")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Barriers and Enablers to Pulmonary Rehabilitation in Low- and Middle-Income Countries: A Qualitative Study of Healthcare Professionals
Authors Bickton FM , Shannon H
Received 10 November 2021
Accepted for publication 24 December 2021
Published 13 January 2022 Volume 2022:17 Pages 141—153
DOI https://doi.org/10.2147/COPD.S348663
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Min Zhang
Fanuel Meckson Bickton,1,2 Harriet Shannon1
1UCL Great Ormond Street Institute of Child Health, London, UK; 2Lung Health Research Group, Malawi-Liverpool-Wellcome Trust Clinical Research Programme, Blantyre, Malawi
Correspondence: Fanuel Meckson Bickton
Lung Health Research Group, Malawi-Liverpool-Wellcome Trust Clinical Research Programme, P.O. Box 30096, Chichiri, Blantyre 3, Malawi
Tel +265 982 55 23 53
Email [email protected]
Introduction: Low- and middle-income countries bear a disproportionately high burden of global morbidity and mortality caused by chronic respiratory diseases. Pulmonary rehabilitation is recommended as a core intervention in the management of people with chronic respiratory diseases. However, the intervention remains poorly accessed/utilised globally, especially in low- and middle-income countries.
Aim: This qualitative study explored barriers and enablers to pulmonary rehabilitation in low- and middle-income countries from the perspective of healthcare professionals with pulmonary rehabilitation experience in these settings.
Methods: Online-based semi-structured in-depth interviews with healthcare professionals were undertaken to data saturation, exploring lived barriers and enablers to pulmonary rehabilitation in their low- or middle-income country. Anonymised interviews were audio-recorded, transcribed verbatim, and analysed using thematic analysis.
Results: A total of seven healthcare professionals from seven low- and middle-income countries representing Africa, Asia, and South America were interviewed. They included five physiotherapists (four females), one family physician (male), and one pulmonologist (female). Themes for barriers to pulmonary rehabilitation included limited resources, low awareness, coronavirus disease 2019, and patient access-related costs. Themes for enablers included local adaptation, motivated patients, coronavirus disease 2019 (which spanned both enablers and barriers), better awareness/recognition, provision of PR training, and resource support.
Conclusion: Barriers to pulmonary rehabilitation in low- and middle-income countries include limited resources, low awareness, coronavirus disease 2019, and patient access-related costs. Enablers include local adaptation, motivated patients, coronavirus disease 2019 (which spanned both enablers and barriers), better awareness/recognition, provision of PR training, and resource support. Successful implementation of these enablers will require engagement with multiple stakeholders. The findings of this study are a necessary step towards developing strategies that can overcome the existing pulmonary rehabilitation evidence-practice gap in low- and middle-income countries and alleviating the burden of chronic respiratory diseases in these countries.
Keywords: chronic respiratory diseases, pulmonary rehabilitation, low-income countries, middle-income countries, barriers, enablers
Introduction
Pulmonary rehabilitation (PR) is a core component in the management of people with chronic respiratory diseases (CRDs). It is defined as
a comprehensive intervention based on a thorough patient assessment followed by patient-tailored therapies, which include, but are not limited to, exercise training, education, and behaviour change, designed to improve the physical and psychological condition of people with chronic respiratory disease and to promote the long-term adherence of health-enhancing behaviours.1
PR leads to significant reductions in symptoms such as dyspnoea, fatigue, anxiety and depression, and significant improvements in exercise tolerance and overall health-related quality of life.2 Data from high-income countries suggest that it also significantly reduces the direct costs of chronic obstructive pulmonary disease (COPD) by decreasing unnecessary use of the healthcare system, particularly unplanned hospital admissions.3 While the bulk of this evidence is based on those with COPD,2 there is also evidence supporting effectiveness of PR in people with other CRDs including asthma,4 post-tuberculosis lung disease5 and bronchiectasis.6 In addition, PR is cost-effective as it may be delivered using minimal, low-cost equipment, making its implementation feasible even in low- and middle-income countries (LMICs) where access to specialist exercise equipment may be limited.7,8
Although PR is recommended in various national and international guidelines for the management of people with CRDs, notably COPD and bronchiectasis,3,9 it remains poorly accessed or underutilised around the world.3,10,11 Specifically, referral and patient uptake is poor.12 In addition, although it is LMICs that are disproportionately burdened by CRDs,13 current PR evidence is mainly based on studies from high income countries.14 Of the eight papers exploring barriers and enablers to PR, none were from LMICs.10,12,15–20 LMICs have different challenges to high income countries in terms of access to resources, meaning that current literature cannot be generalised. Moreover, it has been reported that clinical PR services are not widely available in LMICs21 due to certain barriers. This study aimed to explore those barriers (and enablers) to PR in LMICs from the perspective of health professionals with PR work experience in these countries. This would be a necessary step towards developing strategies that can overcome the existing PR evidence-practice gap.10
Methods
Study Design
This was a qualitative, interview-based study. This method permitted an in-depth exploration of participants’ lived experiences in implementing or delivering PR in an LMIC setting.22 One-to-one semi-structured interviews with participants elicited individual participant insights into their experiences regarding barriers and enablers to PR in their respective LMIC.23,24
Participant Recruitment
Participants were purposively recruited with the inclusion criteria being healthcare professionals with experience in implementing or delivering PR in LMICs. Participants were identified from papers included in two recent systematic reviews on PR in low resource settings,14,25 and the Global RECHARGE network.26 Recruitment emails were sent to the corresponding authors of the papers, along with a consent form, participant information sheet and request to disseminate the invitation to their colleagues. Further to this, an open invitation was posted on Twitter.
Data Collection
Interviews used a topic guide (Supplementary Material 1) informed by published literature and piloted a priori, encompassing open questions around barriers and enablers to PR in an LMIC. The topic guide underwent several stages of development as follows:
- It was first drafted by the lead researcher/author (FMB), followed by senior peer review and suggestions for improvement by his supervisor (HS).
- FMB revised the topic guide accordingly, the outcome of which was the second draft.
- The second draft was then piloted by administering it to FMB’s classmate on the UCL MSc physiotherapy programme in an hour practice in-depth interview on Zoom, in the presence of HS.
- After the pilot session, HS gave FMB feedback to improve the conduct of the interview.
Information regarding each participant’s profession and experience in implementing or delivering PR in their LMIC was also collected. Interviews were conducted at a time and via an online platform (either Microsoft Teams or Zoom) of each participant’s preference or convenience. It had been pragmatically planned that at least six participants would be recruited, as evidence suggests that that a sample of six interviews may have been sufficient to enable development of meaningful themes and useful interpretations.27 However, our final sample size was determined by code and thematic saturation, that is, a point at which no new codes or themes, respectively, are observed in the interview data.28 The lead researcher (FMB) is a qualified physiotherapist with qualitative research experience.29
Data Management and Analysis
Interviews were audio- and video-recorded and later transcribed verbatim. The transcripts were anonymised and compared with the audio interview recordings for completeness and accuracy. Subsequently, transcripts were imported into QSR International’s NVivo 12 qualitative data analysis software for iterative line-by-line coding and inductive thematic analysis30 across all interview data. This involved the lead researcher’s familiarisation with the entire interview data set, by reading and re-reading the transcripts while making reflective notes on the literal content, looking closely at words used by participants, interpreting what the data meant by assigning initial codes or classifications to segments of text, and exploring relationships between these classifications and reducing them to core general themes. Then, the senior author (HS, lead researcher’s supervisor) checked both the codes and themes against the transcripts to confirm that they were accurate and representative of the participants’ views. The identified key themes were refined for referential adequacy by returning to the raw data. Participants’ quotations from the transcripts were extracted to provide supporting data for each final theme when narrating findings.
Results
Results from the participant recruitment process are shown in Figure 1. In summary, a total of seven healthcare professionals from seven LMICs, representing South America, Africa, and Asia, were interviewed.
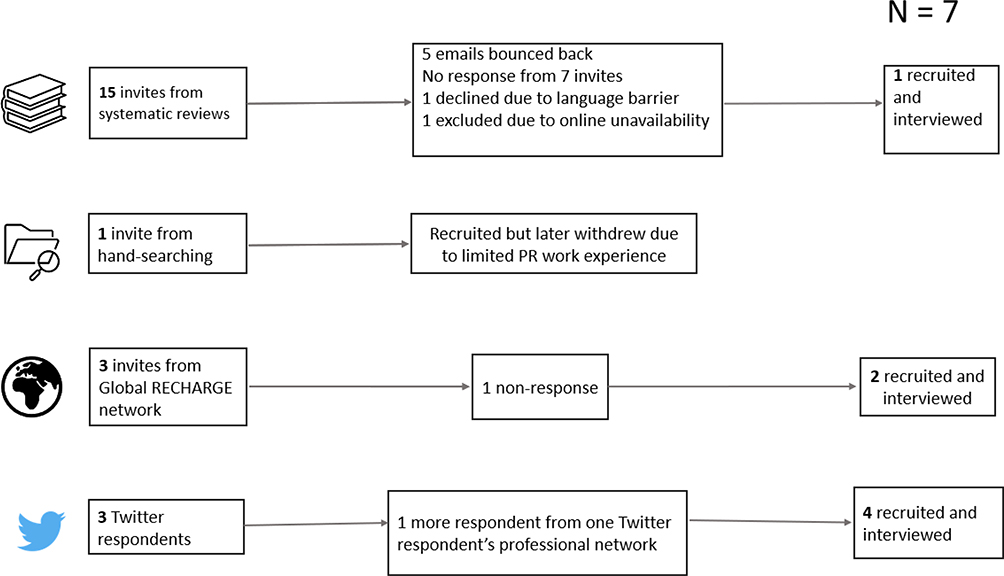 |
Figure 1 Participant recruitment process. |
Countries from Asia were Kyrgyzstan and India, from South America was Argentina, and from Africa were Kenya, Malawi, South Africa, and Zimbabwe (Figure 2).
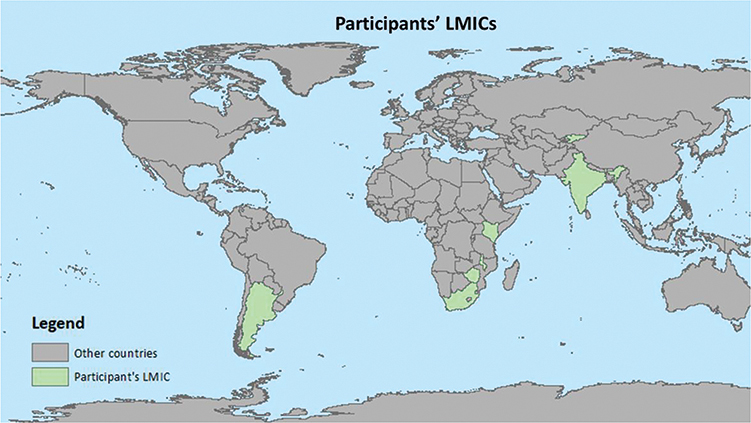 |
Figure 2 Participants’ LMICs. |
Of the seven interviews, four were conducted on Zoom while three were conducted on Microsoft Teams. On average, each interview lasted for 40 minutes (ranging from 20 to 60 minutes). Five of the participants were physiotherapists (four females), one was a family physician (male), and one was a pulmonologist (female).
Of the five physiotherapists, two were respiratory physiotherapists, one was a sports physiotherapist, one was a public health specialist researching the implementation of PR, and one was a professor of PR. All physiotherapists had PR experience in either a clinical or research context within their respective LMIC. Four physiotherapists had experience in implementing and/or delivering a structured PR programme, while one had practised some aspects of PR as part of their broader cardiorespiratory physiotherapy practice. The pulmonologist was leading an ongoing randomised controlled trial of a PR programme, with their roles including leading the exercise component. The family physician had no prior experience with PR but had previously offered research support as a co-supervisor on a student-led PR research project.
Key themes relating to barriers to PR in LMICs were limited resources, low awareness or recognition, Coronavirus Disease 2019 (COVID-19), and patient-unique access barriers (Table 1). Key themes for enablers were local adaptation, motivated patients, COVID-19, better awareness or recognition, available PR training, and available PR resource support (Table 1).
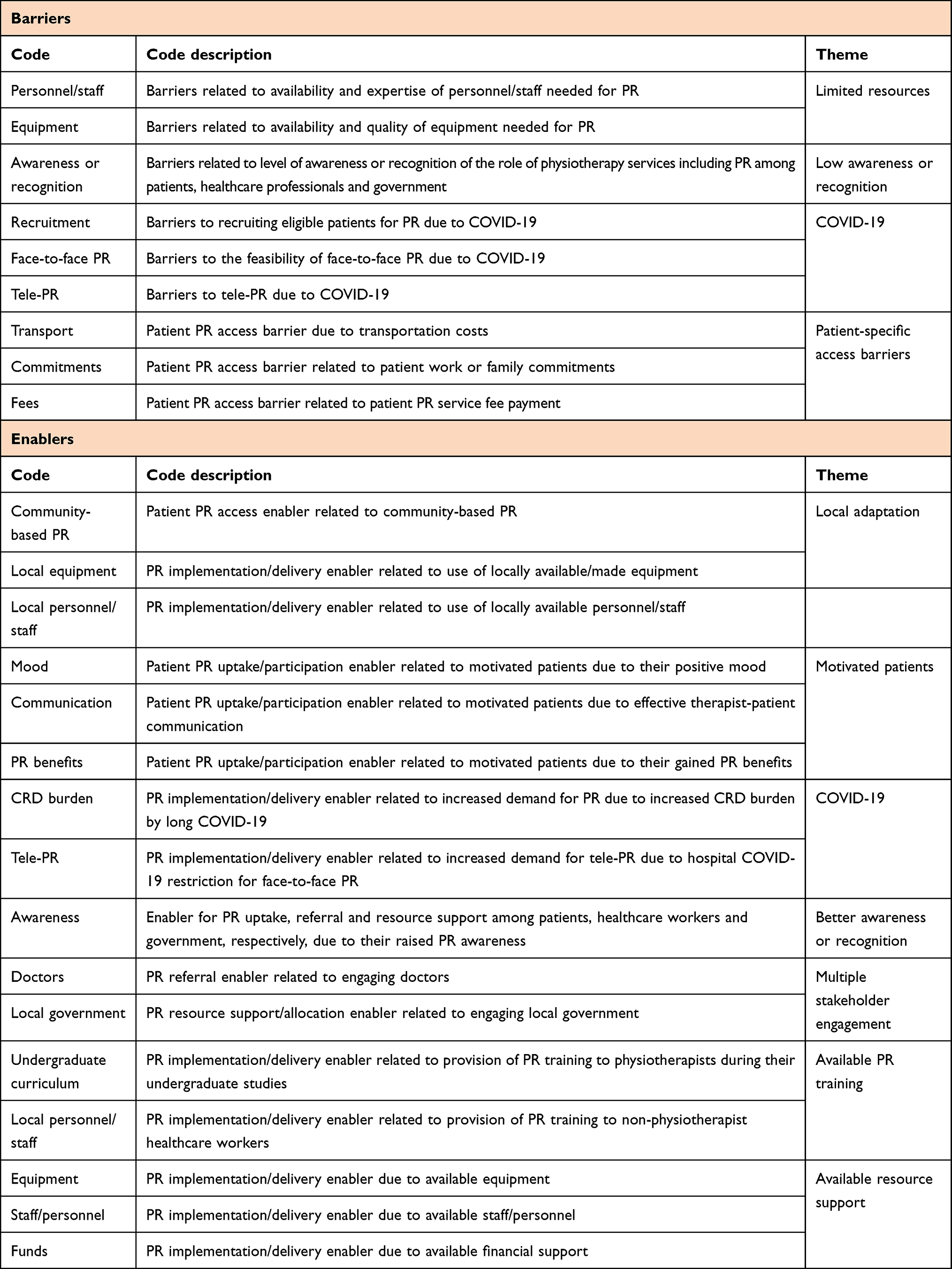 |
Table 1 Codes and Themes That Resulted from the Thematic Analysis |
Barriers
Theme 1: Limited Resources
Participants expressed limited availability of various resources needed to implement and deliver PR as a barrier. The first resource barrier was the shortage of rehabilitation professionals, specifically physiotherapists, who would implement and deliver PR in their setting:
…there are few physiotherapists doing this practice. It’s difficult to find a skilled physiotherapist to do the work. (Argentina participant)
Participants also mentioned a lack of PR knowledge or expertise in PR among the healthcare professionals as another barrier:
…there was nobody who was like you… there was a physio, but they had never heard of pulmonary rehab. So, they did lots of outpatient stuff and parks and all of that, but their respiratory knowledge was next to zero…. (Kenya participant)
Participants attributed this lack of knowledge or expertise to the lack of PR training in their national undergraduate physiotherapy curriculum:
I don’t think they are aware that there’s a whole field of rehabilitation, no. I think part of that is because it’s not part of the curriculum… I think there’s an important gap in the training that’s being offered. (South Africa participant)
Another resource barrier was limited equipment. Either the equipment was not available or, where available, minimal, or of low quality, or could not be utilised:
…you can’t be saying I’m going to use a treadmill because you may not have one. Or in Zimbabwe’s case… you can have that…, but there might be no electricity. (Zimbabwe participant)
This equipment barrier was attributed to the lack of financial support needed to purchase it. For example, in Argentina, patients had to donate funds to purchase the equipment:
…almost all the equipment is donated by the patients… we done collects [donations], so we can purchase some more equipment…. it’s hard to have the hospital to buy the equipment… (Argentina participant)
Theme 2: Low Awareness or Recognition
Another barrier expressed by participants was a general lack of awareness or recognition of CRDs, physiotherapy profession and its services including PR. For example, at the patient level, two participants said the following:
So, the funny part is it is available, but the patients do not know that this is pulmonary rehabilitation. If we ask them, “Have you heard of pulmonary rehabilitation?”, and they would go, “Oh no what is that?” (India participant).
…but the people whom you expected to serve don’t know what we do. And as a result, they don’t understand why we’re important. (Zimbabwe participant)
At the healthcare professional level, one participant said the following:
I think many clinicians, especially doctors, are not aware of what the modality of pulmonary rehabilitation is and what it can offer. Typically, if somebody comes with chest problems, the treatment is inhalers and maybe some other medications to open up the airways. (South Africa participant)
At the national health policy level, one participant said:
The national health policy itself has only one word on chronic respiratory diseases that we would want to cover the management for – COPD. And not even all respiratory diseases. It’s just COPD…. and there is hardly any mention of rehab in the health policy itself. (India participant)
Consequently, this lack of awareness or recognition results in government’s low resource support for physiotherapy services including PR:
And that then translates to government policy. So, when the people on the ground have no idea who you are, the MP in government has no idea who you are. The Minister of Health does not quite understand why we’re making a fuss about you. So, when it comes to budgeting and they only have ten dollars and they have to split it amongst all the health professions, they’re going to think about their doctors, their nurses and pharmacists, you know.… So, because people hardly don’t understand what we do, we are left on the wayside. (Zimbabwe participant)
Theme 3: COVID-19
The restrictions associated with the ongoing COVID-19 pandemic have resulted in low recruitment of eligible patients for PR in LMICs:
Initially, we were supposed to do a face-to-face intervention. But after COVID set in, we are still not allowed to have a lot of patients in one room because they are at risk of contracting the infection. (India participant)
The pandemic has also challenged the expertise of delivering the conventional face-to-face PR. Therefore, some face-to-face PR programmes have been moved to online delivery. However, participants expressed barriers for this delivery model too, including lack of digital access and illiteracy:
…many patients are illiterate… cannot read or write. A second biggest challenge is they don’t have their own smartphones from where we are expecting them to access this web application. (India participant)
Theme 4: Patient Direct and Indirect Costs
Finally, participants mentioned patient direct and indirect costs that are barriers to PR access, including transport costs associated with long distance to travel to a healthcare facility to access PR (direct cost), PR service fees (direct cost), and loss of income due to work time lost to attending PR (indirect cost):
…other people come from far areas… So, transportation costs… can exist as a barrier to participation. (Malawi participant)
So, twice a week you are asking them to forego potential income because Zimbabwe has a 90 percent unemployment rate. So, that means everyone is well just about everyone is self-employed. So, if you don’t work, you don’t earn money and they’re not going to be spending two days a week lining up in a hospital queue to get treatment, that they figure their body will just you know, it will resolve itself. (Zimbabwe participant)
It’s not free. So, it’s either insurance in Kenya, something called NHIS, or patients have to pay, so that is another issue. (Kenya participant)
More participants’ quotes for barriers themes can be found in Supplementary Material 2.
Enablers
Theme 1: Local Adaptation
Despite barriers, participants felt that PR implementation and delivery in their respective LMIC was possible if the intervention could be adapted to their local context. This included use of a community-based PR model to address the transport barrier:
…actually, there wouldn’t be anything stopping a hospital team going to a community health centre once a week and doing it there. And I think that might be better than making the patients pay for transport. (Kenya participant)
Local adaptation also meant the use of locally available staff and equipment:
Community health workers could be trained to guide people in this and be involved with community rehabilitation or pulmonary rehabilitation… it doesn’t have to be a physiotherapist in my mind… If you can have services in the community, people will be more likely to access it. (South Africa participant)
…looking at the equipment for exercise therapy, we manufactured them locally using the locally available resources… for strength training, we actually had to hire a tailor from the village, and he brought his own machine and we just had to go to kaunjika (market) and buy zitenje (cloth) and cut them off into pieces that can accommodate 1kg, 1/2 kg, 2kg, 3kg up to 8kg using sand. (Malawi participant)
Theme 2: Motivated Patients
Participants also described increased motivation of their patients to participate in PR as a facilitator. Several factors contributed to patient motivation including good therapist-patient relationship:
…it’s patients’ mood … patients were really, really enthusiastic and really interested to take part in this study…. It was really easy to communicate with patients…. before the trial, we ask for consent from patients and also ask them what time is more convenient for them when they can participate in our PR trial… So, it was discussed with patients, and they feel themselves really comfortable for this and they find it convenient. (Kyrgyzstan participant)
Some specific components of the PR programme and associated benefits also contributed to patient motivation to participate:
I think the facilitators for patients is that they feel well, they notice that they feel well. And that made that they want to continue to the program with the program… group effect of the sessions…, the dynamic of the session. We try to do a diversity… We don’t do unique training method; we try to use other methods in the programs that the patient feel that they do not do a routine training … (Argentina participant)
Theme 3: COVID-19
Although COVID-19 was perceived as a barrier to PR, also it was also perceived as a facilitator. Specifically, long COVID-19 is an extra CRD burden, thereby increasing the demand for PR, especially tele-PR:
I’ve got a friend that’s got long covid that’s affected her lungs. At this stage, she is using her cell phone to message her children because she gets tired of speaking. She is in desperate need of pulmonary rehab. It’s not available to her …. She’s got to use the Internet …. I think we can use technology. We are having this conversation on two different continents so pulmonary rehabilitation can be done by video conference. I can’t see why not. I think training videos can be made. (South Africa participant)
Theme 4: Better Awareness or Recognition
Participants suggested several ways to improve public awareness and recognition of physiotherapy services such as PR, including public awareness campaigns:
I suppose this would involve a lot of public campaigns… to just enable the public to understand the role of physiotherapy in general and then the role of cardiopulmonary rehabilitation in improving health outcomes. (Zimbabwe Participant)
Such better awareness could potentially increase patient referral for PR among health practitioners:
…medical practitioners and other practitioners know what it entails and what it can offer patients, I think they’d be more likely to prescribe it and to make it to get services running. (South Africa participant)
Theme 5: Multiple Stakeholder Engagement
Participants also hinted the importance of engaging and seeking support of multiple stakeholders to successfully implement PR. These included various members of the multidisciplinary team, such as doctors, and local governments:
…we work together with the doctor that refers the patient with an order of pulmonary rehab. They send the patient with a spirometry (as a minimum), cardiological studies (investigations) so that the patient is able to do the training sessions. (Argentina participant)
So, it actually needs some advocacy and rehabilitation practitioners to engage with governments and provincial decision makers. Those that allocate resources. (South Africa participant)
Theme 6: Available PR Training
Participants also expressed the need for formal training in PR for both physiotherapists and healthcare workers of other cadres including community healthcare workers, doctors, and occupational therapists:
I think also at a training level, the physios need more training… because there’s no point foreigners delivering it. That’s just silly. (Kenya participant)
…if the physiotherapist leaves, then it’s a program that needs to be run by occupational therapist to maybe even one of the doctors or somebody else that needs to initiate it and get things going. So, in low- and middle-income countries, transdisciplinary practice is actually not an option. It’s something we have to build into our curriculum and training… Community health workers could be trained to guide people in this and be involved with community rehabilitation or pulmonary rehabilitation… it doesn’t have to be a physiotherapist in my mind. (South Africa participant)
Theme 7: Available Resource Support
Wherever participants had been able implement and deliver PR successfully, it was because they had resource support in the form of equipment, funds, and staff:
…they help us with the equipment because, you know, we are a developing country. So, we don’t have much money for… yes, financial support for this. So, they give us support, there is a room, there is corridors… our room is already equipped… So, we have enough staff, actually, who really want to participate, to work, to take a salary. (Kyrgyzstan participant)
More participants’ quotes for enabler themes can be found in Supplementary Material 3.
Discussion
This study identified a shortage of healthcare professionals, particularly physiotherapists, as a barrier to PR in LMICs. An important aim of PR is to increase exercise tolerance and functional ability for people limited by their CRD.31 As such, exercise training is a core component of PR which should be prioritised32 and physiotherapists are responsible for supervising this component as they are trained in exercise testing, prescription, and training.32,33 The shortage of physiotherapists in LMICs found in this study corroborates previous evidence; the WHO reported that although there is no universally agreed or recommended minimal number of physiotherapists, the critical shortage of these professionals in LMICs is evident, with fewer than 10 physiotherapists per million inhabitants in many countries in the South of Africa’s Sahara and the South-East Asia Region.34
This study also found a lack PR knowledge or expertise among the available LMIC physiotherapists as another barrier to PR in LMICs. Participants attributed this barrier to a lack of PR training in the physiotherapy undergraduate curriculum. Noteworthy, this training gap is reported to exist in most countries worldwide.35 However, it is more evident in LMICs, especially in the African, Eastern Mediterranean, and South-East Asia regions, where the general current workforce of “skilled” rehabilitation professionals does not necessarily meet the needs of the population.34 Therefore, participants in this study recommended inclusion of formal PR training in their undergraduate training of physiotherapists and other healthcare workers as part of interprofessional education. This is in line with the American Thoracic Society/European Respiratory Society policy statement for enhancing the implementation, use and delivery of PR, which recommends formal training in PR for any healthcare professionals involved in the care of people with COPD.35
Another barrier to PR in LMICs reported by participants in this study was low awareness or recognition of PR by the public including people with CRDs, healthcare professionals and governments. The public is less aware or cognisant of physiotherapy services in their country, including PR. This results in low uptake, attendance, and adherence to PR by people with CRDs as they are not aware of its benefits, a finding that has also been reported elsewhere.36 Participants also said this lack of awareness exists among the healthcare professionals, for example some doctors, which results in fewer referrals of patients with CRDs to a PR programme. This finding is consistent with a Lebanese study which attributed lack of patient referral to PR by chest physicians to absence of awareness and education about PR.37
Consequently, the lack of awareness of PR benefits or value translates into under-funding or under-resource allocation for the service. This is not surprising because LMIC governments have restricted budgets and must prioritise investment in healthcare interventions that are perceived as “high-value”.38 Government authorities cannot perceive PR as a high-value intervention if they are not aware or knowledgeable about its benefits in the first place.
In addition, healthcare services in LMICs compete for resources and, as with other health interventions that require long-term investment, rehabilitation services such as PR appear less attractive than interventions that produce immediate results.39 The primary healthcare needs of populations in LMICs may be so great that attending to people with CRDs feels like a luxury.40 This, coupled with the absence of high-quality impact evaluation studies of PR in LMICs, can make the case for directing resources towards PR more difficult.41 Some participants in this study felt a tilt in favour of medicine in their LMIC which is evident in low numbers of rehabilitation professionals such as physiotherapists who are trained and employed by the government compared to the number of doctors. This doctor dominance over other healthcare professionals in many LMICs may lead them to deprioritize rehabilitation (including PR), which is traditionally delivered by therapists.40
Therefore, participants in this study suggested the need for physiotherapy advocacy or public awareness campaigns to improve awareness and recognition of physiotherapy services including PR. This suggestion resonates with one of the key messages in the American Thoracic Society/European Respiratory Society policy statement on increasing implementation and delivery of PR, that public awareness campaigns are needed to foster public awareness of PR.35
The ongoing COVID-19 pandemic was also mentioned by participants in this study as an access barrier to PR in LMICs. Due to physical distancing requirements to prevent COVID-19 transmission, the pandemic has resulted in low recruitment of people with CRDs for conventional face-to-face PR. In some LMICs, face-to-face PR programmes have been suspended, thereby imposing an unprecedented barrier to PR access by people with CRDs in LMICs, further to other existing access barriers. Similar COVID-19 impact on PR access has been reported in high-income countries.42 In response, some LMICs have tried to move to tele-PR but participants described barriers to this delivery model too, including lack of digital access and literacy. These barriers have also been reported elsewhere.43,44
On the other hand, participants saw COVID-19 as a facilitator for PR in LMICs in that it serves as a stimulus for stakeholders in LMICs to develop rehabilitative interventions such as PR. The disease primarily affects the respiratory system and survivors weaned from mechanical ventilation are at a higher risk of developing post-intensive care syndrome (PICS) or long COVID, requiring treatment with PR.45 However, there is currently a limited evidence base for PR in post-acute COVID-19. The programme will potentially be wider in scope than current PR programmes1 to meet the needs of these individuals and consider the additional burden placed upon survivors by this unique disease, such as social isolation strategies and the associated emotional burden.46 In addition, survivors may be of a different age group to the “usual” PR population and supporting a successful return to work will be important.46
Finally, participants in this study described several direct and indirect costs incurred by patients as access barriers to PR in their LMIC, most notably transportation costs associated with long distance travel to a healthcare facility to access PR. For instance, in Malawi and Uganda, low-income countries in Africa, 84% of each of these countries’ population lives in rural areas/villages, located far from urban areas where higher level health services are concentrated.47,48 Fifty percent of the Malawi population live within five kilometres of their health centre, a walkable distance for a healthy person, though not necessarily for someone seeking health care.49 As a result, people with CRDs living in rural areas would incur significant transport costs to access a centre-based PR service in an urban area. This potentially encourages people living in rural areas to normalise living with their CRD, discouraging them from seeking remote hospital services including PR. As some participants in this study said, for these people, the benefit of sacrificing their hard-earned income on transport would weigh lesser than that of sacrificing it on food. Travel and transport have been frequently cited as patient-related barriers to uptake of centre-based PR programmes elsewhere.50–58
To address this barrier, all participants from Africa in this study suggested the need for a community-based PR. This would reduce the need for people with CRDs in remote rural areas to travel significant distances to access PR. This suggestion is not new as it fits the already existing wider community-based rehabilitation model established in 1978 by the WHO as an approach for social inclusion in resource-constrained settings and focused on working with people with disabilities within their communities.40 Social outcomes and cost-effectiveness studies have shown positive emerging evidence of community-based rehabilitation as a service delivery approach in settings with a scarcity of resources.59 Recently, a community-based PR programme conducted in a non-healthcare facility with patients with several CRDs demonstrated positive effects on patients’ exercise capacity, health-related quality of life, and a reduction in respiratory-related hospital admissions in the 12 months following the programme.60
Participants in the current study suggested that such community-based PR would be possible with the use of locally available equipment within the communities and would be delivered by locally available non-rehabilitation professionals such as community healthcare workers (ie, through task shifting61). However, unlike rehabilitation professionals like physiotherapists, community healthcare workers are, by nature of their job, not trained in PR. Therefore, PR delivered by community healthcare workers may compromise the professional standards of PR and safety of patients. Capacity-building in PR for community healthcare workers by physiotherapists would be needed.62
Study Strengths and Limitations
This is the first original multi-country and multi-continental study to explore barriers and enablers to PR in LMICs. The use of in-depth interviews permitted exploration of participants’ lived experiences with an ever-widening explanation.22 By purposively recruiting healthcare professionals with PR experience in LMIC, the study collected first-hand information on lived barriers and enablers to PR in LMICs. However, only 7 out of 142 LMICs63 were represented in this study, which limits the generalisability of the findings to all LMICs, although data saturation was reached. Furthermore, most participants in this study were physiotherapists (71%), which limits the generalisation of the findings to healthcare professionals of different professions, who are also members of the multidisciplinary PR team, including nurses64 and occupational therapists.65 These might have different experiences or perspectives regarding barriers and enablers to PR in LMICs.
Conclusions and Recommendations
From the perspective of healthcare professionals who participated in this study, barriers to PR in LMICs include limited resources (including shortage of PR expertise), low awareness or recognition of physiotherapy services including PR, COVID-19, and access costs incurred by patients including transport costs associated with long distance travel to a healthcare facility to access PR. Enablers include provision of PR training and resources (ie, funding), local adaptation (including community-based PR), tele-PR in the face of COVID-19, and public awareness campaigns. Successful implementation of these enablers will require engagement with multiple stakeholders including people with CRDs and their families or caregivers, rehabilitation professionals including physiotherapists, other members of the multidisciplinary team such as doctors, and government authorities including ministries of health. Future studies should evaluate the extent to which implementation of these enablers can improve access to PR and subsequent reduction of CRD burden in LMICs.
Data Sharing Statement
The data analysed in this study are available from the corresponding author upon reasonable request.
Ethical Approval
Ethical approval was granted by the UCL Research Ethics Committee (Project ID: 20465/001). It was deemed “low risk” and was approved via chair’s action. Each participant was given an information sheet and was asked to provide written informed consent, which they reiterated verbally at the start of their interview. Each participant’s informed consent included publication of their anonymized responses.
Acknowledgments
We thank the participants who contributed their time, experience, and insights to this study. We thank Ms Josan Sutherland, an Advanced Neurological Physiotherapy Master's student at the University College London, UK, on whom the interview topic guide used in this study was pilot-tested. We thank Mr Patrick Kalonde, a Geographical Information Systems (GIS) Master’s student at St Cloud State University, USA, for his assistance with the technical design of the figures.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Institute for Health Research (NIHR) (using the UK’s Official Development Assistance (ODA) Funding) and Wellcome [221465/Z/20/Z] under the NIHR-Wellcome Partnership for Global Health Research. The views expressed are those of the authors and not necessarily those of Wellcome, the NIHR or the Department of Health and Social Care.
Disclosure
The authors declare no competing interests.
References
1. Spruit MA, Singh SJ, Garvey C, et al. An official American Thoracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. 2013;188(8):e13–e64. doi:10.1164/rccm.201309-1634ST
2. Bolton CE, Bevan-Smith EF, Blakey JD, et al. British Thoracic Society guideline on pulmonary rehabilitation in adults. Thorax. 2013;68(Suppl2):ii1–ii30. doi:10.1136/thoraxjnl-2013-203808
3. Johnston K, Grimmer-Somers K. Pulmonary rehabilitation: overwhelming evidence but lost in translation? Physiother Can. 2010;62(4):368–373. doi:10.3138/physio.62.4.368
4. Majd S, Apps L, Chantrell S, et al. A feasibility study of a randomized controlled trial of asthma-tailored pulmonary rehabilitation compared with usual care in adults with severe asthma. J Allergy Clin Immunol Pract. 2020;8(10):3418–3427. doi:10.1016/j.jaip.2020.05.052
5. Ando M, Mori A, Esaki H, et al. The effect of pulmonary rehabilitation in patients with post-tuberculosis lung disorder. Chest. 2003;123(6):1988–1995. doi:10.1378/chest.123.6.1988
6. Patel S, Cole AD, Nolan CM, et al. Pulmonary rehabilitation in bronchiectasis: a propensity-matched study. Eur Respir J. 2019;53(1):1801264. doi:10.1183/13993003.01264-2018
7. Griffiths TL, Phillips CJ, Davies S, et al. Cost effectiveness of an outpatient multidisciplinary pulmonary rehabilitation programme. Thorax. 2001;56(10):779–784. doi:10.1136/thorax.56.10.779
8. Patel S, Palmer MD, Nolan CM, et al. Supervised pulmonary rehabilitation using minimal or specialist exercise equipment in COPD: a propensity-matched analysis. Thorax. 2021;76(3):264–271. doi:10.1136/thoraxjnl-2020-215281
9. Spinou A, Chalmers JD. Respiratory physiotherapy in the bronchiectasis guidelines: is there a loud voice we are yet to hear? Eur Respir J. 2019;54(3):1901610. doi:10.1183/13993003.01610-2019
10. Johnston KN, Young M, Grimmer-Somers KA, et al. Why are some evidence-based care recommendations in chronic obstructive pulmonary disease better implemented than others? Perspectives of medical practitioners. Int J Chron Obstruct Pulmon Dis. 2011;6:659–667. doi:10.2147/copd.S26581
11. Rochester CL, Vogiatzis I, Holland AE, et al. An official American Thoracic Society/European Respiratory Society policy statement: enhancing implementation, use, and delivery of pulmonary rehabilitation. Am J Respir Crit Care Med. 2015;192(11):1373–1386. doi:10.1164/rccm.201510-1966ST
12. Watson JS, Adab P, Jordan RE, et al. Referral of patients with chronic obstructive pulmonary disease to pulmonary rehabilitation: a qualitative study of barriers and enablers for primary healthcare practitioners. Br J Gen Pract. 2020;70(693):e274–e284. doi:10.3399/bjgp20X708101
13. Brakema EA, Vermond D, Pinnock H, et al. Implementing lung health interventions in low- and middle-income countries: a FRESH AIR systematic review and meta-synthesis. Eur Respir J. 2020;56(1):2000127. doi:10.1183/13993003.00127-2020
14. Habib GMM, Rabinovich R, Divgi K, et al. Systematic review of clinical effectiveness, components, and delivery of pulmonary rehabilitation in low-resource settings. NPJ Prim Care Respir Med. 2020;30(1):52. doi:10.1038/s41533-020-00210-y
15. Johnston K, Grimmer-Somers K, Young M, et al. Which chronic obstructive pulmonary disease care recommendations have low implementation and why? A pilot study. BMC Res Notes. 2012;5(652). doi:10.1186/1756-0500-5-652
16. Johnston KN, Young M, Grimmer KA, et al. Barriers to, and facilitators for, referral to pulmonary rehabilitation in COPD patients from the perspective of Australian general practitioners: a qualitative study. Prim Care Respir J. 2013;22(3):319–324. doi:10.4104/pcrj.2013.00062
17. Oates GR, Niranjan SJ, Ott C, et al. Adherence to Pulmonary Rehabilitation in COPD: a qualitative exploration of patient perspectives on barriers and facilitators. J Cardiopulm Rehabil Prev. 2019;39(5):344–349. doi:10.1097/hcr.0000000000000436
18. Spitzer KA, Stefan MS, Drake AA, et al. “You leave there feeling part of something”: a qualitative study of hospitalized COPD patients’ perceptions of pulmonary rehabilitation. Int J Chron Obstruct Pulmon Dis. 2020;15:575–583. doi:10.2147/copd.S234833
19. Stokes T, Tumilty E, Latu ATF, et al. Improving access to health care for people with severe chronic obstructive pulmonary disease (COPD) in Southern New Zealand: qualitative study of the views of health professional stakeholders and patients. BMJ Open. 2019;9(11):e033524. doi:10.1136/bmjopen-2019-033524
20. Thorpe O, Kumar S, Johnston K. Barriers to and enablers of physical activity in patients with COPD following a hospital admission: a qualitative study. Int J Chron Obstruct Pulmon Dis. 2014;9:115–128. doi:10.2147/copd.S54457
21. Singh SJ, Halpin DMG, Salvi S, et al. Exercise and pulmonary rehabilitation for people with chronic lung disease in LMICs: challenges and opportunities. Lancet Respir Med. 2019;7(12):1002–1004. doi:10.1016/s2213-2600(19)30364-9
22. de Sousa Pinto JM, Martín-Nogueras AM, Morano MTAP, et al. Chronic obstructive pulmonary disease patients’ experience with pulmonary rehabilitation: a systematic review of qualitative research. Chron Respir Dis. 2013;10(3):141–157. doi:10.1177/1479972313493796
23. Hak T. 2 Waarnemingsmethoden in kwalitatief onderzoek [Observation methods in qualitative research]. In: Lucassen PLBJ, Hartman TCO, editors. Kwalitatief Onderzoek: Praktische Methoden Voor de Medische Praktijk [Qualitative research: Practical methods for medical practice]. Houten: Bohn Stafleu van Loghum; 2007:13–25. [in Dutch].
24. Mack N, Woodsong C, Macqueen K, et al. Qualitative research methods: a data collector’s field guide. 2005.
25. Bickton FM, Fombe C, Chisati E, et al. Evidence for pulmonary rehabilitation in chronic respiratory diseases in sub-Saharan Africa: a systematic review. Int J Tuberc Lung Dis. 2020;24(10):991–999. doi:10.5588/ijtld.19.0526
26. Orme MW, Free RC, Manise A, et al. Global RECHARGE: establishing a standard international data set for pulmonary rehabilitation in low- and middle-income countries. J Glob Health. 2020;10(2):020316. doi:10.7189/jogh.10.020316
27. Guest G, Bunce A, Johnson L. How many interviews are enough? Field Methods. 2006;18:59–82. doi:10.1177/1525822X05279903
28. Vasileiou K, Barnett J, Thorpe S, Young T. Characterising and justifying sample size sufficiency in interview-based studies: systematic analysis of qualitative health research over a 15-year period. BMC Med Res Methodol. 2018;18(1):148. doi:10.1186/s12874-018-0594-7
29. Manda-Taylor L, Bickton FM, Gooding K, et al. A formative qualitative study on the acceptability of deferred consent in adult emergency care research in Malawi. J Empir Res Hum Res Ethics. 2019;14(4):318–327. doi:10.1177/1556264619865149
30. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
31. Garrod R, Lasserson T. Role of physiotherapy in the management of chronic lung diseases: an overview of systematic reviews. Respir Med. 2007;101(12):2429–2436. doi:10.1016/j.rmed.2007.06.007
32. Ries AL, Bauldoff GS, Carlin BW, et al. Pulmonary rehabilitation: joint ACCP/AACVPR evidence-based clinical practice guidelines. Chest. 2007;131(5 Suppl):4s–42s. doi:10.1378/chest.06-2418
33. Jenkins S, Hill K, Cecins N. State of the art: how to set up a pulmonary rehabilitation program. Respirology. 2010;15(8):1157–1173. doi:10.1111/j.1440-1843.2010.01849.x
34. World Health Organization. The need to scale up rehabilitation [Internet]. Geneva; 2017 [cited October 2, 2021]. Available from: https://apps.who.int/iris/handle/10665/331210.
35. Vogiatzis I, Rochester CL, Spruit MA, et al. Increasing implementation and delivery of pulmonary rehabilitation: key messages from the new ATS/ERS policy statement. Eur Respir J. 2016;47(5):1336. doi:10.1183/13993003.02151-2015
36. McCarron EP, Bailey M, Leonard B, et al. Improving the uptake: barriers and facilitators to pulmonary rehabilitation. Clin Respir J. 2019;13(10):624–629. doi:10.1111/crj.13068
37. Farah R, Groot W, Pavlova M, Coquart J. Pulmonary rehabilitation in Lebanon “What do we have”? A national survey among chest physicians. PLoS One. 2021;16(7):e0254419. doi:10.1371/journal.pone.0254419
38. Leech AA, Kim DD, Cohen JT, et al. Are low and middle-income countries prioritising high-value healthcare interventions? BMJ Glob Health. 2020;5(2):e001850. doi:10.1136/bmjgh-2019-001850
39. Rosenbaum AJ, Maine RG. Improving access to laparoscopy in low-resource settings. Ann Glob Health. 2019;85(1). doi:10.5334/aogh.2573
40. AlHeresh R, Cahn PS. Expanding global rehabilitation services through international academic-community partnerships. Ann Glob Health. 2020;86(1):71. doi:10.5334/aogh.2876
41. Saran A, White H, Kuper H. Evidence and gap map of studies assessing the effectiveness of interventions for people with disabilities in low-and middle-income countries. Campbell Syst Rev. 2020;16(1):e1070. doi:10.1002/cl2.1070
42. American Thoracic Society. Case studies of services restarting pulmonary rehabilitation programmes following the COVID-19 pandemic [Internet]. Available from: https://www.thoracic.org/members/assemblies/assemblies/pr/quarterly-bite/case-studies-of-services-restarting-pulmonary-rehabilitation-programmes-following-the-covid-19.php.
43. Leochico CFD. Adoption of telerehabilitation in a developing country before and during the COVID-19 pandemic. Ann Phys Rehabil Med. 2020;63(6):563–564. doi:10.1016/j.rehab.2020.06.001
44. Tsutsui M, Gerayeli F, Sin DD. Pulmonary rehabilitation in a post-COVID-19 world: telerehabilitation as a new standard in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2021;16:379–391. doi:10.2147/copd.S263031
45. Siddiq MAB, Rathore FA, Clegg D, et al. Pulmonary Rehabilitation in COVID-19 patients: a scoping review of current practice and its application during the pandemic. Turk J Phys Med Rehab. 2020;66(4):480–494. doi:10.5606/tftrd.2020.6889
46. Spruit MA, Holland AE, Singh SJ, et al. COVID-19: interim guidance on rehabilitation in the hospital and post-hospital phase from a European Respiratory Society- and American Thoracic Society-coordinated international task force. Eur Respir J. 2020;56(6):2002197. doi:10.1183/13993003.02197-2020
47. Dowhaniuk N. Exploring country-wide equitable government health care facility access in Uganda. Int J Equity Health. 2021;20(1):38. doi:10.1186/s12939-020-01371-5
48. Geoffroy E, Harries AD, Bissell K, et al. Bringing care to the community: expanding access to health care in rural Malawi through mobile health clinics. Public Health Action. 2014;4(4):252–258. doi:10.5588/pha.14.0064
49. Varela C, Young S, Mkandawire N, et al. Transportation barriers to access health care for surgical conditions in Malawi: a cross sectional nationwide household survey. BMC Public Health. 2019;19(1):264. doi:10.1186/s12889-019-6577-8
50. Arnold E, Bruton A, Ellis-Hill C. Adherence to pulmonary rehabilitation: a qualitative study. Respir Med. 2006;100(10):1716–1723. doi:10.1016/j.rmed.2006.02.007
51. Fan VS, Giardino ND, Blough DK, et al. Costs of pulmonary rehabilitation and predictors of adherence in the National Emphysema Treatment Trial. COPD. 2008;5(2):105–116. doi:10.1080/15412550801941190
52. Fischer MJ, Scharloo M, Abbink JJ, et al. Participation and drop-out in pulmonary rehabilitation: a qualitative analysis of the patient’s perspective. Clin Rehabil. 2007;21(3):212–221. doi:10.1177/0269215506070783
53. Harris D, Hayter M, Allender S. Improving the uptake of pulmonary rehabilitation in patients with COPD: qualitative study of experiences and attitudes. Br J Gen Pract. 2008;58(555):703–710. doi:10.3399/bjgp08X342363
54. Holland AE, Mahal A, Hill CJ, et al. Benefits and costs of home-based pulmonary rehabilitation in chronic obstructive pulmonary disease - a multi-centre randomised controlled equivalence trial. BMC Pulm Med. 2013;13:57. doi:10.1186/1471-2466-13-57
55. Keating A, Lee AL, Holland AE. Lack of perceived benefit and inadequate transport influence uptake and completion of pulmonary rehabilitation in people with chronic obstructive pulmonary disease: a qualitative study. J Physiother. 2011;57(3):183–190. doi:10.1016/s1836-9553(11)70040-6
56. O’Shea SD, Taylor NF, Paratz JD. But watch out for the weather: factors affecting adherence to progressive resistance exercise for persons with COPD. J Cardiopulm Rehabil Prev. 2007;27(3):
57. Sabit R, Griffiths TL, Watkins AJ, et al. Predictors of poor attendance at an outpatient pulmonary rehabilitation programme. Respir Med. 2008;102(6):819–824. doi:10.1016/j.rmed.2008.01.019
58. Young P, Dewse M, Fergusson W, et al. Respiratory rehabilitation in chronic obstructive pulmonary disease: predictors of nonadherence. Eur Respir J. 1999;13(4):855–859. doi:10.1034/j.1399-3003.1999.13d27.x
59. World Health Organization. Guidelines approved by the guidelines review committee. In: Khasnabis C, Heinicke Motsch K, Achu K, et al. editors. Community-Based Rehabilitation: CBR Guidelines. Geneva: World Health Organization; 2010:67.
60. Cecins N, Landers H, Jenkins S. Community-based pulmonary rehabilitation in a non-healthcare facility is feasible and effective. Chron Respir Dis. 2017;14(1):3–10. doi:10.1177/1479972316654287
61. Smith S, Deveridge A, Berman J, et al. Task-shifting and prioritization: a situational analysis examining the role and experiences of community health workers in Malawi. Hum Resour Health. 2014;12:24. doi:10.1186/1478-4491-12-24
62. Nesbit KC, Clark A. Rehabilitation training for community health workers: a five-year study. Int J Health Promot Educ. 2019;57(1):3–12. doi:10.1080/14635240.2018.1538808
63. Wellcome. Low- and middle-income countries; 2021 [cited October 2, 2021]. Available from: https://wellcome.org/grant-funding/guidance/low-and-middle-income-countries.
64. Akinci AC, Olgun N. The effectiveness of nurse-led, home-based pulmonary rehabilitation in patients with COPD in Turkey. Rehabil Nurs. 2011;36(4):159–165. doi:10.1002/j.2048-7940.2011.tb00084.x
65. Easthaugh S, Bradley G, Peel L, et al. Occupational therapy-led pulmonary rehabilitation: a practice analysis. Br J Occup Ther. 2019;82(12):770–774. doi:10.1177/0308022619871030
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.