Back to Journals » Pragmatic and Observational Research » Volume 17
Barriers and Facilitators for Equitable Clinical Research Among Pragmatic Trialists: A Qualitative Study
Authors Short O ![]() , McLeod KR, Erpenbeck K
, McLeod KR, Erpenbeck K ![]() , McCamic E, Ibemere SO
, McCamic E, Ibemere SO ![]() , Harrington CB, Khazanie P, Gonzalez-Guarda RM
, Harrington CB, Khazanie P, Gonzalez-Guarda RM ![]()
Received 24 December 2025
Accepted for publication 19 May 2026
Published 8 June 2026 Volume 2026:17 591363
DOI https://doi.org/10.2147/POR.S591363
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Kris Bennett
Olivia Short,1,* Kaitlyn R McLeod,2,* Kaitlin Erpenbeck,2 Elizabeth McCamic,3 Stephanie O Ibemere,1,4 Cherise B Harrington,5 Prateeti Khazanie,2 Rosa M Gonzalez-Guarda1
1School of Nursing, Duke University, Durham, NC, USA; 2School of Medicine, University of Colorado Anschutz Medical Campus, Aurora, CO, USA; 3Duke Clinical Research Institute in the School of Medicine, Duke University, Durham, NC, USA; 4Duke Global Health Institute, Duke University, Durham, NC, USA; 5Department of Public Education, North Carolina Central University, Durham, NC, USA
*These authors contributed equally to this work
Correspondence: Olivia Short, School of Nursing, Duke University, Durham, NC, USA, Email [email protected]
Purpose: There is a growing urgency to address health inequities in clinical trial design. Pragmatic trials hold promise in addressing inequities in research. We conducted a rapid qualitative analysis of barriers and facilitators to implementing health equity practices in pragmatic trials within the NIH Pragmatic Trials Collaboratory, informed by the DUSON-INFUSE checklist.
Participants and Methods: A descriptive qualitative design was used to address barriers and facilitators to equitable pragmatic trials. Twelve semi-structured interviews with primary investigators and research associates were conducted. Included trials were selected to represent a variety of phases of funding and study progress to examine the full lifecycle of research. Interview transcripts were summarized using a standardized matrix. Rapid qualitative analysis was implemented to condense data into four emergent themes.
Results: Trialists were in the enrollment (n=8), follow-up (n=1), and completion (n=3) phases of their research. Study themes described how (1) funding timelines dictate community relationship building, (2) concordant identities between research teams and study populations promote equity, (3) community alignment on priorities facilitates success, and (4) intervention flexibility is necessary to support participant engagement.
Conclusion: To optimize the potential for pragmatic clinical trials to reduce health inequities, all phases of research must be designed with health equity in mind. This includes funding timelines and research budget planning that leave space for relationship building, as well as co-developed priorities between investigators and communities to ensure research fosters trust and engagement.
Keywords: health services accessibility, clinical trials, study design, qualitative research
Introduction
Health equity is a more recent research priority1–4 defined by the World Health Organization as
the absence of unfair, avoidable or remediable differences among groups of people…achieved when everyone can attain their full potential for health and well-being.5
Health equity requires removal of structural and societal obstacles to health, such as poverty, discrimination, and their downstream effects including unaffordable healthcare and housing—all of which disproportionately affect excluded and marginalized groups.6,7 While the research landscape has shifted toward addressing equity rather than simply identifying disparities, trialists struggle to incorporate it systematically.3
Explanatory trials often use restrictive eligibility criteria or complicated consent processes,8 underrepresenting racially and ethnically minoritized individuals,9 pregnant people,10 or those with serious comorbidity or social disadvantage.11 These underrepresented groups often face the greatest health challenges.12–15 While explanatory trials play a key role in advancing science, studies with highly selective populations may not reflect real-world practice, threatening generalizability, and scientific equity—the opportunity for all to benefit from scientific advances.11,16
Funders have responded to these challenges by focusing on diversity in research,17 encouraging more realistic exclusion criteria and funding supplements to support diversity in clinical trial research teams and participants.18,19 In the NIH Pragmatic Trials Collaboratory (NIH Collaboratory), for example, funders previously used an incentive strategy to increase diversity in clinical trial participation and community engagement (Figure 1). However, even when clinical trials ensure diverse representation, it does not mean that diverse perspectives, needs, or experiences are also represented.20,21 Thus, addressing health equity in pragmatic trials requires a multifaceted approach.
 |
Figure 1 Funder-required health equity components in NIH Collaboratory Trials 2012–2024. A search was conducted on NIH RePORTER (reporter.nih.gov) to determine how many of the 35 NIH Collaboratory Trials included a required health equity focus from the funder’s request for application. Key words included equity, health equity, community, community health, engagement, and advisory. |
Pragmatic trials have the potential to improve health equity.22,23 Designed to work with real-world complexities, pragmatic trials are typically characterized by limited exclusion criteria and flexible protocols and recruitment strategies23 but are conducted in historically inequitable systems with logistical challenges.24 A review of 62 pragmatic trials found only 3.2% had equity-relevant objectives and 6.5% planned diverse enrollment.25 Further, the research workforce lacks diversity relative to studied populations, and evidence suggests pragmatic trials do not automatically address health equity by design.21 Thus, pragmatic trials that improve health equity cannot be expected to emerge without intention, including diverse stakeholder engagement22 and a research culture that views health disparities as ethical health system obligations.26
Several frameworks help trialists intentionally integrate health equity throughout the research lifecycle.27,28 The NIH Collaboratory supports this integration using frameworks including the Duke University School of Nursing’s DUSON-INFUSE (Implementing a New Focus on Equity in Research) checklist,29 a guide and self-assessment tool for incorporating equity in study design and research teams across planning, proposal development, study conduct, and dissemination. Our goal is to enable pragmatic trialists and funders to integrate health equity principles into research with high-level takeaways. This study explores barriers and facilitators to implementing health equity practices in pragmatic trials, using DUSON-INFUSE to inform data generation and analysis.
Materials and Methods
Design
A qualitative descriptive design with rapid qualitative analysis (RQA) was used to explore barriers and facilitators to incorporating health equity into pragmatic clinical trials among NIH Collaboratory trialists.30,31 RQA is a rigorous and action-oriented approach for targeting quickly evolving issues such as health inequities with shorter time-frames and constrained resources without compromising rigor, making it an appropriate design for this project.30–32 Combined with a pragmatic perspective, judging knowledge by its ability to solve real-world problems rather than by adhering to a single epistemology, RQA emphasizes relevance, flexibility, and rapid applicability. The Planning for and Assessing Rigor in Rapid Qualitative Analysis checklist guided study conduct and reporting.30 The DUSON-INFUSE checklist29 informed our data generation and analysis procedures, including the interview guide, summary templates (Table 1), and matrices (Table 2). Members of the NIH Collaboratory Community Health Improvement Core with experience in healthy equity, qualitative research, and pragmatic trials provided iterative review of the interview guide. This study received institutional review board approval.
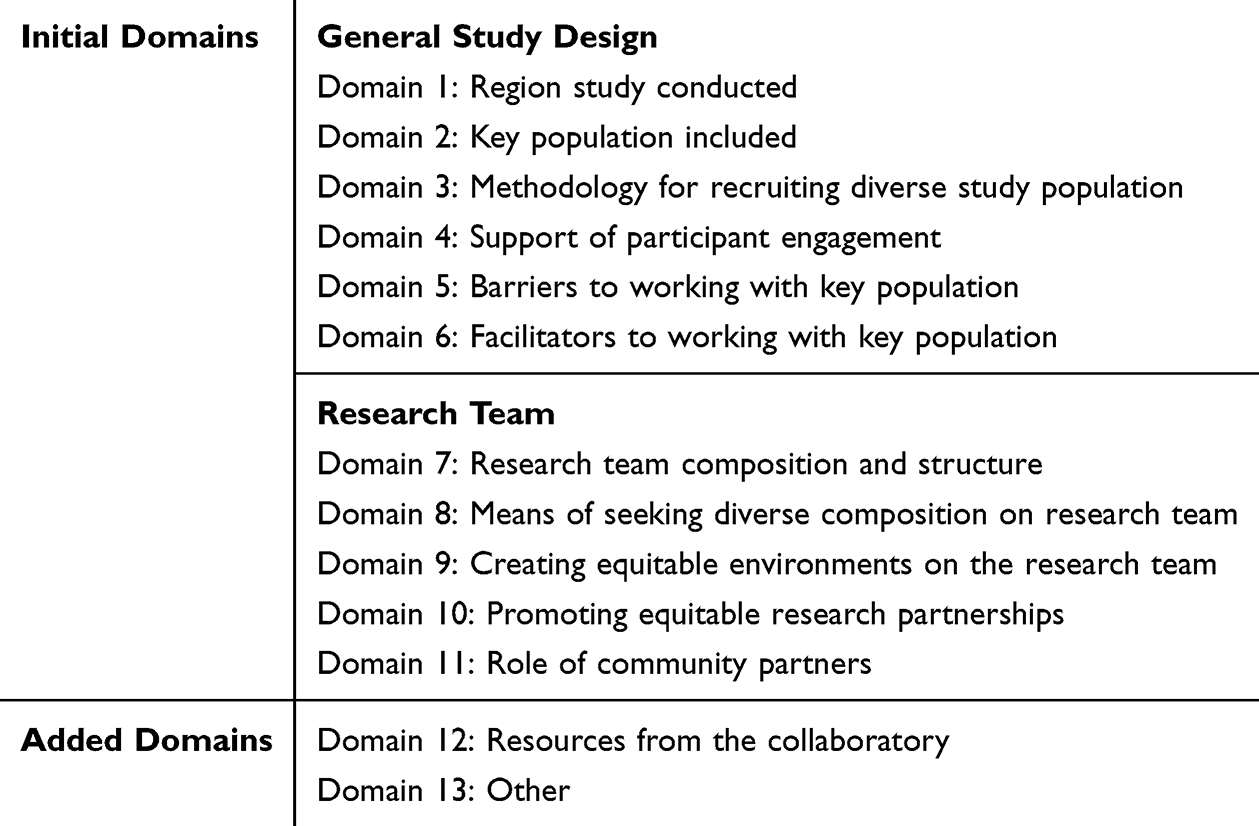 |
Table 1 Summary Template Domains |
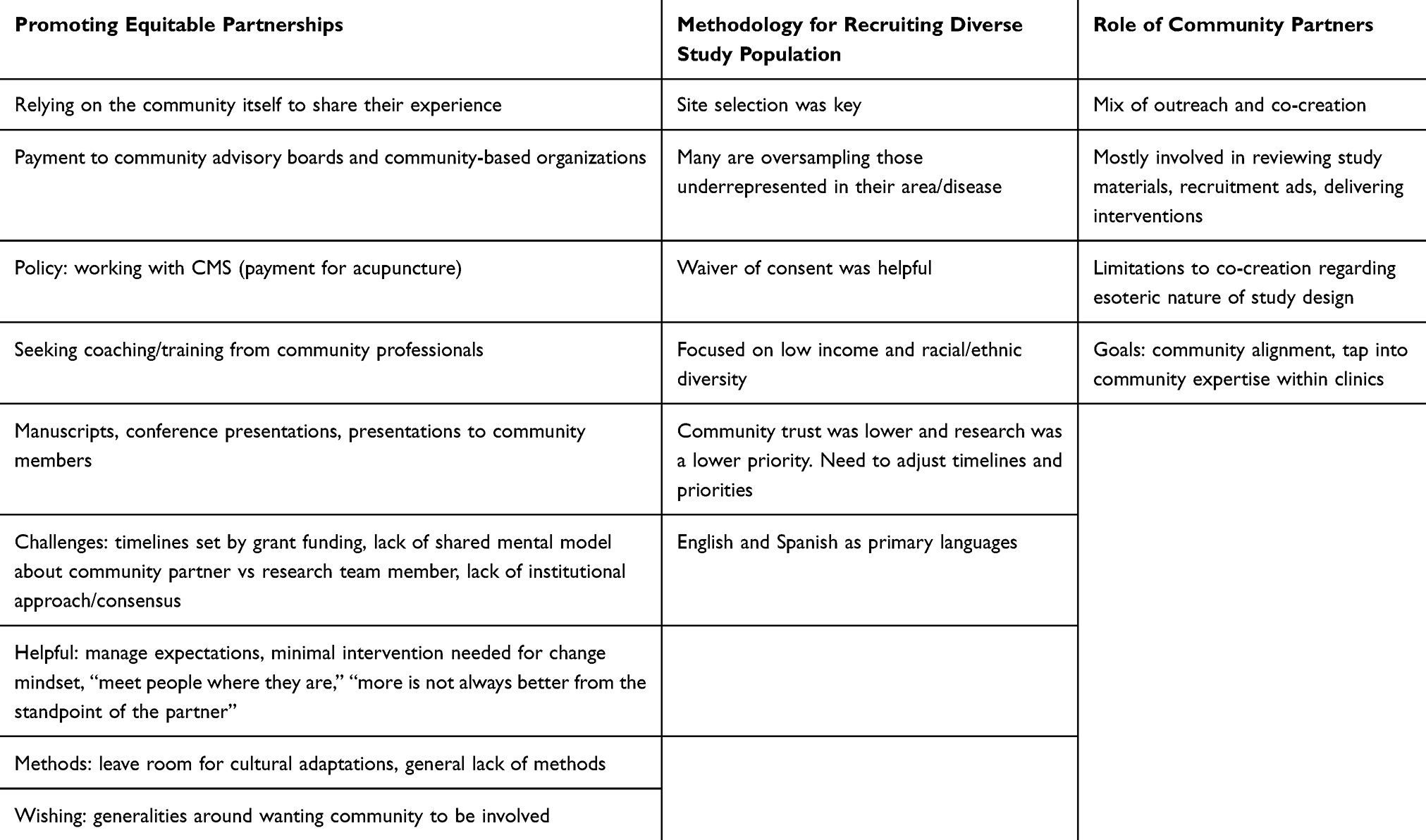 |
Table 2 Examples from Consensus-Derived Matrix Summaries |
Sample and Setting
Semi-structured interviews were conducted with 12 NIH Collaboratory Principal Investigators or Research Associates in spring 2024 (Table 1). Eligible trialists used pragmatic designs and were mostly multi-site and multi-institutional. Trialists were recruited from the NIH Collaboratory by email and purposively sampled by funding stage (UG3, UH3, R01, and completed projects). While sampling was driven by time and resource availability, suitable for RQA, the final sample supported strong information power through a focused aim, specific sample, and concentrated interview guide.30,33 The UG3/UH3 Cooperative Agreement funds research in two phases: UG3 supports feasibility studies for up to two years; successfully completed projects transition to UH3 for three additional implementation years.34 These trials operated within NIH initiatives promoting equity in clinical trials and community engagement (Figure 1).
Procedures
Verbal informed consent was obtained before study procedures. Focused, semi-structured interviews were conducted by a member of the NIH Collaboratory not personally known by the trialists using secure Zoom video with automatic transcription. Interviews lasted approximately 30 minutes. Memos documented interviewer thoughts and assumptions,35,36 and transcripts and audio recordings were manually audited for accuracy. The interview guide is provided (Supplementary Figure 1).
Data Analysis
A team of three analysts (including the interviewer) and two mentors used effective communication and clear roles to adhere to the rapid timeline. We completed analyses as planned during summer 2024 after all data generation. First, an analyst created summary templates based on the interview guide. All analysts iteratively read three identical interviews and independently developed brief 2–3 page summary templates (Table 1), which were discussed to establish consistency and accuracy of summaries. Summaries were concise but complete and relevant to the research question. At this time, two additional domains were added to capture information important to the research question which did not fit into pre-existing domains. Summary templates were completed by dividing remaining interviews among the analysts. Transcript line numbers and brief quotes enabled referencing the raw data for validation.
Next, analysts independently copied their summaries into matrices in Microsoft Excel with domains as columns and trialists as rows. The lead analyst reviewed all matrices. Iterative consensus decision-making was used to develop a final combined matrix (Table 2). Lastly, emergent, summative themes that crossed domains were identified and described.
Trustworthiness
Iterative reflection on data, memos, and team consultation with qualitative experts enhanced credibility and dependability.30,36 Member checking with interviewees and triangulation further strengthened findings.37 Direct quotes, reflexivity, and active searching for disconfirming evidence ensured confirmability, while detailed descriptions of methods and findings facilitated transferability.37
Self-Reflexivity and Positionality
The analysis and mentorship team acknowledged identities as White and Latina cisgender women and gender non-conforming professionals covering early to mid-career (1–23 years’ experience) with expertise spanning internal medicine, nursing, cardiology, qualitative methodology, health equity, and clinical trial implementation. We acknowledge how these identities and roles shaped knowledge production and trialist engagement.37
Results
Trialists included Principal Investigators (n=11) and Research Associates (n=1) (Table 3) testing a range of interventions from patient communications to provider-delivered treatments across enrollment (n=8), follow-up (n=1), and completion (n=3) stages. More recent trials were required by funders to promote health equity, and trialists identified corresponding strategies in their designs and research teams (Figure 1). Analysis of barriers and facilitators across domains generated four themes.
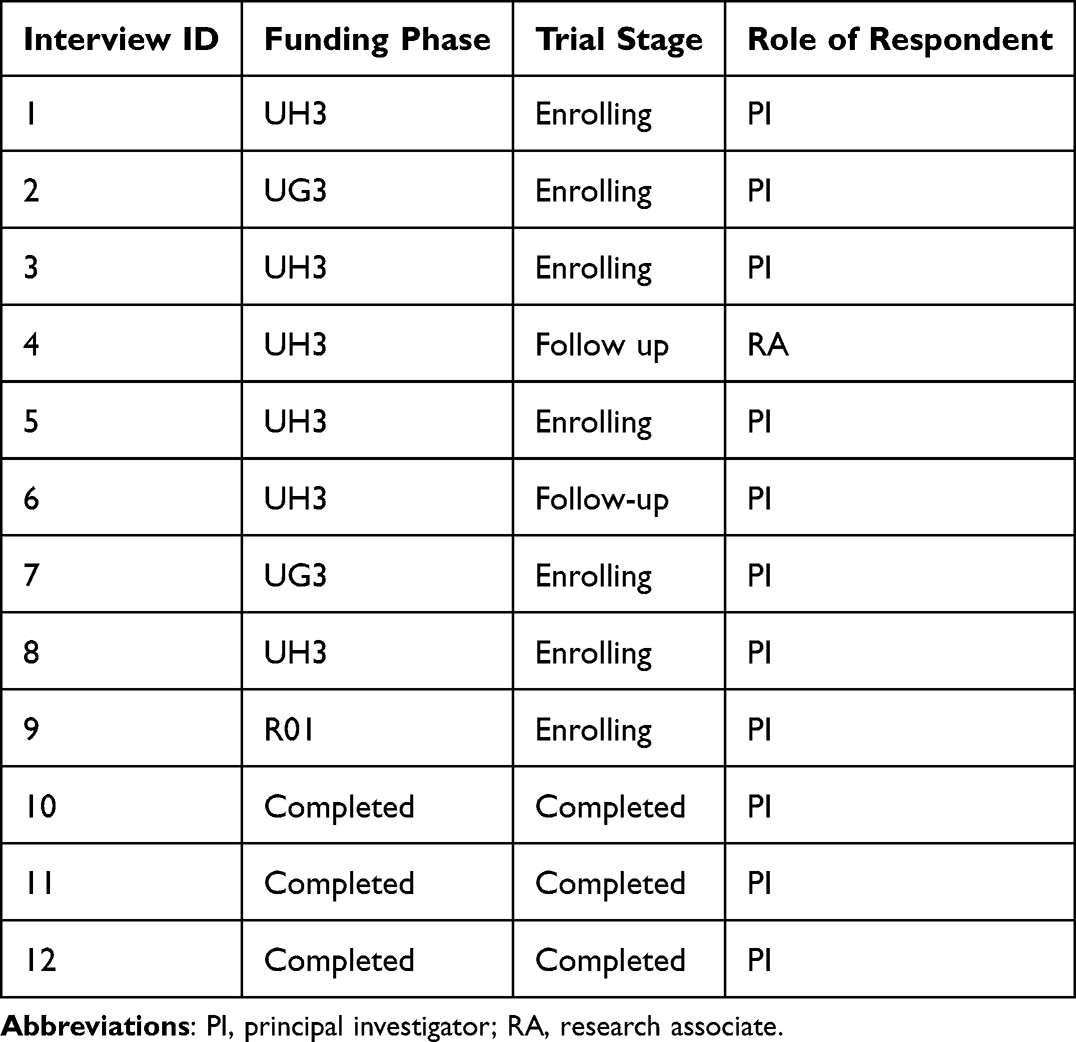 |
Table 3 Characteristics of Interview Respondents |
Theme 1: Funding Timelines Dictate Relationship Building
Trialists believed that intentionality and sufficient time for planning would allow for the ideal: co-creation with the community. Encouraged by more recent funders’ requirements to incorporate health equity into pragmatic trials (Figure 1), trialists expressed the desire to increase the time available for research teams to develop community relationships. However, they felt hindered by current research conduct, for example, the typical Request for Application (RFA) timeline.
Ideally, we would have co-created the study design and gotten an idea for the nurse care manager from like rural engagement. I think that wasn’t feasible given the timeline of how fast we had to submit a big grant. I think from when it was published to when I had to submit it was 2 months and I can’t get an IRB approved to get that work done in 2 months. (Interview 7)
Because current funding timelines and research norms did not allow time for relationship development, it favored the use of existing research partnerships. As one trialist described:
So, the core group of the study team really evolved from a group that was pre-existing. We had been collaborating for years on projects that had to do with primarily back pain…And, we had a number of RCTs that we’ve done together, as well as observational studies over the years…It’s essentially taking advantage of research groups that were pre-existing and applying them to new questions. (Interview 12)
Trialists from earlier studies described using supplements for community engagement. However, recent trials in the NIH Collaboratory were required by funders to incorporate health equity into the study design (Figure 1), and these trialists described health equity as central to the inception of their project and provided more concrete examples for how this was accomplished. For instance, a trialist emphasized the importance of designing with equity from the start rather than trying to retrofit equity into the design after being funded.
And I think if anything the lesson learned is that, going forward, we have to start with that lens. Right, in terms of when we’re writing the grant and, certainly in terms of study design and implementation to consider that lens, the health equity lens, all the time. (Interview 9)
When reflecting on how one might build partnerships, trialists described resources that allowed for this investment of time such as being part of a network that has relationships with community practices, or team members with a history of working with the community. Additionally, one trialist noted that it was important their academic research group had partnered with community health centers before and developed a good working relationship.
Theme 2: Concordant Identities Between Research Teams and Study Populations Facilitate Equity but are Not Sufficient for Building Equitable Teams
Shared social identity, or identity concordance, between research staff and the study population was perceived by trialists as a significant facilitator of health equity in pragmatic trial design. Trialists noted that research team members who shared lived experience with the populations and conditions being addressed were most in tune with what was working or not working with study participants. These integrated community partners brought with them lived experience, which grounded the research in local contexts.
A good bit of that diversity [on the research team] is really within the community partners. We absolutely had to have Spanish speaking individuals who were part of the research staff...not just Spanish speakers, but people culturally who understood some of the issues… (Interview 1)
Trialists used several strategies to build teams with identity concordance. During hiring, one trialist stated that they utilized a diversity, equity, and inclusion statement in the hiring application, and another asked during interviews about cultural knowledge and experiences working with the community. Others describe the importance of a meaningful job description, including a description of the desired lived experience to allow for self-selection of applicants. To enhance equitable teams, various community engagement strategies were used, including inviting community members as speakers or hiring them as consultants. One investigator described a community engagement panel as a group of consultants on the team whose compensations should align with equity principles.
However, having community members and individuals with identity concordance on the team was seen as helpful but not sufficient in integrating a health equity lens. Trialists described the need to create an equitable and inclusive environment during meetings. For example, one trialist noted that “we do have team members who are racial and ethnic minorities, and I do notice sometimes they speak less” (Interview 7); this trialist recommended that leaders invite these voices intentionally if appropriate, have one-on-one conversations, or encourage the use of Zoom chat to comfortably interrupt. Others emphasized the importance of trialists and community members to listen to one another assuming good will, allowing for a feeling of safety in discussing difficult topics.
Additionally, trialists commented on how “privilege has always seeped into science” (Interview 10), reinforcing exclusionary academic hierarchies that limit diversity and meaningful community involvement. Encouraging team members with concordant identities to contribute might involve mitigating “investigator versus other” mentalities (Interview 11).
In terms of, kind of, equity and making sure everybody’s voice was heard. We didn’t play on privilege or cast, you know, preconceived ideas of where people stand. I’m not sure we did much formal. We do more of that now in the studies I’m working on to really try to understand, kind of, hidden biases. (Interview 10)
However, despite a desire for equity and representation on research teams, many endorsed the challenge of achieving this. Some trialists described how hiring freezes during COVID or embedded designs restricted study teams to pre-existing employees, which typically did not represent the populations being studied, with one trialist noting they were “at the mercy of the people who work at that health system” (Interview 8). Another reflected on representation on their team:
Well, I mean, if you think about the study that we have, we have a study that’s adults over 65, and no one on my study team is over 65, and one person on the [overall] study team is over 65. And so, if you think we might be missing the perspective of the community that we are serving, then yes, we are missing that. (Interview 8)
Theme 3: Community Alignment on Priorities Facilitates Success
When trialists sought solutions with communities that shared a mutual concern, forward momentum was achieved. As one trialist described, community alignment was necessary for the project’s inception.
The very first step that was essential to making this project a reality was the support of the community partners that this was an issue that they deal with…Is pain management something that people in the clinical setting care about? And fortunately, the answer was yes...but if the answer had been no, this project wouldn’t exist and that would be appropriate. (Interview 1)
Trialists expressed concern about overburdening under-resourced populations due to historical research practices. These concerns were exacerbated by misalignment between research topic and community priorities, or when study teams held assumptions about a population based on prior experiences or generalizations. Others noted de-prioritization of research in community settings because of limited resources and competing demands. Overall, there was less concern about burdening communities when studies were co-created or in alignment between research teams and the community. Trialists described the importance of integrating strategies to ensure this alignment and finding areas of mutual benefit emerged as one of these key strategies. For example, one team described the process of finding mutual benefit:
When we started, the clinics were very skeptical about our project because they didn’t have resources…and they also didn’t want any changes in their EHR…But, at one of our advisory committees, we kind of figured out what they did want…and all of a sudden, they got really excited…It was just like everybody went from apathy to excitement when they felt like this is something I want and need. (Interview 10)
Theme 4: Intervention Flexibility Facilitates Participant Engagement
Trialists recognized that anticipating areas of adaptability to support participant engagement by meeting people “where they are” is critical and pragmatic. As one trialist noted, “We have to be very flexible...the person might be like, ‘I’ve got 20 minutes on my lunch break, and I can go out to my car, and we can talk’” (Interview 1). Other examples of flexibility included working with those delivering the intervention to offer night and weekend times.
People in the communities we’re working with do not have one single 9 to 5 job, and they may have 20 min at some odd time of the day that we do our best to accommodate. So, you know, I wasn’t as attentive to this in the design, but as we’ve brought on staff to work with the patients and deliver the interventions, I’ve become increasingly attentive…Are you a person who could be available in the early evening or the early morning? Because we have people that we need to accommodate in those times and not just sort of normal business hours. (Interview 1)
Trialists also commented on limited technology access and technological literacy, emphasizing the need to strategize ahead of time about how to distribute and support technologies.
Recognizing broadband and technology access can be an issue, we have budgeted actually monies for people—for patients who need it—to get iPads and data plans so that they can participate. (Interview 7)
Ensuring concordant identities (see Theme 2) was identified as a key strategy to responsively address participant needs. For example, one trialist described: “A lot of veterans want to really help other veterans” (Interview 2) and leveraged veterans in recruitment. Trialists also described the importance of balancing rigor in design with respect for communities being addressed. For example, a trialist described equity as sharing resources across different study arms (eg, intervention and control).
Discussion
We explored how pragmatic trialists incorporated health equity principles in their research teams and study designs by interviewing trialists participating in the NIH Collaboratory, observing trends between funding requirements, timelines, and trialist strategies. We identified barriers to health equity integration and mitigation strategies. While findings align with community-based participatory research literature,38 this study situates them in pragmatic designs and extends work showing pragmatic trials may inadvertently perpetuate health disparities unless strategically mitigated.9 In fact, it is the strategic positioning of pragmatic trials at the intersection of research, healthcare, and community that can provide real opportunities to address health equity.22
Trials funded prior to 2023 lacked health equity and/or community engagement requirements (Figure 1). We observed that the introduction of health equity funder requirements shifted the focus from broad racial and ethnic diversity in the study population toward addressing specific health inequities (eg, maternal health disparities). Trialists with funder requirements were able to incorporate equity from inception; earlier-funded trials less frequently described their study as explicitly designed to address health equity, though many utilized supplements for community engagement. This aligns with a recent review of health equity in pragmatic trials for Alzheimer’s and dementia,25 suggesting funding contingent on community participation impacts equity-focused trial design.
Theme 1 shows current funding timelines promote the use of pre-existing teams and relationships, privileging the status quo and limiting hiring of individuals who share identity with the community being served (Theme 2). This team-based constraint corresponds with trialists’ concerns that health system practices conflict with equity-relevant practices24 and highlights the challenging nature of pragmatic trial design where embedded teams are often utilized. Traditional explanatory and translational trials may face fewer team selection barriers than investigator-driven pragmatic trials given their departure from routine processes.
Trialists’ attempts to align investigator priorities with community (Theme 3) underscore the need for restructured funding mechanisms. Investigator-driven pragmatic designs lack inherent power-sharing, community-centered questions, and social change objectives, all hallmarks of community-based participatory research, making intentional alignment more difficult.38,39 Funders should allocate time in a grant’s lifecycle for developing community relationships, designing equitable trials, and building research teams with shared community identity. These strategies are foundational to designing for equity and may reduce future time pressures. Otherwise, tight timelines favor working with established groups and practices.
Theme 4, which describes flexible interventions as critical for participant engagement, refutes the notion that “clinically embedded” and “flexible” cannot coexist in pragmatic trial design and that pragmatic trials are only accessible insofar as barriers to care are reduced.23 Flexible interventions are desired by pragmatic trial participants and enhance accessibility,40 help mitigate systemic barriers to care, and optimize the potential for all to benefit from the intervention (eg, extending benefits to the control condition), particularly for populations most affected by the conditions under study. Flexibility to enhance equity may be more acceptable in pragmatic than explanatory randomized trials since pragmatic designs prioritize real-world applicability and feasibility while explanatory trials prioritize internal validity. Sharing resources across arms as our trialists mentioned can improve equity and external validity if transparently documented and analytically addressed.
This study addresses a critical gap in the literature. While many call for increased attention to health equity in trials, few assess the experiences of pragmatic trialists implementing it in teams and designs. Understanding our trialists’ broad definitions of health equity was essential, as was ensuring team consensus to facilitate data generation and analysis. This reflects health equity’s complex development, particularly in the United States,6 where changes in government priorities revoked NIH health equity consideration in 2025.41–45 Providing resources and training to increase trialists’ capacity to integrate health equity is foundational to scientific equity and optimizing trial benefits for all populations. The DUSON-INFUSE checklist,29 one component of a health equity toolkit, can guide pragmatic trialists to design for equity.
Limitations
Diverse trial representation enhances transferability but limits in-depth examination of specific conditions and populations; findings may not generalize to other trial designs. Additionally, we interviewed trialists throughout the research lifecycle. Interviewing trialists across the research lifecycle introduced recall bias for completed projects, some of which had concluded years ago. Only one trialist was a research associate, and findings may be skewed toward principal investigator perspectives. The sampling method may have missed enriching perspectives. Importantly, our findings should be interpreted in light of recent federal removal of NIH health equity and diversity requirements,41–45 which has created investigator confusion and hesitancy about explicitly incorporating equity in research and reduced funding for health equity-focused research. Because our trialists described funding as important for equity-focused design, findings must be evaluated within this shifting policy context.
Future Directions
Most trialists agreed that equitable recruitment and enrollment are ethically essential and strengthen research relevance. Trialists used diverse methods such as providing broadband and other technology access and support, flexible scheduling, and culturally concordant staff. However, trialists need to go beyond these strategies to address equity more holistically.
Future studies should harness the experience of research associates and front-line implementers who navigate the gap between ideal design and real-world practice. New methods are needed to address equity beyond recruitment, particularly for pragmatic trials, where integration with clinical settings creates distinct challenges around funding, institutional policies, and hierarchical cultures. Exploring these trade-offs will enable trialists to conduct trials that are both pragmatic and aligned with a public health mission to reduce health inequities and improve health for all.
Conclusion
This study identifies barriers and facilitators to advancing health equity through pragmatic trials, which minimize friction and burden compared to traditional studies by operating within existing ecosystems. Pragmatic trialists’ real-world experience demonstrates that health equity can and is addressed within pragmatic designs, despite initial assumptions to the contrary. Community alignment and representation in research is paramount but nuanced. Building health equity into trials takes time and intentionality, and it must be reflected in funding timelines and research budget prioritization, otherwise inequities will persist.
Abbreviations
NIH, National Institutes of Health; DUSON-INFUSE, Duke University School of Nursing-Implementing a New Focus on Equity in Research; PI, principal investigator; RA, research associate.
Data Statement
Data will be made available upon request by contacting author Kaitlyn R. McLeod.
Ethics Statement
This study was approved by the Duke University Health Systems Institutional Review Board, protocol Pro00085360, including verbal consent. Consent was obtained for all study participants prior to study commencement. Study participants consented to participation, publication of direct quotes, and possibility of loss of anonymity due to the unique aspects of each trial and the number of trials in the NIH Collaboratory.
Acknowledgments
The authors wish to thank their NIH Collaboratory colleagues and trialists participating in the study, as well as our peer reviewers.
Funding
This work was supported within the National Institutes of Health (NIH) Pragmatic Trials Collaboratory through cooperative agreement U24 AT009676 from the National Center for Complementary and Integrative Health (NCCIH), the National Institute of Allergy and Infectious Diseases (NIAID), the National Cancer Institute (NCI), the National Institute on Aging (NIA), the National Heart, Lung, and Blood Institute (NHLBI), the National Institute of Nursing Research (NINR), the National Institute of Minority Health and Health Disparities (NIMHD), the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), the NIH Office of Behavioral and Social Sciences Research (OBSSR), and the NIH Office of Disease Prevention (ODP). This work was also supported by the NIH through the NIH HEAL Initiative under award number U24 AT010961. The content is solely the responsibility of the authors and does not necessarily represent the official views of NCCIH, NIAID, NCI, NIA, NHLBI, NINR, NIMHD, NIAMS, OBSSR, or ODP, or NIH or its HEAL Initiative.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bunnell R, Ryan J, Kent C. CDC office of science and CDC excellence in science committee. Toward a new strategic public health science for policy, practice, impact, and health equity. Am J Public Health. 2021;111(8):1489–11. doi:10.2105/AJPH.2021.306355
2. Srinivasan S, Williams SD. Transitioning from health disparities to a health equity research agenda: the time is now. Public Health Rep. 2014;129(2):71–76. doi:10.1177/00333549141291S213
3. Henry BV, Chen H, Edwards MA, Faber L, Freischlag JA. A new look at an old problem: improving diversity, equity, and inclusion in scientific research. Am Surg. 2021;87(11):1722–1726. doi:10.1177/00031348211029853
4. Warnecke RB, Oh A, Breen N, et al. Approaching health disparities from a population perspective: the National Institutes of Health Centers for Population Health and Health Disparities. Am J Public Health. 2008;98(9):1608–1615. doi:10.2105/AJPH.2006.102525
5. World Health Organization. Health equity. Available from: https://www.who.int/health-topics/health-equity#tab=tab_1.
6. Braveman P. Health inequalities, disparities, equity: what’s in a name? Am J Public Health. 2025;115(7):996–1002. doi:10.2105/AJPH.2025.308062
7. Lewis CL, Yan A, Williams MY, et al. Health equity: a concept analysis. Nursing Outlook. 2023;71(5):102032. doi:10.1016/j.outlook.2023.102032
8. Weiss EM, Porter KM, Sullivan TR, et al. Equity concerns across pediatric research recruitment: an analysis of research staff interviews. Academic Pediatrics. 2024;24(2):318–329. doi:10.1016/j.acap.2023.06.032
9. Quiñones AR, Mitchell SL, Jackson JD, et al. Achieving health equity in embedded pragmatic trials for people living with dementia and their family caregivers. J Am Geriatrics Soc. 2020;68(S2). doi:10.1111/jgs.16614
10. Scaffidi J, Mol B, Keelan J. The pregnant women as a drug orphan: a global survey of registered clinical trials of pharmacological interventions in pregnancy. BJOG. 2017;124(1):132–140. doi:10.1111/1471-0528.14151
11. Welch MJ, Lally R, Miller JE, et al. The ethics and regulatory landscape of including vulnerable populations in pragmatic clinical trials. Clin Trial. 2015;12(5):503–510. doi:10.1177/1740774515597701
12. Duma N, Vera Aguilera J, Paludo J, et al. Representation of minorities and women in oncology clinical trials: review of the past 14 years. J Oncol Pract. 2018;14(1):e1–e10. doi:10.1200/JOP.2017.025288
13. Gong IY, Tan NS, Ali SH, et al. Temporal trends of women enrollment in major cardiovascular randomized clinical trials. Can J Cardiol. 2019;35(5):653–660. doi:10.1016/j.cjca.2019.01.010
14. Khan MS, Shahid I, Siddiqi TJ, et al. Ten-year trends in enrollment of women and minorities in pivotal trials supporting recent us food and drug administration approval of novel cardiometabolic drugs. J Am Heart Assoc. 2020;9(11):e015594. doi:10.1161/JAHA.119.015594
15. National Academies of Sciences. Engineering, and Medicine; Policy and Global Affairs; Committee on Women in Science, Engineering, and Medicine; Committee on Improving the Representation of Women and Underrepresented Minorities in Clinical Trials and Research. In: Bibbins-Domingo K, Helman A, editors. Improving Representation in Clinical Trials and Research: Building Research Equity for Women and Underrepresented Groups. Washington (DC): National Academies Press (US). 2022.
16. Varma T, Jones CP, Oladele C, Miller J. Diversity in clinical research: public health and social justice imperatives. J Med Ethics. 2023;49(3):200–203. doi:10.1136/medethics-2021-108068
17. Haidich AB, Ioannidis JP. Patterns of patient enrollment in randomized controlled trials. J Clin Epidemiol. 2001;54(9):877–883. doi:10.1016/s0895-4356(01)00353-5
18. Hill KA, Desai MM, Chaudhry SI, Nguyen M, Boatright D. NIH diversity supplement awards by year and administering institute. JAMA. 2021;326(23):2427–2429. doi:10.1001/jama.2021.19360
19. Ginther DK, Schaffer WT, Schnell J, et al. Race, ethnicity, and NIH research awards. Science. 2011;333(6045):1015–1019. doi:10.1126/science.1196783
20. Rogers J, Kelly UA. Feminist intersectionality: bringing social justice to health disparities research. Nurs Ethics. 2011;18(3):397–407. doi:10.1177/0969733011398094
21. Gilmore-Bykovskyi A, Croff R, Glover CM, et al. Traversing the aging research and health equity divide: toward intersectional frameworks of research justice and participation. Meeks S, ed. Gerontologist. 2022;62(5):711–720. doi:10.1093/geront/gnab107
22. Ali J, Davis AF, Burgess DJ, et al. Justice and equity in pragmatic clinical trials: considerations for pain research within integrated health systems. Learn Health Syst. 2022;6(2):e10291. doi:10.1002/lrh2.10291
23. Dember LM. The potential for pragmatic trials to reduce racial and ethnic disparities in kidney disease. J Am Soc Nephrol. 2022;33(9):1649–1651. doi:10.1681/ASN.2022030301
24. Pauly B, Revai T, Marcellus L, Martin W, Easton K, MacDonald M. “The health equity curse”: ethical tensions in promoting health equity. BMC Public Health. 2021;21(1):1567. doi:10.1186/s12889-021-11594-y
25. Nicholls SG, Al-Jaishi AA, Niznick H, et al. Health equity considerations in pragmatic trials in Alzheimer’s and dementia disease: results from a methodological review. Alz Dem Diag Ass Dis Mo. 2023;15(1):e12392. doi:10.1002/dad2.12392
26. Booker SQ, Baker TA, Esiaka D, et al. A historical review of pain disparities research: advancing toward health equity and empowerment. Nursing Outlook. 2023;71(3):101965. doi:10.1016/j.outlook.2023.101965
27. Chin MH, Clarke AR, Nocon RS, et al. A roadmap and best practices for organizations to reduce racial and ethnic disparities in health care. J Gen Intern Med. 2012;27(8):992–1000. doi:10.1007/s11606-012-2082-9
28. Byrd JT, Daniels CL, Flores DD, et al. Establishing a research racial justice task force to improve diversity, equity, and inclusion in nursing research. Nurs Outlook. 2022;70(5):758–761. doi:10.1016/j.outlook.2022.06.004
29. Center for Nursing Research Racial Justice Taskforce. In: DUSON-INFUSE Checklist. Duke University School of Nursing; 2022.
30. Kowalski CP, Nevedal AL, Finley EP, et al. Planning for and assessing rigor in rapid qualitative analysis (PARRQA): a consensus-based framework for designing, conducting, and reporting. Implement Sci. 2024;19(1):71. doi:10.1186/s13012-024-01397-1
31. Hamilton AB, Finley EP. Qualitative methods in implementation research: an introduction. Psychiatry Res. 2019;280:112516. doi:10.1016/j.psychres.2019.112516
32. St George SM, Harkness AR, Rodriguez-Diaz CE, Weinstein ER, Pavia V, Hamilton AB. Applying rapid qualitative analysis for health equity: lessons learned using “ears” with Latino communities. Int J Qual Methods. 2023;22. doi:10.1177/16094069231164938
33. Malterud K, Siersma VD, Guassora AD. Sample size in qualitative interview studies: guided by information power. Qual Health Res. 2016;26(13):1753–1760. doi:10.1177/1049732315617444
34. National Institutes of Health. Activity codes. Available from: https://grants.nih.gov/funding/activity-codes.
35. Glesne C. Becoming Qualitative Researchers: An Introduction.
36. Suzuki LA, Ahluwalia MK, Arora AK, Mattis JS. The pond you fish in determines the fish you catch: exploring strategies for qualitative data collection. Counsel Psychol. 2007;35(2):295–327. doi:10.1177/0011000006290983
37. Tracy SJ. Qualitative quality: eight “big-tent” criteria for excellent qualitative research. Qual Inq. 2010;16(10):837–851. doi:10.1177/1077800410383121
38. Wallerstein N, Oetzel JG, Sanchez-Youngman S, et al. Engage for equity: a long-term study of community-based participatory research and community-engaged research practices and outcomes. Health Educ Behav. 2020;47(3):380–390. doi:10.1177/1090198119897075
39. Wallerstein N, Duran B. Community-based participatory research contributions to intervention research: the intersection of science and practice to improve health equity. Am J Public Health. 2010;100(S1):S40–S46. doi:10.2105/AJPH.2009.184036
40. Harr ED, Rodriguez RD, Baez JE, et al. Increasing equity within randomized control trials: a qualitative analysis of focus groups from a multi-site, pragmatic clinical trial. Global Adv Integrat Med Health. 2025;14:27536130251349111. doi:10.1177/27536130251349111
41. National Institutes of Health v American Public Health Association. 601 (Supreme court of the United States 2025). Available from: https://www.supremecourt.gov/docket/docketfiles/html/public/25a103.html.
42. United States. Executive order 14332: improving oversight of federal grantmaking. 2025. Available from: https://www.federalregister.gov/documents/2025/08/12/2025-15344/improving-oversight-of-federal-grantmaking.
43. United States. Executive order 14151: ending radical and wasteful government DEI programs and preferencing. 2025. Available from: https://www.federalregister.gov/documents/2025/01/29/2025-01953/ending-radical-and-wasteful-government-dei-programs-and-preferencing.
44. United States. Executive order 14168: defending women from gender ideology extremism and restoring biological truth to the federal government. 2025. Available from: https://www.federalregister.gov/documents/2025/01/30/2025-02090/defending-women-from-gender-ideology-extremism-and-restoring-biological-truth-to-the-federal.
45. United States. Executive order 14173: ending illegal discrimination and restoring merit-based opportunity. 2025. Available from: https://www.federalregister.gov/documents/2025/01/31/2025-02097/ending-illegal-discrimination-and-restoring-merit-based-opportunity.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025