Back to Journals » Vascular Health and Risk Management » Volume 15
B-Type Natriuretic Peptides (BNP) and Tissue Doppler E/e´ Before and After 4 Weeks Standard Treatment of African Heart Failure Subjects: The ABU-BNP Longitudinal Survey
Authors Onyemelukwe OU ![]() , Oyati AI, Danbauchi SS
, Oyati AI, Danbauchi SS ![]() , Obasohan A
, Obasohan A ![]()
Received 8 April 2019
Accepted for publication 20 September 2019
Published 20 December 2019 Volume 2019:15 Pages 559—569
DOI https://doi.org/10.2147/VHRM.S211498
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Obiageli Uzoamaka Onyemelukwe, 1 Albert Imhoagene Oyati, 1 Solomon Sulei Danbauchi, 2 Austine Obasohan 3
1Department of Medicine, Ahmadu Bello University Teaching Hospital, Zaria, Nigeria; 2Department of Medicine, Jos University Teaching Hospital, Jos-Plateau State, Nigeria; 3Department of Medicine, University of Benin Teaching Hospital, Benin, Edo State, Nigeria
Correspondence: Obiageli Uzoamaka Onyemelukwe
Department of Medicine, Ahmadu Bello University Teaching Hospital, Zaria, Nigeria
Tel +234 8187351600
Email [email protected]
Background: The study aimed at determining the response of BNP and tissue Doppler (TD) E/e´ to standard heart failure (HF) therapy in an African black population as data on these are lacking in Africa. BNP assessment in relation to HF severity and its association with its predictors were also determined.
Methods: It was a longitudinal-analytical study with a one month follow-up among 100 HF patients seen at Ahmadu Bello University Teaching Hospital, Zaria-Nigeria. Two-way Repeated Measures ANOVA determined BNP levels before and after treatment according to the HF severity. Wilcoxon-Signed Ranks test determined the difference in BNP and TD E/e´ before and after treatment. Pearson’s correlation assessed log-transformed BNP’s association with its predictors.
Results: BNP significantly (p< 0.001) rose with increasing severity of HF from 386.6 ± 186.5 pg/mL to 581.7 ± 299.0 pg/mL to 805.0 ± 484.0 pg/mL in the NYHA II-IV HF, respectively, with consequent fall in a similar fashion following treatment. The Median (IQR) BNP levels reduced significantly (p< 0.001) from 450 (362.5, 712.5) to 275.0 (225, 375.2) pg/mL with a 38.9% reduction over 4 weeks associated with significant improvement in TD E/e´, structural and functional parameters. Ln 10BNP was significantly (p< 0.001) positively correlated to TD E/e´ before (r=0.51) and after treatment (r=0.43). Likewise, Ln 10BNP was significantly (p< 0.05) negatively correlated to ejection fraction & fractional shortening before and after treatment.
Conclusion: BNP and tissue Doppler can serve as useful tools in the assessment of the effectiveness of African HF treatment and functional capacity over 4 weeks. TD E/e´ may be a reliable non-invasive estimate of left ventricular filling pressures and diastolic dysfunction.
Keywords: B-type natriuretic peptide, pulsed tissue doppler, left ventricular filling pressure, African heart failure, before and after 4 weeks standard therapy
Corrigendum for this paper has been published
Introduction
B-type natriuretic peptide, a neurohormone secreted by the cardiomyocytes in response to myocardial stretch from pressure/volume overload as seen in heart failure, neurohormonal and cytokine stimulation, ischaemia/hypoxia and hydrosaline retention,1,2 has been demonstrated alongside with tissue Doppler (TD) E/e´ from several studies in European countries and the United States of America to be useful in the diagnosis, monitoring and prognostication of heart failure.1–11 BNP has been shown to be an excellent biomarker of cardiovascular disease while TD E/e´ unlike BNP has been demonstrated to be more specific for left ventricular filling pressures and diastolic dysfunction with less influence of morphological cardiac changes as well as haemodynamic changes on right heart catheterization.2 It has, therefore, been suggested that the combination of BNP and TD E/e´ in the diagnosis and prognostication of HF may be complementary to each other.3,10
Studies regarding these indices are however lacking in sub-Saharan Africa as the large body of evidence had emanated from the white population. This study was therefore aimed at determining the response of BNP and TD derived mitral E/e´ to standard heart failure therapy over a four weeks period in an African black population bearing in mind the genetic, geographical and racial differences in a heterogeneous global society. Further assessment of the BNP levels with New York Heart Association (NYHA) class severity of HF as well as the relationship between BNP levels and TD derived E/e´, some echocardiographic parameters and its predictors, before and after treatment were also envisaged.
Method
Study Design/Inclusion and Exclusion Criteria
It was a longitudinal analytical study with a one-month follow-up, carried out among HF patients seen at the accident & emergency, medical wards and cardiac clinic of Ahmadu Bello University Teaching Hospital, Zaria, Nigeria between November 2015 and August 2016. Consecutively, 100 decompensated heart failure subjects whose aetiologies were mainly hypertensive HF, peripartum cardiomyopathy, rheumatic valvular heart disease because of the predominance in our environment and other aetiologies as they presented were enrolled prospectively and followed up over a 4 weeks period.
Only patients from the African black population were included. Subjects included were adult male and female decompensated heart failure patients >18 years of age who satisfied the Framingham criteria for definite HF13 and who were in the New York Heart Association (NYHA) class II-IV heart failure.14 Patients who had simultaneous echocardiography as well as blood sampling done within 24 hrs of enrolment were included. Additional 75 healthy controls were also randomly surveyed to determine the baseline BNP levels in the normal healthy population (Unpublished data).
Patients were excluded on account of HF from congenital heart disease, echocardiographic evidence of pericardial disease, severe mitral stenosis/calcifications, hypertrophic cardiomyopathy as well as historical/electrocardiographic evidence of atrial fibrillation or myocardial infarction.10,15 HF subjects with historical evidence of concomitant hepatic disease; renal impairment {estimated glomerular filtration rate (eGFR <60 mL/min) by Cockroft-Gault equation};16 concomitant respiratory diseases like chronic obstructive pulmonary disease (COPD) and bronchial asthma via medical follow-up records were also excluded. Patients who had 3 months prior history of drug compliance to standard guideline directed medical therapy (GDMT) inclusive of angiotensin-converting enzyme (ACE) inhibitors/angiotensin receptor blockers (ARBs), aldosterone antagonists, β-blockers as well as diuretics were also excluded.6
More so, HF subjects with historical and fasting blood glucose (FBG) evidence of diabetes (FBG ≥7 mmol/L) were also excluded. Subjects without clinical improvement/non-responders (clinical symptoms and signs unabated by 4th week) or those deceased as well as subjects lost to follow up were also excluded.
Ethical Clearance was obtained from the Health Research Ethical Committee (HREC), ABUTH, Zaria, Nigeria with Reference Number ABUTHZ/HREC/K11/2015. The study was carried out according to the Helsinki’s declaration and written informed consent was obtained from all participants. It also adheres to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for an observational study of this nature.
Null Hypotheses:
- There is no reduction in BNP levels and TD E/e´ following 4 weeks treatment of HF in African blacks
- BNP level does not worsen with increasing clinical severity of heart failure
- There is no relationship between plasma BNP and TD E/e´, as well as echocardiographic left ventricular systolic functions and structural parameters.
Sample Size Determination
This was determined by sample size calculation formula in clinical trials viz-a-viz:12
n= (Z 1-β+ Z 1-)2 ÷d2
With an estimated attrition rate of approximately 20% (non-response and indeterminate results) i.e. 20/100 x 32 = 6.4, for the subjects before and after treatment, the estimated sample size was approximately 40, which is the minimum number required. However, 100 patients were recruited to increase the statistical power and take care of attrition, out of which 75 patients completed follow up.
Clinical and Laboratory Methods
Subjects had a well-structured medical questionnaire, interviewer-administered by 2 trained research assistants (medical doctors). Anthropometrics (weight, height and body mass index (BMI) in kg/m2) as well as blood pressures were obtained for all patients based on standard protocol.17 HF diagnosis was established based on the Framingham’s criteria.13 HF diagnosis requires at least 2 major criteria or 1 major and 2 minor criteria; hence this was applied in the study.
Blood samples for plasma BNP were collected from the antecubital vein of either arm. This was apportioned into two 5mL aliquots and placed into labelled potassium ethylenediaminetetraacetic acid (EDTA) containing plastic vacutainer tubes and plain specimen bottles, respectively. A drop (500 kallikrein inactivator U/mL) of aprotinin (trasylol®) had been previously added to each tube. Within 4 hrs of collection, the samples were taken to the Immunology laboratory of ABUTH, Zaria, Nigeria in ice cubes and centrifuged at 1800 revolutions per minute for 20 mins. Plasma was separated within one to two hours and divided into aliquots in cryovials with subsequent storage at −70ºC in the anti-retroviral laboratory of ABUTH, Zaria, Nigeria until final assay according to the standard protocol of the manual. The kit had a detection range of 31.25–2000 pg/mL and coefficient of variation <10%.
Electrocardiography, chest X-ray and detailed echocardiography were done for all subjects. The day the patients were enrolled/blood sampled and echocardiographed was designated as week 0. Patients were placed on standard anti-failure medications inclusive of angiotensin-converting enzyme inhibitor/angiotensin receptor blockers (ACEI/ARB’s), β-blockers, aldosterone antagonists, digitalis, diuretics and phosphodiesterase inhibitors/antiplatelet as per the protocol of the cardiology unit of ABUTH, Zaria. Some ACEI/ARBs were provided by the free will donation of Micro Nova Pharmaceutical Industries Nigeria Ltd. for subjects who could not afford their standard therapy. Clinical re-assessment, blood sampling and repeat echocardiography were done at week 4 only if exercise tolerance had improved and clinical symptoms/signs of HF had abated. This was determined by 2 trained research assistants (cardiologists) blinded to BNP levels. Patients were followed up with weekly calls and text messages while those on admission had closer monitoring to ensure strict compliance with therapy.
Plasma BNP Measurement
Plasma BNP in-vitro quantitative assay was done at the end of the study in one batch at the Immunology laboratory of ABUTH, Zaria using the BNP Direct Enzyme-linked Immunosorbent assay (ELISA) kit by Elabscience Biotechnology Co., Ltd with Lot Number: AK0016JUL15068 and Catalog Number: E-EL-H0598. The kit used the competitive ELISA assay method.
Tissue Doppler Echocardiography
Echocardiography was performed for all subjects by an experienced consultant cardiologist (AO) (with over 10 years experience) blinded to all clinical and BNP data using the SONOSCAPE SSI-18 2-D/3-Dimensional Doppler and colour flow machine with tissue Doppler facility and a 3.5 megahertz (MHz) convex probe. Two-dimensional echocardiography was performed according to the recommendations of the American Society of Echocardiography and indexed to body surface area.18,19 The left ventricular ejection fraction (LVEF) and fractional shortening (LVFS) were calculated by the machine via the Teicholz calculation formula. The LVEF was also confirmed by visual estimation on multiple views by the experienced echocardiographer. Most aetiologies of HF in our population are hypertensive and cardiomyopathy related hence M-mode assessment was appropriate.15
The pulse wave tissue Doppler imaging (TDI) was performed in the apical four chamber view to acquire mitral annular velocities by pressing on the TDI and pulse wave (PW) buttons on the echocardiography machine. The sample volume was positioned at or 1 cm within the septal annular area of the mitral leaflets and adjusted within 5–10 mm, to cover the longitudinal excursion of the mitral annulus in both systole and diastole.18,19
Primary measurements were the systolic (S), early diastolic (e´) and late diastolic velocities (á). All measurements were averaged over 3 cardiac cycles in sinus rhythm. The left ventricular filling pressure (LVFP) was determined via manual calculation of the ratio of mitral inflow E velocity to tissue Doppler-derived e´ velocity (E/e´).10,18–20 The septal E/e´ ratio was used. An E/e´ ratio <8 was considered to be normal while a ratio >15 was considered to reflect an increased LVFP.10
Statistical Analysis
Data were validated and analysed by SPSS version 25-software (IBM). Data were checked for normality of distribution using the Kolmogorov–Smirnov test. Categorical variables were presented as frequency and percentages with comparisons made with Chi-square (X2) test. Numerical data were presented as Mean ± SD and non-parametric data were presented as Median + Interquartile Range (IQR) with the 25th and 75th percentiles considered. Comparison between Median BNP levels and TD E/e´ parameters of HF patients before and after treatment were determined by Wilcoxon Signed Ranks test. Mann–Whitney U-test was used to determine the sex variation of BNP levels. Kruskal Wallis test determined the difference in BNP levels with increasing severity of HF while the Two-way repeated Measures Analysis of Variance (ANOVA) was used to determine the BNP levels before and after treatment between the 3 NYHA classes of HF. TD E/e´ was recoded into 3 variables, viz.: <8 as 1; 8.1–15 as 2 and >15.1 as 3 both before and after treatment variables. Kruskal Wallis test determined the difference in Median (IQR) BNP levels between the different grades of TD derived E/e´. Skewed BNP data and some parameters were naturally log-transformed to reduce the skewness. Pearson’s correlation analysis was used to determine the relationship between log-transformed BNP and some echocardiographic parameters inclusive of TD E/e´, LVEF/LVFS, left atrial diameter (LAD), left ventricular Internal diameter in diastole (LVIDd) as well as some predictors of BNP such as age, sex, BMI, GFR and HF duration, both before and after treatment of HF, respectively. P-value ≤0.05 was assumed as the level of statistical significance at 95% Confidence Interval.
Results
Subject Participation
A total of 100 patients were recruited. Of these, 75 (75.0%) patients completed follow up and had complete data while 25 (25.0%) were excluded on account of being deceased, non-responders, associated chronic liver disease and loss to follow up (Figure 1).
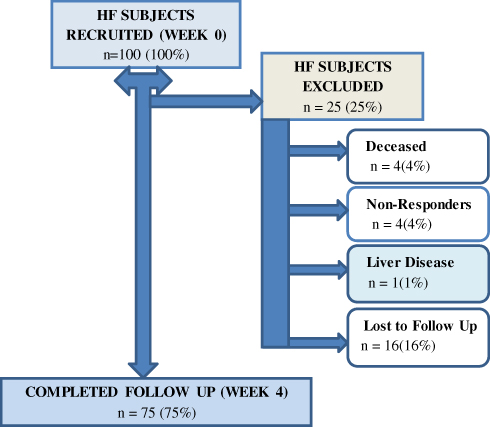 |
Figure 1 Subjects' participation in the ABU-BNP longitudinal survey. Abbreviations: HF, heart failure; n, number of subjects. |
Socio-Demographic and Clinical Characteristics of the Study Population
There was a female preponderance in this study (Table 1). The Mean ± SD age of the study population was 44.8 ± 15.2 years with no significant (p=0.90) difference in age distribution between both sexes (Table 1). The Median (IQR) BNP levels were significantly (p=0.002) higher in females than males before treatment of HF using the Mann Whitney U-test. The trend was similar following treatment, though not of statistical significance (p=0.38) (Table 1). Hausa/Hausa-Fulani’s were the predominant tribe followed by other minority Northern ethnic groups (Table 1). A small proportion of patients had their HF duration <3 months while most had HF >9 months (Table 1). There were more subjects in the NYHA class 3 followed by NYHA class IV with a combination of both classes {56 (74.7%)} being more represented (Table 1). Only 19 (25.3%) were in the NYHA class II. Hypertensive heart failure was the commonest cause of HF followed by peripartum cardiomyopathy, rheumatic valvular heart disease and dilated cardiomyopathy, respectively (Table 1). The Mean ± SD baseline systolic and diastolic blood pressures were 118.3 ± 26.4 mmHg and 85.5 ± 19.5 mmHg, respectively, with a significant (p<0.001) reduction in both following treatment (Table 1). Likewise, there was a significant (p<0.001) reduction in BMI from week 0 to week 4 following treatment (Table 1).
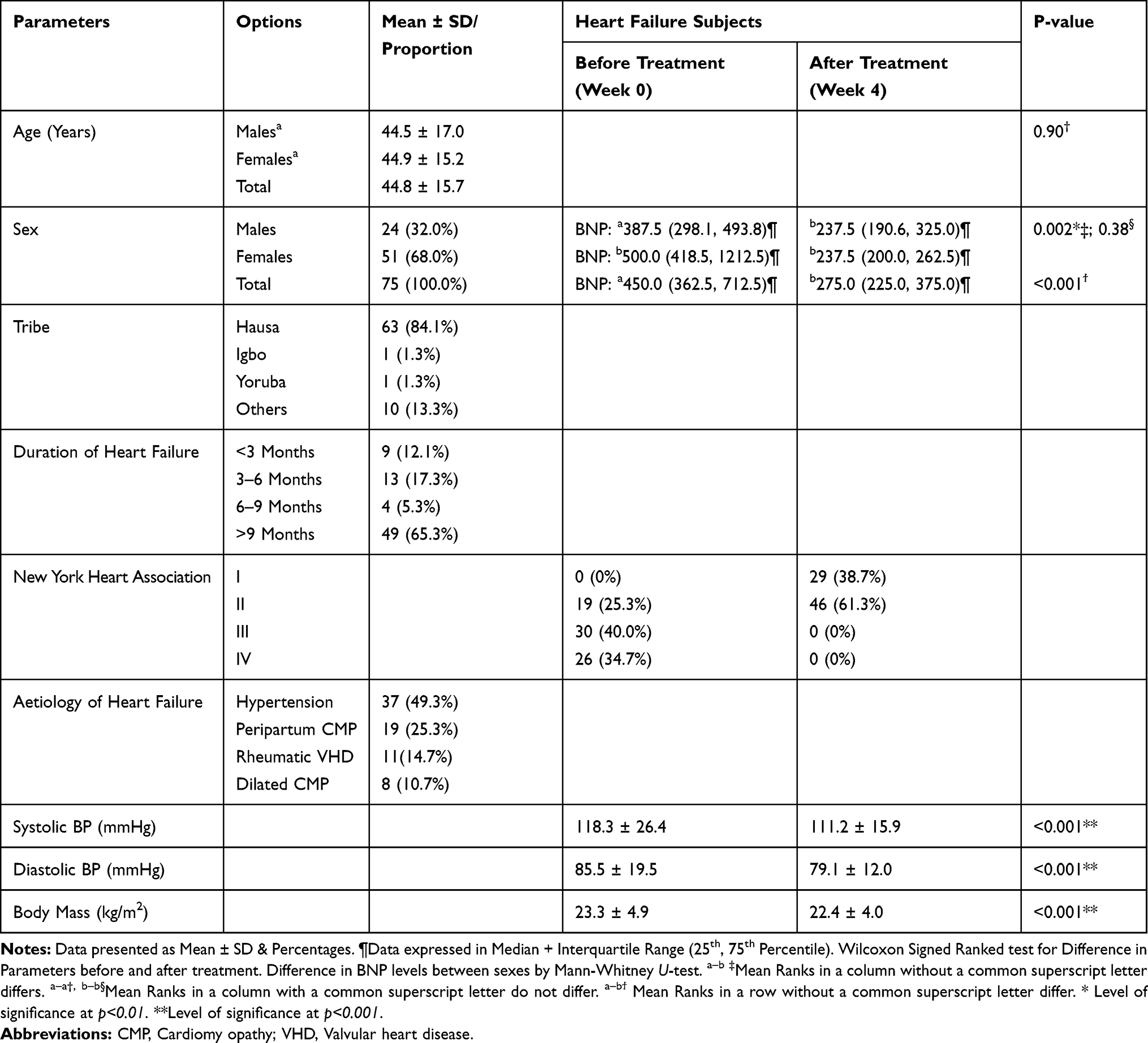 |
Table 1 Socio-Demographic & Clinical Characteristics of the Study Population |
BNP Levels and NYHA Functional Class Severity of HF Before and After Treatment
Furthermore, the study showed a significant (p<0.001) rise in Mean ± SD BNP levels with increasing severity of HF from the NYHA class II to the NYHA class IV using the Kruskal Wallis test (Figure 1). Following treatment, the BNP levels decreased significantly (p<0.001) in each NYHA class (Figure 1) by way of the two-way Repeated Measures ANOVA (Figure 2).
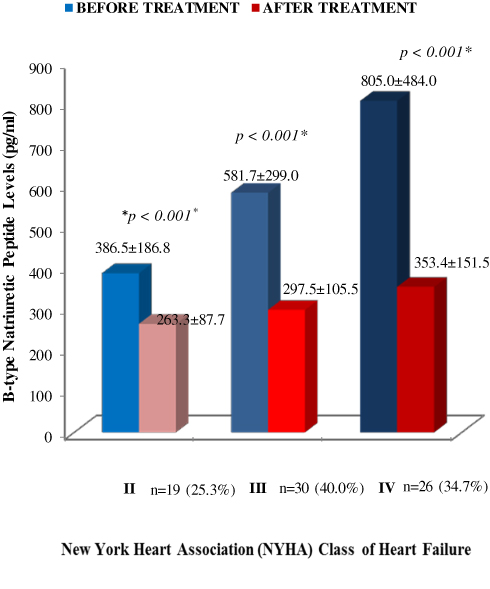 |
Figure 2 Distribution of BNP levels according to NYHA class of heart failure. Data presented as Mean ± SD. Difference between each class of HF before treatment by Krus kall Wallis test; difference between BNP levels before and after treatment in 3 classes of HF by Two-way Repeated Measures ANOVA; n: total number of subjects in each NYHA class of HF; *Level of significance at p<0.001. ANOVA: analysis of variance. |
Drug History of the HF Study Population
Patient’s treatments were individualized and most were on 4 to 5 drug combination therapy with counselling on adherence ensured. The ACEI/ARBs were mostly used followed by diuretics, aldosterone antagonists and digitalis, respectively, while β- blockers were least utilized (Figure 3).
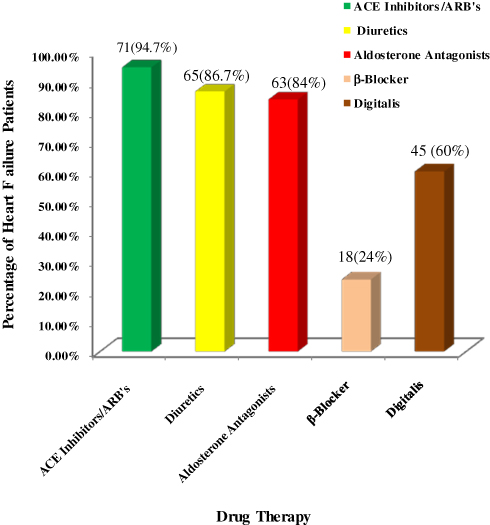 |
Figure 3 Distribution of heart failure therapy for 4 weeks. |
Echocardiographic Left Ventricular Parameters and BNP Levels Before and After HF Treatment
Following standard HF therapy of 4 weeks, there was a significant (p<0.05) improvement in some echocardiographic LV function parameters as well as decrease in BNP levels via the Wilcoxon Signed Ranked test. The Mean ± SD LVEF improved significantly (p<0.001) with a similar improvement in Mean ± SD LVFS (Table 2). There was a significant (p=0.005) reduction in Mean ± SD LVIDd as well as Mean ± SD LAD (p<0.001) following treatment of 4 weeks (Table 2). The Median (IQR) TD derived E/e´ showed a significant (p<0.001) reduction in pre-treatment levels after 4 weeks of therapy (Table 2). The Median (IQR) BNP levels reduced significantly (p<0.001) from (362.5, 712.5) pg/mL to 275.0 (225, 375.2) pg/mL with a 38.9% reduction in levels over 4 weeks (Table 2).
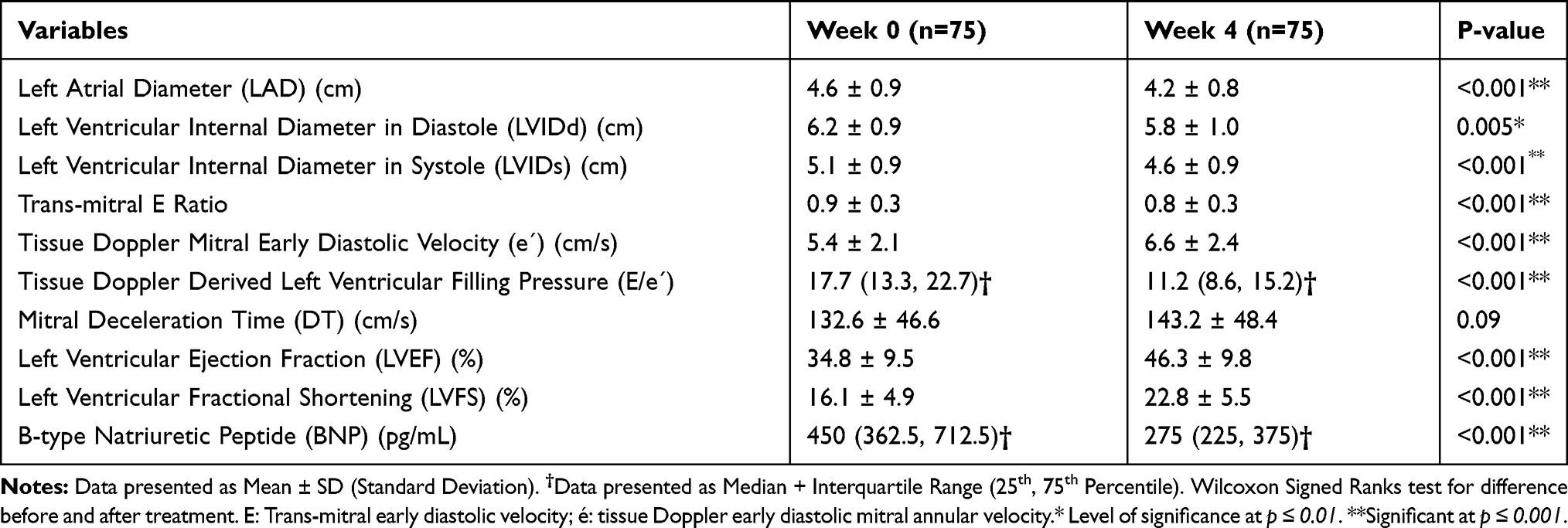 |
Table 2 Echocardiographic Parameters and BNP Levels Before and After 4 Weeks Treatment of HF |
BNP Levels in Relation to Left Ventricular Filling Pressure (E/e´) Before and After Treatment of HF
Table 3 shows that at week 0, the Median (IQR) BNP level was highest in HF subjects with elevated LVFP (E/e´>15). There was a statistically significant (p=0.001) difference between the 3 grades of TD E/e´ using the Kruskal Wallis test. With application of the post hoc test, the Median (IQR) BNP levels of those subjects within the highest non-invasive estimate of LVFP (E/e´>15) were significantly (p<0.001) higher than those within the “gray zone” (8–15) of E/e´ as well as those within normal LVFP (E/e´<8) (p=0.002) (Table 3). Furthermore, following treatment, there was a similar trend (p=0.01), as the BNP levels of those within the highest non-invasive estimate of LVFP were significantly (p=0.01) higher than those within the normal as well as those within the “gray zone” (p=0.03) (Table 3). There was no significant (p>0.05) difference in BNP levels between subjects within normal LVFP and those within the “gray zone” both before and after HF treatment (Table 3).
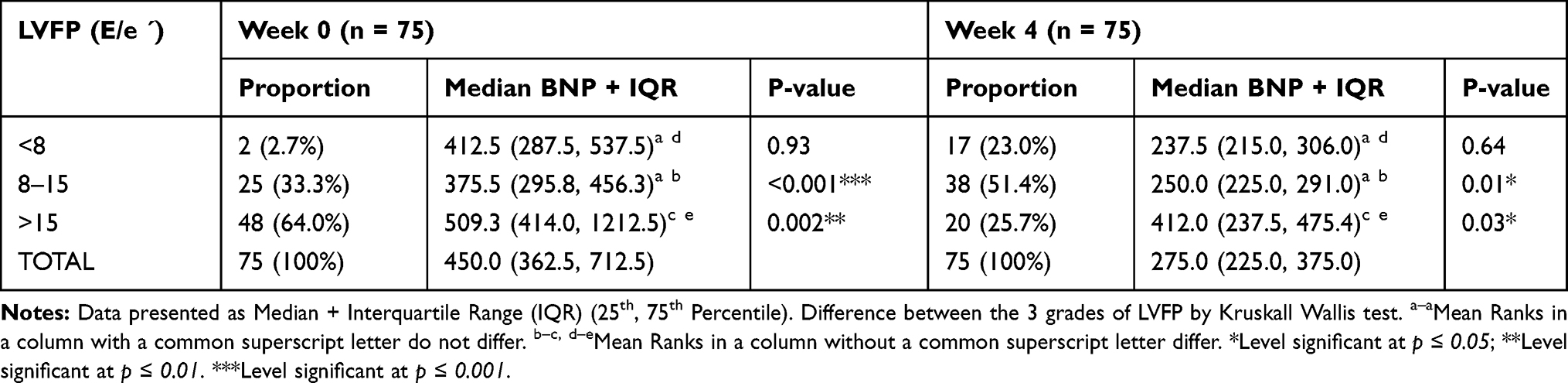 |
Table 3 BNP Levels in Relation to Left Ventricular Filling Pressure (E/E´) Before and After Treatment of HF |
Relationship Between Plasma BNP and Echocardiographic Left Ventricular Function Parameters as Well as Some Predictors of BNP Levels Before and After HF Treatment
The Pearson’s correlation analysis showed a significant (p<0.05) negative relationship of log-transformed BNP with LVEF & LVFS both before and after treatment of HF (Table 4). TD derived E/e´ showed a positive relationship with log-transformed plasma BNP before (r=0.51; p<0.001) and after (r=0.43; p<0.001) treatment of HF. Other parameters significantly (p≤0.05) positively correlated to plasma BNP were: LAD (p=0.01) before and after treatment, respectively; LVIDd before (p=0.02) and after treatment (p=0.01); sex before (p=0.002) and after treatment (p=0.02) as well as age before treatment (p=0.01) only (Table 4). NYHA class was also significantly (p=0.001 & p<0.001) positively correlated to BNP before and after treatment, respectively (Table 4). On the other hand, the BMI (p=0.01 & p=0.05) and HF duration (p<0.001 & p=0.001) were significantly negatively correlated to BNP levels before and after treatment, respectively. The GFR was inversely significantly (p=0.02) correlated to BNP only before HF treatment (Table 4).
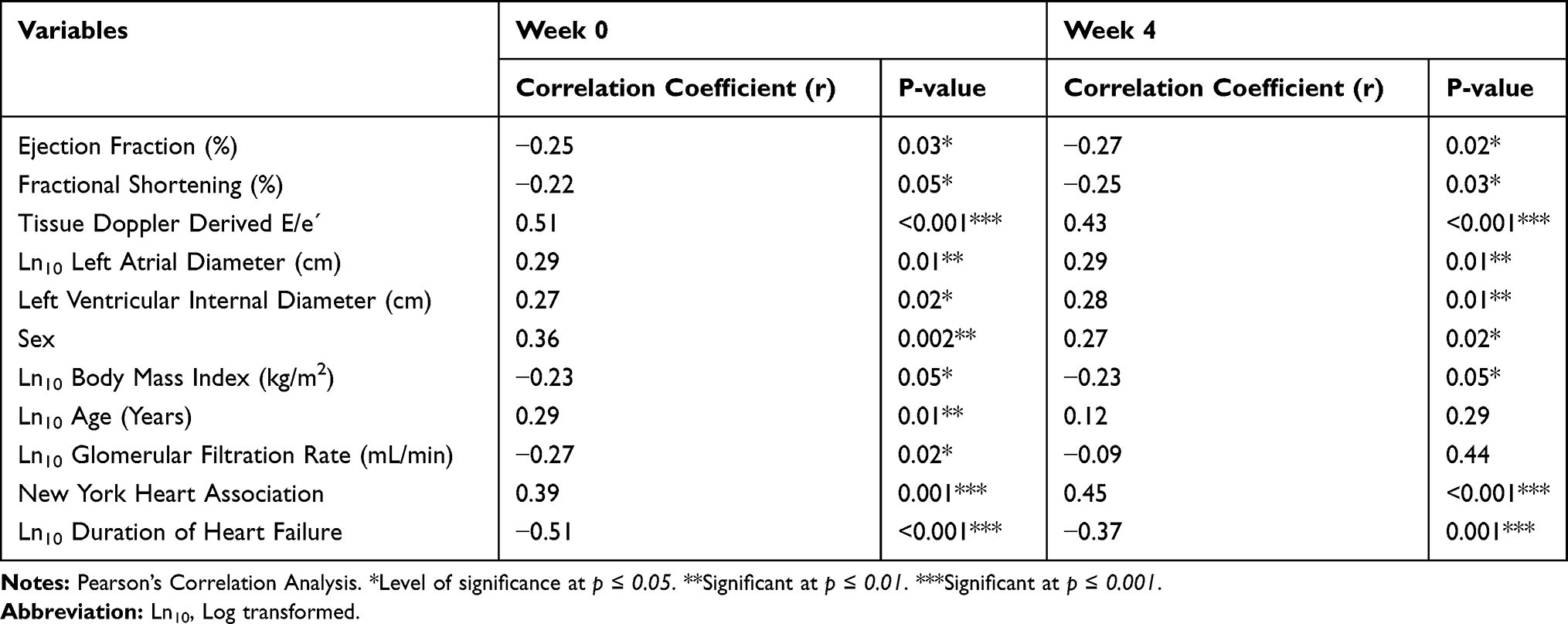 |
Table 4 Relationship Between Log-Transformed BNP and Some Echocardiographic Parameters as Well as Predictors of BNP Before and After Treatment |
Discussion
To the knowledge of the authors, this is the first study to document the response of BNP and TD E/e´ to standard HF therapy in a black African population over a designated period of 4 weeks. The study showed that following treatment of HF, BNP levels decreased significantly (p<0.001) from high pre-treatment values with a 38.9% reduction rate over 4 weeks, similar to other studies in European countries and the United States of America.4,21,22 Ito and co-workers reported a significant (p<0.01) fall in BNP levels over 42 days treatment of their HF subjects3 while Murdoch et al demonstrated a 42% reduction in BNP levels at 4 weeks following treatment.21 The Prospective Comparison of Angiotensin Receptor Neprilysin Inhibitor (ARNI) with Angiotensin Receptor Blocker (ARB) on Management of Heart Failure with Preserved Ejection Fraction (PARAMOUNT HF) trial showed a 23% drop in the equivalent biomarker NT-proBNP over a longer duration of 12 weeks in the LCZ696 group as against those on Valsartan therapy.22 The present study therefore confirms the existing evidence that with conventional medical therapy of majorly heart failure with reduced ejection fraction (HFrEF) inclusive of ACEI/ARB’s for 4 weeks, there is marked fall in BNP levels as a result of reduction in volume/pressure overload and LVFPs from counteraction of the effect of vasoconstrictor molecules and renin-angiotensin-aldosterone pathway. Studies have shown that a reduction in BNP or NT-proBNP levels ≥30% from initial values may actually give signals towards improved prognosis.1,23 This fact has been utilized in monitoring and follow-up of HF subjects in clinics with varying results in which some studies support the need for BNP-guided treatment of out-patient HF while others refute the need for this.23
It was based on the large body of evidence in white population that BNP has been incorporated into national and international cardiovascular guidelines for heart failure like the American Heart Association (AHA) and the European Society of Cardiology (ESC).3,4,7–11,18,20,24 However, in low-middle income countries in sub-Saharan Africa like Nigeria, BNP is far from being utilized regularly in the management of HF at the primary, secondary and tertiary health care levels. Hence, this study has shown that BNP may provide valuable information regarding the effectiveness of drug therapy and patient-specific outcome to therapy.
Further to this and associated with BNP reductions following treatment was an improvement in LVEF and LVFS, depicting improvement in systolic functions as well as a reduction in TD derived LVFPs (E/e´). The LAD and LVIDd also reduced in size following treatment. Similar studies have shown that natriuretic peptides rise in acute decompensated HF and fall with successful treatment in a pattern that mirrors reduction in LVFPs, improvement in LV structure and function as well as improved functional capacity as seen in this study.4,8,21 Therapies proven to be of immense benefit in HFrEF include the ACEI/ARB’s which was used in 94.7% of HF subjects in this study, spironolactone, β-blockers and the newer valsartan-neprilysin inhibitor combination therapy.1,6,9,25–29 Cardiac resynchronization therapy also appears to reduce NP levels with corresponding improvement in cardiac remodelling and clinical outcomes.8,9 Other drugs like the diuretics in addition to the aforementioned reduce NP levels; hence, many patients with chronic stable HF have been reported to have BNP levels within the normal range of <100 pg/mL.6,8,9 Digoxin and β-blockers however increase NP levels.6,9,30,31 The increase from β-blocker therapy occurs initially, as it blocks the adrenergic stimulation that acts to decrease BNP release, with subsequent decline in BNP levels in the long term.31 This was however not objectively assessed in this study and very few subjects were placed on β-blockers. The result of this study therefore shows that with optimal recommended conventional drugs especially ACEI/ARB’s, African HF patients responded to therapy with improvement in echocardiographic LVFs and structure, attributed to a reduction in ventricular volume and pressure overload and consequently LVFP following treatment.
Furthermore, the improvement in non-invasive TD estimate of LVFP (E/e´) was evidenced by the reduction in the proportion of HF patients with the highest pre-treatment BNP levels to less than half, associated with a reduction in BNP levels following treatment (Table 3). Also, a similar trend was observed for those within the “gray zone” of E/e´, who had their proportion increase to almost 51% from 33% as a result of response to therapy, with concurrent decrease in BNP levels following treatment. This may further support the use of BNP and TD E/e´ in the monitoring of treatment and response to therapy in Africans.
Consistent with previous reports,4,8,9,15,24 the BNP levels were found to be higher with increasing severity of breathlessness based on the NYHA functional class with lower levels in the NYHA class II and highest levels in the NYHA IV. This is expected, as with worsening of systolic function, there is an increase in volume and pressure overload as well as filling pressures. These consequently act as stimuli for stretching the cardiomyocytes to synthesize and release more and more of BNP to counteract the vasoconstrictor effects of the neurohormonal systems and thereby stabilize the functional capacity of the heart. The reduction in BNP levels with improving functional status was also shown following treatment, further buttressing the prognostic effect of optimal GDMT on BNP levels and consequently functional status of the patients.
Importantly, the tissue Doppler E/e´ showed moderate positive correlation to BNP levels before and after treatment, respectively. This shows that TD E/e´ may be a reliable non-invasive estimate of LVFP and diastolic dysfunction confirming previous reports from Western countries.32–35 This finding was also consistent with reports from Ito and colleagues who documented a significant (p<0.05) moderate correlation (r=0.51) of BNP to E/e´ following treatment of their HF subjects.4 It, therefore, means that with worsening HF and associated rise in LVFPs, the ventricular myocytes respond to wall stretch, pressure/volume overload and hydro-retention by releasing more BNP with reverse effect following treatment.2,4
The TD imaging is a technique which directly assesses myocardial velocities and has been shown from studies in European countries and the United States to non-invasively estimate LVFP as well as establish HF diagnosis in dyspnoeic patients.10,36 It is however limited with respect to the “gray zone” as we11 as its low validity in HF with atrial fibrillation (AF), severe mitral stenosis/calcification, mitral valve repair/prosthetic valves, left ventricular assist devices, left bundle branch block and pacemaker induced ventricular rhythm.10,18,20,36 Hence, the strict selection criteria in this study. The combination of BNP with TD will further enhance interpretation for subjects within the “gray zone.” On a further note, within clinical practice in sub-Saharan Africa, the non-invasive assessment of LVFPs is often overlooked and the focus is often on estimation of ejection fraction and assessment of LV volumes in the diagnosis of HF.32
However, this study confirms previous findings on the need for non-invasive assessment of LVFP alongside BNP levels in African HF.
Likewise, albeit with lower correlation values, BNP was inversely correlated to systolic functions before and after HF treatment similar to some previous report.9 This suggests that BNP levels rise with worsening systolic function and consequently fall with improved LVEF following treatment. Similar reports for the equivalent biomarker NT-proBNP have been documented by Ajuluchukwu et al15 and Ojji et al31 in Nigeria. These findings may provide evidence that BNP may be an important determinant of LV systolic and diastolic functions as well as serve as a good monitor for patients on HF treatment.
Finally, the study further showed that BNP levels were significantly positively related to age and sex with an inverse relationship to BMI and GFR as reported previously.1,2,4,37–41 The weak correlation values, however, may be attributed to the heterogeneity of the study population, viz.: combined systolic and diastolic dysfunction; normal and abnormal ejection fraction; younger age groups studied as against the older age in industrialized nations; selection criteria with exclusion of subjects with severe renal impairment, diabetes and liver disease as well as the variety of diagnosis in this study. The elderly group which is the group expected to show great changes with BNP was represented by very few subjects. Obesity has been shown to be associated with very low BNP levels as the natriuretic clearance receptors (NPR-C) which clears BNP from the system are more expressed in adipocytes thereby resulting in increased receptor-mediated BNP clearance and consequently lower levels.1,39–41 The sex-specific relations of BNP were supported by the higher BNP levels in females compared to males. The reason for this may be attributed to hormonal differences, with oestrogenic stimulation of BNP release as opposed to androgenic inhibition of the same.39 Heart failure duration was also negatively related to BNP levels signifying that the longer the duration of HF, the lower the BNP levels on account of exhaustion of the ventricular biomarker synthesis and reduced effectiveness of the natriuretic peptide system in long-standing HF, despite dramatic increases in its circulatory levels.40,41
Limitations
Time and resource did not allow opportunity for long-term follow-up of these patients using BNP and TD to determine their prognostic effect over time. Due to the non-availability of the ASE/ESC recommended Modified Simpson’s method of assessment of LVEF, the M-mode was used. However, this is appropriate in our setting as most of the aetiologies of HF are hypertensive and cardiomyopathy related.15 Studies have validated the use of non-invasive TD estimation of LVFPs which could have been more objectively assessed invasively but for lack of availability in resource-poor centres like ours.
Conclusion
Conclusively, this study shows that BNP and TD can serve as useful tools in the assessment of the effectiveness of African HF treatment as it showed a 38.9% reduction in BNP levels associated with improved TD E/e´, LV functional and structural parameters, as well as NYHA functional capacity following treatment of 4 weeks. Tissue Doppler E/e´ may be a reliable non-invasive estimate of diastolic left ventricular filling pressures and diastolic dysfunction.
Recommendations
BNP-guided therapy can be instituted in the health-care facilities of low-middle income countries in sub-Saharan Africa like Nigeria for aggressive optimization of conventional therapy in the reduction of filling pressures and better patient management. TD derived estimate of LVFP should be routinely done in the echocardiographic assessment of African HF subjects. Further longitudinal studies should be carried out across all geopolitical zones of the country to determine the prognostic significance of BNP and TD in the management of HF.
Abbreviations
ABU, Ahmadu Bello University; BNP, B-type Natriuretic Peptide; NT Pro-BNP, N-Terminal pro B-type Natriuretic Peptide; HF, Heart Failure; LVFP, Left Ventricular Filling Pressure; NYHA, New York Heart Association; ANOVA, Analysis of Variance; E/e´, Ratio of Trans-mitral early diastolic velocity to tissue Doppler early diastolic mitral annular velocity; HHF, Hypertensive Heart Failure; RVHD, Rheumatic Valvular Heart Disease; PPCM, Peripartum Cardiomyopathy.
Acknowledgment
We are indebted to Prof. G.C. Onyemelukwe as well as Prof. M.S. Isa for their contributions in the primary project.
Authors' Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Weber M, Hamm C. Role of B-type natriuretic peptide (BNP) and NT-proBNP in clinical routine. Heart. 2006;92(6):843–849. doi:10.1136/hrt.2005.071233
2. Palazzuoli A, Beltrami M, Ruocco G, Pellegrini M, Nuti R. The role of natriuretic peptides for the diagnosis of left ventricular dysfunction. Sci World J. 2013;784670–784680. doi:10.1155/2013/784670.10
3. Dokainish H, Zoghbi WA, Lakkis NM, et al. Incremental predictive power of B-type natriuretic peptide and tissue doppler echocardiography in the prognosis of patients with congestive heart failure. J Am Coll Cardiol. 2005;45(8):1223–1226. doi:10.1016/j.jacc.2005.01.025
4. Ito K, Kawai M, Nakane T, et al. Serial measurements associated with an amelioration of acute heart failure: analysis of repeated quantification of plasma brain natriuretic peptide levels. Eur Heart J. 2012;1(3):240–247.
5. Al Bannay R, Husain AA. Role of tissue Doppler imaging in assessing left ventricular diastolic dysfunction severity. Does it hold the same ability? Said Med J. 2012;33(1):34–38.
6. Doust J, Lehman R, Glasziou P. The role of B-type natriuretic peptide testing in heart failure. Am Fam Phys. 2006;74(11):1893–1900.
7. Silver W, Maisel A, Yancy CW, et al. Brain natriuretic peptide consensus panel 2004; a clinical approach for the diagnostic, prognostic, screening, treatment, monitoring and therapeutic roles of natriuretic peptides in cardiovascular disease. Cong Heart Fail. 2004;5(3):1–30.
8. Desai SA. Are serial BNP measurements useful in heart failure management: the art of medicine remains long. Circulation. 2013;127(4):509–516. doi:10.1161/CIRCULATIONAHA.112.120493
9. Troughton RW, Frampton CM, Yandle TG, Espine EA, Nicholls MG, Richards AM. Treatment of heart failure guided by plasma amino terminal brain natriuretic peptide (N-BNP) concentrations. Lancet. 2000;355(9210):1126–1130. doi:10.1016/S0140-6736(00)02060-2
10. Dokainish H. Combining tissue Doppler echocardiography and B-type natriuretic peptide in the evaluation of left ventricular filling pressures: review of the literature and clinical recommendations. Can J Cardiol. 2007;23(12):983–989. doi:10.1016/S0828-282X(07)70861-9
11. Zhang Z, Li R, Yang F, Xi L. Natriuretic peptide family as diagnostic/prognostic biomarker and treatment modality in management of adult and geriatric patients with heart failure: remaining issues and challenges. J Geriatric Cardiol. 2018;15(5):540–546.
12. Chow SC, Liu JP. Classification of Clinical Trials, in Design and Analysis of Clinical Trials: Concepts and Methodologies.
13. Ho KL, Pinsky JL, Kannel WB, Levy D. The epidemiology of heart failure: the Framingham Study. J Am Coll Cardiol. 1993;22(4):6A–13A. doi:10.1016/0735-1097(93)90455-A
14. Ponikowski P, Voors AA, Anker SD, et al. European Society of Cardiology guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur J Heart Fail. 2016;18(8):891–975.
15. Ajuluchukwu JN, Ekure EN, Mbakwem AC, Okoromah CN, Oladipo OO. Reliability and accuracy of point-of-care amino-terminal proBNP in congestive heart failure patients. Intern J Cardiol. 2010;9(1):1–15.
16. Cockroft DW, Gault MH. Prediction of creatinine clearance from creatinine. Nephron. 1976;16(1):31–41. doi:10.1159/000180580
17. WHO.WHO STEP wise Approach to surveillance (STEPS). Waist Circumference and Waist-Hip Ratio: Report of a WHO Expert Consultation. Geneva: World Health Organization (WHO), Geneva; 2008.
18. Nagueh SF, Smiseth OA, Appleton CP, et al. Recommendation for the evaluation of left ventricular diastolic dysfunction by echocardiography: an update of the ASE & European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2016;29(4):277–314. doi:10.1016/j.echo.2016.01.011
19. Lang RM, Badano LP, Mor-Avi V, et al. Recommendation for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2015;28(1):1–39. doi:10.1016/j.echo.2014.10.003
20. Nagueh SF, Smiseth OA, Appleton CP, et al. Diastolic function by echocardiography: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J-Cardiovasc Imag. 2016;17(12):1321–1360. doi:10.1093/ehjci/jew082
21. Murdoch DR, McDonagh TA, Byrne J. Titration of vasodilator therapy in chronic heart failure according to plasma brain natriuretic peptide concentration: randomized comparison of the hemodynamic and neuroendocrine effects of tailored versus empirical therapy. Am Heart J. 1999;138(6):1126–1132. doi:10.1016/S0002-8703(99)70079-7
22. Solomon SD, Zile M, Pieske B, et al. The angiotensin receptor neprilysin inhibitor LCZ696 in heart failure with preserved ejection fraction: a Phase 2 double blind randomised controlled trial. The prospective comparison of ARNI with ARB in the management of heart failure with preserved ejection fraction. The Lancet. 2012;380(9851):1387–1395.
23. Hussain S, Kayani AM, Munir R. Effect of a regimen of optimal medical therapy on brain natriuretic peptide (BNP) levels in heart failure in the Pakistani population. Pak Heart J. 2012;45(1):17–21.
24. Maisel AS, Krishnaswamy P, Nowak RM, McCord J, Hollander JE, Duc P; For the Breathing Not Properly Multinational Study Investigators. Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure. N Engl J Med. 2002;347(3):161–167. doi:10.1056/NEJMoa020233
25. SOLVD Investigators. Effect of enalapril on survival in patients with reduced left ventricular ejection fractions and congestive heart failure. N Engl J Med. 1991;325(5):293–302.
26. Pitt B, Zannad F, Remme WJ; For the Randomized Aldactone Evaluation Study Investigators, et al. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. N Engl J Med. 1999;341(10):709–717. doi:10.1056/NEJM199909023411001
27. CIBIS-II Investigators and Committees. The Cardiac Insufficiency Bisoprolol Study II (CIBIS II): a randomised trial. Lancet. 1999;353(9146):9–13.
28. MERIT-HF Study Group. Effect of metoprolol CR/XL in chronic heart failure: metoprolol CR/XL randomised intervention trial in congestive heart failure (MERIT-HF). Lancet. 1999;353(9169):2001–2007. doi:10.1016/S0140-6736(99)04440-2
29. McMurray JJ, Packer M, Desai AS, et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med. 2014;371(11):993–1004. doi:10.1056/NEJMoa1409077
30. Heinrich K, Prendergast HM, Erickson T. Chronic digoxin toxicity and significantly elevated BNP levels in the presence of mild heart failure. Am J Emerg Med. 2005;23(4):561–562. doi:10.1016/j.ajem.2004.10.009
31. Mark D, Mark R, Nicholls MG, et al. Introduction of metoprolol increases plasma B-type cardiac natriuretic peptides in mild stable heart failure. Circulation. 2006;113(7):977–985. doi:10.1161/CIRCULATIONAHA.105.567727
32. Lancellotti P, Galderisi M, Edvardsen T, et al. Echo-Doppler estimation of left ventricular filling pressure: results of the multicentre EACVI Euro-filling study. Eur Heart J Cardiovasc Imaging. 2017;18(9):961–968. doi:10.1093/ehjci/jex067
33. Andersen OS, Smiseth OA, Dokainish H, et al. Estimating left ventricular filling pressure by echocardiography. J Am Coll Cardiol. 2017;69(15):1937–1948. doi:10.1016/j.jacc.2017.01.058
34. Balaney B, Medvedofsky D, Mediratta A, et al. Invasive validation of the echocardiographic assessment of left ventricular filling pressures using the 2016 diastolic guidelines: head-to-head comparison with the 2009 guidelines. J Am Soc Echocardiogr. 2018;31(1):79–88. doi:10.1016/j.echo.2017.09.002
35. Sato K, Grant AD, Negishi K, et al. Reliability of updated left ventricular diastolic function recommendations in predicting elevated left ventricular filling pressure and prognosis. Am Heart J. 2017;189:28–39. doi:10.1016/j.ahj.2017.03.022
36. Mak GS, DeMaria A, Clopton P, Maisel AS. Utility of b-type natriuretic peptide in the evaluation of left ventricular diastolic dysfunction: comparison with tissue Doppler imaging recordings. Am Heart J. 2004;148(5):895–902. doi:10.1016/j.ahj.2004.02.016
37. Ojji DB, Opie LH, Lecour S, et al. The proposed role of plasma NT pro-brain natriuretic peptide in assessing cardiac remodelling in hypertensive African subjects. Cardiovasc J Afr. 2014;25(5):233–238. doi:10.5830/CVJA-2014-050
38. Redfield MM, Rodcheffer RJ, Jacobsen SJ, et al. Plasma brain natriuretic peptide concentration: impact of age and gender. J Am Coll Cardiol. 2002;40(5):976–982. doi:10.1016/S0735-1097(02)02059-4
39. Madamanchi C, Alhosaini H, Sumida A, Runge MS. Obesity and natriuretic peptides, BNP and NT-proBNP: mechanisms and diagnostic implications for heart failure. Int J Cardiol. 2014;176(3):611–617. doi:10.1016/j.ijcard.2014.08.007
40. Yandle TG, Richards AM. B-type natriuretic peptide circulating forms: analytical and bioactivity issues. Clin Chem Acta. 2015;448(6):195–205. doi:10.1016/j.cca.2015.07.004
41. Martinez RA, Richards AM, Burnett JC, Januzzi JL
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.