")
Back to Journals » Infection and Drug Resistance » Volume 16
Bacteremia Caused by Kalamiella piersonii Found in an Infant During the Course of Gastrointestinal Food Allergy
Authors Sada J , Hirai J , Ota K, Numoto S, Honma H, Mori N , Sakanashi D, Mikamo H, Okumura A
Received 12 January 2023
Accepted for publication 29 March 2023
Published 2 May 2023 Volume 2023:16 Pages 2647—2651
DOI https://doi.org/10.2147/IDR.S402364
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Jun Sada,1 Jun Hirai,2,3 Koki Ota,1 Shingo Numoto,1 Hitoshi Honma,1 Nobuaki Mori,2,3 Daisuke Sakanashi,3 Hiroshige Mikamo,2,3 Akihisa Okumura1
1Department of Pediatrics, Aichi Medical University Hospital, Nagakute, Aichi, Japan; 2Department of Clinical Infectious Diseases, Aichi Medical University Hospital, Nagakute, Aichi, Japan; 3Department of Infection Control and Prevention, Aichi Medical University Hospital, Nagakute, Aichi, Japan
Correspondence: Jun Sada, Department of Pediatrics, Aichi Medical University Hospital, 1-1, Yazako-karimata, Nagakute, Aichi, 480-1195, Japan, Tel +81-561-62-3311, Fax +81-561-76-2673, Email [email protected]
Abstract: Kalamiella piersonii is rare pathogen, and its pathogenicity to humans has been unknown. We describe an infant with bacteremia caused by Kalamiella piersonii. The patient was a 2-month-old girl presented with diarrhea, poor oral intake, and vomiting. The patient was tentatively diagnosed with acute enterocolitis. After admission, the patient developed a fever and blood culture yielded Gram-negative cocci, first determined to be Pantoea septica by matrix-assisted laser desorption/ionization time-of-flight mass spectrometry. However, genetic analysis of 16S rRNA allowed its identification as Kalamiella piersonii (GenBank accession number is OQ547240). Other housekeeping genes such as gyrB, rpoB, and atpD also identified the isolated strain as Kalamiella piersonii. The patient was successfully treated with cefotaxime without sequelae. Later, the patient was diagnosed as non-IgE-mediated gastrointestinal food allergy. Our experience indicated that Kalamiella piersonii is a potential human pathogen that can cause invasive infections even in infants and children. Identification of Kalamiella piersonii is difficult with routine conventional tests, and detailed studies including genetic analyses are necessary to clarify the pathogenicity of Kalamiella piersonii in humans.
Keywords: Kalamiella piersonii, 16S rRNA, non-IgE-mediated gastrointestinal food allergy, matrix-assisted laser desorption/ionization time-of-flight mass spectrometry
Introduction
Kalamiella piersonii gen. nov., sp. nov. (Kalamiella piersonii) is a motile Gram-negative organism in the order Enterobacterales of a proposed genus and species belonging to the family Erwiniaceae. Historically, this species was first isolated from the International Space Station using a meta-genome approach. It is named after the scientist Abdul Kalam and the space microbiologist Duane Pierson.1 Initially, the PathogenFinder algorithm predicted that Kalamiella piersonii strains will not be human pathogens.1 However, there have been two reports of human infections with Kalamiella piersonii,2,3 although did not involve children. Here, we report Kalamiella piersonii bacteremia in a 2-month-old girl.
Case Report
A 2-month-old girl was admitted to our hospital because of diarrhea, poor oral intake, and vomiting for 7 days. She was born by spontaneous vaginal delivery at 41 weeks of gestation and weighed 2956 g at birth. She was mixed fed and had shown good weight gain. At admission, her body temperature was 36.7°C; blood pressure, 105/55 mmHg; heart rate, 130 beats per minute; and respiratory rate, 30 times per minute. Her abdomen was flat and soft with no signs of pain on palpation. Laboratory tests showed a white blood cell count of 9000/µL (neutrophils: 22.2%), normal serum levels of electrolytes, and a C-reactive protein (CRP) level of 0.05 mg/dL. Her urinalysis results were unremarkable. Bacterial cultures of blood, urine, and stool were negative at admission. Abdominal X-ray showed a gasless abdomen, but abdominal ultrasonography revealed bowel wall edema in the small intestine.
Initially, the patient was treated with intravenous fluids, based on a tentative diagnosis of acute enterocolitis, but the diarrhea did not improve. On the fourth day of hospitalization, she developed a fever of 39°C and lethargy. Laboratory tests revealed an increased white blood cell count of 17,500 µ/L (neutrophils: 43.0%), and an elevated serum CRP level of 10.02 mg/dL. Intravenous cefotaxime (CTX) and ampicillin (AMC) were started after the sepsis work-up.
A blood culture on the fourth day of hospitalization revealed a Gram-negative bacillus. Bacterial cultures of urine and stool yielded no growth of the pathogen. Initially, this microorganism was identified as Pantoea septica by matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS, MALDI Biotyper ver. 9.0.0.0; Bruker Daltonics, Billerica, MA, USA), with low identification and spectral scores of 1.75. An additional microbiological examination conducted to identify the organism isolated from the blood allowed its identification as Kalamiella piersonii, based on 16S rRNA gene sequencing and 100% homology (1409 of 1409 bases) with a sequence in the EZBioCloud 16S database (http://www.ezbiocloud.net/eztaxon). Table 1 shows additional housekeeping genes analysis using gyrB, rpoB, and atpD based on the previous investigation.4 The results identified the isolated strain as Kalamiella piersonii based on homology of 98.65% (950 of 963 bases) in gyrB, 96.10% (1083 of 1094 bases) in rpoB, and 98.88% (880 of 890 bases) in atpD using NCBI Blast database (http://blast.ncbi.nlm.nih.gov/Blast.cgi). Table 2 shows the antimicrobial susceptibility of the isolated strain of Kalamiella piersonii as determined using the MicroScan WalkAway system with the NM2J panel (Beckman Coulter). The minimum inhibitory concentration was measured based on the Enterobacteriaceae category of the Clinical and Laboratory Standards Institute M100-S26. VITEK@ 2 GN ID card (bioMérieux, France) classified the isolated strain into Pantoea spp. (98% binumber 4607710151500210). GenBank accession number of the 16SrRNA sequences of Kalamiella piersonii isolated from our patient is OQ547240.
 |
Table 1 Identification of Isolated Strain Based on Housekeeping Genes Analysis with NCBI Blast Database |
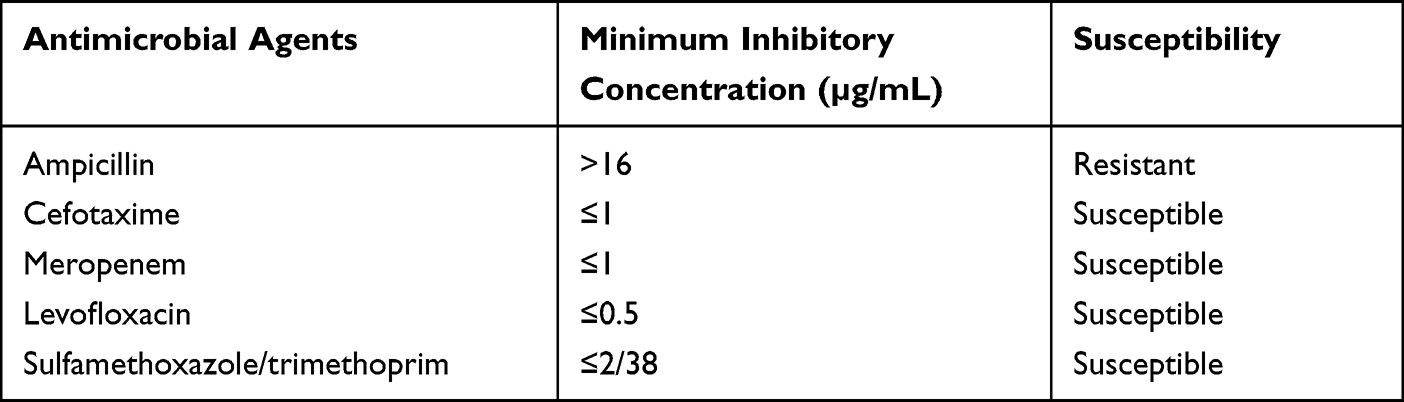 |
Table 2 Antibiotic Susceptibility |
The patient’s fever subsided and her general condition quickly improved after intravenous CTX and AMC. In accordance with the results of the antimicrobial susceptibility test, CTX monotherapy was continued for 10 days. However, her diarrhea persisted even after successful antimicrobial treatment. As a non-IgE-mediated gastrointestinal food allergy was suspected, the patient’s oral milk intake was substituted by elemental formula, after which her diarrhea gradually improved. Allergen-specific IgE testing, performed to confirm the diagnosis, showed a value of 4.43 IU/mL for milk. Lymphocyte stimulation tests using kappa-casein, lactoferrin, and human alpha-lactalbumin were negative. The occult blood or eosinophils were not detected in stool, whereas calprotectin was detected. An oral food challenge of infant formula resulted in recurrence of diarrhea. Based on these results, she was diagnosed with a non-IgE-mediated gastrointestinal food allergy. She was fed elemental formula and had no recurrence of diarrhea for >2 months after discharge.
Discussion
There have been only two reports of Kalamiella piersonii infection. Rekha et al investigated the pathogenicity of Kalamiella piersonii isolated from the urine of a male patient with symptomatic kidney stone disease.2 The isolated bacterium was taxonomically identified as Kalamiella piersonii following a detailed genomic analysis. Although the patient had no symptoms of active urinary tract infection, the isolated strain of Kalamiella piersonii displayed several features indicative of its urinary tract association and involvement in struvite crystallization. Alpizar-Rivas et al reported Kalamiella piersonii bacteremia in a 56-year-old woman with end-stage nonischemic cardiomyopathy, diabetes, and chronic obstructive pulmonary disease.3 The patient was presumed to have developed bacteremia via her indwelling catheter. That report showed that Kalamiella piersonii may be present in the human gastrointestinal tract and cause invasive infection in susceptible individuals, such as immunocompromised hosts. The infection in our patient demonstrated that Kalamiella piersonii can cause bacteremia even in infants with no obvious immunological compromise.
The route of infection was unclear in our patient. One possibility is bacterial translocation related to her non-IgE-mediated gastrointestinal food allergy. Indeed, our patient had severe diarrhea prior to Kalamiella bacteremia and her level of calprotectin in stool was elevated, indicative of mucosal damage that could have facilitated bacterial translocation.5 However, there is no supportive evidence that gastrointestinal food allergy may cause bacterial translocation, as stool culture was negative and bacteremia due to bacterial translocation has not been reported in infants with non-IgE-mediated gastrointestinal food allergy. There was no evidence of a urinary tract infection: her urinalysis was normal and the urine bacterial culture was negative. While catheter infection may have been possible, Kalamiella piersonii is unlikely to be indigenous to the skin. We were unable to find a possible source of infection in this patient, as the patient had no clinical signs or symptoms outside of gastrointestinal tract. The difficulty in determining the route of infection is also seen in the patient reported previously. The patient reported by Alpizar-Rivas et al was presumed to have catheter-related infection, although the authors also stated that the definition of catheter-related infection was not fulfilled.3 In this patient, there was no other clinical findings to indicate the route of infection. Detailed microbiological analysis such as PCR panels using samples from multiple sites including blood, gastrointestinal tract, and urinary tract will be required in order to understand the pathogenicity of Kalamiella piersonii in humans.
The prevalence of Kalamiella piersonii infection may be underestimated. One of the problems regarding the identification of Kalamiella piersonii is that routine conventional tests, such as automated chemical tests, poorly distinguish between Kalamiella spp. and Pantoea spp. because of their similar biochemical characteristics. Although MALDI-TOF MS is a useful tool for microbial identification in clinical diagnostic microbiology,6 it also cannot identify Kalamiella piersonii, due to limitations in current databases and libraries. A determination of the true prevalence of Kalamiella piersonii bacteremia requires not only an automated identification system but also appropriate biochemical tests, such as 16S rRNA and rpoB gene analysis. The strain isolated from our patient was first classified as Pantoea septica, based on MALDI-TOF MS, but after a genetic analysis it was reclassified as Kalamiella piersonii. It is noteworthy that Kalamiella piersonii was also misclassified as Pantoea agglomerans or Salmonella by MALDI-TOF MS or automated phenotypic identification in the patients reported by Alpizar-Rivas et al.3 Thus, without a genetic analysis, Kalamiella piersonii infection can be mistaken as Pantoea septica infection.
Based on previous genomic analyses, Kalamiella piersonii has multiple drug resistance mechanisms, such as efflux pump systems and chromosomally encoded beta-lactamase genes related to penicillin and cephalosporin resistance.1,2 The strain isolated from our patient was resistant to penicillin but susceptible to cephalosporin. Additional cases are needed to assess multiple drug resistance in Kalamiella piersonii.
In summary, we describe a case of Kalamiella piersonii bacteremia in an infant with non-IgE-mediated gastrointestinal food allergy. Kalamiella piersonii is a potential human pathogen that can cause invasive infections even in infants and children. Detailed studies, including genetic analyses, are necessary to clarify the pathogenicity of Kalamiella piersonii in humans.
Abbreviations
CRP, C-reactive protein; CTX, cefotaxime; AMC, ampicillin; MALDI-TOF MS, matrix-assisted laser desorption/ionization time-of-flight mass spectrometry.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics and Concern
This research complies with the guidelines for human studies and is in accordance with the Declaration of Helsinki. This report is approved by the institutional review board of the Aichi Medical University Hospital. Written informed consent for publication of their details was obtained from the parents.
Acknowledgments
The authors are grateful to their colleagues for the management of the patient and to the subject for participating in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors and co-workers did not receive any specific funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Singh NK, Wood JM, Mhatre SS, et al. Metagenome to phenome approach enables isolation and genomics characterization of Kalamiella piersonii gen. nov., sp. nov. from the International Space Station. Appl Microbiol Biotechnol. 2019;103(11):4483–4497. doi:10.1007/s00253-019-09813-z
2. Rekha PD, Hameed A, Manzoor MAP, et al. First report of pathogenic bacterium Kalamiella piersonii isolated from urine of a kidney stone patient: draft genome and evidence for role in struvite crystallization. Pathogens. 2020;9(9):711. doi:10.3390/pathogens9090711
3. Alpizar-Rivas R, Cameron A, Hay CM. Human disease caused by Kalamiella piersonii. Annal Intern Med Clin Cases. 2022;1:e210220.
4. Brady C, Cleenwerck I, Venter S, et al. Phylogeny and identification of Pantoea species associated with plants, humans and the natural environment based on multilocus sequence analysis (MLSA). Syst Appl Microbiol. 2008;31(6–8):447–460. doi:10.1016/j.syapm.2008.09.004
5. Calvani M, Anania C, Cuomo B, et al. Non-IgE- or mixed IgE/Non-IgE-mediated gastrointestinal food allergies in the first years of life: old and new tools for diagnosis. Nutrients. 2021;13(1):226. doi:10.3390/nu13010226
6. Tsuchida S, Umemura H, Nakayama T. Current status of matrix-assisted laser desorption/ionization-time-of-flight mass spectrometry (MALDI-TOF MS) in clinical diagnostic microbiology. Molecules. 2020;25(20):4775. doi:10.3390/molecules25204775
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.