Back to Journals » Infection and Drug Resistance » Volume 16
Bacterial Species and Inflammatory Cell Variability in Respiratory Tracts of Patients with Chronic Obstructive Pulmonary Disease Exacerbation: A Multicentric Study
Authors Salama KS, Moazen EM ![]() , Elsawy SB
, Elsawy SB ![]() , Kotb SF, Mohammed EM
, Kotb SF, Mohammed EM ![]() , Tahoun SA
, Tahoun SA ![]() , Ramadan MAA, Abd Elhamid SM
, Ramadan MAA, Abd Elhamid SM ![]() , Bahi RHM, Mohammad EA
, Bahi RHM, Mohammad EA
Received 27 December 2022
Accepted for publication 1 April 2023
Published 11 April 2023 Volume 2023:16 Pages 2107—2115
DOI https://doi.org/10.2147/IDR.S402828
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Khadiga SM Salama,1 Eman M Moazen,1 Sawsan B Elsawy,1 Sanaa F Kotb,1 Eid M Mohammed,2 Sara A Tahoun,3 Marwa A A Ramadan,3 Samar M Abd Elhamid,3 Rania H M Bahi,4 Etemad A Mohammad5
1Chest Diseases Department, Faculty of Medicine for Girls, Al-Azhar University, Cairo, Egypt; 2Chest Diseases Department Faculty of Medicine for Men’s, Al-Azhar University, Cairo, Egypt; 3Clinical Pathology Department Faculty of Medicine for Girls, Al-Azhar University, Cairo, Egypt; 4Chest Diseases Department Faculty of Medicine, Zagazig University, Zagazig, Egypt; 5Chest Diseases Department Faculty of Medicine, Benha University, Benha, Egypt
Correspondence: Sawsan B Elsawy, Chest Diseases Department, Faculty of Medicine for Girls, Al-Azhar University, Cairo, Egypt, Email [email protected]
Background and Aim: Acute exacerbation of chronic obstructive pulmonary disease (AECOPD) has profound effects on disease progression and patients’ quality of life. Emerging evidence suggests an association between alterations in the respiratory microbiome flora species and airway inflammation in patients with AECOPD. The present study aimed to describe the inflammatory cells and bacterial microbiome distributions in respiratory tract in Egyptian patients with AECOPD.
Subjects and Methods: The present cross-sectional study included 208 patients with AECOPD. Sputum and broncho-alveolar lavage samples from the studied patients were submitted to microbial cultures using appropriate media. Total and differential leukocytic counts and were done via automated cell counter.
Results: The present study included 208 AECOPD patients. They comprised 167 males (80.3%) and 41 females (19.7%) with an age of 57.9 ± 4.9 years. AECOPD was categorized as mild, moderate and severe in 30.8%, 43.3% and 26%, respectively. Sputum samples had significantly higher TLC, neutrophil percent and eosinophil percent when compared with BAL samples. In contrast, lymphocyte percent was significantly higher in BAL samples. Sputum specimens had significantly lower frequency of positive growths (70.2% versus 86.5%, p = 0.001). Among the identified organisms, sputum specimens had significantly lower frequency of Strept. pneumoniae (14.4% versus 30.3%, p = 0.001), Klebsiella pneumoniae (19.7% versus 31.7%, p = 0.024), Haemophilus influenzae (12.5% versus 26.9%, p = 0.011), Pseudomonas aeruginosa (2.9% versus 10%, p = 0.019) and Acinetobacter spp. (1.9% versus 7.2%, p = 0.012) growths when compared with BAL samples.
Conclusion: The present study could identify a distinctive pattern of inflammatory cell distribution in sputum and BAL samples of AECOPD patients. The most commonly isolated organisms were Klebsiella pneumoniae and Strept. pneumoniae.
Keywords: chronic obstructive pulmonary disease, COPD exacerbation, inflammatory cells, bacterial microbiome, sputum culture, bronchoalveolar culture
Introduction
Chronic obstructive pulmonary disease (COPD) is a major cause of chronic morbidity. It is one of the top three causes of death worldwide and 90% of these deaths occur in low- and middle-income countries.1,2 Airways of almost 50% of stable COPD patients are colonized by potentially pathogenic microorganisms (PPMs). The most commonly isolated microbes are H. influenzae, M. catarrhalis, S. pneumoniae, S. aureus, and P. aeruginosa.3
Acute exacerbation of chronic obstructive pulmonary disease (AECOPD) is an acute and sustained worsening of a patient’s condition from a stable state.4 Possible risk factors include air pollution, seasonal change, ethnic background, associated comorbidities, poor exercise capacity and obesity.5 Management strategy usually includes bronchodilators and corticosteroids as first-line treatments. In patients with severe exacerbations, noninvasive ventilation, magnesium, ketamine, and epinephrine may be considered. Mechanical ventilation may be needed in selected situations.6
AECOPD has profound effects on disease progression and patients’ quality of life. Prevention of early recurrence and identification of causative agents remains one of the top unmet needs in management of AECOPD.7 Remarkably, newly developed vaccines against the most frequent bacteria identified in AECOPD are assessed by undergoing trials.8 Emerging evidence suggests an association between alterations in the respiratory microbial flora species and airway inflammation in patients with AECOPD.9 Identification of respiratory microbiome has been increasingly recognized as a cornerstone in a modern management direction of AECOPD.10,11
Interestingly, it has been shown that clinical features of AECOPD can significantly vary between various populations. This is probably related to genetic and environmental factors. In addition, variations in the distributions of the respiratory microbiota between various populations may be a contributing factor.12 For example, the predominant isolated organism in one South Korean study13 and another Ethiopian one14 was Pseudomonas aeruginosa, while Klebsiella pneumoniae prevailed in an Indian study.15 It was also noted that isolated organisms may vary between upper and lower respiratory tracts in patients with stable COPD and AECOPD.16 In addition, exaggerated inflammatory response in AECOPD patients was related to poor outcome.17 Distribution of inflammatory cells in respiratory tracts of AECOPD patients may be related to disease severity and treatment response.18,19
The present study aimed to describe the isolated bacterial species and inflammatory cell distributions in upper and lower respiratory tracts in Egyptian patients with AECOPD.
Patients and Methods
This cross-sectional study was conducted at chest diseases and clinical pathology departments of Al-Zahraa, Al-Hussein, Zagazig and Benha university hospitals during the period from January 2022 to August 2022. An informed written consent was gotten from every patient before enrollment into the study in accordance with Declaration of Helsinki guidelines. The study was approved by the ethical committee of Al-Azhar University Faculty of Medicine for Girls.
The study included 208 patients with AECOPD. COPD was diagnosed, and its severity was graded according to the modified criteria defined in the Global Initiative for Chronic Obstructive Lung Disease guidelines.20 Clinically, an exacerbation was defined as a worsening of respiratory symptoms that led the patient to contact health-care facilities and assessed using the Anthonisen criteria.21 AECOPD was staged as mild if there was worsening of symptoms that were self-managed (eg increase in salbutamol use) and improved without systemic corticosteroids or antibiotics. Moderate AECOPD was defined if treatment with systemic corticosteroids or antibiotics or both was required. Severe AECOPD was defined if hospitalization was required.22
Spirometry was performed according to the standard recommendations.23 Fixed airways obstruction was diagnosed if there was post-bronchodilator FEV1/FVC <0.7. Patients were excluded if they refused to perform or did not complete fiberoptic bronchoscopy (FOB) or if they had other chest diseases.
Sputum Sampling
Sputum samples were collected in the day of admission and before starting antibiotic or steroid therapy according to Shepherd.24 Samples were placed in a sterile container and delivered immediately to the microbiology laboratory where they were rapidly processed in less than two hours.
Bronchoalveolar Lavage Sampling
Bronchoalveolar lavage (BAL) sampling was performed in the same day of admission before starting antibiotic or steroid therapy after detailed explanation of the technique to the patients. Oxygen was administered by a nasal cannula, and flows were adjusted upward from 2 L/minute to keep oxygen saturation >90%. With the patient placed in a semi-supine position under midazolam (2.5- mg) sedation and topical anesthesia, the fiberoptic bronchoscope (FOB) was introduced through the nose, passed through the vocal cords, and a complete airway inspection was performed. FOB was gently impacted or “wedged” through both middle lobe and lingual bronchi. BAL was obtained by aspiration of any secretion and instillation of 80 mL of sterile isotonic saline solution followed by immediate aspiration by suction into a clean and sterile container (polypropylene). The BAL fluid was transported to the microbiology laboratory immediately and processed in less than two hours.25
Examination of Sputum and BAL Gram-Stained Smear
Before counting the inflammatory cells or culturing sputum sample, a Gram-stained smear was done directly from the specimen to assess the quality of the sample using Bartlett’s grading system (Q score). Sputum samples harboring ≥10 leucocytes with <25 squamous epithelial cells per low-power field (˂10/LPF) were accepted and cultured.26 If the sputum or BAL samples were considered of good quality (lower respiratory tract specimen), examination of the slide under oil immersion (1000X) magnification for bacteria was done and culturing the specimen was performed.
Cultivation, Quantification and Identification of Sputum and BAL Specimens
Sputum and BAL cultures were done on routine media used for the isolation and identification of respiratory pathogens including (blood agar, chocolate agar, and MacConkey agar). Semi-quantitative cultures were done using the calibrated loop method. About 0.1 mL of specimen was plated onto solid media, and CFU were counted. CFU/mL was calculated using the formula: cfu/mL = (no. of colonies × dilution factor)/volume of culture plate.27
Blood agar and chocolate agar plates were incubated in 5–7% CO2, while MacConkey agar plates were incubated in aerobic conditions. All plates were incubated at 36.0 ±1.0 °C for 24 hours.28 To avoid overestimation of airway colonization with bacterial microbiome, specimens with CFU ˂104 /mL were considered colonization and excluded from the study, whereas specimens with CFU ≥104 / mL were considered infection and further processed for the identification of bacteria using biochemical reactions.29 For gram-positive bacteria, catalase, mannitol fermentation, DNAse, and optochin sensitivity tests were used while for gram-negative bacteria, TSI, LIA, MIO, Indole, Citrate utilization, Urease and Oxidase tests were used.
Total Leukocytic and Differential Leukocytic Count in Sputum and BAL
After good processing of sputum and BAL samples, small amounts of liquefied sputum and BAL fluid specimens were centrifuged at an appropriate speed, resuspended, and analyzed for TLC and differential count. TLC and differential count were done via automated cell counter using a hematological analyzer (SysmexXE-21N, Kobe, Japan). The TLC/mL and the percentage of neutrophils, lymphocytes and eosinophils were recorded.
Statistical Analysis
Data were statistically analyzed by the Statistical Package for Social Science (SPSS) program version 17.0 (SPSS Inc., Chicago, USA). The Shapiro–Wilk test was used for testing normality of the studied variables. Descriptive analysis was done for each item, and the results were expressed mean ±SD for parametric data, and as percentages for nominal data. Comparisons to assess the difference between the groups were done using the Chi-square X2 test for qualitative data and by independent t-test for parametric data. A linear correlation coefficient was used for the detection of a correlation between inflammatory cells in sputum and its corresponding one in BAL. Statistical significance was considered at a p value <0.05.
Results
The present study included 208 AECOPD patients. They comprised 167 males (80.3%) and 41 females (19.7%) with an age of 57.9 ± 4.9 years. AECOPD was categorized as mild, moderate and severe in 30.8%, 43.3% and 26%, respectively. Other clinical findings of the studied patients are shown in Table 1. Total and differential leukocytic counts in sputum and BAL are shown in Table 2. Sputum samples had significantly higher TLC (6.5 ± 1.2 versus 5.6 ± 1.5 cells/mL, p = 0.001) neutrophil percent (83.4 ± 7.4 versus 38.1 ± 18.6, p = 0.001) and eosinophil percent (2.8 ± 1.6 versus 0.7 ± 0.7, p = 0.001) when compared with BAL samples. In contrast, lymphocyte percent was significantly higher in BAL samples (2.5 ± 1.2 versus 14.1 ± 6.6, p = 0.001) (Table 2). Correlation analysis identifies significant correlation between TLC and differential count elements in sputum and BAL samples (Table 3).
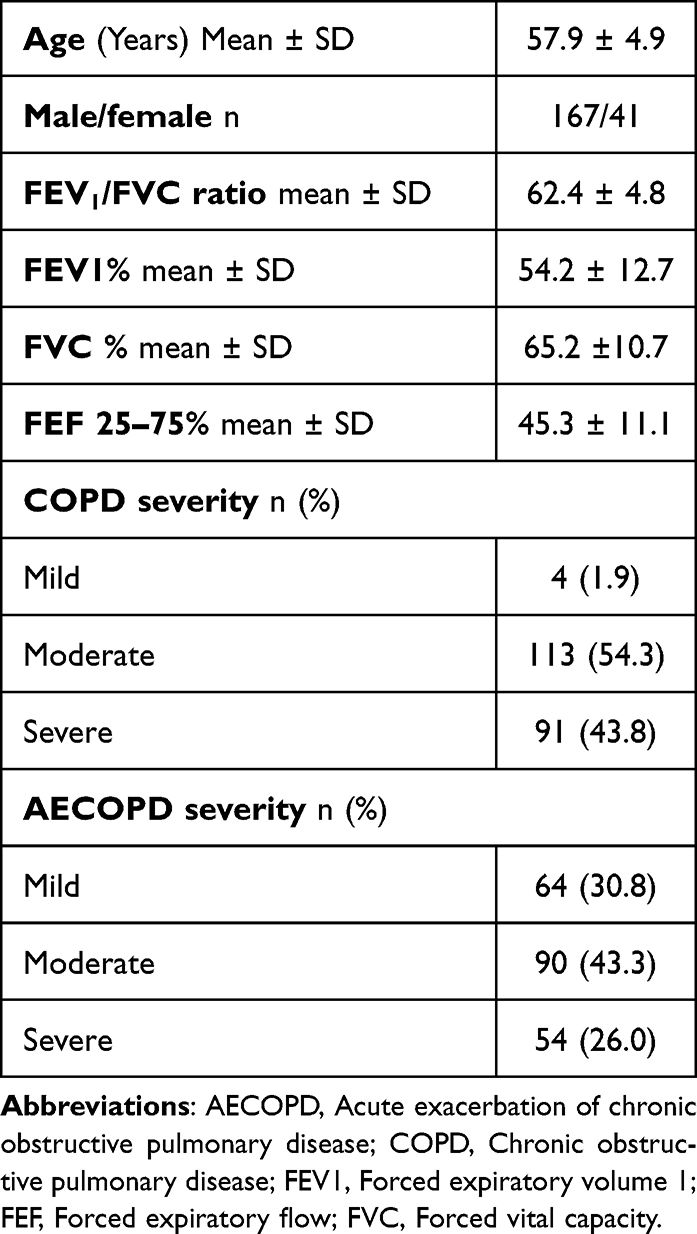 |
Table 1 Characteristics of Studied Patients (n = 208) |
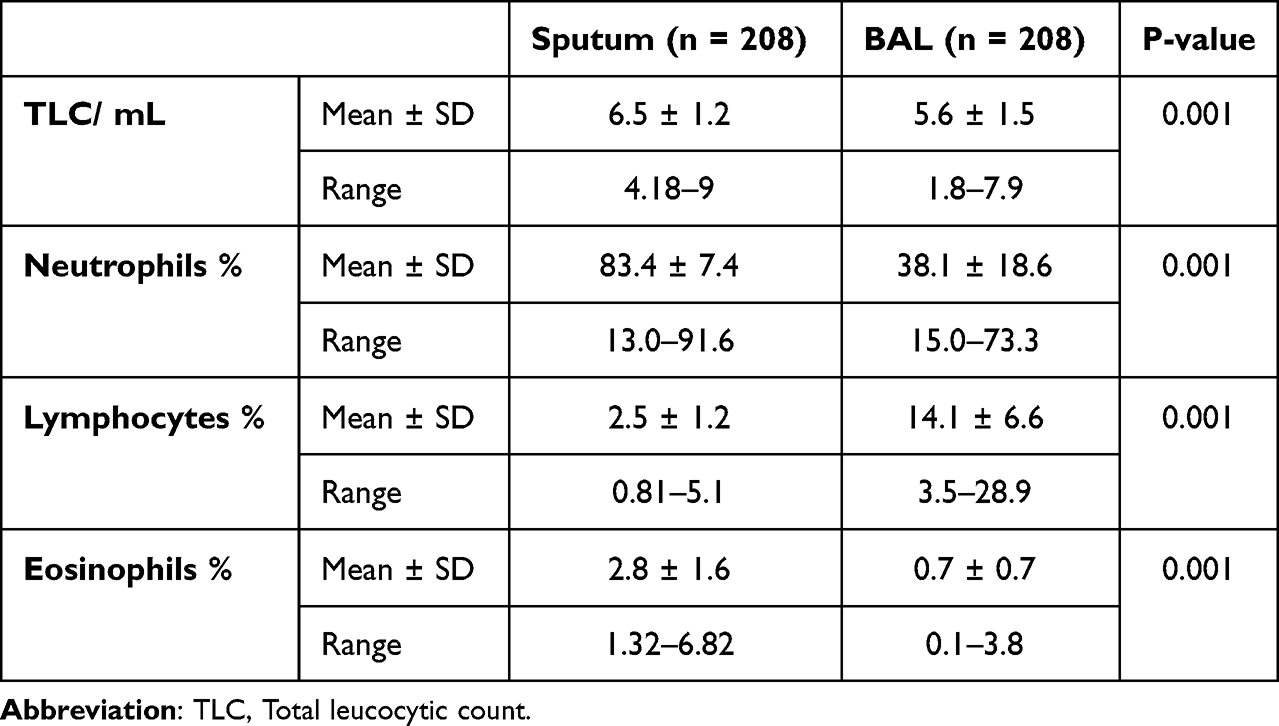 |
Table 2 Comparison of Inflammatory Cells Between Sputum and BAL in Patients with AECOPD |
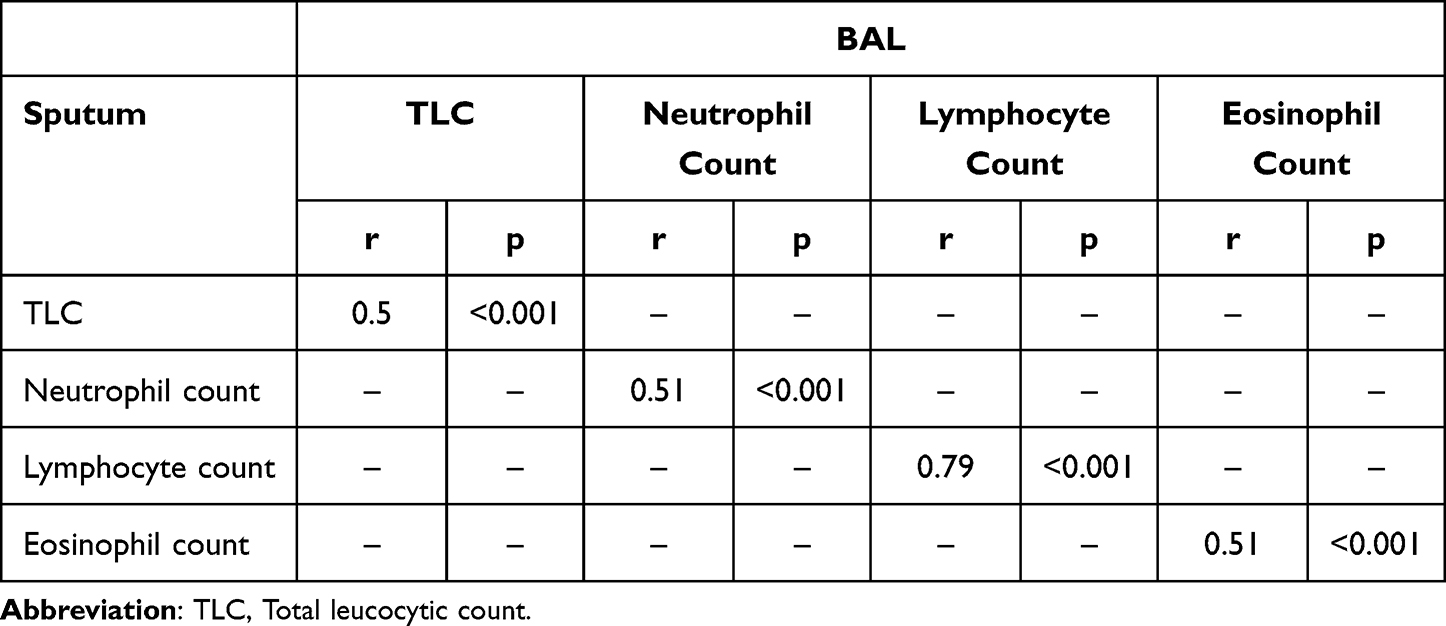 |
Table 3 Correlation Between Sputum and BAL Cellular Findings |
Sputum specimens had significantly higher frequency of positive growths (70.2% versus 86.5%, p = 0.001). Among the identified organisms, sputum specimens had significantly lower frequency of Strept. pneumoniae (14.4% versus 30.3%, p = 0.001), Klebsiella pneumoniae (19.7% versus 31.7%, p = 0.024), Haemophilus influenzae (12.5% versus 26.9%, p = 0.011), Pseudomonas aeruginosa (2.9% versus 10%, p=0.019), and Acinetobacter spp. (1.9% versus 7.2%, p = 0.012) growths when compared with BAL samples (Table 4, Figures 1 and 2).
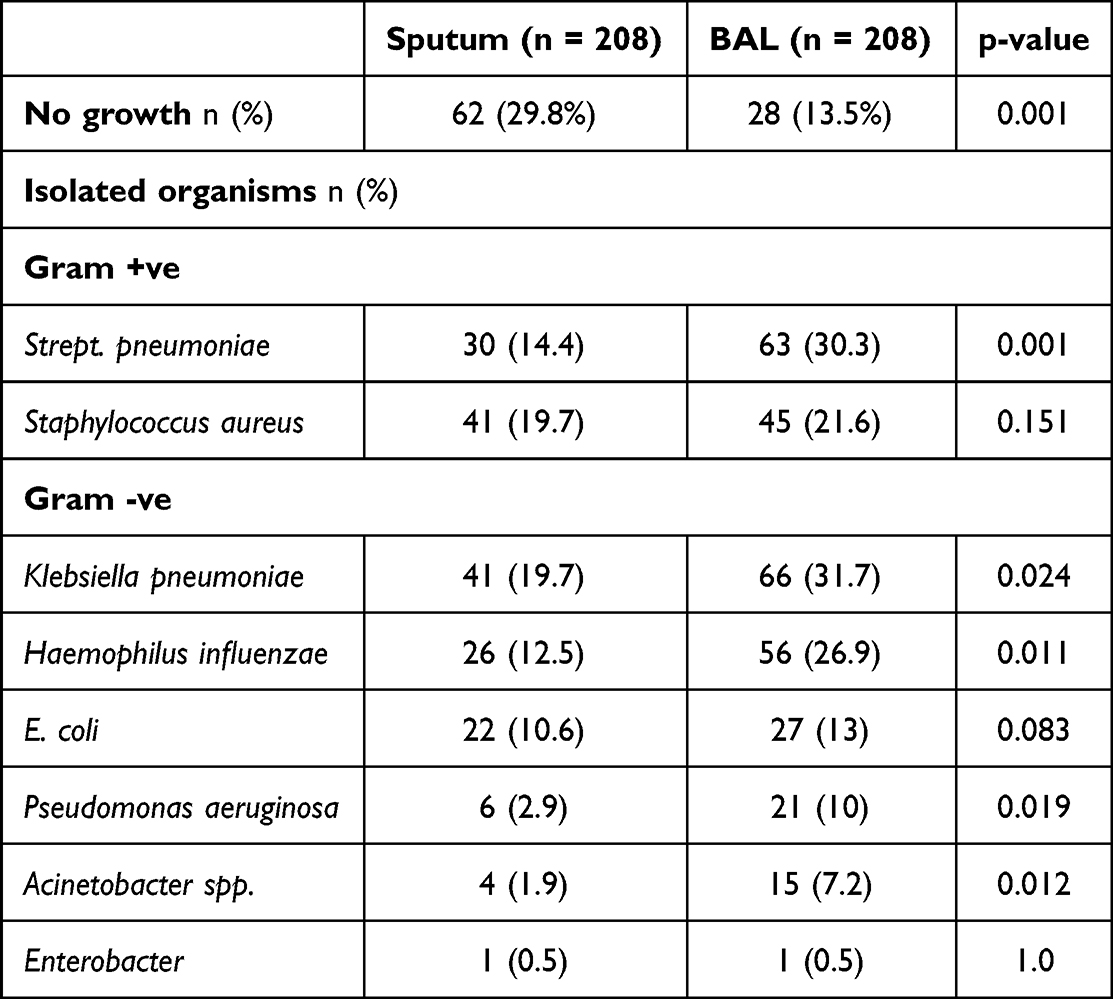 |
Table 4 Comparison of Bacterial Microbiome Between Sputum and BAL in Patients with AECOPD |
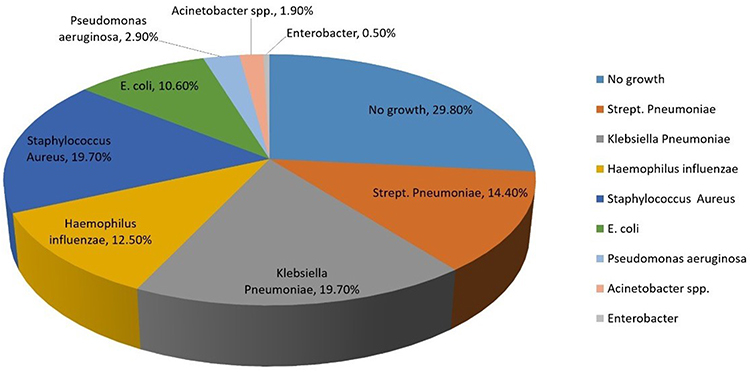 |
Figure 1 Distribution of bacterial organisms in large airways in patients with COPD exacerbation. |
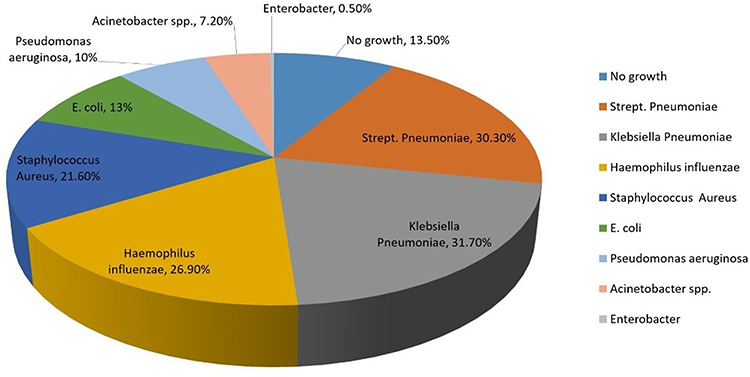 |
Figure 2 Distribution of bacterial organisms in small airways in patients with COPD exacerbation. |
Distribution of bacterial microbiome combinations is shown in Table 5. BAL samples retrieved significantly higher frequency of two (31.5% versus 17.1%) and three (15.5% versus 0.0%) organisms as compared to sputum samples.
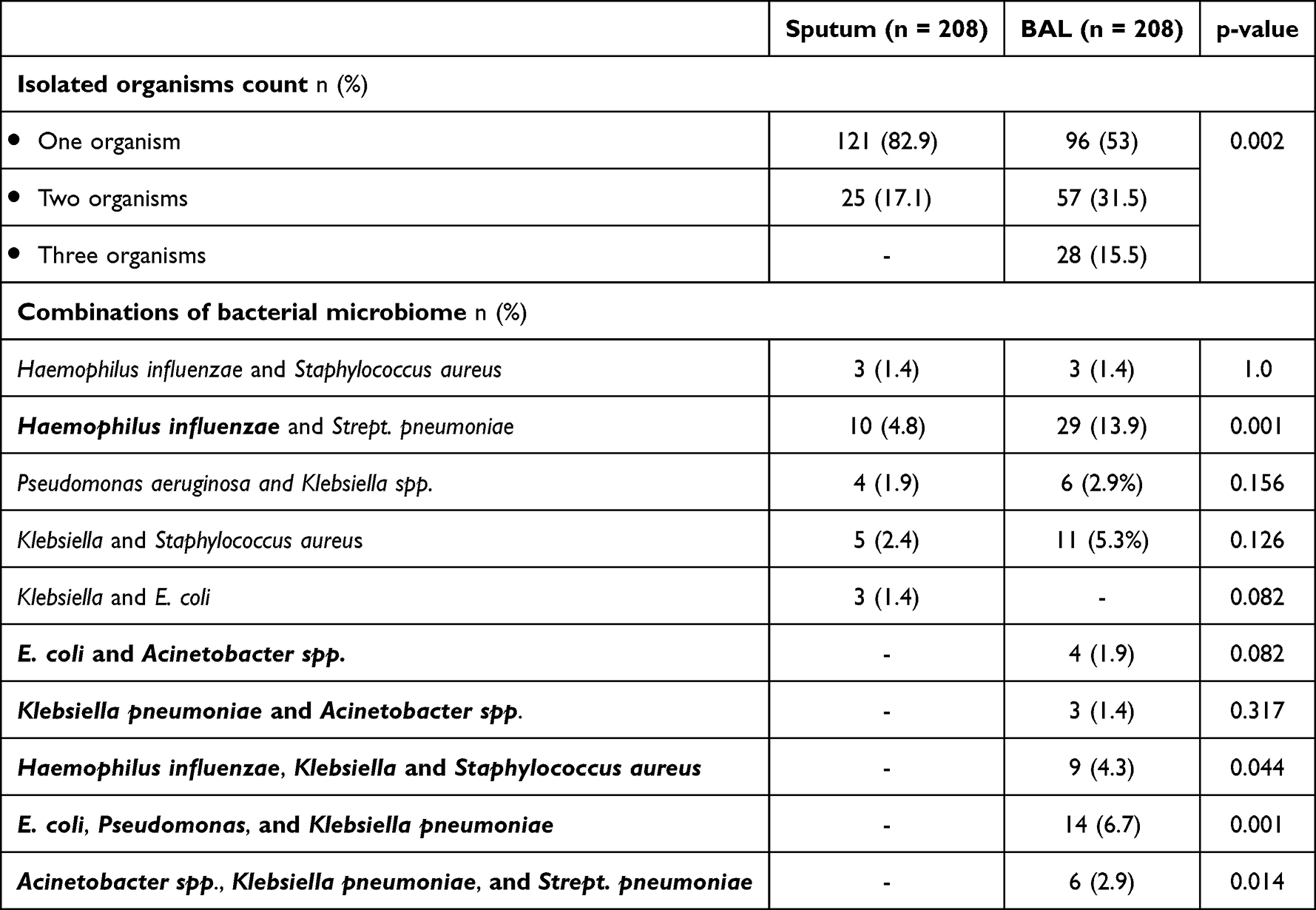 |
Table 5 Distribution of Bacterial Microbiome Combinations in Sputum and BAL in Patients with AECOPD |
Discussion
In the present study, we could identify a distinctive pattern of inflammatory cell distribution in sputum and BAL samples of AECOPD patients. Our findings are in line with Maestrelli et al30 who found that the relative proportion of inflammatory cells was different in sputum, BAL, and bronchial mucosa. Accumulation of neutrophils in the airways is recognized as a prominent feature of COPD, with the extent of neutrophilic infiltration both in the airways and tissues correlating with disease severity.31 The higher neutrophil percentage in sputum may be attributed to the fact that sputum originates from the upper and mid airways that are well known for their neutrophil-rich secretions compared with BAL.32
In current study, we found that only the level of lymphocytes in sputum was significantly lower than in BAL. We speculated that the low level of lymphocytes in the sputum better reflected the immunosuppression of COPD and further information is required to evaluate the correlation between lymphocytes and COPD. In COPD, sputum consists mainly of neutrophils, while it has less macrophage and even less lymphocytes. BAL, on the other hand, consists mainly of macrophages, with less neutrophils and lymphocytes.33
In the present study, there were higher rates of isolation of Klebsiella pneumoniae, Strept. pneumoniae, Haemophilus influenzae, Pseudomonas aeruginosa, and Acinetobacter spp. from BAL than sputum. These findings indicate that in patients with AECOPD, the bronchiolar and alveolar compartments are harboring more bacterial microbiome than large airways.
In comparison, De Serres et al34 found that the most frequently isolated organism from sputum of 108 patients with AECOPD was S. aureus. Sharan35 found that the commonest isolate was Klebsiella pneumoniae followed by Staphylococcus aureus from sputum of 107 patients with AECOPD. Monsó et al36 found that the most prevalent microorganism in sputum of COPD exacerbation patients was H. influenzae followed by M. catarrhalis and S. pneumoniae.
In another study, Streptococcus was the most commonly isolated organism in sputum of 36 Chinese patients with AECOPD.37 Another work from Norway38 found that Streptococcus, Veillonella, Prevotella and Gemella were the most abundant genera in patients with moderate and severe COPD exacerbations, while the study of Goolam Mahomed et al39 identified Haemophilus and Streptococcus as the most common genera.
This disagreement reflects the diverse respiratory microbiome components among different populations with AECOPD which may be attributed to genetic, immunological and environmental factors.
Altered microbial profile in the respiratory tract may predispose to AECOPD through multiple mechanisms. Recently, Zhu et al,40 suggested that changes of microbiota can modify interleukin-17a (IL-17a) expression by downregulating microRNAs (miR-122 and miR-30a) expression. Findings of the present study may have significant therapeutic implications. Prevention of AECOPD by modifying the lower respiratory tract using different medications was suggested.41
In conclusion, the present multicentric study documented the microbial profile of the upper and lower respiratory tract of Egyptian patients with AECOPD. We could identify a distinctive pattern of inflammatory cell distribution in sputum and BAL samples of AECOPD patients. The most commonly isolated organisms were Klebsiella Pneumoniae and Strept. pneumoniae.
Conclusions of the present study may have some limitations. Microbial findings during exacerbations were not compared to corresponding results in the stable state which are strongly recommended in a subsequent study. Also, the microbial isolation and identification methods used by the present study have known limitations regarding specificity, sensitivity and reliability, which may differ from that used by other studies.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the ethical committee of Al-Azhar University Faculty of Medicine for Girls (Approval No. 886), and all patients provided informed consent before enrolment.
Informed Consent
Informed consent was obtained from all patients.
Consent for Publication
All authors reviewed the manuscript and approved its submission.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests.
References
1. Singh D, Agusti A, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease: the GOLD science committee report 2019. Eur Respir J. 2019;53(5). doi:10.1183/13993003.00164-2019
2. Bakakos P, Schleich F, Alchanatis M, et al. Induced sputum in asthma: from bench to bedside. Curr Med Chem. 2011;18:1415–1422. doi:10.2174/092986711795328337
3. Armitage MN, Spittle DA, Turner AM. A systematic review and meta-analysis of the prevalence and impact of pulmonary bacterial colonisation in stable State Chronic Obstructive Pulmonary Disease (COPD). Biomedicines. 2021;10(1):81. doi:10.3390/biomedicines10010081
4. Dubourg G, Abat C, Rolain JM, et al. Correlation between sputum and bronchoalveolar lavage fluid cultures. J Clin Microbiol. 2015;53(3):994–996. doi:10.1128/JCM.02918-14
5. Phillips TM, Moloney C, Sneath E, et al. Associated factors, assessment, management, and outcomes of patients who present to the emergency department for acute exacerbation of chronic obstructive pulmonary disease: a scoping review. Respir Med. 2022;193:106747. doi:10.1016/j.rmed.2022.106747
6. Long B, Rezaie SR. Evaluation and management of asthma and chronic obstructive pulmonary disease exacerbation in the emergency department. Emerg Med Clin North Am. 2022;40(3):539–563. doi:10.1016/j.emc.2022.05.007
7. MacLeod M, Papi A, Contoli M, et al. Chronic obstructive pulmonary disease exacerbation fundamentals: diagnosis, treatment, prevention and disease impact. Respirology. 2021;26(6):532–551. doi:10.1111/resp.14041
8. Andreas S, Testa M, Boyer L, et al. Non-typeable Haemophilus influenzae-Moraxella catarrhalis vaccine for the prevention of exacerbations in chronic obstructive pulmonary disease: a multicentre, randomised, placebo-controlled, observer-blinded, proof-of-concept, phase 2b trial. Lancet Respir Med. 2022;10(5):435–446. doi:10.1016/S2213-2600(21)00502-6
9. Liu J, Ran Z, Wang F, Xin C, Xiong B, Song Z. Role of pulmonary microorganisms in the development of chronic obstructive pulmonary disease. Crit Rev Microbiol. 2021;47(1):1–12. doi:10.1080/1040841X.2020.1830748
10. Zinellu A, Zinellu E, Pau MC, et al. A comprehensive systematic review and meta-analysis of the association between the neutrophil-to-lymphocyte ratio and adverse outcomes in patients with acute exacerbation of chronic obstructive pulmonary disease. J Clin Med. 2022;11(12):3365. doi:10.3390/jcm11123365
11. Waeijen-Smit K, Houben-Wilke S, DiGiandomenico A, Gehrmann U, Franssen FME. Unmet needs in the management of exacerbations of chronic obstructive pulmonary disease. Intern Emerg Med. 2021;16(3):559–569. doi:10.1007/s11739-020-02612-9
12. Millares L, Monso E. The microbiome in COPD: emerging potential for microbiome-targeted interventions. Int J Chron Obstruct Pulmon Dis. 2022;12(17):1835–1845. doi:10.2147/COPD.S371958
13. Seo H, Sim YS, Min KH, et al. The relationship between comorbidities and microbiologic findings in patients with acute exacerbation of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2022;20(17):855–867. doi:10.2147/COPD.S360222
14. Mussema A, Beyene G, Gashaw M. Bacterial isolates and antibacterial resistance patterns in a patient with acute exacerbation of chronic obstructive pulmonary disease in a tertiary teaching hospital, Southwest Ethiopia. Can J Infect Dis Med Microbiol. 2022;31(2022):9709253.
15. Kaleem Ullah M, Malamardi S, Siddaiah JB, et al. Trends in the bacterial prevalence and antibiotic resistance patterns in the acute exacerbation of chronic obstructive pulmonary disease in hospitalized patients in South India. Antibiotics. 2022;11(11):1577. doi:10.3390/antibiotics11111577
16. Beasley V, Joshi PV, Singanayagam A, Molyneaux PL, Johnston SL, Mallia P. Lung microbiology and exacerbations in COPD. Int J Chron Obstruct Pulmon Dis. 2012;7:555–569. doi:10.2147/COPD.S28286
17. Liang C, Mao X, Niu H, et al. Characteristics, management and in-hospital clinical outcomes among inpatients with acute exacerbation of chronic obstructive pulmonary disease in china: results from the phase i data of ACURE Study. Int J Chron Obstruct Pulmon Dis. 2021;25(16):451–465. doi:10.2147/COPD.S281957
18. He ZY, Ou LM, Zhang JQ, et al. Effect of 6 months of erythromycin treatment on inflammatory cells in induced sputum and exacerbations in chronic obstructive pulmonary disease. Respiration. 2010;80(6):445–452. doi:10.1159/000321374
19. Ho CG, Milne S, Li X, et al. Airway Eosinophilia on bronchoalveolar lavage and the risk of exacerbations in COPD. Biomedicines. 2022;10(6):1412. doi:10.3390/biomedicines10061412
20. De Nuccio F, Piscitelli P, Toraldo DM. Gut-lung microbiota interactions in Chronic Obstructive Pulmonary Disease (COPD): potential mechanisms driving progression to COPD and epidemiological data. Lung. 2022;200:773–781. doi:10.1007/s00408-022-00581-8
21. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management and prevention of chronic pulmonary disease; 2021. Available from: http://www.goldcopd.org/Guidelines/guidelines-resources.html.
22. Sato M, Chubachi S, Sasaki M, et al. Impact of mild exacerbation on COPD symptoms in a Japanese cohort. Int J Chron Obstruct Pulmon Dis. 2016;9(11):1269–1278.
23. Graham BL, Steenbruggen I, Miller MR, et al. Standardization of spirometry 2019 update. an official American Thoracic Society and European respiratory society technical statement. Am J Respir Crit Care Med. 2019;200(8):e70–e88. doi:10.1164/rccm.201908-1590ST
24. Shepherd E. Specimen collection 4: procedure for obtaining a sputum specimen. Nurs Times. 2017;113(10):49–51.
25. Reynolds HY. Bronchoalveolar lavage and other methods to define the human respiratory tract milieu in health and disease. Lung. 2011;189(2):87–99. doi:10.1007/s00408-011-9284-5
26. Lee YJ, Shin S, Roh EY, et al. Acceptability of sputum specimens for diagnosing pulmonary tuberculosis. J Korean Med Sci. 2015;30:733–736. doi:10.3346/jkms.2015.30.6.733
27. Balouiri M, Sadiki M, Ibnsouda SK. Methods for in vitro evaluating antimicrobial activity: a review. J Pharm Anal. 2016;6(2):71–79. doi:10.1016/j.jpha.2015.11.005
28. Bhattacharya AK. Role of sputum cultures in diagnosis of respiratory tract infections. Lung India. 2006;23:20. doi:10.4103/0970-2113.44426
29. Baselski V, Klutts JS, Baselski V, et al. Quantitative cultures of bronchoscopically obtained specimens should be performed for optimal management of ventilator-associated pneumonia. J Clin Microbiol. 2013;51:740–744.
30. Maestrelli P, Saetta M, Di Stefano A, et al.Comparison of leukocyte counts in sputum, bronchial biopsies, and bronchoalveolar lavage. Medicine. 1995;152(6 Pt 1):1926–1931.
31. Agnė B, Jolanta J, Rimantas S, et al. The effect of induced sputum and bronchoalveolar lavage fluid from patients with chronic obstructive pulmonary disease on neutrophil migration in vitro. Medicina. 2010;46(5):315–332. doi:10.3390/medicina46050044
32. Attaa MSS, Baessa AI, Abdullah MHM. Comparative study between bronchoalveolar lavage and induced sputum in the diagnosis of inflammatory lung diseases. Egypt J Bronchol. 2017;11:81–87. doi:10.4103/ejb.ejb_78_16
33. Tsoumakidou M, Tzanakis N, Siafakas NM. Induced sputum in the investigation of airway inflammation of COPD. Respir Med. 2003;97(8):863–871. doi:10.1016/S0954-6111(03)00035-0
34. De Serres G, Lampron N, La Forge J, et al. Importance of viral and bacterial infections in chronic obstructive pulmonary disease exacerbations. J Clin Virol. 2009;46(2):129–133. doi:10.1016/j.jcv.2009.07.010
35. Sharan H. Aerobic bacteriological study of acute exacerbations of chronic obstructive pulmonary disease. J Clin Diagn Res. 2015;9(8):DC10–DC12. doi:10.7860/JCDR/2015/14515.6367
36. Monso E, Ruiz J, Rosell A, et al. Bacterial infection in chronic obstructive pulmonary disease. A study of stable and exacerbated outpatients using the protected specimen brush. Am J Respir Crit Care Med. 1995;152(4 pt 1):1316–1320. doi:10.1164/ajrccm.152.4.7551388
37. Wang J, Chai J, Sun L, Zhao J, Chang C. The sputum microbiome associated with different sub-types of AECOPD in a Chinese cohort. BMC Infect Dis. 2020;20(1):610. doi:10.1186/s12879-020-05313-y
38. Leiten EO, Nielsen R, Wiker HG, et al. The airway microbiota and exacerbations of COPD. ERJ Open Res. 2020;6(3):00168–2020. doi:10.1183/23120541.00168-2020
39. Goolam Mahomed T, Peters RPH, Allam M, et al. Lung microbiome of stable and exacerbated COPD patients in Tshwane, South Africa. Sci Rep. 2021;11(1):19758. doi:10.1038/s41598-021-99127-w
40. Zhu K, Zhou S, Xu A, et al. Microbiota imbalance contributes to COPD deterioration by enhancing IL-17a production via miR-122 and miR-30a. Mol Ther Nucleic Acids. 2020;22:520–529. doi:10.1016/j.omtn.2020.09.017
41. Han Y, Hua J, He B, Zhang J. Inhaled antibiotics and airway bacterial decolonization for patients with chronic obstructive pulmonary disease: the rationale and future. J Transl Int Med. 2022;10(3):181–184. doi:10.2478/jtim-2022-0005
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association of Frailty with Patient-Report Outcomes and Major Clinical Determinants in Patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease
Yang M, Liu Y, Zhao Y, Wang Z, He J, Wang Y, Anme T
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:907-919
Published Date: 12 April 2024
The Role of Advanced Lung Cancer Inflammation Index in Predicting COPD Exacerbation Risks
Kwok WC, Leung SHI, Tam TCC, Chau CH, Lam FM, Ho JCM
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:559800
Published Date: 31 January 2026