")
Back to Journals » International Journal of General Medicine » Volume 17
Awareness, Knowledge, Attitude, and Skills (AKAS) of Telemedicine and Its Use by Primary Healthcare Providers
Authors Barnawi NA , Al-Otaibi H, Alkhudairy AI, Alajlan MA, Alajlan RA , Alay SM, Alqahtani SM, Bushnak IA, Abolfotouh MA
Received 11 December 2023
Accepted for publication 13 March 2024
Published 19 March 2024 Volume 2024:17 Pages 1047—1058
DOI https://doi.org/10.2147/IJGM.S452641
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mihajlo Jakovljevic
Najla A Barnawi,1,2 Hazza Al-Otaibi,1,3 Abdulaziz I Alkhudairy,4 Mohammed A Alajlan,4 Renad A Alajlan,5 Saeed M Alay,6 Saad Mohammed Alqahtani,7 Ibraheem A Bushnak,1 Mostafa A Abolfotouh1
1King Abdullah International Medical Research Center (KAIMRC)/King Saud Bin Abdulaziz University for Health Sciences/Ministry of National Guard Health Affairs, Riyadh, Saudi Arabia; 2College of Nursing, King Saud Bin Abdul-Aziz University for Health Science (KSAU-HS), Riyadh, Saudi Arabia; 3Pharmaceutical Care Department, King Abdulaziz Medical City, Ministry of National Guard Health Affairs, Riyadh, Saudi Arabia; 4College of Medicine, King Saud Bin Abdul-Aziz University for Health Science (KSAU-HS), Riyadh, Saudi Arabia; 5College of Medicine, Imam Muhammad Ibn Saud Islamic University (IMSIU), Riyadh, Saudi Arabia; 6College of Pharmacy, King Saud Bin Abdul-Aziz University for Health Science (KSAU-HS), Riyadh, Saudi Arabia; 7College of Medicine, King Khalid University, Abha, Saudi Arabia
Correspondence: Mostafa A Abolfotouh, King Abdullah International Medical Research Center/ King Saud bin Abdulaziz University for Health Sciences, Riyadh/ Ministry of National Guard Health Affairs, POB 22490, Riyadh, 11426, Saudi Arabia, Email [email protected]
Background: This study aimed to determine the rate of telemedicine (TM) use and the levels of awareness, knowledge, attitude, and skills of TM among primary healthcare (PHC) providers.
Methods: In a cross-sectional study, 104 PHC providers were subjected to a validated AKAS scale via Survey Monkey. The tool consists of 4 parameters that users can respond to using a 4-point Likert scale to assess their awareness (12 statements), knowledge (11 statements), attitude (11 statements), and skills (13 statements) on TM. Total and percentage mean scores (PMS) were calculated for each parameter. Participants were categorized in each parameter into three categories: low (≤ 49% score), average (50– 70% score), and high (≥ 71% score) levels. The association of AKAS levels with personal characteristics and TM use was investigated. The significance was set at p< 0.05.
Results: One-half of participants (51%) reported current use of TM, and two-thirds (63.5%) reported a high level of AKAS, with a PMS of 72.9± 14.7, 95% CI: 70.1– 75.7. There were significant associations between the following: years of experience and levels of knowledge (&KHgr;2LT = 6.77, p= 0.009) and skills (&KHgr;2LT = 4.85, p = 0.028), respectively; and total household income and levels of skills (&KHgr;2LT = 6.91, p= 0.009). The rate of TM use was significantly associated with awareness levels (&KHgr;2LT = 6.14, p = 0.013). Lack of training ranked as the first barrier (45.5%), followed by connection problems and tools’ unavailability (35.1% each). The participants recommended providing TM training (41.1%) and stabilization of connection and networking signals (30.1%).
Conclusion: Despite their high level of TM awareness, the rate of TM use by PHC providers is less than satisfactory. Establishing standardized TM training and supporting the network signals are recommended. A large-scale study on the impact of TM integration with PHC services is necessary.
Keywords: telehealth, telecommunication, e-medicine, e-health integration, universal health coverage, Saudi, PHCs
Introduction
Telemedicine (TM) has various terms within the medical-care-based context, such as telehealth, e-health, and e-medicine; however, all these terms sustain the importance of operationalizing e-communication to provide high-quality healthcare services. The TM Guide to Assessing Telecommunications in Health Care1 defined TM utilization as using electronic and telecommunications technologies to provide and support health care when distance separates the participants. It includes utilizing information and communication technologies, tools, and services integrated into diagnostic, therapy, rehabilitation, and medical decision-making virtually or at a distance.
The utilization of TM, mainly during the COVID-19 pandemic, was a successful tool for managing various health-based conditions, increasing safe-distance care accessibility, improving care quality, and reducing healthcare costs in multiple areas and circumstances.2–8 TM could efficiently reach underserved areas such as rural communities and remote regions.4,9 It is a cost-effective strategy in such areas as it reduces geographical distance barriers, such as travel time, and sustains the concept of a home-bound healthcare approach that enhances patients’ and healthcare providers’ therapeutic communication.2,4,5,9–13
Integrating TM within healthcare services enhances care quality time, decreases cost-related expenses and readmission rates, reduces frequent visits, readmissions, and the time patients spend accessing health services and increases compliance.2,12,14 It delivers healthcare using different modalities embedded in information and communication technologies. It aims to advance healthcare, ranging from individual to population levels, by allowing the exchange of patient information for diagnosis and management of health problems, primary care prevention, and education of physicians via distance learning.9,14,15
TM services within primary healthcare centers (PHCs) improve the quality of care to exceed the traditional patient consultation. It enhances the continuity of care at the primary care level.16–18 It accelerates the achievement of universal health coverage by boosting primary care because it overcomes the shortage of qualified healthcare personnel.19–22 The demand for PHC services varies greatly, even within the same country, depending on the catchment region.23,24 and this requires the use of TM to minimize inequalities and poor healthcare quality.18–20,24–27 The efficacy of TM utilization by healthcare workers depends on their awareness, knowledge, attitude, and self-efficacy about TM. Several key associated factors are age, gender, social role, marital status, and income.28–31
Previous studies have shown that healthcare providers with higher levels of education tend to exhibit greater awareness and understanding of TM.32,33 Evidence also indicated that some healthcare providers with specific specialties, such as primary care and psychiatry, have a higher knowledge and awareness of TM due to its direct relevance to their practice.4,20,34,35 years of experience within the healthcare specialty is another factor that increases TM awareness among healthcare providers.4,34,36,37 The healthcare providers’ geographical locations have a positive association with the level of TM awareness due to their potential to address healthcare disparities and improve access to care in remote regions.4,38,39 Organizational support is another factor that actively promotes the healthcare providers’ knowledge, skills, and awareness about TM and its integration, which enhances their practice.4,40,41 There is a need to examine and investigate the levels of awareness, knowledge, attitude, and skills among the healthcare providers in the PHCs.
In the Ministry of National Guard Health Affairs (MNG-HA), telemedicine is known as telehealth. It was introduced through the Corporate Clinical Performance and Innovation (CCPI) department, established in 2016, to achieve safe, efficient, effective, and innovative clinical care.42 The aim is to establish and deliver telehealth as an essential part of clinical practice, focusing on outpatient, primary care, telemonitoring, and chronic disease management. This is accomplished by integrating artificial intelligence (AI) in clinical practice to support its safety and quality and to deliver the basics of data science training to all clinical staff.43 There are several telemedicine programs in the MNG-HA, which include tele-health in the Ambulatory Care Clinic (ACC), tele-health in PHCs, tele-pathology, tele-radiology, tele-ICU, tele-emergency care, personal health records, personal health apps, and public health. One of the Saudi Vision 2030 strategies is establishing a complete and accelerated implementation of virtual care and TM services, mainly in the PHCs. This study aimed to determine the rate of TM use and levels of TM’s awareness, knowledge, attitude, and skills among MNG-HA’s PHC providers in Riyadh city.
Methods
Study Design
This study was an a cross-sectional study using an online questionnaire via Survey Monkey (https://www.surveymonkey.com/r/JK5CFQW) (accessed on 26 July 2022) restricted to one participant per unique internet protocol (IP) address.
Study Setting
MNG-HA provides medical services to all National Guard employees and their dependents in the Central, Western, and Eastern Regions and Madinah Provinces through Family Medicine and PHCs. Its vast scope includes more than 51 PHCs, including satellites and special character clinics. The services rendered include medical and dental care; health promotion, prevention, and rehabilitation; urgent care services; ophthalmology and ENT; and mission coverage. Ambulatory care services for obstetrics, gynecology, and pediatrics are also available in the main PHCs.44 This study targeted the healthcare workers in the PHCs of MNG-HA in Riyadh city.
Study Participants
A convenient sampling technique was used to select the participants. These included Saudi and non-Saudi licensed healthcare providers, including resident practitioners, working full-time at any MNG-HA PHCs in Riyadh city for at least six months, and having basic English skills. Interns, students, or those who hold temporary positions in PHCs at the MNG-HA premises were excluded from the study. In a previous study, the sample size was calculated based on a prevalence of 39.53% for high skills related to telemedicine on AKAS. With a 95% confidence limit and a 10% margin of error, the estimated sample size was 92 participants; those who responded to a completed questionnaire were 104 participants.
Data Collection Methods
Personal characteristics:
The investigators developed a set of questions that covered general demographic data and current use of the TM [Utilization of the TM includes utilizing any information and communication technologies, tools, and services integrated into diagnostic, therapy, rehabilitation, and medical decision-making virtually or at a distance].1
Assessment of TM Awareness, Knowledge, Attitude, and Skills:
The previously validated TM Awareness, Knowledge, Attitude, and Skills (TM-AKAS) tool45 assessed the participants’ awareness, knowledge, attitude, and skills. This tool was previously examined for its reliability.46 The Cronbach’s alpha for the five parameters were as follows: (Awareness = 0.784, Knowledge = 0.625, attitude =0.720, and skills = 0.890. The tool has five sections:
- The first section of the TM-AKAS covers the awareness parameter and has 12 items that assess the participants’ TM awareness. Each item was responded to with “Know about it” (2 points), “Heard of it” (1 point), and “Don’t know” (0 points). Awareness was assessed in four categories: general information about TM education and learning of TM, providing distance healthcare and risk management, and diagnostic procedure of TM. Total and percentage awareness scores were calculated for each participant. The levels of awareness were categorized into three categories: low (≤ 49% score), average (50–70% score), and high levels (≥ 71% score).
- The second section covers the knowledge parameter that has 11 close-ended statements. Each statement was responded to with “yes” (1 point) and “no” (0 point). Knowledge was assessed in patient e-management and e-communication and patient follow-up and recording. Total and percentage knowledge scores were calculated for each participant. The levels of knowledge were categorized into three categories: low (≤ 49% score), average (50–70% score), and high levels (≥ 71% score).
- The third section covers the attitude parameter, which has 11 statements that measure the healthcare providers’ attitude toward utilizing the TM on a 5-point Likert scale. The total attitude score ranged from 11 to 55 points, where 11 indicates the lowest score, and 55 is the highest. The attitude was assessed in two categories—accessibility and the existence of TM in a healthcare context and TM’s influence on the quality of healthcare services. Total and percentage awareness scores were calculated for each participant. The levels of attitude were categorized into three categories: (≤ 49% score), average (50–70% score), and high levels (≥ 71% score).
- The fourth section covers the TM skills parameter, which has 13 statements; each was responded with “expert” (3), “mediocre” (2), “learner” (1), and “unskilled” (0). Skills were assessed in three categories: e-communication, e-copying, scanning and documenting, downloading, installing software, and setting up. The total attitude score ranged from 0 to 39 points, where 0 indicates the lowest score and 39 is the highest. Total and percentage awareness scores were calculated for each participant. The levels of skills were categorized into three categories: low (≤ 49% score), average (50–70% score), and high levels (≥ 71% score).
- The fifth section includes four open-ended questions, which allowed the respondents to express their barriers against the use of TM in PHC practice and recommendations to upgrade its use.
Data Analysis
Data entry and statistical analysis were performed with the statistical package for the social science (SPSS) software program for Windows (version 28.0.1.1, © Copyright IBM Corporation, Armonk, NY, USA). Descriptive statistics such as percentages, means, standard deviations, and 95% confidence intervals were calculated. The Pearson Chi-square test and Chi-square test for linear (X2LT) trend were applied for categorical data, and a student-independent t-test was used for continuous data. Statistical significance was considered at p <0.05 for all analyses.
Ethical Considerations
Participation in this study was voluntary. Participants were assured in a written informed consent that their responses would remain anonymous. They were asked to respond to the survey if they agreed to the informed consent. The Institutional Review Board (IRB) of the Ministry of National Guard-Health Affairs (MNG-HA) approved the study, with reference # RSS22R/012/07. This study was conducted in accordance with the Declaration of Helsinki.
Results
Personal Characteristics of PHC Providers
Table 1 shows the personal characteristics of a total of 104 PHC providers with different professional backgrounds, including nurses (31, 29.8%), physicians (29, 27.9%), and other professional backgrounds such as pharmacists, health educators, and technicians (44, 42.3%). Most of the study participants (80, 76.9%) were 44 years old or less. Females represented the largest portion of the study participants (62, 59.6%) compared to their male counterparts (42, 40.4%). Bachelor’s degree holders showed the highest percentage in this study (81, 77.9%). Most of the study participants were married (67, 64.4%) and lived with their families. (92, 88.5%). More than half of the participants (58, 55.8%) had seven years of experience or more. Most participants (77, 74%) reported the need for <30 minutes to arrive at the intended PHC every day. Nearly one-half of the study participants (53, 54.6%) reported seeing less than 30 patients per day, and 51% reported current use of TM.
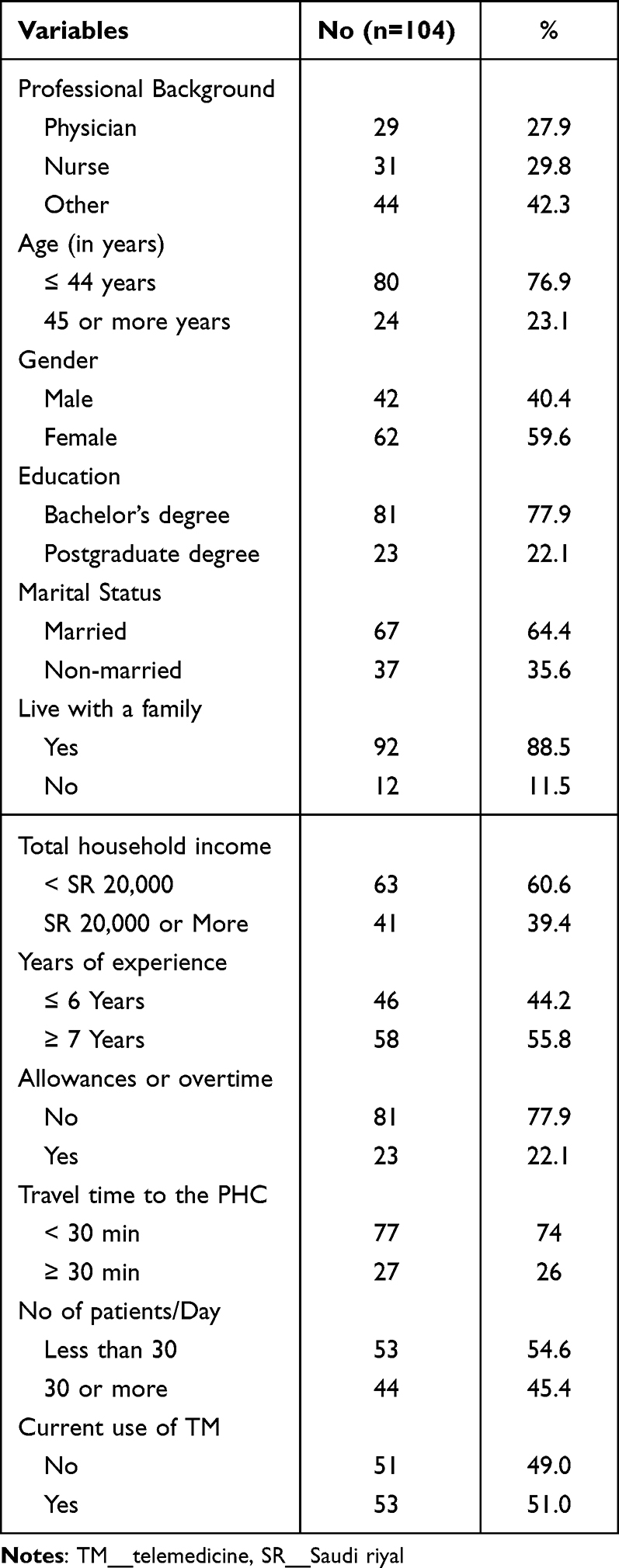 |
Table 1 Personal Characteristics About the Healthcare Providers Who Works in the MNG-HA PHCs |
Levels of AKAS Parameters Among the Healthcare Providers
Table 2 shows the levels of awareness, knowledge, attitude, and skills (AKAS) among the primary healthcare providers at the MNG-HA according to different AKAS parameters in PHCs at MNG-HA. Nearly two-thirds of participants (63.5%) reported a high level of AKAS. However, this figure was the highest for knowledge parameter (85.6%), followed by attitude (70.2%), awareness (65.4%) and skill (49.0%) parameters. The overall percentage mean score (PMS) of AKAS score for participants was (72.9±14.7, 95% CI: 70.1–75.7). It was the highest for knowledge parameter (85.8±18.7, 95% CI: 82.2–89.4), followed by awareness parameter (74.3±25.1, 95% CI: 69.5–79.1), attitude parameter (73.4±18.7 CI: 69.8–77.0) and then skills parameter (68.1±24.7 CI: 63.4–72.8). This table also shows the PMS of the components of each AKAS parameter. It was the highest in the “patient follow-up and recording” in the knowledge parameter (94.4 ± 17.5), followed by “provided distance healthcare and risk management” in the awareness parameter (79.8 ± 27.6), “accessibility and the existence of TM” in attitude parameter (78.5 ± 23.1), and “e-communication” in skills parameter (73.3 ± 23.6).
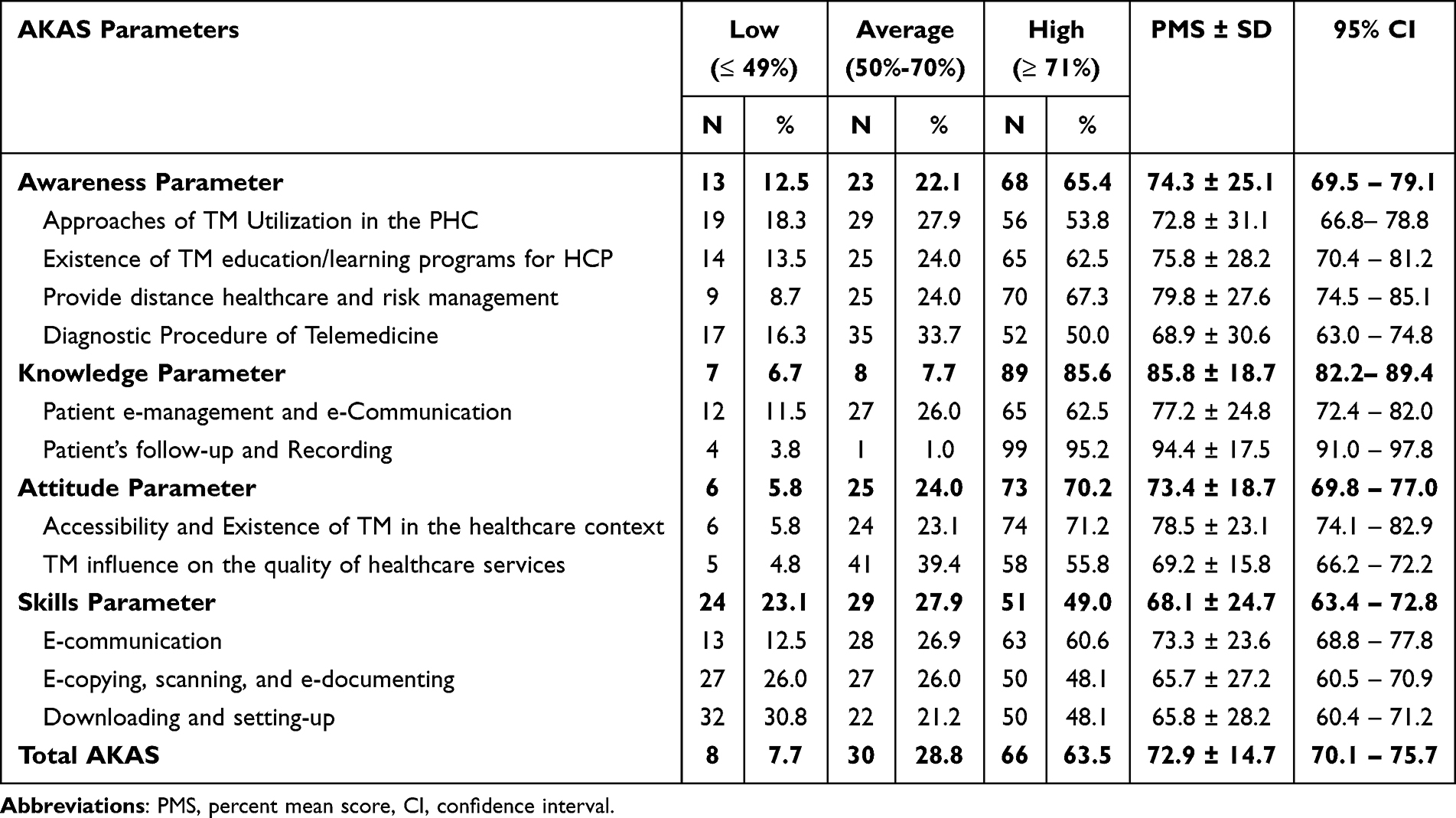 |
Table 2 Levels of Awareness, Knowledge, Attitude, and Skills (AKAS) Among the Primary Healthcare Providers at the MNG-HA According to Different AKAS Parameters |
Association of Awareness, Knowledge, Attitude, and Skills (AKAS) with Personal Data
Table 3 shows the relationship between the TM AKAS parameters and the personal data of the study participants. The result shows a significant association between years of experience and the level of knowledge (χ2LT = 6.77, p= 0.009) and the level of skills in TM (χ2LT = 4.85, p= 0.028). The skill level was also significantly associated with the total household income (χ2LT = 6.91, p = 0.009).
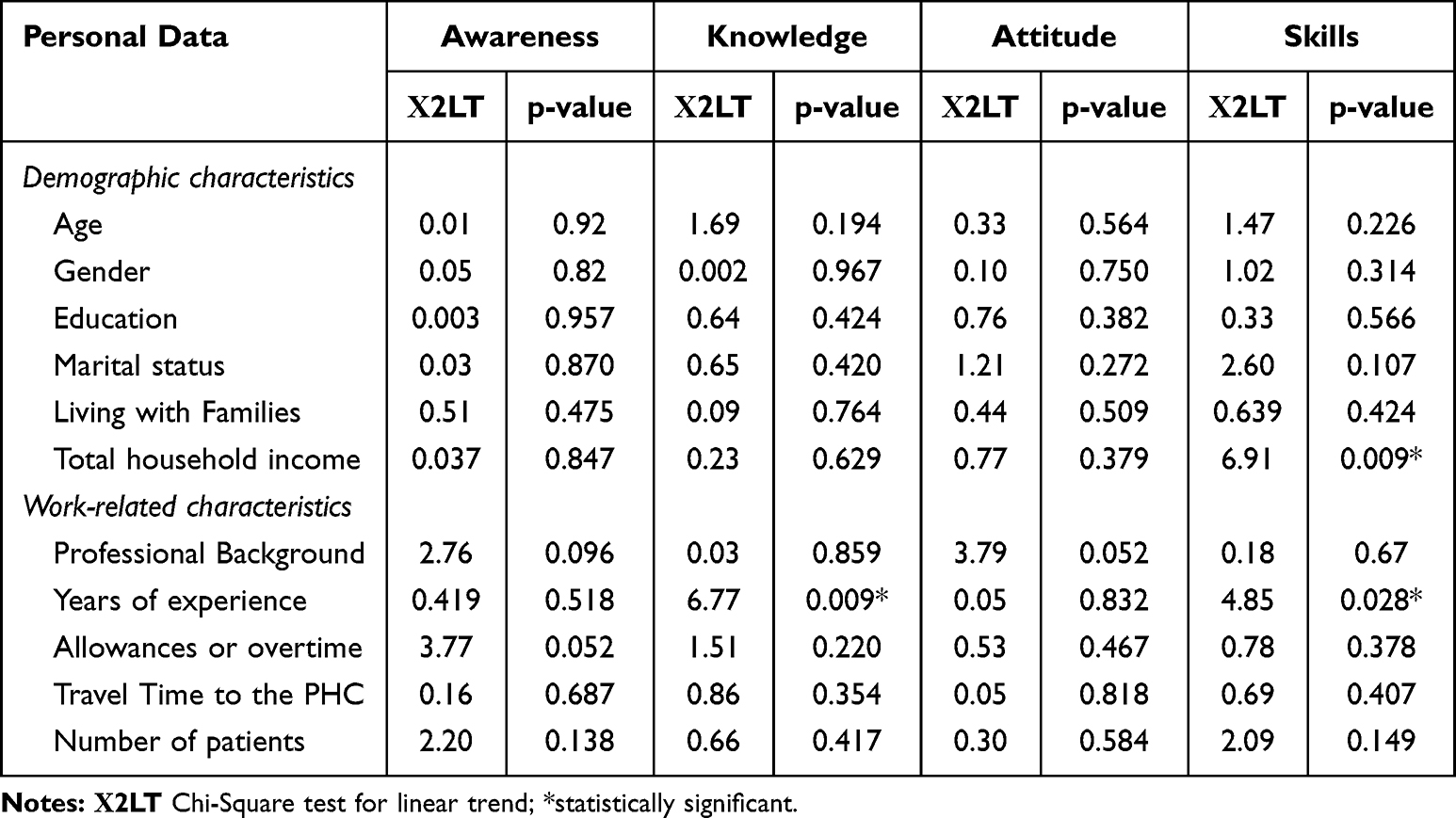 |
Table 3 Association Between the Levels of Telemedicine AKAS Parameters and Some Demographic and Work-Related Characteristics Among the Primary Healthcare Providers at the MNG-HA |
Association of Awareness, Knowledge, Attitude, and Skills (AKAS) with Telemedicine Use
Table 4 shows a significant increase in the rate of TM use from 30.8% in a low level of awareness parameters score to 34.8% and 60.3% in average and high awareness levels, respectively (χ2LT = 6.14, p = 0.013). However, the use of TM was not associated with knowledge (p=0.436), attitude (p=0.345), skills (p=0.366), or overall AKAS (p=0.095) levels.
 |
Table 4 Association Between AKAS Parameters and Telemedicine Use Among the Primary Healthcare Providers at the MNG-HA |
Barriers and Suggestions for Using Telemedicine in the NGHA PHCs
Table 5 shows the main barriers to and recommendations for healthcare providers’ use of TM in PHC settings. Lack of training ranked as the first barrier (45.5%), followed by connection problems and unavailability of the tools (35.1% each). Other barriers were unlikely to use it or preferred to be physically in the clinic (11.7% each). The participants’ leading suggestions included more TM training (41.1%) and stabilization of connection and networking signals (30.1%).
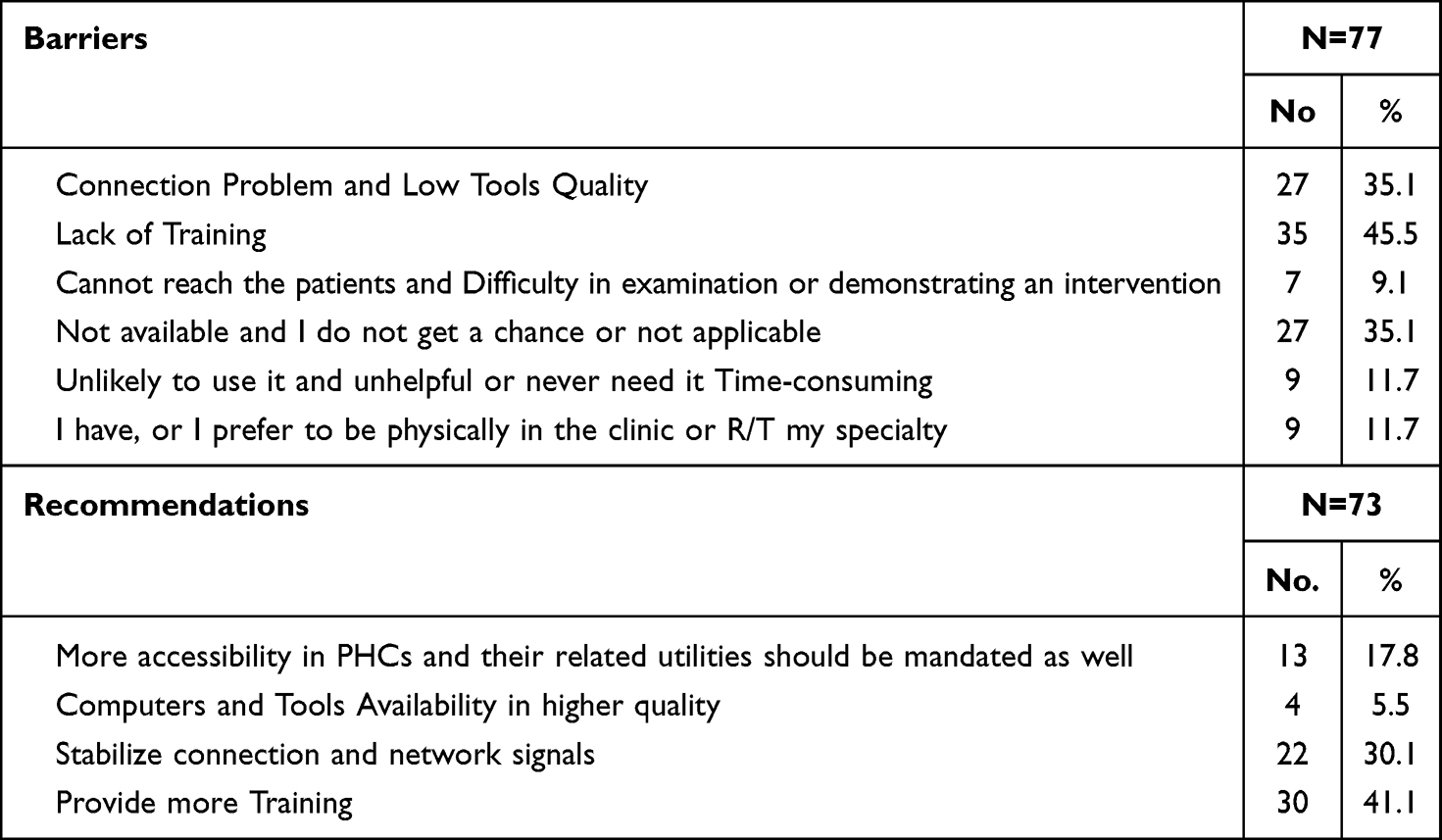 |
Table 5 Barriers and Suggestions for Using Telemedicine in the NGHA PHCs |
Discussion
Our study showed high category scores in most of the AKAS’s parameters with the highest level in awareness parameter. It also highlights that some personal and work-related characteristics, such as the total income, professional background, years of experience, receiving allowances, or overtime, may positively impact the use of TM within the PHC. Further, lack of training ranked as the first barrier, and the provision of TM training was the main recommendation by the participants.
Examining TM’s awareness, knowledge, attitude, and skills within the PHCs at MNG-HA is essential in Saudi healthcare, mainly to comply with the Saudi Vision 2030 that calls for healthcare transformation.47–51 Nearly two-thirds of participants reported a high level of AKAS. However, this figure was the highest for knowledge parameters (85.6%), followed by attitude and awareness, while the skill parameters came last. These findings agree with those of a previous study of healthcare workers in Libya during the COVID-19 pandemic, where the highest level of AKAS was in knowledge (86.5%), while the lowest was in skills, which was around 36%.52 The low proportion of participants whose skills were high in our study (40%) agreed with the figure of 39.5% reported by healthcare professionals in the Datta study.53 However, Fouad et al, 2023 revealed that attitude toward telemedicine was high among the studied mental healthcare providers while average among the other studied variables [awareness, knowledge, and skills].46 These findings indicate that effective TM integration may lead to a positive utilization by the healthcare providers in the PHCs.
This low proportion of those reporting a high skill level in our study could explain the study results of barriers reported by healthcare workers, such as lack of training that ranked as the first barrier, followed by connection problems and unavailability of the tools. Several studies had similar results in various healthcare settings and approaches, such as home care,54 mental health,55 allied health, the nursing profession,56 and various clinical settings.36 PHC workers’ leading suggestions were more TM training and stabilization of connection and networking signals. Based on several studies, there is a need to consider the importance of including other Blockchain technologies in maintaining information security and medical record confidentiality in TM training, mainly in advanced technology tools such as Artificial Intelligence (AI).57–59 Considering such Blockchain technologies, training is essential to minimize the potential ethical barriers that may occur while using the TM by the PHC providers.
Our study showed that one-half of the participants had been using the TM during the study period. Several national and international studies highlight the positive impact of increasing healthcare professionals’ awareness of the effective utilization and integration of TM in healthcare.52,60–63 This was in agreement with the results of our study, where a significant difference was shown between the TM users group and the non-user group in the awareness parameter in favor of the TM user group. This increased healthcare providers’ awareness about the effective use of TM increases the acceptability of it among the patients and the healthcare providers,36,63–65 facilitates and accelerates the integration of the TM within the PHCs.61,63,66–69 Other studies imply that the current use of TM could positively impact the awareness levels of TM among healthcare providers.46,52,67 However, because of its cross-sectional design, the present study does not guarantee the temporal relationship between TM awareness and its use.
Various studies addressed several factors such as the total income, professional background, years of experience, receiving allowances or overtime, and current use of TM as significant factors that should be reconsidered to sustain effective integration and utilization of the TM in the PHCs.4,38,67,70–73 Our study results also reveal that some personal and work-related characteristics are associated with the levels of AKAS parameters among PHC providers. These characteristics include the total income associated with skill level and the duration of experience related to levels of knowledge and skills. In a study on PHC workers in Libya, respondents with professional computer skills had significantly higher awareness and attitude scores than those without. Andersen et al examined the key sociodemographic factors that enhanced the use of TM during the COVID-19 pandemic. They revealed that gender, race/ethnicity, educational attainment, confidence in filling out medical forms, and the COVID-19 fear scale were the major factors associated with TM use.74 However, none of these factors had any significant association with TM-AKAS parameters in our study.
Limitations and Strengths
This study has some limitations: it was conducted only on PHC workers at the Ministry of National Guard; thus, the generalization of the findings may suffer from reporting bias. The study sample did not represent all PHC workers in the study setting; thus, the study might have been subject to selection bias. However, while the numbers are not representative, they provide baseline and significant results showing that problems occur in this population, which warrant further investigation. Moreover, the survey was conducted online, which could result in selection bias. The data were self-reported, making it subject to recall bias. The cross-sectional design does not guarantee the cause-and-effect relationship; thus, it is difficult to determine whether the exposure (demographic and work-related factors) or outcome (levels of awareness, knowledge, attitude, and skills on TM) came first.
Conclusions
This is the first study in Saudi Arabia to investigate PHC workers in a comprehensive survey about awareness, knowledge, attitude, and skills on TM and its use by PHC providers. It may act as a pilot study for others from similar countries on the hot topic of TM. The rate of TM use by PHC providers is less than satisfactory despite their high level of TM awareness. It highlights that some personal and work-related characteristics, such as the total income, professional background, years of experience, receiving allowances, or overtime, may positively impact the use of TM within the PHC. Lack of training ranked as the first barrier, and the provision of TM training was the main recommendation by the participants.
The study highlighted some recommendations to integrate TM within the PHC at MNGHA effectively. One of the recommendations is to provide training about TM for all the healthcare providers in the PHC centers and the potential healthcare receivers. Further, there is a need to enhance the connection stability and equip the PHC centers with high-quality audio-visual tools. Several studies show some challenges related to the capabilities and features of TM and the healthcare management system.4,75 However, such challenges could be easily overcome in the MNGHA in the existence of the Best-Care. The existence of such digital or electronic medical system is a core strategy that supports TM integration easily in the PHCs.4 A large-scale study on the impact of training on TM and its integration with PHC services is recommended.
Abbreviations
KAMC, King Abdulaziz Medical city; MNGHA, Ministry of National Guard-Health Affairs; KAIMRC, King Abdullah International Medical Research Center; IRB, Institutional Review Board; TM, telemedicine; PHCs, primary healthcare centers; CCPI, Corporate Clinical Performance and Innovation; ACC, Ambulatory Care Clinic.
Data Sharing Statement
Most of the data supporting our findings is contained within the manuscript, and all others, excluding identifying/confidential data, will be shared upon request from the corresponding author [[email protected]].
Ethics Approval and Consent to Participate
Participation in this study was voluntary. Participants were assured in a written informed consent that their responses would remain anonymous. They were asked to respond to the survey if they agreed to the informed consent. The study protocol was approved by the Institutional Review Board (IRB) of the Ministry of National Guard-Health Affairs (MNGHA), Riyadh, Saudi Arabia (Ref. # RSS22R/012/07). This study was conducted under the Declaration of Helsinki.
Acknowledgments
This study was initiated by King Abdullah International Medical Research Center/King Saud bin-Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia. The study was one of the research projects of the 13th Research Summer School program conducted during July–August 2022 under the full supervision of the KAIMRC staff. All individuals included in this section have consented to the acknowledgment.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Field MJ. Telemedicine: A Guide to Assessing Telecommunications for Health Care. The National Academies Press; 1996.
2. Atmojo JT, Sudaryanto WT, Widiyanto A, Ernawati E, Arradini D. Telemedicine, cost effectiveness, and patients satisfaction: a systematic review. J Heal Policy Manag. 2020;5(2):103–107. doi:10.26911/thejhpm.2020.05.02.02
3. Bhaskar S, Bradley S, Chattu VK, et al. Telemedicine as the new outpatient clinic gone digital: position paper from the pandemic health system resilience PROGRAM (REPROGRAM) international consortium (Part 2). Front Public Health. 2020;8:1–16. doi:10.3389/fpubh.2020.00410
4. Haleem A, Javaid M, Singh RP, Suman R. Telemedicine for healthcare: capabilities, features, barriers, and applications. Sensors Int. 2021;2(100117). doi:10.1016/j.sintl.2021.100117
5. Snoswell CL, Taylor ML, Comans TA, Smith AC, Gray LC, Caffery LJ. Determining if telehealth can reduce health system costs: scoping review. J Med Internet Res. 2020;22(10):e17298. doi:10.2196/17298
6. Nittari G, Khuman R, Baldoni S, et al. Telemedicine practice: review of the current ethical and legal challenges. Telemed e-Health. 2020;26(12):1427–1437. doi:10.1089/tmj.2019.0158
7. Greiwe J. Telemedicine Lessons learned during the COVID-19 pandemic. Curr Allergy Asthma Rep. 2022;22(1):1–5. doi:10.1007/s11882-022-01026-1
8. Getachew E, Adebeta T, Muzazu SGY, et al. Digital health in the era of COVID-19: reshaping the next generation of healthcare. Front Public Health. 2023:11. doi:10.3389/fpubh.2023.942703
9. Rush KL, Seaton C, Li E, Oelke ND, Pesut B. Rural use of health service and telemedicine during COVID-19: the role of access and eHealth literacy. Health Informatics J. 2021;27(2):146045822110200. doi:10.1177/14604582211020064
10. Gupta N, Gupta MK, Joshi NK, et al. Is telemedicine a holy grail in healthcare policy: clinicians’ and patients’ perspectives from an apex institution in Western India. BMC Health Serv Res. 2023;23(1):1–11. doi:10.1186/s12913-022-09013-y
11. Kichloo A, Albosta M, Dettloff K, et al. Telemedicine, the current COVID-19 pandemic and the future: a narrative review and perspectives moving forward in the USA. Fam Med Community Heal. 2020;8(3):1–9. doi:10.1136/fmch-2020-000530
12. Lindenfeld Z, Berry C, Albert S, et al. Synchronous home-based telemedicine for primary care: a review. Med Care Res Rev. 2023;80(1):3–15. doi:10.1177/10775587221093043
13. Steindal SA, Nes AAG, Godskesen TE, et al. Patients’ experiences of telehealth in palliative home care: scoping review. J Med Internet Res. 2020;22(5):1–11. doi:10.2196/16218
14. Mubaraki AA, Alrabie AD, Sibyani AK, Aljuaid RS, Bajaber AS, Mubaraki MA. Advantages and disadvantages of telemedicine during the COVID-19 pandemic era among physicians in Taif, Saudi Arabia. Saudi Med J. 2021;42(1):110–115. doi:10.15537/SMJ.2021.1.25610
15. Waqas A, Teoh SH, Lapão LV, Messina LA, Correia JC. Harnessing Telemedicine for the provision of health care: bibliometric and scientometric analysis. J Med Internet Res. 2020;22(10):e18835. doi:10.2196/18835:
16. Breton M, Deville-Stoetzel N, Gaboury I, et al. Telehealth in primary healthcare: a portrait of its rapid implementation during the covid-19 pandemic | téléconsultations de première ligne: portrait d’une mise en oeuvre rapide pendant la pandémie de COVID-19. Healthc Policy. 2021;17(1):73–90. doi:10.12927/hcpol.2021.26576
17. Gudi N, Konapur R, John O, Sarbadhikari S, Landry M. Telemedicine supported strengthening of primary care in WHO South East Asia region: lessons from the COVID-19 pandemic experiences. BMJ Innov. 2021;7(3):580–585. doi:10.1136/bmjinnov-2021-000699
18. Ray KN, Kahn JM. Connected subspecialty care: applying telehealth strategies to specific referral barriers. Acad Pediatr. 2020;20(1):16–22. doi:10.1016/j.acap.2019.08.002
19. Tao W, Zeng Z, Dang H, et al. Towards universal health coverage: lessons from 10 years of healthcare reform in China. BMJ Glob Heal. 2020;5(3):1–9. doi:10.1136/bmjgh-2019-002086
20. Beheshti L, Kalankesh LR, Doshmangir L, Farahbakhsh M. Telehealth in primary health care: a scoping review of the literature. Perspect Heal Inf Manag. 2022;19(1):104470.
21. Akintunde TY, Akintunde OD, Musa TH, et al. Expanding telemedicine to reduce the burden on the healthcare systems and poverty in Africa for a post-coronavirus disease 2019 (COVID-19) pandemic reformation. Glob Heal J. 2021;5. doi:10.1016/j.glohj.2021.07.006
22. Vaishya R, Javaid M, Khan IH, Haleem A. Artificial intelligence (AI) applications for COVID-19 pandemic. Diabetes Metab Syndr Clin Res Rev. 2020;14:337–339. doi:10.1016/j.dsx.2020.04.012
23. Al Saffer Q, Al-Ghaith T, Alshehri A, et al. The capacity of primary health care facilities in Saudi Arabia: infrastructure, services, drug availability, and human resources. BMC Health Serv Res. 2021;21(1):1–15. doi:10.1186/s12913-021-06355-x
24. World Health Organization. Imbalances in rural primary care, a scoping literature review with an emphasis on the WHO European region. Tech Ser Prim Heal Care; 2018. Available From: https://apps.who.int/iris/bitstream/handle/10665/346351/WHO-HIS-SDS-2018.58-eng.pdf?sequence=1.
25. Qin C, Liu M, Guo X, Liu J. Human resources in primary health-care institutions before and after the new health-care reform in China from 2003 to 2019: an interrupted time series analysis. Int J Environ Res Public Health. 2022;19(10):6042. doi:10.3390/ijerph19106042
26. Mohammadiaghdam N, Doshmangir L, Babaie J, Khabiri R, Ponnet K. Determining factors in the retention of physicians in rural and underdeveloped areas: a systematic review. BMC Fam Pract. 2020;21(1):1–23. doi:10.1186/s12875-020-01279-7
27. Streeter RA, Snyder JE, Kepley H, Stahl AL, Li T, Washko MM. The geographic alignment of primary care health professional shortage areas with markers for social determinants of health. PLoS One. 2020;15(4):1–20. doi:10.1371/journal.pone.0231443
28. Ahmed T, Baig M, Bashir M, Gazzaz Z, Butt N, Khan S. Knowledge, attitudes, and perceptions related to Telemedicine among young doctors and nursing staff at the King Abdul-Aziz University Hospital Jeddah, KSA. Niger J Clin Pr. 2021;24(4):464–469. doi:10.4103/njcp.njcp_34_20
29. Reed ME, Huang J, Graetz I, et al. Patient characteristics associated with choosing a telemedicine visit vs office visit with the same primary care clinicians. JAMA Network Open. 2020;3(6):1–10. doi:10.1001/jamanetworkopen.2020.5873
30. Clare CA. Telehealth and the digital divide as a social determinant of health during the COVID-19 pandemic. Netw Model Anal Heal Inform Bioinforma. 2021;10(1):1–3. doi:10.1007/s13721-021-00300-y
31. Ncube B, Mars M, Scott RE, Prenestini A. Perceptions and attitudes of patients and healthcare workers towards the use of telemedicine in Botswana: an exploratory study. PLoS One. 2023;18(2):1–14. doi:10.1371/journal.pone.0281754
32. Kennedy BM, Rehman M, Johnson WD, Michelle B, Leonard R, Katzmarzyk PT. Healthcare providers versus patients’ understanding of health beliefs and values. Patient Exp J. 2017;4(3):29–37. doi:10.35680/2372-0247.1237
33. Alboraie M, Allam MA, Youssef N, et al. Knowledge, applicability, and barriers of Telemedicine in Egypt: a national survey. Int J Telemdicine Appl. 2021;2021:1–8. doi:10.1155/2021/5565652
34. Mazandarani M, Lashkarbolouk N, Hashemi M. Evaluation of awareness and attitude of Telemedicine among primary healthcare workers in deprived area health centers. Int J Telemdicine Appl. 2023;2023:1–7.
35. Ye J, He L, Beestrum M. Implications for implementation and adoption of telehealth in developing countries: a systematic review of China’s practices and experiences. NPJ Digit Med. 2023;6(174):1–14. doi:10.1038/s41746-023-00908-6
36. Alghamdi SM, Aldhahir AM, Alqahtani JS, Siraj RA, Alqarni AA. Healthcare providers perception and barriers concerning the use of telehealth applications in Saudi Arabia. HealthCare. 2022;10:1–11. doi:10.3390/healthcare10081527
37. Assaye BT, Jemere AT. Knowledge and awareness of health professionals towards telemedicine services in Northwest, Ethiopia. Digit Heal. 2022;8:1–11. doi:10.1177/20552076221143250
38. Haimi M. The tragic paradoxical effect of telemedicine on healthcare disparities ‑ a time for redemption: a narrative review. BMC Med Inform Decis Mak. 2023;4:1–10. doi:10.1186/s12911-023-02194-4
39. Barbosa W, Zhou K, Waddell E, Myers T, Dorsey ER. Improving access to care: Telemedicine across medical domains. Annu Rev. 2021;42:463–481. doi:10.1146/annurev-publhealth-090519-093711
40. Naqvi SZ, Ahmad S, Rocha IC, et al. Healthcare workers knowledge and attitude toward Telemedicine during the COVID-19 pandemic: a Global Survey. Cureus. 2022;14(10):1–12. doi:10.7759/cureus.30079
41. Elhadi M, Elhadi A, Bouhuwaish A, Alshiteewi F. Telemedicine awareness, knowledge, attitude, and skills of health care workers in a low-resource country during the COVID-19 pandemic: cross-sectional Study. J Med Intenet Res. 2020;23(2):1–10. doi:10.2196/20812
42. Ministry of National Guard Health Affairs. Clinical performance and innovation; 2021. Available from: https://ngha.med.sa/English/AboutNGHA/ccpi/Pages/default.aspx.
43. Ministry of National Guard – Health Affairs. Tele-Health; 2023. Available from: https://ngha.med.sa/English/AboutNGHA/ccpi/Pages/TeleHealth.aspx.
44. Zayapragassarazan Z, Kumar S. Awareness, knowledge, attitude and skills of Telemedicine among health professional faculty working in teaching hospitals. J Clin Diagn Res. 2016;10(3):1–4. doi:10.7860/JCDR/2016/19080.7431
45. Zayapragassarazan Z. Telemedicine – awareness, knowledge, attitude & skills (AKAS) questionnaire. Jawaharlal Institute of Postgraduate Medical Education & Research; 2020. Available from: https://www.researchgate.net/publication/344121385%0ATelemedicine.
46. Fouad AA, Osman MA, Abdelmonaem YMM, Karim NAHA. Awareness, knowledge, attitude, and skills of telemedicine among mental healthcare providers. Middle East Curr Psychiatry. 2023;30(1). doi:10.1186/s43045-022-00272-3
47. Veettil ST, Anodiyil MS, Khudadad H, Kalathingal MA, Alnuaimi AS. Knowledge, attitude, and proficiency of healthcare providers in cardiopulmonary resuscitation in a public primary healthcare setting in Qatar. Front Cardiovasc Med. 2023;1–8. doi:10.3389/fcvm.2023.1207918
48. Assiri HA, Alkhaldi YM, Alsaleem SA, Alqarni HM. Knowledge, attitude and practices of PHC physicians in Aseer region regarding management of acute asthma. J Fam Med Prim Care. 2021;10(5):1882–1889. doi:10.4103/jfmpc.jfmpc
49. Alkhatlan H, Almutairi BT, Shazly M. Knowledge, attitude and practice of primary health care providers regarding E-health: a Validation. Greener J Med Sci. 2016;6(1):18–24. doi:10.15580/GJMS.2016.1.021716040
50. Biruk K, Abetu E. Knowledge and attitude of health professionals toward Telemedicine in resource-limited settings: a cross-sectional study in north west Ethiopia. J Healthc Eng. 2018;2018:1–7. doi:10.1155/2018/2389268
51. Du S, Cao Y, Zhou T, et al. The knowledge, ability, and skills of primary health care providers in SEANERN countries: a multi-national cross-sectional study. BMC Health Serv Res. 2019;19(602):1–8. doi:10.1186/s12913-019-4402-9
52. Elhadi M, Elhadi A, Bouhuwaish A, et al. Telemedicine awareness, knowledge, attitude, and skills of health care workers in a low-resource country during the COVID-19 pandemic: cross-sectional study. J Med Internet Res. 2021;23(2). doi:10.2196/20812
53. Datta R, Singh A, Mishra P. A survey of awareness, knowledge, attitude, and skills of telemedicine among healthcare professionals in India. Med J Armed Forces India. 2021;79(6):702–709. doi:10.1016/j.mjafi.2021.08.017
54. Almathami HKY, Vlahu-gjorgievska E, Win KT. Barriers and facilitators that influence Telemedicine-based, real-time, online consultation at patients’ homes: systematic literature review. J Med Intenet Res. 2020;22(2):1–30. doi:10.2196/16407
55. Adem JB, Zeleke T, Walle AD, et al. Awareness and readiness of mental healthcare providers to implement telemental health services and associated factors at public referral hospitals in Addis Ababa City, Ethiopia. BMJ Open. 2023;13(e069671):1–13. doi:10.1136/bmjopen-2022-069671
56. Rettinger L, Kuhn S. Barriers to video call – based telehealth in allied health professions and nursing: scoping review and mapping process. J Med Internet Res. 2023;25:1–30. doi:10.2196/46715
57. Khan AA, Wagan AA, Laghari AA, Gilal AR, Aziz IA, Talpur BA. BIoMT: a state-of-the-art consortium serverless network Architecture for healthcare system using blockchain smart contracts. IEEE Access. 2022;10:78887–78898. doi:10.1109/ACCESS.2022.3194195
58. Khan AA, Laghari AA, Shaikh ZA, Dacko-Pikiewics Z, Kot S. Internet of things (IoT) security with blockchain technology: a state-of-the-art review. IEEE Access. 2022;10:122679–122695. doi:10.1109/ACCESS.2022.3223370
59. Khan AA, Laghari AA, Shaikh AA, Dootio MA, Estrela VV, Lopes RT. A blockchain security module for Brain-Computer Interface (BCI) with Multimedia Life Cycle Framework (MLCF). Neurosci Informatics. 2022;2(1):100030. doi:10.1016/j.neuri.2021.100030
60. Alqurashi H, Mohammed R, Alghanmi AS, Alanazi F. The perception of health care practitioners regarding Telemedicine during COVID-19 in Saudi Arabia: mixed methods study. JMIR Form Res. 2023;7(e47065):1–16. doi:10.2196/47065
61. Albaghdadi AT, Daajani MM. Perceptions, satisfaction, and barriers to Telemedicine use: a community-based study from Jeddah, Saudi Arabia. Cureus. 2023;15(6):1–16. doi:10.7759/cureus.40738
62. Abogosh AK, Alsedrah AM, Alhindi AH, Alfehaid RH. Utilization of Telemedicine during COVID-19 in Saudi Arabia: a multicenter study. Cureus. 2023;15(7). doi:10.7759/cureus.41541
63. Alkhanbashi R, Zedan H. Telemedicine policy availability and awareness: directions for improvement. Smart Homecare Technol TeleHealth. 2022;9:1–9. doi:10.2147/SHTT.S368486
64. Alzahrani SA, Khouja JH, Ghamdi SA, Alotaybi M, Bargawi A. Telemedicine acceptability among patients of primary health care clinics in the western region, Saudi Arabia. Cureus. 2023;15(6):1–8. doi:10.7759/cureus.40857
65. Jung S, Kweon H, Kim E, Kim S, Choi J, Cho D. Preference and awareness of Telemedicine in primary care patients. Korean J Fam Med. 2012;33(1):25–33. doi:10.4082/kjfm.2012.33.1.25
66. Alshammari MH. Electronic-health in Saudi Arabia: a review. Int J Adv Appl Sci. 2021;8(6):1–10. doi:10.21833/ijaas.2021.06.001
67. Ghaddaripouri K, Baigi S, Abbaszadeh A, Habibi MM. Attitude, awareness, and knowledge of telemedicine among medical students: a systematic review of cross ‐ sectional studies. Heal Sci Rep. 2023;6(1156):1–12. doi:10.1002/hsr2.1156
68. Bashir MS, Lalithabai DS, Alotaiby S, Abu-shaheen A. Health care professionals knowledge and attitudes toward telemedicine. Frontiers Public Heal. 2023;11:1–8. doi:10.3389/fpubh.2023.957681
69. Aldebasi B, Alhassan AI, Al-nasser S, Abolfotouh MA. Level of awareness of Saudi medical students of the internet-based health- related information seeking and developing to support health services. BMC Med Inform Decis Mak. 2020;8(209):1–8. doi:10.1186/s12911-020-01233-8
70. Ashley C, Williams A, Dennis S, et al. Telehealth’s future in Australian primary health care: a qualitative study exploring lessons learnt from the COVID- 19 pandemic. BJGP Open. 2023;7(2):1–10. doi:10.3399/BJGPO.2022.0117
71. Mahmoud K, Jaramillo C, Barteit S. Telemedicine in low- and middle-income countries during the COVID-19 pandemic: a scoping review. Front Public Health. 2022;10(914423):1–15. doi:10.3389/fpubh.2022.914423
72. Gajarawala Shilpa N, Pelkowski NJ. Telehealth benefits and barriers. J Nurse Pract. 2021;17(2):218–221. doi:10.1016/j.nurpra.2020.09.013
73. de Albornoz CS, Sia K, Harris A. The effectiveness of teleconsultations in primary care: systematic review. Fam Pract. 2021;2021:1–15. doi:10.1093/fampra/cmab077
74. Andersen JA, Felix HC, Su D, Selig JP, Ratcliff S, Mcelfish PA. Factors associated with Arkansans' first use of telehealth during the COVID-19 pandemic. Int J Telemdicine Appl. 2022;28(5953027):1–10. doi:10.1155/2022/5953027
75. Achenbach SJ, Brien O. Health law and policy brief Telemedicine: benefits, challenges, and its great potential. Heal Law Policy Br. 2020;14:1.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.