually initiated by COPD-related symptoms. Physical benefits observed by quitting and strong willpower facilitated smoking cessation, while exposure to smoking environment and strong addiction to nicotine led to relapse. COPD smokers in China preferred auricular acupressure to pharmacotherapy.
Keywords: chronic obstructive pulmonary disease, smoking cessation, tobacco, qualitative research, acupuncture
Background
Smoking remains a global public health issue. More than 480,000 people die prematurely each year, and one-fifth of premature deaths are related to cigarette smoking.1 Smoking is closely related to the occurrence and development of chronic obstructive pulmonary disease (COPD).2 The GBD study in 2019 reported that of 369 diseases and injuries globally, COPD was the sixth leading cause of death and for people aged 50–74, COPD was the fourth most common cause of death.3 Reports suggest that the prevalence of COPD is as high as 11.7% worldwide, and it is expected that this will be as high as 4.5 million people dying of COPD each year by 2030.4 COPD is a chronic respiratory disease, mainly manifesting as recurrent cough, expectoration, breathlessness, chest tightness and wheezing. The pathological changes include chronic inflammation, with increased numbers of specific inflammatory cell types in the lung, and structural changes caused by repeated injury and repair.5 Narrowing and inflammation of peripheral airways results in decreased FEV16, in addition to the narrowing of the airways, there is also a loss of small airways, and which may lead to airflow limitation.7 This impacts significantly on patients’ quality of life due to persistent symptoms or acute exacerbations. According to the pyramid of value for COPD interventions in the British Thoracic Society report in 2012, flu vaccination was considered as the most valuable therapy for patients at a risk of COPD.8
However, for patients diagnosed with COPD, smoking is a major risk factor for COPD.2 Smoking cessation in patients with COPD can effectively reduce the risk of death by 32–84%,9 relieve respiratory symptoms, and reduce the number of acute exacerbations, and therefore smoking cessation intervention should be implemented through the entire COPD process.10 Guidelines recommend that smoking cessation should be the primary evidence-based intervention for patients with COPD.11–13
However, smoking cessation in patients with COPD differs from general smokers. A study in 2006 suggested that between 30.4% and 40.3% patients with moderate or severe COPD were current smokers,14 but they had not received any additional smoking cessation advice or pharmacotherapy than general smokers.15 Moreover, COPD patients usually have a higher nicotine dependence, but their willingness to quit does not increase correspondingly.16 Although studies suggested that COPD-related symptoms or exacerbations motivated patients to stop smoking,17,18 previous studies have also found that smokers with COPD abroad had more difficulties in quitting than non-COPD smokers as they had been smoking cigarettes for a longer time and they exhibited lower self-efficacy.19 Currently, the recommended interventions for smoking cessation mainly include behavioral support, pharmacotherapy, and complementary and alternative therapies.20 The approved pharmacotherapies for smoking cessation are nicotine replacement therapy (NRT) includes nicotine patches or chewing gum, bupropion, and varenicline. However, studies have founded that about 20% smokers failed to use pharmacotherapies to aid smoking cessation as the doctor prescribed, often with inadequate dosage and duration.21,22 There are as many as 1 billion COPD patients in China, with a prevalence of 13.7% in people over 40 years of age, making it the third leading cause of death in China.23 A study suggested that good adherence to smoking cessation treatment could significantly improve smoking cessation efficacy in Chinese smokers with COPD.24 Therefore, poor treatment adherence also challenges the efficacy of pharmacotherapy. To make matters worse, pharmacotherapy for smoking cessation in China is not as common as they are abroad.25 Acupuncture and related interventions as complementary therapies have been also used for smoking cessation in China and abroad, including traditional transdermal needle acupuncture, acupressure which refers to continuous acupoints stimulates by seeds or acu-pellets,26,27 as well as Chinese herbal medicine external use at acupoints.28
However, only a small number of smokers with COPD achieved quitting successfully in China, and smoking cessation behavior is significantly affected by different social contexts. The aim of this study was to explore in detail using a qualitative method the barriers and facilitators for smoking cessation in Chinese smokers with COPD and which could help determine appropriate interventions and improve the likelihood of successful quitting.
Methods
Study Design
A qualitative approach was employed using semi-structured interviews which would allow participants to adequately express their feelings, attitudes, or experiences regarding smoking cessation and smoking cessation interventions. An in-depth understanding of research issues can be elicited with qualitative study design. A combination of convenience and purposive sampling was used. The Capability, Opportunity, and Motivation-Behavior (COM-B)29 framework was applied to guide the data collection and analysis. The framework hypothesizes that the interaction among individual’s capability, opportunity, and motivation changes an individual’s behavior. The reporting of the study followed the consolidated criteria for reporting qualitative research (COREQ), a checklist which ensures explicit and comprehensive reporting in qualitative studies.30
Ethical Approval
Prior to the interviews, ethical approval was granted from Ethics Committee of Beijing University of Chinese Medicine (2021BZYLL0103) and Fangshan hospital affiliated to Beijing University of Chinese Medicine (FZYLK-2021-019).
Study Sample
Study participants were recruited from patients admitted to respiratory wards in two hospitals (Fangshan and Yuehua), affiliated to Beijing University of Chinese Medicine.
The eligibility criteria were as follows: current smokers or ex-smokers, defined as: (1) current smokers who had smoked 100 cigarettes in their lifetime and currently smoked daily (“everyday” smoker) or only on some days (“some days” smoker); (2) ex-smokers who had smoked at least 100 cigarettes in their lifetime but had stopped smoking in the last 28 days at the time of the interview; (3) who were diagnosed with COPD (stage I–III) according to the GOLD guideline,11 the diagnostic criteria of COPD were dyspnea, chronic cough, sputum production, and a history of exposure to risk factors for COPD, as well as a post-bronchodilator FEV1(Forced Expiratory Volume in the first second)/FVC (Forced Vital Capacity) <0.70, and the classification of airflow limitation severity in patients with FEV1/ FVC < 0.70 was based on post-bronchodilator FEV1 as follows: FEV1≥ 80%, Stage I (Mild); 50% ≤ FEV1< 80%, Stage II (Moderate); 30% ≤ FEV1< 50%, Stage III (Severe); (4) 18–90 years of age; (5) cognitively able to participant in an interview; (6) and willing to participate and provide signed informed consent. The study sample was recruited by asking respiratory physicians and nurses to distribute electronic recruitment advertisements to hospitalized smokers with COPD, the electronic recruitment adverts were distributed to participants through WeChat group on cellphone. Male and female participants from different social backgrounds and ages, who had tried different smoking cessation methods were included to maximize the variation in our sample.
Data Collection
All the interviews were conducted by a doctoral candidate (YYZ) who was also a trained physician. The researcher and participants had never met before the interview. A brief introduction was made to the participants before the interview about the researcher, study aim, procedures for data collection, and principle of voluntary participation and the right to withdraw at any time from the study. Prior to the interview, written informed consent was obtained from all participants. An interview guideline was created followed using the COM-B framework,29 and a pilot interview was conducted before formal interview to make sure the interview guide was complete and thought-provoking. The pilot interview was conducted by YYZ and we added information of physical and mental changes after quitting smoking, and attitude towards e-cigarettes to interview guide after pilot interview. The interviews were composed of open-ended questions that encouraged the participants to talk about their feelings, experiences and preferences regarding smoking cessation in their own words. The guideline-based questions included the reasons to start smoking and understanding of the relationship between COPD and smoking; motivation to quit, quitting experiences; methods that they had undergone, and their attitude towards pharmacotherapy, behavior support, acupuncture, and e-cigarettes; knowledge of smoking cessation clinics in China, and expected smoking cessation support. The interview guide is shown in Table 1. The basic demographic questionnaire was given to every participant to fill out before interviews. Interviews were taped with a digital voice recorder, and the researcher also took notes of interviewee’s speech and body language. Interviews ceased after discussion when no new information emerged. The study’s sample was recruited at respiratory wards from two hospitals. Overall 32 smokers diagnosed with COPD participated in this interview. The interviews were conducted between June and August 2020 in independent wards in Fangshan and Yuehua hospitals which are affiliated to Beijing University of Chinese Medicine, and the duration of each interview lasted approximately 25–30 minutes.
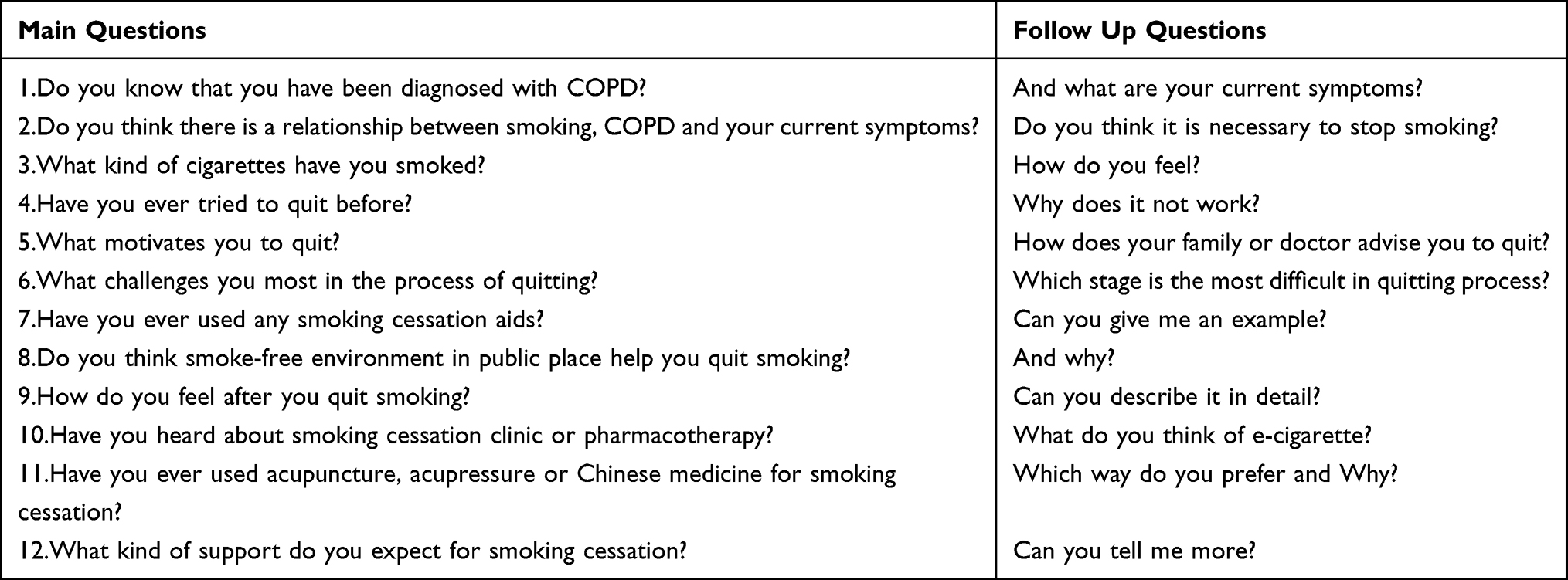 |
Table 1 Interview Guideline for Smokers with COPD on Smoking Cessation |
Data Analysis
All the interviews were recorded and transcribed by (YYZ and WTT), and WTT did not participate in the interview. We also checked the transcribed information with the notes taken by the researcher during the interview to ensure the transcribed information was complete and accurate. Any discrepancies were clarified bilaterally, and each transcript was completely anonymous. Thematic analysis was applied to analyze the data, following the procedures recommended by Braun and Clarke,31 but using a deductive method32,33 to reveal concepts and themes reflected in the COM-B framework. However, new inductive themes were also identified in the coding process. After transcription, YYZ uploaded the transcripts onto NVivo 12 software. The two researchers read and re-read the transcribed interviews to obtain the initial codes after discussion, and then the initial codes were clustered into categories and themes. Disagreements were resolved by discussion and agreement between the two researchers.
Results
Characteristics of Participants
There were 29 males and 3 females, aged 37 to 85 years, 17 ex-smokers and 15 current smokers. The history of COPD among participants varied from < 1 year to > 20 years, and 6 participants were in hospital due to an acute exacerbation of COPD, and the other 26 subjects were diagnosed with COPD stage I or II. The duration of smoking varied between 14 years and 70 years. Fourteen smokers had only used cigarettes, 11 smokers had used cigarettes and home-made tobacco, 7 were multiple users of cigarettes, home-made tobacco, and e-cigarettes. However, cigarettes were the most popular and were used for the longest time among participants, home-made tobacco was only used when participants were young, and e-cigarettes were the least commonly used and had been taken for the shortest time period. The demographic characteristics and smoking history of participants are shown in Table 2.
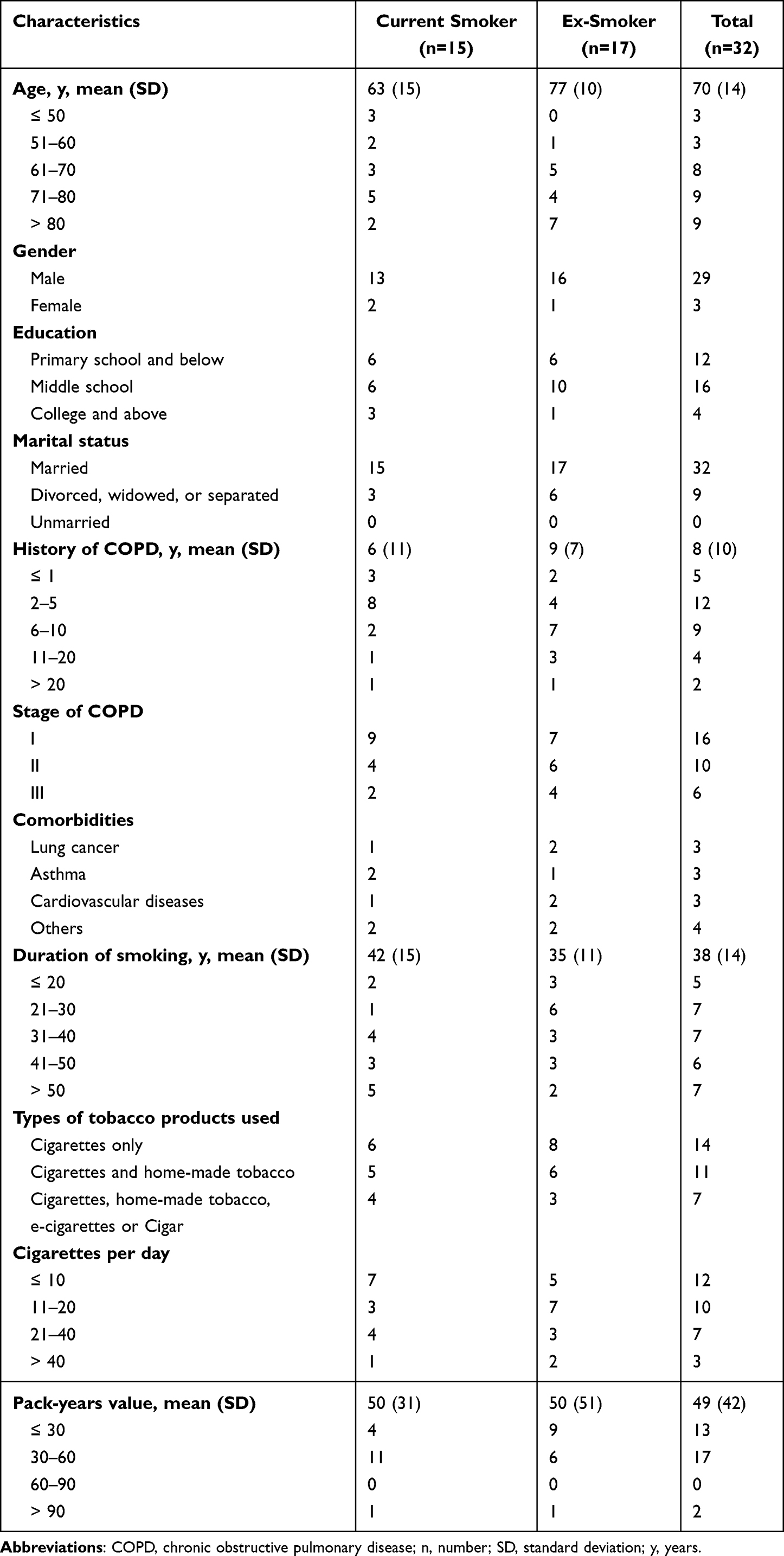 |
Table 2 Characteristics of the Included Smokers with COPD |
Themes and Categories
Twenty-seven interviews were audio recorded, the remaining 5 participants refused to be audio recorded but agreed to be recorded in writing, and YYZ took detailed field notes as far as possible. In the written informed consent form, the risk that the conversation will be recorded and that the conversation will be anonymized was explained to every participant, and every participant agreed and signed the written informed consent form. Three inter-related themes and 10 categories emerged: smokers’ automatic or reflective motivation is a prerequisite for quitting, maintaining psychological or physical capability to quit smoking, and opportunities that facilitate smokers to quit smoking. The themes and categories are shown in Table 3. The preliminary thematic map development prior to the alignment to the COM-B model is shown in Figure 1. The barriers and facilitators that influence smoking cessation behavior are shown in Figure 2.
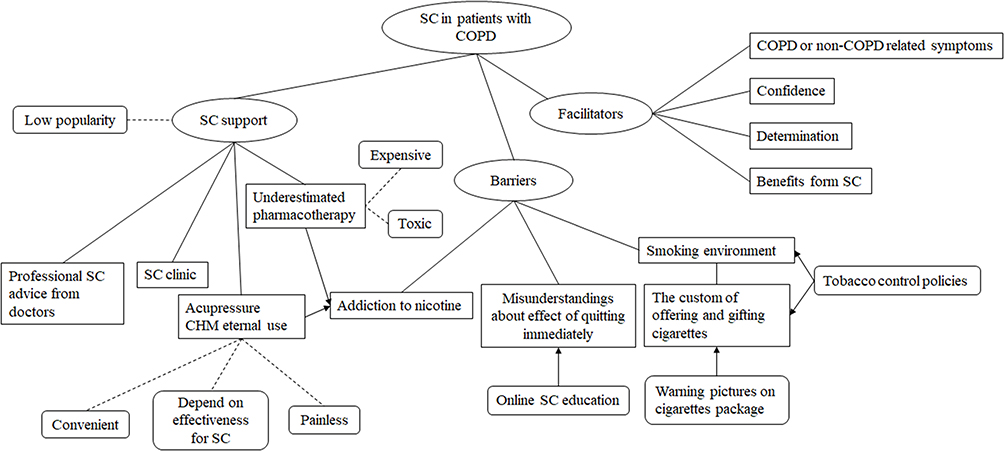 |
Figure 1 The preliminary thematic map. SC, smoking cessation; CHM, Chinese herbal medicine. |
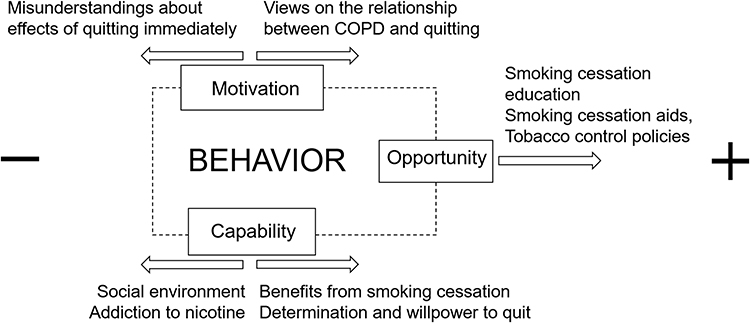 |
Figure 2 Barriers and facilitators that influence smoking cessation behavior |
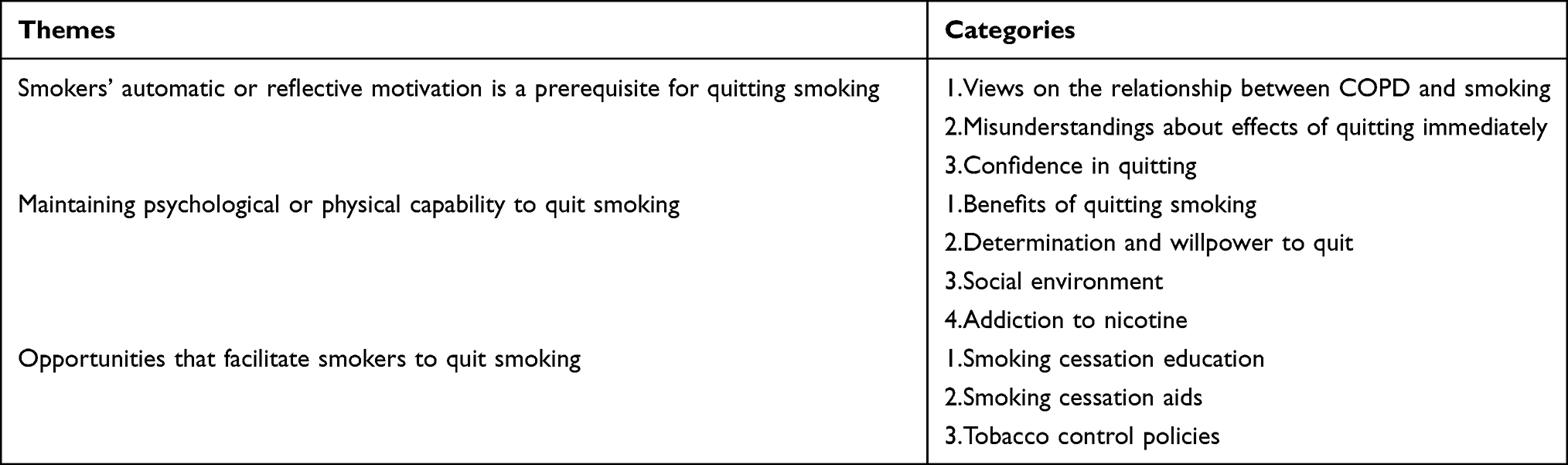 |
Table 3 The Themes and Categories Emerging from the Semi-Structured Interviews |
Theme 1:Smokers’ Automatic or Reflective Motivation is a Prerequisite for Quitting Smoking
Interviewees regardless of whether they were current smokers or ex-smokers believed that personal motivation to quit smoking was a prerequisite. Although social support or smoking cessation support may be helpful in quitting, yet they maintained that the quitting process needed to be initiated by themselves. However, their quitting motivation was closely affected by views on the relationship between COPD and smoking, misunderstandings about effects of quitting immediately, and confidence in quitting.
Only when I realized the importance to stop smoking, can I have enough motivation to find helpful ways to stop smoking; otherwise, advice from family members or doctors was useless to me (Interviewee 13; ex-smoker).
Views on the Relationship Between COPD and Smoking
The majority of participants were of lower level of education, some of them knew little about COPD. However, COPD-related symptoms or syndromes such as COPD exacerbations, recurrent cough, breathlessness and wheezing usually motivated them to stop smoking, and most participants considered that smoking was the major cause of these discomforts. Additionally, pulmonary computed tomography (CT) scans, pulmonary function test and advice from their doctors also improved quitting motivation. On the other hand, some ex-smokers stopped smoking due to non-COPD related reasons, such as surgery, coronary heart disease, and oral diseases.
Smoking induced serious cough and wheeze, and got worse especially at night. I felt that there was a “chick” in my throat and I can hear the loud chicken sounds clearly, which made me breathless and therefore I had to give up smoking (Interviewee 1; ex-smoker).
I went to a doctor for serious cough, the doctor advised me to take a lung CT screening, and I was told that there was something wrong with my lung, I needed to stop smoking, or else, I would not able to walk freely due to severe wheezing. Therefore, I followed his advice and stopped smoking (Interviewee 22; ex-smoker).
I used to be a worker and smoked heavily to relieve fatigue and boredom, however, my collarbone was broken in a work accident, the doctor managed to operate on me, so I stopped smoking in hospital since smoking would induce cough and further influence bone recovery (Interviewee 14; ex-smoker).
Misunderstandings About Effects of Quitting Immediately
Although most participants were aware of the harms of smoking, they were reluctant to give up smoking immediately due to some misunderstandings that immediate quitting led to serious disease and even death, hence, they usually reduced the consumption of cigarettes rather than quitting.
I wanted to stop smoking, but I dared not to stop immediately. It was said that for long-term smokers there were some tobacco ingredients in your blood and you were used to them, and once quitting, you would get really sick. One of my friend who smoked similar to me, and he died suddenly after stopping smoking, so I would rather cut down gradually before quitting (Interviewee 15; current smoker).
To give up smoking at once, I tried once but I cannot make it. In addition, I heard that it was very dangerous to stop smoking suddenly, I had also read some similar messages shared by my friends online (Interviewee 22; current smoker).
Confidence in Quitting
Most of current smokers with COPD had attempted to give up smoking at least once but failed, and therefore the failed experience hindered their motivation to quit again due to lack of confidence.
I tried 3 times to quit, but all my efforts ended in failure, worse still, I smoked more heavily than ever, I will never try again (Interviewee 9; current smoker).
I was getting old, I attempted to quit once but relapsed, it was terrible and I did not want to quit any more. My son usually bought expensive cigarettes for me, I thought they were less harmful (Interviewee 15; current smoker).
Theme 2: Maintaining Psychological or Physical Capability to Quit Smoking
Smoking cessation was a long-term process and maintaining the capability to quit was also challenging. Smokers who were motivated to quit had to overcome psychological or physical difficulties with strong determination and willpower in the quitting process. For example, serious nicotine addiction, and smoking environment affected this. While resolution or relief of COPD-related symptoms kept them away from cigarettes.
Benefits of Quitting Smoking
One of the important reasons for smokers who motivated to keep away from cigarettes was physical benefits perceived from quitting. Symptoms associated with COPD were relieved or disappeared after quitting. Most of ex-smokers complained serious coughing when they were exposed to secondhand smoke.
I felt better after I stopped smoking, I did not cough as usual as before and my throat did not itch anymore, surprisingly, the “chick” sound in my throat when I slept at night also disappeared (Interviewee 20; ex-smoker).
I was much more sensitive to secondhand smoke after I stopped smoking, I coughed seriously and felt very discomfort in my lungs when exposed to secondhand smoke (Interviewee 24; ex-smoker).
Determination and Willpower to Quit
Personal determination and willpower were viewed as the most important factors for successful cessation, and were determinant and decisive factors to achieve smoking cessation. Brief advice from doctors or family members was less effective than smokers’ own determination in decision-making for smoking cessation. Only when smokers have a strong determination to quit, can they stay away from cigarettes.
I thought successful quitting mainly depended on myself rather than others, if I was not determined, nobody can force me to quit. For example, I decided to give up smoking when I was chatting with a friend in a park, since then, I had never smoked (Interviewee 7; ex-smoker).
I relapsed twice because my friends shared cigarettes with me, in fact, I had a strong craving for cigarette and failed to say no to cigarettes. For the last time I attempted to quit, I tried my best to control my urge to cigarettes and refused all cigarettes from friends, and nearly one year later, the smoke did not smell good to me anymore (Interviewee 13; ex-smoker).
Social Environment
It was a common phenomenon to share and gift cigarettes in China, most participants believed that offering or accepting cigarettes was an effective way to maintain good social relationships, and was also a basis for doing business with partners. Therefore, relapse usually occurred when they were offered cigarettes.
I once relapsed when I went to office and my colleagues offered a cigarette to me, it smelled so delicious, I swallowed like a child watching the cigarette in my hand and I cannot help smoking again (Interviewee 24; ex-smoker).
I did not like smoking either because it made me cough, my wife and children urged me to give up smoking. However, as a salesman I needed to meet many different clients and offered cigarette to them every day, and it was considered impolite and may further influence my business if I did not smoke. So, I did not smoke when I was at home and relapsed when I was at work (Interviewee 12; current smoker).
Addiction to Nicotine
Another important factor for relapse was severe addiction to nicotine. We found that some participants who motivated to quit often relapsed due to strong smoking cravings or withdrawal symptoms. However, smokers who were less addicted to nicotine found it easier to stop smoking.
I found it was very difficult for me to give up smoking, I had smoked for more than 40 years, during the time I quit, I was upset, bored, yawning, and even had insomnia at night. I had a strong urge for cigarettes, it was terrible for me to stop smoking (Interviewee 31; current smoker).
I had not smoked a cigarette since I decided to quit smoking, and I was not addicted to cigarettes although I was a long-term smoker (Interviewee 8, 14; ex-smoker).
Theme 3: Opportunities That Facilitate Smokers to Quit Smoking
In view of misunderstandings about the effects of quitting immediately, and limited knowledge of COPD and smoking, smoking cessation education was desperately needed. Referring to professional smoking cessation aids, few participants had tried pharmacotherapy or auricular acupressure. Additionally, for some hardcore smokers, they said they were pinning their hopes on tobacco control policies.
Smoking Cessation Education
Although the majority of participants were aware of the harms of smoking, they did not realize the danger of smoking and smoking addiction when they started smoking. In terms of smoking cessation, there were still some misunderstandings or insufficient recognition about smoking cessation. Additionally, very few participants had heard about the smoking cessation clinics, let alone the detailed professional help provided by smoking cessation clinics.
I had heard about the smoking cessation clinic on TV, but I knew little about it since I had to work every day and had no time for seeing a doctor. Therefore, I think some vivid online pictures or well-known experts opinion on smoking cessation may be more suitable for young people (Interviewee 12; current smoker).
I did not think it was necessary to turn to doctors for smoking cessation, for older and sick people, it was inconvenient to participant in any on-site activities, but online smoking warnings were effective for preventing young people from smoking (Interviewee 17; current smoker).
In terms of experiences and perceptions for e-cigarettes, some participants used e-cigarettes for smoking cessation, while others used them for curiosity or for fun. Overall, participants used e-cigarettes for shorter periods of time and had limited knowledge of its safety.
I once smoked e-cigarettes for curiosity, and I felt that the more I smoked, the more I craved for it since e-cigarettes failed to bring me satisfaction and pleasure as tobacco cigarettes give. I found e-cigarettes cannot take the place of cigarettes, so I abandoned it (Interviewee 17; current smoker).
My son bought e-cigarettes for me to help me stop smoking, it was too expensive for long-term use. Although e-cigarettes were less harmful and less smoky, there was still some irritation to respiratory tract, I can feel it (Interviewee 24; ex-smoker).
Smoking Cessation Aids
In terms of pharmacotherapy, only 2 participants had taken smoking cessation medications, but for a short period of time due to high price or limited benefits. Most of participants had never heard of pharmacotherapy and they were reluctant to take any western or Chinese medicines, because they considered that any kind of medication was toxic and should not be abused. Behavior support from general practitioners or social media was usually simple and insufficient. Three participants had tried auricular acupressure and maintained that they prefer acupressure to medications. While for other participants, whose attitude towards these therapies depended on their effectiveness and convenience.
I had taken smoking cessation medications for a month, which were prescribed by a doctor in smoking cessation clinic, but I cannot remember its specific name, it was expensive and costs as much as eight hundred Yuan. I felt less addicted to cigarettes at that time but I did not continue to use medication after I ran out of it (Interviewee 24; ex-smoker).
Acupuncture has been widely used for smoking cessation for a long time in China. In this interview, we found that participants were more likely to receive acupressure therapy rather than acupuncture due to pain and inconvenience. They felt that acupressure was effective for suppressing cravings for cigarettes and relieving psychological pressures induced by smoking cessation.
I felt less craving for cigarettes after I was given auricular acupressure treatment during hospitalization, I was surprised to find that I was not always thinking about smoking as before, the smell of cigarette was not as good as it used to be. In addition, I also slept better at night (Interviewee 33; current smoker).
I thought auricular acupressure was a convenient and suitable method for me since I did not need to go to hospital every day, I went to for a treatment every 2 or 3 days. Moreover, it was effective for me in aiding cessation, I pressed the acupoints when I wanted to smoke, and I used to smoke 40 cigarettes a day and now less than 10. Meanwhile, I felt much more relieved psychologically after received acupressure treatment than I struggled to stop smoking by myself (Interviewee 32; current smoker).
Tobacco Control Policies
Some of current smokers with COPD who were heavily addicted to cigarettes turned to national tobacco control policies. They were usually unwilling to give up smoking or had attempted to quit but failed.
I found there were no vivid warning pictures on Chinese cigarette packs, only small and simple text warning. I often relapsed due to exposure to smoking environment, and I thought it would be useful for preventing offering and gifting cigarettes to friends if there were some warning pictures on the package since it was considered unlucky in China (Interviewee 12; current smoker).
I hope that all the tobacco industries would be shut down at once, and smoking cessation should be enforced, and smoking should be banned in any public or private circumstances, only in this case, can I achieve cessation successfully (Interviewee 9, 21; current smokers).
Discussion
Research Question
Smoking cessation was the key intervention for patients with COPD, and smoking cessation notably played an important role in improving pulmonary functional parameters in patients with COPD,34 and was also beneficial for severe COPD patients.35 However, smoking cessation in patients with COPD differs from general smokers, and few COPD smokers quit successfully. Therefore, the interview explored the barriers and facilitators for smoking cessation among Chinese smokers with COPD, from their own motivation to quitting, smoking cessation interventions, and tobacco-related policies and culture in China.
Main Findings
Finally, three themes and ten categories based on the COM-B framework29 were identified: smokers’ automatic or reflective motivation is a prerequisite for quitting smoking, maintaining psychological or physical capability to quit smoking, and opportunities that facilitate the smokers to quit smoking. Almost all of the interviewees regardless of whether they were current or ex-smokers believed that personal motivation was a prerequisite for successful quitting, and that the quitting process needed to be initiated by themselves. This was consistent with a previous qualitative study on COPD smokers.36 We found that motivation to quit was usually initiated by COPD-related symptoms. However, some participants were still reluctant to stop smoking due to misunderstandings that quitting too fast led to bigger harms to health, and thus they chose to reduce cigarette consumption gradually. Other COPD smokers were discouraged by previous failed quitting attempts and had no confidence in quitting. Smokers who were motivated to quit had to overcome various psychological or physical difficulties in the quitting process. We found that one of important motivators for COPD smokers to stay smoke free were the physical benefits they experienced from quitting and this motivated them to sustain quitting. In addition, we consistently found that lack of determination and willpower was the decisive reason for relapse.37 The majority of participants achieved smoking cessation successfully by their own determination. Additionally, some participants complained serious withdrawal symptoms, and they always struggled desperately with these unbearable feelings and then relapsed. As was reported, nicotine dependence played a negative role in achieving successful smoking cessation.38 Participants rarely turned to professional help in quitting attempts, but some of them discussed that brief verbal advice from doctors played an important role, especially when they were told the consequences of smoking. However, the majority of health-care workers did not provide smoking cessation interventions based on 5As (Ask, Advice, Assess, Assist, and Arrange).39 In terms of pharmacotherapy, most participants were not aware of or underestimated its efficiency, this was similar to a previous study.40 Acupuncture and related therapies have been used for smoking cessation in China and abroad,26 and we found that participants were more willing to accept auricular acupressure or Chinese herbal medicine external use rather than any oral medicine. However, for other participants, their attitudes toward any smoking cessation intervention depended on its effectiveness and convenience.
Novelties About This Work
The Custom of Offering and Gifting Cigarettes Induced Relapse
It is a unique custom in China to offer and gift cigarettes to each other, and which was considered as an effective way to develop or maintain social relationships, and many qualitative studies have found that this was a vital factor for relapse.41–43 We found that vivid warning pictures on cigarette package were potentially effective for preventing smoking initiation or relapse. This was consistent with a research that pictorial health warnings on cigarette packs may be beneficial to reduce sharing and gifting cigarettes among Chinese smokers.44
COPD Smokers Prefer Acupressure Over Oral Medicines
For participants who had tried auricular acupressure, they considered it was convenient and painless, and they did not need to go to hospital every day. Moreover, they felt that auricular acupressure was effective for suppressing cravings for cigarettes and relieving psychological pressure from smoking cessation. A qualitative study also found that acupressure was beneficial for reducing smoking cravings for a short time.45
Online Smoking Cessation Education
It was necessary to recognize the different physical activity level among patients with COPD, and to improve the efficacy of behavior change interventions.46 Therefore, for smokers with COPD who had difficulties in getting around or adult smokers with limited time, online smoking cessation education was more appropriate for them. A guideline recommended that digital and mobile health intervention could be an adjunctive option to help people stop smoking.47 Digital therapeutic intervention was found superior to very brief advice in achieving smoking cessation.48 Therefore, vivid and interesting videos or expert interviews, or tailored smartphone app on smoking cessation informed by the principles of cognitive behavioral therapy could be pushed to smokers by various social media.
Tobacco Control Policies
Moreover, smoke-free regulations in public places needed to be further strengthened, which may benefit smokers who lack strong willpower to quit. China has set a series of tobacco control policies in public places since 2013, and there are at least 20 cities have issued local regulations on tobacco control. Smoking is forbidden in public places, and China also set up smoking cessation clinics to discourage smoking.49 However, there is still a long way to go to decrease the adult smoking rate from 28% to 20% by 2030. The UK has implemented comprehensive tobacco control policies,50 and these policies successfully led to a reduction of 23% in smoking rates.51 Similarly, Australia has passed legislation that all the cigarette packages should be plain packaging.52 Hence, more comprehensive and stricter tobacco control policies are needed in China, such as increasing cigarette taxes, pictorial health warnings on cigarette packs, advertising restrictions, and cessation treatment supports.
Strengths and Limitations
This study was designed and conducted following qualitative study methodology in order to add new detailed information to current very limited data on the experiences and perceptions surrounding smoking cessation in patients with COPD in China. The interview was guided by COM-B framework, and the 32 participants were from a range of ages and diverse socio-economic backgrounds. We also collected information related to their onset of smoking and current smoking status, which may provide insights into factors that influenced their successful quitting. However, the main limitation of study was that the face-to-face interviews were conducted in independent ward in hospital and which may make the participants less relaxed, though interviewing in a home environment may have created more bias. Additionally, some ex-smokers were also included in the interview; therefore, the recollection of their smoking cessation experiences and perceptions may be affected by recall bias.
Conclusions
The motivation to quit among smokers with COPD of stage I–III was usually initiated by cough or wheezing, although participants had a limited knowledge of COPD. Physical benefits from quitting and strong willpower facilitated smoking cessation. While exposure to cigarettes in social contacts and strong addiction to nicotine usually led to relapse. COPD smokers in China were more inclined to use auricular acupressure rather than pharmacotherapy. Online smoking cessation education, and professional smoking cessation interventions from general physicians are desperately needed. Additionally, warning pictures on cigarette package and strengthened smoke-free regulations may be helpful to smoking cessation.
Abbreviations
5A, 5 Ask, Advice, Assess, Assist, and Arrange to follow up; COPD, chronic obstructive pulmonary disease; COM-B, Capability, Opportunity, Motivation-Behavior; COREQ, Consolidated criteria for reporting qualitative research; CT, computed tomography; GOLD, Global Initiative for Chronic Obstructive Lung Disease.
Data Sharing Statement
The raw data (interview transcript) that support the findings of this study are available from the corresponding author (JPL) (email: [email protected]) upon reasonable request. The data are not publicly available due to information shared in these interviews that could comprise the privacy of research participants.
Ethics Approval and Consent to Participate
The study was approved by Ethics Committee of Beijing University of Chinese Medicine (2021BZYLL0103) and Fangshan hospital affiliated to Beijing University of Chinese Medicine (FZYLK-2021-019). Written informed consent was obtained prior to interviews.
Acknowledgments
Many thanks to Doctor Yang Baojiang in Fangshan hospitals for his considerable support and assistance in patient recruitment. The researchers would like to express special thanks to all participants who kindly took part in this interview.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study is supported by the National Key Research and Development Project: Adding Chinese herbal medicine to antibiotic treatment for acute exacerbation of chronic obstructive pulmonary disease (Grant no. 2018YFE0102300).
Disclosure
All authors declare that they have no competing interests.
References
1. The health consequences of smoking-50 years of progress: a report of the surgeon general. Atlanta, GA: U.S: Department of Health and Human Services; 2014. Available from: http://www.surgeongeneral.gov/library/reports/50-years-of-progress/.
2. Eisner MD, Anthonisen N, Coultas D, et al. An official American Thoracic Society public policy statement: novel risk factors and the global burden of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2010;182(5):693–718. doi:10.1164/rccm.200811-1757ST
3. GBD. 2019 diseases and injuries collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–1222. doi:10.1016/S0140-6736(20)30925-9
4. Adeloye D, Chua S, Lee C, et al. Global and regional estimates of COPD prevalence: systematic review and meta-analysis. J Glob Health. 2015;5(2):020415. doi:10.7189/jogh.05-020415
5. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management and Prevention of COPD 2018. Available from: https://goldcoped.org/.
6. Hogg JC, Chu F, Utokaparch S, et al. The nature of small-airway obstruction in chronic obstructive pulmonary disease. NEngl J Med. 2004;350(26):2645–2653. doi:10.1056/NEJMoa032158
7. McDonough JE, Yuan R, Suzuki M, et al. Small-airway obstruction and emphysema in chronic obstructive pulmonary disease. N Engl J Med. 2011;365(17):1567–1575. doi:10.1056/NEJMoa1106955
8. British Thoracic Society. IMPRESS guide to the relative value of COPD interventions. British Thoracic Society Reports, 2012. Available from: https://www.networks.nhs.uk/nhs-networks/impressimproving-and-integrating-respiratory.
9. van Eerd EA, van der Meer RM, van Schayck OC, et al. Smoking cessation for people with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2016;2016(8):CD010744. doi:10.1002/14651858
10. Woodruff PG, Barr RG, Bleecker E, et al. Clinical significance of symptoms in smokers with preserved pulmonary function. N Engl J Med. 2016;374(19):1811–1821. doi:10.1056/NEJMoa1505971
11. The Global Initiative for Chronic Obstructive Lung Diseases (GOLD). Global strategy for diagnosis, management and prevention of COPD. 2020 report. Available from: https://goldcopd.org/gold-reports/.
12. Singh D, Agusti A, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease: the GOLD science committee report 2019. Eur Respir J. 2019;53(5):1900164. doi:10.1183/13993003.00164-2019
13. British Thoracic Society. Chronic obstructive pulmonary disease in over 16s: diagnosis and management. London: National Institute for Health and Care Excellence (UK); 2019.
14. Bednarek M, Gorecka D, Wielgomas J, et al. Smokers with airway obstruction are more likely to quit smoking. Thorax. 2006;61(10):869–873. doi:10.1136/thx.2006.059071
15. Toljamo T, Kaukonen M, Nieminen P, et al. Early detection of COPD combined with individualized counselling for smoking cessation: a two-year prospective study. Scand J Prim Health. 2010;28(1):41–46. doi:10.3109/02813431003630105
16. Stratelis G, Mölstad S, Jakobsson P, et al. The impact of repeated spirometry and smoking cessation advice on smokers with mild COPD. Scand J Prim Health. 2006;24(3):133–139. doi:10.1080/02813430600819751
17. Kuna P, Kuprys-Lipinska I. The attitude of patients suffering from COPD towards addiction to smoking and attempts to smoking cessation. Eur Respir J. 2014;44(Suppl 58):4195.
18. Sozener CZ, Araslan F, Soyyigit S, et al. Perceptions and attitudes of the asthma, COPD and allergic rhinitis patients towards smoking and smoking cessation. Allergy Eur J Allergy Clin Immunol. 2015;70:320.
19. van Eerd EA, van Rossem CR, Spigt MG, et al. Do we need tailored smoking cessation interventions for smokers with COPD? A comparative study of smokers with and without COPD regarding factors associated with tobacco smoking. Respiration. 2015;90(3):211–219. doi:10.1159/000398816
20. Shields PG, Herbst RS, Arenberg D. Smoking cessation, version 1.2016, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2016;14(11):1430–1468. doi:10.6004/jnccn.2016.0152
21. Solberg LI, Parker ED, Foldes SS, et al. Disparities in tobacco cessation medication orders and fills among special populations. Nicotine Tob Res. 2010;12(2):144–151. doi:10.1093/ntr/ntp187
22. Zeng F, Chen CI, Mastey V, et al. Effects of copayment on initiation of smoking cessation pharmacotherapy: an analysis of varenicline reversed claims. Clin Ther. 2011;33(2):225–234. doi:10.1016/j.clinthera.2011.02.013
23. Wang C, Xu JY, Yang L, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health [CPH] study): a national cross-sectional study. Lancet. 2018;391(10131):1706–1717. doi:10.1016/S0140-6736(18)30841-9
24. Qin R, Liu Z, Zhou X, et al. Adherence and efficacy of smoking cessation treatment among patients with COPD in China. Int J Chron Obstruct Pulmon Dis. 2021;16:1203–1214. doi:10.2147/COPD.S301579
25. Zhao X. Analysis of the construction status of some smoking cessation clinics in China in 2016: Chinese Center for Disease Control and Prevention; 2018.
26. White AR, Rampes H, Liu JP, et al. Acupuncture and related interventions for smoking cessation. Cochrane Database Syst Rev. 2011;(1):CD000009. doi:10.1002/14651858.CD000009.pub3
27. Lee EJ. Auricular acupressure and positive group psychotherapy with motivational interviewing for smoking cessation. Holist Nurs Pract. 2019;33(4):214–221. doi:10.1097/HNP.0000000000000333
28. Zheng X, Qu NN, Ma LJ, et al. Clinical study of Chinese herbal medicine external use at acupoint combined with 5A program on smokers with nicotine dependence (phlegm and blood stasis syndrome). J Liaoning UnivTradit Chin Med. 2019;21(3):4.
29. Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterizing and designing behavioral change interventions. Implement Sci. 2011;6:42. doi:10.1186/1748-5908-6-42
30. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
31. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
32. Patton MQ. Qualitative Research & Evaluation Methods.
33. Braun V, Clarke V. Can I use TA? Should I use TA? Should I not use TA? Comparing reflexive thematic analysis and other pattern-based qualitative analytic approaches. Couns Psychother Res. 2021;21(1):37–47. doi:10.1002/capr.12360
34. Pezzuto A, Carico E. Effectiveness of smoking cessation in smokers with COPD and nocturnal oxygen desaturation: functional analysis. Clin Respir J. 2020;14(1):29–34. doi:10.1111/crj.13096
35. Pezzuto A, D’Ascanio M, Grieco A, et al. Functional benefit of smoking cessation in severe COPD patients undergoing bronchial valve implantation. Eur J Intern Med. 2019;68:55–59. doi:10.1016/j.ejim
36. Wilson JS, Elborn JS, Fitzsimons D. ‘It’s not worth stopping now’: why do smokers with chronic obstructive pulmonary disease continue to smoke? A qualitative study. J Clin Nurs. 2011;20(5–6):819–827. doi:10.1111/j.1365-2702.2010.03319.x
37. Buczkowski K, Dachtera-Frąckiewicz M, Luszkiewicz D, et al. Reasons for and scenarios associated with failure to cease smoking: results from a qualitative study among polish smokers who had unsuccessfully attempted to quit. Patient Prefer Adherence. 2021;15:2071–2084. doi:10.2147/PPA.S320798
38. May S, West R, Hajek P, et al. Social support and success at stopping smoking. J Smok Cessat. 2007;2:47–53. doi:10.1375/jsc.2.2.47
39. Tamirat T. Health workers’ practice towards smoking cessation intervention based on 5A’s model and associated factors in public hospitals, Hadiya Zone, Southern Ethiopia. Patient Relat Outcome Meas. 2021;12:291–298. doi:10.2147/PROM.S322049
40. Hammond D, McDonald PW, Fong GT, et al. Do smokers know how to quit? Knowledge and perceived effectiveness of cessation assistance as predictors of cessation behaviour. Addiction. 2004;99(8):1042–1048. doi:10.1111/j.1360-0443.2004.00754.x
41. Mao A, Yang T, Bottorff JL, et al. Personal and social determinants sustaining smoking practices in rural China: a qualitative study. Int J Equity Health. 2014;13:11–12. doi:10.1186/1475-9276-13-12
42. Wang J, Li C, Jia C, et al. Smoking, smoking cessation and tobacco control in rural China: a qualitative study in Shandong Province. BMC Public Health. 2014;14(1):916. doi:10.1186/1471-2458-14-916
43. Zhang J-Y, Chan SS-C, Fong DY-T, et al. The social context of smoking cessation in China: an exploratory interview study. Tob Control. 2012;21:57–58. doi:10.1136/tc.2010.040691
44. Liao Y, Tang J, McNeill A, et al. Impact of cigarette package warnings on attitudes towards sharing and gifting cigarettes in China: a nationwide study of smokers and non-smokers. Tob Control. 2021:
45. Aumann I, Tedja L, Von der schulenburg JM. Experiences of COPD patients with existing smoking cessation programs and their preferences for improvement - A qualitative analysis. Tob Induc Dis. 2016;14(1):31. doi:10.1186/s12971-016-0097-4
46. Scheermesser M, Reicherzer L, Beyer S, et al. The influence of pulmonary rehabilitation and counselling on perceptions of physical activity in individuals with COPD - A qualitative study. Int J Chron Obstruct Pulmon Dis. 2021;16:2337–2350. doi:10.2147/COPD.S315130
47. NICE guideline. Behaviour change: digital and mobile health interventions (NG183), 2020. Available from: https://www.nice.org.uk/guidance/ng183.
48. Webb J, Peerbux S, Smittenaar P, et al. Preliminary outcomes of a digital therapeutic intervention for smoking cessation in adult smokers: randomized controlled trial. JMIR Ment Health. 2020;7(10):e22833. doi:10.2196/22833
49. Tao FX. A study on the implementation of comprehensive smoking ban policy in public places-taking Nanjing as an example. Nanjing Univ Sci Technol. 2020. doi:10.27241/d.cnki.gnjgu.2020.000873
50. Scottish Executive. Smoking, health and social care (Scotland) act 2005. Available from: https://www.legislation.gov.uk/asp/2005/13/contents.
51. Levy DT, Currie L, Clancy L. Tobacco control policy in the UK: blueprint for the rest of Europe? Eur J Public Health. 2013;23(2):201–206. doi:10.1093/eurpub/cks090
52. Wakefield M. Welcome to cardboard country: how plain packaging could change the subjective experience of smoking. Tob Control. 2011;20(5):321–322. doi:10.1136/tc.2011.044446
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.