")
Back to Journals » Clinical Interventions in Aging » Volume 18
Attitudes, Beliefs, and Current Practices Carried Out by Family Physicians in Spain Regarding the Prevention of Road Injuries in Older Adults: A Nationwide Cross-Sectional Study
Authors Jiménez-Mejías E, Ruiz-Rodríguez FI, Martín-delosReyes LM, Herrero-Rubí J, Rivera-Izquierdo M, Martínez-Ruiz V, Lardelli-Claret P
Received 3 October 2022
Accepted for publication 10 January 2023
Published 10 March 2023 Volume 2023:18 Pages 375—385
DOI https://doi.org/10.2147/CIA.S390903
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Maddalena Illario
Eladio Jiménez-Mejías,1– 4 Fátima Isabel Ruiz-Rodríguez,1,5 Luis Miguel Martín-delosReyes,1 José Herrero-Rubí,1 Mario Rivera-Izquierdo,1,3 Virginia Martínez-Ruiz,1– 3 Pablo Lardelli-Claret1– 4
1Department of Preventive Medicine and Public Health, University of Granada, Granada, Spain; 2Centros de Investigación Biomédica en Red de Epidemiología y Salud Pública (CIBERESP), Madrid, Spain; 3Instituto de Investigación Biosanitaria de Granada (ibs.GRANADA), Granada, Spain; 4Chair SEMERGEN-UGR of Teaching and Research in Family Medicine, University of Granada, Granada, Spain; 5Doctorate Program in Clinical Medicine and Public Health, University of Granada, Granada, Spain
Correspondence: Virginia Martínez-Ruiz, Department of Preventive Medicine and Public Health, University of Granada, Granada, 18016, Spain, Tel +34 958242064, Email [email protected]
Purpose: The activities related to the prevention of crash injuries in older adults (PCIOA) performed by Family Physicians (FPs) have been scarcely studied. Our aim was to estimate the frequency of PCIOA activities performed by FPs in Spain and its association with attitudes and beliefs regarding this health problem.
Methods: We conducted a cross-sectional study in a nationwide sample of 1888 FPs working in Primary Health Care Services, recruited from October 2016 to October 2018. Participants completed a validated, self-administered questionnaire. Study variables included three scores related to current practices (General Practices, General Advice and Health Advice), several scores related to attitudes (General, Drawbacks and Legal), demographic and workplace characteristics. To obtain the adjusted coefficients and their 95% confidence intervals, we applied mixed effects multi-level linear regression models and the likelihood-ratio test to compare multi-level and one-level models.
Results: The frequency of PCIOA activities reported by FPs in Spain was low. The General Practices Score was 0.22/1, the General Advice Score was 1.82/4, the Health Advice Score was 2.61/4, and the General Attitudes Score was 3.08/4. The importance given to road crashes in the elderly obtained 7.16/10, the role that FPs should play in the PCIOA obtained 6.73/10, and the current perceived role obtained 3.95/10. The General Attitudes Score and the importance that FPs give themselves in the PCIOA were associated with the three Current Practices Scores.
Conclusion: The frequency of activities related to the PCIOA that FPs usually carry out in Spain is far below desirable standards. The average level of attitudes and beliefs about the PCIOA of the FPs working in Spain seems adequate. The variables of the most pronounced FPs associated with the prevention of traffic accidents in older drivers were age over 50 years, female sex and foreign nationality.
Keywords: family physicians, road injuries, prevention, primary health care
Plain Language Summary
- 1888 family physicians (FPs) working in Primary Health Care Services completed a validated, self-administered questionnaire.
- The frequency of activities aimed to the prevention of crash injuries in older adults reported by FPs in Spain was low.
- Developing strategies aimed at increasing the involvement of FPs in PCIOA activities is an urgent need.
Introduction
Older adults are increasingly exposed to the risk of road traffic.1,2 The underlying reasons can be summarized in the following points: aging has been associated with a progressive decline in the abilities to drive or use the road as pedestrians;3–5 the prevalence of several diseases that can affect driving ability (and the medications used to treat them) increases with age;6–8 the severity of road traffic injuries is higher among older people than among younger people, especially due to the greater frailty of the human body and the subsequent greater effect of the energy released in the accident on it, leading to higher mortality, morbidity, loss of quality of life, days of hospitalization, and many other health problems caused by road crashes;9,10 and, finally, people are living increasingly longer.11 Therefore, the absolute and relative numbers of older road users is rising.11 In addition, their mobility is also increasing.1,12,13
The above facts highlight the need to implement multi-sectorial strategies aimed at the prevention of crash injuries in older adults (PCIOA). In fact, this was the approach of the Spanish Road Safety Strategy 2011–2020.14 Undoubtedly, Primary Health Care (PHC) should be one of the main professional sectors involved in these preventive strategies,15–17 since its intrinsic characteristics (high accessibility, comprehensive and longitudinal care) place it in a privileged position to play a leading role in the PCIOA. The possible roles of Family Physicians (FPs) in this regard could be divided into two main activities: i) informing and advising older people and their relatives about the health risks related to driving or walking, the specific circumstances in which this risk is higher and how to manage them; and ii) detecting older drivers at high-risk and applying selective prevention strategies to them, ranging from specific counseling to issuing legal reports leading to the withdrawal of driving licenses.18–21 Several guidelines have been developed in some countries aimed to instruct FPs on efficient PCIOA activities.1,22–24
Unfortunately, this theoretical approach contrasts sharply with the activities related to the PCIOA that FPs are currently carrying out, which show enormous heterogeneity across different countries and even within countries.25–27 In Spain, medical check-ups —every 5 years— for the renewal of the driving license of drivers over 65 years are performed independently of PHC (ie, in specific Driver Check Centers).28 On the other hand, although the Spanish Society of Family and Community Medicine elaborated a general guideline of activities for the prevention of road traffic injuries,29 no specific Spanish guidelines regarding PCIOA activities in PHC are available to date. Therefore, in Spain there is no nationwide protocol on this topic and the role of FPs is yet to be defined. Although we hypothesize that the level of involvement of Spanish FPs in PCIOA activities is low and heterogeneous, no previous national studies addressing this issue have been performed. In addition, assuming that the application of activities related to the PCIOA is based mainly on the criteria of each FP, it seems particularly relevant to know their awareness, attitudes and beliefs about the importance of traffic accidents in the elderly as a public health problem, as well as their preventive role in this regard. It is logical to think that both the beliefs and attitudes of FPs regarding a specific health problem will influence their clinical practice.30 In fact, FPs carry out many preventive strategies aimed at the most prevalent diseases in the elderly, such as cardiovascular diseases, diabetes or chronic respiratory diseases.31 Any strategy aimed at disseminating the activities related to the PCIOA among FPs should be based on a deep knowledge of this topic, as well as on the barriers that FPs perceive to develop these activities, including lack of knowledge, low awareness, or lack of time due to the large volume of visits by patients with chronic conditions.32 Furthermore, carrying out activities related to the PCIOA can also be influenced by factors such as sex and age of the doctor, the number of elderly patients in their roster, the years of experience, or the urban or rural setting where they carry out their activity. Again, studies on these issues remain scarce in Spain.
In an attempt to fill this information gap, we designed the present study which aims to highlight both the perception and preventive activities of FPs regarding traffic accidents and mortality in older drivers, a vulnerable group of road users for the reasons mentioned above. To this end, the main objectives were: first, to estimate the frequency of PCIOA activities routinely performed by a national sample of FPs in Spain, as well as to describe their attitudes and beliefs regarding this health problem; and second, to assess the relationship between PCIOA activities and the attitudes, beliefs, and other demographic and work-related variables of FPs.
Methods
Study Design and Sample Selection
We conducted a cross-sectional study based on the completion of a self-administered questionnaire in Spain from October 2016 to October 2018. The study design is detailed in a previous work.33 The objective of this study was to design and validate a self-administered questionnaire that measures the knowledge, attitudes and current practices (CP) of FPs in Spain regarding the prevention of road injuries in older adults. As a result, our questionnaire showed acceptable validity to assess the knowledge, attitudes, and prevention strategies regarding traffic injuries in older drivers by Spanish FPs. The target population was all FPs in Spain, both from Basic Primary Care Teams and Emergency Departments. The only inclusion criterion was that the FPs agreed to complete the questionnaire after having been informed verbally and in writing about the purposes of the study. We applied two strategies to recruit the sample: i) contacting by e-mail the FPs affiliated to the three main scientific societies of FPs in Spain and requesting them to complete the online version of the questionnaire; and ii) distributing and collecting the printed version of the questionnaire among the FPs who attended the main PHC conferences held in Spain during the study period. A total of 1897 FPs completed the questionnaire. After excluding 9 questionnaires in which respondents did not fill in the information regarding the Autonomous Community of residence, the final sample comprised 1888 FPs.
Source of Information
The design (Supplementary File 1) and validation process of the questionnaire are also available elsewhere.33 It included questions aimed at measuring three constructs: Attitudes about PCIOA, Knowledge about road traffic injuries in the elderly (ie, people over 65 years old), and Current Practices regarding PCIOA. For the present study, we used the following information:
1) Questions included in the Current Practices construct: six items about the performance or not of preventive activities (scoring 1 point for each affirmative response) and a Likert-type subscale including 14 items exploring the frequency of advice given to elderly patients (1, never or almost never; 2, sometimes; 3, usually; 4, always). Factor analysis grouped these 20 items into three factors, and the corresponding mean scores were constructed for each one: General Practices Score (GPS), General Advice Score (GAS) and Health Advice Score (HAS). The value of the Kaiser-Meyer-Olkin test was 0.945 and the Bartlett’s sphericity test yielded a χ2 value of 16,848.877 (df = 190; p < 0.001). The Cronbach’s α score was 0.919. Table 1 details the items included in each score.
 |
Table 1 Descriptive Parameters of All Items and Scores Exploring PCIOA Activities in the Entire Sample and for Each Sex (All Estimates are Weighted Considering the True Distribution of Family Physicians Across Autonomous Communities and Sex; See Methods for Details) |
2) Questions addressing the Attitudes and Beliefs of FPs: A Likert-type subscale with 11 items exploring the level of agreement to statements related to possible PCIOA activities (1, disagreement; 2, indifferent; 3, partially agree; 4, strongly agree). Factor analysis distributed them into three factors, and we obtained the corresponding mean scores for each one: general statements regarding PCIOA (General Attitudes Score), possible drawbacks for implementing PCIOA activities (Drawback Score) and legal issues regarding PCIOA (Legal Score). Table 2 details the items included in each factor. Three other items (measured on a 0–10 scale) exploring the importance given by FPs to road crashes in the elderly, the theoretical role that they believe they should play regarding the PCIOA, and their opinion on the role that they currently play about PCIOA were considered separately and were identified as another factor in the factorial analysis. The value of the Kaiser-Meyer-Olkin test was 0.849 and the Bartlett’s sphericity test yielded a χ2 value of = 7213.885 (df = 91; p < 0.001). The Cronbach’s α score was 0.793.
 |
Table 2 Descriptive Parameters for All the Items and Scores Exploring Attitudes and Beliefs of Family Physicians Regarding PCIOA in the Whole Sample and for Each Sex (All Estimates are Weighted Considering the True Distribution of Family Physicians Across Autonomous Communities and Sex, See Methods for Details) |
3) Other demographic and occupational variables: age, sex, nationality, and FP status (specialist or trainee). In the case of specialists, years of work experience, the number of patients in the roster, the proportion of those patients over 65 years, and the type and location of the PHC center (the categories of these variables are shown in Supplementary Table 1).
Analysis
The Spanish ACs have their own competencies regarding health administration and show important cultural and social differences between them. As the distribution of respondents from each AC in our sample was not representative of the corresponding proportion of FPs in Spain, all information was weighted by the ratio between the observed proportion of each AC and sex groups of FPs in our sample and the true proportion of each AC and sex groups of FPs estimated in Spain (data from the Ministry of Health).34 We obtained weighted descriptive parameters for all variables in groups 1) and 2).
To estimate the adjusted association between the three Current Practices Scores and the variables in groups 2) and 3), mixed-effects multi-level linear regression models were initially applied, specifying random effects at the AC level, to obtain the adjusted coefficients and their 95% confidence interval for each category of the independent variables. We applied the likelihood-ratio test to compare multi-level and one-level models, and we applied the latter for GAS and HAS (including Autonomous Community as another independent variable) because no significant (< 0.1) p-values were found. We fitted the models for the entire sample of FPs and separately for the subset of specialists. Coefficients could be interpreted as the mean units of increase or decrease of each score for each category of the independent variable compared to the reference category, after adjusting for the rest of the variables in the model. We analyzed collinearity in all models by calculating variance inflation factors (VIFs) for each independent variable. In the models for the entire sample of FPs, all VIFs were lower than 5, thus ruling out collinearity. For the subset of specialists, all VIFs were lower than 10 except for some age categories (highly correlated with experience), but none of them were greater than 30.
All analyses were performed using Stata software, version 16.35
Results
Supplementary Table 1 shows the crude and weighted demographic and work-related characteristics of the sample. According to weighted estimates, 54.6% of the respondents were female. The mean and median ages were 40.4 (standard deviation —SD—, 12.7) and 38 years (interquartile range —IR—, 28 to 53), respectively. Forty-four percent were in the last year of their training program as FP. In the subgroup of specialists, the mean and median years of experience were 18.6 (SD, 10.4) and 19.5 years (IR, 10 to 27), respectively.
Table 1 shows the weighted descriptive parameters of the items measuring current practices focused on the PCIOA. The mean value of General Practices Score (GPS) was 0.22 (out of a maximum of 1). Regarding the items included in this score, the proportion of FPs who reported performing PCIOA activities ranged from 2.7% for using any guideline to 50.0% for writing reports requested by Driver Check Centers. Although 42.8% of FPs reported giving some PCIOA-related advice to their elderly patients, only 19.2% asked them whether they drove, and only 11.1% registered this information in medical records. The mean General Advice Score (GAS) in the whole sample was 1.82, which would correspond to a frequency of giving general advice “slightly less than sometimes”. Only three pieces of advice (use public transport, travel in company, and avoid driving at night) scored higher than 2. The piece of advice with the lowest frequency of being reported (1.57) was “when you visit any specialists, remember them that you drive”. The mean Health Advice Score (HAS) in the entire weighted sample was 2.61, an intermediate value between “sometimes” and “usually”. The most frequent piece of advice was related to not drinking alcohol (2.98), followed by not taking drugs without consultation (2.85).
Table 2 shows the weighted descriptive parameters of the items and scores measuring attitudes and beliefs. The General Attitudes Score was 3.08, which corresponds to “partially agree”, while Drawbacks Score and Legal Score were lower (2.68 and 2.36, respectively). Remarkably, we observed a low level of agreement (slightly higher than “indifferent”) regarding the statement “FPs should be responsible for the renewal of driving licenses in the elderly”. The importance given to road crashes in the elderly ranked 7.16 points over 10, a value slightly higher than that obtained for the role that FPs should play in PCIOA (6.73), and much higher than the role currently perceived (only 3.95 points).
Table 3 displays the results of the multivariate models fitted for the three Current Practices Scores in the whole sample of FPs. Increasing age from 50 years onward was directly related to GPS and the oldest age group also showed higher GAS values. Female sex and foreign FP showed significant higher values for HAS. The General Attitudes Score and the current importance that FPs place on themselves in PCIOA showed a positive association with all three Current Practices Scores. The importance given to road injuries in the elderly as a health problem was directly related to GAS and HAS, while the Legal Score showed an inverse association with HAS. In the model fitted for the subset of specialists (Supplementary Table 2), the pattern of associations was almost the same as that described for the entire sample of FPs, except for the lack of association between scores and age (highly correlated with experience), which was in fact replaced by the highest level of experience in the model for GPS.
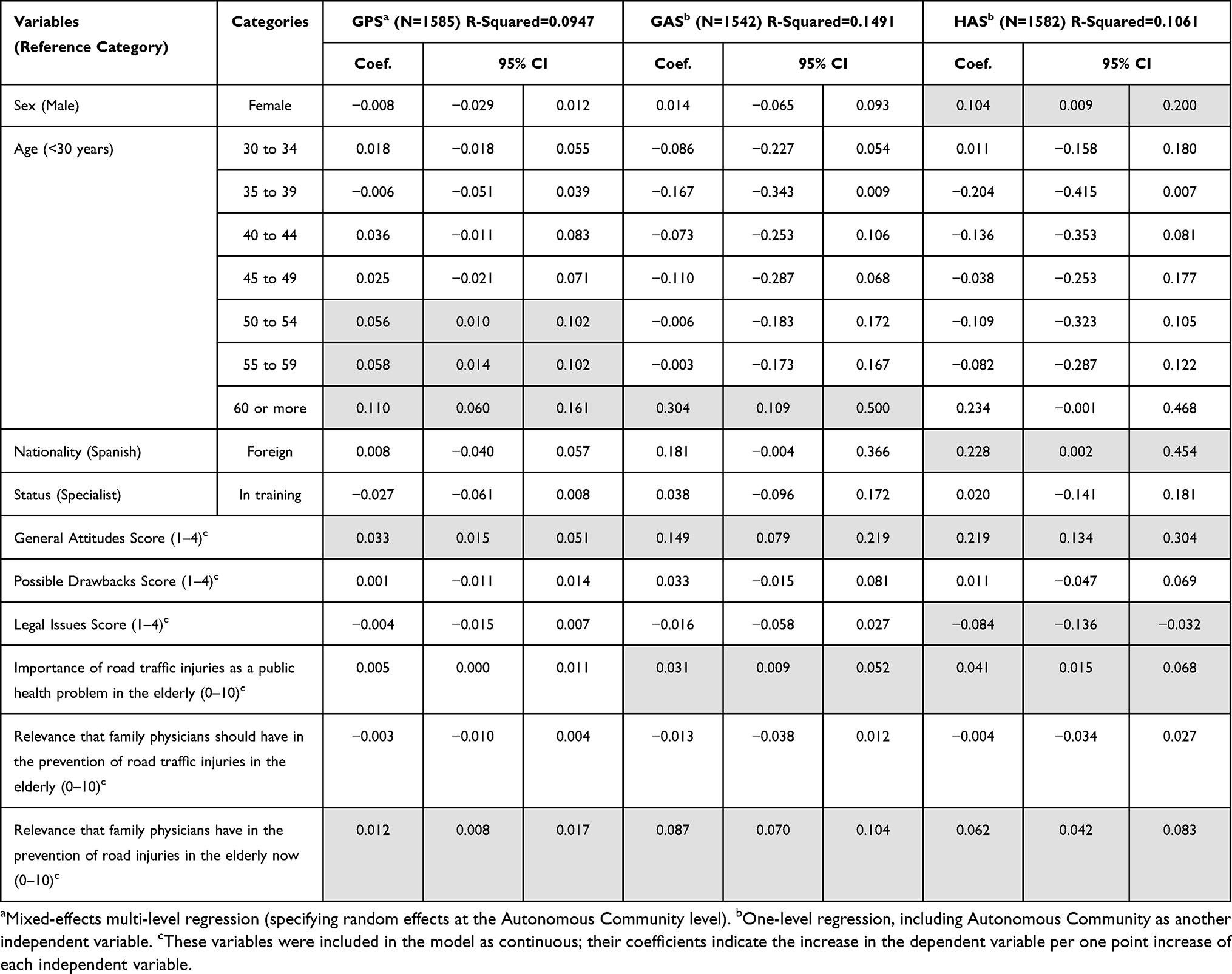 |
Table 3 Multivariate Regression Models for the Three PCIOA Activity Scores in the Whole Sample of Family Physicians with Complete Values for All the Variables. Shaded Areas Indicate Coefficients Whose 95% Confidence Interval Excluded 0 |
Discussion
Our results have revealed, as expected, that the frequency of PCIOA-activities reported by FPs in Spain is low. The most frequently reported activity (ie, preparing reports about the capabilities of older people for driving) was performed at the request of Spanish Driver Check Centers. Apart from that, the frequency of any preventive advice was lower than “usually” and, for most of the advice related to general recommendations, it did not even reach the level of “sometimes”. The most frequent advice was related to health problems of the elderly (eg, alcohol consumption, drug use, or visual or hearing problems). Another study conducted in Switzerland also showed a less than optimal adherence of FPs to recommendations regarding some PCIOA activities.36
The extremely low frequency of reporting the use of specific guidelines is striking. This result, together with the high level of agreement with the statement “FPs would benefit from having guidelines about PCIOA”, suggests that most FPs are not aware of the existence of or do not have easy access to currently available guidelines. These findings are in line with those reported in previous studies in other countries. For instance, Sebo37 found that only a minority of Swiss physicians (17%) regularly used a reference guide, although most of them consider that it would be very useful. A similar finding was observed in an earlier study by Jang et al38 among Canadian FPs: almost a quarter of them were not aware of the Canadian guide.
In contrast to the low frequency of PCIOA activities reported by FPs, their average general awareness of road traffic injuries in the elderly and their preventive role seems satisfactory. Family physicians generally agree with most of the proposed routine activities, with the exception of taking responsibility for the renewal of driver licenses. This finding is also consistent with that reported by Jang et al:38 45% of the physicians in their study did not consider themselves the most qualified professionals to assess driving fitness.
There is a large difference between the mean value of the theoretical importance given by FPs to their own role on PCIOA and the actual importance (6.73 vs 3.95). In other words, FPs are aware that they are currently doing much less than they should do regarding PCIOA. Previous studies have also shown this discrepancy between awareness and current practices. For example, Meuser et al stated that 72% of healthcare professionals recognize that driving during senescence is a clinical concern, but only 33% discuss this issue during patient anamnesis in the consultation.39 When FPs were asked (also in the present questionnaire, data not shown) about the main resources needed to implement PCIOA activities, more than half of them indicated the need for more time per patient as a high priority, a necessity permanently demanded by FPs in Spain.40
As expected, our results indicate that the personal awareness of FPs regarding PCIOA seems to be the main determinant of their current practices: higher values in the General Attitudes Score and in the current relevance regarding PCIOA were strongly related to high PCIOA activities scores. Also noteworthy is the inverse association between the Legal Score and HAS: those FPs more favorable to being vested with legal attributes to perform PCIOA activities are those who reported giving less health advice to their older patients. This association suggests that the level of performance of these PCIOA activities could depend on the legal empowerment to do it.
Once the attitudes and beliefs of FPs were considered in the analysis, the remaining demographic and workplace variables play a much less important role in the frequency of PCIOA activities. Multivariate analyses showed significantly higher values of HAS in female FPs. This finding is consistent with previous studies suggesting that female doctors hold longer consultations, provide more information, and include more socio-emotional aspects in the interview.41–44 This fact could be explained by the relationship between female gender and involvement in informal care due to gender roles in a culture that still assumes that it is the woman who must take the main role of care for older adults (although not consciously done).44 On the other hand, the association between older FPs and a higher frequency of involvement in PCIOA-related activities seems logical: it is easier for older FPs to put themselves in the role of older drivers, better understand their specific problems regarding driving or walking and, consequently, to pay more attention to prevent them.
Our study has some limitations. Regarding the representativeness of our sample, the volunteer bias must be considered: FPs who answered the questionnaire may have been more motivated or interested about this particular issue than the whole population of FPs. This fact, along with the absence of blinding about the purpose of the survey could have led respondents to overestimate their positive attitudes and beliefs regarding PCIOA, as well as their performance of PCIOA-related activities. These facts further support the main finding of our study, namely the low frequency of PCIOA activities among FPs in Spain. On the other hand, if the aforementioned sources of bias were non-differential (ie, not associated with other physician-related variables), the magnitude of the coefficients obtained from multivariate models would probably be underestimated (ie biased toward the null value). Otherwise, our results are strengthened by the large sample size of FPs from all the Spanish Autonomous Communities, as well as by the use of a validated questionnaire.
In view of the results obtained, it seems necessary to develop strategies aimed at increasing the involvement of FPs in PCIOA-related activities, with the aim of incorporating them into their routine clinical practices. Experiences on this objective in other countries are encouraging.19,45 For instance, Dow and Jacques stated that, after giving theoretical training to physicians, the quantity and quality of clinical reports of patients with pathologies that can affect driving increased.26 Undoubtedly, it is necessary to increase the knowledge and visibility of the existing guides focused on PCIOA activities. In addition, the development of a Spanish Guide for PCIOA in PHC, which contemplates the specific characteristics of our National PHC System seems highly recommendable. This guide could emphasize the routine use of standard check questions for older patients, such as the self-administered pre-consultation patient questionnaire on the health of older drivers developed in Switzerland.37
Conclusion
The frequency of activities related to the PCIOA that FPs usually carry out in Spain is far below desirable standards, especially those related to the General Practices Score. On the other hand, the average level of attitudes and beliefs about the PCIOA of FPs working in Spain seems adequate. The main variables related to FPs that were associated with the prevention of traffic accidents in older drivers were age over 50 years, female sex and foreign nationality.
Data Sharing Statement
The datasets used for this study are available upon reasonable request to the corresponding author. All the methods, materials and original questionnaire used for this work are included in this manuscript and its Supplementary Files. This study was not pre-registered.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of Granada Province (Reference Code: 1451-N-17.I.P.). All participants received information regarding the study goals and signed informed consent prior to inclusion. To ensure the confidentiality of the data, participants were anonymized through a code accessible only to the researchers. Informed consent and personal data were kept separately.
Acknowledgments
The authors wish to acknowledge the Chair SEMERGEN-UGR of Teaching and Research in Family Medicine (University of Granada) for their support and A.J. Láinez Ramos-Bossini for improving the use of English in the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. NHTSA.National Highway Traffic Safety Administration. Clinician’s Guide to Assessing and Counseling Older Drivers. NHTSA; 2015. Available from: https://www.nhtsa.gov/sites/nhtsa.dot.gov/files/documents/812228-cliniciansguidetoolderdrivers.pdf.
2. International Transport Forum. Road Safety Annual Report 2020. OECD/ITF; 2020.
3. Anstey KJ, Wood J, Lord S, Walker JG. Cognitive, sensory and physical factors enabling driving safety in older adults. Clin Psychol Rev. 2005;25(1):45–65. doi:10.1016/j.cpr.2004.07.008
4. Liu J, Fujii Y, Fujii K, et al. Pre-frailty associated with traffic crashes in Japanese community-dwelling older drivers. Traffic Inj Prev. 2022;23(2):73–78. doi:10.1080/15389588.2022.2030473
5. Moon S, Ranchet M, Akinwuntan AE, et al. The impact of advanced age on driving safety in adults with medical conditions. Gerontology. 2018;64(3):291–299. doi:10.1159/000486511
6. Monárrez-Espino J, Laflamme L, Rausch C, Elling B, Möller J. New opioid analgesic use and the risk of injurious single-vehicle crashes in drivers aged 50–80 years: a population-based matched case-control study. Age Ageing. 2016;45(5):628–634. doi:10.1093/ageing/afw115
7. Rizzo M. Impaired driving from medical conditions: a 70-year-old man trying to decide if he should continue driving. JAMA. 2011;305(10):1018–1026. doi:10.1001/jama.2011.252
8. Zitoun S, Baudouin E, Corruble E, Vidal JS, Becquemont L, Duron E. Use of potentially driver-impairing drugs among older drivers. BMC Geriatr. 2022;22(1):4. doi:10.1186/s12877-021-02726-5
9. Ayuso M, Sánchez R, Santolino M. Does longevity impact the severity of traffic crashes? A comparative study of young-older and old-older drivers. J Safety Res. 2020;73:37–46. doi:10.1016/j.jsr.2020.02.002
10. Li G, Braver ER, Chen LH. Fragility versus excessive crash involvement as determinants of high death rates per vehicle-mile of travel among older drivers. Accid Anal Prev. 2003;35(2):227–235. doi:10.1016/s0001-4575(01
11. Eurostat. Estructura Demográfica y Envejecimiento de La Población. Eurostat; 2020.
12. Haustein S, Siren A. Older people’s mobility: segments, factors, trends. Transp Rev. 2015;35(4):466–487. doi:10.1080/01441647.2015.1017867
13. Lidbe A, Adanu EK, Penmetsa P, Jones S. Changes in the travel patterns of older Americans with medical conditions: a comparison of 2001 and 2017 NHTS data. Transp Res Interdiscip Perspect. 2021;11:100463. doi:10.1016/j.trip.2021.100463
14. Dirección General de Tráfico. Estrategia de Seguridad Vial 2011–2020. [Safety Road Strategy 2011–2020]. Dirección General de Tráfico; 2010. Spanish.
15. Betz ME, Jones J, Genco E, et al. Perspectives on tiered older driver assessment in primary care settings. Gerontologist. 2016;56(2):272–281. doi:10.1093/geront/gnu038
16. Martín Cantera C. La prevención de las lesiones de tráfico por los médicos de familia: algunas reflexiones sobre la situación actual. Aten Primaria. 2005;36(3):123–125. Spanish. doi:10.1157/13077476
17. Rivera-Izquierdo M, Valverde-Cano LM, Martínez-Ruiz V, et al. Prevention of road crashes in older adults: perspectives on facilitators, barriers and the role of the family doctor. BMC Geriatr. 2021;21(1):635. doi:10.1186/s12877-021-02569-0
18. Amick MM. Managing older adult driving safety in the primary care setting. Med Health R I. 2012;95(7):220–221.
19. Jiménez Mejías E, Martín de Los Reyes LM, Martínez RV. Eficacia de las intervenciones formativas sobre médicos de atención primaria en la prevención de accidentes de tráfico en ancianos. Med Fam SEMERGEN. 2019;45(7):489–496. Spanish. doi:10.1016/j.semerg.2019.01.005
20. Ma T, Chee JN, Hanna J, et al. Impact of medical fitness to drive policies in preventing property damage, injury, and death from motor vehicle collisions in Ontario, Canada. J Safety Res. 2020;75:251–261. doi:10.1016/j.jsr.2020.09.003
21. Wallis KA, Matthews J, Spurling GK. Assessing fitness to drive in older people: the need for an evidence‐based toolkit in general practice. Med J Aust. 2020;212(9):396. doi:10.5694/mja2.50588
22. Driver & Vehicle Licensing Agency. Assessing fitness to drive– a guide for medical professionals. Department for Transport; 2021. Available from: https://www.gov.uk/government/collections/assessing-fitness-to-drive-guide-for-medical-professionals.
23. Hill LJN, Pignolo RJ, Tung EE. Assessing and counseling the older driver: a concise review for the generalist clinician. Mayo Clin Proc. 2019;94(8):1582–1588. doi:10.1016/j.mayocp.2019.03.023
24. Waka Kotahi NZ Transport Agency. Medical Aspects of Fitness to Drive. A Guide for Health Practitioners. New Zealand: Transport Agency; 2014.
25. Adler G, Rottunda SJ. The driver with dementia: a survey of physician attitudes, knowledge, and practice. Am J Alzheimers Dis Other Demen. 2011;26(1):58–64. doi:10.1177/1533317510390350
26. Dow J, Jacques A. Educating doctors on evaluation of fitness to drive: impact of a case-based workshop. J Contin Educ Health Prof. 2012;32(1):68–73. doi:10.1002/chp.21124
27. Martín Cantera C. La Factibilidad Del Consejo Preventivo Sobre Accidentes de Tráfico En Atención Primaria. [The Feasibility Of Traffic Accident Preventive Advice In Primary Care]. Universidad Autónoma de Barcelona; 2005. Available from: https://www.mutuamotera.org/gn/web/documentos/contenidos/2005_consejo_preventivo_accidentes_trafico_atencion_primaria.pdf.
28. Ministerio de la Presidencia y para las Administraciones Territoriales. Orden PRA/375/2018, de 11 de Abril, Por La Que Se Modifica El Anexo IV Del Reglamento General de Conductores, Aprobado Por Real Decreto 818/2009, de 8 de Mayo; 2018. Available from: www.boe.es.
29. Córdoba García R; Grupo de educación sanitaria y promoción de la salud del PAPPS. Cómo Ayudar a Prevenir Las Lesiones Por Accidentes de Tráfico. [How to Help Preventing Road Crashes]. Ministerio de Sanidad y Consumo; 2015. Spanish.
30. Chan B, Austin P. Patient, physician, and community factors affecting referrals to specialists in Ontario, Canada. Med Care. 2003;41:500–511. doi:10.1097/01.MLR.0000053971.89707.97
31. Aguilar-Palacio I, Carrera-Lasfuentes P, Solsona S, Sartolo MT, Rabanaque MJ. Utilización de servicios sanitarios en ancianos (España 2006–2012): influencia del nivel de salud y de la clase social. [Use of health services in the elderly (Spain 2006–2012): influence of health level and social class]. Aten Primaria. 2016;48(4):235–243. Spanish. doi:10.1016/j.aprim.2015.01.016
32. Jang RW, Man-Son-Hin M, Molnar FJ, Hogan DB, Marshall SC, Auger J. Family physicians’ attitudes and practices regarding assessments of medical fitness to drive in older persons. J Gen Intern Med. 2007;22(4):531–543. doi:10.1007/s11606-006-0043-x
33. Jiménez-Mejías E, Rivera-Izquierdo M, Miguel Martín-delosReyes L, et al. Development and validation of a questionnaire measuring knowledge, attitudes, and current practices of primary healthcare physicians regarding road injury prevention in older adults. Fam Pract. 2022;39(3):537–546. doi:10.1093/fampra/cmab148
34. Ministerio de Sanidad, Seguridad Social e Igualdad. Consulta Interactiva del SNS. [Interactive consultation of the SNS. Statistical Portal; 2019]. Portal Estadístico; 2019. Available from: https://pestadistico.inteligenciadegestion.mscbs.es/publicoSNS/S.
35. StataCorp. Stata Statistical Software: Release 16. StataCorp; 2019.
36. Sebo P, Haller DM, Favrat B, Huber P, Mueller Y, Vaucher P. Adherence to guidelines when evaluating fitness-to-drive in the elderly: a practice review of Swiss physicians. Swiss Med Wkly. 2018;148:w14632. doi:10.4414/smw.2018.14632
37. Sebo P. Physicians’ views on the usefulness of practical tools for assessing the driving ability of older drivers: a cross-sectional study. Fam Med Community Health. 2020;8(3):e000332. doi:10.1136/fmch-2020-000332
38. Jang RW, Man-Son-Hing M, Molnar FJ, et al. Family physicians’ attitudes and practices regarding assessments of medical fitness to drive in older persons. J Gen Intern Med. 2007;22(4):531–543. doi:10.1007/s11606-006-0043-x
39. Meuser TM, Carr DB, Berg-Weger M, Niewoehner P, Morris JC. Driving and dementia in older adults: implementation and evaluation of a continuing education project. Gerontologist. 2006;46(5):680–687. doi:10.1093/geront/46.5.680
40. De Pablo González R. La necesidad de recuperar la calidad asistencial y la dignidad del profesional en la Atención Primaria de salud. [The need to recover the quality of care and the dignity of the professional in Primary Health Care]. Semergen. 2003;29(1):14–16. Spanish. doi:10.1016/S1138-3593(03)74149-5
41. Delgado A, López-Fernández LA. Práctica profesional y género en atención primaria. [Professional practice and gender in primary care]. Gac Sanit. 2004;18(4):112–117. Spanish. doi:10.1157/13062259
42. Frank E, Segura C, Shen H, Oberg E. Predictors of Canadian physicians’ prevention counseling practices. Can J Public Health Rev Can Sante Publique. 2010;101(5):390–395. doi:10.1007/BF03404859
43. Roter DL, Hall JA, Aoki Y. Physician gender effects in medical communication: a meta-analytic review. JAMA. 2002;288(6):756–764. doi:10.1001/jama.288.6.756
44. Delgado A, López-Fernández L, Luna JD. Being a male or female doctor is different in medical practice. Aten Primaria. 2001;28:219–234. doi:10.1016/s0212-6567(01
45. Byszewski AM, Graham ID, Amos S, et al. A continuing medical education initiative for Canadian primary care physicians: the driving and dementia toolkit: a pre- and postevaluation of knowledge, confidence gained, and satisfaction. J Am Geriatr Soc. 2003;51(10):1484–1489. doi:10.1046/j.1532-5415.2003.51483
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.