")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Balancing Life and Death During the Golden Minute – Midwives’ Experiences of Performing Newborn Resuscitation
Authors Ljungblad LW , Skovdahl K, McCormack B , Dahl B
Received 24 June 2020
Accepted for publication 13 August 2020
Published 17 September 2020 Volume 2020:13 Pages 943—952
DOI https://doi.org/10.2147/JMDH.S268959
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Linda Wike Ljungblad,1 Kirsti Skovdahl,2 Brendan McCormack,2,3 Bente Dahl1
1Centre for Women’s, Family and Child Health, Faculty of Health and Social Sciences, University of South-Eastern Norway, Kongsberg N-3603, Norway; 2Faculty of Health and Social Sciences, University of South-Eastern Norway, Kongsberg N-3603, Norway; 3Divisions of Nursing, Occupational Therapy & Arts Therapies, Centre for Person-Centred Practice Research, School of Health Sciences, Queen Margaret University, Musselburgh, East Lothian EH21 6UU, UK
Correspondence: Linda Wike Ljungblad
Faculty of Health and Social Sciences, University of South-Eastern Norway, P.O. Box 235, Kongsberg N-3603, Norway
Tel +47 93458429
Email [email protected]
Purpose: To explore midwives’ experiences in performing newborn resuscitation on maternity wards.
Patients and Methods: It was a qualitative study, using a phenomenological hermeneutic approach. Individual interviews with 16 clinical midwives working in Norwegian maternity wards were conducted from August 2018 to January 2019.
Results: The complexity underlying how midwives balance responsibility and vulnerability when performing newborn resuscitation during the Golden Minute was revealed. Midwives described the stress they experienced during resuscitation events and their need for support and confirmation after performing newborn resuscitation.
Conclusion: The vulnerability and responsibility that midwives bear for mothers and newborns simultaneously affected midwives in several ways. We saw that midwives need support and confirmation to be prepared for newborn resuscitation. We also found that a lack of knowledge, skills and experience were barriers to midwives feeling prepared. Simulation training, including tailored programs, are suggested to improve midwives’ skills and help them feel prepared for real-life resuscitations. The importance of midwives’ assessment during the Golden Minute and further investigation from other perspectives are needed to understand fully this clinical complexity.
Keywords: experiences, Golden Minute, midwife, newborn resuscitation, qualitative research
Introduction
I was alone with life and death in my hands. My hands were shivering and I was sweating. The adrenaline was pumping. I was terrified. It was like being on the top of the mountain on the verge of falling down. Was this baby already dead? I felt numb. Would help arrive too late this time? I pretended to be calm outwardly, but inside I felt helplessness and chaos. The baby had been doing fine throughout labour. Did I ignore something? What will my colleagues say?
An included midwife (3) in this study is describing a situation where she had to perform newborn resuscitation.
Globally, midwives on maternity wards experience non-breathing newborns every day.1,2 A reduction in infant mortality can be prevented through immediate newborn assessment and resuscitation.3 Broadly defined, newborn resuscitation is a set of interventions undertaken immediately after delivery to support the onset of breathing and circulation for newborns.4 Newborns generally require little assistance to adapt to extrauterine life, but worldwide up to 10% need immediate help with their breathing.5 Less than 1% require advanced resuscitation.6
The Golden Minute refers to the first 60 s of a newborn’s life,7 during which the complex but natural transition from intra- to extrauterine life occurs.8 Typically, midwives perform newborn assessment during the Golden Minute. Guidelines for basic newborn assessment suitable for contexts worldwide have been developed to facilitate effective practice when newborn resuscitation is required.9,10 It is important that the skills specific to newborn assessment and the provision of help when needed be relevant to the various contexts that exist.11 Newborn resuscitation skills are essential components in midwifery care and should be improved continuously.12
In Norway, maternity care is differentiated and decentralized on three levels: university hospitals, medium-sized maternity clinics and midwifery-led birth wards. Midwives possess the necessary qualifications and legal authority to assist normal births and identify pathological conditions, and are required to contact an obstetrician or pediatrician if needed. Consequently, they must be capable of quick decision-making, which in turn necessitates both knowledge and experience.13
Research concerning midwives’ experiences of performing newborn resuscitation is scarce. However, the need to clarify guidelines, responsibilities and the importance of teamwork in newborn resuscitation has been emphasized.14 Furthermore, lack of experience, knowledge, skills, inadequate teamwork and organizational constraints sometimes prevent midwives from performing newborn resuscitation.15,16 Studies demonstrate that midwives find it challenging to assess non-breathing newborn babies,17 they lack skills to resuscitate newborns and adequate help is not always immediately available.18 Understanding the role as a midwife is important to improve confidence and knowledge in newborn resuscitation19 and studies describe that strengthening newborn resuscitation skills has resulted in improved birth outcomes.20 To improve resuscitation skills, frequent hands-on training programs have been recommended.21
In the global context, several publications highlight the need for understanding and exploring the complexity in newborn resuscitation for midwives both in low- and high-income countries. So far, research about midwives performing newborn resuscitation has focused on practical hands-on training, skills and teamwork. However, we have not been able to locate studies addressing the complexity of these situations, including not only skills, hands-on-training and teamwork, but also the emotional challenges midwives’ experience when faced with a non-breathing newborn. This paper is a contribution from a highly developed medical system. We therefore designed a study to explore midwives’ experiences of performing newborn resuscitation on maternity wards.
Patients and Methods
We conducted a qualitative study, using a phenomenological hermeneutic approach.22 This design was appropriate to explore midwives’ experiences in newborn resuscitation, as previous research about the topic was scarce.
Recruitment
We anticipated recruiting nineteen midwives to the study, but in the end interviewed 16 midwives as data saturation had been reached (see data analysis section).24 To recruit eligible midwives, we posted an invitation to participate in the study on a Norwegian midwifery forum on Facebook consisting of 2300 midwives in August and September 2018. We also undertook snowball sampling. Midwives working on high-risk and midwifery-led maternity wards in several hospitals were asked to pass along word-of-mouth information and/or flyers to colleagues they believed would meet the inclusion criteria.23 The inclusion criteria were registered midwives who had performed newborn resuscitation during the Golden Minute on Norwegian maternity wards. Nineteen midwives contacted the first author to participate in the study. They all fulfilled the inclusion criteria.
Participants
The participants were female, native speakers of Scandinavian languages, aged 32–61 years, and lived in different parts of Norway. They worked at small midwifery-led wards, maternity clinics or university hospitals where the number of deliveries varied from 30 to 7000 births annually. Their working experience varied from one to 35 years (mean 14 years), and they had varied experience of newborn resuscitation from 26 different maternity wards (Table 1). Fourteen participants had graduated from Norwegian university colleges or universities and two from other Nordic countries. A majority had completed other forms of postgraduate education or courses, and some had experience of working abroad.
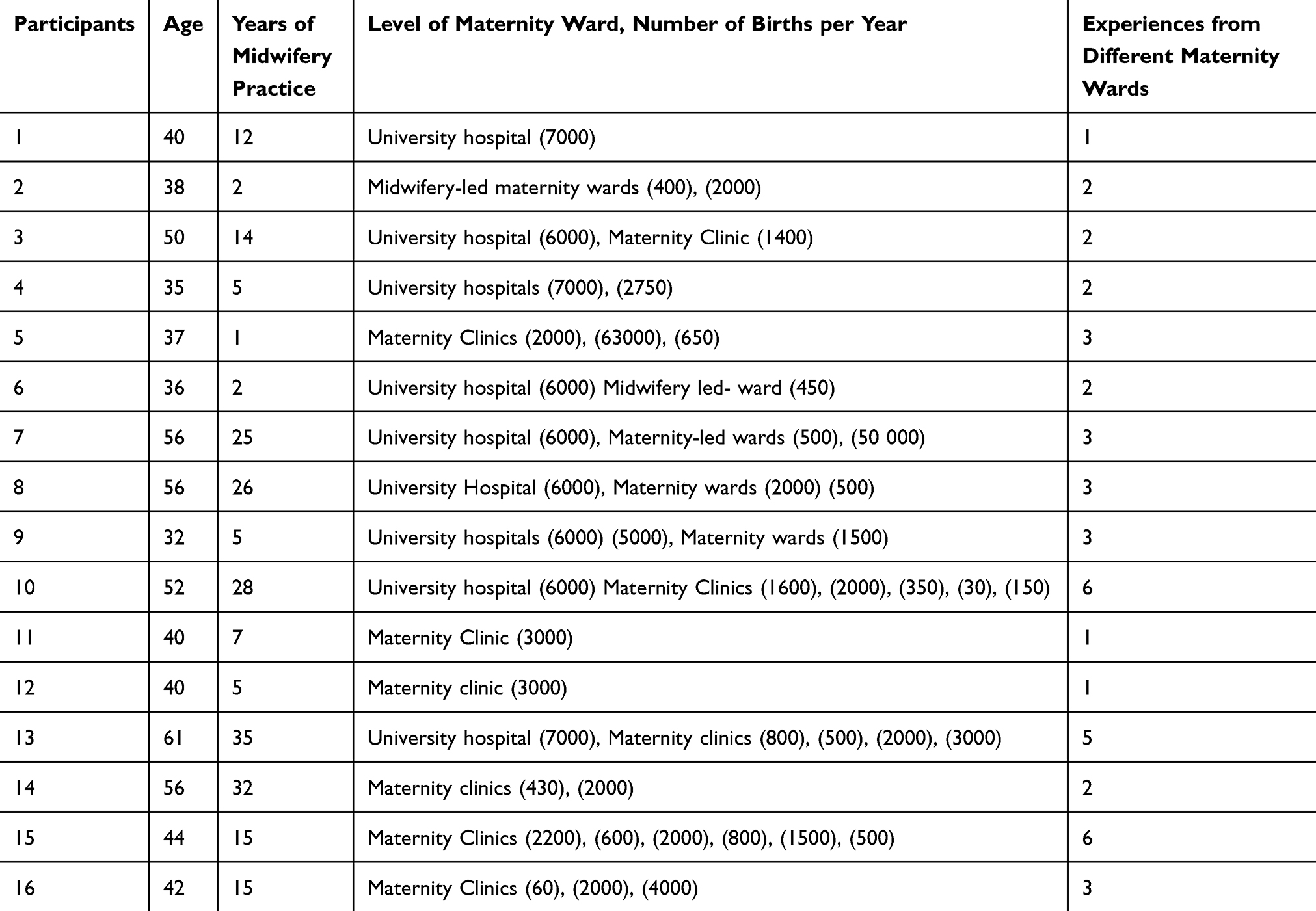 |
Table 1 Description of Included Participants |
Data Collection
The first author conducted individual interviews between August 2018 and January 2019 at different locations chosen by the participants. All interviews were conducted in the Norwegian language as all participants understood and spoke the language. The conducted interviews had two aims: I) to explore midwives' experiences of performing newborn resuscitation and II) to explore midwives’ experiences about what constitutes relevant content and structure in a newborn resuscitation program. This paper focuses on the first aim. Two pilot interviews were conducted with colleagues handpicked by the first author prior to the start of the study. These were not included, but were essential to adjusting the interview technique and interview questions. The interviews took place where the participants wished to be interviewed and started with an open-ended question: “Could you please tell me about a situation when you experienced a non-breathing newborn baby immediately after delivery”. The participants were encouraged to narrate their experiences of performing newborn resuscitation freely and were only interrupted by follow-up questions when clarification or further elaboration was needed. Field notes were written during and immediately after each interview. The interviews lasted 22–49 mins (mean 32). All interviews were digitally recorded and transcribed verbatim by the first author.
Ethics
The study was conducted in accordance with the WMA Declaration of Helsinki Ethical Principles for Medical Research in Human Subjects.25 Approval for the study was granted by The Regional Committee for Medical and Health Research Ethics (2018/975). The Norwegian Centre for Research Data assessed the study and considered it to be outside the scope of sections 2 and 4 of the Health Research Act (60726). Prior to interviews, all participants received written and oral information about the study, including assurances of anonymity and confidentiality. Prior to being included in this study, all participants provided informed consent to publish anonymised data material, including quotes. They were informed that they could withdraw from the study at any time without giving reasons. If participation led to any adverse emotional reactions, participants could contact the first author, but none did so.
Data Analysis
We used a phenomenological hermeneutic method consisting of three phases to analyze the data.22 The method was developed to understand morals and ethical thinking of nurses and physicians expressed in interview texts. In this analysis method, the interpretation implies a dialectic movement between the text as a whole and parts of the text, influenced by Ricoeur’s phenomenological hermeneutic interpretation theory.26
First, we conducted a naïve or open-minded reading to gain an overall impression of the text, providing access to midwives' experiences of performing newborn resuscitation. We then undertook a structural analysis by dividing the text into meaning units, ie, sentences, parts of sentences or paragraphs containing related meaning content. These meaning units were in turn condensed into themes and sub-themes. The structural analysis aimed to explain what the text was saying. It was an iterative process, and we validated or refuted the meaning units based on our impressions from the naïve reading.22 Lastly, we formulated a comprehensive understanding by re-reading the text as a whole while taking into consideration our preunderstanding, the naïve reading and the structural analysis as well as relevant studies.
Results
Naïve Understanding
Most participants experienced newborn resuscitation to be one of the most frightening situations a midwife can experience. They described feeling an enormous and simultaneous responsibility for the mother and newborn when performing newborn resuscitation and noted their experiences of a life-and-death-perspective in such situations. They talked about being courageous enough, feeling uncertainty, scrutinizing themselves and being critical of own skills. They described physical symptoms from the stress that such situations could cause and experienced that they swung between feeling like experts during normal births and novices when performing newborn resuscitation. They feared they would be found to be insufficiently competent or would be blamed or scapegoated.
Structural Analysis
Four themes emerged from the analysis. An overview of the themes and sub-themes is presented in Table 2.
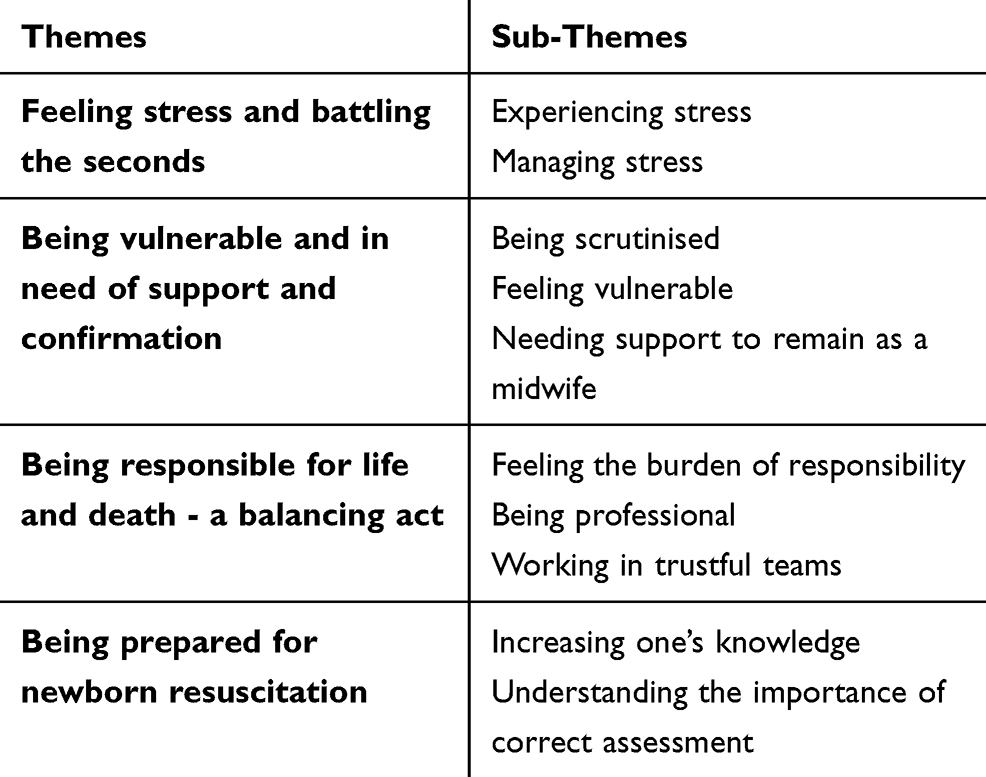 |
Table 2 Overview of Themes and Sub-Themes |
Feeling Stress and Battling the Seconds
Experiencing Stress
Most participants could experience physical symptoms from stress when they performed newborn resuscitation. A participant stated that she felt as if the heavy burden she bore was a weighty stone wandering through her body, from her heart to her stomach. Others experienced an extreme adrenaline rush, describing their bodies as being in “high gear”. They could perceive this adrenaline rush as being positive because it helped them focus, or as being negative, because it could make them almost lose control. When elaborating on the emotions, the participants noted that they felt anxious, sick or panicked. Some experienced a sense of internal chaos, others an extremely elevated pulse rate. Some felt cold, clammy, sweaty or incapable of thought or communication, while others cried or vomited. A participant described her feelings thus:
… I felt like the blood drained from my body … a huge adrenalin rush … like being on the top of a mountain on the verge of falling down …. (3)
Another participant stated that she started to shiver so much that she had difficulty controlling her hands when opening ampoules. Others described a numb feeling all over their body, a type of panic, and that they could “feel shaky” for hours afterwards. The adrenaline rush was stronger when they were under time pressure and they noted that newborn resuscitation was one of the most frightening situations a midwife can experience and described the stress felt during the situation as incomparable to anything else.
Managing Stress
The midwives experienced multiple challenges when having to initiate newborn resuscitation, noting that the situation was stressful until help arrived and that bearing responsibility for the mother and newborn simultaneously made them feel insufficient. The time that elapsed until adequate help arrived could differ, as well as their experiences of this time. Some were alone, perceiving the seconds go by terribly slowly, as if time had slowed down. Some could access help through a video monitor, while others were never alone. A participant stated that she felt as if she was waiting for help for an entire shift, while in reality, the time that elapsed was 3.5 mins. Some midwives found it difficult to state accurately how long they were waiting for help, but noted that they managed to perform a great number of tasks while waiting.
It felt like I was waiting for help for 3 hours … but it was only 4 minutes … it was more than enough … and it felt like 3 hours … do they never come?. (12)
One midwife decided to initiate newborn resuscitation herself, even if she felt that she was skilled insufficiently because it took a long time for help to arrive. Another blacked out during a newborn resuscitation, even though she had practiced a hundred times on manikins. All midwives, even those who had been teaching colleagues, stated that simulated situations did not match real-life clinical situations.
Being Vulnerable and in Need of Support and Confirmation
Being Scrutinized
The midwives were scared they would perform newborn resuscitation incorrectly. They spoke of blaming themselves and their need for confirmation after newborn resuscitation. Such self-blame could include whether they acted quickly enough or whether they should have identified risk indicators earlier. They described balancing multiple challenges simultaneously and questioning their own assessments. After a newborn resuscitation, they experienced that they were scrutinised and that both colleagues and/or parents could blame them, noting that such scrutiny and blame was a heavy burden to bear:
We seek to find someone or something to blame of course … it’s natural that you seek to find a reason or a scapegoat … if the reason was an infection, it would be easier to accept, and the midwife did not have to become the scapegoat …. (14)
The participants were afraid they would be unable to defend their actions or that they would be blamed for having forgotten to do something during newborn resuscitation. A midwife noted that after the death of a baby she received unpleasant private messages from the mother, which she described as a heavy burden.
Feeling Vulnerable
The midwives expressed their emotions, frustrations and sorrows in several ways. A participant described her experience as a painful secret that she had never shared, others were left “alone” after an incident and expressed frustration that their colleagues did not support them. Another said she felt like she fell into a deep black hole and was struggling to get out of the hole. Yet another revealed her vulnerability after the death of a baby by describing the misunderstood care she received:
… and the worst part was that when we should have a debriefing, I was told that I did not need to come because they would protect me from it … it was absolutely horrible … It was my delivery, and I knew what really happened in that labour room … all [those] thoughts I needed to discuss afterwards, and I would not be allowed to attend … it was misunderstood care for me …. (3)
This midwife perceived that she would have needed support and confirmation from her colleagues. The participants also mentioned respect and disrespect from professionals from other professions as being an important factor in their feeling vulnerable. Some midwives stated that they experienced misunderstood care and could not answer when asked how they should prepare themselves to face such situations again.
Needing Support to Remain as a Midwife
The midwives stated that they needed support and confirmation from their colleagues after a newborn resuscitation. While some received support from their midwife leaders, others did not. They spoke of the importance of being debriefed after the resuscitation, noting that not talking about the experience could leave them traumatized. A participant mentioned that she would have left the profession if not for the support she received from her colleagues:
It was absolutely horrible … I was scared and cried … I had good colleagues who supported and comforted me, luckily, and they stood by me during the next delivery … I believed that I did a good job, but the results turned out to be wrong … I just wanted to stop being a midwife … and start selling shoes in a shop or work in a grocery store … if I make a mistake during delivery, the baby can actually die …. (11)
The participants needed confirmation to maintain their self-confidence regarding their capacity to assess similar situations correctly in the future because such situations could appear like “a thunderbolt out of the blue”.
Being Responsible for Life and Death – A Balancing Act
Feeling the Burden of Responsibility
The midwives perceived their inherent responsibility for life and death to be a challenging burden. A participant spoke of the responsibility she bore during newborn resuscitation as feeling like she was caring for her own baby, who was hovering between life and death. They revealed a fear of being considered negligent, and noted that the profession was “tough” and not for everyone. Some mentioned that they could lose focus, “lose themselves” or even “lose their heads” when performing newborn resuscitation and one midwife illustrated her actions by comparing herself to a duck:
I try to behave like a duck when I receive unexpected non-breathing newborns … ducks swim quietly and [glide along] the surface of the water, while their legs [beat furiously like] drumsticks below the surface … the parents need you to be calm even if your heart is beating inside painfully …. (8)
A midwife described feeling numb when resuscitating a baby while calming the parents down simultaneously. Another described how she struggled to support a mother’s birthing partner who was crying in the corridor, saying that if newborn resuscitation did not “break” her (the midwife), nothing would.
Being Professional
Most midwives perceived themselves to be novices, not experts, during newborn resuscitation, which they attributed to adrenaline and fear. Some questioned whether they were responsible for a baby’s death. They spoke of the importance of balancing various factors when critical situations occurred: a normal Apgar score, a baby’s slow onset of breathing and their patience and skills in identifying risk factors during delivery. A participant mentioned that she as a midwifery student learned the importance of remaining calm from a supervisor, who she experienced as being a good role model:
I remember that I was impressed by my supervisor … she did not panic, but kept calm … she acted quickly and was explicit in giving clear instructions … I remember that I wanted to be like her … she was a good role model, because she kept the acute situation calm. (16)
Most midwives revealed that one important characteristic of being professional was being a good role model. They described the importance of balancing several skills simultaneously when performing newborn resuscitation, and learned from colleagues that mistakes were not allowed. Many also experienced that providing parents with good care in chaotic situations was difficult.
As part of being professional, the midwives sought to be available for parents who had experienced a traumatic resuscitation for some weeks after the incident, stating that it was important that they answer questions for as long as needed. One midwife even said that the families with whom she had close contact with after newborn resuscitation would have a place in her heart forever. Yet some noted that midwife leaders did not always encourage such actions or could even provide resistance to midwives acting in such a manner, requiring the midwives to act during their free time.
Working in Trustful Teams
The midwives expressed the need to understand newborn resuscitation fully. They maintained that good collaboration with other professionals was important, noting underlying challenges such as sharing information correctly or getting qualified help quickly. They expressed that cooperation was important when performing resuscitation, expressed here as “complementing one another”: sharing information correctly, receiving qualified help quickly. Such cooperation should be based on collective knowledge. A participant described her key for success:
I discovered a huge gap in knowledge about natural transition … I have increased and shared my knowledge with my colleagues, so we have the same [knowledge] base … when we have the same base, we do not have to discuss … to succeed with newborn resuscitation, we have to maintain this collective base. (3)
The midwives perceived themselves to be an important link between the various team members. Some explicitly stated that they needed qualified help when performing newborn resuscitation, but could encounter scared, inexperienced paediatricians. They noted the various perspectives that other professionals could have and emphasized the importance of trusting in themselves as midwives to provide safe care. To maintain their resuscitation skills, some frequently trained with other professionals. Others stated that they trained every second year but would prefer training that was more frequent.
Being Prepared for Newborn Resuscitation
Increasing One’s Knowledge
The midwives expressed the need to increase their knowledge of newborn resuscitation, and an experienced midwife described her attainment of knowledge as a “steep learning curve” because she learned from her mistakes. The participants described being prepared as understanding how and when one should act so as to provide the best care. They noted that each clinical experience was an opportunity to learn, share and engage in quality improvements. Yet they felt that being prepared for newborn resuscitation was incredibly difficult; even ventilation was considered a difficult skill. A midwife spoke of her wish to increase her knowledge:
… it felt like burning under my feet in an extremely difficult situation … I have not spoken to any colleagues about this experience … it has been aggravating and somewhat educational for me … but I really want to increase my knowledge from all situations to be more prepared for unexpected newborn resuscitation …. (10)
Some participants used the terms “inadequate or unprepared” when describing themselves initiating newborn resuscitation alone, maintaining that they were insufficiently experienced to bear such a responsibility. They noted that after traumatic situations they were unable to talk about the experience. One midwife described how, after a negative outcome she decided that she wanted to become skilled at performing newborn resuscitation. They repeated that all midwives would experience non-breathing newborns eventually. They spoke of their lack of experience and the need for continuous, repeat training, while also revealing a broad variation in the practical training they had received.
Understanding the Importance of Correct Assessment
The midwives highlighted that they were the first profession to assess each baby after delivery. They emphasized that newborns’ natural transition from intra- to extrauterine life took time. Some even claimed that they had the clinical skill to determine which newborns would need resuscitation. A participant spoke of the importance of acting and not waiting:
I was worried, and knew this was about life and death … that’s why it is important to act, not wait for another professional [who is] more knowledgeable than me … sometimes I think that I am only a midwife, and therefore I cannot initiate newborn resuscitation … but you are responsible for life and death …. (11)
They perceived that although they were calmer when they were prepared, they nonetheless felt the burden of their responsibility and were frightened to perform an assessment incorrectly. Several participants related that they were extremely focused when performing resuscitation, comparing it to having “tunnel vision”; they knew their role and what they had to do. Some spoke of the need for “automatic hands” and systematic work when performing resuscitation. Still, a midwife questioned whether she would ever be prepared sufficiently, noting that she feared the day when her knowledge would be insufficient. All participants stated that assessments must be performed correctly, but noted the challenges underlying the acquisition of such skills and knowledge.
Discussion and Comprehensive Understanding
From the findings, we discerned the complexity underlying how midwives balance stress when performing newborn resuscitation during the Golden Minute. The midwives seemed to be vulnerable, and they needed support and confirmation to manage the enormous responsibility they bore.
Our interpretation of the results can be presented through one midwife’s quote where she compares midwives performing newborn resuscitation with the metaphor of a swimming duck; above the surface of the water, the duck swims calmly while underneath its legs paddle furiously. The duck appears untroubled and calm, similar to how midwives strive to present themselves as professionals. This metaphor describes midwives’ lived experiences in a dimension that, while not translatable, it adds depth meaning to the text.26 Using this metaphor, we understand the complexity inherent in performing newborn resuscitation.
Our understanding is based on person-centredness and a person-centred practice framework that focuses on the constructs necessary for providing a person-centred service.27 The framework pays attention to the characteristics of person-centred services at all levels of an organization and thus is a whole-systems approach to developing and ensuring a person-centred service. We use this framework at all levels throughout this study.
Performing newborn resuscitation in complex settings, midwives are expected to appear professionally competent.27 Some participants revealed the complexity of newborn resuscitation in everyday clinical practice, and the extent of the burden of responsibility that they bear as midwives. They described how the stress linked to such responsibility affected them in varied ways. They felt anxious, sick or panicked or could even cry or vomit after a newborn resuscitation, noting physical symptoms from the stress they experienced. We also found that when the midwives performed newborn resuscitation alone they perceived that time moved slowly, regardless of the actual length of time that elapsed before help arrived. This is in line with Trevisanuto et al (2016), who found that those participating in a newborn resuscitation program perceived time intervals to be shorter than the actual time intervals.28 Seemingly, when there is a lot at stake, time appears to move slowly. Nevertheless, this fact highlights how the situation for midwives differs from that of pediatricians or neonatal nurse practitioners, who have no responsibility for the mother, as well the obstetricians, who have no responsibility for the baby. This underlines the complexity of newborn resuscitation for midwives.
When understanding that midwives feel vulnerable and need support after newborn resuscitation, vulnerability needs to be considered. The expression of emotions, frustrations and sorrows are typical responses to vulnerability and some of the responses used by the midwives in this study. One explanation for this can be that midwives are dependent on others.27 Midwives revealed that they sought support and confirmation from their colleagues, and furthermore stated that after a newborn resuscitation they needed support if they were to continue working as midwives. This places them in an apparent dichotomy, as on one hand they need support from colleagues and need to make themselves dependent on others for this; whilst on the other, this can be seen by others as a weakness. Seen both here and in other studies, midwives perceive support and confirmation from their organization, management and colleagues as being important, but challenging.27 In our study, some participants received frequent daily support from their midwifery leaders, while others did not. Some even experienced that, in an attempt to provide support, their midwifery leaders did not debrief them, which was perceived as misunderstood care. The extent to which nurses and midwives feel supported by their organization is a key consideration in their retention as employees and has been demonstrated in numerous studies as the key factor as to why nurses and midwives leave their job.29 This factor was also evident in the findings of this study and according to one midwife, she would have left her profession if not for the support she received from her colleagues. Stress experienced by lack of support can also impact on a midwife’s ability to assume the responsibility needed in newborn resuscitation. This support is related as an essential component for midwives to remain as midwives after stressful and traumatic experiences.27
The midwives felt newborn resuscitation to be a burden of responsibility. Even if midwives have not necessarily chosen the responsibility inherent in performing newborn resuscitation, they cannot avoid it. We found that being responsible included midwives being professionally competent.27 Being responsible for life and death is challenging, and midwives in other studies have demonstrated poor skills levels in basic newborn resuscitation.21,30 Here the participants described how, when performing newborn resuscitation, they became novices instead of experts, a change they associated with adrenaline and fear. This demonstrates how difficult it is to perform newborn resuscitation in real life, and highlights the importance of training in newborn resuscitation if midwives are to be expected to assume responsibility for it as a part of their professional role.
In our study, midwives expressed the need to increase their knowledge, and noted that while real-life experience gave them the opportunity to learn and develop, it was difficult or even impossible to prepare for newborn resuscitation. They also highlighted the importance of performing newborn assessment correctly. Even if they focus on normality, midwives are continuously aware of pathological changes. Various researchers have found that midwives report a lack of knowledge, skills and experience in newborn resuscitation.15,16,21 Researchers saw improved technical skills and teamwork in newborn resuscitation after multidisciplinary team training.31 Our study suggests that simulation is necessary but not sufficient with regard to preparing midwives, even though simulation training is currently the most commonly used method to develop newborn resuscitation skills.
This study represents midwives’ experiences with newborn resuscitation in a context characterized by low tolerance for maternal or newborn deaths. Obviously, this influences midwives' perceptions of responsibility, stress and vulnerability regarding newborn resuscitation. We recommend further research from other perspectives and cultural contexts to understand fully this clinical complexity about midwives’ experiences in performing newborn resuscitation.
Strengths and Limitations
The research group included two professors, an associate professor and a doctoral candidate. Two members are nurses and two have extensive practice in nurse-midwifery, including newborn resuscitation. This provided a solid knowledge base our clinical and theoretical backgrounds ensured inside – as well as outside perspectives on newborn resuscitation.
To ensure trustworthiness, a large amount of data about midwives' experiences performing newborn resuscitation at maternity wards was provided.24 During the interviews, participants were given the opportunity to share rich descriptions of their experiences to provide credibility. A detailed description of the research process, including data collection and analysis are described to ensure transferability. However, we are aware that our interpretation is one possible way of understanding midwives’ experiences of performing newborn resuscitation.26
The interviews consisted of one open question, limiting the possibility that our pre-conceptions would influence the data material. However, because the participants took a strong interest in the research topic their willingness to participate might influence the findings.24 The possibility of bias in the sample is present because midwives place a significant importance on newborn resuscitation as a key area of practice. However, their interest in this practice also demonstrates their motivation to participate in this study. Some midwives described situations from many years previously, and recall bias might also be an issue in the sample.
Conclusion
The vulnerability and responsibility that midwives bear for mothers and newborns simultaneously affected midwives in several ways. We saw that midwives need support and confirmation to be prepared for newborn resuscitation. We also found that a lack of knowledge, skills and experience were barriers to midwives feeling prepared. Simulation training, including tailored programs and debriefing, is suggested to improve midwives’ skills and help them feel prepared for real-life resuscitations. The importance of midwives’ assessment during the Golden Minute and further investigation from other perspectives are needed to understand fully this clinical complexity.
Acknowledgments
We thank all of the midwives who, by sharing their experiences of performing newborn resuscitation, contributed to this study.
Disclosure
The authors declare no conflict of interests for this work.
References
1. Opiyo N, English M. In-service training for health professionals to improve care of seriously ill newborns and children in low-income countries. Cochrane Database Syst Rev. 2015;5:Cd007071.
2. Black RE, Cousens S, Johnson HL, et al. Global, regional, and national causes of child mortality in 2008: a systematic analysis. Lancet. 2010;375(9730):1969–1987. doi:10.1016/S0140-6736(10)60549-1
3. Lee AC, Cousens S, Wall SN, et al. Neonatal resuscitation and immediate newborn assessment and stimulation for the prevention of neonatal deaths: a systematic review, meta-analysis and Delphi estimation of mortality effect. BMC Public Health. 2011;11(Suppl 3):S12. doi:10.1186/1471-2458-11-S3-S12
4. American Academy of Pediatrics and American Heart Association. Textbook of Neonatal Resuscitation (NRP).
5. Vali P, Mathew B, Lakshminrusimha S. Neonatal resuscitation: evolving strategies. BMC Mater Health Neonatol Perinatol. 2015;1.
6. Wall S, Lee ACC, Niermeyer S, et al. Neonatal resuscitation in low-resource settings: what, who, and how to overcome challenges to scale up? Int J Gynecol Obstetrics. 2009;107(Supplement):S47–S64. doi:10.1016/j.ijgo.2009.07.013
7. Steele C. Helping babies breathe around the world. JOGGN J Obstetric Gynecol Neonatal Nurs. 2013;42:243–246. doi:10.1111/1552-6909.12019
8. Morton SU, Brodsky D. Fetal Physiology and the Transition to Extrauterine Life. Clin Perinatol. 2016;43(3):395–407. doi:10.1016/j.clp.2016.04.001
9. World Health Organization. Guidelines on Basic Newborn Resuscitation. Guidelines on Basic Newborn Resuscitation Web site. https://www.who.int/maternal_child_adolescent/documents/basic_newborn_resuscitation/en/.
10. Wyllie J, Bruinenberg J, Roehr CC, Rudiger M, Trevisanuto D, Urlesberger B. European Resuscitation Council Guidelines for Resuscitation 2015: section 7. Resuscitation and support of transition of babies at birth. Resuscitation. 2015;95:249–263. doi:10.1016/j.resuscitation.2015.07.029
11. Ljungblad LW, Sandvik SO, Lyberg A. The impact of skilled birth attendants trained on newborn resuscitation in Tanzania: A literature review. Int J Afri Nurs Sci. 2019;11.
12. Enweronu-Laryea C, Dickson KE, Moxon SG, et al. Basic newborn care and neonatal resuscitation: a multi-country analysis of health system bottlenecks and potential solutions. BMC Pregnancy Childbirth. 2015;15(Suppl 2):S4.
13. Skåre C, Kramer-Johansen J, Steen T, et al. Incidence of Newborn Stabilization and Resuscitation Measures and Guideline Compliance during the First Minutes of Life in Norway. Neonatology. 2015;108(2):100–107. doi:10.1159/000431075
14. Wrammert J, Sapkota S, Baral K, Kc A, Malqvist M, Larsson M. Teamwork among midwives during neonatal resuscitation at a maternity hospital in Nepal. Women Birth. 2017;30(3):262–269. doi:10.1016/j.wombi.2017.02.002
15. Alhassan A, Fuseini AG, Osman W, Basour Adam A. Knowledge and Experience of Neonatal Resuscitation among Midwives in Tamale. Nurs Res Pract. 2019;2019:3652608. doi:10.1155/2019/3652608
16. Kassab M, Alnuaimi K, Mohammad K, Creedy D, Hamadneh S. Midwives’ Experiences, Education, and Support Needs Regarding Basic Newborn Resuscitation in Jordan. Clin Nurs Res. 2016;25(3):291–309. doi:10.1177/1054773815619388
17. Moshiro R, Ersdal HL, Mdoe P, Kidanto HL, Mbekenga C. Factors affecting effective ventilation during newborn resuscitation: a qualitative study among midwives in rural Tanzania. Glob Health Action. 2018;11(1):1423862. doi:10.1080/16549716.2018.1423862
18. Graham S, Gill A, Lamers D. A midwife program of newborn resuscitation. Women Birth. 2006;19(1):23–28. doi:10.1016/j.wombi.2005.12.002
19. Carolan-Olah M, Kruger G, Brown V, Lawton F, Mazzarino M. Development and evaluation of a simulation exercise to prepare midwifery students for neonatal resuscitation. Nurse Educ Today. 2016;36:375–380. doi:10.1016/j.nedt.2015.09.009
20. Mildenberger C, Ellis C, Lee K. Neonatal resuscitation training for midwives in Uganda: strengthening skill and knowledge retention. Midwifery. 2017;50:36–41. doi:10.1016/j.midw.2017.03.017
21. Rovamo LM, Mattila -M-M, Andersson S, Rosenberg PH. Testing of midwife neonatal resuscitation skills with a simulator manikin in a low-risk delivery unit. Pediatrics Int. 2013;55(4):465–471. doi:10.1111/ped.12083
22. Lindseth A, Norberg A. A phenomenological hermeneutical method for researching lived experience. Scand J Caring Sci. 2004;18(2):145–153. doi:10.1111/j.1471-6712.2004.00258.x
23. Creswell JW, Poth CN. Qualitative Inquiry & Research Design: Choosing Among Five Approaches.
24. Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105–112. doi:10.1016/j.nedt.2003.10.001
25. World Medical Association. Declaration of Helsinki Ethical Principles for Medical Research Involving Human Subjects 1964
26. Ricoeur P. Interpretation Theory: Discourse and the Surplus of Meaning. Fort Worth, Texas: Texas Christian University Press; 1976.
27. McCormack B, McCance T, Klopper H. Person-Centred Practice in Nursing and Health Care: Theory and Practice.
28. Trevisanuto D, De Bernardo G, Res G, et al. Time Perception during Neonatal Resuscitation. J Pediatr. 2016;177:103–107. doi:10.1016/j.jpeds.2016.07.003
29. Slater P, O’ Halloran P, Connolly D, McCormack B. Testing of the Factor Structure of the Nursing Work Index‐Revised. Worldviews Evid Based Nurs. 2010;7(3):123–134. doi:10.1111/j.1741-6787.2009.00158.x
30. Khriesat W, Kassab M, Hamadneh S, Mohammad K, Hamadneh J, Khader YS. Infant Resuscitation Practices of Midwives in a Developing Country. Adv Neonatal Care. 2017;17(5):400–406. doi:10.1097/ANC.0000000000000418
31. Rubio-Gurung S, Putet G, Touzet S, et al. In situ simulation training for neonatal resuscitation: an RCT. Pediatrics. 2014;134(3):e790–e797. doi:10.1542/peds.2013-3988
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.