Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Awareness, Stigma, and Cultural Beliefs About Diabetes: A Qualitative Study of Somali Patients and Families
Authors Mohamed AA ![]() , Jayte M, Abdi FD, Abdi I, Khalif A
, Jayte M, Abdi FD, Abdi I, Khalif A
Received 10 September 2025
Accepted for publication 23 November 2025
Published 27 November 2025 Volume 2025:18 Pages 4359—4366
DOI https://doi.org/10.2147/DMSO.S565175
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Melissa Olfert
Abdifitah Abdullahi Mohamed,1 Mohamed Jayte,2 Farah Dubad Abdi,2 Ilhan Abdi,1 Abdikani Khalif3
1Department of Microbiology, Kampala International University, Kampala, Uganda; 2Department of Internal Medicine, Kampala International University, Kampala, Uganda; 3Department of Paediatrics at Kampala International University, Kampala, Uganda
Correspondence: Mohamed Jayte, Internal Medicine Department at Kampala International University, P.O. Box 7062, Kampala, Uganda, Tel +256 55272543, Email [email protected]
Background: Diabetes mellitus is an escalating public health issue globally, with Africa facing a heavy burden due to weak health systems and scarce resources. In Somalia, limited data and deep-rooted cultural perceptions significantly influence disease understanding and management.
Methods: A qualitative descriptive design was employed between March and May 2025. In-depth interviews were conducted with diabetic patients and their family members using a semi-structured guide. Data were transcribed, translated into English, and thematically analyzed following Braun and Clarke’s framework.
Results: Awareness of diabetes varied widely. While some participants identified heredity, diet, and inactivity as causes, others attributed the disease to divine punishment, witchcraft, or the “evil eye.” Stigma was pervasive, with diabetes often compared to HIV/AIDS, resulting in concealment, social withdrawal, and delayed care-seeking. Cultural and spiritual beliefs strongly shaped treatment choices, with many resorting first to traditional healers, herbal remedies, or prayers. Families were both supportive and obstructive—offering care and financial aid but also perpetuating misconceptions and discouraging disclosure. Barriers to biomedical care included high insulin costs, medication shortages, long waiting times, and lack of culturally appropriate counselling. Participants expressed deep emotional distress, fear of complications, and loss of income due to illness.
Conclusion: Diabetes management in Somalia is deeply influenced by stigma, culture, and family dynamics. Culturally tailored education, family engagement, collaboration with traditional leaders, and stronger health system support are vital to improving care and outcomes.
Keywords: diabetes mellitus, cultural beliefs, stigma, family support, qualitative research, Somalia
Introduction
Diabetes mellitus (DM), often referred to as diabetes, is the fastest-growing chronic disease globally in the 21st century, causing disability and premature death among people within the most economic and productive age group.1 Diabetes has reached pandemic levels, with a prevalence rate of 10.5%, and accounted for 6.7 million deaths globally and 416,000 deaths in Africa in 2021.1,2 Most people with diabetes (432.7 million) live in lower- and middle-income countries, where they develop the disease earlier, experience higher morbidity, and die sooner than their counterparts in developed nations.2 The global number of adults aged 20–79 years living with diabetes rose from 151 million in 2000 to 537 million in 2021.1
In Africa, the burden is equally concerning. Approximately 24 million adults aged 20–79 were living with diabetes in 2021, representing a regional prevalence of 4.5%.2 Projections indicate that this number will rise by 129% to 55 million by 2045, making Africa the region with the highest expected increase worldwide.2 Despite this growing burden, awareness of diabetes remains low, with more than half of the affected population undiagnosed.2
In Somalia, diabetes has emerged as a growing public health challenge. According to the International Diabetes Federation, the prevalence of diabetes among Somali adults aged 20–79 was estimated at 5.2% in 2019,3 and up to 24% among psychiatric patients.3 The coexistence of weak healthcare infrastructure, limited resources, and cultural misconceptions further complicates diabetes management in Somalia.
Across the broader NCD spectrum—such as hypertension, cardiovascular diseases, and cancer—studies in sub-Saharan Africa have shown that stigma, fatalistic beliefs, and social misconceptions hinder diagnosis, disclosure, and adherence to treatment. Similarly, traditional and spiritual beliefs often compete with biomedical explanations, shaping health-seeking behaviors and delaying appropriate care. Family structures also play a crucial role, acting as both sources of emotional and financial support and as channels for reinforcing cultural interpretations of illness.4
Despite the growing prevalence of diabetes in Somalia, there is limited research exploring how cultural beliefs, stigma, and family dynamics influence diabetes awareness and management. This study seeks to fill that gap by examining awareness, stigma, and cultural beliefs about diabetes among patients and their families in Mogadishu. By addressing the social and cultural dimensions of diabetes—a rarely explored area in Somalia—this study provides novel insights that can inform culturally sensitive policies and interventions. Findings will be shared with the Somali Ministry of Health and other stakeholders to guide national strategies for diabetes prevention and control.
Methods
Study Area and Design
The study took place at Deynile Hospital, a regional facility in Mogadishu serving urban and peri-urban populations. We used a qualitative descriptive design with reflexive thematic analysis (Braun & Clarke). We selected this approach because it preserves participants’ accounts in accessible language while allowing in-depth interpretation of shared meanings and patterns—appropriate for exploring lived experiences, cultural beliefs, stigma, and family roles around diabetes in this context.
Participants, Sampling and Sample Size
Participants were purposively sampled to capture a range of experiences (maximum-variation sampling by sex, age, illness duration, education, and socioeconomic background). Inclusion criteria: adults (≥18 years) diagnosed with type 2 diabetes for ≥6 months and their primary family caregivers who provided regular support. Exclusion criteria: critically ill patients, those with severe cognitive impairment, and people with only type 1 diabetes (to keep the sample clinically homogeneous). Recruitment continued until data saturation, defined a priori as no new codes or themes emerging across three consecutive interviews. Saturation was reached after 20 interviews; two additional interviews were completed to confirm theme stability, giving a final n = 22 (14 patients, 8 family members). During recruitment, four eligible individuals declined participation (refusals logged). No material incentives were offered; participants received refreshments and travel reimbursement per local ethics guidance.
Data Collection Procedures
Data were collected March–May 2025 using semi-structured in-depth interviews and two small focus group discussions to explore shared social meanings. The interview guide (open-ended prompts on knowledge, causes, help-seeking, stigma, family roles, emotional impact, and barriers) was developed from literature and expert input, and pretested with two patients and one caregiver at a nearby clinic; minor wording and flow edits were made. Interviews lasted 30–60 minutes and were conducted in a private room at the hospital at times chosen by participants to maximise comfort. The primary interviewer was not part of the patients’ clinical team to reduce power dynamics. Sessions were audio-recorded with consent; detailed field notes captured non-verbal cues and context.
Translation, Transcription and Quote Validation
Interviews conducted in Somali were transcribed verbatim in Somali and then translated into English. Translation was performed by a bilingual research assistant with formal training in translation and experience in health research. A second independent bilingual translator back-translated selected transcripts; discrepancies were reconciled through discussion with the study team. To reduce translation bias, key participant quotations used in the manuscript were checked against the original Somali transcripts and presented to participants during member-checking (see below) for validation of meaning.
Data Analysis and Reflexivity
We used reflexive thematic analysis per Braun & Clarke. Transcripts were read repeatedly for immersion, coded inductively in NVivo 12, and codes iteratively grouped into candidate themes. Coding and theme development were led by the primary analyst and reviewed in regular consensus meetings with a second coder; disagreements were resolved through discussion and reference to the data. Reflexive journaling was maintained by researchers to document assumptions, decisions, and potential biases; an audit trail recorded coding memos, theme evolution, and analytic decisions. To enhance dependability, a sample of transcripts was double-coded and coding consistency discussed.
Trustworthiness and Rigor
We applied strategies to strengthen credibility, transferability, dependability and confirmability: investigator triangulation (multiple analysts), method triangulation (interviews + FGDs + field notes), peer debriefing with qualitative experts, thick descriptions of context, and an audit trail. Member checking involved sharing a thematic summary with six purposively selected participants (patients and caregivers) to confirm interpretations and to validate selected quotations. We adhered to reporting standards using the COREQ 32-item checklist (completed and available on request).
Results
Participants’ Characteristics
A total of 22 participants were interviewed, including 14 patients with diabetes and 8 family caregivers. Participants’ ages ranged from 28 to 72 years. Of the patients, 8 were female and 6 male. Most participants had completed primary or secondary education, while 3 had tertiary education. Occupations included farmers, traders, civil servants, and housewives. Family caregivers were spouses, children, and siblings actively involved in patients’ daily care and adherence to treatment (Table 1).
 |
Table 1 Background Information of Participants in in-Depth Interviews (IDI) |
Emergent Themes and Categories
Analysis of interviews and focus group discussions revealed seven main themes, each with multiple categories, capturing patients’ and families’ experiences with diabetes as showing Table 2.
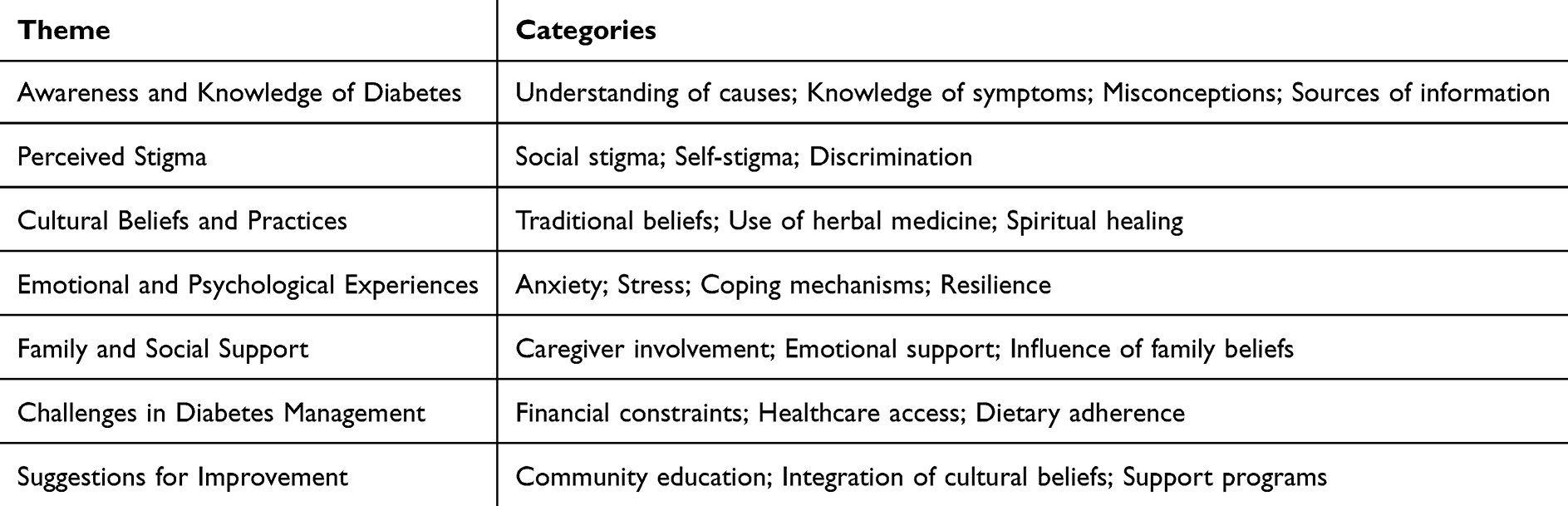 |
Table 2 Emergent Themes and Categories |
Awareness and Knowledge of Diabetes
Participants demonstrated varying levels of knowledge about diabetes, influenced by medical advice, family experience, and community beliefs.
Understanding of Causes
Most patients recognized diabetes as related to diet, heredity, and lifestyle, though some also attributed it to spiritual causes.
Patient:I know diabetes is about high sugar in the blood, but some say it comes from curses or spirits – 48-year-old female patient.
Family member:We think it can come from wrongdoings or envy, but we follow the doctor’s advice too – 52-year-old male caregiver.
Knowledge of Symptoms
Fatigue, frequent urination, excessive thirst, and weight loss were commonly mentioned.
Patient:I was always tired and thirsty; that is why I went to the hospital – 54-year-old male patient.
Family member:I noticed my mother drinking a lot and feeling weak, so we brought her to the clinic – 45-year-old daughter.
Misconceptions
Some participants believed diabetes was contagious or caused by spiritual attacks.
Patient:Some in my village think diabetes is from spirits – 60-year-old male patient.
Family member:People say it’s a curse, but we still follow hospital treatment – 38-year-old female caregiver.
Sources of Information
Knowledge came from healthcare providers, family members, and community discussions.
Patient:I learned about my diet from the nurse, but neighbors also advise me about herbs – 60-year-old female patient.
Family member:We get advice from doctors and elders about taking care of patients – 35-year-old male caregiver.
Perceived Stigma
Stigma affected both social interactions and self-esteem among patients.
Social Stigma
Patient:I hide my condition because people think I am cursed or weak – 36-year-old male patient.
Family member:Neighbors avoid inviting her to gatherings; they act as if she is contagious – 44-year-old female caregiver.
Self-Stigma
Patient:I feel ashamed to tell anyone I have diabetes – 50-year-old female patient.
Family member:He does not want anyone to know; he is embarrassed – 38-year-old female caregiver.
Discrimination
Patient:At work, they look at me differently after knowing I have diabetes – 50-year-old female patient.
Family member:People treat my brother differently, thinking he cannot do his usual work – 42-year-old male caregiver.
Cultural Beliefs and Practices
Participants often combined biomedical treatment with traditional and spiritual practices.
Traditional Beliefs
Patient:Part of my diabetes comes from family curses, so I also pray – 60-year-old male patient.
Family member:We follow rituals alongside hospital treatment – 38-year-old female caregiver.
Use of Herbal Medicine
Patient:I combine hospital medicine with herbs; both help me recover – 60-year-old male patient.
Family member:I prepare herbal remedies with prescribed medicines to support my father – 52-year-old male caregiver.
Spiritual Healing
Patient:I pray daily and take my medicine; both help – 54-year-old female patient.
Family member:We encourage him to pray and follow treatment; both are important – 35-year-old female caregiver.
Emotional and Psychological Experiences
Anxiety
Patient:I worry when my sugar is high even after taking medicine – 54-year-old female patient.
Family member:I feel anxious seeing my mother weak; I worry about her – 45-year-old female caregiver.
Stress
Patient:Managing diet, medicines, and checking sugar is stressful – 42-year-old male patient.
Family member:Supporting him daily is stressful – 38-year-old female caregiver.
Coping Mechanisms
Patient:I rely on my children and prayers to manage stress – 62-year-old male patient.
Family member:We talk and encourage him to take medicines – 35-year-old female caregiver.
Resilience
Patient:Even though it is difficult, I try to follow advice and keep sugar under control – 50-year-old female patient.
Family member:Despite challenges, we ensure he continues treatment – 52-year-old male caregiver.
Family and Social Support
Caregiver Involvement
Patient:My children remind me to take my medicine and sometimes accompany me to the hospital – 62-year-old male patient.
Family member:I monitor my mother’s medications and meals – 45-year-old female caregiver.
Emotional Support
Patient:Family encouragement keeps me motivated – 54-year-old female patient.
Family member:We try to make him feel supported – 35-year-old female caregiver.
Influence of Family Beliefs
Patient:My spouse believes in herbs, so we use them with hospital medicine – 48-year-old female patient.
Family member:We combine cultural practices with medical advice for better care – 38-year-old female caregiver.
Challenges in Diabetes Management
Financial Constraints
Patient:Insulin is expensive; sometimes we cannot afford it – 48-year-old male patient.
Family member:It is hard to pay for medicines every month – 52-year-old male caregiver.
Healthcare Access
Patient:The hospital is far; transport costs delay visits – 50-year-old female patient.
Family member:We travel long distances for appointments; it is exhausting – 45-year-old female caregiver.
Dietary Adherence
Patient:It is hard to follow the recommended diet at home – 54-year-old female patient.
Family member:Preparing special meals is difficult when the family eats traditional foods – 38-year-old female caregiver.
Discussion
This study explored how awareness, stigma, and cultural beliefs shape diabetes experiences among patients and families at Deynile Hospital, Mogadishu. Participants showed partial biomedical understanding of diabetes, often blended with spiritual and supernatural explanations such as witchcraft, envy, or divine punishment. These beliefs influenced early help-seeking, with many combining biomedical treatment with traditional or faith-based remedies. Diabetes was also highly stigmatized—frequently associated with HIV/AIDS or death—leading to concealment, shame, and delayed care. Families played dual roles: providing essential financial and emotional support while sometimes reinforcing misconceptions or fear. Structural barriers such as high costs of medicines, long travel distances, poor communication, and lack of refrigeration for insulin further limited adherence and continuity of care.
These patterns mirror findings from other African contexts where chronic diseases like hypertension, cancer, and cardiovascular disease are entangled with cultural beliefs and stigma that delay biomedical engagement.1–3 The coexistence of biomedical and spiritual explanatory models—observed in West and East Africa—illustrates that awareness alone does not ensure timely care or adherence without culturally congruent education and family engagement.2,5
Traditional and herbal remedies were commonly used, often viewed as spiritually “cleansing” or safer alternatives to insulin. Similar practices have been documented across sub-Saharan Africa, driven by accessibility, cost, and distrust of formal care.4 Engaging trusted traditional and faith healers through dialogue and safe referral mechanisms may therefore enhance care-seeking and minimize harmful delays.
Stigma emerged as a central theme linking cultural beliefs, social exclusion, and psychological distress. As seen across NCD literature, stigma reduces self-care and increases social withdrawal. Interventions targeting stigma—such as community dialogues, peer-support networks, and culturally framed public messaging—are essential for early diagnosis and sustained management.3,5
Family involvement significantly shaped coping and treatment outcomes. Evidence from other African studies supports family-centered interventions, which improve adherence and glycemic control.5,6 Structured family education and inclusion in counselling sessions can strengthen understanding and reduce misconceptions.
Participants also expressed profound emotional distress, echoing high rates of depression and anxiety among diabetic patients in similar contexts.3,7 Integrating simple screening tools (eg, PHQ-2, DASS) and basic psychosocial support within diabetes clinics could help address these unmet needs.
Health-system barriers—costly or unavailable medicines, clinic delays, and transport difficulties—directly constrained self-management. Strengthening supply chains, subsidizing essential drugs, decentralizing insulin distribution, and improving provider–patient communication are actionable steps to improve adherence and outcomes.8–10
The study’s strength lies in its inclusion of both patients and family members, offering holistic insights into social and cultural dynamics. However, as a single-site qualitative study, findings may not be generalizable to all Somali regions. Social-desirability bias may have influenced some responses, particularly on stigma and faith practices. Nonetheless, thematic convergence with regional literature enhances the credibility and transferability of findings.
Recommendations
Improving diabetes care in Somalia requires culturally sensitive, multi-level strategies. Education should integrate biomedical knowledge with local beliefs, involving families, community leaders, and traditional healers. Stigma-reduction campaigns, family-inclusive counselling, and engagement with trusted healers can promote timely care. Strengthening health systems—ensuring medicine availability, affordability, and access—and integrating basic psychosocial support are essential to improve adherence, early diagnosis, and long-term outcomes.
Strengths and Limitations
This study provides a nuanced understanding of diabetes in Somalia by including both patients and family members, capturing social, cultural, and familial influences on health behaviours. Reflexive thematic analysis, member checking, and triangulation enhanced credibility, offering context-specific insights for culturally sensitive interventions. Limitations include the single-hospital design, purposive sampling, potential social-desirability.
Conclusion
This study explored awareness, stigma, and cultural beliefs surrounding diabetes among patients and families at Deynile Hospital, Mogadishu. Findings show that diabetes is perceived through both biomedical and supernatural lenses, with stigma often tied to HIV-related misconceptions and fear of social exclusion. Families strongly influence health-seeking behaviour, sometimes enabling treatment but also perpetuating myths.
These insights highlight the need for culturally sensitive interventions that engage patients, families, community leaders, and traditional healers. Reducing stigma, enhancing public awareness, and ensuring affordable access to medicines and psychosocial support are essential to strengthen diabetes care in fragile settings like Somalia. Integrating cultural understanding into health services can promote early diagnosis, improve adherence, and ultimately reduce preventable complications and improve quality of life.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
Ethical approval was obtained from the Somalia Ministry of Health, Institutional Review Board, under reference number MH-S130089B. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki. Written informed consent to participate was obtained from all participants prior to enrollment.
Consent for Publication
Written informed consent was obtained from all participants, which included consent for publication of anonymized responses and direct quotes.
Author Contributions
Mohamed Jayte (MJ): Conceptualization, Methodology, Investigation, Data Curation, Writing – Original Draft.
Abdifitah Abdullahi Mohamed (AAM): Formal Analysis, Writing – Review & Editing.
Abdikani Kalif (AK): Investigation, Resources, Writing – Review & Editing.
Ilhan Abdi (IA): Investigation, Writing – Review & Editing.
Farah Dubad Abdi (FDA): Supervision, Methodology, Validation, Writing – Review & Editing.
All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study did not receive any funding.
Disclosure
The authors declare that they have no competing interests.
References
1. International Diabetes Federation. IDF Diabetes Atlas.
2. World Health Organization. Global report on diabetes. Geneva: WHO; 2016.
3. Atun R, Davies JI, Gale EAM, et al. Diabetes in sub-Saharan Africa: from clinical care to health policy. Lancet Diabetes Endocrinol. 2017;5(8):622–667. doi:10.1016/S2213-8587(17)30181-X
4. Pastakia SD, Pekny CR, Manyara SM, Fischer L. Diabetes in sub-Saharan Africa – from policy to practice to progress: targeting the existing gaps for future care for diabetes. Diabetes Metab Syndr Obes. 2017;10:247–263. doi:10.2147/DMSO.S126314
5. Hjelm K, Mufunda E. Zimbabwean diabetics’ beliefs about health and illness: an interview study. BMC Int Health Hum Rights. 2010;10(1):7. doi:10.1186/1472-698X-10-7
6. Kolo ES, Babatunde OA, Chijioke A, Balogun MO. Perception of diabetes and adherence to treatment among patients in north-central Nigeria. Niger J Clin Pract. 2017;20(4):454–460. doi:10.4103/1119-3077.196120
7. Nam SL, Fielding K, Avalos A, Dickinson D, Geissler PW, Grant AD. The relationship of diabetes stigma with illness management and health-seeking behaviour in South Africa: a qualitative study. BMC Public Health. 2021;21(1):1640. doi:10.1186/s12889-021-11665-0
8. Sobngwi E, Ndour-Mbaye M, Boateng KA, et al. Type 2 diabetes control and complications in specialised diabetes care centres of six sub-Saharan African countries: the Diabcare Africa study. Diabet Res Clin Pract. 2012;95(1):30–36. doi:10.1016/j.diabres.2011.10.018
9. Osei-Yeboah J, Owiredu WKBA, Norgbe GK, et al. Perceptions and beliefs about the causes of diabetes among patients attending a specialist clinic in Ghana. BMC Public Health. 2020;20:830.
10. Fekadu A, Alem A, Shibre T, Fekadu D. Perception, attitudes and treatment-seeking behaviour of diabetes patients in Jimma, southwest Ethiopia: a qualitative study. BMC Endocr Disord. 2010;10:15. doi:10.1186/1472-6823-10-15
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
“If I Wear Glasses, I Will Go Blind”: Misconceptions, Stigma, and Nonadherence to Spectacle Wear in Somalia’s Outpatient Eye Clinics
Mohamed AA, Omar AA, Hassan Orey FA
Clinical Optometry 2026, 18:601110
Published Date: 30 April 2026
Polypharmacy Experience of Middle-Aged and Elderly Patients with Type 2 Diabetes Comorbidity: A Qualitative Study
Han Z, Wang L
Patient Preference and Adherence 2026, 20:605584
Published Date: 9 July 2026