Back to Journals » Infection and Drug Resistance » Volume 16
Bacteriological Quality and Antimicrobial Resistant Patterns of Foodborne Pathogens Isolated from Commonly Vended Street Foods in Arba Minch Town, Southern Ethiopia
Authors Alelign D ![]() , Yihune M
, Yihune M ![]() , Bekele M
, Bekele M ![]() , Oumer Y, Beyene K
, Oumer Y, Beyene K ![]() , Atnafu K
, Atnafu K
Received 5 March 2023
Accepted for publication 6 May 2023
Published 10 May 2023 Volume 2023:16 Pages 2883—2899
DOI https://doi.org/10.2147/IDR.S411162
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Suresh Antony
Dagninet Alelign,1 Manaye Yihune,2 Muluken Bekele,2 Yisiak Oumer,1 Kassaw Beyene,3 Kaleb Atnafu1
1Department of Medical Laboratory Sciences, Arba Minch University, Arba Minch, Ethiopia; 2School of Public Health, Arba Minch University, Arba Minch, Ethiopia; 3Department of Midwifery, Arba Minch University, Arba Minch, Ethiopia
Correspondence: Dagninet Alelign, Tel +251-964-428-118, Email [email protected]
Background: Ready-to-eat foods sold by street vendors act as potential sources for the spread of various foodborne infectious diseases. Thus, local determination of the level of foodborne bacterial pathogens and their antimicrobial resistance pattern is essential.
Methods: A community-based cross-sectional study was conducted from September 5th, 2022 to December 31th, 2022. The required data were collected by a structured questionnaire and observation checklist. Randomly selected street-vended foods were aseptically collected, and the bacteriological quality was assessed by using culture techniques. Different biochemical tests were used to identify and characterize bacterial isolates. The antimicrobial-resistant test for isolated foodborne bacterial pathogens was carried out by using the Kirby-Bauer disc diffusion method. The data were analyzed using SPSS version 22.
Results: A total of 34.2% (113/330) with a 95% CI of 29.1– 39.4 of commonly consumed street-vended foods were identified as having unsatisfactory total mean aerobic bacterial counts (> 105 CFU/g; 4.3 × 105 CFU/g). The mean total Enterobacteriaceae, coliform, and staphylococcal counts were found to be 1.4 × 105 CFU/g, 2.4 × 104 CFU/g, and 3.4 × 104 CFU/g, respectively. A total of 12.7% (42/330) of foodborne pathogens were recovered attributed to Staphylococcus aureus (31, 9.4%), Salmonella species (6, 1.8%), and E. coli O157:H7 (5, 1.5%). 6.5% and 16.1% of isolated S. aureus were found to be methicillin-resistant and multidrug-resistant (MDR), respectively. Additionally, 33.3% of Salmonella isolates and 40% of E. coli O157:H7 isolates were found to be MDR.
Conclusion: Street-vended foods in this setting have a considerable number of unsatisfactory bacterial qualities, along with drug-resistant foodborne pathogens. Thus, more effective health education and training for vendors, regular inspections of vending sites, and regular surveillance of drug resistance patterns of foodborne pathogens are all essential.
Keywords: bacteriological quality, street-vended foods, Arba Minch, Ethiopia
Introduction
Street food refers to a wide-ranging variety of readily available foods prepared and/or sold by vendors from a street side location in a public place for immediate consumption without further processing or preparation.1–3 They are very popular among urban dwellers, particularly for middle- and low-income sectors of the population, because they are relatively inexpensive, convenient, and easily accessible on the sidewalk.4–7 However, concerns have been raised about the safety and quality of street-vended foods, particularly from a food safety perspective, despite the fact that the importance of street-vended food cannot be overstated.8–10
Studies on street foods have highlighted them as a major public health risk.11,12 Epidemiological evidence has estimated that foods unsafe for consumption, including street-vended foods, cause 7.69% (600 million) of the world’s population (7.8 billion) to suffer from foodborne diseases every year, and 7.5% of all deaths (56 million) annually are due to foodborne illnesses.13,14 A great proportion is attributed to countries where street food vending is prevalent and has been implicated in up to 70% of traced outbreaks, which has necessitated that street food safety remains a principal priority.10,15 More than 60% of the burden of foodborne illnesses is associated with bacterial contamination and foodborne intoxications.14,16 Staphylococcus aureus, enteropathogenic Escherichia coli, Salmonella species, Shigella species, Bacillus cereus, and Clostridium perfringens are some of the commonly detected foodborne pathogens in street-vended food items.3,13,17
The burden associated with street foodborne diseases like diarrhoea, cholera, typhoid fever, and food poisoning can occur in individuals of all ages, while 40% of the foodborne disease burden is accounted for by school-age children and persons living in low-income sub-regions of the world.18–20 Moreover, travelers’ diarrhea associated with consumption of street-vended food is a major inconvenience for visitors arriving in low-income countries and may be an important factor inhibiting tourism.6,9,21 In Ethiopia, next to typhoid fever, foodborne-associated diarrheal disease represents the second leading cause of death.6,9,22 These are frequently attributed to a lack of basic infrastructure and services, difficulty in controlling the large numbers of street food vending operations because of their diversity, mobility, and temporary nature, unavailability of pure water, and insufficient reheating of cooked food.22–24 Likewise, those who participate in the street food vendor sector are often poorly educated, unlicensed, and untrained in food hygiene, and they work under crude, unsanitary conditions with little or no knowledge about the causes of foodborne disease.10,23
Consequently, different studies6,7,11 conducted on the microbial quality of different items of ready-to-eat foods vended on the street in low-income countries, including Ethiopia, revealed that different levels of contamination and the majority of isolated foodborne bacterial pathogens were resistant to commonly prescribed antibiotics and stated that street-vended foods were a common medium for the transmission of antimicrobial-resistant pathogens and had become a major threat in low-income countries due to the ease of infection resulting from poor living standards and a lack of access to adequate medical treatment.25–29
However, nothing has been done on the bacterial quality and antimicrobial resistance patterns of foodborne bacterial pathogens among street foods offered in the study area. While in Arba Minch town, it is common to see many street foods being sold in shops, in outdoor marketplaces, and more commonly at roadsides near waste drainage in an irregular way. It is also common to see people purchase those foods from vendors and consume them right away. Therefore, this study was designed to address the bacteriological quality and antimicrobial resistance pattern of foodborne pathogens in commonly consumed street-vended foods in Arba Minch town, southern Ethiopia.
Materials and Methods
Study Design, Study Area and Period
A community-based cross-sectional study was conducted in five vending sites (Sikela, Shecha, Yetnebersh, Limat, and Konso Sefer) of Arba Minch town, southern Ethiopia, from September 5th, 2022, to December 31st, 2022, where there are a high number of vendors and customers as well as an abundance of the types of street foods sold there. Arba Minch is the seat of administration for the Gamo Zone, which is located in southern Ethiopia, 454 kilometres away from Addis Ababa. In the town, there are many resorts, hotels, restaurants, and cafeterias, and alongside them are different ready-to-eat foods being vended in the streets of the town. The city of Arba Minch and its surroundings (the presence of 40 springs, proximity to Nech-Sar National Park, being a crocodile ranch, and being enriched with banana and mango) are endowed with diverse and impressive tourist attractions, and for the majority of tourists, street-vended fast foods are the first choice, unlike foods in hotels and resorts.
Sample Size Determination and Sampling Technique
The single population proportion formula was used with the assumptions that the proportion (p) of street-vended food samples showed total colony counts beyond the acceptable limits set for microbiological quality of ready-to-eat foods was taken from a previous study in Hawassa (31%),7 a 95% confidence level (Z α/2 = 1.96) and a 5% degree of precision (d = 0.05). As a result, 330 frequently vended and highly consumed street foods (Potato Chips (n = 75), Koker (n = 75), Sambusa (n = 75), Ambasha (n = 60), and Bombolino (n = 45)) were collected (Table 1) with a simple random sampling technique from seventy-five street food vendors at the selected five vending sites: from Sikela (n = 75), Shecha (n = 75), Yetnebersh (n = 45), Limat (n = 60) and Konso Sefer (n = 75).
 |
Table 1 The Ingredients and Description of Commonly Vended Street Foods Microbiological Analysed from Arba Minch Town, Southern Ethiopia, 2022 |
Data Collection Method and Tools
Data regarding the socio-demographic characteristics and personal hygiene practices of vendors as well as the area of sanitation in which the food was vended were collected through face-to-face interviews and observation by using structured questioners and observational checklists [Annex I].
Sample Collection and Transportation
Well-trained data collectors collected approximately 100 g of food samples aseptically using sterile aluminium foil from each item of street food and transported them using an icebox within 3–5 °C. The samples were processed in the Medical Microbiology and Parasitology Laboratory of Arba Minch University at the College of Medicine and Health Sciences within 1 hour after collection. The collected street-vended food samples were cut into smaller pieces with a sterile surgical blade, picked up with sterile forceps, and weighed at 10 g with an electronic digital scale for total aerobic bacterial, coliform, Enterobacteriaceae, and Staphylococcus counts and 25 g for Salmonella species detection. The measured 10 g and 25 g samples were homogenised in a measured volume of 90 mL and 225 mL of buffered peptone water (BPW) [Oxoid, Hampshire, UK], respectively, and shaken vigorously using a vortex to dislodge adhered bacteria.30 The homogenate sample gave a 1:10 dilution, from which further dilution was made by adding 1 mL of homogenate into 9 mL of BPW. Serial dilutions of 10−2 and up to 10−6 were made using test tubes and then inoculated into the appropriate culture media (Figure 1).6,7,30
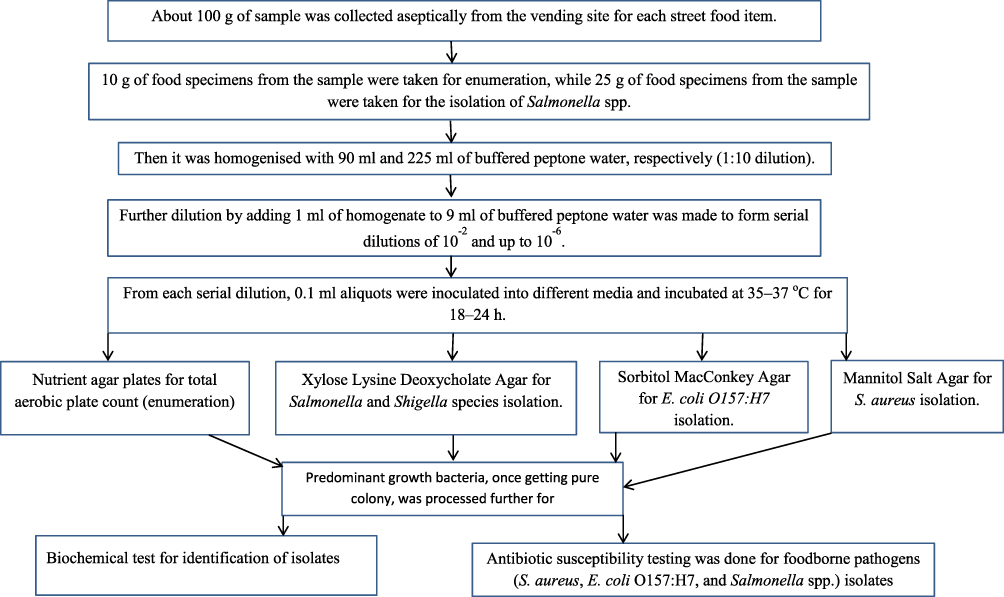 |
Figure 1 Laboratory procedures flow chart for microbiological analysis of selected street-vended foods from Arba Minch Town, Southern Ethiopia, 2022. |
Bacterial Enumeration, Isolation and Identification
In the homogenized or mixed tube, 0.1 mL of aliquots were transferred using an automatic micropipette with sterile disposable tips and spread using an L-shaped sterile wire spreader onto nutrient agar plates [Oxoid, Hampshire, UK] for the total aerobic plate count and incubated for 24–48 h at 30–35 °C. The colonies were counted from plates containing more than 30 and less than 300 microbial colonies.7,10 The average counted colonies were expressed in colony forming units per gram (CFUg−1) after multiplying by the dilution factor.2,17,31 Simultaneously, 0.1 mL aliquots of an appropriate dilution were spotted on MacConkey Agar plates and incubated at 30–35 °C for 24–48 h to count Enterobacteriaceae and coliform. Pink to reddish-purple colonies with or without haloes of precipitate were considered members of the Enterobacteriaceae, while pure pink colonies were considered coliforms. The microbiological qualities of street foods were classified by different labels; however, the classification varies among types of isolated pathogens: (a) Satisfactory: results are within expected microbiological levels and present no food safety concern. No action is required. (b) Acceptable: results are within expected microbiological levels but are at the upper range. Some action may be required to ensure food handling controls continue to be effective. (c) Unsatisfactory: results are outside expected microbiological levels and indicate poor food handling practices. Further actions are required to re-establish effective food handling controls. (d) Potentially hazardous: indicates results exceed expected microbiological levels to a level that presents an immediate food safety concern.2,17
The predominant bacterial contaminants were identified by randomly picking 10–15 colonies with distinct morphological differences such as colour, size, and shape from countable plates. After purification by repeated plating, the isolated bacteria were characterised to the genus and species level by using cell morphology, Gram staining, and different biochemical tests [HiMedia Laboratory Pvt. Ltd., Mumbai, India], such as Triple Sugar Iron Agar (TSI), Simmon Citrate, Indole production, Gas, and H2S production, Urease, Motility, Methyl Red-Voges Proskauer (MR-VP), and Oxidase.7,32,33
Isolation of Staphylococcus aureus
From the serial dilutions, 0.1 mL of the aliquot was spread onto Mannitol Salt Agar (MSA) [HiMedia Laboratory Pvt. Ltd., Mumbai, India] and incubated at 37 °C for 20–48 h. After incubation, golden yellow colonies on MSA, the catalase test (Remel Europe Ltd., Dartford, UK), coagulase activity (Remel Europe Ltd., Dartford, UK), and Gram staining were used to characterise S. aureus isolates.6,10,33
Isolation of E. coli O157:H7 Serogroup
From the serial dilutions, 0.1 mL of the aliquot was added into 5 mL of brain-heart infusion broth and incubated for 24 h at 37 °C for selective enrichment. Then, a 0.1-mL sample from the enrichments was subcultured onto Sorbitol MacConkey agar [HiMedia Laboratory Pvt. Ltd., Mumbai, India] plates recommended as the selective medium for isolation and detection of E. coli O157:H7. Unlike typical E. coli, the E. coli O157:H7 serogroup does not ferment Sorbitol and consequently grows colourless colonies following 24 h of incubation.34,35 Thus, morphologically typical colonies producing a colourless (sorbitol non-fermenter) colony were then tested for lactose fermentation on MacConkey agar [HiMedia Laboratory Pvt. Ltd., Mumbai, India] along with different biochemical tests.6,7,32,33
Isolation of Salmonella and Shigella Species
The detection was performed by taking 25 g of street food samples into 225 mL of BPW [Oxoid, Hampshire, UK] and incubated at 37 °C for 24 h. Then, 1 mL of pre-enrichment broth culture was added to 10 mL of selenite faecal broth and again incubated at 37 °C for 24 h. Thereafter, a wire loopful of suspension from a tube was streaked onto Xylose Lysine Deoxycholate Agar (XLD) [HiMedia Laboratory Pvt. Ltd., Mumbai, India]. The presumptive colonies (a black colony surrounded by a red colour) were picked off and further characterised by a battery of biochemical tests and by Gram staining.10,32,33
Antimicrobial Susceptibility Testing
Antimicrobial susceptibility test was performed on Mueller Hinton agar [HiMedia Laboratory Pvt. Ltd., Mumbai, India] by using Kirby-Bauer disk diffusion techniques.36 The inoculation was incubated at 35–37 °C for 16–18 h according to the Clinical and Laboratory Standards Institute (CLSI).37 Morphologically identical 3–5 pure colonies of foodborne pathogenic bacteria from the overnight incubated nutrient agar media were suspended in nutrient broth by using sterile wire loop with reference to 0.5 McFarland standards and incubated at 37 °C for up to 4 h. Then by using sterile cotton swab, the broth was uniformly inoculated into Mueller Hinton agar media. After 3–5 minutes of inoculation, selected antibiotic discs were applied to the surface of the medium by considered the size of the plate.
Antibiotic discs [Abtek Biologicals Ltd., UK] were selected for isolated foodborne pathogens as per the CLSI 2020 guideline37 and by considering the commonly prescribed antibiotics for the treatment of foodborne diarrhoea in the area. Penicillin (10 μg), cefoxitin (30 μg), gentamicin (10 μg), erythromycin (15μg), tetracycline (30 μg), doxycycline (30 μg), ciprofloxacin (5 μg), clindamycin (10 μg), cotrimoxazole (25 μg), and chloramphenicol (30 μg) were utilised for testing isolated S. aureus, while Salmonella spp. and E. coli O157: H7 isolates were tested with antibiotics including ampicillin (10 μg), amoxicillin-clavulanic acid (30 μg), cefepime (30μg), ceftriaxone (5 μg), meropenem (10 μg), gentamicin (10 μg), azithromycin (15 μg), tetracycline (30 μg), doxycycline (30 μg), ciprofloxacin (5 μg), cotrimoxazole (1.25 μg), and chloramphenicol (30 μg). Then, after overnight incubation at 37 °C, the diameter of the zone of inhibition was measured by millimetre and interpreted as susceptible, intermediate, or resistant.37
Data Quality Management
The quality and reliability of data was ensured from data collection up to final microbiological identification by strictly following the standard operating procedures (SOPs) and by giving adequate training and follow-up for data and sample collectors. All required equipment and reagents were autoclaved, and icebox was used for sample transportation and samples were analyzed without delay. Reagent expiration date, appropriate storage conditions, and standard control strains like Escherichia coli ATCC 25922 and Staphylococcus aureus ATCC 25923 were used to check the quality of solid and liquid culture media, biochemical tests, and performance of antibiotic disk before use as per the manufacturer’s instruction.37 Significant foodborne pathogens were identified from pure culture following standard microbiological procedures.32,33
Data Analysis and Interpretation
Data was coded and entered by using Epi-data version 4.6 and exported to SPSS version 22 for further cleaning and analysis. Descriptive statistics like frequency, mean and percentage were calculated. A binary logistic regression model was used to assess associations between dependent and independent variables. Odds ratio (OR) with its corresponding 95% confidence interval (CI) was estimated. A variable with a p-value < 0.25 in the bivariate analysis was considered as candidates for further multivariate analysis. Adjusted odds ratio (AOR) with a corresponding 95% confidence interval and variables with a p-value < 0.05 were considered as statistically significant. Microbiological quality of street foods with >105 CFU/g of aerobic bacteria or mesophiles, >104 CFU/g of Enterobacteriaceae, >103 CFU/g of coliform, >10 CFU/g of enteropathogenic E. coli and 102 to 104 CFU/g of Staphylococcus species were considered unsatisfactory for consumption with this level of contamination, which results in foodborne illness. Detection of Salmonella species within 25 gram of street-vended ready-to-eat foods and Shigella species was considered as potentially hazardous.2,17
Ethical Considerations and Consent to Participate
The project protocol was approved by the Arba Minch University College of Medicine and Health Sciences’ Institutional Research Ethics Review Board (Ref. No. IRB/1158/2021). In accordance with the Helsinki Declaration, the written consent was taken from all street food vendors and, moreover, vendors aged below 18 years old were approved by the ethics review committee to provide informed consent on their own behalf after explaining the objective of the study.
Operational Definition
Foodborne Pathogens
In this study, only Staphylococcus aureus, Salmonella species, and Escherichia coli O157:H7 isolates were considered foodborne pathogens.
Escherichia coli O157:H7
Escherichia coli O157:H7 was determined as an E. coli serogroup, which does not ferment Sorbitol and consequently grows colourless colonies on Sorbitol MacConkey agar medium following 24 h of incubation.34,35
Multidrug Resistance (MDR)
Multidrug resistance (MDR) was defined as isolated foodborne bacterial pathogens that resist at least one antimicrobial drug in three or more antimicrobial categories.37
Results
Socio-Demographic Characteristics of Street Food Vendors
Of the 75 street food vendors recruited for this study, the majority (48, 64%) were female. Thirty-three (44%) of the vendors were between the ages of 15 and 25; 23 (30.7%) were between the ages of 26 and 35; and 19 (25.3%) were over the age of 36. In relation to educational status, sixteen (21.3%) were illiterate, 28 (37.3%) and 26 (34.7%) had completed their primary and secondary school, respectively, and five (6.7%) were in college or above. About 26 (34.7%), 38 (50.7%), and 11 (14.5%) vendors had vending experience of less than five years, six to ten years, and more than eleven years, respectively, and about 51 (68%) vendors were unmarried.
Food-Handling and Hygienic Practices of Vendors
Among the overall food vendors, 28 (37.3%) vendors were ambulant, and 22 (29.3%) vendors had the practice of handling food for customers with their bare hands. While serving food, only 16 (21.3%) vendors were covered their hair. About 55 (73.3%) vendors reported having no training in managing and ensuring the safety of food. Despite the fact that 45 (60%) vendors were aware of foodborne illnesses from various sources, 8 (10.6%) vendors had a history of a foodborne illness, especially diarrhea and abdominal cramps. Closed bins and toilets were inaccessible for 24 (32%) and 38 (50.7%) vendors, respectively, at nearby vending sites (Table 2).
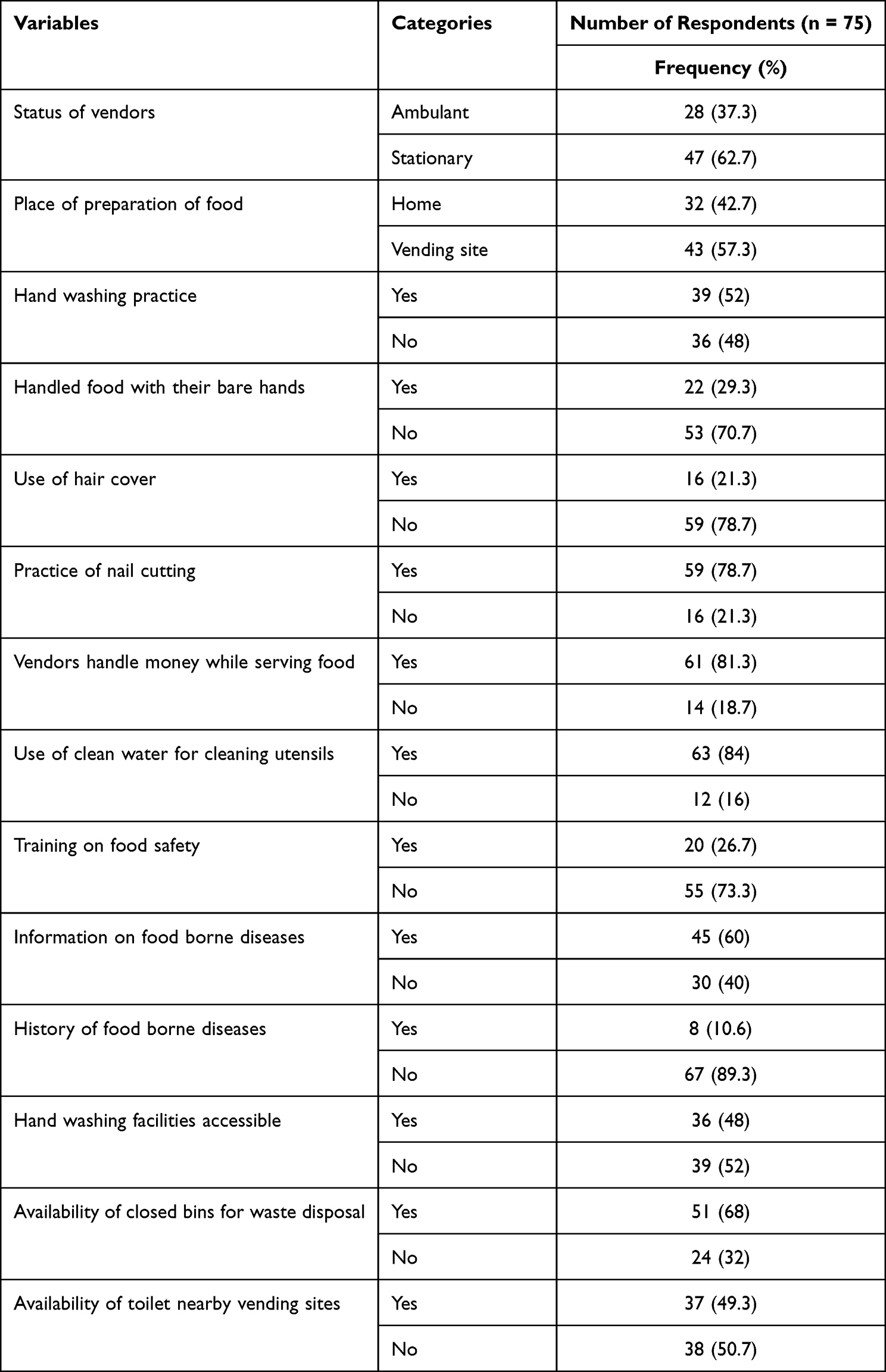 |
Table 2 Food-Handling Practices, Vendors Personal Hygiene and Awareness on Foodborne Disease in Arba Minch Town, Southern Ethiopia, 2022 |
Hygiene of Commonly Vended Street Foods
A total of 330 samples of street food—Potato Chips (75, 22.7%), Sambusa (75, 22.7%), Koker (75, 22.7%), Ambasha (60, 18.2%), and Bombolino (45, 13.6%)—were gathered in the Sikela, Shecha, Yetnebersh, Limat, and Konso Sefer vending sites. Of which, 77 (23.3%) of the collected street foods were vended on tables without cover, and 52.1% of foods were vended near waste drainage (within 1–2 meters). In the display case, we observed that 56.1% of foods were directly exposed to dust and sunlight. Likewise, 56.1% of foods were transported from place to place in an unsafe way, mainly from the market and bus station vending areas (Table 3).
 |
Table 3 Hygienic Safety of Commonly Vended Street Foods from Selected Vending Sites in Arba Minch Town, Southern Ethiopia, 2022 |
Bacteriological Quality of Street-Vended Foods
A total of 330 samples of street food were tested for bacterial contamination, and the study found that 99 (30%), 123 (37.3%) and 113 (34.2%) of the food samples had satisfactory (<103 CFU/g), acceptable (≥103, <105 CFU/g) and unsatisfactory (>105 CFU/g) total mean aerobic bacterial contamination, respectively. Of which, about 25.7% (29/113) and 21.2% (24/113) of “Ambasha” and “Sambusa” street food items were found to have unsatisfactory total aerobic bacterial load, respectively, while only 5.5% (18/113) of “Potato Chips” samples had unsatisfactory bacterial contamination (Figure 2).
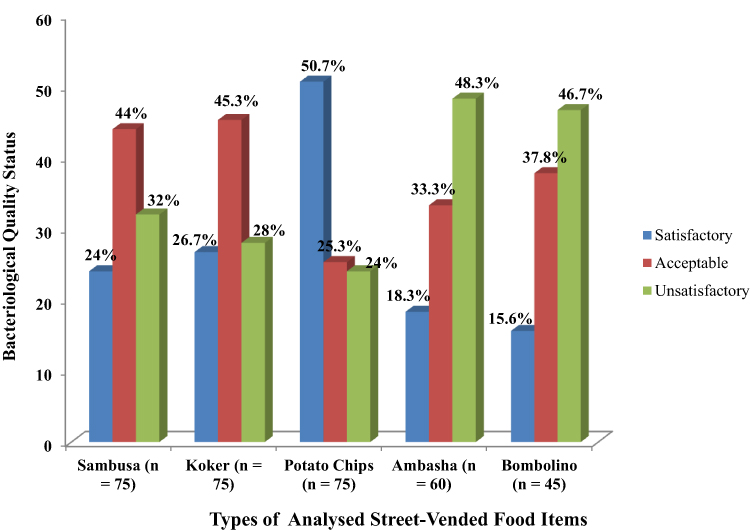 |
Figure 2 Bacteriological quality classification of street-vended foods (n = 330) by total aerobic bacterial count from selected vending sites in Arba Minch Town, Southern Ethiopia, 2022. |
Among commonly vended street food samples with unsatisfactory bacterial contamination, the overall mean total aerobic bacterial count was recorded to be 4.3 × 105 CFU/g, ranging from 3.1 × 105 to 6.2 × 105 CFU/g. The highest average aerobic bacterial counts were registered from Ambasha (6.2 × 105 CFU/g), followed by Koker (4.1 × 105 CFU/g), and Sambusa (3.8 × 105 CFU/g), while the smallest average aerobic bacterial count was obtained from potato chips with 3.1 × 105 CFU/g. In addition, the total mean Enterobacteriaceae count was 1.4 × 105 CFU/g, and the value ranged from 2.1 × 104 to 3.4 × 105 CFU/g. Likewise, the mean coliform count was 2.4 × 104 CFU/g, in which the value ranged from 1.6 × 103 to 4.8 × 104 CFU/g, and the total mean staphylococcal count was 3.4 × 104 CFU/g, which varied from 4.3 × 103 to 5.2 × 104 CFU/g (Table 4).
 |
Table 4 Mean Total Aerobic Bacterial, Enterobacteriaceae, Coliform, and Staphylococcal Counts Among Commonly Vended Street Foods at Selected Vending Sites in Arba Minch Town, Southern Ethiopia, 2022 |
Regarding the vending sites, the highest mean of aerobic bacterial count (2.5 × 106 CFU/g) and Enterobacteriaceae count (4.4 × 105 CFU/g) from street vending food was recorded from samples collected from “Sikela” followed by food samples from “Shecha” with 2.3 × 106 CFU/g, and “Konso Sefer” with 2.3 × 106 CFU/g. The mean coliform count was high among street food samples from “Shecha” with 2.3 × 104 CFU/g, while the highest staphylococcal count was identified from street foods collected from ‘Konso Sefer’ (Table 4).
Factors Associated with Unsatisfactory Bacteriological Quality
Bivariate and multivariate logistic regression analyses were conducted to determine factors associated with the unsatisfactory bacteriological quality of commonly vending street foods. Thus, by using a p-value less than or equal to 0.25 in bivariate analysis as a cutoff point, multivariate logistic regression analysis using conditional backward methods revealed that vending style [AOR = 1.82, 95% CI: (1.12–2.94)], proximity of vending areas to waste drainage [AOR = 2.04, 95% CI: (1.25–3.29)], exposure of street foods to dust, sunlight, and winds [AOR = 4.99, 95% CI: (3.05–8.16)], and inappropriate way of street food transportation [AOR = 2.35, 95% CI: (1.38–3.98)] were found to be statistically significant to the unsatisfactory bacteriological quality of street-vended foods (Table 5).
 |
Table 5 Factors Associated with Unsatisfactory Bacteriological Quality of Commonly Vended Street Foods from Selected Vending Sites in Arba Minch Town, Southern Ethiopia, 2022 |
Distribution of Predominant Bacterial Isolates from Street-Vended Foods
Among the 113 street food samples with an unsatisfactory bacterial contamination limit (>105 CFU/g), 137 bacteria were predominantly isolated and grouped under eight distinct genera. Twenty-four double bacterial contamination were registered in samples from 7, 6, 5, 4, and 2 of “Ambasha”, “Sambusa”, “Koker”, “Bombolino”, and “Potato Chips”, respectively. Gram-negative bacteria were the dominant contaminants, constituting 77.4% of predominant isolates. E. coli was the most common isolate, accounting for 42 (30.7%), followed by S. aureus 31 (22.6%), and Citrobacter spp. 21 (15.3%). 4.4% (6/137) of Salmonella spp. were isolated, while Shigella spp. was not detected (Table 6).
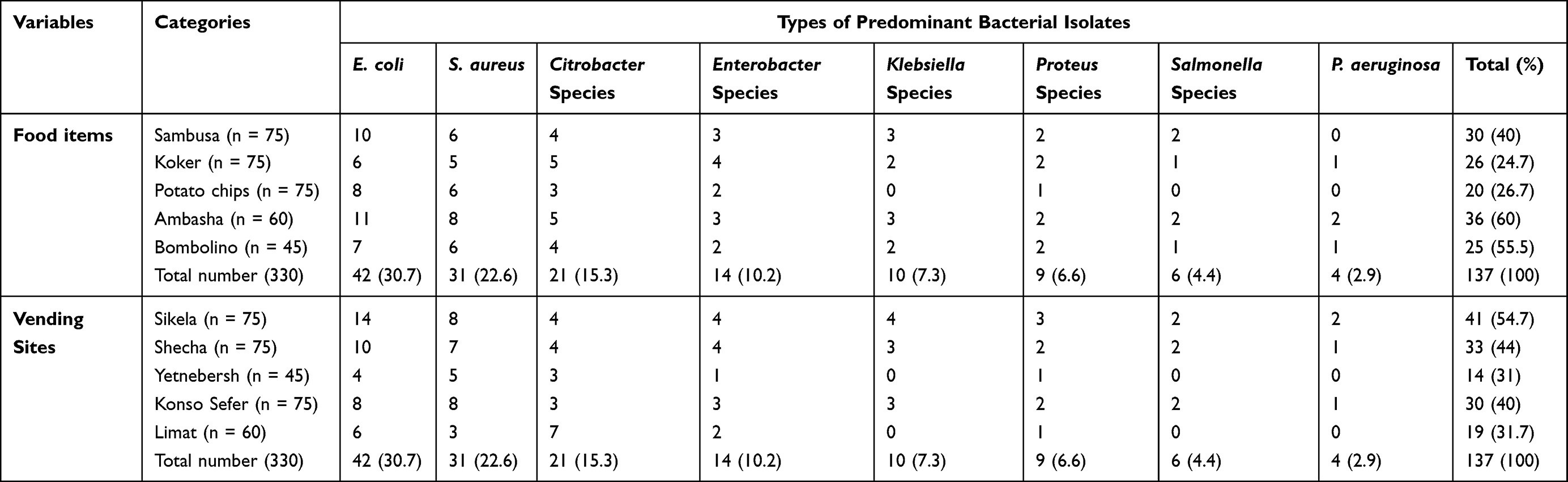 |
Table 6 Distribution of Predominant Bacterial Isolates (n = 137) from Commonly Vended Street Foods at Selected Vending Sites in Arba Minch Town, Southern Ethiopia, 2022 |
Prevalence of Foodborne Pathogenic Bacterial Isolates
From a total of 330 common street food samples tested, 42 (12.7%) foodborne pathogens were recovered. The isolated foodborne pathogens were 31 (9.4%) S. aureus, 6 (1.8%) Salmonella spp., and 5 (1.5%) E. coli O157:H7 (Sorbitol MacConkey non-fermenter among a total of 42 E. coli isolates). E. coli O157:H7 was isolated from “Sambusa” (n = 2), “Ambasha” (n = 2), and “Potato Chips” (n = 1). The maximum number of S. aureus was isolated from street foods from “Sikela” and “Konso Sefer” vending sites. Likewise, Salmonella spp. were isolated from street foods from ‘Sikela,’ ‘Shecha,’ and ‘Konso Sefer’ vending sites with equal distribution (n = 2) (Table 6).
Antimicrobial Susceptibility Profiles of the Isolated S. aureus
Out of the 31 isolates of S. aureus tested, relatively higher resistance was observed to penicillin 17 (54.8%) and tetracycline 16 (51.6%). Moreover, 6.5% (n = 2) of S. aureus isolates were found to be methicillin-resistant S. aureus (MRSA). On the other hand, isolated S. aureus exhibited 80.6%, 70.9%, and 61.3% susceptibility to gentamicin, clindamycin, and ciprofloxacin, respectively. Five S. aureus isolates (16.1%) were found to be multidrug-resistant (MDR) (Table 7).
 |
Table 7 Antimicrobial Susceptibility Patterns of S. aureus Isolated from Commonly Vended Street Foods at Selected Vending Sites in Arba Minch Town, Southern Ethiopia, 2022 |
Antimicrobial Susceptibility Profiles of Isolated Salmonella Spp. and E. coli O157:H7
Four of the six identified Salmonella spp. were ampicillin and tetracycline-resistant. Furthermore, three Salmonella spp. isolates were azithromycin resistant. Amoxicillin-clavulanate and meropenem were relatively efficient against five isolated Salmonella spp. Similarly, four identified sorbitol non-fermenter E. coli (E. coli O157:H7) strains were found to be ampicillin-resistant. Meropenem, on the other hand, was effective against four isolates of E. coli O157:H7. MDR was determined among two of each Salmonella spp. and E. coli O157:H7 isolate (Table 8).
 |
Table 8 Antimicrobial Resistance Profiles of Salmonella Spp. and E. coli O157:H7 Isolates from Commonly Vended Street Foods at Selected Vending Sites in Arba Minch Town, 2022 |
Discussion
In this study, 34.2% (113/330) with a 95% CI of 29.1–39.4 of frequently vended and highly consumed street food samples were found to be unsatisfactory due to being contaminated with indicator organisms and/or foodborne pathogens, which were comparable with a previous study done in Hawassa, Ethiopia (31%).7 However, the result of this study was lower than studies conducted in different parts of Ethiopia: Gonder (ranges from 61.1% to 82.8%),6,21 Addis Ababa (70%),38 and Jigjiga (72%).9 In contrast, the finding of this study was higher than the report from the study in Bangladesh (12%).24 The kinds of street food involved, their compositions, bacteriological quality label interpretation difference and vendor personal hygiene and serving practices as well as the diversity of the environments and climatic circumstances could all contribute to the disparities in the setting.
The overall mean total aerobic bacterial count was recorded to be 4.3 × 105 CFU/g, ranging from 3.1 × 105 to 6.2 × 105 CFU/g, which was in line with the reports obtained from Gonder, 1.10 × 105 to 3.61 × 105 CFU/g,21 and Kumasi, Ghana (5.9 × 105 CFU/g).39 On the other hand, the findings of this study were lower than the studies conducted in Hawassa (1.7 × 105 to 6.7 × 106 CFU/g),7 Jigjiga (1.9–4.6 × 106 CFU/g),9 and Tirumala, India (12.16–25.81 × 105 CFU/g).40 In contrast, this finding was higher than reports from Gondar (6.64 × 104 CFU/g)6 and Lagos, Nigeria, which ranged from 2.98 × 103 CFU/g to 4.09 × 104 CFU/g.28 These differences are primarily brought on by variations in food type and ingredients, preparation techniques, personal hygiene, vendor management, and serving practices, as well as a variety of environments and climatic conditions, which are favorable for bacterial proliferation.
“Ambasha” (6.2 × 105 CFU/g), “Koker” (4.1 × 105 CFU/g), and “Sambusa” (3.8 × 105 CFU/g) account for the maximum range of unsatisfactory high mean aerobic bacterial counts. This might be because “Ambasha” has a higher water activity, which may favor bacterial proliferation, and “Sambusa” has some internal ingredients that serve as excellent media for bacterial multiplication after being contaminated at room temperature, whereas “Koker” was mostly vended by ambulant vendors and handled excessively during transport, storage, and sale. In contrast, “Potato Chips” were the least contaminated among the foods tested. This could be due to the low moisture content and the manner in which these foods are handled and displayed. Unlike other street food items, we noticed that these “Potato Chips” were displayed by being covered with paper sheets.7,9,21,38
In this study, the mean total coliform count was 2.4 × 104 CFU/g, which ranged from 1.6 × 103 to 4.8 × 104 CFU/g, which is to some extent comparable with 2.6 × 103 to 1.9 × 105 CFU/g documented in Addis Ababa,38 8.3 × 104 CFU/g documented in Jigjiga,9 and 2.6 × 103 to 5.2 × 104 CFU/g reported in Hawassa.7 In contrast, our finding is much higher than the 3 × 102 to 6.4 × 103 CFU/g and 0.3–6.4 × 103 CFU/g reported in Gondar6,21 and the 2.8 × 102 to 3.99 × 103 CFU/g in Tirumala, India.40 Whereas the mean total Enterobacteriaceae count of 1.4 × 105 CFU/g recovered in this study, ranging from 2.1 × 104 to 3.4 × 105 CFU/g, which was higher than the 5.55 × 104 reports from Gonder, Ethiopia,6 from Hawassa, Ethiopia, 8.2 × 103 to 6.8 × 104 CFU/g,7 the 104–105 CFU/g reports from Sikkim, India,41 the 1.0 to 4.7 × 104 CFU/g reports made in Ghana,39 and the 6 × 10 to 8 × 102 CFU/g reports made in Egypt.42 Similarly, the mean staphylococcal count was 3.4 × 104 CFU/g, which was consistent with results ranging from 1.4 to 2.9 × 104 CFU/g documented in Jigjiga.9 The high coliform, Enterobacteriaceae, and staphylococcal counts observed in this study could be attributed to post-processing contamination as well as poor hygienic conditions among vendors and their vending environments.
In contrast to findings from studies in Jimma and Jigjiga, Ethiopia,9,10 in this study, E. coli was the most predominant isolate, constituting 42 (30.7%), followed by S. aureus 31 (22.6%), and Citrobacter spp. 21 (15.3%), which suggests that the hands of people who handle food serve as the primary means of transferring bacteria from feces, noses, and skin to food. Additionally, some foods are kept in their original cooking pans until they are sold or reheated, which can lead to a prolonged holding period and favor the development of E. coli and S. aureus.6,7,21
In this study, 42 (12.7%) with a 95% CI of 9.4–16.4 of foodborne pathogens (S. aureus, 31 (9.4%), Salmonella spp., 6 (1.8%), and E. coli O157:H7, 5 (1.5%)) were recovered, which was in line with reports from the study in Bangladesh (12%).24 On the other hand, the overall number of isolated foodborne pathogens in this study was lower than previous studies conducted in different parts of Ethiopia.6,9,21 Unlike a study done in Addis Ababa, Ethiopia,38 but consistent with previous studies, no Shigella spp. were encountered.6,9,21 These foodborne pathogens could have been contaminated by vendors while being prepared or handled, or they could have come from contaminated water used to cleanse hands and utensils. The contamination of street foods with S. aureus stored at ambient temperature, could lead to food poisoning. Similarly, the presence of E. coli O157:H7 in ready-to-eat street foods could attribute to severe gastroenteritis and further complications; however, the prevalence discovered in this study (1.5%) was much lower than previous studies.6,7,43 On the other hand, the prevalence of Salmonella spp. (1.8%) in this study was higher than the zero report in the study conducted in Gonder.6,21 In contrast, the finding is much lower than reports from studies in Jigjiga (19.7%),9 Hawassa (12.7%),7 Jimma town (13.13%),10 and Bahir Dar (57.5%).29 The isolation of this organism from ready-to-eat street food is suggestive of poor hand hygiene and handling practices. Therefore, proper sanitary measures need to be taken when serving ready-to-eat street foods.
Additionally, the ongoing emergence and re-emergence of antibiotic-resistant foodborne bacterial pathogens necessitates concerted efforts.6,7,10,38 This study revealed that among the 31 isolates of S. aureus tested, relatively higher resistance was observed to penicillin 17 (54.8%) and tetracycline 16 (51.6%). On the other hand, isolated S. aureus exhibited 80.6%, 70.9%, and 61.3% susceptibility to gentamicin, clindamycin, and ciprofloxacin, respectively. The finding is comparable with previous studies done in different parts of Ethiopia.6,7,10 6.5% of S. aureus isolates were found to be MRSA, which is lower than the studies conducted in Benin (15.18%)44 and Hawassa (28.6%).7 Likewise, 16.1% of isolated S. aureus were found to be MDR; this finding is below the reports from the study done in Jimma Town, south-western Ethiopia (38.3%).10 66.7% (4/6) of isolated Salmonella spp. were resistant to ampicillin and tetracycline; however, amoxicillin-clavulanate and meropenem were effective for 83.3% (5/6) of isolated Salmonella spp. MDR Salmonella spp. was discovered in 33.3% (2/6) of isolates, which is greater than the values reported in Jimma, Ethiopia (14.29%).10 Eighty percent (4/5) of isolated E. coli O157:H7 strains were found to be ampicillin-resistant; however, more than 60% (3/5) responded better to amoxicillin-clavulanate, gentamicin, and meropenem. The proportion of MDR E. coli O157:H7 isolates was found to be 40% (2/5). The finding is in agreement with study findings in different parts of Ethiopia,6,7,10 and Dhaka, Bangladesh.45 The possible justification for the difference and increased prevalence of antibiotic-resistant foodborne pathogens could be the extensive spread of antimicrobial-resistant bacterial strains in the community, the source of contamination, vendor health status, community awareness towards the use of antimicrobials, and the easy availability of drugs without a prescription.
In terms of vendor profiles, the majority (64%) of vendors were female. The finding is in line with other studies carried out in Ethiopia and elsewhere, including Gondar, Addis Ababa, Jigjiga, and Jimma.6,9,10,38 The majority (40%) of the food vendors had no information on foodborne diseases, in line with a previous study conducted in Gondar, where 42.5% to 58.3% of the food vendors had knowledge of foodborne diseases.6,21 From the present study, it has been found that 29.3% of the food vendors served foods with bare hands, which is actually lower than reported in studies conducted in Gonder (45.8%) and Jigjiga (47.62%).6,9 The majority (73.3%) of the food vendors had no training in food safety, which is similar to a study in Gonder, Ethiopia (79.2%).6
In the current study, street-vended foods with unsatisfactory (>105 CFU/g) bacterial quality were statistically associated with ambulant vending styles, which were found to be 1.82 times more likely to be contaminated than foods sold among stationary vendors [AOR = 1.82, 95% CI: 1.12–2.94], whereas street foods sold near waste drainage were 2.04 times more likely to be contaminated with indicator and/or foodborne pathogens [AOR = 2.04, 95% CI: 1.25–3.29]. Likewise, street foods exposed to direct dust particles and sunlight due to the absence of shelter from vending areas are found to be 4.99 times more likely to be contaminated with unsatisfactory loads of bacteria [AOR = 4.99, 95% CI: 3.05–8.16]. Similarly, street foods transported by vendors in an inappropriate way (without cover, leaving them exposed to different insects and dust particles) were more than twice as likely to be contaminated by bacteria in unsatisfactory loads [AOR = 2.35, 95% CI: 1.38–3.98]. Overall, these findings were consistent with reports from different studies conducted in Ethiopia.6,9,22,46 Unsanitary surroundings, as well as poor personal hygiene of vendors due to a lack of training on proper handling and processing, are potential sources of post-processing contamination of ready-to-eat foods.7,21,22
Limitation of the Study
The range of foodborne bacterial pathogens investigated was constrained because the current research did not address pathogens like Campylobacter spp. and Bacillus cereus that have particular isolation requirements. Due to financial and material constraints, only Sorbitol MacConkey agar medium was utilised for the isolation of E. coli O157:H7 strain isolates and the antimicrobial susceptibility pattern was done only for S. aureus, Salmonella spp., and E. coli O157:H7 isolates. Similarly, the minimum inhibitory concentration (MIC) required for vancomycin susceptibility testing for S. aureus was carried out.
Conclusion and Recommendation
In this study, a significant number (113, 34.2%) of the street-vended foods were found to have a total mean aerobic bacteriological quality that was unsatisfactory (>105 CFU/g; 4.3 × 105 CFU/g). The total mean of Enterobacteriaceae, coliform, and staphylococcal counts were 1.4 × 105 CFU/g, 2.4 × 104 CFU/g, and 3.4 × 104 CFU/g, respectively. S. aureus (31, 9.4%), Salmonella spp. (6, 1.8%), and E. coli O157:H7 (5, 1.5%) were identified and made up 12.7% of foodborne bacterial pathogen prevalence. Higher resistance was observed to penicillin (54.8%) and tetracycline (51.6%) among isolated S. aureus. 6.5% and 16.1% of S. aureus isolates were found to be MRSA and MDR, respectively. Likewise, MDR Salmonella spp. and E. coli O157:H7 isolates were determined to be 33.3% (n = 2) and 40% (n = 2), respectively. Ambulant vending style, proximity of vending areas to waste drainage, exposure of street foods to dust, sunlight, and winds, and an inappropriate way of street food transportation were found to be statistically significant for the unsatisfactory bacteriological quality of street-vended foods. As a result, comprehensive health education and training for street food vendors, regular inspections of vending area environmental sanitation, and regular antibiotic resistance testing for foodborne bacteria are required. The study, on the other hand, provides helpful baseline data for public health specialists in the management of human infections caused by foodborne disease in the surveyed area. However, more research into the molecular characterization of foodborne bacterial pathogens is required.
Abbreviation
ATCC, American Type Culture Collection; BPW, Buffered Peptone Water; CLSI, Clinical and Laboratory Standards Institute; CFU, Colony Forming Unit.
Data Sharing Statement
The datasets generated during the current study are available from the corresponding author on reasonable request under the Ethics Committee’s approval.
Acknowledgments
We acknowledge the technical and financial support provided by the Arba Minch University Research Directorate. Our gratitude also goes out to the food vendors at a selected vending area in Arba Minch town for agreeing to take part in the research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The project was funded by the Arba Minch University Research Directorate.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. ImathIu S. Street vended foods: potential for improving food and nutrition security or a risk factor for foodborne diseases in developing countries? Curr Nutr Food Sci. 2017;5(2):55–65. doi:10.12944/CRNFSJ.5.2.02
2. Centre for Food Safety. Microbiological guidelines for food (for ready-to-eat food in general and specific food items). Hong Kong: Food and Environmental Hygiene Department. 2014. Accessible from: https://www.cfs.gov.hk/english/food_leg/files/food_leg_Microbiological_Guidelines_for_Food_e.pdf.
3. Teferi SC. Street food safety, types and microbiological quality in Ethiopia: a critical review. Am J Appl Sci. 2020;6(3):67–71. doi:10.11648/j.ajasr.20200603.12
4. Barcelon EG, Collado DMR, Eustaquio SA, et al. Consumer perception and microbiological analysis on safety of street food dipping sauces. Asian J Agric Food Sci. 2015;3(1):1.
5. Tabashsum Z, Khalil I, Nazimuddin M, Mollah A, Inatsu Y, Bari ML. Prevalence of foodborne pathogens and spoilage microorganisms and their drug resistant status in different street foods of Dhaka city. Agric Food Anal Bacteriol J. 2013;3(4):281–292.
6. Amare A, Worku T, Ashagirie B, Adugna M, Getaneh A, Dagnew M. Bacteriological profile, antimicrobial susceptibility patterns of the isolates among street vended foods and hygienic practice of vendors in Gondar town, Northwest Ethiopia: a cross sectional study. BMC Microbiol. 2019;19(1):120. doi:10.1186/s12866-019-1509-4
7. Eromo T, Tassew H, Daka D, Kibru G. Bacteriological quality of street foods and antimicrobial resistance of isolates in Hawassa, Ethiopia. Ethiop J Health Sci. 2016;26(6):533–542. doi:10.4314/ejhs.v26i6.5
8. Canini ND, Bala JJO, Maraginot EN, Mediana BCB. Evaluation of street food vending in Ozamiz City. J Multidiscip Stud. 2013;1(1). doi:10.7828/jmds.v1i1.391
9. Bereda TW, Emerie YM, Reta MA, Asfaw HS. Microbiological safety of street vended foods in Jigjiga City, Eastern Ethiopia. Ethiop J Health Sci. 2016;26(2):163–172. doi:10.4314/ejhs.v26i2.10
10. Nemo R, Bacha K, Ketema T. Microbiological quality and safety of some-street-vended foods in Jimma Town, southwestern Ethiopia. Afr J Microbiol Res. 2017;11(14):574–585. doi:10.5897/AJMR2014.7326
11. Lee H, Yoon Y. Etiological agents implicated in foodborne illness world wide. Food Sci Anim Resour. 2021;41(1):1. doi:10.5851/kosfa.2020.e75
12. Bizuye A, Tewelde S, Agimas A, Asfaw M, Tadele E, Mesfin E. Bacteriological quality of street vending potato chips in Gondar Town, North West Ethiopia. Int J Bacteriol Virol Immunol. 2014;1(2):14.
13. Alemu G, Mama M, Siraj M. Bacterial contamination of vegetables sold in Arba Minch Town, Southern Ethiopia. BMC Res Notes. 2018;11(1):775. doi:10.1186/s13104-018-3889-1
14. Buted DR, Ylagan A. Street food preparation practices. Asia Pac J Educ Arts Sci. 2014;1(2):53–60.
15. Birgen BJ, Njue LG, Kaindi DM, Ogutu FO, Owade JO. Determinants of microbial contamination of street-vended chicken products sold in Nairobi County, Kenya. Int J Food Sci. 2020;2020:1–8. doi:10.1155/2020/2746492
16. World Health Organization. WHO Estimates of the Global Burden of Foodborne Diseases: Executive Summary. World Health Organization; 2015.
17. Salamandane A, Silva AC, Brito L, Malfeito-Ferreira M. Microbiological assessment of street foods at the point of sale in Maputo (Mozambique). Food Qual Saf. 2021;5. doi:10.1093/fqsafe/fyaa030
18. World Health Organization. WHO Estimates of the Global Burden of Foodborne Diseases: Foodborne Disease Burden Epidemiology Reference Group 2007–2015. World Health Organization; 2015.
19. Scott E. Food safety and foodborne disease in the 21st century. Can J Infect Dis. 2003;14:277–280. doi:10.1155/2003/363984
20. Kirk M, Ford L, Glass K, Hall G. Foodborne illness, Australia, circa 2000 and circa 2010. Emerg Infect Dis. 2014;20(11):1857. doi:10.3201/eid2011.131315
21. Derbew G, Sahle S, Endris M. Bacteriological assessment of some street vended foods in Gondar, Ethiopia. Int J Food Saf. 2013;15(6):33–38.
22. Adane M, Teka B, Gismu Y, Halefom G, Ademe M. Food hygiene and safety measures among food handlers in street food shops and food establishments of Dessie town, Ethiopia: a community-based cross-sectional study. PLoS One. 2018;13(5):e0196919. doi:10.1371/journal.pone.0196919
23. Omemu A, Aderoju S. Food safety knowledge and practices of street food vendors in the city of Abeokuta, Nigeria. Food Control. 2008;19(4):396–402. doi:10.1016/j.foodcont.2007.04.021
24. Islam S, Nasrin N, Rizwan F, et al. Microbial contamination of street vended foods from a university campus in Bangladesh. Southeast Asian J Trop Med Public Health. 2015;46(3):480–485.
25. Ma L, Chen H, Yan H, Wu L, Zhang W. Food safety knowledge, attitudes, and behavior of street food vendors and consumers in Handan, a third tier city in China. BMC Public Health. 2019;19(1):1128. doi:10.1186/s12889-019-7475-9
26. Odeyemi OA, Sani NA. Antibiotic resistance and burden of foodborne diseases in developing countries. Future Sci. 2016;2:FSO139. doi:10.4155/fsoa-2016-0023
27. Oladipo I, Adejumobi O. Incidence of antibiotic resistance in some bacterial pathogens from street vended food in Ogbomoso, Nigeria. Pak J Nutr. 2010;9(11):1061–1068. doi:10.3923/pjn.2010.1061.1068
28. Akinyemi K, Fashola M, Habib N, Akinwande E. Vended foods In Lagos, Nigeria: a potential reservoir for the spread of emerging strains of drug resistant bacteria. Health. 2013;5(4):675–680. doi:10.4236/health.2013.54089
29. Kibret M, Tadesse M. The bacteriological safety and antimicrobial susceptibility of bacteria isolated from street-vended White lupin (Lupinus albus) in Bahir Dar, Ethiopia. Ethiop J Educ Sci. 2013;23(1):19–26.
30. Kiiyuki C. Laboratory manual of food microbiology for Ethiopian Health and Nutrition Research Institute (Food Microbiology Laboratory). Unido Project; 2003:28–33.
31. Authority NF. Microbiological quality guide for ready-to-eat foods: a guide to interpreting microbiological results. NSW/FA/CP028/0906; 2009:1–9.
32. Bergey S. Manual of systematic bacteriology; 2010. Accessible from: https://link.springer.com/chapter/10.1007/978-0-387-21609-6_13.
33. Cheesbrough M. District Laboratory Practice in Tropical Countries, Part 2. Cambridge university press; 2006. Accessible from: https://www.medbox.org/preview/5255d6e1-05d4-41a9-beb2-02b60e695ecc/doc.pdf.
34. Manafi M, Kremsmaier B. Comparative evaluation of different chromogenic/fluorogenic media for detecting Escherichia coli O157: H7 in food. Int J Food Microbiol. 2001;71(2–3):257–262. doi:10.1016/S0168-1605(01)00610-9
35. Islam MZ, Christensen JP, Biswas PK. Sorbitol non-fermenting shiga toxin-producing Escherichia coli in cattle on smallholdings. Epidemiol Infect. 2015;143(1):94–103. doi:10.1017/S0950268814000351
36. Kirby B. Kirby-Bauer disk diffusion susceptibility test protocol. Am Soc Microbiol. 2009;66:208.
37. Wayne PA; CLSI. Performance Standards for Antimicrobial Susceptibility Testing CLSI Supplements M100. Clinical and Laboratory Standards Institute; 2020. Accessible from: https://www.nih.org.pk/wp-content/uploads/2021/02/CLSI-2020.pdf.
38. Muleta D, Ashenafi M. Bacteriological profile and holding temperatures of street-vended foods from Addis Ababa. Int J Environ Health Res. 2001;11(1):95–105. doi:10.1080/09603120020019683
39. Mensah P, Yeboah-Manu D, Owusu-Darko K, Ablordey A. Street foods in Accra, Ghana: how safe are they? Bull World Health Organ. 2002;2002:546–554.
40. Suneetha C, Manjula K, Depur B. Quality assessment of street foods In Tirumala. Asian J Exp Biol Sci. 2011;2(2):207–211.
41. Kharel N, Palni U, Tamang JP. Microbiological assessment of ethnic street foods of the Himalayas. J Ethn Foods. 2016;3(3):235–241. doi:10.1016/j.jef.2016.01.001
42. Ismalia SA. Microbiological quality of hawawshy consumed in Ismailia, Egypt. J Food Saf. 2006;26:251–263. doi:10.1111/j.1745-4565.2006.00047.x
43. Hanashiro A, Morita M, Matté GR, Matté MH, Torres EA. Microbiological quality of selected street foods from a restricted area of São Paulo city, Brazil. Food Control. 2005;16(5):439–444. doi:10.1016/j.foodcont.2004.05.004
44. Sina H, Baba-Moussa F, Kayodé A, et al. Characterization of Staphylococcus aureus isolated from street foods: toxin profile and prevalence of antibiotic resistance. J Appl Biosci. 2011;46:3133–3143.
45. Al Mamun M, Rahman SMM, Turin TC. Microbiological quality of selected street food items vended by school-based street food vendors in Dhaka, Bangladesh. Int J Food Microbiol. 2013;166(3):413–418. doi:10.1016/j.ijfoodmicro.2013.08.007
46. Arias Y, Bauchet J, Ricker J, Neuhofer Z Food safety programs and academic evidence in Senegal; 2020. Accessible from: https://ag.purdue.edu/food-safety-innovation-lab/wp-content/uploads/2021/01/FSIL-Food-Safety-Programs-and-Academic-Evidence-in-Senegal.pdf.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.