Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 18
Autoantibody Ordering Patterns Across a Tertiary Hospital: A Retrospective Audit
Authors Alqatari SG ![]() , Al Shubbar MD
, Al Shubbar MD ![]() , Alodaini A
, Alodaini A ![]() , Obeid OE, Alhussain M, Aldajani K
, Obeid OE, Alhussain M, Aldajani K ![]() , Hasan M
, Hasan M ![]() , Al-Abdulwahab AA
, Al-Abdulwahab AA ![]() , Alasaker NA, Alzuhair HM, AlNujaidi DY, Alwaheed AJ
, Alasaker NA, Alzuhair HM, AlNujaidi DY, Alwaheed AJ ![]() , Aldarweesh HH, AlSulaiman RS
, Aldarweesh HH, AlSulaiman RS ![]() , Alghamdi R, Alkuwaiti MA
, Alghamdi R, Alkuwaiti MA
Received 15 February 2026
Accepted for publication 23 June 2026
Published 30 June 2026 Volume 2026:18 603681
DOI https://doi.org/10.2147/OARRR.S603681
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Chuan-Ju Liu
Safi G Alqatari1 , Mohammed D Al Shubbar1, Amal Alodaini2, Obeid E Obeid3, Mohammed Alhussain1, Khalid Aldajani1, Manal Hasan1, Abdullah A Al-Abdulwahab1, Norah A Alasaker1, Hajer Musaab Alzuhair1, Danya Y AlNujaidi1, Abrar J Alwaheed1, Huda Hassan Aldarweesh1, Reem S AlSulaiman1, Raghad Alghamdi1, Mohanad A Alkuwaiti1
1Department of Internal Medicine, College of Medicine, Imam Abdulrahman Bin Faisal University, King Fahd University Hospital, Dammam, Eastern Province, 31441, Saudi Arabia; 2Department of Pathology and Laboratory Medicine, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Eastern Province, 31441, Saudi Arabia; 3Department of Microbiology, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Eastern Province, 31441, Saudi Arabia
Correspondence: Mohammed D Al Shubbar, Email [email protected]
Background: Autoantibody testing supports the diagnosis of systemic autoimmune diseases, but indiscriminate use in low pre-test probability settings can reduce test positivity and inflate direct laboratory costs. Hospital-wide audits of real-world ordering practices across specialties remain scarce and, to our knowledge, have not been reported in the Gulf region.
Objectives: To describe the test positivity rate, direct laboratory cost, and departmental variation of hospital-wide autoantibody testing in a tertiary center in the Eastern Province of Saudi Arabia.
Methods: We conducted a retrospective hospital-wide audit of all autoantibody tests ordered across 15 clinical departments at King Fahd University Hospital between 1 January and 30 April 2024. Test volumes, positivity rates, and direct laboratory costs were summarized at departmental and subspecialty levels. Rheumatology was compared with all non-rheumatology services as a pre-specified inferential contrast using chi-square or Fisher exact tests with 95% Wilson confidence intervals and Benjamini–Hochberg adjustment across per-marker comparisons; the unit of analysis was the test order.
Results: A total of 5973 autoantibody tests were performed in 1059 patients, with an overall test positivity rate of 16.3% (95% CI 15.4– 17.2). Total direct laboratory expenditure was USD 509,136, of which 87% was attributable to negative results. Test positivity ranged from 26% in Pediatrics to ≤ 7% in Neurology and Neurosurgery. Rheumatology had a higher positivity rate (24.4%, 95% CI 22.2– 26.8) than non-rheumatology services combined (13.9%, 95% CI 12.9– 14.9; p< 0.001), with the largest absolute differences for antinuclear antibodies (88.7% vs 35.7%; p< 0.001) and SSA antibodies (27.9% vs 5.9%; p< 0.001). Direct cost per positive result was USD 364 in Rheumatology versus USD 606 in non-rheumatology services.
Conclusions: In this single-center audit, autoantibody ordering practices clustered into two descriptive patterns: hypothesis-driven, higher-positivity testing within specialist care and broader, lower-positivity panel use in several non-specialist services. These differences were statistically significant and most plausibly reflect more disciplined application of pre-test probability by specialists, although referral filtering and case-mix differences contribute and cannot be fully separated from clinician-level reasoning in this dataset. These patterns suggest that targeted diagnostic stewardship—reflex-cascade algorithms, order-menu redesign, and indication-based gating—could concentrate autoantibody testing where pre-test probability is highest, improving positivity and reducing avoidable cost without restricting clinical access.
Keywords: autoantibodies, test positivity rate, laboratory utilization, cost analysis, diagnostic stewardship, antinuclear antibodies, rheumatology, Saudi Arabia
Introduction
Autoantibody testing is central to the diagnosis and classification of systemic autoimmune diseases,1 A broad range of assays is routinely used across specialties to evaluate patients with unexplained inflammatory or systemic presentations.1,2 When applied in appropriate clinical contexts, these tests provide substantial diagnostic value; for example, ANA positivity is an entry criterion for systemic lupus erythematosus classification, and disease-specific autoantibodies can delineate clinically meaningful subtypes.3 However, their widespread availability has also enabled increasingly indiscriminate use, particularly in settings with low pre-test probability, diminishing diagnostic yield and increasing the risk of non-contributory or misleading results.4,5
Growing evidence indicates that autoantibody tests are frequently overutilized worldwide.6 Broad autoimmune panels are often requested despite poorly defined clinical suspicion, resulting in high testing volumes with modest diagnostic yield.7 Audits from high-income health systems consistently show that most results are negative or clinically non-contributory. In a Canadian regional analysis, fewer than 17% of ANA, anti-dsDNA, and ENA tests were positive, and nearly half of ENA/anti-dsDNA orders were placed concurrently with the initial ANA rather than in a stepwise manner.6 Inefficient repeat testing further compounds this problem: ANA is frequently reordered after an initial negative result, despite seroconversion to a clinically meaningful titer occurring in only a small minority of patients (≈1%).6 Together, these findings illustrate how reflexive panel ordering consumes laboratory resources while providing limited incremental diagnostic value.
The consequences of indiscriminate autoantibody testing extend beyond cost and workload. In low pre-test probability populations, positive results are disproportionately likely to represent false positives or incidental findings rather than true disease markers.7–9 ANA reactivity, for instance, is detectable in a substantial minority of healthy individuals and across numerous non-rheumatic conditions.9–11 In low pre-test probability settings, indiscriminate serologic screening increases false-positive results and may prompt unnecessary follow-up testing and patient anxiety.7 In some cases, misleading laboratory signals expose patients to unnecessary investigations or incorrect diagnostic labels, representing a recognized form of iatrogenic harm.4,12 Consequently, autoantibody overutilization represents not only an economic inefficiency but also a clinically meaningful patient-safety concern.
In response, international initiatives have emphasized high-value, indication-based testing. The Choosing Wisely campaign—endorsed by organizations including the American College of Rheumatology and the Canadian Rheumatology Association—discourages ANA testing in the absence of clinical features suggestive of systemic autoimmune disease.7 This guidance reflects a core diagnostic stewardship principle: when pre-test probability is low, a positive result is statistically more likely to represent an incidental or false-positive finding than a true disease signal.7,11,12 Complementary stewardship interventions, including clinician education, audit-and-feedback, and laboratory algorithms restricting downstream testing unless screening results justify escalation, have demonstrated measurable benefit. Such strategies reduce unnecessary ANA ordering, improve positivity rates by concentrating testing in higher-risk populations, and can substantially decrease autoantibody testing expenditure without compromising detection of clinically meaningful disease.6,12
Despite these advances, hospital-wide audits capturing autoantibody utilization across all clinical departments remain uncommon and are particularly scarce in tertiary-care centers in the Arabian Peninsula and the broader Middle East. To our knowledge, no comparable institution-wide multi-assay evaluation has been published from the Gulf region. A recent large Saudi audit of antinuclear antibody testing reported substantial repeat and inappropriate ordering concentrated outside rheumatology, but addressed only a single marker. Whether such patterns extend across the broader autoantibody panel and differ by clinical department remains unexamined in this setting—the gap this hospital-wide, multi-assay audit is designed to address.13 This gap is clinically relevant because autoimmune disease prevalence, training pathways, referral structures, and laboratory access vary by region, and indiscriminate serologic testing in this setting carries both substantial resource implications and the potential for diagnostic harm.
To address this gap, we conducted a hospital-wide retrospective audit of all autoantibody orders placed during the first four months of 2024 at King Fahd University Hospital, a major tertiary center in the Eastern Province of Saudi Arabia. We quantified the test positivity rate, mapped utilization patterns and direct laboratory cost across 15 departments, and compared Rheumatology with the pooled non-rheumatology services as a pre-specified inferential contrast. We use the term test positivity rate (positive tests / total tests performed) throughout, in preference to diagnostic yield, because this study does not adjudicate clinical appropriateness against a gold standard. The novelty of this work lies in being, to our knowledge, the first hospital-wide multi-assay autoantibody audit from the Eastern Province of Saudi Arabia, integrating positivity, direct cost, and department-level utilization in a single tertiary center. By describing the institutional “geography” of ordering—including high-volume, low-positivity hotspots—this study provides a pragmatic evidence base to inform targeted diagnostic stewardship interventions.
Materials and Methods
Study Design and Setting
This is a retrospective hospital-wide audit using routinely collected laboratory and financial data, conducted at King Fahd University Hospital (KFUH), a tertiary academic referral center affiliated with Imam Abdulrahman Bin Faisal University in Dammam, Eastern Province, Saudi Arabia. The study characterized hospital-wide autoantibody testing in terms of test positivity rate, direct laboratory cost, and departmental variation in ordering practices. All autoantibody orders placed across all clinical departments between 1 January 2024 and 30 April 2024 inclusive were eligible for inclusion. The four-month window was chosen to balance completeness of recent ordering behavior against the manual data-extraction workload required for an institution-wide audit; this window also corresponds to the most recent complete operational quarter before data extraction began. The study adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cross-sectional studies.14,15
Data Sources and Collection
Data was obtained from the hospital’s laboratory information system, which is accessed through electronic medical records. For each month of the study period, the authors manually extracted comprehensive data for all patients who had testing of the predefined panel of 28 autoantibody assays placed during the study period in any clinical department. The extracted data included patient demographics, ordering department, test requisition dates, laboratory results, and associated costs. Financial data, including unit test costs and departmental expenditures, were obtained from the hospital’s financial records system. All data were de-identified prior to analysis in accordance with institutional privacy protocols.
Laboratory Methods and Definitions
ANA testing was performed using indirect immunofluorescence assay on HEp-2 cells, the international reference method for ANA detection.16 A positive ANA result was defined a priori as a titer of ≥1:160, consistent with the Agmon-Levin et al international recommendations16 and with KFUH laboratory reporting conventions. Although a 1:80 cutoff is endorsed by the 2019 EULAR/ACR SLE classification criteria for screening purposes,3 a 1:160 threshold was selected to reflect real-world clinical interpretation in our institution and to improve specificity in a low pre-test probability mixed-specialty population, where the 1:80 cutoff is known to yield a high proportion of clinically non-contributory positives.5,9–11 Tests with titers below 1:160 were classified as negative. For patients with multiple ANA tests during the study period, each test was counted as a separate order (test-level unit of analysis); patient-level counts are reported separately where indicated.
This study examined autoantibody testing at two levels: (i) an initial ANA test performed by indirect immunofluorescence on HEp-2 cells, used as a high-sensitivity screening assay for systemic autoimmune rheumatic diseases, and (ii) extended autoantibody panel tests, including disease-specific markers such as anti-double-stranded DNA (anti-dsDNA), extractable nuclear antigens (SSA, SSB, Smith, RNP), rheumatoid factor, anti-cyclic citrullinated peptide (anti-CCP) antibodies, ANCA, and additional specialized autoantibodies (total panel = 28 assays). Extended panel testing was performed following positive ANA or based on specific clinical suspicion, although adherence to stepwise ordering was not assessed at the individual order level. Throughout this manuscript, “ANA testing” refers specifically to the initial screening test, while “autoantibody testing” refers to the complete panel of 28 antibody markers evaluated in this study.
All autoantibody assays were performed in the Department of Laboratory Medicine, King Fahd University Hospital, on the routine clinical immunology service. Antinuclear antibodies were detected by indirect immunofluorescence on HEp-2 cells; the extractable nuclear antigen markers (anti-Sm, anti-Ro/SSA, anti-La/SSB, anti-RNP, anti-Scl-70), antiphospholipid antibodies (anti-β2-glycoprotein I and anti-cardiolipin), PR3, MPO, and anti-tissue transglutaminase were measured by chemiluminescent immunoassay, while anti-dsDNA, ANCA, and the liver/connective-tissue immunofluorescence assays (AMA, anti-LKM, ASMA, EMA) were performed by indirect immunofluorescence. The analytical method for each individual assay is detailed in Supplementary Table 1.
Study Variables and Measurements
The primary descriptive outcomes were test positivity rate and direct laboratory cost per positive result by department and subspecialty. The test positivity rate was calculated as the number of positive tests divided by the total number of tests performed, expressed as a percentage with 95% Wilson confidence intervals where applicable. Total departmental expenditure was calculated by multiplying the number of tests by the standard unit cost per test. Direct laboratory cost attributable to negative results was defined as the number of negative tests multiplied by the unit cost; we use this term in place of “budget loss” to reflect that negative results are an inherent and often informative outcome of diagnostic testing, not a financial loss per se. The negative-expenditure proportion for each department was calculated as the cost of negative tests divided by total expenditure. Departments were classified by negative-expenditure proportion into descriptive efficiency categories: good (<80%), borderline (80–85%), poor (85–90%), and inappropriate (>90%). These categories are descriptive labels used to communicate utilization patterns and should not be interpreted as quality-of-care judgments at the individual clinician or department level.
Departmental Classification and Subgroup Analysis
Clinical departments were categorized into two main groups for comparative analysis: specialist departments (Rheumatology) and non-specialist departments (all other clinical services). Internal Medicine was further subdivided into subspecialty services, including Rheumatology, Hepatology, Nephrology, Hematology, Cardiology, Pulmonology, Infectious Diseases, General Internal Medicine, Endocrinology, and Gastroenterology to examine within-department variation. For extended antibody panel analysis, test performance was evaluated across three contexts: Rheumatology department only, all hospital departments combined, and all hospital departments excluding Rheumatology.
Cost Analysis
All costs were expressed in United States Dollars (USD) and represent the hospital’s 2024 internal (true) direct laboratory unit costs—the actual per-assay cost to the laboratory of performing each test—rather than hospital charge rates or payer reimbursement values. These costs include direct laboratory expenditure only and do not capture downstream costs (imaging, referrals), indirect costs, or institutional overhead. For each department we calculated total expenditure (number of tests × unit cost), direct cost attributable to negative results (number of negative tests × unit cost), and direct cost per positive result (total expenditure ÷ number of positive tests). The overall hospital-wide direct cost was determined by summing expenditures across all departments. We do not present hypothetical savings projections, as these would require assumptions about clinical appropriateness that cannot be adjudicated from the retrospective dataset; instead, we report observed cost per positive as a benchmarking metric.
Statistical Analysis
The unit of analysis was the individual test order. Continuous variables were summarized as totals or means and categorical variables as counts and percentages. Test positivity was expressed as positive tests divided by total tests performed and reported with two-sided 95% Wilson score confidence intervals (without continuity correction). The pre-specified primary inferential contrast was the Rheumatology department versus the pooled non-rheumatology services, evaluated for overall positivity and for each antibody marker. Each 2×2 comparison used Pearson chi-square without continuity correction when every expected cell count was ≥5, and the two-sided Fisher exact test otherwise. Effect sizes were reported as absolute differences in positivity (percentage points); odds ratios were not reported because the study design does not estimate sampling-based exposure–disease associations. Per-marker p-values were adjusted by the Benjamini–Hochberg (BH) procedure across a pre-specified family of 21 markers for which the 2×2 comparison was non-degenerate (≥1 positive in either arm and ≥2 tests in each arm); anti-parietal cell antibody, with only one test in the Rheumatology arm, was excluded on this basis. Department-by-department pairwise testing was not performed because case-mix heterogeneity between individual departments precludes meaningful causal interpretation; department-level findings are reported descriptively with Wilson 95% confidence intervals. Because the unit of analysis is the test order and a single patient could contribute multiple orders, the independence assumption is approximate; patient-level linkage was not retrievable, so a cluster-robust sensitivity analysis could not be performed and is acknowledged as a limitation. No a priori power calculation was undertaken because the study analyzed the full population of eligible orders during the audit window rather than a sample. A sensitivity analysis at the 2019 EULAR/ACR 1:80 ANA cutoff was not performed because raw titer values below the 1:160 reporting threshold were not retrieved from the laboratory information system extract (instead considered as negative). All tests were two-sided at α = 0.05. Analyses were performed in Python 3.11 (SciPy 1.11, statsmodels 0.14) and cross-validated in R 4.x.
Ethical Considerations
This study was approved by the Institutional Review Board of Imam Abdulrahman Bin Faisal University on 15 December 2024 (protocol code IRB-2024-01-435). The requirement for informed consent was waived given the retrospective design using de-identified routine laboratory and financial data. All data were handled in accordance with institutional data-protection policies and applicable regulations, and no patient-identifying information was included in the final dataset or analyses.
Results
Department-Level Autoantibody Testing Volume and Positivity Rates
Across 15 clinical departments, 5973 autoantibody tests were performed in 1059 patients, yielding an overall test positivity rate of 16.3% (95% CI 15.4–17.2; Table 1). Internal Medicine accounted for the largest testing volume with 2846 tests (47.6%), followed by Neurology with 1487 (24.9%), and Family Medicine with 332 (5.6%). The remaining 12 departments collectively contributed 1308 tests (21.9%). Test positivity rates differed by department. Pediatrics demonstrated the highest positivity (26%), followed by Internal Medicine (21%) and Orthopedics (20%). In contrast, Neurology (7%) and Neurosurgery (2%) showed markedly lower positivity, while Radiology and Psychiatry had 0% positivity (Table 1). High-volume departments exhibited heterogeneous performance, with positivity ranging from 7% to 26%. Department-level comparisons are presented descriptively with rounded percentages; formal inferential testing across departments was not performed for the reasons outlined in §2.7.
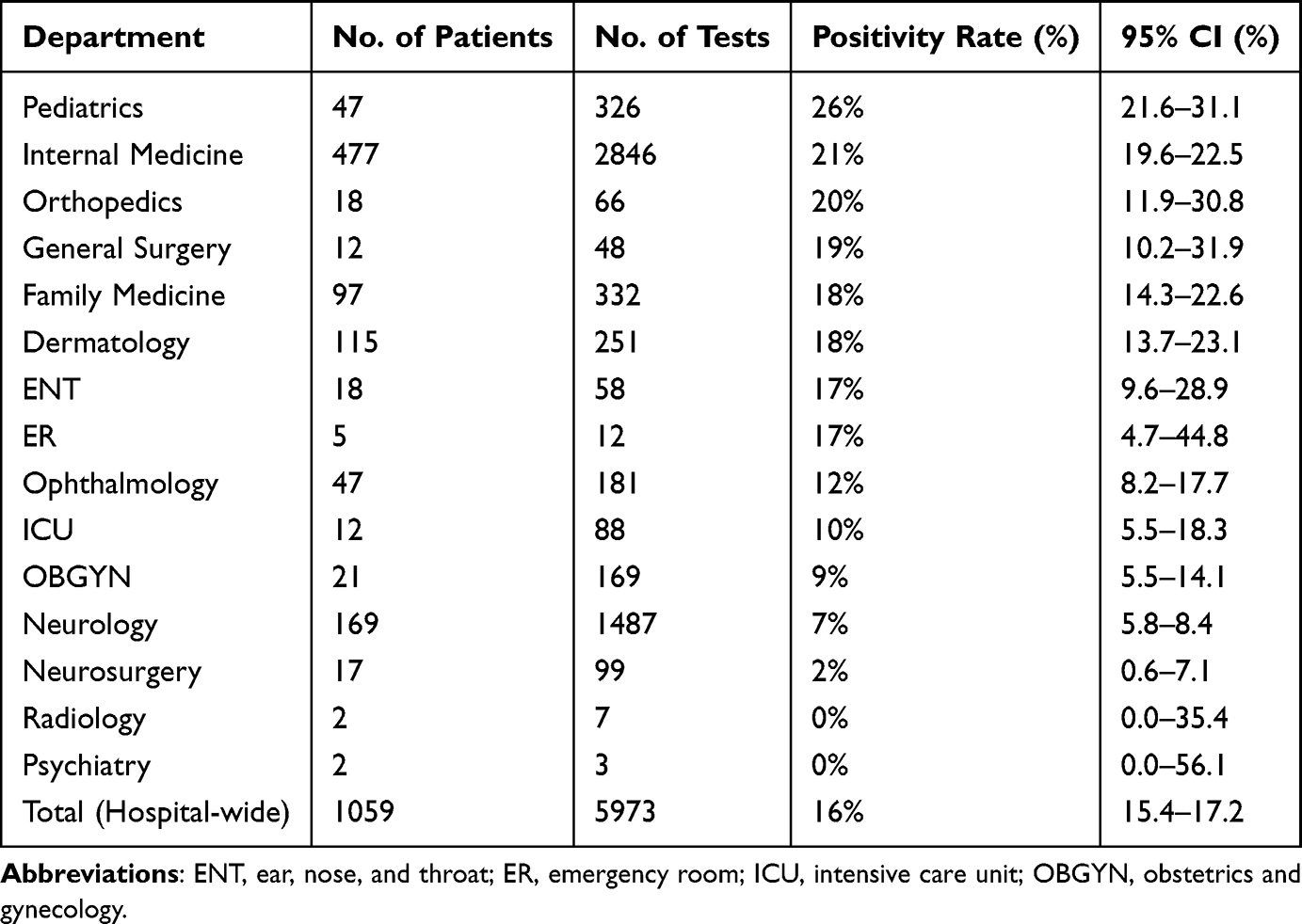 |
Table 1 Autoantibody Testing Volume and Positivity Rate by Department |
Department-Level Autoantibody Testing Costs and Negative-Result Expenditure
Total hospital expenditure for autoantibody testing during the study period was USD 509,136, of which USD 440,525.33 (87%) was attributable to negative results (Table 2). The overall direct cost per positive result for the hospital was USD 524. Internal Medicine incurred the highest absolute expenditure at USD 246,733.33, with 83% attributable to negative tests. Neurology accounted for USD 133,762.67, with 94% attributable to negative tests. Radiology (USD 573.33) and Psychiatry (USD 138.67) had complete negative-expenditure proportions. Across departments, the negative-expenditure proportion ranged from 77% in Pediatrics to 100% in Radiology and Psychiatry. Several medium-volume departments—including Ophthalmology, Dermatology, and OBGYN—showed persistently high negative-expenditure proportions at 85%, 85%, and 94%, respectively, despite moderate total spend (Table 2). The departmental performance matrix (Figure 1) summarizes the joint distribution of test volume, positivity, and expenditure. Rheumatology itself fell within the Borderline efficiency tier (81% negative-expenditure proportion); no department other than Pediatrics achieved Good efficiency (<80% negative expenditure).
 |
Table 2 Department-Level Autoantibody Testing Costs and Negative-Result Expenditure |
 |
Figure 1 Department-level Autoantibody Testing Performance and Cost Efficiency. Bubble area is proportional to total departmental testing expenditure (USD). Departments with identical test positivity rates have been offset vertically for visual clarity. |
Internal Medicine Subspecialty Performance
Within Internal Medicine, subspecialty-level analysis revealed marked heterogeneity in both spending and negative-expenditure proportion (Table 3). Rheumatology accounted for 119,778.67 USD in expenditure with an 81% negative-expenditure proportion, representing the largest subspecialty expenditure. General Internal Medicine spent 64,832.00 USD with an 84% negative-expenditure proportion. Hepatology, despite relatively lower volume, demonstrated a 77% negative-expenditure proportion with 11,578.67 USD expended. The highest negative-expenditure proportions were observed in Cardiology and Infectious Diseases, both at 100%, though these subspecialties represented smaller absolute expenditures. Hematology exhibited a 91% negative-expenditure proportion, while Gastroenterology and Endocrinology showed 87% negative-expenditure proportions.
 |
Table 3 Internal Medicine Subspecialty Autoantibody Testing Costs and Negative-Result Expenditure |
Moreover, testing volume and positivity rates among Internal Medicine subspecialties further demonstrated the performance gradient (Table 4). Rheumatology performed 1346 tests with a 24% positivity rate among 165 patients, substantially higher than other subspecialties. General Internal Medicine conducted 764 tests with a 19% positivity rate across 159 patients. Hepatology achieved a 28% positivity rate, but this was based on a smaller volume of 134 tests conducted on 30 patients. Notably, several subspecialties, including Cardiology and Infectious Diseases demonstrated 0% positivity. The aggregate Internal Medicine performance of 2846 tests with 21% positivity concealed this marked subspecialty-level heterogeneity.
 |
Table 4 Internal Medicine Subspecialty Autoantibody Testing Volume and Positivity Rate |
Hospital-Wide Antibody Panel Performance
Hospital-wide autoantibody testing encompassed a comprehensive panel of 28 different antibody assays, each demonstrating varying diagnostic performance (Table 5). ANA screening, the most frequently ordered test, showed 45% positivity (560 positive of 1254 tests). Disease-specific antibody positivity rates varied: anti-dsDNA showed 9% positivity from 548 tests; anti-Smith antibody, 9% from 303 tests; and SSA antibody, 12% from 360 tests. Thyroid antibodies showed higher positivity rates, with TPO at 33% (28/86) and TG at 34% (26/77). Several antibody tests yielded very low or zero positivity, including SCL-70 at 0% (0/64), TTG at 0% (0/4), and HLA-B27 at 0% (0/1). HLA-B51 was an outlier with 2/2 positive (100%); given the trivial test volume, this should not be interpreted as a performance signal and was excluded from comparative analyses. The overall test positivity rate across all assays was 16.3% (95% CI 15.4–17.2).
 |
Table 5 Antibody Test Performance Across All Hospital Departments |
Rheumatology Department Antibody Performance
Antibody testing within the Rheumatology department showed higher positivity than the hospital-wide aggregate (Table 6). Among 165 Rheumatology patients, ANA testing yielded 88.7% positivity (188/212 tests; 95% CI 83.7–92.3). Disease-specific antibodies also showed enhanced positivity rates in the specialist context: anti-dsDNA reached 15.1% positivity (24/159 tests; 95% CI 10.4–21.5), SSA demonstrated 27.9% positivity (29/104 tests; 95% CI 20.2–37.2), and RNP showed 14.0% positivity (6/43; 95% CI 6.6–27.3). Anti-CCP testing in Rheumatology yielded 17.9% positivity (12/67; 95% CI 10.6–28.7). The overall positivity rate for all antibody tests ordered by Rheumatology was 24.4% (329/1346; 95% CI 22.2–26.8). Direct cost per positive result in Rheumatology was USD 364.
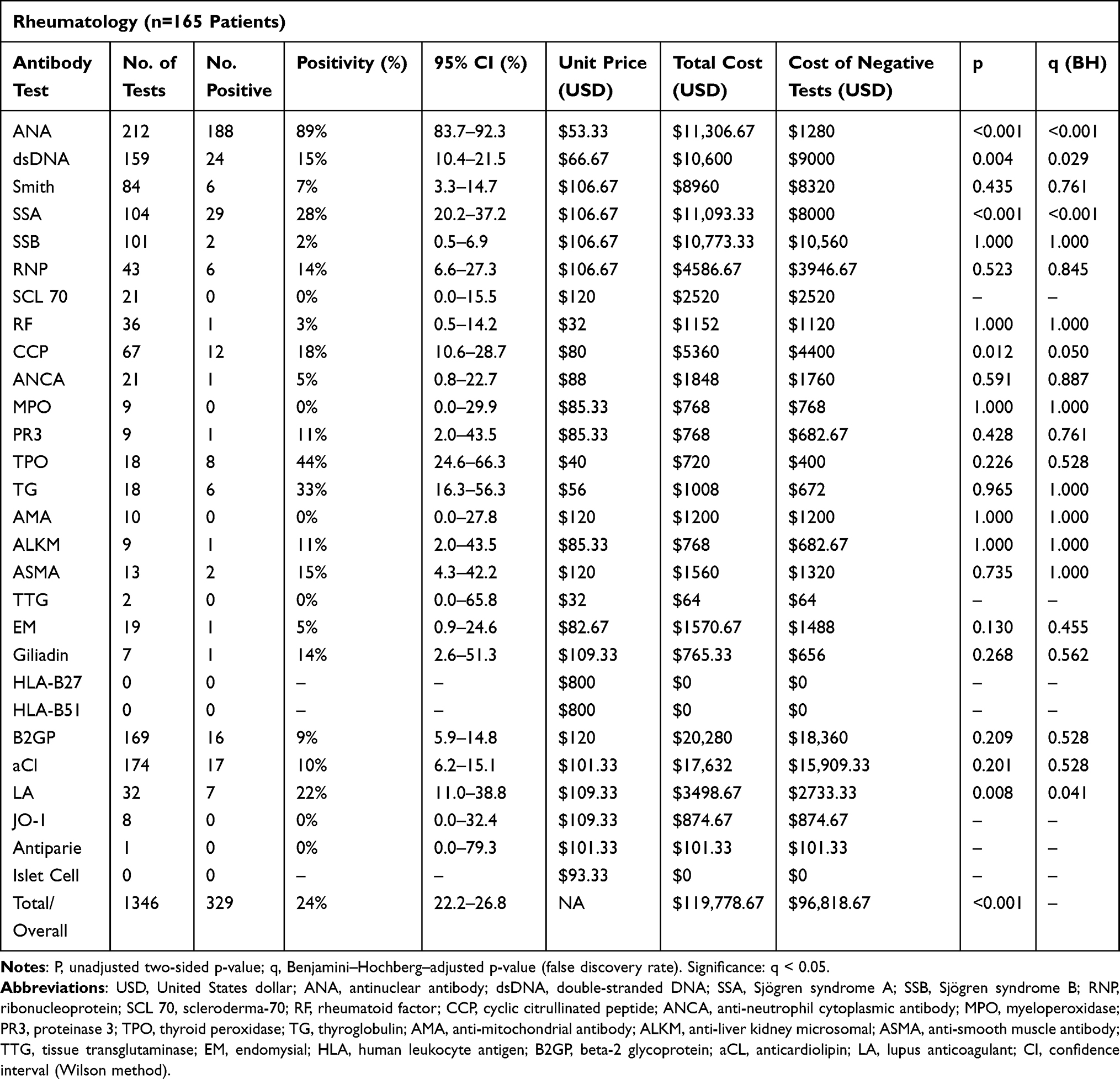 |
Table 6 Antibody Test Performance in Rheumatology Department |
Non-Rheumatology Department Antibody Performance
Antibody testing performance in non-rheumatology departments showed lower positivity across most markers (Table 7). ANA positivity among the 894 non-rheumatology patients was 35.7% (372/1042 tests; 95% CI 32.8–38.7), substantially lower than in Rheumatology (88.7%; χ2 p<0.001). Anti-dsDNA positivity was 7.2% (28/389; 95% CI 5.0–10.2) compared with 15.1% in Rheumatology (χ2 p=0.004). SSA positivity was 5.9% (15/256; 95% CI 3.6–9.4) versus 27.9% (χ2 p<0.001). Anti-CCP positivity was 6.9% (11/160; 95% CI 3.9–11.9) versus 17.9% (χ2 p=0.012). Lupus anticoagulant showed 4.5% (4/88; 95% CI 1.8–11.1) versus 21.9% (7/32) in Rheumatology (Fisher p=0.008). The overall positivity rate for all antibody testing in non-rheumatology departments was 13.9% (643/4627; 95% CI 12.9–14.9), lower than Rheumatology’s 24.4% (χ2 p<0.001). Direct cost per positive result in non-rheumatology services was USD 606, compared with USD 364 in Rheumatology. The comparative table (Table 8) summarizes this descriptive difference in test performance across clinical contexts.
 |
Table 7 Antibody Test Performance in Non-Rheumatology Departments |
 |
Table 8 Antibody Test Positivity Rates (%) Across Clinical Contexts |
Specialist versus Non-Specialist Testing Patterns
Direct comparison between Rheumatology and the combined non-rheumatology services revealed a consistent positivity gap across key autoimmune markers (Figure 2 and Tables 6, 7). For ANA testing, the gap was largest in absolute terms, with Rheumatology at 88.7% versus 35.7% in non-rheumatology services (Δ = 53 percentage points; χ2 p<0.001). SSA antibody showed a 22-point gap (27.9% vs 5.9%; χ2 p<0.001). Anti-dsDNA was 15.1% versus 7.2% (χ2 p=0.004), and anti-CCP was 17.9% versus 6.9% (χ2 p=0.012). Some assays showed similar positivity regardless of ordering context, including SSB (2.0% vs 2.0%; Fisher p=1.0), TG (33.3% vs 33.9%; χ2 p=0.96), TPO (44.4% vs 29.4%; χ2 p=0.23), and ANCA (4.8% vs 4.0%; Fisher p=0.59). These were pre-specified inferential contrasts; the statistically significant differences quantify real between-context gaps that most plausibly reflect more disciplined, pre-test-probability-anchored ordering by specialists, with referral filtering and case mix contributing as partial mediators that cannot be fully separated in this retrospective dataset. Notably, Smith (7% vs 10%), RF (3% vs 5%), SSB (2% vs 2%), and TG (33% vs 34%) showed no meaningful positivity gap between Rheumatology and non-Rheumatology settings.
 |
Figure 2 Rheumatology vs. Non-Rheumatology Testing Performance: The Expertise Gap. The 10 most frequently ordered markers are displayed. Note: non-specialist positivity rates equal or exceed specialist rates for Smith (7% vs 10%), RF (3% vs 5%), SSB (2% vs 2%), and TG (33% vs 34%). |
The cost-efficiency waterfall chart (Figure 3) illustrates the cumulative direct-cost impact of this differential performance, showing progressive accumulation of negative-result expenditure across the USD 509,136 total expenditure through the inappropriate (>90% negative expenditure), poor (85–90%), borderline (80–85%), and good (<80%) efficiency categories. The Borderline efficiency tier (80–85%) accounted for the largest share of negative-result expenditure at 44.7% (USD 227,808), driven predominantly by Internal Medicine.
 |
Figure 3 Cost-Efficiency Waterfall: Distribution of Negative-Result Expenditure. Total expenditure: USD 509,135.99 (100%). Expenditure on negative tests: USD 440,525.32 (86.5%). Expenditure on positive tests: USD 68,610.67 (13.5%). Negative-result expenditure by efficiency tier: Inappropriate 30.7%, Borderline 44.7%, Poor 6.8%, Good 4.3%. |
Discussion
In this hospital-wide audit at a tertiary academic center, autoantibody testing yielded an overall test positivity rate of 16.3% (95% CI 15.4–17.2) against a direct laboratory expenditure of USD 509,136, of which 87% was attributable to negative results. Test positivity varied sharply by clinical context. Rheumatology achieved a positivity rate of 24.4% (95% CI 22.2–26.8), whereas the pooled non-rheumatology services achieved 13.9% (95% CI 12.9–14.9; χ2 p<0.001). Direct cost per positive result mirrored this gradient, at USD 364 in Rheumatology versus USD 606 in non-rheumatology services. The contrast was driven not by isolated outliers but by a coherent pattern across multiple disease-specific assays—most prominently ANA (88.7% vs 35.7%; χ2 p<0.001) and SSA (27.9% vs 5.9%; χ2 p<0.001)—after Benjamini–Hochberg adjustment.
This positivity gradient reflects the structural difference between specialist and non-specialist diagnostic environments rather than a difference in clinician diligence. Rheumatologists order autoantibody panels in a phenotype-anchored, confirmatory mode: a defined clinical syndrome generates a pre-test probability that justifies the assay, and the test is interpreted against that prior. Non-specialist services—internal medicine wards, the emergency department, and consult teams managing undifferentiated patients—operate under different epistemic constraints. They confront systemic inflammation, organ dysfunction, or constitutional symptoms of uncertain origin, and autoantibody panels are frequently deployed to broaden, rather than confirm, a differential diagnosis. This pattern is consistent with broader observations that diagnostic testing is overutilized when readily accessible and culturally framed as a discretionary add-on rather than a hypothesis-linked confirmatory tool,17–19 and with reports of attenuated positivity outside rheumatology-guided pathways.4,19
Neither approach is inherently inappropriate; both reflect rational responses to the information environment in which the clinician is operating. The relevant distinction is that phenotype-anchored ordering uses autoantibodies as their developers intended—to classify disease, refine diagnoses, and identify clinically meaningful subtypes1–3—whereas exploratory ordering predictably dilutes predictive value, because the test’s positive predictive value declines steeply as pre-test probability falls.
Internal Medicine illustrated this gradient most clearly. Within the department, Hepatology emerged as a high-yield subspecialty (positivity ≈28%), consistent with phenotype-driven indications for autoimmune hepatitis, primary biliary cholangitis, and primary sclerosing cholangitis, in which ANA, ASMA, AMA, and anti-LKM are anchored to defined hepatic syndromes. Rheumatology and Hepatology therefore exemplify the same operating logic from different anatomical vantage points: clinical phenotype precedes serology, and serology confirms or refines an existing hypothesis. Neurology, in contrast, exhibited a high-volume, low-positivity pattern (≈7%) that reflects the systemic-screening role autoantibody panels are asked to play in undifferentiated neurological presentations. A critical interpretive caveat applies: autoimmune encephalitis is mediated by neural surface and intracellular antibodies (eg, anti-NMDAR, anti-LGI1, anti-CASPR2), and these neural-antigen panels are not available at our institution. The Neurology ordering captured here therefore cannot support work-up of autoimmune encephalitis and should not be interpreted as such. The subspecialty pattern as a whole supports a gradient model in which diagnostic yield is determined by the prevalence of relevant disease in the tested population and by how tightly each order is tethered to a defined clinical question—precisely the targets that Choosing Wisely–type stewardship frameworks aim to address.7,20
The specialist–non-specialist positivity gradient was not uniform across assays, and several markers—including anti-Smith, rheumatoid factor, anti-SSB, and thyroglobulin antibodies—showed comparable or marginally higher positivity in non-rheumatology settings (Figure 2). Anti-SSB is the most instructive example: positivity was identical in Rheumatology and non-rheumatology services (2.0% in both; 2/101 versus 5/249; Fisher p=1.000), in contrast to anti-SSA, which showed one of the widest specialist gaps in the dataset (27.9% versus 5.9%; χ2 p<0.001). This dissociation is best explained by the biology of the two markers rather than by ordering behavior. Anti-SSA/Ro is both more sensitive than anti-SSB/La in Sjögren syndrome and is detectable across a broader range of connective-tissue diseases, including systemic lupus erythematosus, so it retains diagnostic signal even when applied to a clinically diverse population.21 Anti-SSB/La, by contrast, almost never occurs in isolation: it is typically found together with anti-SSA, whereas anti-SSA is frequently positive when anti-SSB is negative.22,23 Isolated anti-SSB positivity (anti-SSB-positive, anti-SSA-negative) carries limited and increasingly questioned diagnostic value,22,23 and anti-SSB/La was removed from the 2016 ACR/EULAR classification criteria for primary Sjögren syndrome, which now retain only anti-SSA/Ro among the serologic items.24 The ordering data in our own cohort reinforce that this is an assay-level phenomenon rather than a specialist-versus-non-specialist one: within Rheumatology, anti-SSA and anti-SSB were ordered in near-lockstep (104 and 101 tests, respectively), consistent with the two being requested together as a fixed “Sjögren panel” rather than selected individually on clinical grounds. When a low-yield assay is reflexively co-ordered with a higher-yield partner in this way, its positivity rate is governed by the test’s intrinsic performance and not by who orders it—so even disciplined specialist ordering cannot raise the positivity of anti-SSB above its biological ceiling.
Thyroglobulin antibodies illustrate the same principle through a different mechanism. Positivity was high and essentially equal across contexts (33% in Rheumatology versus 34% in non-rheumatology services; χ2 p=0.96), with no specialist advantage. This reflects how the assay is used in practice rather than a difference in ordering discipline: anti-thyroglobulin antibody is not employed as a population screening test for thyroid disease but is requested almost exclusively in patients already under evaluation or follow-up for established thyroid pathology—most prominently as an adjunct to serum thyroglobulin in the surveillance of differentiated thyroid cancer, where thyroglobulin antibodies are co-measured because they interfere with the thyroglobulin assay.25 For autoimmune thyroid disease, anti-thyroglobulin adds little discriminatory information beyond anti-thyroid peroxidase antibody and is not recommended as a primary or screening marker.25 Because the assay is therefore ordered into an already thyroid-disease-enriched population in both specialist and non-specialist settings, its positivity reflects that pre-selection rather than the ordering clinician’s specialty, and the absence of a rheumatology gap is expected.
Taken together, the flat positivity of anti-SSB, anti-Smith, rheumatoid factor, and thyroglobulin antibodies across clinical contexts does not contradict the central finding; rather, it refines it. Stewardship gains are concentrated in phenotype-sensitive assays whose pre-test probability is genuinely modifiable by clinical selection, whereas markers that are uniformly low-yield wherever they are applied—or that are confined to a pre-selected disease population—warrant a different intervention: scrutiny of whether they should be offered as standalone or reflexively bundled orders at all.
Assay-level analysis identified the testing patterns most amenable to systems-based intervention. Man et al documented closely analogous behavior in a Canadian regional cohort—high-volume ANA ordering, frequent early repeat requests after negative results, and concurrent ordering of ENA/anti-dsDNA with ANA—and showed that a reflex-cascade algorithm, repeat suppression, and cancellation of ENA/anti-dsDNA when the index ANA is negative could reduce costs by approximately 30% without compromising case detection.6 Stewardship is most durable when embedded in workflow rather than left to individual restraint, and EHR order-menu redesign has been shown to shift testing patterns toward Choosing Wisely–consistent practice.20 A pragmatic stewardship package for our institution would combine ANA-positive reflex gating before ENA sub-serologies and anti-dsDNA, mirroring Man et al6 and Yeo et al;26 order-menu restructuring to discourage concurrent ENA panel selection in ANA-negative samples;20 indication-anchored EHR prompts for ANCA orders outside compatible phenotypes;27 and audit-and-feedback dashboards benchmarking departmental positivity to internal Rheumatology ordering. Comparable interventions in other settings have reduced unnecessary ANA testing and improved positivity without harming case detection,12 reinforcing that the operative principle is better testing where it makes sense rather than less testing everywhere.12 The assay-level rationale follows directly: ANA reactivity occurs in healthy individuals and in numerous non-rheumatic conditions, so its positive predictive value collapses when applied as broad screening.9–11 ENA sub-serologies should be restricted to ANA-positive patients with compatible connective-tissue features;7 real-world data confirm that ENA positivity in ANA-negative patients is rarely clinically meaningful,26,28 and concurrent rather than sequential ordering of ANA and ENA carries measurable downstream economic consequences.29 Our pattern of high-volume disease-specific testing with weak positivity outside specialist contexts is consistent with the broader phenomenon described as specialized-test drift, in which high-specificity assays are pulled into low-probability screening because they are easy to order.17 The same logic applies to antiphospholipid and vasculitis serologies: APS markers are interpretable only when anchored to thrombosis or pregnancy morbidity rather than indiscriminate screening,30 and Mandl et al demonstrated that applying explicit ANCA test-ordering guidelines reduced ordering by approximately 23% and lowered the false-positive rate by 27% without missing cases of ANCA-associated vasculitis.27
Several considerations frame the interpretation of these findings. The study’s principal strength is its hospital-wide scope: it evaluates autoantibody utilization across the entire institution rather than within a single specialty, enabling direct comparison between probability-enriched and low–pre-test-probability settings inside a single institutional environment. By integrating ordering volume, positivity, and direct cost, the analysis takes a systems-level view rather than isolated test performance, and similar specialty-associated differences in ANA positivity reported elsewhere support the external coherence of the pattern.31 Several limitations warrant explicit acknowledgment. The retrospective design precludes direct adjudication of appropriateness at the individual test level and cannot support causal claims about ordering quality even where statistical contrasts are significant. Referral and selection bias represent a partial confounder of the Rheumatology versus non-rheumatology contrast: Rheumatology evaluates a pre-enriched population, so the observed positivity gap reflects both more disciplined specialist ordering and higher baseline disease prevalence, and the two contributions cannot be fully separated in this dataset—though the interventional literature confirms that non-specialist workflows can adopt rheumatology-style stewardship logic with measurable benefit.7,20 The single-center design limits generalizability, though our hospital-wide positivity of 16.3% falls within the 13–22% range reported in multi-specialty audits from North America and Europe.4,6,19 The cost analysis captures only direct laboratory expenditure and therefore underestimates the true economic footprint of low-positivity testing, which is more accurately represented by downstream serology, imaging, specialist referrals, length of stay, and treatment changes triggered by non-contributory or false-positive results. Structured chart review was not feasible, so we cannot confirm documented pre-test probability or downstream clinical impact at the order level; demographic and clinical covariates (age, sex, primary diagnosis) were not consistently available; the four-month audit window does not permit assessment of seasonal or temporal trends; and because the unit of analysis is the individual test order rather than the patient, observations are not strictly independent, so reported p-values should be read as approximate. Finally, neural autoantibody assays are not offered at our institution, so a deeper analysis of neurological autoantibody utilization was not possible.
Conclusion
Autoantibody testing at our institution clusters into two operational patterns: a phenotype-anchored, confirmatory mode in specialist services that achieves higher positivity at lower cost per positive result, and a broader exploratory mode in non-specialist services managing undifferentiated patients that accumulates the majority of the USD 509,136 spent on negative results. The implication is not to constrain clinical access to autoantibody testing but to engineer the workflow around it. We propose four concrete interventions: ANA-positive reflex gating before downstream ENA and anti-dsDNA testing, EHR order-menu redesign that prevents concurrent ENA selection in ANA-negative samples, indication-anchored prompts for ANCA and antiphospholipid panels, and audit-and-feedback dashboards that benchmark departmental positivity against internal specialist ordering rather than against an arbitrary external target. A prospective implementation study—ideally an interrupted time series capturing positivity, total testing volume, downstream investigations, and patient-level outcomes—is the appropriate next step to determine whether these interventions improve diagnostic value without compromising case detection.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of Imam Abdulrahman Bin Faisal University on 15 December 2024 (protocol code IRB-2024-01-435).
Data Sharing Statement
The data presented in this study are not publicly available due to institutional policies and ethical restrictions related to patient confidentiality and hospital financial records. De-identified data may be made available from the corresponding author upon reasonable request, subject to Institutional Review Board approval and institutional data-sharing agreements.
Informed Consent Statement
Patient consent was waived due to the retrospective nature of the study using de-identified routine laboratory and financial data.
Acknowledgments
During the preparation of this manuscript, the authors used ChatGPT (OpenAI) for language editing and stylistic refinement. The authors reviewed, edited, and verified the content and take full responsibility for the integrity of the work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Xiao ZX, Miller JS, Zheng SG. An updated advance of autoantibodies in autoimmune diseases. Autoimmunity Rev. 2021;20(2):102743. doi:10.1016/j.autrev.2020.102743
2. Weiner M, Segelmark M. The clinical presentation and therapy of diseases related to anti-neutrophil cytoplasmic antibodies (ANCA). Autoimmunity Rev. 2016;15(10):978–18. doi:10.1016/j.autrev.2016.07.016
3. Aringer M. EULAR/ACR classification criteria for SLE. Semin Arthritis Rheumatism. 2019;49(3):S14–S17. doi:10.1016/j.semarthrit.2019.09.009
4. Rajendran R, Salazar JH, Seymour RL, Laposata M, Zahner CJ. Overutilization and underutilization of autoantibody tests in patients with suspected autoimmune disorders. Diagnosis. 2021;8(4):497–503. doi:10.1515/dx-2020-0139
5. Pisetsky DS. Antinuclear antibody testing — misunderstood or misbegotten? Nat Rev Rheumatol. 2017;13(8):495–502. doi:10.1038/nrrheum.2017.74
6. Man A, Shojania K, Phoon C, et al. An evaluation of autoimmune antibody testing patterns in a Canadian health region and an evaluation of a laboratory algorithm aimed at reducing unnecessary testing. Clin Rheumatol. 2013;32(5):601–608. doi:10.1007/s10067-012-2141-y
7. Yazdany J, Schmajuk G, Robbins M, et al. Choosing wisely: the American College of Rheumatology’s top 5 list of things physicians and patients should question. Arthritis Care Res. 2013;65(3):329–339. doi:10.1002/acr.21930
8. Self SE. Autoantibody Testing for Autoimmune Disease. Clinics Chest Med. 2010;31(3):415–422. doi:10.1016/j.ccm.2010.04.001
9. Li X, Liu X, Cui J, et al. Epidemiological survey of antinuclear antibodies in healthy population and analysis of clinical characteristics of positive population. Clin Lab Anal. 2019;33(8):e22965. doi:10.1002/jcla.22965
10. Satoh M, Chan EKL, Ho LA, et al. Prevalence and sociodemographic correlates of antinuclear antibodies in the United States. Arthritis Rheum. 2012;64(7):2319–2327. doi:10.1002/art.34380
11. Zanussi JT, Zhao J, Wei WQ, et al. Clinical diagnoses associated with a positive antinuclear antibody test in patients with and without autoimmune disease. BMC Rheumatol. 2023;7(1):24. doi:10.1186/s41927-023-00349-4
12. Y P-PB, Neumark E, Kivity S, Tayer-Shifman OE. Mitigating overuse of antinuclear antibody (ANA) testing through educational intervention: a study in internal medicine and neurology departments. Clin Rheumatol. 2024;43(12):3935–3939. doi:10.1007/s10067-024-07180-3
13. Alyami MB, Hakeem MN, Fadil AI, Jee BA, ElAbbasy HM, Ankawi G. Frequency of repeating antinuclear antibody testing: when less is more. Cureus. 2024. doi:10.7759/cureus.52347
14. Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61(4):344–349. doi:10.1016/j.jclinepi.2007.11.008
15. Cuschieri S. The STROBE guidelines. Saudi J Anaesth. 2019;13(5):31. doi:10.4103/sja.SJA_543_18
16. Agmon-Levin N, Damoiseaux J, Kallenberg C, et al. International recommendations for the assessment of autoantibodies to cellular antigens referred to as anti-nuclear antibodies. Ann Rheumatic Dis. 2014;73(1):17–23. doi:10.1136/annrheumdis-2013-203863
17. Zhi M, Ding EL, Theisen-Toupal J, Whelan J, Arnaout R. The landscape of inappropriate laboratory testing: a 15-year meta-analysis. PLoS One. 2013;8(11):e78962. doi:10.1371/journal.pone.0078962
18. Patel H, DeMasters D, Tofferi J. Antinuclear antibody multiplex utilization across a large federal hospital system: an investigation of ordering practices and rheumatologic outcomes. J Rheumatol. 2025. doi:10.3899/jrheum.2024-0641
19. Mohammed AS, Boddu P, Mael D, Samee M, Villines D. Inappropriate use of commercial antinuclear antibody testing in a community-based US hospital: a retrospective study. J Commun Hosp Internal Med Perspect. 2016;6(4):32031. doi:10.3402/jchimp.v6.32031
20. Barry C, Kaufman S, Feinstein D, et al. Optimization of the order menu in the electronic health record facilitates test patterns consistent with recommendations in the choosing wisely initiative. Am J Clin Pathol. 2020;153(1):94–98. doi:10.1093/ajcp/aqz134
21. Fayyaz A, Kurien BT, Scofield RH. Autoantibodies in Sjögren’s Syndrome. Rheum Dis Clin North Am. 2016;42(3):419–434. doi:10.1016/j.rdc.2016.03.002
22. Vílchez-Oya F, Balastegui Martin H, García-Martínez E, Corominas H. Not all autoantibodies are clinically relevant. Classic and novel autoantibodies in Sjögren’s syndrome: a critical review. Front Immunol. 2022;13:1003054. doi:10.3389/fimmu.2022.1003054
23. Cioni P, Chretien P, Goulvestre C, et al. Isolated anti-SS-B (La) antibodies: rare occurrence and lack of diagnostic value. RMD Open. 2025;11(1):e005212. doi:10.1136/rmdopen-2024-005212
24. Shiboski CH, Shiboski SC, Seror R, et al. 2016 American College of Rheumatology/European League Against Rheumatism classification criteria for primary sjögren’s syndrome: a consensus and data-driven methodology involving three international patient cohorts. Arthritis Rheumatol. 2017;69(1):35–45. doi:10.1002/art.39859
25. Giovanella L, D’Aurizio F, Algeciras-Schimnich A, et al. Thyroglobulin and thyroglobulin antibody: an updated clinical and laboratory expert consensus. Eur J Endocrinol. 2023;189(2):R11–R27. doi:10.1093/ejendo/lvad109
26. Yeo AL, Ojaimi S, Le S, Leech M, Morand E. Frequency and clinical utility of antibodies to extractable nuclear antigen in the setting of a negative antinuclear antibody test. Arthritis Care Res. 2023;75(7):1595–1601. doi:10.1002/acr.24990
27. Mandl LA, Solomon DH, Smith EL, Lew RA, Katz JN, Shmerling RH. Using antineutrophil cytoplasmic antibody testing to diagnose vasculitis: can test-ordering guidelines improve diagnostic accuracy? Arch Intern Med. 2002;162(13):1509. doi:10.1001/archinte.162.13.1509
28. Huang J, Dargham BB, Luggen M. Diagnostic utility of antibodies to extractable nuclear antigens in the absence of positive antinuclear antibodies. Cureus. 2025. doi:10.7759/cureus.93419
29. Ethington E, Melrose E, Stratman EJ. The relative timing, outcomes, and economic impact of anti-nuclear antibody (ANA) and extractable nuclear antigen (ENA) laboratory ordering. Clin Med Res. 2024;22(3):123–126. doi:10.3121/cmr.2024.1937
30. Barbhaiya M, Zuily S, Naden R, et al. 2023 ACR/EULAR antiphospholipid syndrome classification criteria. Ann Rheumatic Dis. 2023;82(10):1258–1270. doi:10.1136/ard-2023-224609
31. Santos WFS, Cantuária APDC, Félix DDC, Nardes LK, De Melo ICS. The influence of demography and referral medical specialty on the detection of autoantibodies to HEP-2 cells in a large sample of patients. Adv Rheumatol. 2022;62(1):32. doi:10.1186/s42358-022-00264-1
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.