Back to Journals » Journal of Pain Research » Volume 13
Balance Control in Patients with Subacute Non-Specific Low Back Pain, with and without Lumbar Instability: A Cross-Sectional Study
Authors Hlaing SS ![]() , Puntumetakul R
, Puntumetakul R ![]() , Wanpen S, Boucaut R
, Wanpen S, Boucaut R
Received 22 September 2019
Accepted for publication 8 April 2020
Published 23 April 2020 Volume 2020:13 Pages 795—803
DOI https://doi.org/10.2147/JPR.S232080
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Robert B. Raffa
Su Su Hlaing,1,2 Rungthip Puntumetakul,2,3 Sawitri Wanpen,2,3 Rose Boucaut4
1Human Movement Sciences, School of Physical Therapy, Faculty of Associated Medical Sciences, Khon Kaen University, Khon Kaen 40002, Thailand; 2Research Center in Back, Neck, Other Joint Pain and Human Performance, Khon Kaen University, Khon Kaen 40002, Thailand; 3School of Physical Therapy, Faculty of Associated Medical Sciences, Khon Kaen University, Khon Kaen 40002, Thailand; 4International Centre for Allied Health Evidence, University of South Australia, School of Health Sciences, Adelaide, SA 5001, Australia
Correspondence: Rungthip Puntumetakul
School of Physical Therapy, Faculty of Associated Medical Sciences, Khon Kaen University, 123 Mittraphap Road, Muang District, Khon Kaen 40002, Thailand
Tel +66 834196186
Fax +66 432020856
Email [email protected]
Background: Patients with low back pain (LBP) have poorly coordinated neuromuscular control, which may alter the normal postural stability of the spine. Altered movement control may occur at any stage of LBP.
Purpose: (1) To identify differences in balance control and proprioceptive sense between subacute non-specific LBP (NSLBP) patients with and without lumbar instability (LI) and healthy subjects and (2) to investigate the correlation between factors of motor control deficits and balance.
Patients and Methods: Thirty-six participants matched by gender, age, and body mass index (BMI) were allocated into three groups of 12: subacute NSLBP patients with LI, subacute NSLBP patients without LI, and healthy subjects. Balance, proprioceptive sense, pain, functional disability, and fear of movement were evaluated.
Results: Subacute NSLBP patients with LI exhibited greater impairments in balance control, proprioceptive sense, and functional ability than patients without LI (p< 0.05). Subacute NSLBP patients showed more impairments in balance control, proprioceptive sense, and fear of movement than healthy subjects (p< 0.001), with the following effect sizes (partial η2) for static balance on stable and unstable surface: 0.597 and 0.560, anticipatory balance: 0.417, and dynamic balance: 0.536; proprioceptive sense: 0.676; and fear of movement: 0.379. Significant fair correlations were found between (1) static balance and proprioceptive sense, functional disability, and fear of movement; (2) functional reach test (FRT) and pain; and (3) the five times sit to stand test (FTSTS) and functional disability.
Conclusion: Subacute NSLBP patients with LI showed greater impairment in balance control than patients without LI. Reduced proprioceptive sense, increased pain, functional disability, and fear of movement were fairly related to impaired balance.
Keywords: motor control, joint repositioning error, non-specific low back pain, instability
Introduction
Low back pain (LBP) is one of the most common musculoskeletal disorders and a leading cause of activity limitation that can eventually result in disability, decreased quality of life, and work absenteeism.1–3 Approximately 85–95% of LBP cases have no identifiable cause or pathology and are thus categorized as non-specific LBP (NSLBP).4,5 A previous systematic review estimated the worldwide prevalence of chronic LBP to be 20.1%, increasing linearly from the third decade of a lifetime.6 In Myanmar, LBP is the most prevalent musculoskeletal disorder and approximately 30% of patients who attend physiotherapy departments suffer from LBP. Candotti and coworkers (2015) conducted an epidemiological study in Brazil and determined that 27.7% of back pain patients suffered from a functional disability, with postural changes of the spine present in 22.7% of subjects.7
Optimal postural control is critical for performing daily functional activities. In patients with NSLBP, the underlying mechanism of impaired postural control is unclear and may be affected by many factors.8,9 For example, pain may cause a reduction in joint position sense.9–11 Further, key stabilization muscles of the trunk, the lumbar multifidus (LM) muscles, can atrophy within 24 hours of LBP onset, leading to impaired proprioception and spinal stability.12–14 Sub-optimal motor control may increase the compressive load on the spine, leading to further injury and pain.10,15
Previous commentary reviews have proposed that adaptation to pain leads to the redistribution of activity within and between muscles in patients with LBP, causing patients to move differently and altering their motor control.16,17 Adaptations in motor control arising from LBP have shown an inconsistent, large degree of individual variation and are classified into two types: tight control and loose control. Such motor behavior adaptations are only beneficial in the short term and may lead to long-term consequences that compromise the quality of movement and increase trunk stiffness with decreased damping (velocity control).15 Further, decreased quality of postural recovery and greater perturbation to the spine may occur due to less frequently used preparatory motion, which may impair spinal stability.18
Patients with NSLBP who adapt with the loose type of control demonstrate reduced spinal motor control, which may be related to the inconsistent rapid and larger amplitude movements when repeating the same task. Spinal motor control failure causes larger degrees of tissue strain, leading to lumbar instability (LI). LI is defined as the inability of the stabilizing system of the spine to retain the spinal neutral zones within physiological limits.19 The neutral zone is the area in which spinal flexibility is high and spinal motion is produced against minimal internal resistance. Spinal stability is delivered by three systems: the passive, active, and neural control subsystems.19 Dysfunction in any one of these stabilization systems results in lumbar spine instability.
Altered movement control may occur at any stage of LBP, and abnormally large intervertebral motions in patients with LI may cause tissue strain and pain and affect the segmental stability of the spine.19 Sung et al explored the dysfunction of motor control in patients with acute and subacute LBP.20 However, their study results could not be generalized to patients with subacute LBP because they only studied a subgroup of patients with trunk movement coordination impairment. To date, there remains a lack of knowledge concerning differences in trunk motor control deficits between subacute NSLBP patients with LI and those without LI.
If balance impairment is identified early in the onset of LBP, it can provide useful clinical information that could be incorporated into rehabilitation programs. This could help to reduce the recurrence rate of NSLBP and prevent transition to a chronic stage. The present study aimed to examine balance control in subacute NSLBP patients with and without LI and determine factors associated with impaired balance.
Methods
Participants
This cross-sectional study involved both participants with subacute NSLBP and healthy subjects. Participants with sub-acute NSLBP referred by medical doctors for physiotherapy treatment were recruited as outpatients from the Department of Physiotherapy at the Spine Center of Yangon Orthopedic Hospital (Myanmar). Twelve participants who had not had LBP in the prior three months were recruited as healthy, asymptomatic subjects through invitations distributed via social media and flyers.
The inclusion criteria required that each NSLBP participant be 20–50 years old, have subacute NSLBP of a duration between 6 and 12 weeks, be without radiating pain below the knee, experience a moderate level of pain as measured by the visual analog scale (VAS; 3–7), and experience functional disability as indicated by a modified Oswestry Disability Questionnaires (MODQ) score of 19% or greater.
The exclusion criteria for all study participants were as follows: serious spinal pathologies and deformities, sensory and neurological deficits, changes in reflex or abnormal sensations of the lower extremities related to spinal nerve root involvement, congenital abnormalities, spondylolisthesis, osteoarthritis, rheumatoid arthritis, ankylosing spondylitis, and visual and vestibular disorders. Subjects with lower extremity injuries that had occurred within the prior six months, brain injuries, pregnancies, body mass indexes (BMI) >30 kg/m2, and conditions affecting balance (eg, drug or alcohol consumption) were excluded.
Screening Procedure
Screening tests were used to determine eligibility to participate in the study, and demographic data were collected through direct interviews. All participants were screened with dizziness handicap inventory questionnaires to exclude vestibular disorders. Participants with subacute NSLBP were categorized into two groups (with LI and without LI) through clinical testing for LI.20–24 Subacute NSLBP patients who presented with at least five signs from 14 clinical tests of LI were classified as having LI. These 14 tests were as follows: sit to stand, lumbar flexion >53 degrees, total extension >26 degrees, interspinous gap change during flexion-extension, an aberrant movement pattern test, Beighton’s hypermobility scale >2 points, painful catch sign test, passive lumbar extension test, passive accessory intervertebral movements test, passive physiological intervertebral movements test in flexion and extension, posterior shear test, prone instability test, and average straight leg raising >91 degrees.
The inter-rater reliabilities of the 14 clinical tests for LI were determined before the onset of the study through the assessment of 10 participants by two different researchers, each having many years of experience in assessing LI. The agreement percentages between the researchers ranged from 70% to 100% with kappa values ranging from 0.35 to 1.00. The sensitivity and specificity of the 14 clinical tests for LI are described in Appendix 1.
Thirty-six subjects were matched by gender, age (± 5 years), and BMI (±2 kg/m2).20 Subjects were allocated into one of three groups of 12 (1:1:1): subacute NSLBP patients with LI, subacute NSLBP patients without LI, and healthy subjects. A flow diagram shows the steps followed by participants throughout the course of the study (Figure 1).
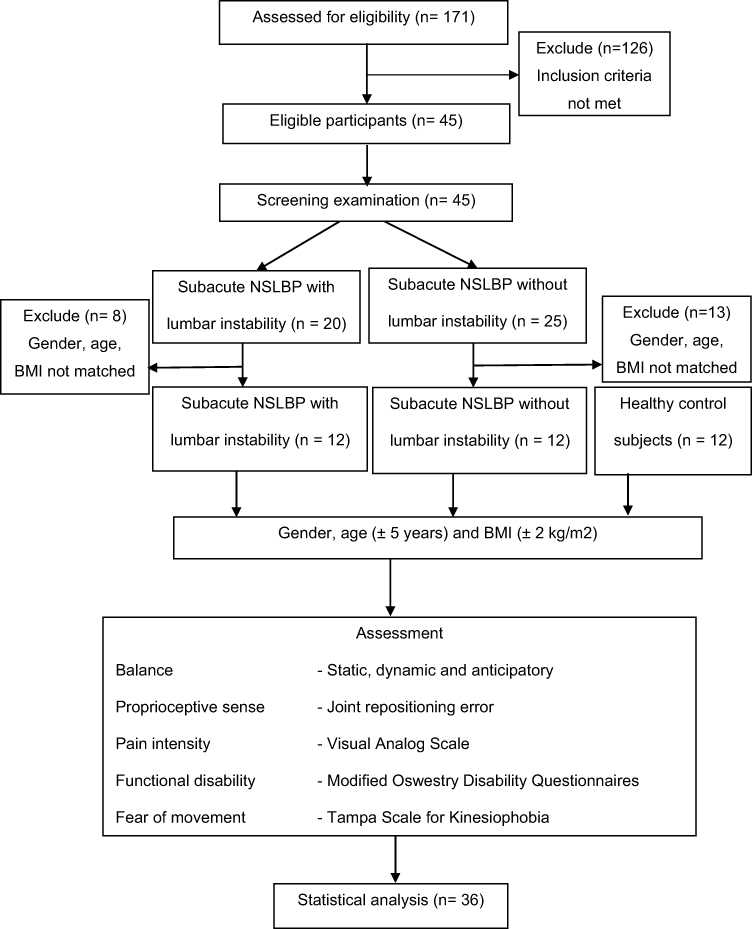 |
Figure 1 Flow diagram of the participant pathway through the study. |
Assessment Procedure
At first, participants were assessed subjectively: pain was measured using the VAS, functional disability was determined using the MODQ, and the Tampa Scale for Kinesiophobia (TSK) was used to evaluate fear of movement. Next, proprioceptive sense was measured with participants in the sitting position. Finally, balance (static, anticipatory, and dynamic) was assessed. Each of the tests was performed three times with one-minute rest intervals, and the average values of the measurements were considered for analysis. The testing procedures for proprioception and balance were performed as follows.
Proprioceptive Sense
Joint repositioning error was used to assess proprioceptive sense. Each participant was asked to sit with their feet supported and their arms placed on their thighs, and the examiner guided the lumbar spine to a neutral position (hips 90° and knees 90°). A 10-cm tape measure with mm markings was placed on the lumbosacral region, with the central marking (5 cm) on sacral segment 1 (S1) as the starting point of the measurement. A laser pointer was placed on a stable base and adjusted to be level and positioned directly on the starting point. The participant was instructed to remember the target position (neutral); move from the maximum anterior tilt to the maximum posterior tilt twice, maintaining each position for 5 seconds; and then return to the neutral target position. The deviation from the starting point was measured in cm using the laser line on the tape measure.25,26 The participants practiced the repositioning test twice before the assessment started.
Balance
Static, anticipatory, and dynamic balance were assessed with Romberg’s test, the FRT, and the FTSTS, respectively.
Romberg’s test was used to investigate static balance control. The participants were tested in a single-leg stance with their eyes open, first on a stable surface (SS) and then on an unstable surface (SUS).27,28 For the starting position, each participant stood on their dominant leg (determined by the football kicking test),29 with the unsupported leg in the neutral hip and 90º knee flexion position and their arms crossed at chest level; the examiner observed this position for 60 seconds.30–32 In each test condition (SS and SUS), each participant was asked to hold the position and the amount of time for which they held the position was recorded.
A functional reach test was used to measure anticipatory balance control. Each participant stood beside a wall and was instructed to reach forward, perpendicular to a wall, with their shoulders flexed at 90 degrees and with their elbows extended. The distance from the starting point to the reach point was measured with a measuring tape from the location of the third metacarpal along the horizontal axis.33,34
The five times sit to stand test (FTSTS) was used to measure dynamic balance control and functional alteration of transitional movement. Each subject sat on a standard chair (height = 43 cm, depth = 47.5 cm) with their arms crossed over their chest. The timer started when the assessor said “go” and stopped when the subject’s buttocks touched the chair after the fifth repetition.35
Inter-rater reliability tests for the balance and proprioceptive sense tests were performed on 10 patients with subacute NSLBP. These tests showed excellent reliability (intraclass correlation coefficient (ICC): 0.92–1).36
Sample Size
Sample size was calculated by detecting the mean difference of percentage changes of dynamic balance (FTSTS test) between the groups (∆2=10.56) and by using a pooled variance estimation (σ2=1.08) from the pilot study. The sample size was calculated with a test power of 0.80 and α=0.05. At least 11 subjects from each group were needed for this calculation. In the present study, there were 12 subjects in each group, totaling 36 subjects across all groups.
Statistical Analysis
The STATA version 10.1 (StataCorp, 4905 Lakeway Drive College Station, Texas 77845, USA) was used to analyze all data. Demographic characteristics among the three groups, including age, weight, height, and BMI, were calculated. The Shapiro–Wilk test was used to test for the normality distribution of all data. One-way analysis of variance (ANOVAs) was used to explore significant differences between the participant groups. Bonferroni post-hoc tests were used to identify the locations of significant differences within each analysis. Bivariate Pearson correlations were used to determine existing relationships between balance and factors of motor control deficits. The significance level was set at p<0.05.
Results
The demographic data and clinical characteristics of all participants are shown in Table 1. There were no significant differences in demographic data or clinical characteristics between the three groups (p>0.05).
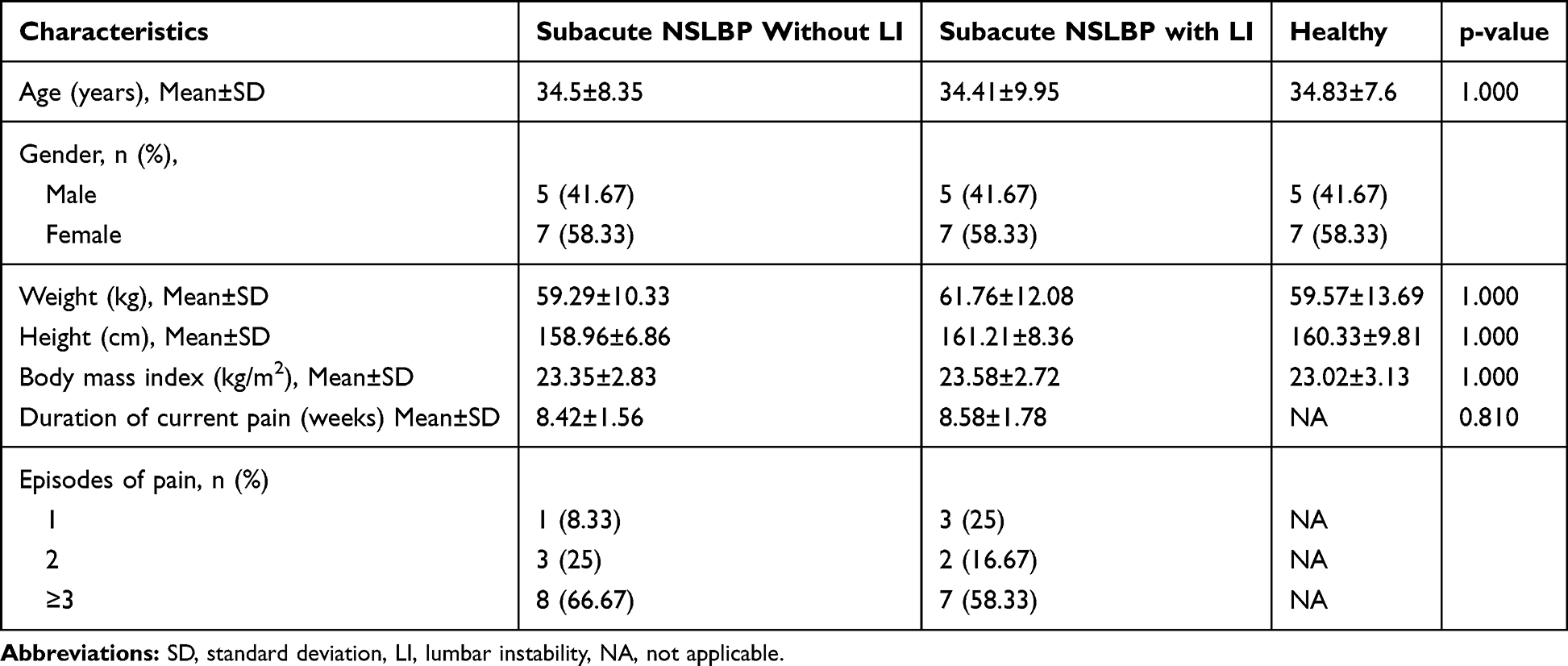 |
Table 1 Demographic and Clinical Characteristics of the Participants (n= 12 in Each Group) |
Significant differences among the three groups on measures of balance control, proprioception, and fear of movement (p<0.001) are presented in Table 2. The effect sizes were as follows: static balance on stable and unstable surface: partial η2=0.597 and partial η2 =0.560, anticipatory balance: partial η2=0.417, and dynamic balance: partial η2=0.536; proprioception: partial η2=0.676, and fear of movement: partial η2 =0.379.
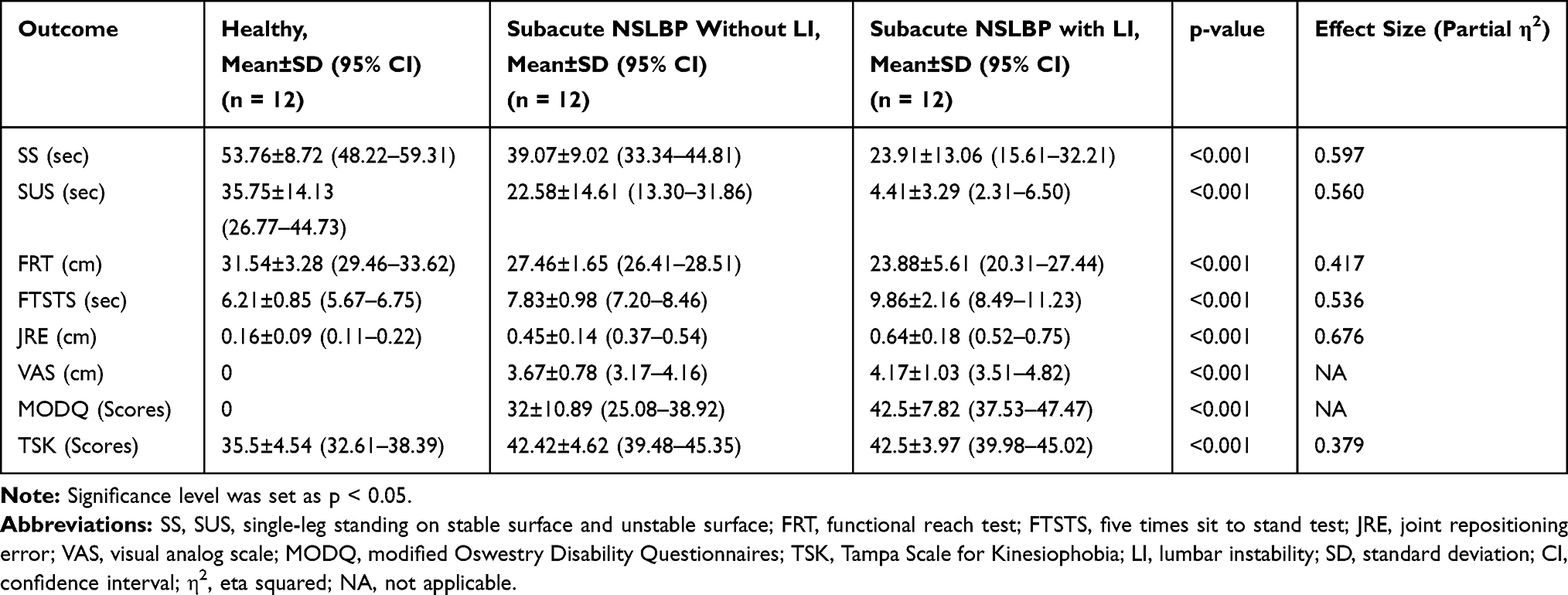 |
Table 2 Comparison of Outcome Variables in Healthy Subjects, Subacute NSLBP Patients Without and with Lumbar Instability |
As shown in Table 3, among the two groups of subacute NSLBP patients with and without LI, the LI subjects exhibited more impairment than the subjects without LI in standing balance on both stable (p=0.004) and unstable surfaces (p=0.002), in FTSTS (p=0.005), in joint repositioning error (p=0.009), and in functional disability (p=0.007). No significant differences were found between subacute NSLBP patients with LI and subacute NSLBP patients without LI for the FRT (p=0.090), pain (p=0.330), or fear of movement (p=1.000).
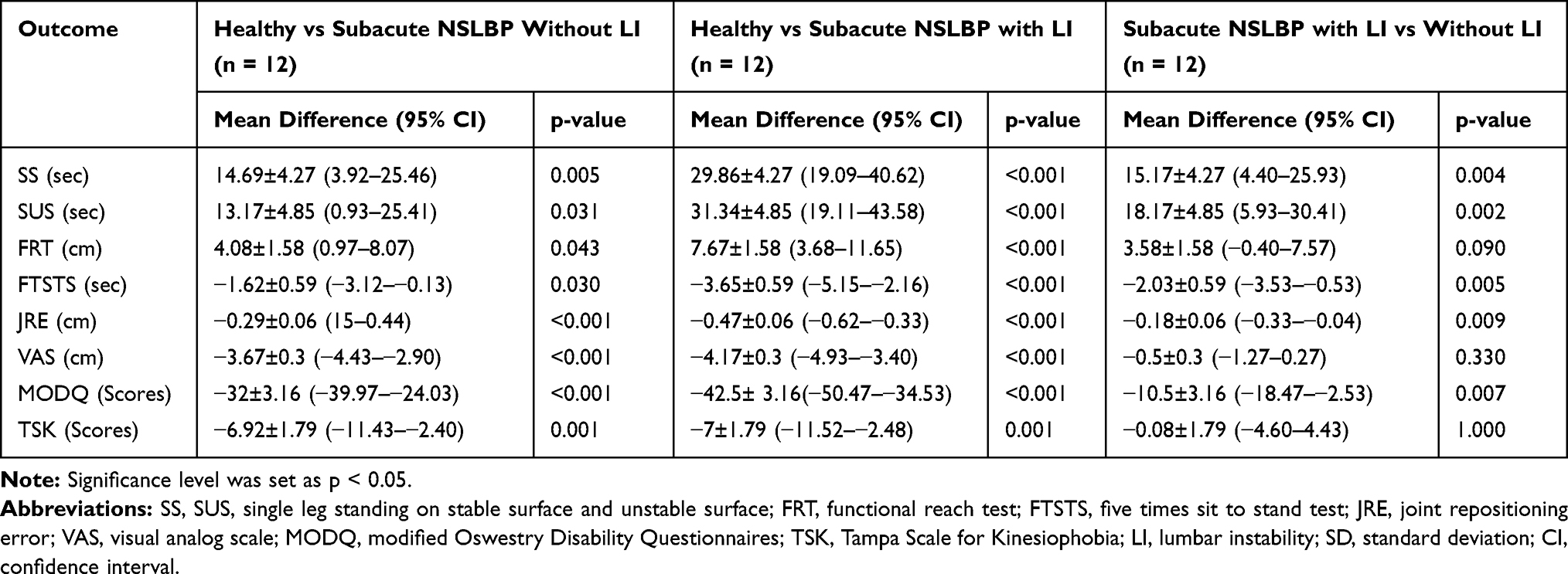 |
Table 3 Comparison of Balance, Proprioceptive Sense, Pain, Functional Disability and Fear of Movement Between Groups |
The correlation results regarding balance and factors of motor control deficits in patients with subacute NSLBP are listed in Table 4. Significant negative correlation was found between standing on a stable surface with functional disability (r= −0.367, p=0.039), standing on an unstable surface with joint repositioning error (r= −0.349, p=0.047), functional disability (r= −0.526, p=0.004), fear of movement (r=−0.350, p=0.047), and pain with the FRT (r= −0.423, p=0.020). In contrast, FTSTS was significantly, positively correlated with functional disability (r=0.460, p=0.012) and fear of movement (r=0.349, p=0.047). There was a significant fair correlation between balance and factors of motor control deficits.
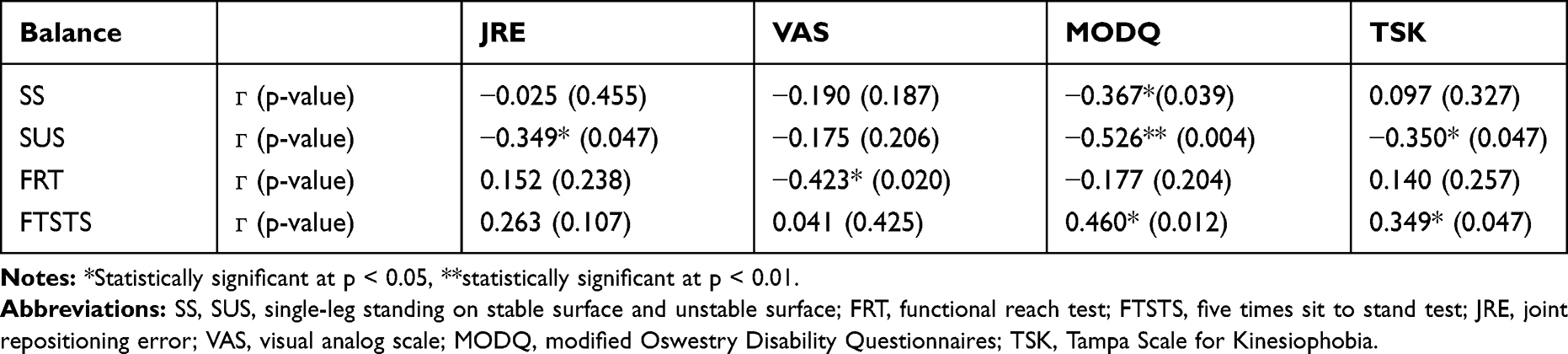 |
Table 4 Pearson Correlation Between Balance and Motor Control Deficit Factors in Subacute Nonspecific Low Back Pain (n= 24) |
Discussion
Impairment in the static and dynamic balance of patients with LI may result from a loss of spinal motion stiffness due to reduced excitability of the trunk muscles.17 This may lead to increasingly abnormal segmental spine mobility, which may trigger a significant alteration in the major stabilizing structure of the spine.19 In the present study, LBP patients with LI exhibited more impairment in static balance control than LBP patients without LI. Changes in somatosensory input and motor organization also affect the stability of the spine, resulting in impaired balance control.22 Further, sustained end-range movement causes tissue strain, pain, and degeneration of the spine.37 Chronic LBP patients with LI have reduced strength, reduced endurance, and delayed onset time with limited feed-forward activation of the LM muscle compared to healthy controls and chronic LBP patients without LI.38,39
Subacute NSLBP patients with and without LI had more impairment in balance control, proprioception, and fear of movement than healthy subjects (p < 0.001). These findings are in line with those of previous studies that concluded that patients with chronic LBP had more motor control impairments in the standing position when compared to healthy control subjects.40,41 A recent systematic review by Koch and Hȁnsel (2019) also concluded that there were differences in certain parameters of postural control in quiet standing between patients with NSLBP and healthy subjects.42
A previous study by Sung et al evaluated the lumbar stability index, relative standstill time, of patients with and without LBP and found that the stability index significantly decreased, particularly when visual feedback was blocked, for patients with LBP.43 In the present study, patients with subacute NSLBP demonstrated a shorter single-leg standing time than healthy control subjects, even with their eyes open. This finding supports the previous work of Mok et al, which concluded that balance control quality is compromised in patients with LBP and is associated with poor use of spinal motion.44
Comparing proprioceptive sense between the three participant groups of the current study – that is, subacute NSLBP patients with and without LI and healthy control subjects – healthy subjects displayed minimum joint reposition error, whereas subacute NSLBP patients with LI presented maximum joint reposition error. This may have been because patients with LI have disordered segmental stability with reduced proprioceptive acuity due to disrupted afferent input from the injured muscle spindles. The results of a previous study by Brumagne et al revealed that proprioception was altered in patients with LBP, whereas Asell et al found no difference in joint repositioning error between NSLBP patients and healthy control subjects; this inconsistence finding may have been due to the heterogeneity of assessment methods and familiarization processes used in these studies.45,46
Although pain intensity did not differ significantly between the two groups of subacute NSLBP, the patients with LI showed more functional disability than the subacute NSLBP patients without LI. This difference may have arisen from segmental instability due to disorders in the spinal control systems. Recent commentary articles by van Dieën et al proposed that patients with LI may use a loose type of control arising from decreased postural control variability and increased compressive load and degeneration of the spine, which could lead to disability and recurrent pain.17 This idea seems to support our finding that subacute NSLBP patients with LI have greater functional impairment than subacute LBP patients without LI.
The greater level of fear of movement found in subacute NSLBP patients may have been due to patients relying less on fine-tuning motor control and exhibiting spine stiffening strategies to enhance spinal stability. Excessive spinal movements and sustained end-range alignment result in excessive tissue strain and pain.37 Muscle splinting, stiffening a segment to prevent movement, and planning to splint the painful area may occur as an adaptation to acute pain/injury and lead to further problems. Karayannis and coworkers (2013) reported that fear of movement was positively associated with trunk stiffness in patients with LBP.47 Although our study examined patients with subacute NSLBP, almost 70% of patients had more than three episodes of previous pain. This could have influenced our findings due to residual motor control deficits.
The negative fair correlation found between standing balance on an unstable surface and joint repositioning error, functional disability, and fear of movement may have arisen from a deficit in the functioning of key stabilization muscles of the trunk triggered by changes in sensory signals that cause alterations in sensory-motor control. Additionally, deep LM muscles in patients with subacute NSLBP perform an extensor function instead of a nondirectional recruitment pattern and exhibit a stiffening strategy that may adversely affect postural stability and balance.48 Decreased proprioceptive acuity in patients with subacute NSLBP may reduce their ability to retain a neutral spinal posture, reduce coordinated muscle activation, decrease spinal segmental movement, and reduce reliance on fine-tuning motor control, possibly leading to disability and recurrent pain.
The significant, negative fair correlation between the functional reach test and pain, and the positive fair correlation between the five times sit to stand test and functional disability may have occurred because patients with subacute NSLBP used a stiffening strategy for motor control, which corresponded to their pain levels. Thus, patients with severe pain have minimal forward reach, and more disabled patients require more time to perform the five times sit to stand test.
Limitations
There were some limitations to the present study. The present study used 14 clinical tests of LI to categorize patients with and without LI; these tests are commonly used by physiotherapists in the clinic. Functional flexion-extension radiography must be performed to confirm the clinical categorization of the LBP patients into two groups (having LI and not having LI); however, this method is high-tech and costly. The sample size recruited for this study was only adequate for the first objective; future research should consider whether the sample size is adequate to address all the study objectives. Unfortunately, the findings of previous studies could not have been used to make calculations based on the magnitude of the differences found or effect sizes as no similar study has reported on the subacute stage of NSLBP. Finally, future studies should utilize electromyography (EMG) to detect the activity of the trunk muscles in subacute NSLBP patients with and without LI.
Conclusion
The present study revealed that subacute NSLBP patients with LI showed greater impairment than NSLBP patients without LI across multiple tests of static and dynamic balance, proprioceptive sense, and functional disability. Patients with subacute NSLBP displayed significantly impaired balance control and proprioceptive sense compared to matched healthy subjects. Clinically, this suggests that treatment of LBP should focus not only on pain and disability but also on the resolution of motor control changes.
Data Sharing Statement
The authors will allow sharing of deidentified participant data, about balance and proprioception. The data will be available for anyone who wishes to access the data for any purpose. The data will be accessible immediately following publication, and within six months of the publication date. Contact should be made via the principal investigator [email protected].
Ethics and Consent Statement
This study was approved by the Ethics Committees for human research of the Khon Kaen University (Thailand) and the University of Public Health (Myanmar) in accordance with the Declaration of Helsinki. The study was registered at clinical trials.in.th (registration number: TCTR20180829002). All eligible participants were provided with an explanation about the objectives and procedures of the study and were asked to sign an informed consent form prior to commencing the study.
Acknowledgments
The authors thank the participants for their willingness to participate in this study, Research Center in Back, Neck, Other Joint Pain and Human Performance (BNOJPH), and Khon Kaen University, Khon Kaen, Thailand for providing the research funding.
Author Contributions
All the authors of this study contributed based on the substantial contributions to conception and design, data acquisition, or data analysis and interpretation; drafting the article or critically revising it for important intellectual content; final approval of the version to be published; and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of the work are appropriately investigated and resolved.
Disclosure
All of the authors report they have no conflicts of interest in this work.
References
1. Airaksinen O, Brox JI, Cedraschi C, et al. Chapter 4. European guidelines for the management of chronic nonspecific low pain. Eur Spine J. 2006;15(S2):S192–300. doi:10.1007/s00586-006-1072-1
2. Delitto A, George SZ, Van Dillen L, et al. Low back pain: clinical practice guidelines linked to the international classification of functioning, disability, and health from the orthopaedic section of the American Physical Therapy Association. J Orthop Sports Phys Ther. 2012;42(4):A1–A57. doi:10.2519/jospt.2012.42.4.a1
3. Itz CJ, Geurts JW, Kleef MV, et al. Clinical course of non‐specific low back pain: a systematic review of prospective cohort studies set in primary care. Eur J Pain. 2013;17(1):5–15. doi:10.1002/j.1532-2149.2012.00170.x
4. Deyo RA, Weinstein JN. Low back pain. N Engl J Med. 2001;344(5):363–370. doi:10.1056/nejm200105243442117
5. Ehrlich GE. Low back pain. Bull World Health Organ. 2003;81(9):671–676.
6. Hoy D, Bain C, Williams G, et al. A systematic review of the global prevalence of low back pain. Arthritis Rheumatol. 2012;64(6):2028–2037. doi:10.1002/art.34347
7. Candotti CT, Noll M, Marchetti BV, et al. Prevalence of back pain, functional disability, and spinal postural changes. Fisioter Mov. 2015;28(4):711–722. doi:10.1590/0103-5150.028.004.AO08
8. Lin YH, Sun MH. The effect of lifting and lowering an external load on repositioning error of trunk flexion-extension in subjects with and without low back pain. Clin Rehabil. 2006;20(7):603–608. doi:10.1191/0269215506cr971oa
9. Ruhe A, Fejer R, Walker B. Is there a relationship between pain intensity and postural sway in patients with non-specific low back pain? BMC Musculoskelet Disord. 2011;12(1):162. doi:10.1186/1471-2474-12-162
10. Della Volpe R, Popa T, Ginanneschi F, et al. Changes in coordination of postural control during dynamic stance in chronic low back pain patients. Gait Posture. 2006;24(3):349–355. doi:10.1016/j.gaitpost.2005.10.009
11. Brumagne S, Janssens L, Knapen S, et al. Persons with recurrent low back pain exhibit a rigid postural control strategy. Eur Spine J. 2008;17(9):1177–1184. doi:10.1007/s00586-008-0709-7
12. Hide J, Stokes MJ, Saide M, et al. Evidence of lumbar multifidus muscle wasting ipsilateral to symptoms in patients with acute/subacute low back pain. Spine. 1994;19(Supplement):165–172. doi:10.1097/00007632-199401001-00009
13. Hodges P, Holm AK, Hansson T, et al. Rapid atrophy of the lumbar multifidus follows experimental disc or nerve root injury. Spine. 2006;31(25):2926–2933. doi:10.1097/01.brs.0000248453.51165.0b
14. Lonnemann ME, Paris SV, Gorniak GC. A morphological comparison of the human lumbar multifidus by chemical dissection. J Man Manip Ther. 2008;16(4):E84–92. doi:10.1179/jmt.2008.16.4.84e
15. Hodges PW, van den Hoorn W, Dawson A, et al. Changes in the mechanical properties of the trunk in low back pain may be associated with recurrence. J Biomech. 2009;42(1):61–66. doi:10.1016/j.jbiomech.2008.10.001
16. Hodge PW, Tucker K. Moving differently in pain: a new theory to explain the adaptation to pain. Pain. 2011;152(Supplement):S90–98. doi:10.1016/j.pain.2010.10.020
17. van Dieën JH, Reeves NP, Kawchuk G, et al. Motor control changes in low-back pain: divergence in presentations and mechanisms. J Orthop Sports Phys Ther. 2018:1–24. doi: 10.2519/jospt.2019.7917.
18. Mok NW, Brauer SG, Hodges PW. Failure to use movement in postural strategies leads to increased spinal displacement in low back pain. Spine. 2007;32(19):E537–E543. doi:10.1097/BRS.0b013e31814541a2
19. Panjabi MM. The stabilizing system of the spine part I: function, dysfunction, adaptation, and enhancement. J Spinal Disord. 1992;5(4):383–389. doi:10.1097/00002517-199212000-00001
20. Sung W, Abraham M, Plastaras C, et al. Trunk motor control deficits in acute and subacute low back pain are not associated with pain or fear of movement. Spine. 2015;15(8):1772–1782. doi:10.1016/j.spinee.2015.04.010
21. Cook C, Brismee JM, Sizer PS. Subjective and objective descriptions of clinical lumbar spine instability: a delphi study. Man Ther. 2006;11(1):11–21. doi:10.1016/j.math.2005.01.002
22. Hicks GE, Fritz JM, Delitto A, et al. Interrater reliability of clinical examination measures for identification of lumbar segmental instability. Arch Phys Med Rehabil. 2003;84(12):1858–1864. doi:10.1016/S0003-9993(03)00365-4.
23. Hicks GE, Fritz JM, Delitto A, et al. Preliminary development of a clinical prediction rule for determining which patients with low back pain will respond to a stabilization exercise program. Arch Phys Med Rehabil. 2005;86(9):1753–1762. doi:10.1016/j.apmr.2005.03.033
24. Magee DJ. Orthopaedic Physical Assessment.
25. Enoch F, Kjaer P, Elkjaer A, et al. Inter-examiner reproducibility of tests for lumbar motor control. BMC Musculoskelet Disord. 2011;12(1):114. doi:10.1186/1471-2474-12-114
26. Puntumetakul R, Chalermsan R, Hlaing SS, et al. The effect of core stabilization exercise on lumbar joint position sense in patients with subacute non-specific low back pain: a randomized controlled trial. J Phys Ther Sci. 2018;30(11):1390–1395. doi:10.1589/jpts.30.1390
27. Bohannon RW, Larkin PA, Cook AC, et al. Decrease in timed balance test scores with aging. Phys Ther. 1984;64(7):1067–1070. doi:10.1093/ptj/64.7.1067
28. Steffen T, Seney M. Test-retest reliability and minimal detectable change on balance and ambulation tests, the 36-item short-form health survey, and the unified parkinson disease rating scale in people with parkinsonism. Phys Ther. 2008;88(6):733–746. doi:10.2522/ptj.20070214
29. van Melick N, Meddeler BM, Hoogeboom TJ, et al. How to determine leg dominance: the agreement between self-reported and observed performance in healthy adults. PLoS One. 2017;12(12):e0189876. doi:10.1371/journal.pone.0189876
30. Bohannon RW. Single limb stance times: a descriptive meta-analysis of data from individuals at least 60 years of age. Top Geriatr Rehabil. 2006;22(1):70–77. doi:10.1097/00013614-200601000-00010
31. Goldberg A, Casby A, Wasielewski M. Minimum detectable change for single-leg-stance-time in older adults. Gait Posture. 2011;33(4):737–739. doi:10.1016/j.gaitpost.2011.02.020
32. Michikawa T, Nishiwaki Y, Takebayashi T, et al. One-leg standing test for elderly populations. J Orthop Sci. 2009;14(5):675–685. doi:10.1007/s00776-009-1371-6
33. Duncan PW, Weiner DK, Chandler J, et al. Functional reach: a new clinical measure of balance. J Gerontol. 1990;45(6):M192–197. doi:10.1093/geronj/45.6.M192
34. Norris B, Medley A. The effect of context and age on functional reach performance in healthy adults aged 21 to 94 years. J Geriatr Phys Ther. 2011;34(2):82–87. doi:10.1519/JPT.0b013e31820aac11
35. Bohannon RW, Shove ME, Barreca SR, et al. Five-repetition sit-to-stand test performance by community-dwelling adults: a preliminary investigation of times, determinants, and relationship with self-reported physical performance. Isokinet Exerc Sci. 2007;15(2):77–81. doi:10.3233/IES-2007-0253
36. Portney LG, Watkins MP. Foundations of Clinical Research: Applications to Practice. Upper Saddle River, New Jersey: Pearson Prentice Hall; 2009.
37. Panjabi MM. A hypothesis of chronic back pain: ligament subfailure injuries lead to muscle control dysfunction. Eur Spine J. 2006;15(5):668–676. doi:10.1007/s00586-005-0925-3
38. Silfies SP, Mehta R, Smith SS, et al. Differences in feedforward trunk muscle activity in subgroups of patients with mechanical low back pain. Arch Phys Med Rehabil. 2009;90(7):1159–1169. doi:10.1016/j.apmr.2008.10.033
39. Davarian S, Maroufi N, Ebrahimi I, et al. Trunk muscle strength and endurance in chronic low back pain patients with and without clinical instability. J Back Musculoskelet. 2012;25(2):123–129. doi:10.3233/BMR-2012-0320.
40. Henry SM, Hitt JR, Jones SL, et al. Decreased limits of stability in response to postural perturbations in subjects with low back pain. Clin Biomech. 2006;21(9):881–892. doi:10.1016/j.clinbiomech.2006.04.016
41. Claeys K, Brumagne S, Dankaerts W, et al. Decreased variability in postural control strategies in young people with non-specific low back pain is associated with altered proprioceptive reweighting. Eur J Appl Physiol. 2011;111(1):115–123. doi:10.1007/s00421-010-1637-x
42. Koch C, Hȁnsel F. Non-specific low back pain and postural control during quiet standing. a systematic review. Front Psychol. 2019;10:586. doi:10.3389/fpsyg.2019.00586
43. Sung PS, Yoon B, Lee DC. Lumbar spine stability for subjects with and without low back pain during one-leg standing test. Spine. 2010;35(16):E753–60. doi:10.1097/BRS.0b013e3181d53b9c
44. Mok NW, Brauer SG, Hodges PW. Changes in lumbar movement in people with low back pain are related to compromised balance. Spine. 2011;36(1):E45–52. doi:10.1097/BRS.0b013e3181dfce83
45. Brumagne S, Cordo P, Lysens S, et al. The role of paraspinal muscle spindles in lumbosacral position sense in individuals with and without low back pain. Spine. 2000;25(8):989–994. doi:10.1097/00007632-200004150-00015
46. Åsell M, Sjölander P, Kerschbaumer H, et al. Are lumbar repositioning errors larger among patients with chronic low back pain compared with asymptomatic subjects? Arch Phys Med Rehabil. 2006;87(9):1170–1176. doi:10.1016/j.apmr.2006.05.020
47. Karayannis NV, Smeets RJ, van den Hoorn W, et al. Fear of movement is related to trunk stiffness in low back pain. PLoS One. 2013;8(6):e67779. doi:10.1371/journal.pone.0067779
48. Hodges PW, Danneels L. Changes in structure and function of the back muscles in low back pain: different time points, observations, and mechanisms. J Orthop Sports Phys Ther. 2019;49(6):464–476. doi:10.2519/jospt.2019.8827
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.