Back to Journals » Clinical Ophthalmology » Volume 20
B Vitamins and Ocular Health
Authors Johnson EJ, Poteet J ![]() , Gioia N
, Gioia N ![]() , Maharaj RRL, Benitez-del-Castillo JM, Labetoulle M
, Maharaj RRL, Benitez-del-Castillo JM, Labetoulle M
Received 21 October 2025
Accepted for publication 12 February 2026
Published 12 March 2026 Volume 2026:20 575752
DOI https://doi.org/10.2147/OPTH.S575752
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Elizabeth J Johnson,1 Julie Poteet,2 Neda Gioia,3 Richard RL Maharaj,4 Jose Manuel Benitez-del-Castillo,5 Marc Labetoulle6
1Friedman School of Nutrition Science and Policy, Tufts University, Boston, MA, USA; 2MyEyeDr, Acworth, GA, USA; 3Integrative Vision Corp, Shrewsbury, NJ, USA; 4Prism Eye Institute, Brampton, Ontario, Canada; 5Department of Ophthalmology, Hospital Clinico San Carlos de Madrid, Madrid, Spain; Instituto de Investigaciones Oftalmológicas Ramón Castroviejo, Universidad Complutense de Madrid, Madrid, Spain; Ocumed-Clinica Rementeria, Madrid, Spain; 6Department of Ophthalmology, Quinze-Vingts National Ophthalmology Hospital and Vision Institute, Paris, France; Service d’Ophtalmologie, Hôpital Bicêtre, Assistance Publique-Hôpitaux de Paris, Paris-Saclay University, Kremlin-Bicêtre, France
Correspondence: Julie Poteet, Email [email protected]
Abstract: The B vitamins are a varied family whose members are integral to metabolic pathways and cellular processes throughout the body. Unlike vitamins A, C, and E, the B complex has generally not been considered among the key ingredients of supplements intended to maintain eye health and prevent age-related disease and vision loss. This perspective may be shifting with the emergence of 3 elements: (1) a greater understanding of the pathogenic mechanisms involved in conditions such as age-related macular degeneration, diabetic retinopathy, glaucoma, cataracts, dry eye disease, and other ocular surface disorders; (2) observational studies linking B vitamins to risk of eye disease development or progression; and (3) preclinical and clinical evidence supporting supplementation with B vitamins to improve potential ocular outcomes. This review synthesizes the available data on the role of B vitamins in promoting healthy eye structure and function, highlighting connections between individual vitamins and disease, and discussing the clinical considerations for B vitamin supplementation.
Keywords: age-related macular degeneration, diabetic retinopathy, glaucoma, cataract, dry eye disease, supplementation
Introduction
The realization that nutrition affects eye health came almost 100 years before the term “vitamine” was coined in 1912.1 Indeed, corneal ulcers related to what would later be recognized as vitamin A deficiency were first described in 1816.1 Over the next 200 years, our understanding of the connection between nutrition and health would grow dramatically. It is now both possible and plausible to identify cellular processes and molecular pathways associated with disease and target vitamin-based interventions to counter pathogenic mechanisms. Ocular diseases that can lead to vision loss and for which disease risk is modifiable, including age-related macular degeneration (AMD), diabetic retinopathy, glaucoma, and cataract, are attractive targets for nutritional intervention.2 There is precedent for ocular disease prevention through improving beneficial micronutrient intake: the World Health Organization began recommending vitamin A supplementation in 1988 to combat vitamin A deficiency, a leading cause of blindness in children.2
Historically, vitamins and antioxidants strongly connected with ocular disease prevention included vitamins A, C, and E, and the carotenoids lutein and zeaxanthin.3,4 However, emerging evidence supports a key role for B vitamins in maintaining ocular health and reducing the risk of eye disease development and progression.5–7 Eight vitamins comprise the B complex: B1, B2, B3, B5, B6, B7, B9, and B12, several of which have alternate vitamer forms (molecularly similar organic compounds with shared basic vitamin functions) (Table 1).6,8,9 All B vitamins are water-soluble; therefore, they are not retained in the body to the extent of fat-soluble vitamins (eg, vitamins A, D, E, K) and require daily replenishment.9 Each member of the B vitamins act as coenzymes for essential enzymatic activities supporting diverse cellular and metabolic processes, from glucose metabolism and energy production to neurologic function and myelin synthesis.8,9 Although these functions are widely applicable to systems throughout the body, certain processes are particularly relevant to ocular health.
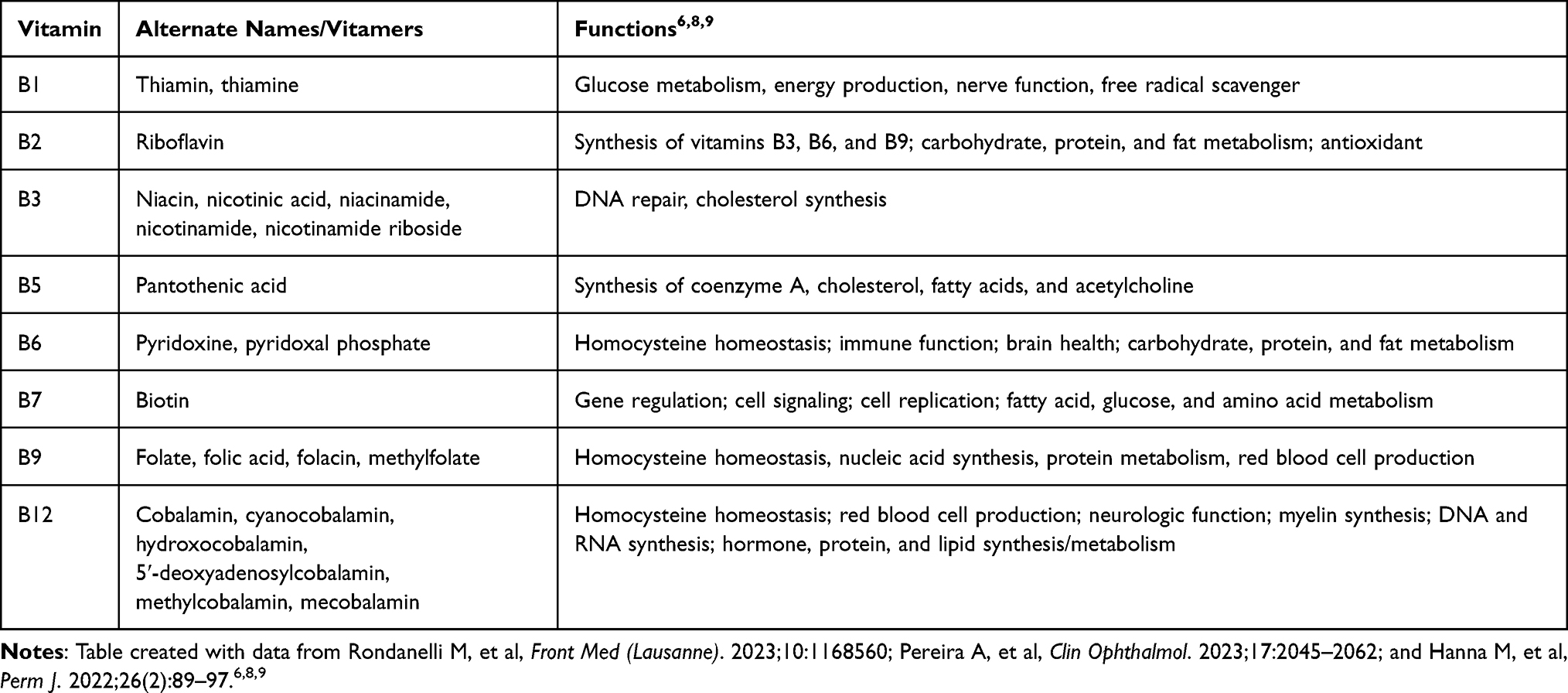 |
Table 1 B Vitamin Overview |
With a growing body of literature driven by preclinical and clinical study data that regularly provide new insights into the connection between B vitamins and ocular functionality, there is a need to synthesize this wealth of information for clinicians and researchers. This narrative review discusses the role of B vitamins in eye health, from the cellular processes in which they participate to the evidence that they modify ocular disease risk. Recommendations for B vitamin supplementation are provided, and future research to fill existing knowledge gaps is discussed.
Methods
Data to inform this narrative review were obtained through a PubMed search of the MEDLINE database to identify publications relevant to the relationship between B vitamins and ocular health using the search terms: “age-related macular degeneration”, “AMD”, “diabetic retinopathy”, “cataract”, “glaucoma”, “intraocular pressure”, “dry eye disease”, “dry eye syndrome”, “keratoconjunctivitis sicca”, “Sjogren’s syndrome”, “ocular rosacea”, “B vitamin”, “vitamin B1”, “vitamin B2”, “vitamin B3”, “vitamin B5”, “vitamin B6”, “vitamin B7”, “vitamin B9”, “vitamin B12”, “thiamin”, “thiamine”, “riboflavin”, “niacin”, “niacinamide”, “pantothenic acid”, “pyridoxine”, “biotin”, “folate”, “folic acid”, “cobalamin”, “cyanocobalamin”, “nicotinic acid”, and “nicotinamide”. The search was conducted in April 2025 and limited to articles published in English within the past 10 years. The titles and abstracts of potential articles were screened for relevance and full text articles of potentially eligible publications were then assessed for inclusion. Reference lists from articles identified through the literature search were used to capture additional relevant publications. Articles were selected based on their relevance and contribution to the understanding of B vitamins and ocular health. Articles were reviewed to identify trends and gaps in the literature, and inconsistencies across the studies. A qualitative evidence synthesis was conducted, highlighting connections between individual vitamins and ocular conditions, and discussing the clinical considerations for B vitamin supplementation.
Biological Role of B Vitamins in Ocular Physiology and Ocular Health
To date, research supports important protective and/or restorative roles for B vitamins in a number of aspects of ocular health and physiology. B vitamins can help modulate the negative ocular consequences of mitochondrial dysfunction and oxidative stress, offer neurotropic and retinal protective benefits, and facilitate homocysteine homeostasis (Figure 1).6,9–19
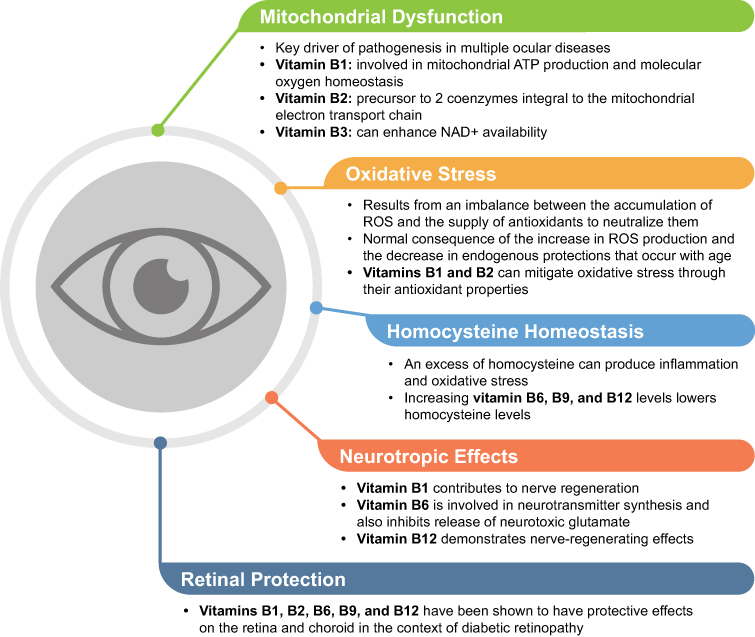 |
Figure 1 Overview of the protective and/or restorative biological roles of B vitamins (bold text) in protecting and/or restoring ocular physiology and ocular health in settings of dysfunction or pathology.6,9–19 Abbreviation: ROS, reactive oxygen species. |
Mitochondrial Dysfunction
The eye, specifically the retina and optic nerve, has a high metabolic demand, rendering it particularly susceptible to the effects of mitochondrial dysfunction.7,10,11 Mitochondrial dysfunction is a key driver of pathogenesis in multiple ocular diseases.10,11 For certain conditions, such as AMD and glaucoma, the aberrant cellular processes involved in disease pathogenesis, including oxidative stress and inflammation, are believed to be predominantly mediated by mitochondrial dysfunction.10 Indeed, preclinical data indicate mitochondrial abnormalities precede detectable optic nerve degeneration in glaucoma.20 Among the putative pathogenic changes are alterations in the metabolism of nicotinamide adenine dinucleotide (NAD), which is a central cofactor in a multitude of metabolic pathways.10,11 NAD+ is generated principally from nicotinamide (vitamin B3), but also can be derived from tryptophan and other vitamin B3 vitamers (eg, nicotinic acid, nicotinamide riboside).11 Aging and chronic oxidative stress deplete NAD+ stores, and reduced NAD+ bioavailability contributes to mitochondrial dysfunction in neurologic and ocular diseases of aging such as Alzheimer’s disease, Parkinson’s disease, AMD, and glaucoma.10,11 These mechanistic observations support the potential for therapeutic benefit from enhancing NAD+ availability in ocular diseases, potentially through vitamin B3 supplementation.10,11 As proof of this concept, increasing NAD+ bioavailability in retinal pigment epithelial cells in vitro through incubation with the vitamin B3 vitamer nicotinamide mononucleotide (NMN) was shown to improve mitochondrial function.21
Mitochondrial energy production also requires vitamin B1 (thiamine) and vitamin B2 (riboflavin).12,13 Vitamin B1 is involved in mitochondrial ATP production and in molecular oxygen homeostasis within mitochondria.13 Vitamin B2 is a precursor to the coenzymes flavin mononucleotide and flavin adenine dinucleotide, which are integral to the mitochondrial electron transport chain.12 Supplementation with vitamin B2 in conjunction with other medications has been used to accelerate visual recovery in Leber hereditary optic neuropathy, a condition in which mitochondrial dysfunction is caused by mutations in mitochondrial genes.12
Oxidative Stress
A consequence of mitochondrial energy generation is the production of reactive oxygen species (ROS).14 Oxidative stress results from an imbalance between the accumulation of ROS and the supply of antioxidants to neutralize them. Oxidative stress is a normal consequence of the increase in ROS production and the decrease in endogenous protections that occur with age.15 Oxidative stress is present in several conditions with ocular manifestations, including AMD, glaucoma, diabetic retinopathy, dry eye disease (DED), and Sjögren’s syndrome,5,22 and is damaging to structural proteins of the lens.23 Vitamins B1 and B2 can mitigate oxidative stress through their antioxidant properties, functioning directly or indirectly as free radical scavengers.6,9
Homocysteine Homeostasis
Oxidative stress related to inflammation can be induced by an excess of homocysteine (ie, hyperhomocysteinemia).16 The most common cause of hyperhomocysteinemia is vitamin B9 deficiency.24 In the eye, homocysteine and associated inflammatory processes are implicated in vascular endothelial cell injury, optic nerve damage, apoptosis of lens epithelial cells, and visual dysfunction.16,23,24 The metabolism of homocysteine involves multiple B vitamins: vitamins B9 and B12 facilitate the conversion of homocysteine into methionine by methylenetetrahydrofolate reductase (MTHFR), and vitamin B6 is necessary for the metabolism of homocysteine to cysteine (Figure 2).16,23,25 Insufficient vitamin supply and certain mutations or polymorphisms in the MTHFR gene interfere with this process, resulting in abnormally high concentrations of homocysteine.16 The reverse is also true: increasing vitamins B6, B9, and B12 lowers homocysteine levels.15,18
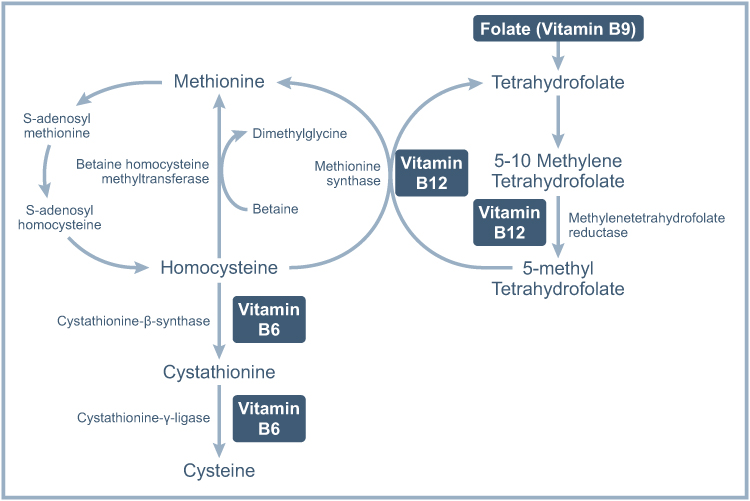 |
Figure 2 Roles of folate (vitamin B9) and vitamins B6 and B12 in homocysteine metabolism. Figure adapted from: Yuan S et al. BMC Medicine 2021;19:97, via a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/).25 |
Homocysteine elevation has been observed in a variety of ocular conditions, including AMD, diabetic retinopathy, glaucoma, cataracts, and retinal vascular occlusion.23,24,26–33 Higher circulating concentrations of homocysteine also have been linked to increased macular thickness in patients with diabetes and retinal nerve fiber thinning in patients with diabetic retinopathy.29,34
A meta-analysis of 11 case-control studies reported significantly higher plasma total homocysteine levels in patients with AMD versus controls (difference, 2.67 µmol/L [95% CI: 1.60–3.74]).26 Interestingly, in subgroup analyses, total plasma homocysteine concentration was greater for patients with exudative AMD (wet AMD) than the overall AMD population, whereas no such elevation was observed for atrophic AMD (dry AMD). Similarly, meta-analysis data have shown an association between elevated plasma homocysteine and risk of primary open-angle glaucoma (POAG), but no such association was found for normal-tension glaucoma (NTG)33,35 or elevated intraocular pressure.36
There is uncertainty regarding the timing of homocysteine elevation and its effect on ocular health. For example, in AMD case-control studies wherein the measurement of homocysteine generally occurs once the disease process has progressed to a diagnosable level, homocysteine elevation is positively associated with the presence of AMD.26 However, in prospective studies, such as the Women’s Health Study and the Physicians’ Health Study II, where homocysteine was measured at baseline and disease presence was assessed during follow-up, higher plasma homocysteine concentration did not confer a significantly increased risk of developing AMD.37,38 Interestingly, the degree of homocysteine elevation has been shown to positively correlate with severity of disease in patients with diabetic retinopathy.28,29 Notably, metformin, a treatment commonly used in patients with diabetes, has been shown to cause vitamin B12 malabsorption9 and an increase in homocysteine.28 Overall, the temporal and causal relationships between homocysteine elevation and adverse effects on eye health remain to be determined.
Neurotropic Effects
Three of the B vitamins are considered to be neurotropic: vitamins B1, B6, and B12.19,39 Vitamin B1 contributes to nerve regeneration through its involvement in energy production via carbohydrate metabolism in nerve cells and by protecting nerve cells from oxidative stress.19 Through its role in amino acid metabolism, vitamin B6 is involved in neurotransmitter synthesis. Vitamin B6 also inhibits release of glutamate, which is neurotoxic, and has been shown to restore sensory nerve function. In addition to promoting nerve cell survival and participating in myelin synthesis, preclinical evidence indicates vitamin B12 demonstrates nerve-regenerating effects. The importance of vitamin B12 in maintaining nerve function related to the cornea is illustrated in a study showing reversal of neurotrophic keratitis through vitamin B12 supplementation in a patient with vitamin B12 deficiency.40
Retinal Protection
B vitamins, including B1, B2, B6, B9, and B12, have been cited for their ability to protect the retina and choroid in the context of diabetic retinopathy.6 Hyperglycemia resulting from uncontrolled or inadequately controlled diabetes mellitus can lead to endothelial dysfunction in retinal capillaries, ultimately resulting in diabetic retinopathy marked by microvascular damage and retinal dysfunction.5 In vitro, vitamin B1 exposure has been shown to neutralize the effects of hyperglycemia on endothelial cells.41 Vitamin B1 normalizes metabolic pathways that are accelerated in a high-glucose environment, thereby reducing the accumulation of ROS and other metabolites such as pyruvate and lactate. Vitamin B1 also exerts protective effects against cell damage and apoptosis in retinal microvascular cells.
Evidence Linking B Vitamins with Specific Ocular Conditions
Ocular Manifestations of B Vitamin Deficiencies
The mechanistic connection between ocular health and B vitamins is perhaps most strongly illustrated clinically by the manifestations of vitamin deficiencies. Acute vitamin B1 deficiency, for example, may lead to ocular symptoms associated with Wernicke’s encephalopathy (eg, nystagmus, ophthalmoplegia, diplopia, papilledema), whereas deficiency in vitamin B2 can cause blurred vision and nyctalopia.8,42 Deficiencies in vitamins B9 and B12 are both associated with optic neuropathy and increased risk of AMD, but vitamin B12 deficiency may underlie neuropathic pain in patients with severe DED.8,42,43 Deficiency in biotinidase, an enzyme critical to biotin (vitamin B7) recycling, results in secondary biotin deficiency and is associated with visual loss, optic atrophy, conjunctivitis, and scotoma in a subset of patients.44 However, clinical deficiency in B vitamins is not required to confer increased risk of ocular disease development and progression. The following sections will describe data linking vitamin intake or concentrations with ocular diseases and the effects of B vitamin supplementation.
Age-Related Macular Degeneration
A large body of evidence supports an association between dietary intake or circulating concentrations of B vitamins and risk of AMD, including meta-analyses, prospective and retrospective observational studies, and interventional clinical trials (Table 2).26,38,45–55 Lower dietary intake in patients with AMD versus controls has been reported for all B vitamins except vitamin B7, with the strongest evidence for vitamins B6, B9, and B12.45–48 For example, in the Coimbra Eye Study, which enrolled patients over 55 years of age with AMD (n=768) and age- and sex-matched controls (n=1224), patients without AMD had significantly higher dietary intake of vitamin B9 than those with AMD.46 Multiple studies revealed that dietary intake of B vitamins, including B1, B5, B6, B9, and B12, has an inverse association with both risk of AMD development and risk of AMD progression.38,49–53,55 In the Alienor Study, a prospective, population-based study of participants aged 73 years and older (N=861), risk for advanced AMD decreased with higher dietary intake of vitamins B5 and B6 and with a serum vitamin B9 concentration in the normal range (≥10 nmol/L; vs vitamin B9 deficiency).52 In the multicenter, randomized Age-Related Eye Disease Study (AREDS), after adjustment for demographic, clinical, and other covariates, increased dietary intake of vitamin B9 was significantly associated with reduced risk of progression to advanced nonexudative AMD with geographic atrophy (p = 0.007) for patients aged 55 to 80 years who had at least 1 eye without advanced AMD at baseline (N=2525).50 Combined data from AREDS and AREDS2 (N=8130) further revealed a significant decrease in risk of progression to late AMD with increased dietary intake of vitamins B6 and B9.51 A subsequent analysis found higher dietary intake of vitamins B6, B9, and B12 to be protective against geographic atrophy area–based progression (AREDS: N=508; AREDS2: N=867).55 Over a mean follow-up of 11.2 years in the prospective Physicians’ Health Study II cohort of male physicians aged 55 years and older (N=146), every 1-SD increase in dietary intake of vitamin B6 decreased the risk of AMD by 49%.38
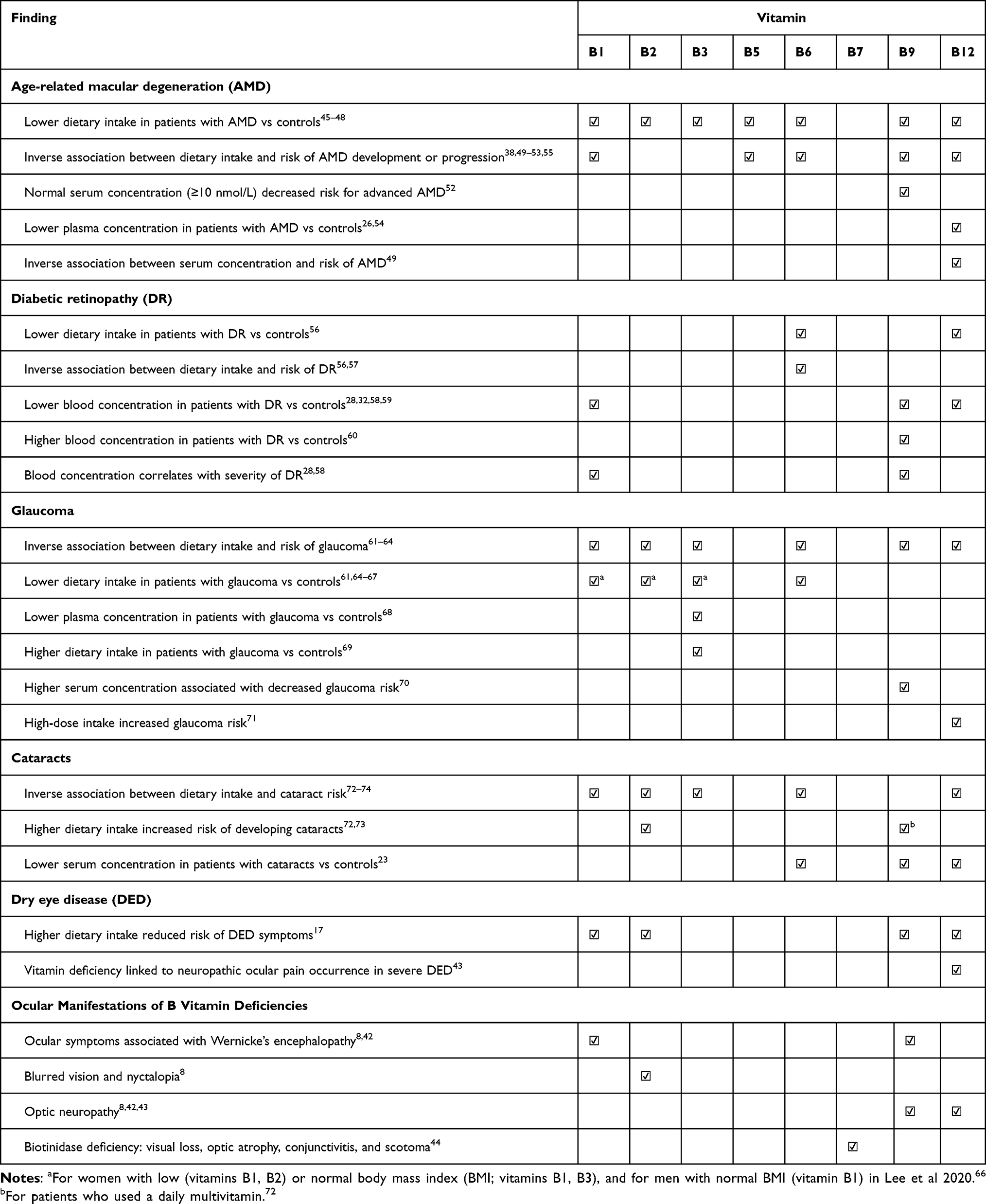 |
Table 2 Associations Between Dietary B Vitamin Intake or Circulating Concentration and Ocular Diseases |
Demographic and clinical factors appear to modify associations between B vitamins and AMD. In a meta-analysis conducted by Huang et al,26 serum vitamin B9 concentration was significantly lower in patients with exudative AMD versus controls, but this finding was not observed for the overall AMD population. Using data from the US-based National Health and Nutrition Examination Survey (NHANES 2005–2008; N=20497), Liu et al48 found that dietary intake of vitamins B1, B2, B6, B9, and B12 was lower in patients with versus without AMD for the overall study population. However, associations between vitamins B1, B2, and B6 and AMD were influenced by the presence of diabetes; the association between vitamin B9 and AMD was influenced by body mass index (BMI); and risk for AMD increased with low dietary intake of vitamin B12 for men but not women. Whereas data from NHANES uncovered a decrease in risk of late AMD with higher dietary intake of vitamin B1, no significant association was observed between dietary intake of vitamin B1 and risk for early AMD.53 In contrast, data from iterations of the Blue Mountains Eye Study (N=1390) found deficiencies in vitamin B9 or B12 increased the risk for early AMD and for any AMD, but only vitamin B12 deficiency increased the risk for late AMD.49 Importantly, vitamin B12 supplementation reduced the risk for early AMD and for any AMD in this study.
B Vitamin Supplementation for the Prevention of AMD Development or Progression
Preclinical data support the potential for B vitamin supplementation as a means of preventing AMD. For example, in vitro exposure to nicotinamide (vitamin B3) ameliorated the development of AMD-related phenotypes in retinal pigment epithelial cells,75 treatment with NMN (vitamin B3) protected cultured retinal pigment epithelial cells from senescence and inflammation by reducing DNA damage and maintaining mitochondrial function,76 and vitamin B6 supplementation suppressed retinal neovascularization in a murine model of AMD.77
Although there have been multiple clinical trials to evaluate whether supplementation is effective for the prevention of AMD development or progression, most of these studies used formulations containing an array of vitamins and minerals,78–81 thereby obscuring the attribution of clinical efficacy to any one agent or class of agents. In the context of B vitamins, a notable exception is the Women’s Antioxidant and Folic Acid Cardiovascular Study (WAFACS), a double-masked, placebo-controlled clinical trial in which women aged 40 years and older with preexisting cardiovascular disease (CVD) or 3 or more CVD risk factors were randomized to treatment with a B vitamin supplement (n=2607) or placebo (n=2598) (Table 3).82 The supplement contained vitamin B6 (50 mg/day), vitamin B9 (2.5 mg/day; in the form of folic acid), and vitamin B12 (1 mg/day). Over an average follow-up duration of 7.3 years, daily B vitamin supplementation decreased the risk of developing AMD by 34% (relative risk [RR], 0.66 [95% CI: 0.47–0.93]; p = 0.02) and the risk of developing visually significant AMD by 41% (RR, 0.59 [95% CI: 0.36–0.95]; p = 0.03). A treatment effect was evident within approximately 2 years for AMD development and within approximately 4 years for visually significant AMD development. The authors speculated that the reduction in AMD risk may be related to homocysteine lowering, direct antioxidant effects, enhanced endothelial nitric oxide concentration and subsequent increase in vascular reactivity, or some combination thereof. Notably, a substudy from WAFACS demonstrated significant reductions from baseline in mean plasma homocysteine concentration for patients who received the B vitamin supplement (p = 0.001) but not for those in the placebo group.83 No serious adverse events linked to study treatment were reported and no ocular adverse events were noted.
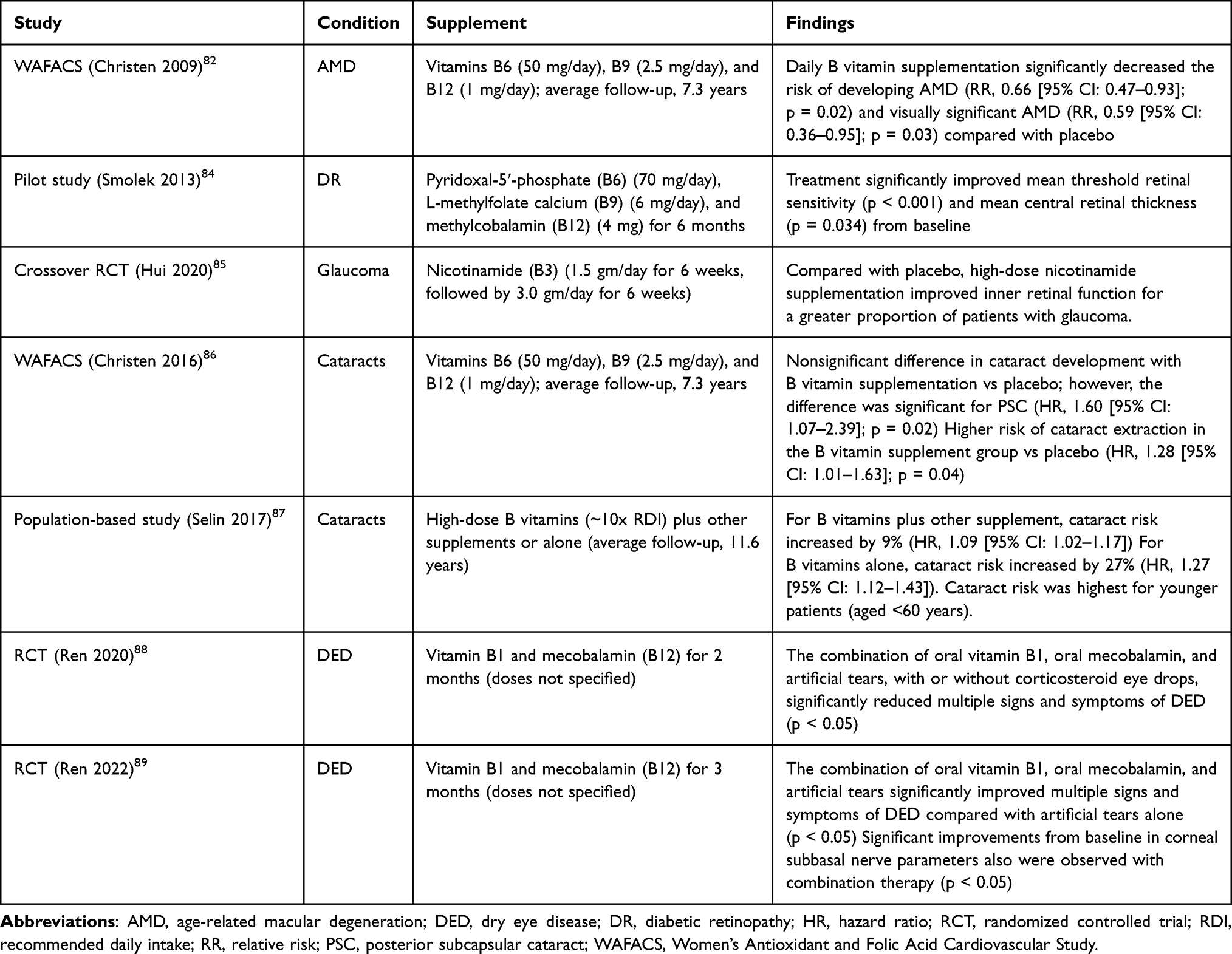 |
Table 3 Studies Evaluating B Vitamin Supplementation in the Development or Progression of Ocular Diseases |
Taken together, the available evidence supports the continued exploration of B vitamin supplementation, particularly with vitamins B6, B9, and B12, for the prevention of AMD development and progression. It is worth noting that existing vitamin formulations for preventing AMD progression, AREDS and AREDS2, do not contain B vitamins. Given the evidence of benefit, augmenting an AREDS formulation with a B vitamin combination such as the one used in WAFACS (which includes higher doses of select B vitamins than typical over-the-counter B vitamin supplements) merits study.
Diabetic Retinopathy
Associations between dietary intake or serum concentrations of several B vitamins and diabetic retinopathy have been identified, although the data are, at times, conflicting (Table 2).28,32,56–60 Using data from a nationwide cohort of patients in Japan aged 40 to 70 years who had type 2 diabetes (N=978), Horikawa et al57 detected an inverse correlation between dietary intake of vitamin B6 and risk of diabetic retinopathy. The hazard ratio (HR) for developing diabetic retinopathy was 0.50 (95% CI: 0.30–0.85; p = 0.010) for patients in the highest versus lowest quartile of vitamin B6. In subgroup analyses, the association of vitamin B6 intake and diabetic retinopathy was maintained for men and for patients with lower glycated hemoglobin (HbA1c) but not for women or younger patients. Significantly lower risk of diabetic retinopathy with higher dietary intake of vitamin B6 also was reported by Ruan et al56 using data from the US-based NHANES 2005–2008 (N=5559). These data further revealed an association between higher dietary vitamin B6 intake and lower risk of all-cause and CVD-related death, as well as lower dietary intake of vitamin B12 in patients with versus without diabetic retinopathy. A meta-analysis that assessed only vitamin B12 reported that serum concentrations were significantly lower in patients with diabetic retinopathy and type 2 diabetes than in patients with type 2 diabetes without retinopathy (p < 0.0001).59 This finding was echoed in a subsequent case-control study (N=100), which additionally demonstrated a negative linear correlation between serum vitamin B12 and serum homocysteine concentrations.32 In a small study of consecutively recruited patients from a single center (N=231), concentrations of vitamin B9 from plasma and from red blood cells were significantly lower in patients with diabetic retinopathy compared with controls (p < 0.001), and there was an inverse correlation between diabetic retinopathy severity and vitamin B9 concentration.28 Similar findings were reported for thiamine pyrophosphate, a derivative of vitamin B1, in a small cross-sectional study (N=80).58
In contrast with the data above, a single-center, retrospective study (N=637) reported higher serum concentrations of vitamin B9 in patients with moderate nonproliferative diabetic retinopathy compared with controls and also indicated serum vitamin B12 concentrations did not differ between patients with versus without diabetic retinopathy.60 In addition, analysis of NHANES 2003–2018 data (N=4595) failed to detect a significant difference in dietary intake of any B vitamins in patients with self-reported, diabetes-related “eye affliction or retinopathy” and controls after adjustment for covariates.90
Evidence Supporting B Vitamin Supplementation in Diabetic Retinopathy
Oral B vitamin supplementation has not been widely studied in the prevention or treatment of diabetic retinopathy. However, data from preclinical studies have revealed multiple positive effects of B vitamin exposure/treatment. For example, vitamin B1 protected cells of the inner blood-retinal barrier from metabolic dysregulation resulting from a diabetes-like microenvironment,91 and the vitamin B1 derivative thiamine pyrophosphate ameliorated hyperglycemia-induced retinopathy in a murine model.92 Nicotinamide (vitamin B3) diminished retinal neurodegeneration in an animal model of diabetes.93 Vitamin B9 prevented retinal thinning and reduced markers of angiogenesis, inflammation, and oxidative stress in a mouse model of diabetes94 and protected retinal vascular endothelial cells from damage generated by a high-glucose environment.95 Dietary vitamin B12 supplementation at least partially prevented retinal thinning; diabetic gliosis; overexpression of hypoxia, vascular permeability, and endoplasmic reticulum stress markers; and apoptosis in the retina in a rat model of diabetes.96
A small open-label, single-arm pilot study treated 10 patients with mild to moderate nonproliferative diabetic retinopathy with a supplement containing pyridoxal-5ʹ-phosphate (vitamin B6), L-methylfolate (vitamin B9), and methylcobalamin (vitamin B12) for 6 months (Table 3).84 Significant improvements from baseline were observed in mean threshold retinal sensitivity (p < 0.001) and mean central retinal thickness (p = 0.034). Although the study was small and uncontrolled, the positive outcomes warrant further study in a larger clinical trial.
Glaucoma
Although there have been individual studies connecting dietary intake or serum concentrations of B vitamins with glaucoma development,61–66,68–71,97 results from meta-analyses are generally equivocal or do not support an association (Table 2).33,35,67,98,99 However, the 2024 meta-analysis from Nicola et al67 reported significantly lower dietary intake of vitamin B3 in patients with glaucoma compared with controls. These data are consistent with findings reported by Kouassi Nzoughet et al68 of lower median vitamin B3 plasma concentration in patients with POAG (N=34) versus controls (N=30), and with data from NHANES 2005–2008 (N=5371) demonstrating that each 1-mg increase in dietary vitamin B3 intake decreased glaucoma risk by 6%.62 Nonetheless, a 2024 report from the Korean National Health and Nutrition Examination Survey (KNHANES) 2017–2018 (N=4195) found significantly higher dietary intake of vitamin B3 in adults aged 60 years and older with glaucoma compared with controls (p = 0.046).69 These discrepancies may indicate that factors within the population influence the determinative value of vitamin B3 for glaucoma risk.
Interestingly, studies have reported differences in associations between B vitamins and glaucoma according to sex, age, and/or BMI.62,63,65,66,70 Using data from KNHANES 2008–2012 data (N=16,770), Jung et al65 detected lower dietary intake of vitamin B1 in patients with glaucoma versus controls for women, but not for men. Associations between low dietary intake of vitamins B1, B2, and B3 and POAG were found to be influenced by BMI and sex, and significant associations between serum vitamin B9 concentration and glaucoma risk were apparent for women and for patients aged <60 years, but not men or older patients.66,70 Similarly, data from the US-based NHANES 2005–2008 (N=5371) revealed that with every 1-mg increase in dietary vitamin B3 intake, an 11% decrease in glaucoma risk in women was observed, but the risk of glaucoma in men was not lowered.62 A subsequent NHANES 2005–2008 analysis found lower self-reported glaucoma prevalence with relatively higher reported vitamin B1 and B12 intake in the overall study population, and with higher vitamin B1 and B2 intake for men.63 Based on International Society Geographical and Epidemiological Ophthalmology (ISGEO) glaucoma criteria, the risk in men was significantly reduced among those in the third quartile of B6 intake. For women, a nonlinear relationship was observed between vitamins B2 and B9 intake and glaucoma risk. These differences based on patient demographics may have influenced the ability to detect overall associations between B vitamins and glaucoma risk, which is reflected in the meta-analysis outcomes.
One study observed increased risk of glaucoma with high-dose intake of vitamin B12. The 2023 analysis of data from NHANES conducted by Liu et al71 assessed dietary intake of vitamin B12 in participants aged 40 years and older who had undergone retinal imaging (N=594). Significant differences in vitamin B12 intake between patients with and without glaucoma (mean vitamin B12 intake: 5.9 vs 4.8 mg; p = 0.033) were observed. After parsing participants by glaucoma presence or absence and dividing patients into quartiles of vitamin B12 intake, low or normal vitamin B12 intake was not associated with glaucoma. However, patients in the highest quartile of dietary vitamin B12 intake, which was considered high-dose intake, were at increased risk for developing glaucoma. As an outlier compared with results from the other studies, replication of these findings is important to determining whether vitamin B12 truly has an adverse effect on glaucoma risk.
B Vitamin Supplementation for Prevention of Glaucoma Development or Progression
Nicotinamide (vitamin B3) exerts multiple beneficial effects that may be neuroprotective in glaucoma, including replenishing NAD+ (which supports mitochondrial function), regulating calcium homeostasis, and reducing oxidative stress.100,101 Interest in nicotinamide for the prevention and treatment of glaucoma was energized by preclinical evidence demonstrating that treatment with nicotinamide protected glaucoma-prone mice from retinal ganglion cell soma or axonal loss, retinal nerve fiber layer thinning, optic nerve degeneration, and early molecular signs of glaucoma.20,102 Nicotinamide was effective when administered either at an age prior to when intraocular pressure elevation was likely to be present or once chronic intraocular pressure elevation was established, and prevented age-related decline in RNA transcripts for NAD-producing enzymes in retinal ganglion cells.20,103
The clinical proof-of-concept came from a crossover, randomized, double-masked clinical trial that assessed the effect of high-dose nicotinamide (vitamin B3) versus placebo on inner retinal function in patients with glaucoma (N=57) (Table 3).85 Nicotinamide treatment was initiated at 1.5 g/day for the first 6 weeks, then increased to 3 g/day for another 6 weeks. After 12 weeks of treatment, a greater proportion of patients in the nicotinamide group experienced improvement in inner retinal functioning compared with placebo. Although high-dose nicotinamide was well tolerated in this study, concerns regarding hepatotoxicity and painful flushing with high-dose nicotinamide led investigators in a subsequent study to treat patients with nicotinamide riboside rather than nicotinamide.104 Outcomes from this study have yet to be published.
Multiple ongoing clinical trials are evaluating nicotinamide, nicotinamide riboside, or nicotinamide and pyruvate for neuroprotection in glaucoma (ClinicalTrials.gov identifiers: NCT05275738, NCT05405868, NCT05695027, NCT06078605, NCT06333236).105,106 The results from these studies will provide more definitive evidence regarding the role of vitamin B3 supplementation for preventing disease progression in glaucoma.
Cataracts
Dietary intake and circulating concentrations of B vitamins have not been as well studied in cataract as they have in AMD and glaucoma. Nonetheless, inverse associations between dietary intake or serum concentrations and cataract risk have been observed for vitamins B1, B2, B3, B6, B9, and B12 (Table 2).23,72–74 There are a couple notable exceptions in which high dietary B vitamin intake was shown to increase cataract risk in particular subpopulations. Data from the AREDS study demonstrated an inverse association between dietary intake of vitamins B2, B6, and B12 and cataract risk for the overall population; however, among study participants who received a standardized daily multivitamin-mineral supplement, risk for development of at least mild posterior subcapsular cataract (PSC) was shown to increase by 61% in those with the highest versus the lowest intake of vitamin B9 (p = 0.02).72 No such association was found among supplement nonusers. Data from KNHANES supported decreased risk of cataract with increased dietary intake of vitamin B1 among men, whereas in women, higher dietary intake of vitamin B2 was associated with increased cataract incidence.73 Additional studies are needed to more fully understand associations between B vitamins and cataract risk in different patient populations.
B Vitamin Supplementation for Cataract Prevention
Preliminary evidence from preclinical studies suggests there is potential for B vitamin supplementation in the treatment of cataract. Riboflavin (vitamin B2) alleviated lens opacity in in vitro models of autophagy-related cataract,107 and nicotinamide (vitamin B3) supported lens epithelial cell survival, positively affected lens fiber cell differentiation and arrangement, and decreased lens-related apoptosis in an in vitro lens regeneration model.108
Data from the WAFACS clinical trial, which we previously described in the context of AMD, also were used to evaluate the role of B vitamin supplementation on cataract prevention (Table 3).86 This analysis included 1969 women without cataract at baseline who were randomized to a supplement containing vitamins B6 (50 mg/day), B9 (2.5 mg/day; in the form of folic acid), and B12 (1 mg/day) and 1956 who were randomized to placebo. During the follow-up period, women treated with the B vitamin supplement experienced a statistically nonsignificant 10% higher risk of cataract compared with the placebo group (HR, 1.10 [95% CI: 0.90–1.33]). The increased risk was significant for PSC (HR, 1.60 [95% CI: 1.07–2.39]; p = 0.02) but not for nuclear sclerosis cataract or any cortical cataract. A 28% higher risk for cataract extraction also was observed in the B vitamin supplementation group compared with placebo (HR, 1.28 [95% CI: 1.01–1.63]; p = 0.04). The authors speculated that the dose of B vitamins used in WAFACS may have been too high for cataract prevention and postulated that increased nitric oxide bioavailability could explain the disparate results in WAFACS for AMD versus cataract. Interestingly, a prospective, population-based study reported increased cataract diagnosis and/or extraction risk (8395 cases) with high-dose B vitamin supplements (10 times the recommended daily intake [RDI] for a B vitamin complex or 25 times the RDI for single B vitamin supplements).87 For patients taking B vitamins plus other supplements, the risk increased by 9% (HR, 1.09 [95% CI: 1.02–1.17), and for those taking B vitamins alone, the risk increased by 27% (HR, 1.27 [95% CI: 1.12–1.43]). For patients taking B vitamins alone, cataract risk was highest for younger patients (aged <60 years). Additional studies are needed to better understand the role B vitamins play in cataract development and whether there are thresholds of supplementation that confer increased versus decreased risk.
Dry Eye Disease and Ocular Surface Disorders
Four B vitamins have been linked to DED symptoms: vitamins B1, B2, B9, and B12 (Table 2).17,43 Within a cohort of patients from the Blue Mountains Eye Study who had completed a dry eye questionnaire (N=1528), 13.4% reported experiencing 2 or more dry eye symptoms and 15.6% reported at least 1 moderate-to-severe symptom.17 The likelihood of experiencing more than 2 dry eye symptoms decreased in the third or fourth quartile of dietary intake for vitamins B1 and B12, respectively. Individual symptoms were significantly associated with dietary intake of vitamins B1 (dryness, itchiness, discomfort), B2 (grittiness), B9 (itchiness, discomfort), and B12 (watering) (p < 0.05 for all comparisons). In addition, a retrospective observational study (N=90) demonstrated reduced neuropathic ocular pain in patients with severe DED when vitamin B12 deficiency was corrected through parenteral supplementation.43
In patients with keratoconus (N=100), a condition in which the cornea thins and becomes cone-shaped, a small, cross-sectional study reported that mean vitamin B2 concentration in blood was significantly lower than in healthy individuals (N=200; p < 0.001).109 No significant differences were observed between cases and controls in blood concentrations of homocysteine and vitamins B9 or B12.
B Vitamin Supplementation and Ocular Surface Disorders
Dry eye disease is often caused by Meibomian gland dysfunction, which increases in prevalence with age.22,110 In preclinical studies, increasing NAD+ bioavailability through topical administration of the vitamin B3 vitamers NMN and nicotinamide riboside restored Meibomian gland activity.110 In vitro exposure to NMN had previously been shown to improve cell viability in corneal epithelial cells subject to hyperosmotic stress, a pathogenic process putatively linked to DED.111 A recent study found that in vitro exposure of corneal epithelial cells to an ophthalmic solution containing vitamin B12 and sodium hyaluronate significantly ameliorated oxidative and inflammatory damage caused by hydrogen peroxide and ultraviolet radiation.112 The solution also accelerated corneal epithelial cell wound healing.
Ocular surface damage (including corneal epithelial squamous metaplasia and abnormal or delayed wound healing that can lead to epithelial erosion, corneal ulcers, and corneal perforation) also is observed in the context of diabetes mellitus.113 Administration of NMN to corneal epithelial cells exposed to a high-glucose environment intended to replicate hyperglycemia-induced damage resulted in improved cell viability, migratory capacity, and tight junctions and a reduction in apoptosis and cellular senescence.113
Clinical studies have explored treatment of DED using both topical and oral B vitamin preparations.88,89,114–116 In this section, we will discuss 2 randomized controlled clinical trials of oral vitamin B supplementation (Table 3).88,89 In the first study, 76 patients with DED were randomized to 2-month treatment with 1 of 4 regimens: artificial tears alone (group 1); corticosteroid eye drops and artificial tears (group 2); oral vitamin B1, oral mecobalamin (vitamin B12), and artificial tears (group 3); and oral vitamin B1, oral mecobalamin, artificial tears, and corticosteroid eye drops (group 4).88 Patients who received B vitamin supplementation (groups 3 and 4) experienced significant improvements from baseline in dryness, foreign body sensation, burning, photophobia, tear film breakup time first, and corneal nerve fiber density. Patients who received corticosteroid eye drops in addition to artificial tears and B vitamin supplementation also experienced reductions in pain, blurred vision, and total symptom score. In the second study, patients aged 18 to 75 years who had DED were randomized to 3-month treatment with oral vitamin B1, oral mecobalamin, and artificial tears (n=94) or artificial tears alone (n=105).89 Compared with the control group, patients who received B vitamin supplementation experienced greater improvements from baseline in conjunctival congestion score, dryness score, corneal fluorescein staining, blurred vision, photophobia, total symptom score, and Ocular Surface Disease Index (p < 0.05 for all). Moreover, significant improvements from baseline were observed in corneal sub-basal nerve parameters for patients who received B vitamin supplementation but not in the control group. These studies support a role for B vitamin supplementation in the treatment of DED, although studies with a larger treatment duration would be beneficial to gain a full understanding of the potential long-term benefits and risks.
Dietary Sources, Supplementation, and Clinical Implications
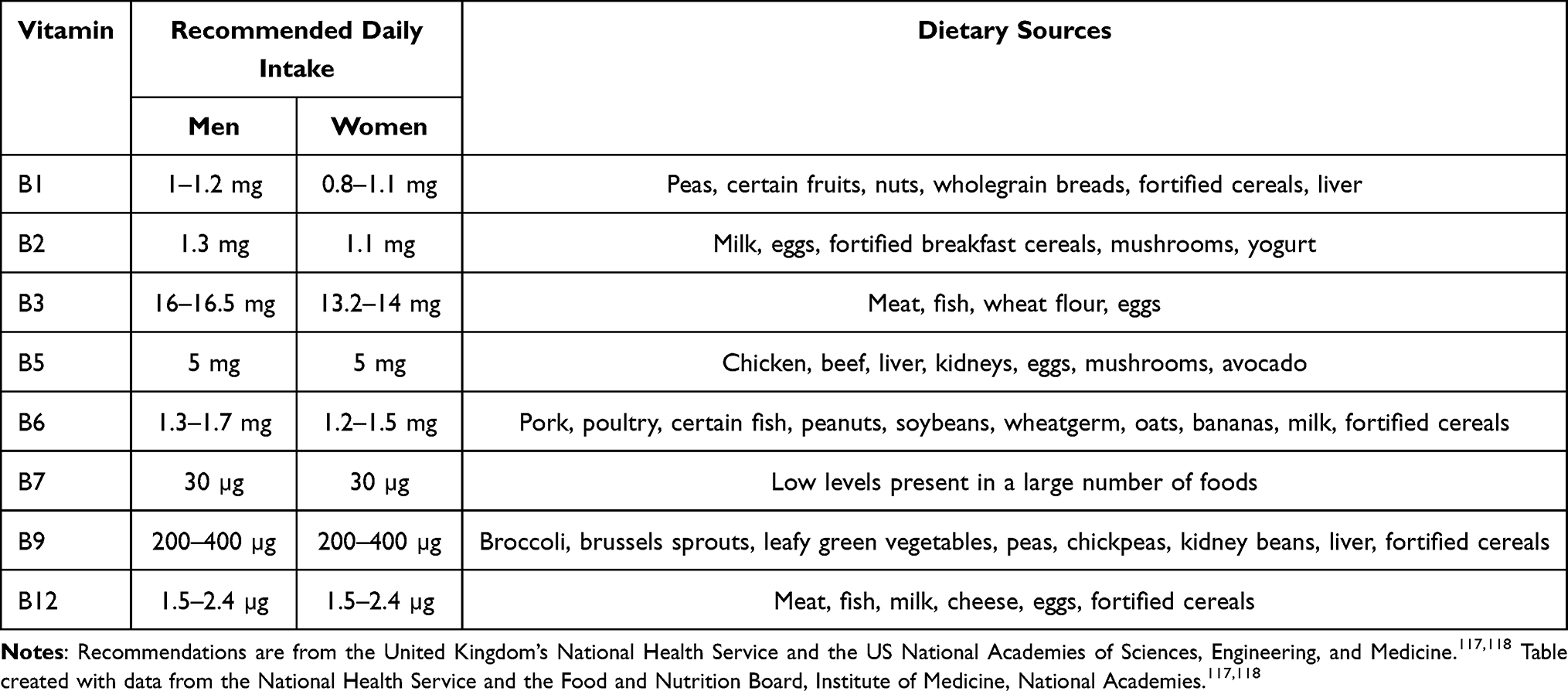
In an effort to maintain sufficient micronutrient intake, governing bodies have established recommended daily intake values; examples for B vitamins are presented in Table 4.117,118 These recommendations are based on population averages and need to be tailored to the individual patient. Vegetarians and vegans, for example, may lack adequate dietary intake of vitamin B12 because most food sources are animal based.119 Similarly, B vitamins may not be absorbed as readily from dietary sources for patients who have had bariatric surgery (vitamins B1 and B12) and older individuals (vitamin B12), thus, requiring supplementation.9,118,120 Micronutrient intake also may be insufficient in patients with autism spectrum disorder due to food aversions and preferences.121 Further, some chronic medications can deplete vitamin B levels over time (eg, proton pump inhibitors, H2-receptor antagonists, metformin, antiepileptic drugs, furosemide) and monitoring of blood levels may be advisable.122 Adequate intake of B vitamins can be achieved through consumption of foods that are high in B vitamins (Table 4), use of dietary supplements, and intake of foods that have been fortified with B vitamins. For the latter, the most ubiquitously applied example is folic acid (vitamin B9) fortification, which was first instituted in Oman almost 30 years ago; many countries followed this practice thereafter to reduce the occurrence of neural tube defects in infants.123 Food fortification rules vary by country, and may include B vitamins in addition to vitamin B9.
 |
Supplementation Strategies in Ocular Diseases
The influence of micronutrient consumption and dietary supplementation is recognized by professional society guidelines as having potential for the prevention or treatment of AMD, cataract, and glaucoma.124–126 Based on evidence from AREDS2, the American Academy of Ophthalmology (AAO) recommends considering supplementation with antioxidant vitamins and minerals in patients with intermediate AMD or who have geographic atrophy in 1 or both eyes and other advanced AMD in 1 eye.124 The National Eye Institute (NEI)‒recommended AREDS2 formulation consists of vitamin C (500 mg), vitamin E (400 IU), lutein/zeaxanthin (10 mg/2 mg), zinc oxide (80 mg), and cupric oxide (2 mg).124,127 The AAO also notes that the Mediterranean diet is associated with lower risk of AMD development and progression. The guidance for cataract and glaucoma is more general. The AAO acknowledges that there is moderate evidence to support multivitamin/mineral supplements to reduce cataract risk,125 and the American Optometric Association notes that B vitamins have “theoretical promise for the treatment of glaucoma or concomitant ocular surface disease”.126 Limitations of the available evidence pose a barrier to stronger or more specific recommendations for dietary supplementation.
The idiom “the more, the better” does not apply to vitamin supplementation. As with other micronutrients, B vitamins can have deleterious effects when used at higher than recommended doses. Niacin (vitamin B3) at doses of more than 3 g/day can be toxic, causing ocular (macular edema, macular cysts) and systemic side effects (flushing, hyperglycemia, hyperuremia, liver toxicity).9,128 A 2025 position statement on nicotinamide use for glaucoma neuroprotection issued jointly by the American Glaucoma Society (AGS) and AAO cautions that “nicotinamide is not approved for glaucoma and its safety is unknown”.106 The statement does not recommend use of nicotinamide at doses of 3 g/day or higher, and further, even for doses <3 g/day, the statement advocates for collaboration with a patient’s primary care physician and periodic liver function testing. High-dose (≥100 mg/day) exposure is also a concern with vitamin B6 due to the potential for peripheral neuropathy.9 Moreover, as noted previously, rather than having a protective effect, high-dose B vitamin supplementation (10x RDI for a B vitamin complex or 25x RDI for single B vitamin supplements) was associated with increased cataract risk in a population-based, prospective study.87
The form of the B vitamin also must be considered when used for supplementation. Vitamin B3 has 3 primary vitamers: niacin (aka nicotinic acid), nicotinamide (aka niacinamide), and nicotinamide riboside.129 Niacin and nicotinamide are the common forms used in supplements. Although nicotinamide does not have the cholesterol-lowering properties of niacin, it offers the benefit of a more favorable safety and tolerability profile.106,129 The AGS-AAO position statement strongly cautions against substituting niacin in place of nicotinamide for glaucoma neuroprotection.106 Nicotinamide riboside is not as widely used in supplements as niacin and nicotinamide, but may offer the advantage of greater oral bioavailability than nicotinamide and is well tolerated.104 For these reasons, nicotinamide riboside rather than other vitamin B3 forms is being used in an ongoing randomized controlled trial as a potential neuroprotective therapy in patients with glaucoma.104 Folic acid, a synthetic form of vitamin B9, is most commonly used in the context of food fortification and supplements. Folic acid does not naturally occur in food sources; is more biologically active than the naturally occurring form, methylfolate; and is slowly metabolized, raising concern about long-term exposure.130 Moreover, high levels of vitamin B9 can mask vitamin B12 deficiency, thereby delaying its identification, potentially past the point where symptoms are reversible.9,24,131 Multiple B12 vitamers (eg, hydroxocobalamin, methylcobalamin, and 5ʹ-deoxyadenosylcobalamin) are used in food fortification and supplements, the most common of which is cyanocobalamin, a synthetic variant.119 Whether these various B vitamin forms have unique effects or differences in efficacy, safety, and tolerability in the context of ocular health remains to be determined.
Gaps in Current Knowledge and Future Research Directions
Developing evidence-based best practices for the use of B vitamin supplementation to maintain optimal eye health and prevent the development or progression of ocular disease requires additional research to fill current knowledge gaps. For example, according to data on dietary intake of B vitamins, demographic or clinical factors may influence results, and these need to be explored to better tailor treatment to the individual patient. Overall, there is a lack of evidence to guide personalized nutrition in the context of ocular diseases, including studies evaluating genetic differences in the effects of B vitamin supplementation.15 As shown in Table 3, clinical trial data for supplements containing a single B vitamin or combinations of B vitamins are limited. Most of the larger supplement clinical trials have involved combinations of multiple vitamins/minerals.78–81 In addition, few of the clinical trials have used the same supplement, and none of the cited studies explored different dosing regimens. Therefore, the optimal dosing regimen for any particular supplement or condition has yet to be determined. For vitamins such as B3, there are multiple vitamer options available, and it remains to be determined whether the clinical effects will be generally similar regardless of the vitamer used or whether particular forms are better suited to particular clinical uses. Lastly, clinical studies are needed to assess the benefits and risks of long-term B vitamin supplementation.
From a clinical practice standpoint, a process for identifying patients who would benefit from nutritional intervention is needed. As suggested by the epidemiologic data, increased ocular disease risk does not require vitamin levels low enough to qualify as clinically deficient. Nonetheless, B vitamin concentrations in the low-but-still-normal range may go undetected in routine clinical practice because they are unlikely to produce overt symptoms and are not typically measured in the absence of clinical indicators of vitamin insufficiency. Clinicians and researchers should consider how best to implement B vitamin supplementation while clinical studies are evaluating its efficacy and safety in the prevention and treatment of ocular disease.
Conclusion
B vitamins play important roles in a range of physiologic processes that are essential for optimal eye health. They are integral to ocular structure and function, and their deficiency has significant clinical ramifications. The available evidence suggests increased risk of multiple eye diseases, including AMD, diabetic retinopathy, glaucoma, cataracts, and DED, with low intake or circulating concentrations of B vitamins. Preclinical data and clinical studies indicate that B vitamin supplementation can be beneficial for the prevention of ocular disease development and/or progression. Nonetheless, there is a need to identify optimal dosing regimens based on the clinical context and to evaluate long-term safety and efficacy in clinical trials. For clinicians, B vitamin supplementation may offer another tool through which they can protect their patients’ vision and maintain their eye health.
Abbreviations
AAO, American Academy of Ophthalmology; AGS, American Glaucoma Society; AMD, age-related macular degeneration; AREDS, Age-Related Eye Disease Study; BMI, body mass index; CVD, cardiovascular disease; DED, dry eye disease; DR, diabetic retinopathy; HR, hazard ratio; KNHANES, Korean National Health and Nutrition Examination Survey; MTHFR, methylenetetrahydrofolate reductase; NAD, nicotinamide adenine dinucleotide; NHANES, National Health and Nutrition Examination Survey; NMN, nicotinamide mononucleotide; NTG, normal-tension glaucoma; POAG, primary open-angle glaucoma; PSC, posterior subcapsular cataract; RCT, randomized controlled trial; RDI, recommended daily intake; ROS, reactive oxygen species; RR, relative risk; WAFACS, Women’s Antioxidant and Folic Acid Cardiovascular Study.
Data Sharing Statement
Data sharing is not applicable to this article, as no datasets were generated or analyzed during the current study.
Acknowledgments
Editorial and medical writing support was provided by Crystal Murcia, PhD, and Pratibha Hebbar, PhD, of Synchrony Medical Communications, LLC, and was funded by Bausch + Lomb.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The manuscript was written independently by the authors, with medical writing and editorial assistance funded by Bausch + Lomb. The authors declared they have not been influenced in any way and at any time by Bausch + Lomb concerning the content of the manuscript.
Disclosure
Elizabeth J Johnson has nothing to report relating to this work. Julie Poteet reports serving as occasional consultant and advisory board committee member for Bausch + Lomb. Neda Gioia reports serving as occasional consultant and advisory board committee member for Bausch + Lomb. Richard R L Maharaj reports serving as occasional consultant and advisory board committee member for Bausch + Lomb. He also reports personal fees from Sun Pharma, Théa Pharma Inc, Labtician Ophthalmics, Inc, and Bausch & Lomb, outside the submitted work. Jose Manuel Benitez-del-Castillo reports serving as occasional consultant for Alcon, Allergan, Bausch + Lomb, DMG, Dompé, GSK, HorusPharma, MSD, Novartis, Quantel, Santen, Shire, Sifi, Topivert, and Théa. Marc Labetoulle reports serving as occasional consultant for Abbvie, Alfa Intes, Biotest, KOL, Marinomed, Nordic, Pol Pharma, Alcon, Allergan, Bausch + Lomb, DMG, Dompe, GSK, HorusPharma, MSD, Novartis, Quantel, Santen, Shire, Sifi, Topivert, and Théa. The authors report no other conflicts of interest in this work.
References
1. Semba RD. The discovery of the vitamins. Int J Vitam Nutr Res. 2012;82(5):310–19. doi:10.1024/0300-9831/a000124
2. Burton MJ, Ramke J, Marques AP, et al. The Lancet Global Health Commission on Global Eye Health: vision beyond 2020. Lancet Glob Health. 2021;9(4):e489–e551. doi:10.1016/S2214-109X(20)30488-5
3. Raman R, Vaghefi E, Braakhuis AJ. Food components and ocular pathophysiology: a critical appraisal of the role of oxidative mechanisms. Asia Pac J Clin Nutr. 2017;26(4):572–585. doi:10.6133/apjcn.082016.01
4. Murkey SP, Agarwal A, Pandit P, Kumar S, Jaiswal A. Unveiling the spectrum of ophthalmic manifestations in nutritional deficiencies: a comprehensive review. Cureus. 2023;15(12):e50311. doi:10.7759/cureus.50311
5. Ruamviboonsuk V, Grzybowski A. The roles of vitamins in diabetic retinopathy: a narrative review. J Clin Med. 2022;11(21):6490. doi:10.3390/jcm11216490
6. Rondanelli M, Gasparri C, Riva A, et al. Diet and ideal food pyramid to prevent or support the treatment of diabetic retinopathy, age-related macular degeneration, and cataracts. Front Med (Lausanne). 2023;10:1168560. doi:10.3389/fmed.2023.1168560
7. Kaufman MW, DeParis S, Oppezzo M, et al. Nutritional supplements for healthy aging: a critical analysis review. Am J Lifestyle Med. 2025;19(3):346–360. doi:10.1177/15598276241244725
8. Pereira A, Adekunle RD, Zaman M, Wan MJ. Association between vitamin deficiencies and ophthalmological conditions. Clin Ophthalmol. 2023;17:2045–2062. doi:10.2147/OPTH.S401262
9. Hanna M, Jaqua E, Nguyen V, Clay J. B vitamins: functions and uses in medicine. Perm J. 2022;26(2):89–97. doi:10.7812/TPP/21.204
10. Cimaglia G, Votruba M, Morgan JE, André H, Williams PA. Potential therapeutic benefit of NAD+ supplementation for glaucoma and age-related macular degeneration. Nutrients. 2020;12(9):2871. doi:10.3390/nu12092871
11. Petriti B, Williams PA, Lascaratos G, Chau KY, Garway-Heath DF. Neuroprotection in glaucoma: NAD(+)/NADH redox state as a potential biomarker and therapeutic target. Cells. 2021;10(6):1402. doi:10.3390/cells10061402
12. Udhayabanu T, Manole A, Rajeshwari M, Varalakshmi P, Houlden H, Ashokkumar B. Riboflavin responsive mitochondrial dysfunction in neurodegenerative diseases. J Clin Med. 2017;6(5):52. doi:10.3390/jcm6050052
13. Marrs C, Lonsdale D. Hiding in plain sight: modern thiamine deficiency. Cells. 2021;10(10):2595. doi:10.3390/cells10102595
14. Kowalczyk P, Sulejczak D, Kleczkowska P, et al. Mitochondrial oxidative stress-a causative factor and therapeutic target in many diseases. Int J Mol Sci. 2021;22(24):13384. doi:10.3390/ijms222413384
15. Mukhtar S, Ambati BK. The value of nutritional supplements in treating age-related macular degeneration: a review of the literature. Int Ophthalmol. 2019;39(12):2975–2983. doi:10.1007/s10792-019-01140-6
16. Elsherbiny NM, Sharma I, Kira D, et al. Homocysteine induces inflammation in retina and brain. Biomolecules. 2020;10(3):393. doi:10.3390/biom10030393
17. Guo B, Gopinath B, Watson S, Burlutsky G, Mitchell P, Ooi K. Associations between intake of dietary micro- and macro-nutrients with dry eye syndrome: Blue Mountains Eye Study. Clin Nutr ESPEN. 2023;54:258–263. doi:10.1016/j.clnesp.2023.01.019
18. Seddon JM, Gensler G, Klein ML, Milton RC. C-reactive protein and homocysteine are associated with dietary and behavioral risk factors for age-related macular degeneration. Nutrition. 2006;22(4):441–443. doi:10.1016/j.nut.2005.12.004
19. Baltrusch S. The role of neurotropic B vitamins in nerve regeneration. Biomed Res Int. 2021;2021:9968228. doi:10.1155/2021/9968228
20. Williams PA, Harder JM, Foxworth NE, et al. Vitamin B3 modulates mitochondrial vulnerability and prevents glaucoma in aged mice. Science. 2017;355:6326):756–760. doi:10.1126/science.aal0092
21. Ebeling MC, Polanco JR, Qu J, Tu C, Montezuma SR, Ferrington DA. Improving retinal mitochondrial function as a treatment for age-related macular degeneration. Redox Biol. 2020;34:101552. doi:10.1016/j.redox.2020.101552
22. Seen S, Tong L. Dry eye disease and oxidative stress. Acta Ophthalmol. 2018;96(4):e412–e420. doi:10.1111/aos.13526
23. Luo J, Chen X, Yang Y, Liu Y, Feng Y, Chen G. Association of MTHFR C667T polymorphism, homocysteine, and B vitamins with senile cataract. J Nutr Sci Vitaminol (Tokyo). 2023;69(2):136–144. doi:10.3177/jnsv.69.136
24. Gu J, Lei C, Zhang M. Folate and retinal vascular diseases. BMC Ophthalmol. 2023;23(1):413. doi:10.1186/s12886-023-03149-z
25. Yuan S, Mason AM, Carter P, Burgess S, Larsson SC. Homocysteine, B vitamins, and cardiovascular disease: a Mendelian randomization study. BMC Med. 2021;19(1):97. doi:10.1186/s12916-021-01977-8
26. Huang P, Wang F, Sah BK, et al. Homocysteine and the risk of age-related macular degeneration: a systematic review and meta-analysis. Sci Rep. 2015;5:10585. doi:10.1038/srep10585
27. Rodrigo F, Ruiz-Moreno JM, García JB, Torregrosa ME, Segura JV, Piñero DP. Color Doppler imaging of the retrobulbar circulation and plasmatic biomarkers of vascular risk in age-related macular degeneration: a pilot study. Indian J Ophthalmol. 2018;66(1):89–93. doi:10.4103/ijo.IJO_488_17
28. Malaguarnera G, Gagliano C, Salomone S, et al. Folate status in type 2 diabetic patients with and without retinopathy. Clin Ophthalmol. 2015;9:1437–1442. doi:10.2147/OPTH.S77538
29. Srivastav K, Saxena S, Mahdi AA, et al. Increased serum level of homocysteine correlates with retinal nerve fiber layer thinning in diabetic retinopathy. Mol Vis. 2016;22:1352–1360.
30. Lei X, Zeng G, Zhang Y, et al. Association between homocysteine level and the risk of diabetic retinopathy: a systematic review and meta-analysis. Diabetol Metab Syndr. 2018;10:61. doi:10.1186/s13098-018-0362-1
31. Tomić M, Vrabec R, Ljubić S, Bulum T, Rahelić D. Plasma homocysteine is associated with nonproliferative retinopathy in patients with type 2 diabetes without renal disease. Diab Metab Syndr. 2022;16(1):102355. doi:10.1016/j.dsx.2021.102355
32. Debnath PR, Debnath DK, Haque AF, Mohammuddunnobi M, Bhowmik NC. Role of vitamin B12 deficiency and hyperhomocysteinemia in diabetic retinopathy. Mymensingh Med J. 2023;32(2):459–462.
33. Li W, Pan J, Wei M, et al. Nonocular influencing factors for primary glaucoma: an umbrella review of meta-analysis. Ophthalmic Res. 2021;64(6):938–950. doi:10.1159/000519247
34. Dong N, Shi H, Tang X. Plasma homocysteine levels are associated with macular thickness in type 2 diabetes without diabetic macular edema. Int Ophthalmol. 2018;38(2):737–746. doi:10.1007/s10792-017-0528-0
35. Li J, Xu F, Zeng R, Gong H, Lan Y. Plasma homocysteine, serum folic acid, serum vitamin B12, serum vitamin B6, MTHFR, and risk of normal-tension glaucoma. J Glaucoma. 2016;25(2):e94–e98. doi:10.1097/IJG.0000000000000269
36. Leibovitzh H, Cohen E, Levi A, et al. Relationship between homocysteine and intraocular pressure in men and women: a population-based study. Medicine. 2016;95(38):e4858. doi:10.1097/MD.0000000000004858
37. Christen WG, Cook NR, Ridker PM, Buring JE. Prospective study of plasma homocysteine level and risk of age-related macular degeneration in women. Ophthalmic Epidemiol. 2015;22(2):85–93. doi:10.3109/09286586.2015.1012272
38. Christen WG, Cook NR, Chiuve SE, Ridker PM, Gaziano JM. Prospective study of plasma homocysteine, its dietary determinants, and risk of age-related macular degeneration in men. Ophthalmic Epidemiol. 2018;25(1):79–88. doi:10.1080/09286586.2017.1362009
39. Bucolo C, Maugeri G, Giunta S, D’Agata V, Drago F, Romano GL. Corneal wound healing and nerve regeneration by novel ophthalmic formulations based on cross-linked sodium hyaluronate, taurine, vitamin B6, and vitamin B12. Front Pharmacol. 2023;14:1109291. doi:10.3389/fphar.2023.1109291
40. Nassiri N, Assarzadegan F, Shahriari M, et al. Vitamin B12 deficiency as a cause of neurotrophic keratopathy. Open Ophthalmol J. 2018;12:7–11. doi:10.2174/1874364101712010007
41. Beltramo E, Mazzeo A, Porta M. Thiamine and diabetes: back to the future? Acta Diabetol. 2021;58(11):1433–1439. doi:10.1007/s00592-021-01752-4
42. Serhan HA, Alma’aitah HW, Irshaidat S, Ameer MA, Asghar MS, Tahir MJ. Ophthalmic manifestations of nutritional deficiencies: a mini review. J Fam Med Prim Care. 2022;11(10):5899–5901. doi:10.4103/jfmpc.jfmpc_790_22
43. Ozen S, Atabey Ozer M, Orçun akdemir M. Vitamin B12 deficiency evaluation and treatment in severe dry eye disease with neuropathic ocular pain. Graefes Arch Clin Exp Ophthalmol. 2017;255:1173–1177.
44. Tankeu AT, Van Winckel G, Elmers J, et al. Biotinidase deficiency: what have we learned in forty years? Mol Genet Metab. 2023;138(4):107560. doi:10.1016/j.ymgme.2023.107560
45. Gopinath B, Liew G, Russell J, Cosatto V, Burlutsky G, Mitchell P. Intake of key micronutrients and food groups in patients with late-stage age-related macular degeneration compared with age-sex-matched controls. Br J Ophthalmol. 2017;101(8):1027–1031. doi:10.1136/bjophthalmol-2016-309490
46. Nunes S, Alves D, Barreto P, et al. Adherence to a Mediterranean diet and its association with age-related macular degeneration. The Coimbra Eye Study-Report 4. Nutrition. 2018;51–52:6–12. doi:10.1016/j.nut.2017.12.010
47. Šalková Kráľová J, Kolář P, Kapounová Z, Veselý P, Derflerová Brázdová Z. Dietary habits and dietary nutrient intake in patients with age-related macular degeneration: a case-control study. Cent Eur J Public Health. 2023;31(2):140–143. doi:10.21101/cejph.a7617
48. Liu Z, Wang Q, Li L, Cai S. Association between dietary consumption of multiple vitamins and age-related macular degeneration: a cross-sectional observational study in the National Health and Nutrition Examination Survey 2005-2008. Front Nutr. 2024;11:1504081. doi:10.3389/fnut.2024.1504081
49. Gopinath B, Flood VM, Rochtchina E, Wang JJ, Mitchell P. Homocysteine, folate, vitamin B-12, and 10-y incidence of age-related macular degeneration. Am J Clin Nutr. 2013;98(1):129–135. doi:10.3945/ajcn.112.057091
50. Merle BMJ, Silver RE, Rosner B, Seddon JM. Dietary folate, B vitamins, genetic susceptibility and progression to advanced nonexudative age-related macular degeneration with geographic atrophy: a prospective cohort study. Am J Clin Nutr. 2016;103(4):1135–1144. doi:10.3945/ajcn.115.117606
51. Agrón E, Mares J, Clemons TE, et al. Dietary nutrient intake and progression to late age-related macular degeneration in the Age-Related Eye Disease Studies 1 and 2. Ophthalmology. 2021;128(3):425–442. doi:10.1016/j.ophtha.2020.08.018
52. Merle BMJ, Barthes S, Féart C, et al. B vitamins and incidence of advanced age-related macular degeneration: the Alienor Study. Nutrients. 2022;14(14):2821. doi:10.3390/nu14142821
53. Zheng Q, Shen T, Xu M, Tan L, Shen Z, Hong C. Association between dietary consumption of vitamin B1 and advanced age-related macular degeneration: a cross-sectional observational study in NHANES 2005-2008. Ophthalmic Res. 2023;66(1):1353–1361. doi:10.1159/000534819
54. Rochtchina E, Wang JJ, Flood VM, Mitchell P. Elevated serum homocysteine, low serum vitamin B12, folate, and age-related macular degeneration: the Blue Mountains Eye Study. Am J Ophthalmol. 2007;143(2):344–346. doi:10.1016/j.ajo.2006.08.032
55. Agrón E, Vance E, Domalpally A, Chew EY, Keenan TDL. Relationships between diet and geographic atrophy progression in the Age-Related Eye Diseases Studies 1 and 2. Nutrients. 2025;17(5):771. doi:10.3390/nu17050771
56. Ruan Y, Zhang P, Jia X, Hua S, Yao D. Association of vitamin B6 intake with the risk and prognosis of diabetic retinopathy: a NHANES-based study. Clin Exp Optom. 2024;107(8):847–856. doi:10.1080/08164622.2023.2300298
57. Horikawa C, Aida R, Kamada C, et al. Vitamin B6 intake and incidence of diabetic retinopathy in Japanese patients with type 2 diabetes: analysis of data from the Japan Diabetes Complications Study (JDCS). Eur J Nutr. 2020;59(4):1585–1594. doi:10.1007/s00394-019-02014-4
58. Cinici E, Dilekmen N, Senol O, Arpali E, Cinici O, Tanas S. Blood thiamine pyrophosphate concentration and its correlation with the stage of diabetic retinopathy. Int Ophthalmol. 2020;40(12):3279–3284. doi:10.1007/s10792-020-01513-2
59. Yang X, Hu R, Zhu Y, et al. Meta-analysis of serum vitamin B12 levels and diabetic retinopathy in type 2 diabetes. Arch Med Res. 2023;54(1):64–73. doi:10.1016/j.arcmed.2022.12.006
60. Xiao X, Zhao J, Lin S, et al. Relationships between retinal vascular characteristics and systemic indicators in patients with diabetes mellitus. Invest Ophthalmol Vis Sci. 2025;66(4):72. doi:10.1167/iovs.66.4.72
61. Taechameekietichai T, Chansangpetch S, Peerawaranun P, Lin SC. Association between daily niacin intake and glaucoma: National Health and Nutrition Examination Survey. Nutrients. 2021;13(12):4263. doi:10.3390/nu13124263
62. Lee SY, Tseng VL, Kitayama K, et al. Associations between niacin intake and glaucoma in the National Health and Nutrition Examination Survey. J Glaucoma. 2023;32(6):443–450. doi:10.1097/IJG.0000000000002216
63. Hou J, Wen Y, Gao S, Jiang Z, Tao L. Association of dietary intake of B vitamins with glaucoma. Sci Rep. 2024;14(1):8539. doi:10.1038/s41598-024-58526-5
64. Yang Z, Zhang J, Zheng Y. Higher vitamin B6 dietary consumption is associated with a lower risk of glaucoma among United States adults. Front Nutr. 2024;11:1363539. doi:10.3389/fnut.2024.1363539
65. Jung KI, Kim YC, Park CK. Dietary niacin and open-angle glaucoma: the Korean National Health and Nutrition Examination Survey. Nutrients. 2018;10(4):387. doi:10.3390/nu10040387
66. Lee JY, Kim JM, Lee KY, Kim B, Lee MY, Park KH. Relationships between obesity, nutrient supply and primary open angle glaucoma in Koreans. Nutrients. 2020;12(3):878. doi:10.3390/nu12030878
67. Nicola CA, Marinescu MC, Firan AM, et al. Systematic review and meta-analysis on the association between daily niacin intake and glaucoma. Nutrients. 2024;16(21):3604. doi:10.3390/nu16213604
68. Kouassi Nzoughet J, Chao de la Barca JM, Guehlouz K, et al. Nicotinamide deficiency in primary open-angle glaucoma. Invest Ophthalmol Vis Sci. 2019;60(7):2509–2514. doi:10.1167/iovs.19-27099
69. Kim J, Park S, Yang YJ. Comparison of food and nutrient intake according to the presence of glaucoma among Korean older adults. Nutr Res Pract. 2024;18(5):701–710. doi:10.4162/nrp.2024.18.5.701
70. Lee JY, Choi JA, Park SP, Jee D. Association between high blood folate levels and glaucoma in a representative Korean population. Invest Ophthalmol Vis Sci. 2024;65(1):6. doi:10.1167/iovs.65.1.6
71. Liu Z, Hu Y, Wang Y, Xu B, Zhao J, Yu Z. Relationship between high dose intake of vitamin B12 and glaucoma: evidence from NHANES 2005-2008 among United States adults. Front Nutr. 2023;10:1130032. doi:10.3389/fnut.2023.1130032
72. Glaser TS, Doss LE, Shih G, et al. The association of dietary lutein plus zeaxanthin and B vitamins with cataracts in the age-related eye disease study: AREDS Report No. 37. Ophthalmology. 2015;122(7):1471–1479. doi:10.1016/j.ophtha.2015.04.007
73. Lee S, Lee S, Jeong M, Jung S, Lee M, Yoo S. The relationship between nutrient intake and cataracts in the older adult population of Korea. Nutrients. 2022;14(23):4962. doi:10.3390/nu14234962
74. Zhuang G-B, Li X, Wu S-N, Zhang S-Q, Zhang Z-J, Dong N. The impact of vitamin E, vitamin B6, and niacin intake on cataract incidence based on NHANES 2005-2008 data. Front Nutr. 2024;11:1406147. doi:10.3389/fnut.2024.1406147
75. Saini JS, Corneo B, Miller JD, et al. Nicotinamide ameliorates disease phenotypes in a human iPSC model of age-related macular degeneration. Cell Stem Cell. 2017;20(5):635–647. doi:10.1016/j.stem.2016.12.015
76. Ren C, Hu C, Wu Y, et al. Nicotinamide mononucleotide ameliorates cellular senescence and inflammation caused by sodium iodate in RPE. Oxid Med Cell Longev. 2022;2022:5961123. doi:10.1155/2022/5961123
77. Ibuki M, Lee D, Shinojima A, Miwa Y, Tsubota K, Kurihara T. Rice bran and vitamin B6 suppress pathological neovascularization in a murine model of age-related macular degeneration as novel HIF inhibitors. Int J Mol Sci. 2020;21(23):8940. doi:10.3390/ijms21238940
78. Parravano M, Tedeschi M, Manca D, et al. Effects of Macuprev® supplementation in age-related macular degeneration: a double-blind randomized morpho-functional study along 6 months of follow-up. Adv Ther. 2019;36(9):2493–2505. doi:10.1007/s12325-019-01016-2
79. Pameijer EM, Heus P, Damen JAA, et al. What did we learn in 35 years of research on nutrition and supplements for age-related macular degeneration: a systematic review. Acta Ophthalmol. 2022;100(8):e1541–e1552. doi:10.1111/aos.15191
80. D’Aloisio R, Di Antonio L, Toto L, et al. Choroidal changes in blood flow in patients with intermediate AMD after oral dietary supplement based on astaxanthin, bromelain, vitamin D3, folic acid, lutein, and antioxidants. Medicina (Kaunas). 2022;58(8):1092. doi:10.3390/medicina58081092
81. Evans JR, Lawrenson JG. Antioxidant vitamin and mineral supplements for slowing the progression of age-related macular degeneration. Cochrane Database Syst Rev. 2023;9(9):CD000254. doi:10.1002/14651858.CD000254.pub5
82. Christen WG, Glynn RJ, Chew EY, Albert CM, Manson JE. Folic acid, pyridoxine, and cyanocobalamin combination treatment and age-related macular degeneration in women: the Women’s Antioxidant and Folic Acid Cardiovascular Study. Arch Intern Med. 2009;169(4):335–341. doi:10.1001/archinternmed.2008.574
83. Albert CM, Cook NR, Gaziano JM, et al. Effect of folic acid and B vitamins on risk of cardiovascular events and total mortality among women at high risk for cardiovascular disease: a randomized trial. JAMA. 2008;299(17):2027–2036. doi:10.1001/jama.299.17.2027
84. Smolek MK, Notaroberto NF, Jaramillo AG, Pradillo LR. Intervention with vitamins in patients with nonproliferative diabetic retinopathy: a pilot study. Clin Ophthalmol. 2013;7:1451–1458. doi:10.2147/OPTH.S46718
85. Hui F, Tang J, Williams PA, et al. Improvement in inner retinal function in glaucoma with nicotinamide (vitamin B3) supplementation: a crossover randomized clinical trial. Clin Exp Ophthalmol. 2020;48(7):903–914. doi:10.1111/ceo.13818
86. Christen WG, Glynn RJ, Chew EY, Albert CM, Manson JE. Folic acid, vitamin B6, and vitamin B12 in combination and age-related cataract in a randomized trial of women. Ophthalmic Epidemiol. 2016;23(1):32–39. doi:10.3109/09286586.2015.1130845
87. Selin JZ, Lindblad BE, Bottai M, Morgenstern R, Wolk A. High-dose B-vitamin supplements and risk for age-related cataract: a population-based prospective study of men and women. Br J Nutr. 2017;118(2):154–160. doi:10.1017/S0007114517001994
88. Ren X, Chou Y, Jiang X, et al. Effects of oral vitamin B1 and mecobalamin on dry eye disease. J Ophthalmol. 2020;2020:9539674. doi:10.1155/2020/9539674
89. Ren X, Chou Y, Wang Y, Jing D, Chen Y, Li X. The utility of oral vitamin B1 and mecobalamin to improve corneal nerves in dry eye disease: an in vivo confocal microscopy study. Nutrients. 2022;14(18):3750. doi:10.3390/nu14183750
90. Zhang G, Sun X, Yuan T, et al. Certain dietary nutrients reduce the risk of eye affliction/retinopathy in individuals with diabetes: National Health and Nutrition Examination Survey, 2003-2018. Int J Environ Res Public Health. 2022;19(19):12173. doi:10.3390/ijerph191912173
91. Mazzeo A, Gai C, Trento M, Porta M, Beltramo E. Effects of thiamine and fenofibrate on high glucose and hypoxia-induced damage in cell models of the inner blood-retinal barrier. Acta Diabetol. 2020;57(12):1423–1433. doi:10.1007/s00592-020-01565-x
92. Cinici E, Ahiskali I, Cetin N, et al. Effect of thiamine pyrophosphate on retinopathy induced by hyperglycemia in rats: a biochemical and pathological evaluation. Indian J Ophthalmol. 2016;64(6):434–439. doi:10.4103/0301-4738.187666
93. Jung KI, Han J-S, Park CK. Neuroprotective effects of nicotinamide (vitamin B3) on neurodegeneration in diabetic rat retinas. Nutrients. 2022;14(6):1162. doi:10.3390/nu14061162
94. Lei X-W, Li Q, Zhang J-Z, Zhang Y-M, Liu Y, Yang K-H. The protective roles of folic acid in preventing diabetic retinopathy are potentially associated with suppressions on angiogenesis, inflammation, and oxidative stress. Ophthalmic Res. 2019;62(2):80–92. doi:10.1159/000499020
95. Wang Z, Xing W, Song Y, et al. Folic acid has a protective effect on retinal vascular endothelial cells against high glucose. Molecules. 2018;23(9):2326. doi:10.3390/molecules23092326
96. Sreenivasa Reddy S, Prabhakar YK, Uday Kumar C, Yadagiri Reddy P, Bhanuprakash Reddy G. Effect of vitamin B12 supplementation on retinal lesions in diabetic rats. Mol Vis. 2020;26:311–325.
97. Atalay K, Savur FG, Kirgiz A, Kaldırım HE, Zengi O. Serum levels of thyroid hormone, vitamin D, vitamin B12, folic acid, C-reactive protein, and hemoglobin in pseudoexfoliation and primary open angle glaucoma. J Fr Ophtalmol. 2019;42(7):730–738. doi:10.1016/j.jfo.2019.01.002
98. Li S, Li D, Shao M, Cao W, Sun X. Lack of association between serum vitamin B6, vitamin B12, and vitamin D levels with different types of glaucoma: a systematic review and meta-analysis. Nutrients. 2017;9(6):636. doi:10.3390/nu9060636
99. Ramdas WD, Schouten JSAG, Webers CAB. The effect of vitamins on glaucoma: a systematic review and meta-analysis. Nutrients. 2018;10(3):359. doi:10.3390/nu10030359
100. Wang LH, Huang CH, Lin IC. Advances in neuroprotection in glaucoma: pharmacological strategies and emerging technologies. Pharmaceuticals (Basel). 2024;17(10):1261. doi:10.3390/ph17101261
101. La Rosa LR, Pepe V, Lazzara F, et al. Retinal protection of new nutraceutical formulation. Pharmaceutics. 2025;17(1):73. doi:10.3390/pharmaceutics17010073
102. Liebmann JM, Cioffi GA. Nicking glaucoma with nicotinamide? N Engl J Med. 2017;376(21):2079–2081. doi:10.1056/NEJMcibr1702486
103. Williams PA, Harder JM, Cardozo BH, Foxworth NE, John SWM. Nicotinamide treatment robustly protects from inherited mouse glaucoma. Commun Integr Biol. 2018;11(1):e1356956. doi:10.1080/19420889.2017.1356956
104. Leung CKS, Ren ST, Chan PPM, et al. Nicotinamide riboside as a neuroprotective therapy for glaucoma: study protocol for a randomized, double-blind, placebo-control trial. Trials. 2022;23(1):45. doi:10.1186/s13063-021-05968-1
105. Babighian S, Gattazzo I, Zanella MS, et al. Nicotinamide: bright potential in glaucoma management. Biomedicines. 2024;12(8):1655. doi:10.3390/biomedicines12081655
106. Shukla AG, Cioffi GA, John SWM, Wang Q, Liebmann JM, American Glaucoma Society and American Academy of Ophthalmology. American Glaucoma Society-American Academy of Ophthalmology position statement on nicotinamide use for glaucoma neuroprotection. Ophthalmol Glaucoma. 2025;8(2):112–116. doi:10.1016/j.ogla.2025.01.002
107. Cui Y, Yu X, Bao J, et al. Lens autophagy protein ATG16L1: a potential target for cataract treatment. Theranostics. 2024;14(10):3984–3996. doi:10.7150/thno.93864
108. Liu X, Zhou Q, Huang Y, et al. Nicotinamide improves in vitro lens regeneration in a mouse capsular bag model. Stem Cell Res Ther. 2022;13(1):198. doi:10.1186/s13287-022-02862-8
109. Sozer O, Ozalp O, Atalay E, Demir SS, Alatas İO, Yildirim N. Comparison of blood levels of vitamin B12, folic acid, riboflavin, and homocysteine in keratoconus and healthy subjects. J Cataract Refract Surg. 2023;49(6):589–594. doi:10.1097/j.jcrs.0000000000001160
110. Sasaki L, Hamada Y, Yarimizu D, et al. Intracrine activity involving NAD-dependent circadian steroidogenic activity governs age-associated meibomian gland dysfunction. Nat Aging. 2022;2(2):105–114. doi:10.1038/s43587-021-00167-8
111. Meng Y-F, Pu Q, Dai S-Y, Ma Q, Li X, Zhu W. Nicotinamide mononucleotide alleviates hyperosmolarity-induced IL-17a secretion and macrophage activation in corneal epithelial cells/macrophage co-culture system. J Inflamm Res. 2021;14:479–493. doi:10.2147/JIR.S292764
112. Lazzara F, Conti F, Maugeri G, D’Agata V, Sotera L, Bucolo C. Corneal protective effects of a new ophthalmic formulation based on vitamin B12 and sodium hyaluronate. Front Pharmacol. 2025;16:1548213. doi:10.3389/fphar.2025.1548213
113. Pu Q, Guo -X-X, Hu -J-J, Li A-L, Li -G-G, Li X-Y. Nicotinamide mononucleotide increases cell viability and restores tight junctions in high-glucose-treated human corneal epithelial cells via the SIRT1/Nrf2/HO-1 pathway. Biomed Pharmacother. 2022;147:112659. doi:10.1016/j.biopha.2022.112659
114. Yang J, Liu Y, Xu Y, et al. A new approach of ocular nebulization with vitamin B12 versus oxytocin for the treatment of dry eye disease: an in vivo confocal microscopy study. Drug Des Devel Ther. 2019;13:2381–2391. doi:10.2147/DDDT.S203464
115. De-Hita-Cantalejo C, Sánchez-González MC, Silva-Viguera C, García-Romera MC, Feria-Mantero R, Sánchez-González JM. Efficacy of hyaluronic acid 0.3%, cyanocobalamin, electrolytes, and P-Plus in menopause patients with moderate dry eye disease. Graefes Arch Clin Exp Ophthalmol. 2022;260(2):529–535. doi:10.1007/s00417-021-05415-6
116. Caruso C, D’Andrea L, Rinaldi M, Senese I, Piscopo R, Costagliola C. Modified sodium hyaluronate conjugated to riboflavin (Har® 0.1%) as lubricant eyedrops in the treatment of dry eye: a prospective randomised study. Heliyon. 2024;10(15):e35527. doi:10.1016/j.heliyon.2024.e35527
117. National Health Service. B vitamins and folic acid. [Updated August 3, 2020]. Available from: https://www.nhs.uk/conditions/vitamins-and-minerals/vitamin-b/Last.
118. Food and Nutrition Board; Institute of Medicine; National Academies. Dietary reference intakes (DRIs): recommended dietary allowances and adequate intakes, vitamins. Institute of Medicine (US) Committee to Review Dietary Reference Intakes for Vitamin D and Calcium. In: Ross AC, Taylor CL, Yaktine AL, Del Valle HB, editors. Dietary Reference Intakes for Calcium and Vitamin D. Washington, DC: National Academies Press; 2011.
119. Temova Rakuša Ž, Roškar R, Hickey N, Geremia S. Vitamin B12 in foods, food supplements, and medicines-a review of its role and properties with a focus on its stability. Molecules. 2022;28(1):240. doi:10.3390/molecules28010240
120. Hari T, Elsherbiny S. Bariatric surgery-what the ophthalmologist needs to know. Eye (London). 2022;36(6):1147–1153. doi:10.1038/s41433-021-01811-8
121. Amescua G, Ahmad S, Cheung AY, et al. Dry eye syndrome Preferred Practice Pattern®. Ophthalmology. 2024;131(4):P1–P49. doi:10.1016/j.ophtha.2023.12.041
122. Jung JW, Park SY, Kim H. Drug-Induced vitamin deficiency. Annals Clin Nutr Metab. 2022;14(1):20–31. doi:10.15747/acnm.2022.14.1.20
123. Tsang BL, Stadnik C, Duong M, Pachón H, Martinez H. Expanding fortification with folic acid: thinking outside the cereal-grain box. Nutrients. 2024;16(9):1312. doi:10.3390/nu16091312
124. Vemulakonda GA, Bailey ST, Kim SJ, et al. Age-related macular degeneration Preferred Practice Pattern®. Ophthalmology. 2025;132(4):P1–P74. doi:10.1016/j.ophtha.2024.12.018
125. Miller KM, Oetting TA, Tweeten JP, et al. Cataract in the adult eye Preferred Practice Pattern®. Ophthalmology. 2022;129(1):P1–P126. doi:10.1016/j.ophtha.2021.10.006
126. AOA Evidence-Based Optometry Guideline Development Group. Care of the patient with primary open-angle glaucoma, 1st edition. [Updated October 5, 2024]. Available from: https://www.aoa.org/a/19461.
127. National Eye Institute. Age-Related Eye Disease Studies (AREDS/AREDS2): major findings. [Updated December 3, 2024]. Available from: https://www.nei.nih.gov/research/clinical-trials/age-related-eye-disease-studies-aredsareds2/about-areds-and-areds2.
128. Domanico D, Verboschi F, Altimari S, Zompatori L, Vingolo EM. Ocular effects of niacin: a review of the literature. Med Hypothesis Discov Innov Ophthalmol. 2015;4(2):64–70.
129. National Institutes of Health. Niacin fact sheet for health professionals. [Updated November 18, 2022]. Available from: https://ods.od.nih.gov/factsheets/Niacin-HealthProfessional/.
130. Smith AD, Sobczyńska-Malefora A, Green R, Reynolds EH, Refsum H. Mandatory food fortification with folic acid. Lancet Glob Health. 2022;10(10):e1389. doi:10.1016/S2214-109X(22)00378-3
131. Miller JW, Smith A, Troen AM, Mason JB, Jacques PF, Selhub J. Excess folic acid and vitamin B12 deficiency: clinical implications? Food Nutr Bull. 2024;45(1 suppl):S67–S72. doi:10.1177/03795721241229503
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Multicenter Effectiveness and Disease Stability Through 3 Years After iStentTrabecular Micro-Bypass with Phacoemulsification in Glaucoma and Ocular Hypertension
Clement C, Howes F, Ioannidis A, Shiu M, Manning D, Lusthaus JA, Skalicky SE, Goodwin TW
Clinical Ophthalmology 2022, 16:2955-2968
Published Date: 1 September 2022
Effects of COVID-19 on Intravitreal Injection Clinic After Lockdown
Hsieh T, Gundlach BS, Ashrafzadeh S, Sarraf D, Tsui I
Clinical Ophthalmology 2022, 16:3089-3096
Published Date: 19 September 2022
Visual Outcomes, Spectacle Independence, and Patient-Reported Satisfaction of the Vivity Extended Range of Vision Intraocular Lens in Patients with Early Glaucoma: An Observational Comparative Study
Kerr NM, Moshegov S, Lim S, Simos M
Clinical Ophthalmology 2023, 17:1515-1523
Published Date: 30 May 2023
Extended Depth-of-Focus Intraocular Lens Implantation in Patients with Age-Related Macular Degeneration: A Pilot Study
Thananjeyan AL, Siu A, Jennings A, Bala C
Clinical Ophthalmology 2024, 18:451-458
Published Date: 13 February 2024
Targeting Senescence, Oxidative Stress, and Inflammation: Quercetin-Based Strategies for Ocular Diseases in Older Adults
Medoro A, Davinelli S, Scuderi L, Scuderi G, Scapagnini G, Fragiotta S
Clinical Interventions in Aging 2025, 20:791-813
Published Date: 7 June 2025