")
Back to Journals » Risk Management and Healthcare Policy » Volume 15
Attitudes, Barriers, Motivations to Sun Protection in Reunion Island’s Schools: Qualitative Study
Authors Leruste S, Marx M, Ah-Mouck C, Yap-Chim L, Sultan-Bichat N, Beylot-Barry M , Spodenkiewicz M, Dumez J , Bertolotti A
Received 14 October 2021
Accepted for publication 11 January 2022
Published 4 May 2022 Volume 2022:15 Pages 895—900
DOI https://doi.org/10.2147/RMHP.S341565
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mecit Can Emre Simsekler
Sebastien Leruste,1 Mathilde Marx,1 Cassie Ah-Mouck,1 Lindsay Yap-Chim,1 Nathalie Sultan-Bichat,2,3 Marie Beylot-Barry,4 Michel Spodenkiewicz,5,6,* Jessica Dumez,1,6,* Antoine Bertolotti3,6,7
1University Department of General Medicine, Saint-Pierre, La Réunion, France; 2Dermatology department, CH Ouest Réunion, St Paul, La Réunion, France; 3MISOLRE, Prevention Association, Saint-Paul, La Réunion, France; 4Dermatology Department, Saint-André Hospital, Bordeaux University Hospital, INSERM U 1053, Bordeaux, Gironde, France; 5Mental Health Department, Reunion University Hospital Sites South, Saint-Pierre, La Réunion, France; 6Inserm CIC1410, Reunion University Hospital, Saint Pierre, La Réunion, France; 7Infectious Diseases-Dermatology Department, Reunion University Hospital, Saint Pierre, La Réunion, France
*These authors contributed equally to this work
Correspondence: Antoine Bertolotti, Inserm CIC1410, Infectious diseases-dermatology department, Reunion University Hospital, 97 av. Président Mitterrand, Saint Pierre, La Réunion, 97448, France, Tel +02 62 35 91 65, Fax +02 62 35 96 51, Email [email protected]
Abstract: The incidence of melanoma in Reunion Island is on the rise and is now one of the highest worldwide. Although the main risk factor of melanoma is sun exposure during childhood, sun protection measures remain insufficient in Reunionese schools. From November 2019 to November 2020, we conducted a qualitative study to explore the attitudes, barriers, and motivations to sun protection among the main actors of children’s protection in Reunion Island. Individual semi-directive interviews were performed with 14 children aged 6 to 10 years, 13 parents, and 13 teachers. The interviews were recorded and transcribed. Relevant data were coded, triangulated, analyzed, and then modeled following the methodology of grounded theory. Sufficiency of the data was sought. All 40 participants described their sun protection habits. Protection was lower during school activities than during leisure activities. Parents identified several practical and financial barriers to sun protection. Teachers pointed out the lack of adequate infrastructure and sun protection training. Responsibility for children’s protection was a point of disagreement between parents and teachers. Children limited their use of protection, mainly for reasons of comfort. Children’s sun protection in schools is the responsibility of educational staff, parents, and society at large. Improving communication between these various actors is necessary. Sun safety campaigns and reorganization of the school environment would allow for better protection of the child population.
Keywords: melanoma, school, environment, preventive medicine and public health, children’s health, sun protection factor
Background
The incidence of melanoma in Reunion Island is on the rise and sun protection measures remain insufficient in Reunionese schools. This study explores the attitudes, barriers, and motivations to sun protection among the main actors of children’s protection, namely parents, teachers, and the children themselves. The attitude towards sun protection was found to depend on the education of the children, the financial means of parents and schools, as well as the constraints of application. Sun safety campaigns and reorganization of the school environment would allow for better protection of the child population.
Introduction
Sun exposure during childhood can cause the development of skin cancer in later years, in particular melanoma, which is the most lethal.1 The worldwide incidence of melanoma is on the rise, with nearly 290,000 new cases diagnosed in 2018.2 The country with the highest age-standardized incidence rate is Australia, where 40.4 cases per 100,000 men and 27.5 cases per 100,000 women were reported in 2018.3 Since 2008, however, this incidence has decreased by 11% in the 14–49 age group following the implementation of effective sun safety campaigns.4 In the French overseas department of Reunion Island, which is characterized by a great diversity of skin phototypes due to multiple migratory flows, the ultraviolet (UV) index is very high – equivalent to that in Australia. The age-standardized incidence rate of melanoma Reunion Island increased fourfold between 1995 and 2015.5 In 2015, it was estimated at nearly 30.0 new cases per 100,000 inhabitants in people with skin phototypes I–III, compared to 13.5 in metropolitan France.5
Over the course of a lifetime, 80% of exposure to UV radiation and 50% of skin damage occur before the age of 21, mainly in the school environment.6 In spite of this, knowledge of the risks associated with sun exposure remains insufficient among children and adolescents.7,8 Similar quantitative data have been reported for Reunion Island by the local association MiSolRé (Mission Soleil Réunion), which has been running sun safety campaigns in elementary schools since 2017.9,10 The aim of this qualitative study was to explore the attitudes, barriers, and motivations to sun protection in Reunion Island with a view to proposing sun protection measures adapted to three populations: teachers, children, and parents.
Method
This qualitative observational descriptive study was conducted in Reunion Island by the association MiSolRé from November 2019 to November 2020. Participants were recruited via telephone by the school principals to whom the study was presented. The following participants were included by convenience sampling: kindergarten, elementary school, or junior high school teachers; adult parents of elementary school children; and elementary school children aged 6 to 10 years. Oral and written informed consent including publication of anonymized responses was obtained from all participants (in the case of children, consent was obtained from their parents and/or legal guardians). Teachers, parents, and children were included until data sufficiency was reached in verbatim analysis. The parents interviewed were not the parents of the children interviewed. Children were interviewed without their parents present. Exclusion criteria were refusal to participate and being a protected adult. The socio-demographic and medical characteristics (sex, age, skin phototype, dermatological history) of participants were collected before the start of the interviews. These characteristics constituted the diversity criteria of our study population.
Three women medical doctors (MM, CAM, and LYC) with two years of experience in qualitative research conducted individual semi-directive interviews face-to-face or by telephone. After a short self-presentation, they asked respondents an icebreaker question and then probed with follow-up questions in an evolving interview process (Supplementary Figure 1). The interviews were audio-recorded digitally and then transcribed verbatim. Some synthesis notes were taken during the interview. Anonymity was guaranteed for all participants.
Data were analyzed following the methodology of grounded theory. Open and axial coding were used to identify emerging themes and to develop a definitive codebook. Two data coders coded the data for each population studied. The resulting codes were compared, and discrepancies were resolved by consensus. Interview data were triangulated (MM, CAM, LYC, SL, AB). Data were modeled for each of the three populations, and an overall model was generated for the entire study population.
The qualitative analysis method was implemented following the Consolidated Criteria for Reporting Qualitative research (COREQ).11
This study was conducted in accordance with the Declaration of Helsinki. It was registered with the Commission nationale de l’informatique et des libertés (# 2215476) and approved by the institutional review board of Reunion University.
Results
A total of 8 elementary school teachers, 3 junior high school teachers, 2 kindergarten teachers, 13 parents of elementary school children, and 14 children aged 6 to 10 years were interviewed from November 2019 to November 2020. The mean interview length was 18.6 minutes for teachers, 12.3 minutes for parents, and 23 minutes for children. The mean age of interviewed children was 7.8 years, with the youngest being 6 years old and the oldest 10 years old. Skin phototype III was the most common (46%) among teachers, and skin phototype IV was found in 36% of children. A personal or family history of skin cancer was found in 31% of teachers, but none was found in parents or children (to the best of their knowledge). Sixty-two percent of parents were managers or liberal professionals (Table 1). An overall model of the data from interviews with the three populations is shown in Figure 1. Participant quotes by theme are reported in Supplementary Table 1. Specific models for each population are presented in Supplementary Figures 2–4.
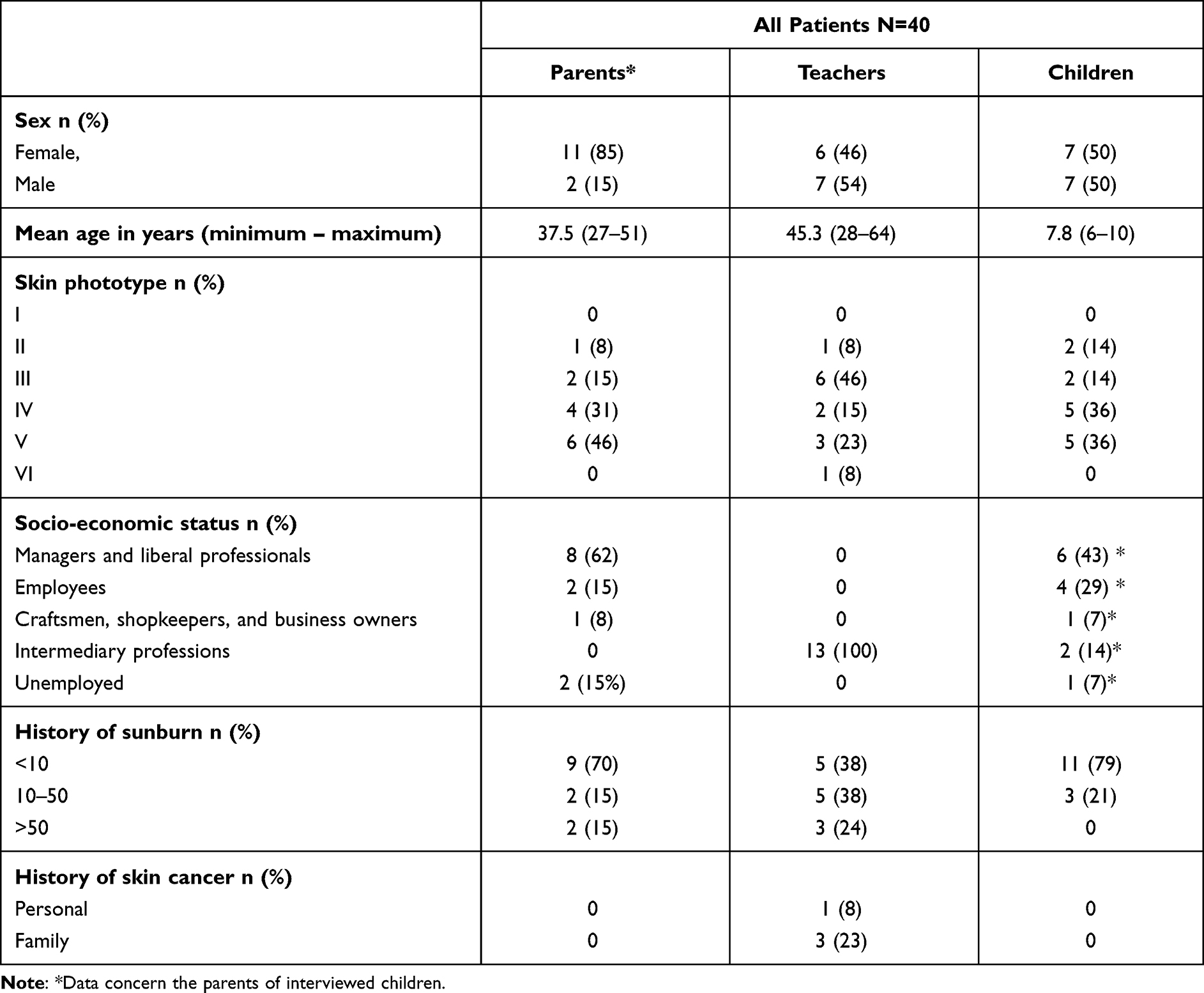 |
Table 1 Demographic and Medical Characteristics of Participants |
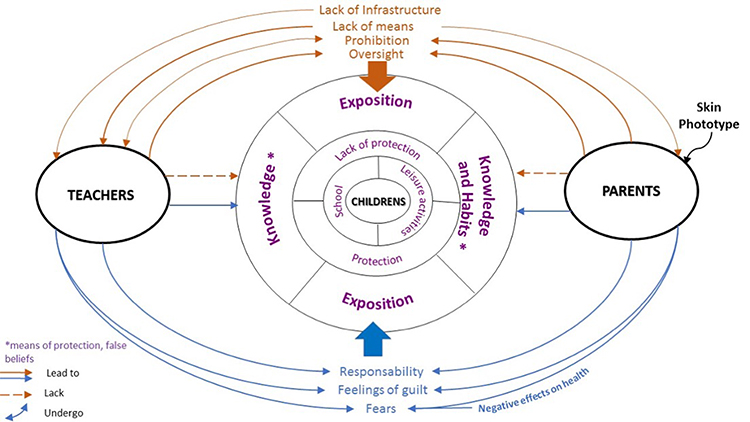 |
Figure 1 Overall model of data from interviews with parents, teachers, and children, Reunion Island. |
The interviews revealed a wide range of (often extreme) sun exposure situations in Reunion Island. Sun exposure occurred during leisure activities or at school (in the case of teachers and children). The intensity of exposure at school was more or less strong, depending on the location and altitude of the school and on seasonality. A high rate of sunburn was observed in children for all skin phototypes combined. A further study may be needed to establish a possible correlation between rate of sunburn and skin phototype.
Different protection measures were used, but each population tended to use the same ones. Protection was either active (sunscreen application, protective clothing, head coverings, sunglasses, etc.) or passive (avoidance behaviors such as seeking shade or avoiding the outdoors during peak UV hours). Children and teachers used sun protection measures less conscientiously at school than during leisure activities (backyard play, beach, hiking, travel, etc.). Parents adapted protection measures to their child’s skin phototype. Children with skin phototypes I–III received the best protection.
Teachers pointed out the lack of available material and human resources, insisting on the inadequacy of infrastructure and the absence of sun protection training. Both parents and teachers highlighted the cost of protection measures and the practical (breakage, loss, theft, etc.), organizational (lack of time, etc.), environmental, and aesthetic barriers to the application of sunscreen to children. Teachers also raised the issue of legal barriers.
Knowledge and attitudes regarding sun protection among the three populations were the result of sun safety campaigns, recommendations by health actors, school education, and, most importantly, parental education. Children highlighted the lack of sun protection in school.
Responsibility for children’s sun protection in school was discussed by parents and teachers. Parents considered that children were the responsibility of the school’s teaching staff. Conversely, teachers felt that parents were responsible for ensuring their children’s sun protection (through putting a cap and sunscreen in their children’s school bag or applying sunscreen to their children before bringing them to school). They also said that practical barriers prevented them from providing sun protection to each of their students individually. Parents and teachers communicated in writing via the children’s notebooks or briefly in person before or after school hours. They agreed that responsibility for children’s sun protection ultimately fell on social and political institutions, and they expected concrete measures from town halls, regional bodies, the Board of Education, or the Regional Health Agency. Both parents and teachers expressed feelings of guilt due to oversights, a sense of responsibility, and fears of the negative effects of overexposure. These feelings were perceived as a driver for better implementation of sun protection measures.
Discussion
Summary
Children’s sun protection is the result of close interactions among parents, children, and educational staff. Parental involvement is paramount.12 In Reunion Island, parents were unquestionably involved in their children’s sun protection during leisure activities. However, unlike the situation in Australia, their involvement in the school setting was inconsistent, as has been reported elsewhere.9,10 All parents displayed this ambivalence, but for some, the idea that they should be involved in their children’s sun protection in school appeared as a revelation. The lack of two-way communication between teachers and parents was blamed for this misunderstanding, especially by members of the lower socio-economic classes.13,14 Teachers expressed fears that they might be accused of abuse if they applied sunscreen to children or helped them get dressed. However, these fears seem disproportionate: they are not justified by the current legislation and could be reduced through better communication between parents and teachers.
Sunscreen use was limited by fears of environmental repercussions. Indeed, it has been suggested that sunscreen contains nanoparticles which can alter the development of living organisms, particularly aquatic organisms.15,16 However, additional studies are needed on the topic as toxicity varies depending on the species and the type of nanoparticles.17
Lastly, a high rate of sunburn was observed in children for all skin phototypes combined. This finding can be explained by the intensity of UV rays in Reunion Island, which is located at the Tropic of Capricorn and is characterized by a mountainous landscape (with a highest point of 3000 m above sea level). Indeed, at noon in high summer, UV rays can reach up to 18 at the main viewing point for the volcano Piton de la Fournaise. We regularly see sunburns in patients with skin phototypes IV and V who have just returned from a weekend trip in the mountains (personal data).
Strengths and Limitations
The individual semi-directive interview format proved to be an appropriate methodological choice given the topic at hand. Interviews were conducted by three researchers (MM, CAM, LYC), one for each population, which made it possible to cover a wide range of schools and to generate a diverse set of data. By combining their findings, the researchers were able to provide a global view of sun protection in Reunionese schools.
However, the study has some limitations. A selection bias linked to participants’ personal motivations resulted from the fact that recruitment was on a voluntary basis. Because of the COVID crisis, participants were partly (40%) recruited from the researchers’ circle of acquaintances, which may have influenced some of the interviews. Nevertheless, theoretical sampling and recourse to different recruitment methods made it possible to reach data sufficiency. Moreover, data triangulation helped to control for subjectivity.
Lastly, the majority of parents interviewed were of high socioeconomic status, which may have biased their assessment of the impact of sun product costs on children’s sun protection.
Comparison with Existing Literature
Participants spontaneously mentioned dermatologists, pharmacists, and school nurses as health professionals in charge of promoting sun safety. General practitioners were mentioned by only one participant, suggesting that sun protection education is lacking in general practice.18 More generally, studies have shown that medical students receive insufficient training on sun protection.19
Unlike the situation in Australia, children’s sun protection was found to be very inconsistent in Reunionese schools.9 The lack of communication between parents and teachers was especially strong in the case of children from the lower socio-economic classes, as has been observed elsewhere.13,14
Studies have stressed the importance of implementing sun protection measures in nurseries to help parents and nursery assistants acquire better sun protection habits and to alter children’s behavior at an earlier stage.20 In accordance with this, a sun safety education program was developed in recent years in France.20 However, it was insufficiently implemented despite a randomized trial showing significant results.21
Implication for Research and/or Practice
Children’s sun protection in schools is the responsibility of educational staff, parents, and society at large. Improved communication between these actors is necessary. Sun safety campaigns inspired by the Australian case and reorganization of the school environment are essential to improve protection in children. A general population study is needed to further influence public health policy.
Ethical Approval
This study was registered with the Commission nationale de l’informatique et des libertés (# 2215476) and approved by the institutional review board of Reunion University.
Acknowledgments
We would like to thank our copy editor Arianne Dorval.
The authors thank the study participants for their valuable input.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ward WH, Farma JM. Cutaneous melanoma: etiology and therapy. Brisbane (AU): Codon Publications; 2017. Availabl from: http://www.ncbi.nlm.nih.gov/books/NBK481860/.
2. Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
3. Cancer today; 2019. Available from: http://gco.iarc.fr/today/home.
4. Smith BJ, Ferguson C, McKenzie J, et al. Impacts from repeated mass media campaigns to promote sun protection in Australia. Health Promot Int. 2002;17(1):51–60. doi:10.1093/heapro/17.1.51
5. Chirpaz E, Warocquier J, Filisetti C, et al. Epidemiology of cutaneous malignant melanoma in Reunion Island. Revue des maladies respiratoires. 2021. doi:10.1016/j.rmr.2021.06.007
6. Green AC, Wallingford SC, McBride P. Childhood exposure to ultraviolet radiation and harmful skin effects: epidemiological evidence. Prog Biophys Mol Biol. 2011;107(3):349–355. doi:10.1016/j.pbiomolbio.2011.08.010
7. Andreola GM, Carvalho VO, de Huczok J, et al. Photoprotection in adolescents: what they know and how they behave. An Bras Dermatol. 2018;93(1):39–44. doi:10.1590/abd1806-4841.20185489
8. Reinau D, Meier C, Gerber N, et al. Sun protective behaviour of primary and secondary school students in North-Western Switzerland. Swiss Med Wkly. 2012;142:w13520. doi:10.4414/smw.2012.13520
9. Breton N, Bruneau L, Miquel J, et al. Children’s and Parent’s knowledges and behaviours in Reunion island on solar prevention. Ann Dermatol Venereol. 2019;146(12):A236–A237. doi:10.1016/j.annder.2019.09.368
10. Monie A, Sultan-Bichat N. Evaluation of a school-based sun safety education program in Reunion Island, 2016 – 2017. Ann Dermatol Venereol. 2019;146(12):A233–234. doi:10.1016/j.annder.2019.09.362
11. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
12. Littlewood Z, Greenfield S. Parents’ knowledge, attitudes and beliefs regarding sun protection in children: a qualitative study. BMC Public Health. 2018;18(1):207. doi:10.1186/s12889-018-5091-8
13. Claudel M, Schneide B, Seiwert D. Bringing primary school and parents closer together: adapting a tool from Quebec to a primary school in France. Rev Int Éduc Fam. 2012;32(2):97–120. doi:10.3917/rief.032.0097
14. Dumoulin C, Thériault P, Duval MA, Tremblay IM. Bringing primary schools and families closer together through new communication practices. Ca. rech éduc savoirs Hors-sér. 2013;9(1):4–18.
15. Nguyen MK, Moon J-Y, Lee Y-C. Microalgal ecotoxicity of nanoparticles: an updated review. Ecotoxicol Environ Saf. 2020;201:110781. doi:10.1016/j.ecoenv.2020.110781
16. Villa S, Maggioni D, Hamza H, et al. Natural molecule coatings modify the fate of cerium dioxide nanoparticles in water and their ecotoxicity to Daphnia magna. Environ Pollut. 2020;257:113597. doi:10.1016/j.envpol.2019.113597
17. Minetto D, Volpi Ghirardini A, Libralato G. Saltwater ecotoxicology of Ag, Au, CuO, TiO2, ZnO and C60 engineered nanoparticles: an overview. Environ Int. 2016;92–93:189–201. doi:10.1016/j.envint.2016.03.041
18. Le Gay D. Experiences, opinions and expectations of general practitioners regarding sun prevention and melanoma screening in the Alpes-Maritimes: qualitative study using semi-structured interviews, 2015.
19. Isvy A. Students of Solar Medicine and Prevention (Knowledge and Practice) [Doctoral dissertation]; 2011. Available from: http://www.sudoc.fr/15201120X.
20. Cesarini P. Living with the sun. Arch Pediatr. 2010;17(6):910–911. doi:10.1016/S0929-693X(10)70174-3
21. Sancho-Garnier H, Pereira B, Césarini P. A cluster randomized trial to evaluate a health education programme “Living with Sun at School”. Int J Environ Res Public Health. 2012;9(7):2345–2361. doi:10.3390/ijerph9072345
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.