Back to Journals » Patient Preference and Adherence » Volume 17
Attitude, Practice, and Knowledge Regarding Fluoridated Toothpaste, Brushing, and Rinse Usage Among Residents of Jeddah City in Saudi Arabia
Authors Al-Zain AO ![]() , Fakhry LM
, Fakhry LM ![]() , Tallab RA, Natto ZS
, Tallab RA, Natto ZS ![]()
Received 10 September 2022
Accepted for publication 15 December 2022
Published 5 January 2023 Volume 2023:17 Pages 23—39
DOI https://doi.org/10.2147/PPA.S389413
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Afnan O Al-Zain,1 Layan M Fakhry,2,* Renad A Tallab,2,* Zuhair S Natto3
1Restorative Dentistry Department, King Abdulaziz University Faculty of Dentistry, Jeddah, Saudi Arabia; 2King Abdulaziz University Faculty of Dentistry, Jeddah, Saudi Arabia; 3Department of Public Health, King Abdulaziz University Faculty of Dentistry, Jeddah, Saudi Arabia
*These authors contributed equally to this work
Correspondence: Afnan O Al-Zain, Restorative Dentistry Department, King Abdulaziz University Faculty of Dentistry, P.O. Box 80209, Jeddah, 21589, Saudi Arabia, Tel +966539116467, Fax +9666403316, Email [email protected]
Purpose: To evaluate and compare the attitude, practice, and knowledge of individuals who use fluoridated and non-fluoridated toothpaste in Jeddah city, Saudi Arabia.
Methods: A digital questionnaire composed of 43 questions were formulated. The questionnaire was divided into five sections: eligibility questions, demographic data, attitude, practice, and knowledge. Content and face validation were done, and convenience sampling was used. The inclusion criteria were any citizen and resident who lives in Jeddah city, Saudi Arabia. Descriptive statistics, Chi-square, and Fischer’s tests were conducted to compare fluoridated and non-fluoridated toothpaste users (α=0.05).
Results: A total of 473 completed participants’ responses were collected. Attitude: 41.8% of fluoridated toothpaste users reported that it was “very important” to rinse to remove the toothpaste compared to non-fluoridated toothpaste users (58.3%) (P-value< 0.001). Healthy teeth were the most important to fluoridated toothpaste users (69.1%) (P < 0.001). Practice: 28.6% of non-fluoridated toothpaste users have been using non-fluoridated toothpaste for > 1 year, and 35.7% of them < 2 years. 73.8% of fluoridated toothpaste users used whitening toothpaste. Significantly higher non-fluoridated toothpaste users (29%) used organic toothpaste (P< 0.001).
Knowledge: 57% of fluoridated toothpaste users believed that a good diet, tooth brushing, and fluoridated toothpaste are important to prevent caries, and the fluoride would strengthen the teeth (P< 0.001). Approximately 60% of non-fluoridated toothpaste users did not know the proper age to start using fluoridated toothpaste (P< 0.001). Also, 47.6% of non-fluoridated toothpaste users avoid using fluoride because it is toxic.
Conclusion: Significantly higher number of Jeddah residents that used fluoridated toothpaste had a better attitude and knowledge than non-fluoridated toothpaste users. Nonetheless, most residents had similar oral hygiene practices. It is suggested to execute educational campaigns to explain the importance of fluoridated toothpaste to the population. Also, individuals should take caution from the source of obtaining their dental information and consult their dentist.
Keywords: fluoride, oral health, awareness, caries prevention
Introduction
Fluoride in toothpaste has significantly influenced dental caries reduction since the 1970s.1 Systematic reviews and Cochrane reviews showed evidence of the role of fluoride in caries prevention.2–7 In addition, a Cochrane review supported the benefits of fluoridated toothpaste compared to non-fluoridated toothpaste in preventing caries.8 Fluoridated toothpaste may be used alone or in combination with other fluoridated products such as fluoride varnish, gels, and mouthwashes for caries prevention.6,7 Using such preventive practices is more cost-effective than treating dental caries.9 It was reported that fluoride could be toxic when ingested excessively.1,10–13 However, when the amount and concentration of dispensed toothpaste are controlled, the risk of toxicity is unlikely.1,10–13 Nevertheless, some individuals are shifting to non-fluoridated toothpaste, which needs attention.
Fluoride’s mechanism of action in controlling the dental caries process is through decreasing enamel demineralization and enhancing remineralization. Forming loosely bound calcium fluoride (CaF2) precipitates on the tooth surface, acting as a reservoir of ions allowing the release of calcium and fluoride ions during acid attacks creating supersaturated plaque environments.12 This would reduce the calcium and phosphate release from enamel due to a change in the ion concentration gradient between tooth structure and plaque fluids.12,13
The presence of fluoride during the enamel demineralization and remineralization process enhances the formation of fluorapatite crystals. The fluorapatite crystals formation occurs by the fluoride incorporation into the enamel microstructure, making the enamel surface more resistant to bacterial acid.12 The current understanding of the mechanism of action of fluoride in caries prevention is topically rather than systematically.12,13 Therefore, fluoride’s preventative effect is not only when the teeth are forming; instead, it is through the life span of the individual.13 Evidence showed that brushing with a fluoridated toothpaste twice daily was sufficient to provide a slow release of fluoride needed to protect teeth against caries.1,2,14–16
The concentration of the fluoridated toothpaste varies depending on the age of the individual and frequency of use.1,8,17,18 The concentration of fluoride in the standard over-the-counter toothpaste is 1000–1500 parts per million (ppm) for adults, the prescription toothpaste for adults contains 5000 ppm of fluoride, and the fluoride concentration in toothpaste for children is 1000 ppm.1,8,18 The fluoride concentration in fluoridated mouthwash is typically 100–500 ppm.1 The concentration of fluoride in the fluoride varnishes is typically 22,600 ppm.17 The recommended amount of fluoridated toothpaste in a toothbrush for children aged below three years is smear (rice grain size), children between 3–6 years should use a maximum of pea size amount, and children above six years should use more than a pea size amount but not the entire length of the of a toothbrush.19 However, a study showed that the effect of fluoridated toothpaste could be reduced by washing out fluoride due to excessive rinsing with water or using non-fluoridated mouthwash immediately after brushing, increasing the fluoride clearance.17 Also, using a mouthwash after brushing may enhance the caries preventive effect, mainly if used between toothbrushing episodes rather than immediately after brushing.17 Therefore, it was suggested that the remaining toothpaste would protect the teeth and increase caries’ preventive effect.15,16,20 To date, the impact of post-brushing rinsing techniques on the anti-caries effect of toothpaste is controversial, not well-established yet, and needs further investigations.15,16
Fluoride toxicity can be either acute or chronic.10,13 It was reported that fluoride toxicity may be manifested in various ways including dental and skeletal fluorosis.1,10–13 The daily exposure to high levels of fluoride in the first eight years during tooth development may cause side effects such as dental fluorosis.5,8,13,21,22 Therefore, to avoid the risk of dental fluorosis, the concentration of the fluoridated toothpaste for children should be taken into consideration, and brushing should be done under adult supervision to control the amount of toothpaste dispensed and so the child does not swallow the toothpaste.1,8,13 The fluoride toxicity reported such as affecting the endocrine system, affecting Thyroid Stimulating Hormone and Insulin levels, or the central nervous system may occur when ingestion high amounts of the fluoride exceeding the probable toxic dose of 5mg F/kg.11,21–23 However, this toxic dose may not be reached with the controlled small amount of toothpaste dispensed daily from a fluoridated toothpaste.1,10–13
A study showed that most people were not knowledgeable about whether toothpaste is fluoridated or not.24 A study targeting Swedish adults showed that most participants had a good attitude towards their oral health, and 95% used fluoridated toothpaste, but more investigation was needed.25 Also, regions of some countries may not have access to fluoridated toothpaste.1,26 Nevertheless, using non-fluoridated toothpaste may not help in the prevention of dental caries.8,27 Organic toothpaste contains natural ingredients. Some types of organic toothpaste used for whitening, such as charcoal can tend to cause abrasion to teeth since the whitening toothpaste contains abrasive particles.23 It was observed that some people are shifting towards non-fluoridated toothpaste because they may believe that fluoride is a toxic agent and has many side effects on our bodies. Not considering that organic toothpaste can increase the risk of caries development since it does not contain any fluoride components. Nevertheless, evidence in the literature is lacking, and more studies are needed to investigate the shift of some individuals toward the use of non-fluoridated toothpaste.
There is a gap in the literature regarding the attitude, practice, and knowledge of fluoridated toothpaste users versus non-fluoridated toothpaste users about fluoridated toothpaste in several countries, including Saudi Arabia. Therefore, this study aims to evaluate and compare the attitude, practice, and knowledge of individuals using fluoridated and non-fluoridated toothpaste regarding fluoridated toothpaste, brushing, and rinse usage among the general population living in Jeddah city, Saudi Arabia. The null hypothesis was that there is no difference between fluoridated toothpaste users and non-fluoridated toothpaste users regarding attitude, practice, and knowledge among the general population living in Jeddah city, Saudi Arabia.
Materials and Methods
A cross-sectional study was conducted. An ethical approval (No. 105-11-20) was obtained from Research Ethical Committee at King Abdulaziz University Faculty of Dentistry. This study complies with the Declaration of Helsinki. A digital questionnaire was formulated via SurveyMonkey product (www.momentive.ai, Momentive Inc., San Mateo, California, USA) to collect the data. The questionnaire was composed of 43 questions, including closed and open-ended questions (Supplementary Material). The questionnaire was divided into five sections: 1) consent and study eligibility questions (5 questions); 2) demographic data (4 questions). The following three sections were questions regarding the: 3) attitude (8 questions), 4) practice (16 questions), and 5) knowledge (9 questions) domains. Each domain included questions about bushing with fluoridated or non-fluoridated toothpaste, rinsing with fluoridated products, and flossing. The last question was an optional open-ended comments section. The questionnaire was prepared in Arabic and English languages to target a larger number of participants. The questions were mainly adopted and modified from validated questionnaires.24,28 Others were newly formulated questions.
Content validation was done by consulting five professional dental experts in the field. The experts reviewed the questionnaire and ensured the questions covered the domains of interest to the study aim, clear questions and options, and measured what the question intended to measure. They were asked to rate each question’s importance and whether each item should be included in the questionnaire. Each expert’s comments were incorporated into the questionnaire prior to face validation. The face validation was performed by piloting the questionnaire by interviewing 12 volunteers from the general population of different age groups and backgrounds to represent the study’s target population. Piloting by interviewing was to assess the clarity of questions and the ability of respondents to understand each question. The feedback from the face validation step was incorporated into the final questionnaire. Convenience sampling was used. The inclusion criteria were any citizen and resident living in Jeddah city in Saudi Arabia over 16 years old. The exclusion criteria were anyone who refused to participate in the study.
The introduction to the survey included the aim and benefits of the survey study, that it holds no potential risk to the participant, and that no sensitive information or identification of the participants would be collected. In addition, participation was entirely voluntary, and by answering yes to the first question, “do you agree to participate in the study”, participants consented to their inclusion. The questionnaire was circulated electronically via WhatsApp to ensure it reached a larger number of individuals.
Power Analysis and Statistical Analysis
The sample size was calculated using the G*power program (version 3.1.9). Assuming the odds ratio of 2.0 based on the reported importance of toothpaste between the two groups that we got from the pilot study and using a ratio of 3:1, a sample size of 412 subjects (103 non-fluoridated toothpaste users and 309 fluoridated toothpaste users), is adequate to obtain a Type I error rate of 5% and a power of 80%. An initial sample size of 473 will be recruited (119 non-fluoridated toothpaste users and 354 fluoridated toothpaste users) to account for about 15% of potential missing data.
Descriptive statistics (frequency and percentage or mean and standard deviation) were used. Chi-square or Fischer’s tests compared fluoridated toothpaste versus non-fluoridated toothpaste users regarding their attitude, practice, and knowledge. Multiple logistic regression analysis was performed using all significant variables from bivariate analysis. A p-value of 0.05 was considered statistically significant. All analyses were performed using SPSS V.26 for Windows (IBM).
Results
Demographics and Descriptive Analysis
A total of 473 individuals answered the questionnaire. Table 1 shows the demographic information of the participants in the study. The mean age of fluoridated toothpaste users (33.8±14.5) was significantly higher than non-fluoridated toothpaste users (30.2±14.1) (p=0.016). More Saudis (89.4%) than non-Saudis (10.6%) participated in the study. Significantly more females (76.1%) than males participated in the study (P<0.001). The majority of the participants (51.4%) had a Bachelor’s degree educational level followed by a high school educational level, and lastly, a Graduate degree and Diploma.
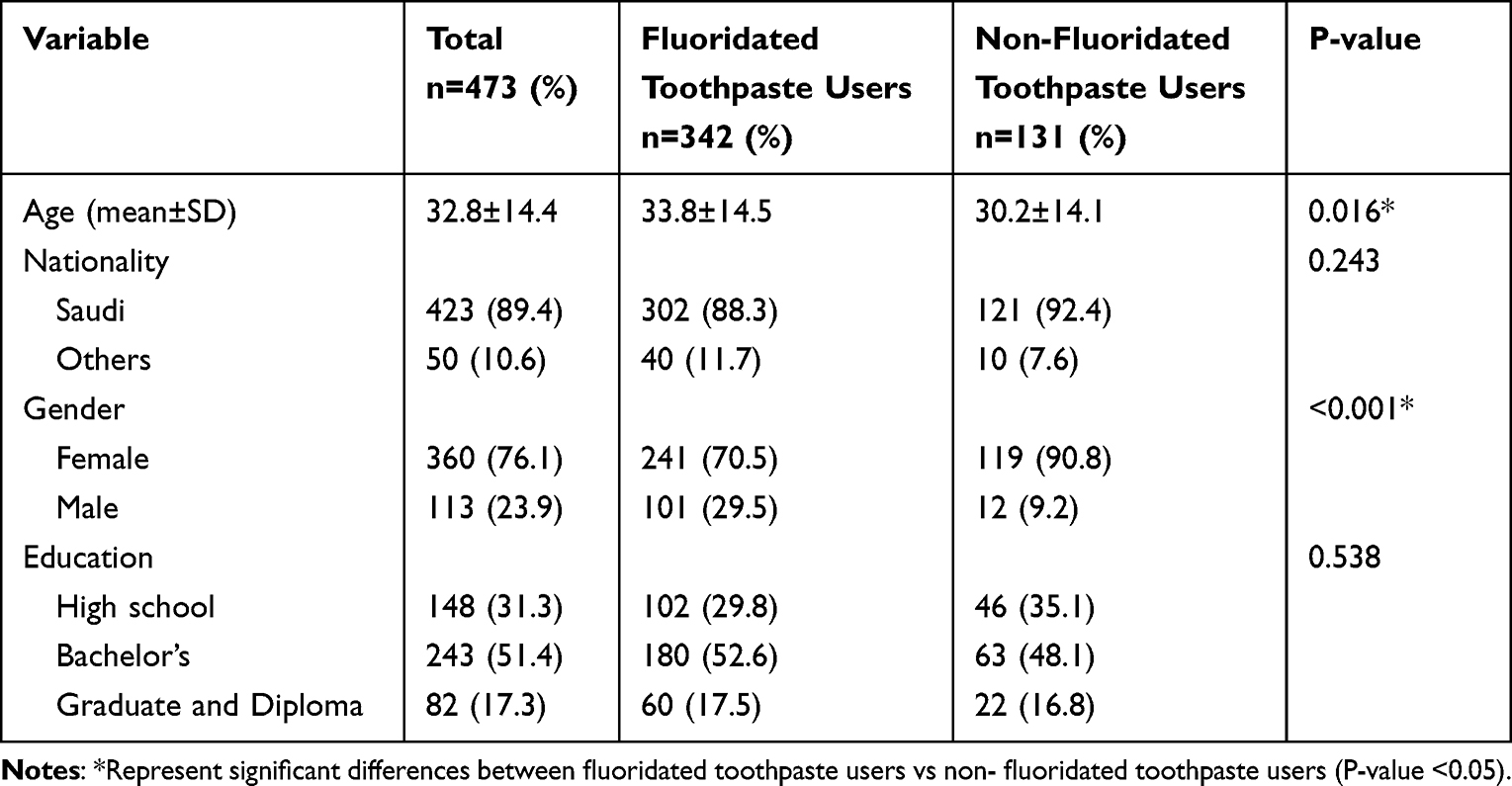 |
Table 1 Demographic Information of the Participants in the Study |
Attitude
Results concerning the attitude are presented in Figures 1 and 2, and Table 2. A significantly higher percentage of fluoridated toothpaste users answered that brushing was “very important” (60.2%) compared to non-fluoridated toothpaste users (32.8%). Individuals that answered that brushing is “not important at all” were non-fluoridated toothpaste users, while individuals who answered “not important” and “slightly important” were mainly using non-fluoridated toothpaste (Figure 1) (P<0.001). When participants were asked why brushing is important, significant differences in the responses were found, where 84.2% of fluoridated toothpaste users mentioned that “it makes their teeth healthy and free of caries” compared to 54.2% of non-fluoridated toothpaste users (Figure 2) (P<0.001). Regarding the importance of rinsing the toothpaste, a significantly higher percentage of fluoridated toothpaste users (41.8%) responded that it is “very important” compared to non-fluoridated toothpaste users (58%) (P=0.002). The reason for their selection was to “remove the toothpaste” selected by 69% of fluoridated toothpaste users and 79.4% of non-fluoridated toothpaste users. When asked about the most important to their teeth, respondents stated that “healthy teeth” was most important for their teeth with a percentage of 69.1%, followed by “white and beautiful-looking teeth” with a percentage of 19.7%, then “painless teeth” by a percentage of 9.3%. When asked about the importance of using toothpaste, significantly higher fluoridated toothpaste users responded that it is “very important” (83.1%) compared to non-fluoridated toothpaste users (74.8%) (P=0.007). When asked about the reason for the importance of their teeth, significantly higher fluoridated toothpaste users (91.8%) selected “makes my teeth healthy and free of caries” compared to non-fluoridated users (84.8%) (P=0.033) (Table 2).
 |
Table 2 Attitude of the Participants Toward Using Fluoridated Toothpaste vs Non-Fluoridated Toothpaste |
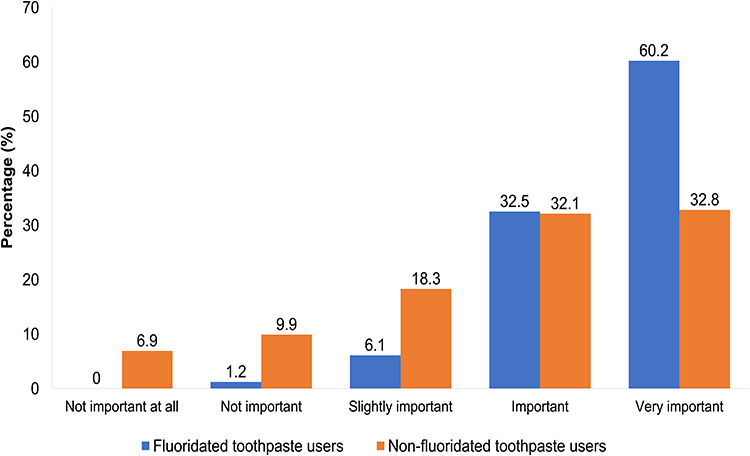 |
Figure 1 Attitude of the participants toward the importance of brushing among fluoridated toothpaste vs non-fluoridated toothpaste users. Significant differences were observed between fluoridated and non-fluoridated toothpaste users (P<0.001). |
 |
Figure 2 Attitude of the participants toward the reason for the importance of brushing among fluoridated toothpaste vs non-fluoridated toothpaste users. Significant differences were observed between fluoridated toothpaste and non-fluoridated toothpaste users (P<0.001). |
Practice
Results concerning participants’ practice are presented in Table 3. Regardless of the type of toothpaste used, most participants (91.2%) brushed their teeth every day, and often they brushed them twice a day (57.9%). The most common brushing pattern was “after wakeup” (82.5%) and “before bed” (76.1%). When asking participants what they use to brush their teeth other than toothpaste, if they do, 10.1% used Miswak, and 9.5% used water only in addition to using toothpaste, regardless of if it was fluoridated toothpaste or not. Most participants (70.6%) dipped the toothbrush under water 1–2 times. Also, 58.9% brushed their teeth for 1–2 minutes, and 81.8% of participants brushed using a regular toothbrush. Regarding non-fluoridated toothpaste users, 28.6% reported that they have been using non-fluoridated toothpaste for less than one year, and 35.7% were using it for more than two years. Most respondents used “whitening toothpaste” (73.8%), followed by “sensitive toothpaste” (31.3%). Significantly higher non-fluoridated toothpaste users used “organic toothpaste” (29%) (P<0.001) and “charcoal toothpaste” (12.2%) (P=0.008). Regarding the amount of toothpaste used, 60.4% of participants stated that they fully cover the toothbrush with toothpaste (full coverage), and 44% of participants “spit out the toothpaste immediately” after brushing regardless of the type of toothpaste used.
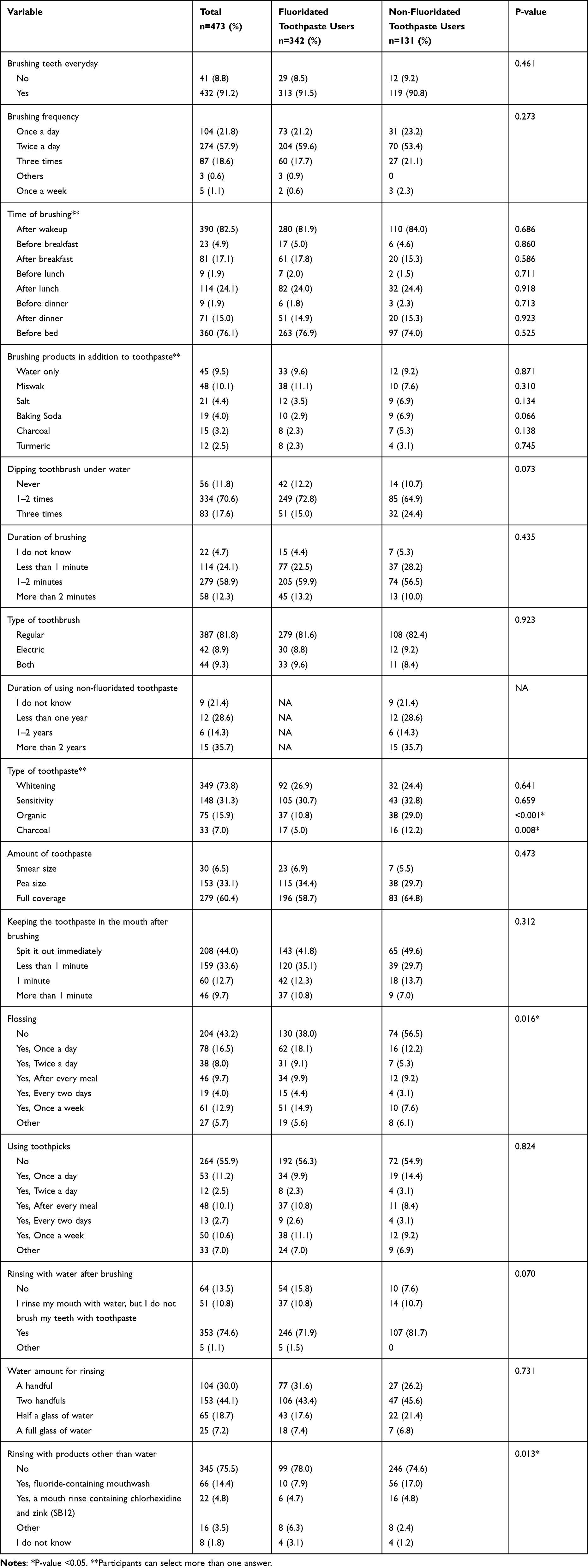 |
Table 3 Practice of the Participants Toward Using Fluoridated Toothpaste vs Non-Fluoridated Toothpaste |
Regarding flossing, a significantly higher number of non-fluoridated toothpaste users (56.5%) do not floss (P=0.016). Moreover, 55.9% of participants did not use toothpicks. In addition, 74.6% of participants rinse their mouth with water after brushing using “two handfuls” of water (44.1%), followed by “a handful” (30%). Significantly more non-fluoridated toothpaste users do not rinse with anything other than water (74.6%) (P=0.013).
Knowledge
Results concerning the knowledge are presented in Figures 3 and 4, and Table 4. Regarding the question asking what prevents caries, significant differences were found, where 57% of fluoridated toothpaste users selected that “Good diet, tooth brushing and fluoride in toothpaste are equally important” to prevent caries compared to 27.5% of non-fluoridated toothpaste users (P<0.001). In addition, significantly more non-fluoridated toothpaste users (39.7%) selected “tooth brushing only” compared to fluoridated toothpaste users (P<0.001) (Table 4). Regarding the question about the effect of fluoridated toothpaste, significantly higher non-fluoridated toothpaste users (37.4%) did not know the effect compared to fluoridated toothpaste users (9.9%) (P<0.001). In addition, significantly higher fluoridated toothpaste users (62%) selected “Strengthens the teeth and prevents caries” compared to non-fluoridated toothpaste users (30.5%) (P<0.001) (Figure 3).
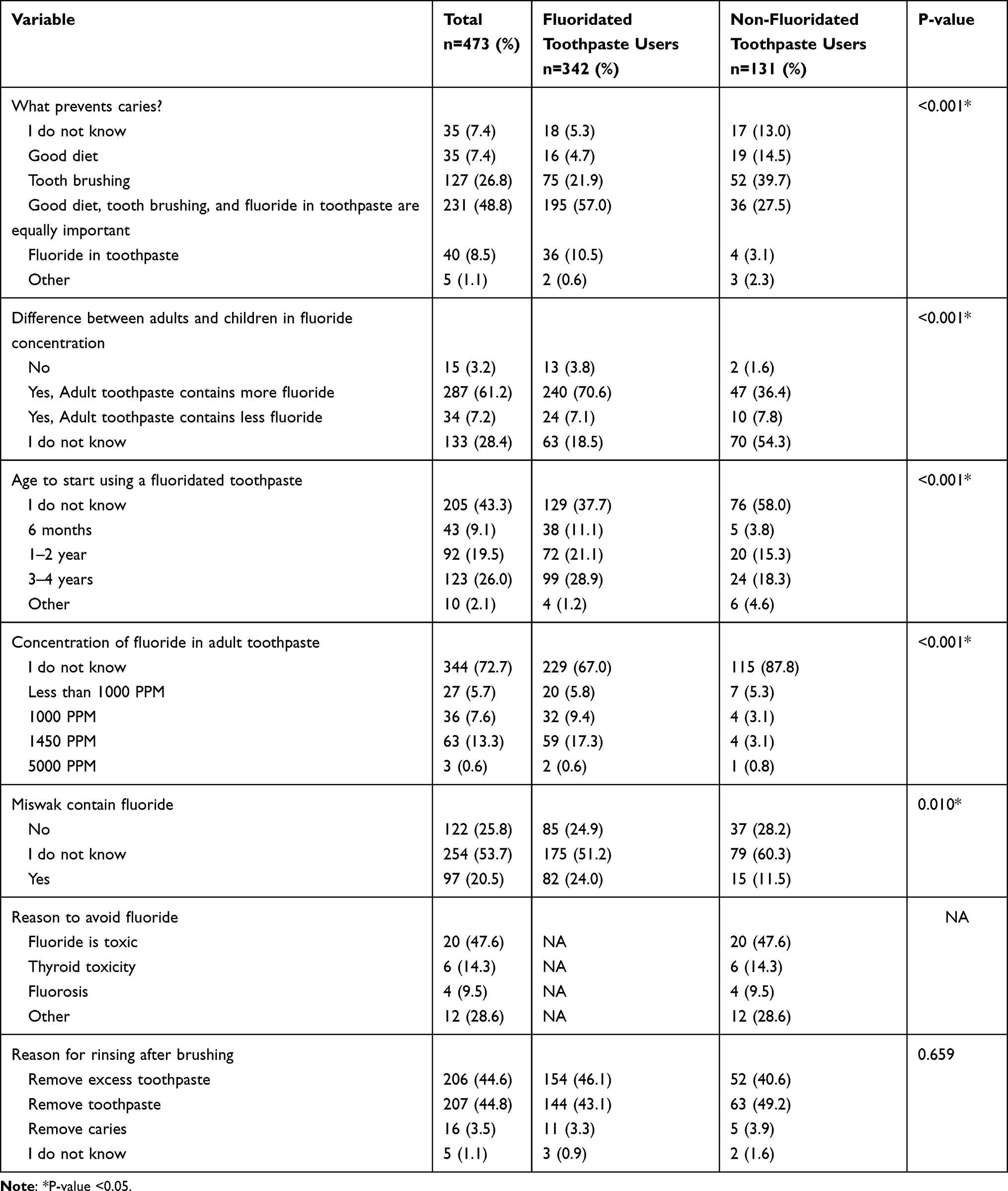 |
Table 4 Knowledge of the Participants Toward Using Fluoridated Toothpaste vs Non-Fluoridated Toothpaste |
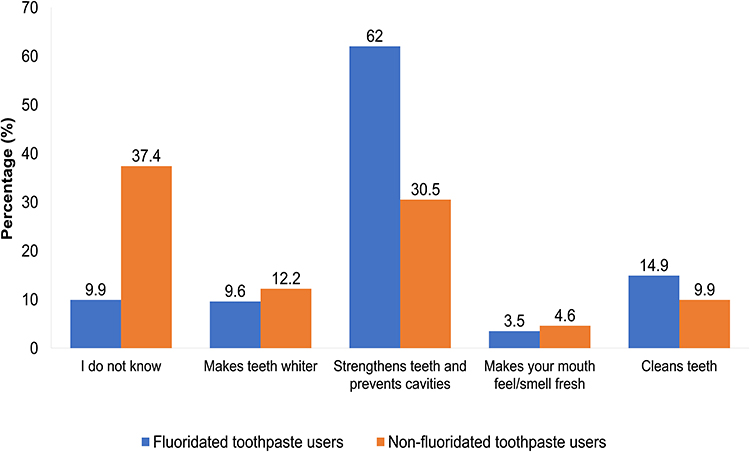 |
Figure 3 Knowledge of participants’ toward the effect of fluoridated toothpaste among fluoridated vs non-fluoridated toothpaste users. Significant differences were observed between fluoridated toothpaste and non-fluoridated toothpaste users (P<0.001). |
Regarding the concentration of the fluoridated toothpaste, significantly higher fluoridated toothpaste users (70.6%) were knowledgeable about the difference between adults and children’s fluoridated toothpaste concentration compared to non-fluoridated toothpaste users (36.4%) (P<0.001). Significantly higher percentages of non-fluoridated toothpaste users (58%) did not know the proper age to start using fluoridated toothpaste and did not know the amount of fluoride in the adult toothpaste (87.8%) (P<0.001). A significantly higher percentage of non-fluoridated toothpaste users (60.3%) did not know whether the Miswak contained fluoride or not (P=0.010). Regarding the reasons to avoid fluoride, 47.6% of the non-fluoridated toothpaste participants reported that “fluoride is toxic” (Table 4).
When selecting a toothpaste to purchase, both the “fluoride concentration” and “the dentist’s recommendation” had a significant difference between the fluoridated toothpaste users and non-fluoridated toothpaste users (P=0.009 and P=0.002, respectively). Where fluoridated toothpaste users select their toothpaste based on the “dentist recommendation” (44.4%) was the most important factor among the participants (Figure 4). Regarding the reason for rinsing after brushing, 44.8% of participants answered to “remove toothpaste” followed by 44.6% of the participants who answered, “remove excess toothpaste” (Table 4).
 |
Figure 4 Knowledge of participants toward what determines which toothpaste to use among fluoridated toothpaste vs non-fluoridated toothpaste users. Significant differences were observed between fluoridated toothpaste and non-fluoridated toothpaste users (P<0.001). |
Regression Models
Table 5 represents the regression model for the participant’s attitude, practice, and knowledge toward fluoridated toothpaste usage.
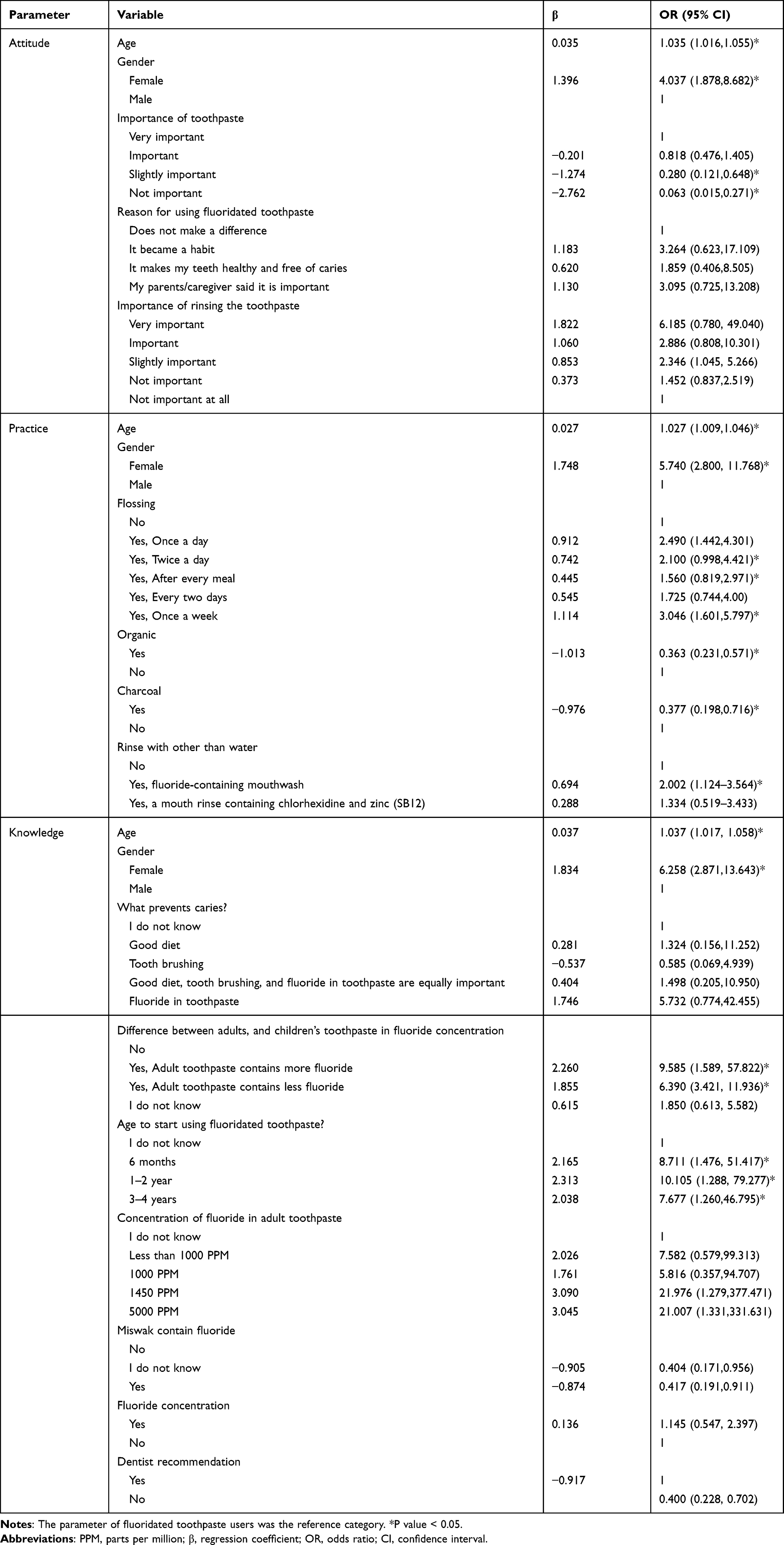 |
Table 5 Regression Model of the Possible Predicting Factors for the Attitude, Practice, and Knowledge of Participants Toward Fluoridated Toothpaste Usage |
Attitude
Age significantly impacted the participant’s attitude toward using fluoridated toothpaste, where it was 1.035 times significantly more likely that older participants would use fluoridated toothpaste (95% CI: 1.016,1.055). Females were significantly more likely to use fluoridated toothpaste by 4.037 times than males (95% CI: 1.878,8.682). Participants who believed it was slightly important or not important at all to use fluoridated toothpaste were significantly less likely to use fluoridated toothpaste by 0.280 (95% CI: 0.121,0.648) and 0.063 times (95% CI: 0.015,0.271), respectively.
Practice
Age significantly impacted the participant’s behavior toward using fluoridated toothpaste, where it was 1.027 times significantly more likely that older participants would use fluoridated toothpaste (95% CI: 1.009,1.046). Females were significantly more likely to have better practice toward fluoridated toothpaste usage by 5.740 times compared to males (95% CI: 2.800, 11.768). Participants who flossed their teeth twice a day were significantly more likely to use fluoridated toothpaste by 2.100 times (95% CI: 0.998,4.421). Furthermore, participants who flossed their teeth after every meal were 1.560 times significantly more likely to use fluoridated toothpaste (95% CI: 0.819,2.971). Also, participants who flossed their teeth once a week was significantly more likely to use fluoridated toothpaste by 3.046 times (95% CI: 1.601,5.797). Participants who used organic toothpaste were significantly 0.363 times less likely to use fluoridated toothpaste (95% CI: 0.231,0.571). Participants who used charcoal toothpaste were significantly 0.377 times less likely to use fluoridated toothpaste (95% CI: 0.198,0.716). Participants who rinsed with fluoride-containing mouthwash were significantly 2.002 times more likely to use fluoridated toothpaste (95% CI: 1.124–3.564).
Knowledge
Age significantly impacted the participant’s knowledge of the usage of fluoridated toothpaste, where it was 1.037 times significantly more likely that older participants would use fluoridated toothpaste (95% CI: 1.017, 1.058). Female participants were significantly 6.258 times more knowledgeable than males (95% CI: 2.871,13.643). Fluoridated toothpaste users were more knowledgeable that adult toothpaste has higher fluoride concentration than children’s toothpaste significantly 9.585 times (95% CI: 1.589, 57.822). On the other hand, fluoridated toothpaste users who believed that adult toothpaste has less fluoride concentration than children’s toothpaste were significantly 6.390 times more than non-fluoridated toothpaste users (95% CI: 3.421, 11.936). Participants who know the age to start using fluoridated toothpaste at six months were significantly 8.711 times more likely to use fluoridated toothpaste (95% CI: 1.476, 51.417). In addition, participants who believed that the age to start using fluoridated toothpaste at 1–2 years were significantly 10.105 times more likely to use fluoridated toothpaste (95% CI: 1.288, 79.277). Also, participants who believed that the age to start using fluoridated toothpaste at 3–4 years were significantly 7.677 times more likely to use fluoridated toothpaste (95% CI: 1.260,46.795).
Discussion
This study showed the attitude, practice, and knowledge of participants that used fluoridated toothpaste compared to non-fluoridated toothpaste. The fact that fluoridated toothpaste users were significantly more knowledgeable about brushing, fluoride, and the role of fluoridated toothpaste play in caries prevention compared to non-fluoridated toothpaste users, could explain their significantly better attitude towards brushing and using toothpaste and the reason why it is important for participants. Nevertheless, the participant’s attitude and knowledge did not significantly impact participants’ practice except in a few areas (type of toothpaste used, flossing, and rinsing with products other than water).
Regarding attitude towards the importance of brushing and using toothpaste, the significantly better responses from fluoridated toothpaste users about its importance could also be explained by the fact that they were significantly more knowledgeable, thereby significantly impacting their attitude towards oral health. Some of the common responses in the “other” option could also explain the reason behind their attitude towards brushing. Participants reported in “others” that brushing was important because they had braces, for their oral hygiene, to prevent caries, remove foul odor, and make teeth smell good, or a combination of these responses. These responses supported why brushing was “important” or “very important” to most participants. On the other hand, when asking about the reason behind the attitude towards the importance of using toothpaste, some common responses in the “other” option included that it was best to use natural ingredients, the toothpaste refreshes the mouth, toothpaste can be replaced by Miswak (natural chewing stick), and it can be replaced with mouthwash. These responses further explain the different beliefs, misconceptions, and lack of knowledge some individuals may have about toothpaste and oral hygiene practices. Nevertheless, regarding the importance of using toothpaste in general, and the attitudes toward dental health and care were similar to the results of another study done by Jensen et al.24
Compared to fluoridated toothpaste users, it was interesting that a significantly higher percentage of non-fluoridated toothpaste users responded that rinsing off the toothpaste is very important, and both groups agreed that the reason was to remove the toothpaste. This indicated that participants were keen to remove excess toothpaste regardless of if they used fluoridated toothpaste or not and regardless of the level of importance. In addition, some participants justified removing remaining toothpaste by rinsing could be just a force of habit. Some common responses in the “other” option regarding the reason behind rinsing the toothpaste included removing food remnants, making their teeth feel cleaner, avoiding swallowing fluoride, and eliminating the possible harmful effect of fluoride. Some participants revealed different reasons for spitting toothpaste without rinsing, one of which was to keep fluoride in the oral cavity. This is justified by the fact that some participants mentioned that they were following their dentists’ recommendations or that people mentioned it was important not to rinse. However, they did not know the reason why. As mentioned previously, there is still controversy and limited evidence-based about post-brushing rinsing, and it needs further investigations. Nevertheless, there was consensus about suggested post-brushing rinsing practices with the limited evidence available.15,16 The consensus suggested was to increase post-brushing fluoride retention by spitting out the excess toothpaste, rinsing with a slurry of fluoridated toothpaste with saliva or rinsing with a fluoride-containing mouthwash.15,16
Regarding practice, a justification that similar percentages (approximately 90%) of participants brushed daily could be that they were taught to do so when they were young, regardless of the type of toothpaste used. A similar justification could explain why approximately 60% of participants brushed twice a day for 1–2 minutes and could explain why approximately 80% of participants brushed after they woke up and before they went to bed, regardless of the toothpaste type used. Our results were in line with another study that showed that most of the Swedish population brushed their teeth twice daily every day for 1–2 minutes.4 Few responses in the “other” option in our study included brushing 4–6 times daily and after every meal. These responses are different variations of toothbrushing habits. The literature supports that the effect of fluoride in caries prevention is increased with increasing the frequency of brushing using a fluoridated toothpaste and with higher fluoride concentration.1,2,5,15,16,29 Nevertheless, evidence showed that brushing twice daily with a fluoridated toothpaste was sufficient to provide the slow release of fluoride needed to protect teeth against caries.1,2,14–16
Regarding the participant’s preferences for using products other than toothpaste to brush their teeth showed that non-fluoridated toothpaste users mainly selected those products except for the Miswak. This could be explained by the cultural effect, as Miswak has been used for decades, usually in combination with fluoridated toothpaste, in oral hygiene practice by various populations and cultures. Moreover, Miswak was advocated to have anti-plaque and anti-gingivitis properties, as well as anti-cariogenic properties.30,31 As for charcoal-based powder, some people believe it has whitening properties. A recent study by Franco et al found that it does not have any bleaching effect.32 Regarding the participant’s knowledge about the presence of fluoride in Miswak, the significant differences may be explained by the fact that Miswak is used as a cultural habit in Saudi Arabia without individuals being aware of its active ingredient.
Regarding brushing with baking soda (Sodium bicarbonate), studies reported that it could effectively enhance plaque removal and improve gingival health.33–36 In addition, it was reported that fluoridated toothpaste containing baking soda to be more effective than fluoridated toothpaste alone in reducing gingival inflammation, bleeding, and plaque removal.33–36 Salt and water fluoridation were reported to be one of the community-level modalities of caries prevention for children. However, using either water or salt fluoridation was recommended to minimize dental fluorosis risk in children under the age of eight with developing teeth.5 Salt fluoridation programs were suggested to be used in countries or areas where fluoridated toothpaste is not readily available.37 Turmeric is a spice commonly used in cooking, also known as Haldi, curcumin, and Curcuma longa was found to have anti-inflammatory, antioxidant, anti-bacterial, anti-viral, anti-fungal, anti-tumor, and wound healing, among other properties.38 A study exhibited that the essential oil of turmeric has anti-cariogenic properties on Streptococcus Mutans at specific concentrations.39 Nevertheless, further investigations are needed regarding the effectiveness of some of these products and their potential preventative effect on caries and their side effects.
Regarding the type of toothpaste used, the significantly higher number of non-fluoridated toothpaste users, which used organic toothpaste and charcoal toothpaste, could also be explained by the participant’s belief that fluoride is toxic. In addition, the belief that organic toothpaste, whether it contains charcoal or not, is better than other types of toothpaste because it contains natural ingredients. In addition, needing to be more knowledgeable about the benefits of fluoride in toothpaste may have influenced their practice. The practices may have also been influenced by social media or their families and friends. Regarding flossing, the significantly higher results that fluoridated toothpaste users floss their teeth could also be because they wanted their teeth to be healthy and free of caries. Common responses in the “other” option in the flossing and toothpick questions included flossing or using toothpicks sometimes or rarely when food is lodged between the teeth. A few respondents mentioned that a water jet was used. Interestingly, a significantly higher percentage of non-fluoridated toothpaste users used fluoridated mouthwash than fluoridated toothpaste users. This may be explained by the fact that non-fluoridated toothpaste users believed that fluoridated toothpaste is harmful but not mouthwash. In addition, they may have thought the lower fluoride concentration in the mouthwash was not harmful, or they were unaware that it contained fluoride.
Regarding the significant differences in knowledge between both groups showed that non-fluoridated toothpaste users had misconceptions about fluoridated toothpaste that could have influenced their attitude and some of their oral hygiene practices. The significantly higher number of participants that knew that a good diet, tooth brushing, and fluoride in toothpaste are equally important to prevent caries, and the effect of fluoridated toothpaste on caries prevention was fluoridated toothpaste users could be explained by the fact that non-fluoridated toothpaste users believed that brushing can prevents caries not the fluoride ingredient in the toothpaste. In addition, the fact that a significantly higher percentage of fluoridated toothpaste users knew the difference between adult and children’s fluoride concentration in the toothpaste, the fluoride concentration in their toothpaste, and the age to start administering fluoride all support our findings where some of the non-fluoridated toothpaste users did not have sufficient knowledge about the effect of the fluoridated toothpaste in caries prevention and did not use fluoridated toothpaste because they believed that fluoride is toxic or harmful to their body. This is also supported by the fact that approximately 29% of the participants reported in the option “others” various reasons for not using fluoridated toothpaste; they are convinced that they do not need it or should never be used. Others believed they did not know why they were not using fluoridated toothpaste, or there was no particular reason for not using it, they did not know what fluoride is, and heard it was not good for them, but they were not sure about the reason, or a mix of the aforementioned different reasons. The 47.6% of non-fluoridated toothpaste users that thought that fluoride is a toxic agent to their health may be due to the social media influence and misleading marketing of other types of toothpaste.
The concern of some people about fluoride toxicity and its side effects on the body may be the reason for their shift toward non-fluoridated toothpaste. However, as mentioned, by this shift, they need to be aware that they are reducing exposure to topical fluoride and, subsequently, increasing their risk of dental caries because it does not contain any fluoride components. For those individuals who are concerned about fluoride toxicity, individuals need to know that toxicity can only occurs after ingestion of high amounts of the fluoride exceeding the toxic dose, which can be either acute or chronic, as previously mentioned.11,13,22 The acute fluoride toxicity that individuals are concerned about with fluoridated toothpaste may occur with ingestion of large quantities of fluoridated toothpaste, which can be a problem explicitly seen with young children.10,11,13,21 In addition, chronic exposure to high fluoride concentrations over a long period may increase the risk of dental fluorosis during tooth development. Some organizations such as The American Academy of Pediatrics recommends using fluoridated toothpaste for children with the eruption of the first tooth by limiting the amount to a smear or a grain of rice.40 Therefore, the amount of fluoride toothpaste dispensed for children under the age of six and brushing should be done under adult supervision.1,8,10,13 The effect of fluoride on endocrine tissues and cancer reported is controversial and needs more investigations.14,41 Nevertheless, such toxicity with fluoridated toothpaste is hardly possible by ingesting a controlled small amount of toothpaste daily with brushing. This further supports our findings that non-fluoridated toothpaste users were less knowledgeable and had misleading information about fluoridated toothpaste.
The significantly higher percentage of fluoridated toothpaste users that purchased their toothpaste based on fluoride in the toothpaste and dentists’ recommendation was not surprising since the main difference between fluoridated and non-fluoridated toothpaste users was the presence of fluoride. Although it was interesting that most fluoridated toothpaste users base their purchase on the presence of fluoride, they did not know the fluoride concentration in the adult toothpaste. This may be because they were keen that it contains fluoride and did not pay attention to its concentration. The significant differences could also be explained by the fact that non-fluoridated toothpaste users are not using fluoridated toothpaste, so they do not know the concentration, and they pay attention only if it contains fluoride or not. As mentioned, evidence showed that the concentration of fluoridated toothpaste varies depending on the age of the individual and frequency of use.1,8,18 Where children need lower fluoride concentration (1000 ppm) compared to adults (1200 ppm), and high caries risk patients would need higher fluoride concentration (5000 ppm in a prescription toothpaste).1,8,18 Nevertheless, the appropriate response about the determination of which toothpaste to purchase among fluoridated toothpaste users is the dentist’s recommendation because it is the most reliable way to get the correct information is by asking the health care professional.
Regarding the regression model of attitude, practice, and knowledge, age and gender were predictors for using fluoridated toothpaste or not for all three aspects investigated. This indicated that females are more attentive to their teeth’s health than males. Moreover, the older the individual is, the more aware of their teeth’s health. The results may have been impacted by the fact that more females than males participated in the study, and females are more interested in their oral health than males. Regarding the attitude regression model, in addition to age and gender, the participant’s beliefs may explain the attitude toward the importance of using toothpaste, significantly impacting their choice of using or not using fluoridated toothpaste. Regarding the practice regression model, in addition to age and gender, flossing, using organic toothpaste and brushing with charcoal, and using a fluoridated mouthwash were predictors for non-fluoridated toothpaste users. In addition, they were more seemingly to rinse their teeth using a fluoridated mouthwash. Non-fluoridated toothpaste users were more likely to rinse the toothpaste most likely to get rid of the fluoridated toothpaste. Also, it was evident that most non-fluoridated toothpaste users were more likely to use organic toothpaste since it is fluoride-free. This supports our findings that fluoridated toothpaste users were more knowledgeable and had better attitudes and practices towards their teeth health than non-fluoridated toothpaste users. Regarding the knowledge regression model, in addition to age and gender, the knowledge of the differences in concentration between adults and children and at which age they should start using fluoridated toothpaste were significant predictors of using fluoridated toothpaste as significantly higher participants mainly were taking the correct information from health care professionals.
Our study has some limitations, such as using convenience sampling, which may not have represented the whole Jeddah city. In addition, using an electronic survey may exclude part of the population which may not be familiar with the electronic surveys.
Conclusion
Individuals who used fluoridated toothpaste have a significantly better attitude toward brushing and using toothpaste and its importance than those who did not use fluoridated toothpaste. Individuals that used fluoridated toothpaste have significantly better practice toward flossing and rinsing with products in addition to or other than water compared to individuals that did not use fluoridated toothpaste. Individuals who used fluoridated toothpaste were significantly more knowledgeable regarding toothpaste than those who did not. Most of the non-fluoridated toothpaste users in Jeddah city do not have sufficient information about the importance of brushing, rinsing, and fluoridated toothpaste and its effects compared to the fluoridated toothpaste users. For that reason, efforts should be made to increase awareness and education among the population about the importance of fluoride in toothpaste. Also, it is advisable that individuals take caution where they get the information and consult their dentist.
Disclosure
The authors report no conflicts of interest in this work.
References
1. O’Mullane DM, Baez RJ, Jones S, et al. Fluoride and oral health. Community Dent Health. 2016;33:69–99.
2. Marinho VC, Higgins JP, Sheiham A, et al. Fluoride toothpastes for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2003;2003:CD002278. doi:10.1002/14651858.CD002278
3. Twetman S. Caries prevention with fluoride toothpaste in children: an update. Eur Arch Paediatr Dent. 2009;10:162–167. doi:10.1007/BF03262678
4. Twetman S, Axelsson S, Dahlgren H, et al. Caries-preventive effect of fluoride toothpaste: a systematic review. Acta Odontol Scand. 2003;61:347–355. doi:10.1080/00016350310007590
5. Pollick H. The role of fluoride in the prevention of tooth decay. Pediatr Clin North Am. 2018;65:923–940. doi:10.1016/j.pcl.2018.05.014
6. Marinho VC, Higgins JP, Sheiham A, et al. Combinations of topical fluoride (toothpastes, mouthrinses, gels, varnishes) versus single topical fluoride for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2004;2004:CD002781. doi:10.1002/14651858.CD002781.pub2
7. Marinho VC, Higgins JP, Sheiham A, et al. One topical fluoride (toothpastes, or mouthrinses, or gels, or varnishes) versus another for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2004;2004:CD002780. doi:10.1002/14651858.CD002780.pub2
8. Walsh T, Worthington HV, Glenny AM, et al. Fluoride toothpastes of different concentrations for preventing dental caries. Cochrane Database Syst Rev. 2019;3:CD007868. doi:10.1002/14651858.CD007868.pub3
9. Marinho VC, Chong LY, Worthington HV, et al. Fluoride mouthrinses for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2016;7:CD002284. doi:10.1002/14651858.CD002284.pub2
10. Duffin S, Duffin M, Grootveld M. Revisiting fluoride in the twenty-first century: safety and efficacy considerations. Front Oral Health. 2022;3:873157. doi:10.3389/froh.2022.873157
11. Ullah R, Zafar MS, Shahani N. Potential fluoride toxicity from oral medicaments: a review. Iran J Basic Med Sci. 2017;20:841–848. doi:10.22038/IJBMS.2017.9104
12. Ten Cate JM, Buzalaf MAR. Fluoride mode of action: once there was an observant dentist. J Dent Res. 2019;98:725–730. doi:10.1177/0022034519831604
13. Martínez-Mier EA. Fluoride: its metabolism, toxicity, and role in dental health. J Evid Based Complement Alternat Med. 2012;17:28–32. doi:10.1177/2156587211428076
14. American Academy of Pediatric Dentistry. Fluoride Therapy. The Reference Manual of Pediatric Dentistry. Chicago, Ill: American Academy of Pediatric Dentistry; 2021:302–305.
15. Parnell C, O’Mullane D. After-brush rinsing protocols, frequency of toothpaste use: fluoride and other active ingredients. Monogr Oral Sci. 2013;23:140–153.
16. Pitts N, Duckworth RM, Marsh P, et al. Post-brushing rinsing for the control of dental caries: exploration of the available evidence to establish what advice we should give our patients. Br Dent J. 2012;212:315–320. doi:10.1038/sj.bdj.2012.260
17. Duckworth RM, Maguire A, Omid N, et al. Effect of rinsing with mouthwashes after brushing with a fluoridated toothpaste on salivary fluoride concentration. Caries Res. 2009;43:391–396. doi:10.1159/000239753
18. Bentley EM, Ellwood RP, Davies RM. Fluoride ingestion from toothpaste by young children. Br Dent J. 1999;186:460–462. doi:10.1038/sj.bdj.4800140
19. Thornton-Evans G, Junger ML, Lin M, et al. Use of toothpaste and toothbrushing patterns among children and adolescents - United States, 2013–2016. MMWR Morb Mortal Wkly Rep. 2019;68:87–90. doi:10.15585/mmwr.mm6804a3
20. Kaczmarek U, Pregiel B, Wrzyszcz-Kowalczyk A, et al. Fluoride levels in saliva after tooth-brushing using fluoride toothpastes with and without rinsing of oral cavity. Ann Acad Med Stetin. 2006;52(Suppl 1):45–49.
21. Iida H, Kumar JV. The association between enamel fluorosis and dental caries in U.S. schoolchildren. J Am Dent Assoc. 2009;140:855–862. doi:10.14219/jada.archive.2009.0279
22. Skórka-Majewicz M, Goschorska M, Żwierełło W, et al. Effect of fluoride on endocrine tissues and their secretory functions -- review. Chemosphere. 2020;260:127565. doi:10.1016/j.chemosphere.2020.127565
23. Ghajari MF, Shamsaei M, Basandeh K, et al. Abrasiveness and whitening effect of charcoal-containing whitening toothpastes in permanent teeth. Dent Res J. 2021;18:51. doi:10.4103/1735-3327.321862
24. Jensen O, Gabre P, Sköld UM, et al. Is the use of fluoride toothpaste optimal? Knowledge, attitudes and behaviour concerning fluoride toothpaste and toothbrushing in different age groups in Sweden. Community Dent Oral Epidemiol. 2012;40:175–184. doi:10.1111/j.1600-0528.2011.00658.x
25. Stenberg P, Håkansson J, Akerman S. Attitudes to dental health and care among 20 to 25-year-old Swedes: results from a questionnaire. Acta Odontol Scand. 2000;58:102–106. doi:10.1080/000163500429217
26. Hobbs M, Marek L, Clarke R, et al. Investigating the prevalence of non-fluoride toothpaste use in adults and children using nationally representative data from New Zealand: a cross-sectional study. Br Dent J. 2020;228:269–276. doi:10.1038/s41415-020-1304-5
27. Fan X, Li X, Wan H, et al. Clinical investigation of the anticaries efficacy of a 1.14% sodium monofluorophosphate (SMFP) calcium carbonate-based dentifrice: a two-year caries clinical trial on children in China. J Clin Dent. 2008;19:134–137.
28. Llodra JC, Phantumvanit P, Bourgeois DM, et al. LLL2: an international global level questionnaire on toothbrushing and use of fluoride toothpaste. Int Dent J. 2014;64(Suppl 2):20–26. doi:10.1111/idj.12128
29. Walsh T, Worthington HV, Glenny AM, et al. Fluoride toothpastes of different concentrations for preventing dental caries in children and adolescents. Cochrane Database Syst Rev;2010. CD007868. doi:10.1002/14651858.CD007868.pub2
30. Saha S, Mohammad S, Saha S, et al. Efficiency of traditional chewing stick (miswak) as an oral hygiene aid among Muslim school children in Lucknow: a cross-sectional study. J Oral Biol Craniofac Res. 2012;2:176–180. doi:10.1016/j.jobcr.2012.10.009
31. Mustafa M, AlJeaidi Z, AlAajam WH, et al. Study of caries prevalence among miswak and non-miswak users: a prospective study. J Contemp Dent Pract. 2016;17:926–929. doi:10.5005/jp-journals-10024-1955
32. Franco MC, Uehara J, Meroni BM, et al. The effect of a charcoal-based powder for enamel dental bleaching. Oper Dent. 2020;45:618–623. doi:10.2341/19-122-L
33. Ghassemi A, Hooper WJ, Vorwerk LM, et al. The effects of two baking-soda toothpastes in enhancing mechanical plaque removal and improving gingival health: a 6-month randomized clinical study. Am J Dent. 2020;33(5):265–272.
34. Myneni SR. Effect of baking soda in dentifrices on plaque removal. J Am Dent Assoc. 2017;148:S4–S9. doi:10.1016/j.adaj.2017.09.004
35. Putt MS, Milleman KR, Ghassemi A, et al. Enhancement of plaque removal efficacy by tooth brushing with baking soda dentifrices: results of five clinical studies. J Clin Dent. 2008;19:111–119.
36. Ghassemi A, Vorwerk LM, Hooper WJ, et al. A four-week clinical study to evaluate and compare the effectiveness of a baking soda dentifrice and an antimicrobial dentifrice in reducing plaque. J Clin Dent. 2008;19:120–126.
37. Vautey S, Ranivoharilanto E, Decroix B, et al. [Salt fluoridation and dental caries: state of the question]. Sante Publique. 2017;29:185–190. French. doi:10.3917/spub.172.0185
38. Chaturvedi TP. Uses of turmeric in dentistry: an update. Indian J Dent Res. 2009;20:107–109. doi:10.4103/0970-9290.49065
39. Lee KH, Kim BS, Keum KS, et al. Essential oil of curcuma longa inhibits Streptococcus mutans biofilm formation. J Food Sci. 2011;76:H226–H230. doi:10.1111/j.1750-3841.2011.02427.x
40. Pediatrics AAo fluoride toothpaste should be used when child’s first tooth erupts: AAP; 2022. Available from: https://www.aap.org.
41. Wong MC, Glenny AM, Tsang BW, et al. Topical fluoride as a cause of dental fluorosis in children. Cochrane Database Syst Rev. 2010;2010:Cd007693. doi:10.1002/14651858.CD007693.pub2
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Gender Differences in Oral Health Knowledge and Practices Among Adults in Jeddah, Saudi Arabia
Rajeh MT
Clinical, Cosmetic and Investigational Dentistry 2022, 14:235-244
Published Date: 4 August 2022
Parental Knowledge and Awareness of Fluoride Varnish Application on Their Children - A Cross-Sectional Study
Almehmadi AH, Bannan A, Ahmad A, Alqadi R, Alhindi A
International Journal of General Medicine 2022, 15:7435-7442
Published Date: 22 September 2022
Obesity-Related Knowledge and Practice Among the Healthcare Professions Students in Saudi Arabia
Elsafi SH, Al-Dossari RH, Al-shaqi RA, Fakirah WE, Al-Dossari RF, Al-sharif OJ, Maawadh RM, Al Musallam LD, Alaohali A, Abu Hassan AM, Alfahad OA, Al Naam YA, Al Zahrani EM
Diabetes, Metabolic Syndrome and Obesity 2024, 17:427-434
Published Date: 26 January 2024
The Effect of an Education Program on School Children Oral Health in Khartoum, Sudan
Albani GFAA, Abdelgadir WI, Mohamed AAA, Yousif M, Mustafa AMA, Almkiy EAA, Mohammed KZM, Mohamed EAS, Alghamdi FAA, Ahmed RG, Hakami MSA, Dinar NA, Alsulami A, Mudawi AIA, Ahmed WAM
Journal of Multidisciplinary Healthcare 2024, 17:1065-1077
Published Date: 12 March 2024
Knowledge, Attitude and Practice Toward Artificial Intelligence Among Healthcare Workers in Private Polyclinics in Jeddah, Saudi Arabia
Serbaya SH, Khan AA, Surbaya SH, Alzahrani SM
Advances in Medical Education and Practice 2024, 15:269-280
Published Date: 5 April 2024