")
Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 11
Awareness of Dental Esthetic Standards Among Dental Students and Professionals
Authors Al-Saleh SA , Al-Shammery DA, Al-Shehri NA, Al-Madi EM
Received 23 July 2019
Accepted for publication 13 November 2019
Published 2 December 2019 Volume 2019:11 Pages 373—382
DOI https://doi.org/10.2147/CCIDE.S224400
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Samar A Al-Saleh,1 Deema A Al-Shammery,2 Nada A Al-Shehri,3 Ebtissam M Al-Madi4
1Department of Prosthetic Dental Science, College of Dentistry, King Saud University, Riyadh 11527, Saudi Arabia; 2Department of Preventive Dentistry, College of Dentistry, Riyadh Elm University, Riyadh, Saudi Arabia; 3Division of Orthodontics, Department of Preventive Dental Sciences, College of Dentistry, Princess Nourah Bint AbdulRahman University, Riyadh, Saudi Arabia; 4Department of Restorative Dental Sciences, College of Dentistry, King Saud University, Riyadh 11527, Saudi Arabia
Correspondence: Ebtissam M Al-Madi
Department of Restorative Dentistry, College of Dentistry, King Saud University, Saudi Arabia
Email [email protected]
Purpose: This study investigated the level of esthetic awareness of dental students and professionals.
Material and methods: Photographs depicting facial and smile features that deviate from universally accepted esthetic standards were presented in a questionnaire. Participants were asked to rate the images and to identify the main discrepant criteria. Eight hundred questionnaires were distributed to dental students, and clinicians. The data were analyzed using chi-square tests, Student’s t-test and one-way ANOVA with Tukey’s post hoc tests for multiple comparisons.
Results: Students had 45.2% correct answers compared to 51.6% for clinicians. Among students, the highest awareness was found among 5th year students, followed by interns, 4th year and 3rd year students. The difference in the percentage of correct answers between clinicians and students overall was significantly higher for some criteria than for others, such as gingival esthetics, lip features, smile zone (incisal plane), facial features, and buccal corridor. Among clinicians, specialists responded correctly more often than did general practitioners in most of the investigated aspects.
Conclusion: The ability of different group samples to diagnose discrepancies of smile esthetics was refined and enhanced with increased clinical experience and knowledge.
Keywords: dental esthetic standards smile features, dental education, esthetic awareness, smile zone
Introduction
An attractive smile is a key feature in maintaining and improving a person’s esthetic appearance and, consequently, self-esteem.1 In addition, a smile has been described as one of the best methods to influence people.2,3 Even though societies dictate their own standards for beauty, meticulous analysis of attractive smiles has shown that repeatable, quantifiable, and unbiased principles can be methodically applied to assess and improve dental esthetics in predictable ways.4 These principles were defined through data collected from basic artistic concepts of beauty, scientific measurements, dental research, diagnostic models, and patients from all over the world.
An esthetically pleasing smile requires an integration of esthetic concepts that harmonize dental composition, dental facial esthetics, and facial esthetics (Davis 2007). Among the facial features that have an important impact on the attractiveness of the smile are facial height, shape, and profile, and particularly, the inter-pupillary plane.5,6 The lips and smile, as they relate to the face, are the main features constituting dental facial esthetics (Ahmad 1998). Lips create the boundaries of the smile, and analysis of the lips should include morphology, curvature and position of the upper lip, relationship between the maxillary anterior teeth and the lower lip, parallelism of the anterior incisal curve with the lower lip, and amount and number of teeth displayed in the smile.6,7 The dental composition includes the position, size, proportion, and shape of the teeth; midline symmetry; and the relationship of the teeth to the gingival tissues and alveolar bone.1,4,6,8 Familiarity with esthetic criteria can help to improve the esthetic condition of the oral and maxillofacial region, particularly given the increased demand for cosmetic dentistry.7,9,10
Since beauty is a highly subjective issue, the esthetic appearance of a patient’s smile mainly depends on what a clinician perceives as beautiful. Therefore, establishing esthetic guidelines can greatly reduce misunderstanding and unneeded treatment and improve outcomes. Knowledge of the different aspects of dental structures and the ability to harmonize the teeth with the patient’s face will help to create esthetically pleasing restorations.11 Many studies have illustrated some starting points to help clinicians diagnose dental esthetic problems, in order to achieve maximum esthetics in dental treatment.12–14
Typically, dental students are required to treat patients’ anterior teeth with cosmetically restorative or prosthetic procedures during their undergraduate training. Knowledge of esthetic criteria and standards is important to guide them in providing treatment, given that they lack practical experience and have not yet developed a trained and observant eye that can readily detect asymmetry or imbalances, as described by Miller.15 Education seems to have a significant influence on esthetic perception and subsequent recommendation for treatment needs.16
The teaching of esthetic dentistry principles varies among dental schools.17 Not many studies have evaluated students’ knowledge on esthetic dentistry gained through teaching provided in dental colleges.18–20 The aim of this study was thus to compare the awareness of variation from ideal esthetic standards among dental students at differing levels of training, general dental practitioners, and dental specialists, as well as to evaluate the ability of the different dental professionals to identify discrepant esthetic criteria. The hypothesis is that students and general dentists have a lower level of awareness of variation from ideal esthetic standards compared to dental specialists, while the null hypothesis is that there is no difference between the different groups.
Materials and Methods
This was a cross-sectional observational study and was approved by Princess Noura bint AbdulRahman University institutional review board (IRB# 18–0186). A color-print questionnaire was developed in English. A statement was included in the questionnaire to clarify the anonymity of the response, as well as the freedom to participate and withdraw at any time, as well as the statement that agreement to respond equated informed consent. It recorded demographic data about the participants, including age, sex, occupational status (dental student, general practitioner, or specialist), dental school and academic year for students, and years of experience for dentists.
The questionnaire was designed to examine awareness of eight different esthetic discrepancies. It consisted of 23 randomized color images of smiles and faces portraying several common esthetic discrepancies. Only two of these images had no clear discrepancies. The esthetic deviations were selected based on the universally accepted esthetic standards, which include the following: facial features (including profile and facial height), lip features (including lip line and fullness), smile zone (including teeth displayed, smile line, and occlusal plane), gingival features (including the amount of tooth displayed, gingival margin, and gingival embrasure), tooth features (including the proportion, shape, and incisal embrasure), buccal corridor, midline shifts, and tooth alignment. The images were taken from different publications. The images were adjusted and cropped to a standardized size, and the nose and chin were removed from the smiling images. The images were grouped randomly, and each page consisted of six images. Figures 1 and 2 represent an example of the investigated items. The questionnaires were presented to three specialists who have more than 15 years in esthetic dentistry practice and asked if each image presented the main deviation from the esthetic standards that it intended to measure. Any unclear items were discussed and then changed or replaced with a clearer image. A pilot trial of 10 participants of the target population was done to assess the clarity and reliability of the questionnaire. The participants included in the pilot were not included in the study.
 |
Figure 1 An image with low lip line representing deviation from lip features ideal esthetic standards. |
 |
Figure 2 A smile image with excessive gingival display representing deviation from gingival ideal esthetic standards. |
A numerical scale ranging from 1 to 10 was placed under each of the images and participants were instructed to rate the images, with 1 being the least esthetic and 10 being the most esthetic, according to the participants knowledge and experience. The participants were asked to identify the main unaesthetic aspect of each image. A letter index was included to indicate the esthetic deviations included in the study (Table 1). An ideal smile would be marked as letter I. The possible index descriptions were printed on the top of each page for the raters’ convenience.
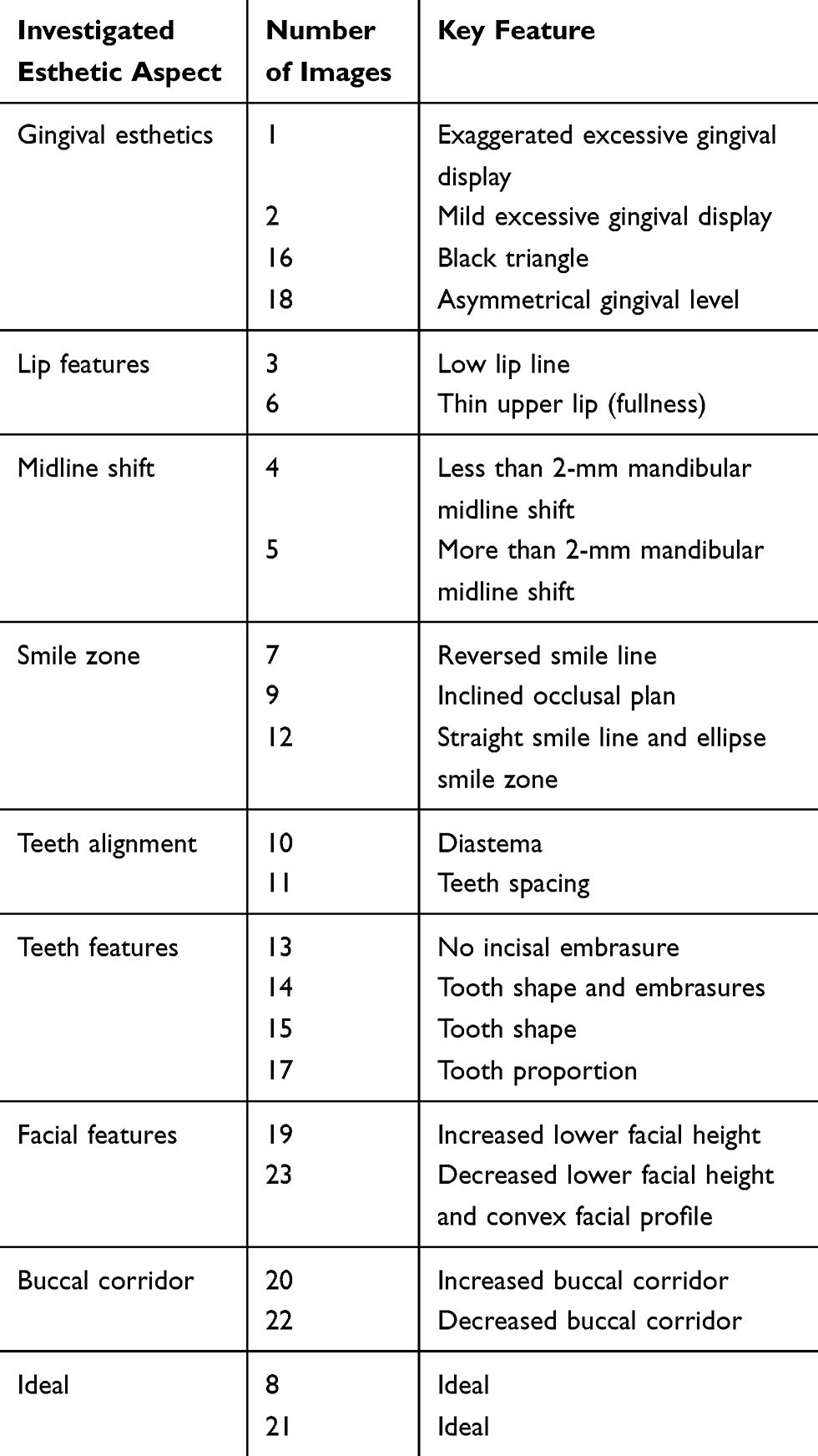 |
Table 1 Discrepant Features of Each Investigated Esthetic Aspect |
The research participants were selected using convenience sampling. The sample population consisted of two groups: dental students at various levels of training and clinicians with different levels of experience. Eight-hundred color-print questionnaires were distributed to two dental schools (public and private) and the main governmental hospitals in Riyadh city. Clinicians included general dental practitioners and specialists in the field of prosthodontics, restorative dentistry, and orthodontics. All undergraduate students who had successfully completed at least 2 years of dental school were asked to participate in the study.
Statistical Analysis
Data were entered and analyzed using statistical package SPSS version 16.0 (SPSS, Inc., Chicago, IL, USA). Mean, standard deviation, and proportion were used to describe the quantitative and qualitative outcome variables. The number of accurate responses for each individual image and investigated aspect was presented in the form of frequency and percentage. Chi-square tests were used to compare proportions of correct responses between subgroups. When overall significant findings were found for more than two subgroups, post hoc analysis with Bonferroni correction was performed to determine which subgroups were statistically different. Independent sample t-tests were used to compare mean scores between two subgroups. For more than two subgroups, one-way analysis of variance (ANOVA) followed by Tukey’s post hoc tests were used when overall significant differences were found. Interclass correlation coefficient was used to evaluate the measure of agreement between students, GPs, professionals in regard to aesthetic ration scores and percentage of correct responses. All inferential analysis was performed with p-values < 0.05 considered as statistically significant.
Results
The questionnaire was completed by 415 of the target group, with a response rate of 51.8%. The ability of all respondents from the different groups to identify the main discrepant features in terms of each investigated esthetic aspect and individual photograph was presented as the frequency of correct diagnosis selection (Tables 2 and 3). Generally, clinicians were more capable of identifying the discrepant features than were students. This ability was significantly higher in the following aspects: gingival esthetics (p = 0.021), midline shift (p = 0.009), tooth features (p = 0.033), facial features (p = 0.004), and buccal corridor (p = 0.001). As the students advanced academically, their ability to evaluate dental esthetics improved.
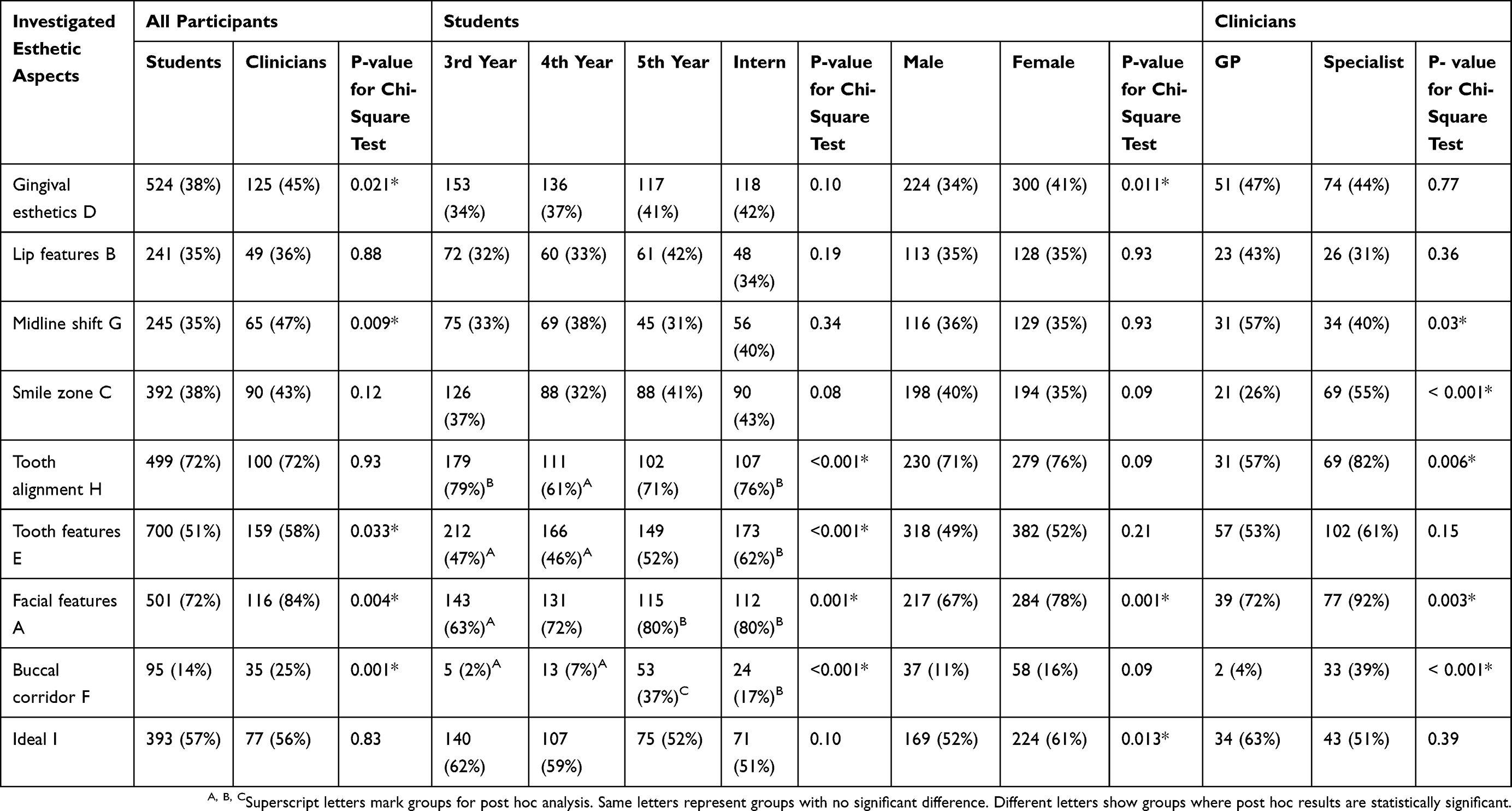 |
Table 2 Frequency and Percentage of Accurate Responses of All Participants to the Investigated Esthetic Aspects |
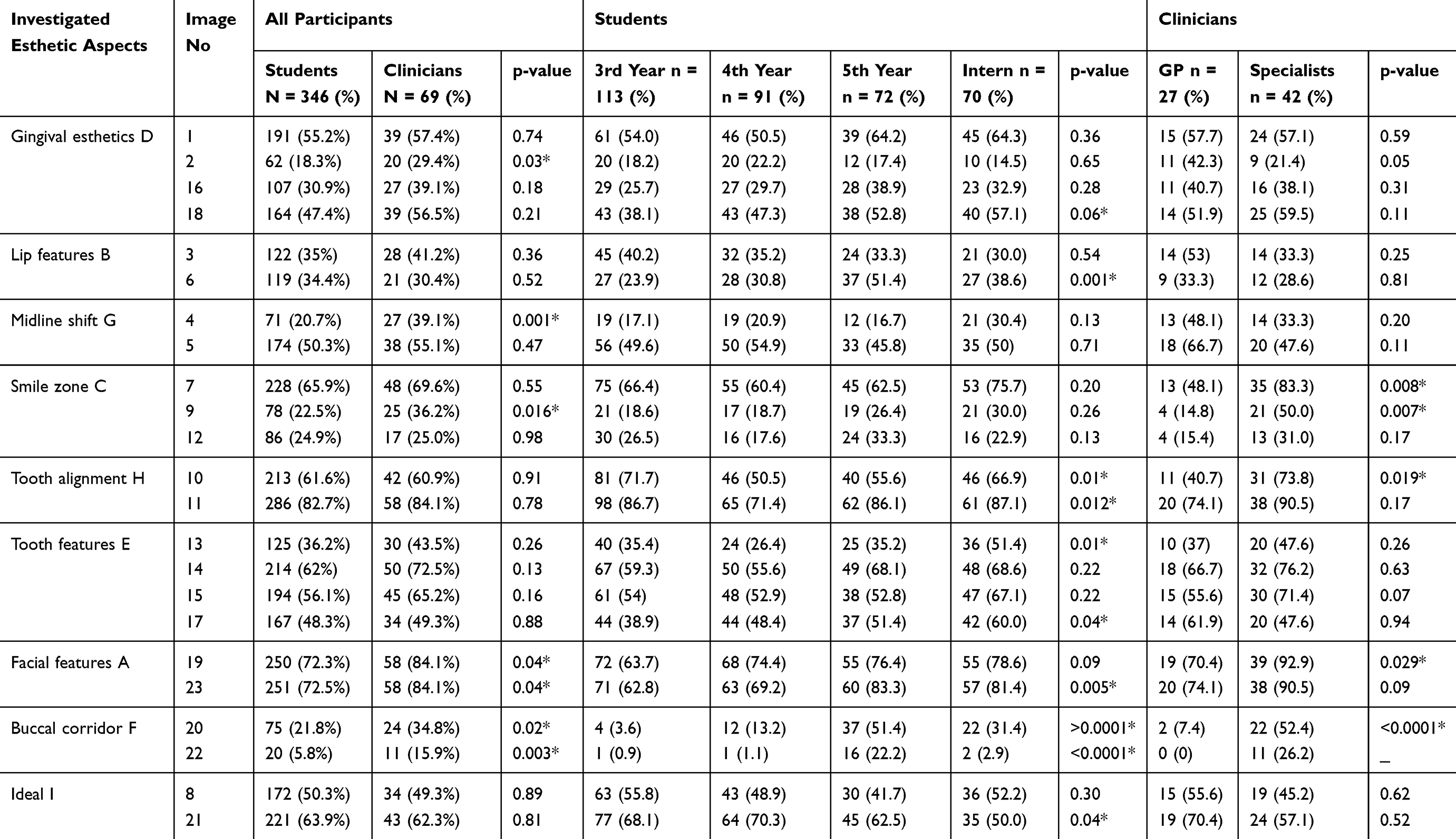 |
Table 3 Frequency and Percentage of Accurate Responses of All Participants for Individual Images |
Examining the individual images revealed that students were less capable of diagnosing mild problems in gingival esthetics, specifically lip feature and midline shift aspects. On the other hand, diagnosis of discrepancies related to tooth proportions and alignment was comparable between students and clinicians. In general, aspects related to buccal corridor, facial height and profile, and occlusal plane were less often identified by students than by clinicians. The specialists’ ability to diagnose discrepant features was significantly higher than that of general practitioners in some discrepant aspects, including facial features, buccal corridor, tooth alignment, and occlusal plane orientation.
The esthetic perceptions of the respondents for each aspect examined and for each image are presented in Tables 4 and 5. Generally, clinicians rated all images, including ideal smiles, as less esthetic than students did.
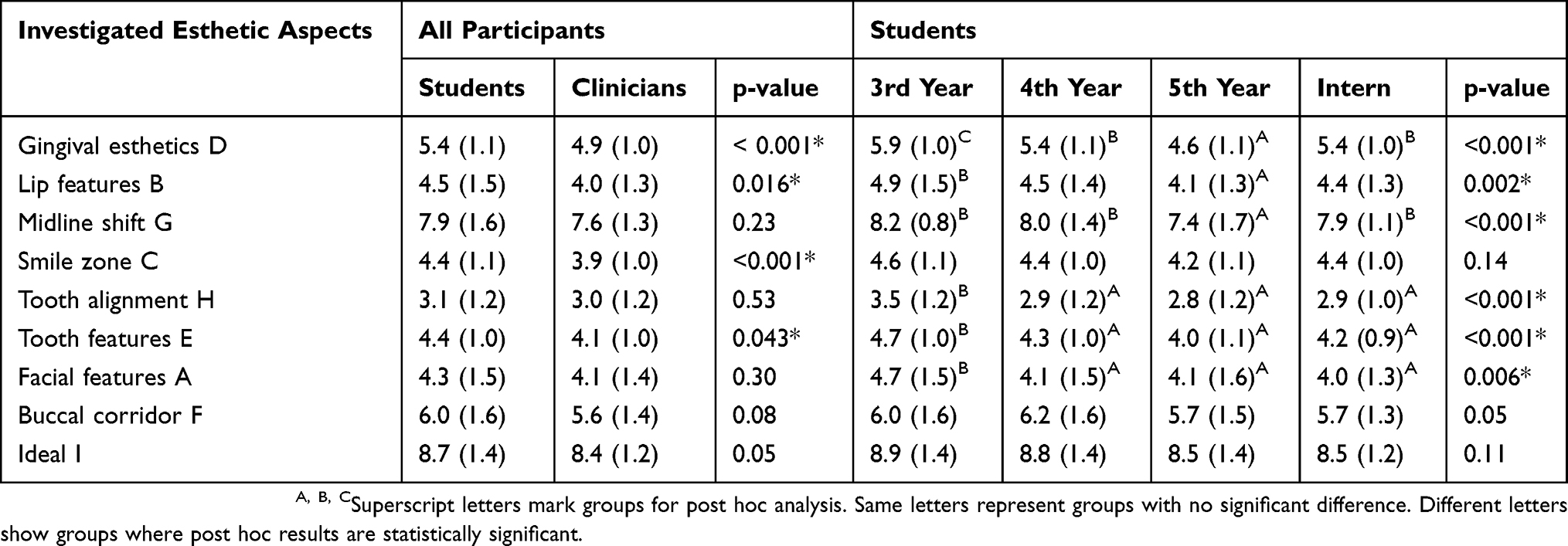 |
Table 4 Mean and Standard Deviation of Participants’ Perception of the Different Esthetic Aspects |
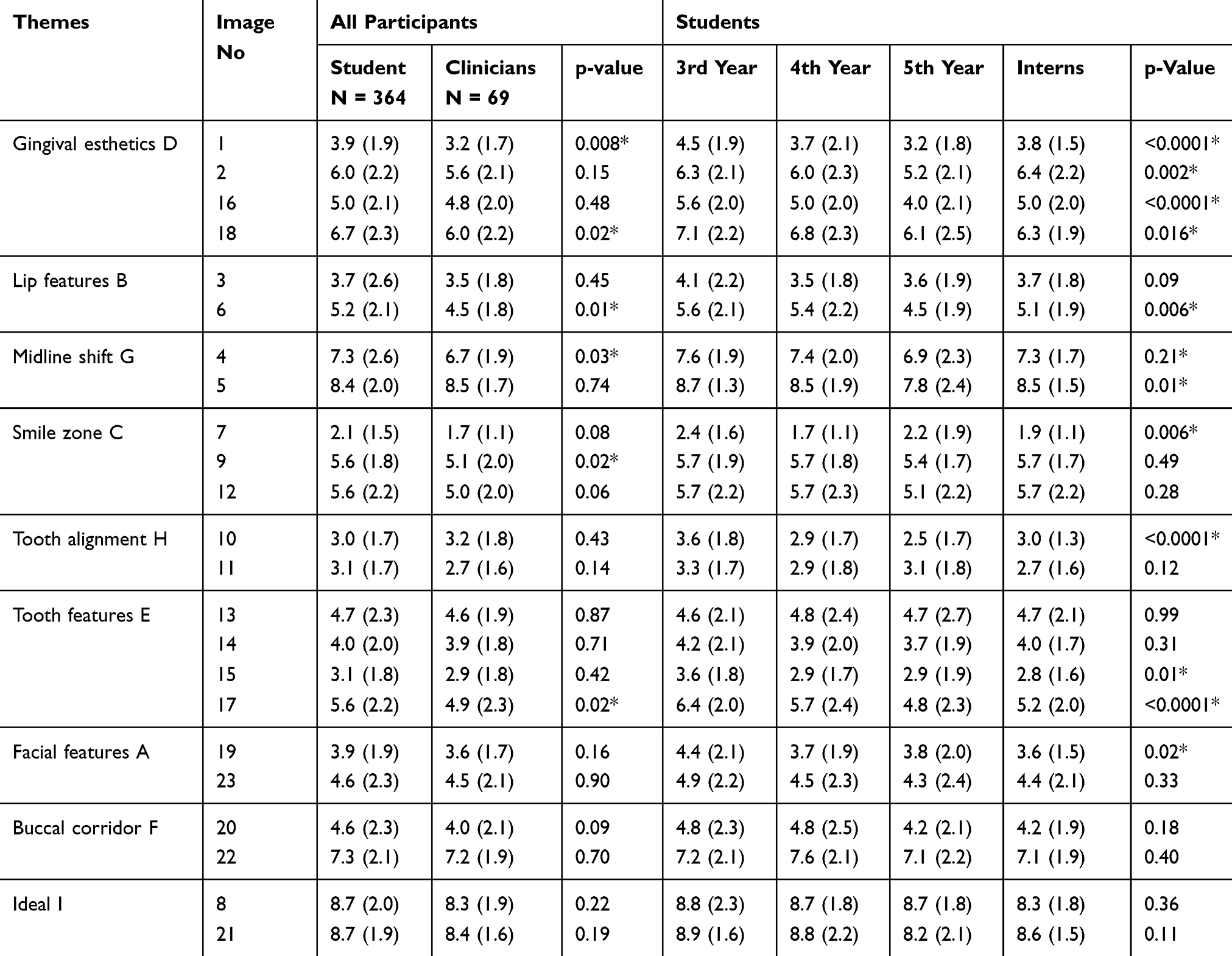 |
Table 5 Mean and Standard Deviation of Participants’ Perception of the Esthetics of Individual Images |
Interclass correlation coefficient (ICC) was used to evaluate the level of agreement between subgroups of study participants (students, GPs, professionals) as shown in Table 6. It shows the degree of consistency between two groups for a group of 23 photos. All ICC values were high (well above 0.8), indicating excellent inter-group reliability in regard to aesthetic ration scores. Students/clinicians and students/professionals also showed excellent inter-group reliability in regard to percentage correct. Only GPs vs professionals showed moderate degree of inter-group reliability (ICC = 0.748).
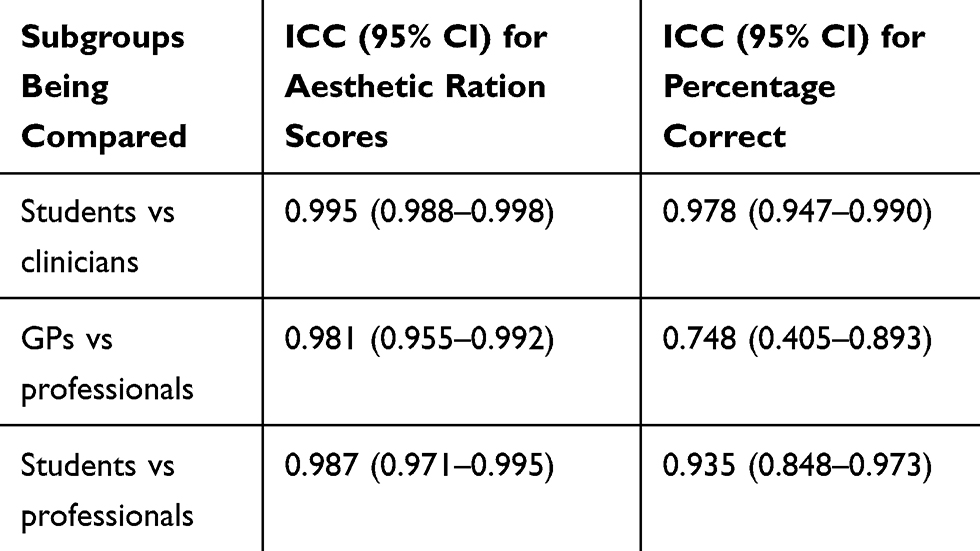 |
Table 6 ICC Values for Various Combinations of Subgroups |
Discussion
It is the responsibility of dental schools to ensure graduation of knowledgeable clinicians equipped to practice dentistry independently. Esthetic dentistry is currently receiving increased attention in dental practice. Many studies and digital smile analysis programs have attempted to formulate a protocol for helping dentists assess smile esthetics to reach an accurate diagnosis and to plan the required treatment.6,12,21,22 To the best of our knowledge, no studies to date have assessed the ability of dental students to analyze and identify various esthetic discrepancies. Most available studies have investigated perceptions of different groups of smiles. These studies have mainly focused on rating smile attractiveness without determining variables that effectively define the discrepancies that compromise the attractiveness of a smile. Many factors can influence perception of esthetics including emotions, motivation, context or setting, cultural background, and past experiences.14,23,24 Diagnosis of smile discrepancies can help a dentist to explain the needed treatment to the patient and to formalize an effective treatment plan.
The validity of using photographic images as an accurate means of smile evaluation has been debated. A smile is a complex and dynamic movement encompassing the interaction of numerous facial muscles that collectively produce various positions of the dento-labial architecture. On the other hand, practice has shown that photographic protocols afford coherent smile data and are an acceptable communication means between clinicians and patients, providing reliable data for favorable esthetic treatment planning.12
In general, the ability to identify a deviation from the ideal in this study was higher among clinicians than among students and increased as the level of education increased. This could be explained by the effect of clinical practice and increased knowledge and experience on refining the capability of dentist to recognize a deviation from the ideal.
Gingival esthetics is an important component of an attractive smile. Esthetic restorations surrounded by with unaesthetic gingival tissue morphology can have a negative impact on a smile.25 Gingival tissues are most pleasing when seen as papillae with minimal display of keratinized and mucosal tissue. Excessive gingival display can severely distract from the overall appearance, regardless of the good appearance of other elements.1 In general, fewer than 50% of respondents were able to diagnose discrepant features related to gingival esthetics. Clinicians were more sensitive in terms of identifying variation from the ideal in the examined esthetic aspects.
In the present study, ratings of the esthetics of the gingival display decreased as the amount of gingival exposure increased. The gingiva-to-lip distance was classified as acceptable if it was within the range of 2 mm.2,6 On the other hand, many studies reported that, at a distance of more than 3 mm, the smile was classified as noticeably unattractive.2,12 More than 50% of the students and the clinicians were able to identify exaggerated gingival display, although clinicians were better at the identification of this feature than were students. The level of detection increased as the students advanced in their academic years due to increased knowledge and clinical experience. Mild gingival exposure of less than 3 mm was not recognized as compromising esthetics by most respondents, which was in agreement with the findings of Machado.12
The level of marginal gingival tissues of the maxillary anterior teeth also influences the esthetic appearance of a smile,25 which should be located along a horizontal line extending from cuspid to cuspid.6 In the current study, the effect of a discrepancy in the gingival margin was detected by only 50% of the study sample. Davis et al reported that the gingival tissue esthetics are often overlooked.6 Gingival and incisal embrasures are key elements affecting the appearance of a tooth within a smile.1 A black interdental triangle is created in the gingival embrasure if it is unfilled and makes a smile less attractive.6 In the present study, clinicians were more able to identify problems in the gingival embrasure. Laypeople and general dentists were reported as being unable to detect an open gingival embrasure, unless it was 3 mm long.2 It could also be misdiagnosed as other discrepancies in tooth features because of the absence of the effect of the embrasure, which helps to define tooth identity.1
Lip analysis is an important feature in assessing a smile. The difference in the upper and lower lip fullness may affect the appearance of the smile.6 The respondents in the present study were able to evaluate these criteria as they rated the images less than 5, but they could not detect the main related discrepant feature. A smile with an average lip line that exposes the maxillary teeth and the interdental papillae is considered to be attractive.6,7 In the present study, a smile with a low lip line was rated as less attractive, in agreement with other studies.7,26 However, the respondents were not able to identify the main reason for considering a smile unpleasant. A considerable number of respondents diagnosed the reason as a discrepancy in the smile zone, which can be explained by the overlap between the two criteria. The smile zone is formed by the inferior border of the upper lip and the superior border of the lower lip. It is the space that includes the teeth and related tissues.6 Fewer than 50% of the respondents were able to diagnose discrepant features in the smile zone. Among the aspects investigated in this respect, more than 50% of respondents were able to identify the elliptical zone and rated images with discrepancies in this feature as an unattractive smile. An elliptical smile zone, where the corner of the mouth is lower than the center of the lower border of the upper lip, is considered less esthetic than the upward or straight smile.7
Parallelism of the maxillary anterior incisal margins with the upper border of the lower lip forms a convex smile line. A convex smile line has been considered more esthetic than a concave (reverse) smile line.27 Similar findings were found in the current study, where the respondents rated the reverse smile line as one of the least esthetic smiles.
An occlusal cant is a form of asymmetry that is obvious when a person smiles, but which can be overlooked on intraoral images or study casts. Chiche and Pinault stated that a canted incisal plane is esthetically unpleasant owing to median asymmetry.28 In this study, the respondents evaluated an image that was rotated by 2 degrees (2-mm incisal plane asymmetry) as acceptable esthetically (>5), but only 36% of the clinicians were able to detect it accurately. This is in agreement with other studies, which reported that deviations in cant are not perceptible unless they exceed 2 degrees.29,30 On the other hand, Kokich and colleagues found that professionals could notice a 1-mm incisal plane asymmetry (1-degree rotation).2
Tooth features play a significant role in determining the esthetics of a smile. Teeth in an esthetically pleasing smile are uniformly positioned with a balanced arrangement within the arch.4 The differences in the width of a tooth arch can be analyzed mathematically. The golden proportion is defined as the ratio of larger and smaller dimensions of repeated elements. This ratio is constant and equal to 1.618:l.0.4 In the present study, all discrepancies related to tooth size were accepted by respondents, with ratings of ≥4.9, which agreed with the finding of Kokich and Parekh.2,31 In contrast, chipped enamel in the central incisor was rated as unacceptable by respondents in this study.
Incisal embrasures are negative spaces formed by adjoining contact areas and between mesial and distal incisal curvatures. The form of the incisal embrasure may be considered an isosceles triangle, with the base and height increasing with distal progression from the midline up to the premolars, where similar contact area stabilizes the progression through the molars. Discrepancy in this criterion was not accepted by the respondents, who rated it around 4. Parekh et al found that most participants preferred natural embrasures.31 Diastema and spacing produced strong negative opinions from respondents in our study, who rated these features as ≥2.7, and it was easily diagnosed. This finding agreed with that of Parekh et al.31
To attain optimal esthetics, the facial midline must match the midline of maxillary and mandibular central incisors, or at least, these lines should be parallel. Small discrepancies of 1.5–2 mm are acceptable.32 Some studies have shown that maxillary midline discrepancies of more than 2.0 mm could be noticed by laypeople.33,34 Ker and colleagues, in a similar study, determined the maximum acceptable value by laypeople to be 2.9 mm.35 In the present study, more than half of the respondents were able to identify a midline shift as a compromising feature in the given image when it exceeded 2 mm. As the maxillary and mandibular midlines do not coincide in three-fourths of the population,3 a small deviation does not impair smile esthetics. The influence of the mandibular midline on esthetics may be lessened when the mandibular incisors have a narrow width and uniform size.36 In our study, a small percentage of respondents could detect this variation when it was less than 2 mm, but they rated the images of midline shift as esthetically highly acceptable.
The buccal corridor is the space created between the buccal surface of the posterior teeth and the lip corners during smiling, which give depth and a natural aspect to the smile.6 The greater and more distinct this negative space becomes, the more the full breadth of the smile is limited.6 In our study, a full buccal corridor was rated as esthetically acceptable and few participants were able to identify this condition. On the other hand, an increased dark space was rated as an unaesthetic condition and a greater number of respondents were able to identify it accurately. This agrees with the findings of Blitz,37 who reported that small buccal corridors are more attractive, and those of Martin et al, who concluded that laypeople favor smiles with no or a small buccal corridor.38
Discrepancies in facial features that include an increased lower facial height and retruded mandible were diagnosed correctly by most of the participants and were rated as unacceptable from an esthetic point of view.
One of the main limitations of this study, in addition, to the use of static smile photographs, is the use of different smile photographs instead of digitally modified photos. Standardization was attempted by cropping each photo to a standard size and eliminating the chin and nose.
The results of this study demonstrated that the low rating of smiles with some discrepancies does not coincide with the ability to detect discrepant features. Esthetic concepts and techniques are currently taught in dental schools, but the results of this study distinguish between actual deviations from the ideal and the perception of a beautiful smile, which may depend on a variety of different factors. Identification of discrepancies and actual perception should be separated and clearly acknowledged in order to accurately understand the patient’s desires for delivering acceptable esthetic treatment accurately. Consolidation of esthetic principles and techniques common to diagnostic and treatment procedures is necessary for the teaching of esthetic restorative dentistry.
Clinical Significance Statement
The ability of different group samples to diagnose discrepancies of smile esthetics were refined and enhanced with increased clinical experience and knowledge.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Moskowitz ME, Nayyar A. Determinants of dental esthetics: a rational for smile analysis and treatment. Compend Contin Educ Dent. 1995;16(12):1164–1166.
2. Kokich VO
3. Miller EL, Bodden WR
4. Snow SR. Esthetic smile analysis of maxillary anterior tooth width: the golden percentage. J Esthet Dent. 1999;11(4):177–184. doi:10.1111/j.1708-8240.1999.tb00397.x
5. Jefferson Y. Facial beauty–establishing a universal standard. Int J Orthod Milwaukee. 2004;15(1):9–22.
6. Davis NC. Smile design. Dent Clin North Am. 2007;51(2):299–318, vii. doi:10.1016/j.cden.2006.12.006
7. Dong JK, Jin TH, Cho HW, Oh SC. The esthetics of the smile: a review of some recent studies. Int J Prosthodont. 1999;12(1):9–19.
8. Ritter DE, Gandini LG
9. Sarver DM. The importance of incisor positioning in the esthetic smile: the smile arc. Am J Orthod Dentofacial Orthop. 2001;120(2):98–111. doi:10.1067/mod.2001.114301
10. Ackerman JL, Proffit WR, Sarver DM. The emerging soft tissue paradigm in orthodontic diagnosis and treatment planning. Clin Orthod Res. 1999;2(2):49–52. doi:10.1111/ocr.1999.2.2.49
11. Phark J-H, Romeo G. Dental anatomical combinations-a guide to ultimate dental esthetics. Smile Dental Journal. 2017;12:3. doi:10.12816/0044019
12. Machado AW. 10 commandments of smile esthetics. Dental Press J Orthod. 2014;19(4):136–157. doi:10.1590/2176-9451.19.4.136-157.sar
13. Manjula W, Sukumar M, Kishorekumar S, Gnanashanmugam K, Mahalakshmi K. Smile: A review. J Pharm Bioallied Sci. 2015;7(Suppl 1):S271. doi:10.4103/0975-7406.155951
14. Li X, Wu B, Cheng X, Li Y, Xie X, Deng F. Esthetic evaluation of implant‐supported single crowns: the implant restoration esthetic index and patient perception. J Prosthodont. 2019;28(1):e51–e58. doi:10.1111/jopr.12659
15. Miller CJ. The smile line as a guide to anterior esthetics. Dent Clin North Am. 1989;33(2):157–164.
16. Falkensammer F, Loesch A, Krall C, Weiland F, Freudenthaler J. The impact of education on the perception of facial profile aesthetics and treatment need. Aesthetic Plast Surg. 2014;38(4):620–631. doi:10.1007/s00266-014-0329-z
17. Osborne PB, Skelton J. Survey of undergraduate esthetic courses in U.S. and Canadian dental schools. J Dent Educ. 2002;66(3):421–425.
18. Manipal S, Mohan CS, Kumar DL, Cholan PK, Ahmed A, Adusumilli P. The importance of dental aesthetics among dental students assessment of knowledge. J Int Soc Prev Community Dent. 2014;4(1):48. doi:10.4103/2231-0762.131266
19. Jaju RA, Nagai S, Karimbux N, Da Silva JD. Evaluating tooth color matching ability of dental students. J Dent Educ. 2010;74(9):1002–1010.
20. Gordan VV, Abu-Hanna A, Imjor IA . Esthetic dentistry in North American dental schools. J Can Dent Assoc. 2004;70(4):230–232.
21. LeSage BP, Dalloca L. Approaches to smile design, mathematical to artistic interpretation. Journal of Cosmetic Dentistry. 2012;28:126–147.
22. Sivakumar N, Sundari K, Chandrasekar S, Kumar M. A review on smile arc-an orthodontist’s perspective. Drug Invention Today. 2018;10, 2630-2635.
23. Zadra JR, Clore GL. Emotion and perception: the role of affective information. Wiley Interdiscip Rev Cogn Sci. 2011;2(6):676–685. doi:10.1002/wcs.147
24. Burgueño-Barris G, Cortés-Acha B, Figueiredo R, Valmaseda-Castellón E. Aesthetic perception of single implants placed in the anterior zone. A cross-sectional study. Med Oral Patol Oral Cir Bucal. 2016;21(4):e488-493.
25. Chu SJ, Tan JH, Stappert CF, Tarnow DP. Gingival zenith positions and levels of the maxillary anterior dentition. J Esthet Restor Dent. 2009;21(2):113–120. doi:10.1111/j.1708-8240.2009.00242.x
26. Basting RT, da Trindade Rde C, Florio FM. Comparative study of smile analysis by subjective and computerized methods. Oper Dent. 2006;31(6):652–659. doi:10.2341/06-24
27. Margolis MJ. Esthetic considerations in orthodontic treatment of adults. Dent Clin North Am. 1997;41(1):29–48.
28. Chiche GJ, Pinault A. Smile rejuvenation: a methodic approach. Pract Periodontics Aesthet Dent. 1993;5(3):37–44.
29. Geron S, Atalia W. Influence of sex on the perception of oral and smile esthetics with different gingival display and incisal plane inclination. Angle Orthod. 2005;75(5):778–784. doi:10.1043/0003-3219(2005)75[778:IOSOTP]2.0.CO;2
30. Padwa BL, Kaiser MO, Kaban LB. Occlusal cant in the frontal plane as a reflection of facial asymmetry. J Oral Maxillofac Surg. 1997;55(8):811–816. doi:10.1016/S0278-2391(97)90338-4
31. Parekh SM, Fields HW, Beck M, Rosenstiel S. Attractiveness of variations in the smile arc and buccal corridor space as judged by orthodontists and laymen. Angle Orthod. 2006;76(4):557–563. doi:10.1043/0003-3219(2006)076[0557:AOVITS]2.0.CO;2
32. Tjan AH, Miller GD, The JG. Some esthetic factors in a smile. J Prosthet Dent. 1984;51(1):24–28. doi:10.1016/S0022-3913(84)80097-9
33. Johnston CD, Burden DJ, Stevenson MR. The influence of dental to facial midline discrepancies on dental attractiveness ratings. Eur J Orthod. 1999;21(5):517–522. doi:10.1093/ejo/21.5.517
34. Cardash HS, Ormanier Z, Laufer BZ. Observable deviation of the facial and anterior tooth midlines. J Prosthet Dent. 2003;89(3):282–285. doi:10.1067/mpr.2003.68
35. Ker AJ, Chan R, Fields HW, Beck M, Rosenstiel S. Esthetics and smile characteristics from the layperson’s perspective: a computer-based survey study. J Am Dent Assoc. 2008;139(10):1318–1327. doi:10.14219/jada.archive.2008.0043
36. Zachrisson BU. Global trends and paradigm shifts in clinical orthodontics. World J Orthod. 2005;6(Suppl):3–7.
37. Blitz N. Criteria for success in creating beautiful smiles. Oral Health. 1997;87(12):38–42.
38. Martin AJ, Buschang PH, Boley JC, Taylor RW, McKinney TW. The impact of buccal corridors on smile attractiveness. Eur J Orthod. 2007;29(5):530–537. doi:10.1093/ejo/cjm063
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.