Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Atherosclerosis Risk Factors in Patients with Reactive Hypoglycemia
Authors Landowska M ![]() , Żebrowska A, Fajer K, Adamek P, Kruk A, Kałuża B, Franek E
, Żebrowska A, Fajer K, Adamek P, Kruk A, Kałuża B, Franek E
Received 21 April 2022
Accepted for publication 2 September 2022
Published 14 October 2022 Volume 2022:15 Pages 3133—3142
DOI https://doi.org/10.2147/DMSO.S371706
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Małgorzata Landowska,1,2 Agata Żebrowska,2 Konrad Fajer,2 Patrycja Adamek,2 Aleksandra Kruk,2 Bernadetta Kałuża,1,2 Edward Franek1,3
1Department of Internal Medicine, Endocrinology and Diabetology, Central Clinical Hospital of the Ministry of Interior and Administration in Warsaw, Warsaw, Poland; 2Students Scientific Group of the Medical University of Warsaw at the Department of Internal Medicine, Endocrinology and Diabetology, Central Clinical Hospital of the Ministry of Interior and Administration in Warsaw, Warsaw, Poland; 3Department of Human Epigenetics, Mossakowski Medical Research Centre Polish Academy of Sciences, Warsaw, Poland
Correspondence: Bernadetta Kałuża, Department of Internal Medicine, Endocrinology and Diabetology, Central Clinical Hospital of the Ministry of Interior and Administration in Warsaw, Wołoska 137, Warsaw, 02-507, Poland, Tel +47 722 14 05, Email [email protected]
Purpose: Glucose metabolism disorders are an established risk factor for atherosclerosis. Although reactive hypoglycemia (RH) can be classified as one of these disorders, its role as a potential atherosclerosis risk factor remains unclear. The aim of the study was to assess whether patients with RH have a higher risk of atherosclerosis.
Patients and Methods: We recruited 178 patients (N=178) with suspected RH who were hospitalized after 2014 and underwent a prolonged 5-hour oral glucose tolerance test. The study cohort was divided into 2 groups depending on the results of the oral glucose tolerance test: Group 1 – subjects without RH (n=44), Group 2 –subjects with RH (n=134).
Results: The analyzed groups differed significantly in terms of the following risk factors for atherosclerosis: high-density lipoprotein (HDL) cholesterol levels (54.3± 18.8 mg/dL vs 63± 18.5 mg/dL, p=0.003) and atherogenic indices (Castelli I: 3.7± 1.2 vs 3.1± 1.3, p=0.004; Castelli II: 2.1± 0.9 vs 1.7± 0.9, p=0.007; the atherogenic index of plasma: 0.34± 0.33 vs 0.18± 0.3, p=0.006; and the atherogenic coefficient: 2.7± 1.2 vs 2.1± 1.3, p=0.004). Univariate logistic regression showed that RH should not be considered to be a predictor of an increased atherogenic index of plasma (odds ratio [OR]=0.3 [95% confidence interval [CI] [0.16– 0.7], p=0.002). Multivariate logistic regression revealed triglyceride levels (OR 1.14 [1.07– 1.2], p=0.001) and body weight (OR 1.07 [1.03– 1.12], p=0.002) to be independent risk factors for atherosclerosis.
Conclusion: Atherosclerosis risk factors are no more prevalent in patients with RH. RH does not increase the risk of an abnormal atherogenic index of plasma.
Keywords: postprandial hypoglycemia, oral glucose tolerance test, body weight, cardiovascular risk, triglycerides
Introduction
Advanced age, male sex, dyslipidemia, arterial hypertension, smoking and glucose metabolism disorders are established risk factors for atherosclerosis.1 Both type 2 diabetes mellitus (DM) and hyperglycemia-associated conditions can be classified as atherosclerotic risk factors related to abnormal glucose metabolism.2 The Thrombolysis in Myocardial Infarction (TIMI) 10A, TIMI 10B, Limitation of Myocardial Infarction following Thrombolysis in Acute Myocardial Infarction (LIMIT-AMI), Action to Control Cardiovascular Risk in Diabetes (ACCORD) and Orofiban in Unstable Angina (OPUS-TIMI 16) trials revealed that irrespective of DM diagnosis, the relationship between post-ST-elevation myocardial infarction blood glucose levels and prognosis can be illustrated as a U-curve.3–7 The 30-day mortality rates in patients with either hypoglycemia or hyperglycemia are comparable and significantly higher than those in subjects with normoglycemia.8,9 This observation may be associated with autonomic nervous system dysfunction, baroreceptor reflex impairment, abnormalities in heart rate variability, and prolongation of the QT interval, all of which can be found in diabetic patients.10–12 Research has shown that patients with diabetic neuropathy may have a higher cardiovascular risk due to compromised counter-regulatory mechanisms following a hypoglycemic episode.13,14 On the other hand, even an adequate response to hypoglycemia, including an increased catecholamine release or corticosteroid production, can be detrimental to the cardiovascular system, promote atherogenesis, and induce hypokalemia.8,13 Furthermore, elevated levels of C-reactive protein, interleukin-6, interleukin-8, tumor necrosis factor alpha, endothelins, or growth factors can be found in diabetic patients during hypoglycemic episodes.15,16 Hypoglycemia has also been identified as a factor responsible for inducing fibrinolytic dysfunction.16 An increase in serum adrenaline levels, which occurs when blood glucose levels are abnormally low, influences platelet and leukocyte function.16 Moreover, hypoglycemia can lead to endothelial dysfunction and abnormal coagulation.10 All the defense mechanisms that prevent an individual from the negative consequences of hypoglycemia appear to be crucial in establishing prognosis in diabetic patients after acute coronary syndrome.17 However, it remains unclear whether or not these defense, counter-regulatory, mechanisms alter the prognosis in otherwise healthy patients who experience reactive hypoglycemia (RH), defined as blood glucose levels lower than 70 mg/dL that occurs 2–5 hours after a meal.18,19 The potential role of RH in atherogenesis has not been thoroughly investigated.18 Few researchers have evaluated the prevalence of atherosclerosis risk factors in patients with RH.18,20 Considering the aforementioned pathogenic mechanisms, an attempt to assess if RH can be recognized as another risk factor for atherosclerosis seems to be warranted. Our knowledge of atherosclerotic burden in patients with RH is largely based on limited data. Therefore, we undertook this study in order to assess the prevalence of atherosclerosis risk factors in patients with RH. The aim of our research was also to determine if RH can be considered as a novel atherosclerosis risk factor.
Materials and Methods
Study Cohort
Our study included 178 subjects, who were hospitalized in the Central Clinical Hospital of the Ministry of Interior and Administration in Warsaw after January 2014. Inclusion criteria were as follows: 1) clinically suspected RH (based on either a history of symptoms potentially associated with hypoglycemia or home-measured blood glucose levels below 70 mg/dL); 2) complete medical records; 3) a prolonged oral glucose tolerance test (OGTT). Patients who were 1) diagnosed with hypoglycemia secondary to medication; a non-islet cell tumor; an insulinoma; hepatic, cardiac, or renal failure; cortisol, glucagon, or epinephrine deficiency; nesidioblastosis; or sepsis; 2) previously diagnosed with pre-diabetes or type 2 DM; 3) positive for antibodies against insulin or insulin receptors; 4) malnourished; and/or 5) diagnosed with chronic conditions (except for arterial hypertension) were excluded from the study.21 Out of all participants, 28 were male (n=28), 27 had a history of hypertension (n=27), no patient has reported being on either lipid-lowering or antidiabetic therapy.
Study Protocol
We analyzed the patients’ medical records for the data on their body weight and history of dyslipidemia and/or hypertension. In order to document hypoglycemic episodes and to exclude other glucose metabolism disorders a prolonged OGTT was performed. Participants underwent an overnight fast of at least 10 hours and were subsequently asked to drink a solution with 75 g of glucose. Blood samples were obtained immediately before and one, two, three, four, and five hours after glucose ingestion. Blood glucose levels were measured using the hexokinase method while insulin levels were assessed via a noncompetitive electrochemiluminescence-based immunoassay. Total cholesterol, HDL-cholesterol, and triglyceride (TG) levels were determined via fluorometric-enzymatic assays. Low-density lipoprotein (LDL) cholesterol levels were calculated using the Friedewald equation. In order to characterize patients in terms of atherosclerotic risk factors, the study group was divided into two subgroups depending on the results of the prolonged OGTT. Subjects whose blood glucose levels were lower than 70 mg/dL at any timepoint after the ingestion of the glucose solution were classified as exhibiting RH and assigned to group 2 (n=134). The remaining individuals were assigned to group 1 (participants without RH) (n=44). The likelihood of developing atherosclerosis was assessed using the atherogenic index of plasma (AIP).22,23 Patients with AIP>0.24 were considered to have an increased cardiovascular risk.24
Definitions
Out of the commonly used atherogenic indices we chose to focus on the AIP as a marker of plasma atherogenicity.22 The AIP is defined as the logarithm of the ratio of molar TG and HDL-cholesterol concentrations.25 AIP values lower than or equal to 0.24 were considered to be normal.26 The two study subgroups were also compared in terms of other atherogenic indices: 1) Castelli’s risk index I (CRI-I), defined as the ratio of total cholesterol to HDL-cholesterol, 2) Castelli’s risk index II (CRI-II), defined as the ratio of LDL-cholesterol to HDL-cholesterol, and 3) atherogenic coefficient (AC), defined as the ratio of non-HDL-cholesterol to HDL-cholesterol.25,27 In order to identify insulin resistance (IR), we used the Homeostasis Model Assessment of Insulin Resistance (HOMA-IR), which is the product of fasting plasma insulin (mU/L) and fasting plasma glucose (mmol/L) divided by 22.5.28 IR was diagnosed when HOMA-IR was greater than or equal to 2.5.29
Hypoglycemia was defined as glucose plasma levels lower than 70 mg/dL.19
Dyslipidemia was defined as total cholesterol≥190 mg/dL, or TG≥150 mg/dL, or LDL-cholesterol ≥115 mg/dL, or HDL-cholesterol<40 mg/dL (for men) and HDL-cholesterol<45 mg/dL (for women).30
Statistical Analysis
Statistical analysis was done with the use of Statistica 13.3, StatSoft Polska Sp. z. o. o. 2022. The relationship between RH and the risk of developing atherosclerosis was estimated using univariate logistic regression. Potential risk factors for developing atherosclerosis were analyzed using multivariate logistic regression. P-values of less than 0.05 were considered to be statistically significant.
Results
Anthropometric Data
Comparing the results of the two analyzed groups, we observed a statistically significant difference in fasting blood glucose and blood glucose levels at hours 3, 4, and 5 of the prolonged OGTT. Interestingly, group 1 and group 2 differed significantly in terms of their fasting insulin levels and insulin levels at hours 4 and 5 after glucose solution ingestion. Surprisingly, HOMA-IR was considerably higher in group 1, with the mean value of 2.7, whereas in group 2, the mean HOMA-IR value was 1.9. A similar tendency was found in terms of body weight and the mean body mass index (BMI). Patients from group 1 had significantly higher BMI when compared with those from group 2.
There was a significant difference in lipid profile results between the analyzed groups. HDL-cholesterol levels were significantly higher in individuals with RH, whereas TG levels were higher in subjects without RH. It is crucial to note that the analyzed groups were significantly different with respect to all atherogenic indices. Even more striking is the fact that non-RH participants on average had higher atherogenic index values than patients with RH (CRI-I – group 1: 3.7±1.2, group 2: 3.1±1.3, p=0.004; CRI-II – group 1: 2.1±0.9, group 2: 1.7±0.9, p=0.007; API – group 1: 0.34±0.33, group 2: 0.18±0.3, p=0.006; AC – group 1: 2.7±1.2, group 2: 2.1±1.3, p=0.004). No significant difference was found between group 1 and group 2 as far as thyroid stimulating hormone and cortisol levels were concerned.
Based on the available data, no significant difference was found between the analyzed groups in terms of smoking status and family history of CVD (smoking(N=61) – group 1(n=18): 3(16.7%), group 2(n=41): 12(27.9%), p=0.35; family history of CVD(N=54) – group 1(n=15): 8(53.3%), group 2(n=39): 21(53.9%), p=0.97).
Analysis of potential atherosclerosis risk factors has been presented in Table 1, whereas the results of multivariate logistic regression are in Table 2. An AIP value of >0.24 was regarded as an indicator of an increased risk of atherosclerosis.
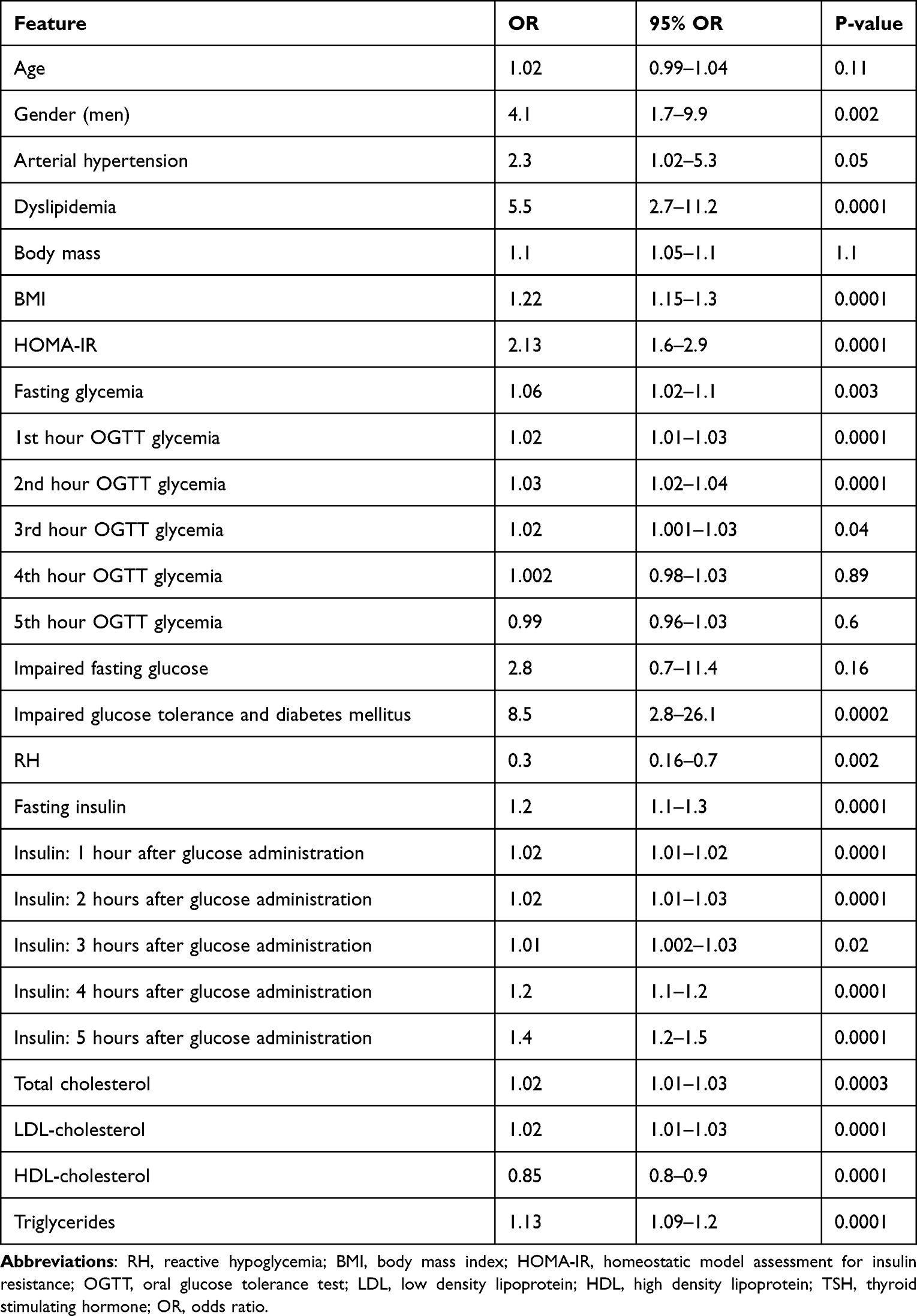 |
Table 1 Univariate Logistic Regression |
 |
Table 2 Multivariate Logistic Regression |
Univariate Logistic Regression
Univariate logistic regression analysis (Table 1) showed that established atherosclerosis risk factors such as dyslipidemia, elevated BMI, or impaired glucose tolerance (IGT) can be considered to be risk factors of atherosclerosis (dyslipidemia OR 5,5 with a 95% Cl of 2.7–11.2, p=0.0001) (BMI OR 1.22 [95% Cl 1.15–1.3], p=0.0001) (IGT OR 8.5 [95% Cl 2.8–26.1], p=0.0002). Similarly, elevated TG levels were found to be a risk factor for atherosclerosis (OR 1.13 [95% Cl 1.09–1.2], p=0.0001). Increased values of both HOMA-IR and fasting insulin can also be viewed as atherosclerosis risk factors (OR 2.13 [95% Cl 1.6–2.9], p=0.0001; OR 1.2 [95% Cl 1.1–1.3], p=0.0001, respectively). The analysis did not reveal RH to increase the risk of atherosclerosis (OR 0.3 [95% Cl 0.16–0.7], p=0.002).
Independent Atherosclerosis Risk Factors
Multivariate logistic regression analysis revealed that elevated TG levels can be regarded as independent risk factors for atherosclerosis (TG OR 1.139 [1.075–1.206], p=0.001) (Table 2). Although increased body weight was found to be independently associated with atherosclerosis, the strength of the association was weak (body weight OR 1.070 [1.025–1.118], p=0.002) (Table 2).
Discussion
RH is defined as glucose plasma levels lower than 70 mg/dL that occurs 2–5 hours after a meal.31 In order to diagnose RH, Whipple triad criteria have to be met.32 This means that hypoglycemic episodes have to occur during a fasting period, glucose intake should lead to symptom suppression, and symptoms have to be associated with low blood glucose levels.33 Depending on the time after which plasma glucose levels fall below 70 mg/dL, RH can be categorized as: idiopathic – occurring approximately 3 hours after a meal, postprandial – occurring within 0.5–2 hours, and late – occurring 4–5 hours after a meal.34 The last category may be related to impaired insulin sensitivity, and thus, late RH can be regarded as a predictor of type 2 DM.31,32
To our knowledge, no large clinical studies have been conducted on the epidemiology of RH. Therefore the prevalence of RH is difficult to estimate. Furthermore, there are no standardized guidelines on how to diagnose RH, and there are various diagnostic glucose cut-off values suggested in literature.34,35
Hypoglycemia can be considered as a major distress to the human body and in some cases can be life-threatening.10 In order to maintain glucose homeostasis, a vast array of counter-regulatory mechanisms evolved to prevent tissues from the negative consequences associated with hypoglycemia.10 Blood glucose levels below 80 mg/dL inhibit insulin secretion, whereas blood glucose lower than 70 mg/dL results in the release of counter-regulatory hormones.8 Glucagon, epinephrine, norepinephrine, growth hormone, and cortisol play a major role in the hormonal response to hypoglycemia.8 In order to estimate the counter-regulatory response to hypoglycemia, insulin, glucose, and morning cortisol levels were measured in blood samples of all patients undergoing this study.36 Contrary to our expectations, no significant differences in cortisol levels were found between the individuals diagnosed with RH and those without this condition. There are several possible explanations for this observation. Firstly, the threshold for hypoglycemia in our study was set at 70 mg/dL in accordance with the American Diabetes Association criteria.19 Cortisol surges when blood glucose levels fall below 58 mg/dL. Thus, some patients who were diagnosed with RH may have not reached the required threshold for cortisol release.37 Secondly, both hyperinsulinemia and the hypoglycemic episodes that precede it diminish the effectiveness of counter-regulatory mechanisms during the subsequent hypoglycemic episodes.14,37 However, the comparison of patients with and without RH did not reveal the predominance of the former group in terms of insulin concentration. Moreover, insulin levels at hours 4 and 5 of the prolonged OGTT were significantly higher in the non-RH group than in the RH group (Table 3). These results seem to support the first explanation of cortisol results.
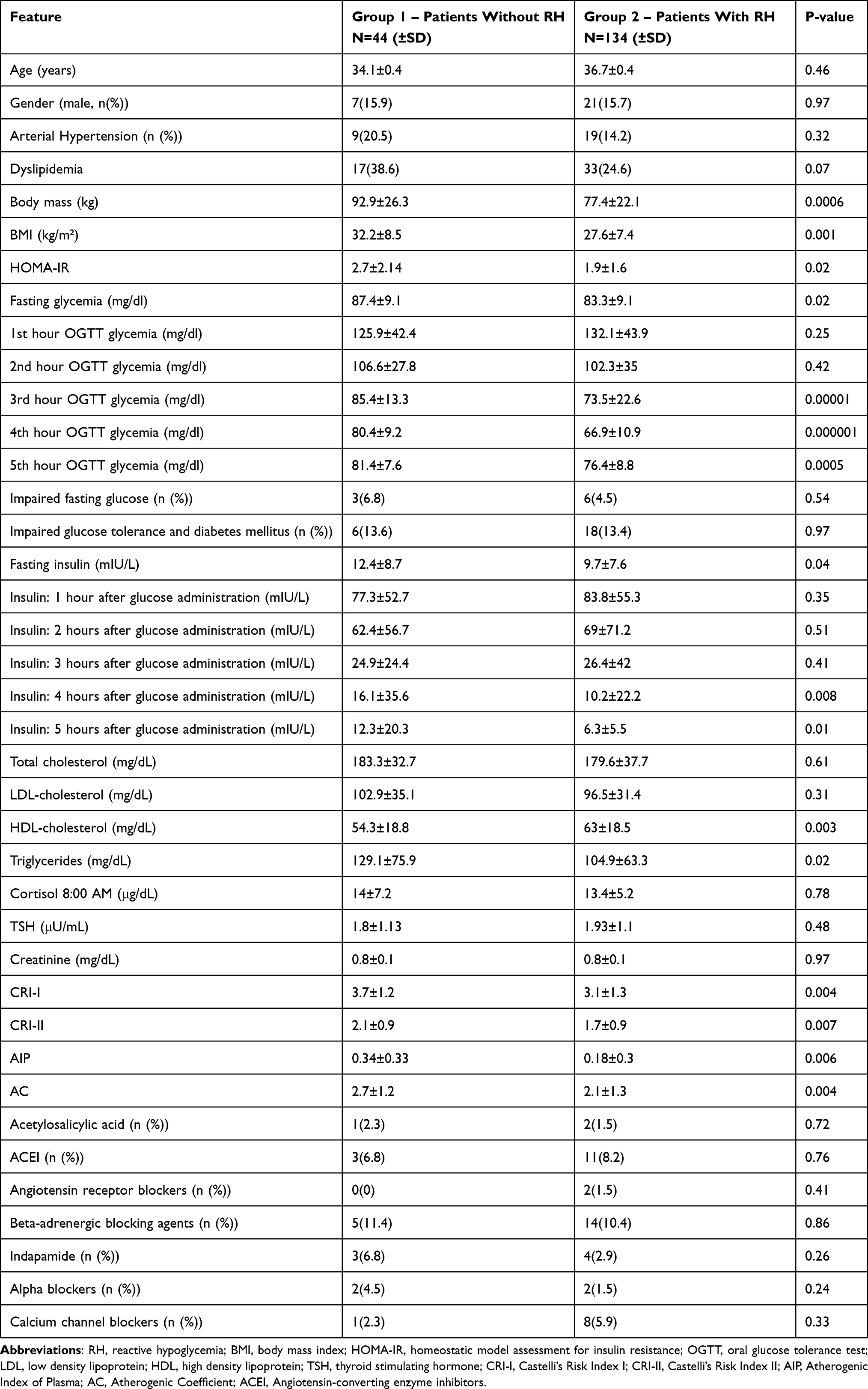 |
Table 3 Anthropometric Data, Blood Tests Results |
Although hypoglycemia-associated counter-regulatory mechanisms are crucial for maintaining glucose homeostasis, their impact on the cardiovascular system can be described as detrimental.36 Hypoglycemia induces abnormal platelet activation, increases the risk of thrombosis, disrupts endothelial function, and can be regarded as a pro-inflammatory state.10,16 Similar pathophysiological changes that occur as part of the counter-regulatory response to hypoglycemia are also responsible for atherosclerotic plaque formation.10,38 However, it is uncertain whether hypoglycemia causes atherosclerosis or rather is only an indicator of the body’s susceptibility to adverse cardiovascular events.16
There is even less research available on the role of RH in the pathogenesis of atherosclerosis. Çiftçi et al [2019] claim to be the first to have explored the association between postprandial RH and subclinical atherosclerosis in reasonably healthy individuals.18 In order to estimate the severity of preclinical atherosclerosis, those authors compared two subgroups of patients (those diagnosed with RH [n=28] and those without RH [n=23]) in terms of carotid intima media thickness (cIMT), epicardial fat tissue (EFT), and high-sensitivity C-reactive protein (hs-CRP) levels. The RH group had significantly worse results in all the above variables in comparison with the control group. Thus, Çiftçi et al demonstrated that patients who suffer from RH are at a higher atherosclerotic risk than healthy subjects.18 Our findings are contrary to those reported by Çiftçi. In order to assess the risk of developing atherosclerosis, we compared the patients with RH with those without RH in terms of four atherogenic indices: CRI-I, CRI-II, API, and AC. Surprisingly, individuals with RH had significantly lower values of all four atherogenic indices than the non-RH subgroup (Table 3). The discrepancy between our and Çiftçi’s results may be due to various factors. For example, our study design differs from Çiftçi’s (2019) in terms of the sample size (n=178 vs n=51) and the method of atherosclerosis risk assessment (atherogenic index values vs cIMT, EFT, and hs-CRP levels).
In order to further explore the relationship between atherosclerosis and RH, we decided to assess if patients with RH differ significantly from the non-RH group in terms of established atherosclerosis risk factors. The 2021 European Society of Cardiology (ESC) Guidelines on cardiovascular disease prevention in clinical practice name five main, modifiable risk factors of atherosclerotic cardiovascular disease (ASCVD): blood apo-B-containing lipoproteins, especially LDL cholesterol, hypertension, cigarette smoking, DM, and adiposity.39 Having taken into consideration a study by Strisciuglio [2020], who proved the utility of HOMA-IR in coronary atherosclerotic disease risk assessment, we additionally characterized our patients in terms of IR (Table 3).40 Interestingly, patients with RH had significantly lower values of BMI and lower body weight than the control group. Additionally, we found that individuals with RH had significantly better insulin sensitivity than non-RH subjects. Nevertheless, no significant difference between the subgroups was found in terms of total and LDL-cholesterol levels (Table 3). The RH subgroup had significantly better results regarding HDL-cholesterol and TG levels (Table 3). Similar observations on glucose and lipid metabolism in patients with RH were made by Hall M. et al (2021), who reported no significant abnormalities in insulin response or alterations in the lipid profile in individuals with RH.34 On the other hand, Lv X et al (2020) found that at hours 3 and 4 of an OGTT, the incidence of RH was higher in obese subjects than in patients with BMI<30 kg/m2. Furthermore, their results showed that an increase of BMI was associated with an upward trend in terms of blood insulin levels. Thus, they concluded that the occurrence of RH may be related to increased body weight and IR.35 The divergent study results may be associated with the lack of standardized guidelines on RH diagnosis and the heterogeneity of study populations.
Another not fully researched aspect of RH is whether this condition can be regarded as a novel atherosclerosis risk factor. Our univariate logistic regression analysis showed that, apart from the well-established atherosclerosis risk factors, such as dyslipidemia (OR=5.5 [2.7–11.2] p=0.0001) or an increased BMI (OR=1.22 [1.15–1.3] p=0.0001), also HOMA-IR (OR=2.13 [1.15–1.3] p=0.0001), fasting insulin (OR=1.2 [1.1–1.3] p=0.0001), and elevated insulin levels at hours 4 and 5 of a prolonged OGTT (OR=1.2 [1.1–1.2] p=0.0001; and OR=1.4 (1.2–1.5) p=0.0001, respectively) may be regarded as atherosclerosis risk factors (Table 1). Our results are consistent with those by Di Pino et al, who investigated a possible link between IR and atherosclerosis. In his review, Di Pino reported that there is considerable evidence indicating a strong association between IR and ASCVD.41 Our analysis showed that, unlike IR, RH cannot be regarded as atherosclerosis risk factor, as it is even associated with a reduced risk of atherosclerosis. Moreover, the risk of atherosclerosis development in patients with RH is over three times lower than that in non-RH individuals (Table 1). However, our multivariate logistic regression analysis did not show this relationship. Only increased body weight (OR=1.070 [1.025–1.118] p=0.002) and TG (OR=1.139 [1.075–1.206] p=0.001) were found to be independent risk factors for atherosclerosis (Table 2). The significant influence of obesity and overweigh on the development of ASCVD is well established.30 According to ESC and European Atherosclerosis Society (EAS) guidelines for the management of dyslipidaemias BMI maintenance in the range of 20–25 should constitute one of the treatment targets for CVD prevention.30 The role of TG in the development of ASCVD was also discussed there. Our results are consistent with the guidelines which indicate that there is causal association between TG-rich lipoproteins (TGRLs), their remnants, and the risk of ASCVD.30 Additional information on the relationship between TG and atherosclerosis was provided by M. Farnier et al. The objective of their review was to summarize recent knowledge on the association between atherosclerosis and TG. The authors argue that although LDL cholesterol-lowering treatment results in substantial ASCVD risk reduction, patients on statin therapy, with increased TG levels have a higher residual risk due to the presence of TGRLs.42 Furthermore, TGRLs have proinflammatory and prothrombotic properties.42 To the best of our knowledge, this is the first time RH has been reported to be associated with a reduced risk of atherosclerosis. Due to the limited number of studies on this topic and the discrepant conclusions that can be drawn from the available literature, further research on the relationship between atherosclerosis and RH is required.
Study Limitations
Our study has some limitations. Firstly, the retrospective character of our study greatly limited any study design modifications. Secondly, the cross-sectional character of our study hindered us from unequivocally determining if RH can be regarded as an atherosclerosis risk factor. Lastly, out of the various methods of atherosclerosis risk stratification presented in the literature, we focused on the AIP. Unfortunately, this situation precludes comparing the results of our study and those that used different methods of atherosclerosis risk assessment.
Conclusions
In conclusion, we found that the prevalence of atherosclerosis risk factors is not increased in patients with RH. Moreover, our study results suggested that RH might be associated with a reduced risk of atherosclerosis. Further research, especially including prospective, longitudinal studies is necessary to establish if RH should be taken into consideration in atherosclerosis risk stratification.
Ethics Approval and Informed Consent
The study protocol, which follows the provisions of the Declaration of Helsinki, had been approved by The Bioethics Committee at the Medical University of Warsaw (approval No. KB/108/2021). It was agreed that due to the retrospective nature of the study the need for informed consent can be waived. Study participants’ data were anonymized. Due diligence was exercised to maintain the confidentiality of the medical records.
Acknowledgments
The study was supported by the Polish Ministry of Education and Science as part of the “Student science clubs create innovations” program.
Funding
Our research was funded by the Polish Ministry of Education and Science from state budget resources as part of the “Student science clubs create innovations” program [grant number: SKN/SP/496715/2021]. The sponsor was not involved in any of the stages of our study.
Disclosure
Prof. Edward Franek MD PhD reports personal fees from Bayer, Boehringer Ingelheim, Novo Nordisk, Eli Lilly, and Servier, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Libby P, Buring JE, Badimon L., et al. Atherosclerosis. Nat Rev Dis Primers. 2019;5(1):56. doi:10.1038/s41572-019-0106-z
2. Poznyak A, Grechko AV, Poggio P, Myasoedova VA, Alfieri V, Orekhov AN. The Diabetes Mellitus-Atherosclerosis Connection: the Role of Lipid and Glucose Metabolism and Chronic Inflammation. Int J Mol Sci. 2020;21(5):1835. doi:10.3390/ijms21051835
3. Tanasijevic MJ, Cannon CP, Wybenga DR, et al. Myoglobin, creatine kinase MB, and cardiac troponin-I to assess reperfusion after thrombolysis for acute myocardial infarction: results from TIMI 10A. Am Heart J. 1997;134(4):622–630. doi:10.1016/S0002-8703(97)70044-9
4. Tanasijevic MJ, Cannon CP, Antman EM, et al. Myoglobin, creatine-kinase-MB and cardiac troponin-I 60-minute ratios predict infarct-related artery patency after thrombolysis for acute myocardial infarction: results from the Thrombolysis in Myocardial Infarction study (TIMI) 10B. J Am Coll Cardiol. 1999;34(3):739–747. doi:10.1016/S0735-1097(99)00274-0
5. Baran KW, Nguyen M, McKendall GR, et al. Double-blind, randomized trial of an anti-CD18 antibody in conjunction with recombinant tissue plasminogen activator for acute myocardial infarction: limitation of myocardial infarction following thrombolysis in acute myocardial infarction (LIMIT AMI) study. Circulation. 2001;104(23):2778–2783. doi:10.1161/hc4801.100236
6. Goff DC, Gerstein HC, Ginsberg HN, et al. Prevention of cardiovascular disease in persons with type 2 diabetes mellitus: current knowledge and rationale for the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial. Am J Cardiol. 2007;99(12A):4i–20i. doi:10.1016/j.amjcard.2007.03.002
7. Bhadriraju S, Ray KK, DeFranco AC, et al. Association between blood glucose and long-term mortality in patients with acute coronary syndromes in the OPUS-TIMI 16 trial. Am J Cardiol. 2006;97(11):1573–1577. doi:10.1016/j.amjcard.2005.12.046
8. Yang SW, Park KH, Zhou YJ. The Impact of Hypoglycemia on the Cardiovascular System: physiology and Pathophysiology. Angiology. 2016;67(9):802–809. doi:10.1177/0003319715623400
9. Fujiwara T, Yoshida M, Yamada H, et al. Lower 1,5-anhydroglucitol is associated with denovo coronary artery disease in patients at high cardiovascular risk. Heart Vessels. 2015;30(4):469–476. doi:10.1007/s00380-014-0502-y
10. Jialal I, Dhindsa S. Hypoglycemia and the predisposition to cardiovascular disease: is the pro-inflammatory-pro-coagulant diathesis a plausible explanation? Atherosclerosis. 2016;251:504–506. doi:10.1016/j.atherosclerosis.2016.06.006
11. Rao AD, Bonyhay I, Dankwa J, et al. Baroreflex Sensitivity Impairment During Hypoglycemia: implications for Cardiovascular Control. Diabetes. 2016;65(1):209–215. doi:10.2337/db15-0871
12. Fitzpatrick C, Chatterjee S, Seidu S, et al. Association of hypoglycaemia and risk of cardiac arrhythmia in patients with diabetes mellitus: a systematic review and meta-analysis. Diabetes Obes Metab. 2018;20(9):2169–2178. doi:10.1111/dom.13348
13. Amiel SA, Aschner P, Childs B; International Hypoglycaemia Study Group. Hypoglycaemia, cardiovascular disease, and mortality in diabetes: epidemiology, pathogenesis, and management. Lancet Diabetes Endocrinol. 2019;7(5):385–396. doi:10.1016/S2213-8587(18)30315-2
14. Sankar A, Khodai T, McNeilly AD, et al. Experimental Models of Impaired Hypoglycaemia-Associated Counter-Regulation. Trends Endocrinol Metab. 2020;31(9):691–703. doi:10.1016/j.tem.2020.05.008
15. EikFilho W, Marcon SS, Krupek T, et al. Blood levels of pro-inflammatory and anti-inflammatory cytokines during an oral glucose tolerance test in patients with symptoms suggesting reactive hypoglycemia. Braz J Med Biol Res. 2016;49(8):e5195. doi:10.1590/1414-431x20165195
16. Joy NG, Tate DB, Younk LM, Davis SN. Effects of Acute and Antecedent Hypoglycemia on Endothelial Function and Markers of Atherothrombotic Balance in Healthy Humans. Diabetes. 2015;64(7):2571–2580. doi:10.2337/db14-1729
17. Murata M, Adachi H, Oshima S, Kurabayashi M. Asymptomatic Reactive Hypoglycemia and Inflammatory Reaction in Patients with Coronary Artery Disease. Int Heart J. 2018;59(4):705–712. doi:10.1536/ihj.17-245
18. Çiftçi FC, Tuğcu AU, Çiftçi Ö. Sub-clinic atherosclerosis in patients with postprandial reactive hypoglycemia. Ann Med Res. 2019;26(12):2941–2947. doi:10.5455/annalsmedres.2019.10.609
19. American Diabetes Association. 6. Glycemic Targets: standards of Medical Care in Diabetes-2021. Diabetes Care. 2021;44(Suppl1):S73–S84. doi:10.2337/dc21-S006
20. Johnston SS, Conner C, Aagren M, Smith DM, Bouchard J, Brett J. Evidence linking hypoglycemic events to an increased risk of acute cardiovascular events in patients with type 2 diabetes. Diabetes Care. 2011;34(5):1164–1170. doi:10.2337/dc10-1915
21. Cryer PE, Axelrod L, Grossman AB, et al. Evaluation and management of adult hypoglycemic disorders: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2009;94(3):709–728. doi:10.1210/jc.2008-1410
22. Edwards MK, Blaha MJ, Loprinzi PD. Atherogenic Index of Plasma and Triglyceride/High-Density Lipoprotein Cholesterol Ratio Predict Mortality Risk Better Than Individual Cholesterol Risk Factors, Among an Older Adult Population. Mayo Clin Proc. 2017;92(4):680–681. doi:10.1016/j.mayocp.2016.12.018
23. Noble-Campbell T. Atherogenic Index in Plasma and Risk of Cardiovascular Events [Dissertation]. Accra: University of Otago; 2019.
24. Akici N, Onal ZE, Gürbüz T, Sağ C, Kilinç S. ATHEROGENIC INDICES IN THE ASSESSMENT OF CARDIOVASCULAR DISEASE RISK IN CHILDREN WITH OBESITY AND SUBCLINICAL HYPOTHYROIDISM. Acta Endocrinol. 2020;16(3):334–338. doi:10.4183/aeb.2020.334
25. Guo J, Wang A, Wang Y, et al. Non-traditional Lipid Parameters as Potential Predictors of Asymptomatic Intracranial Arterial Stenosis. Front Neurol. 2021;12:679415. doi:10.3389/fneur.2021.679415
26. Nwagha UI, Ikekpeazu EJ, Ejezie FE, Neboh EE, Maduka IC. Atherogenic index of plasma as useful predictor of cardiovascular risk among postmenopausal women in Enugu, Nigeria. Afr Health Sci. 2010;10(3):248–252.
27. Fernández-Macías JC, Ochoa-Martínez AC, Varela-Silva JA, Pérez-Maldonado IN. Atherogenic Index of Plasma: novel Predictive Biomarker for Cardiovascular Illnesses. Arch Med Res. 2019;50(5):285–294. doi:10.1016/j.arcmed.2019.08.009
28. Tang Q, Li X, Song P, Xu L. Optimal cut-off values for the homeostasis model assessment of insulin resistance (HOMA-IR) and pre-diabetes screening: developments in research and prospects for the future. Drug Discov Ther. 2015;9(6):380–385. doi:10.5582/ddt.2015.01207
29. Gutch M, Kumar S, Razi SM, Gupta KK, Gupta A. Assessment of insulin sensitivity/resistance. Indian J Endocrinol Metab. 2015;19(1):160–164. doi:10.4103/2230-8210.146874
30. Mach F, Baigent C, Catapano AL, et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020;41(1):111–188. doi:10.1093/eurheartj/ehz455
31. Altuntaş Y. Postprandial Reactive Hypoglycemia. Sisli Etfal Hastan Tip Bul. 2019;53(3):215–220. doi:10.14744/SEMB.2019.59455
32. Hall M, Walicka M, Traczyk I. Hipoglikemia reaktywna jako choroba XXI wieku w ujęciu interdyscyplinarnym [Reactive hypoglycemia - an interdisciplinary approach of the disease of XXI Century]. Wiad Lek. 2020;73(2):384–389. [Polish]. doi:10.36740/WLek202002134
33. Bansal N, Weinstock RS, et al. Non-Diabetic Hypoglycemia. In: Feingold KR, Anawalt B, Boyce A, editors. Endotext. South Dartmouth (MA): MDText.com, Inc; 2020.
34. Hall M, Walicka M, Panczyk M, Traczyk I. Metabolic Parameters in Patients with Suspected Reactive Hypoglycemia. J Pers Med. 2021;11(4):276. doi:10.3390/jpm11040276
35. Lv X, Fang K, Hao W, Han Y, Yang N, Yu Q. Identification of Reactive Hypoglycemia with Different Basic BMI and Its Causes by Prolonged Oral Glucose Tolerance Test. Diabetes Metab Syndr Obes. 2020;13:4717–4726. doi:10.2147/DMSO.S280084
36. Halama A, Kahal H, Bhagwat AM, et al. Metabolic and proteomic signatures of hypoglycaemia in type 2 diabetes. Diabetes Obes Metab. 2019;21(4):909–919. doi:10.1111/dom.13602
37. Rhyu YA, Jang JY, Park S, et al. Impaired Cortisol and Growth Hormone Counterregulatory Responses among Severe Hypoglycemic Patients with Type 2 Diabetes Mellitus. Endocrinol Metab. 2019;34(2):187–194. doi:10.3803/EnM.2019.34.2.187
38. Anogeianaki A, Angelucci D, Cianchetti E, et al. Atherosclerosis: a classic inflammatory disease. Int J Immunopathol Pharmacol. 2011;24(4):817–825. doi:10.1177/039463201102400401
39. Visseren FLJ, Mach F, Smulders YM, et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J. 2021;42(34):3227–3337. doi:10.1093/eurheartj/ehab484
40. Strisciuglio T, Izzo R, Barbato E, et al. Insulin Resistance Predicts Severity of Coronary Atherosclerotic Disease in Non-Diabetic Patients. J Clin Med. 2020;9(7):2144. doi:10.3390/jcm9072144
41. Di Pino A, DeFronzo RA. Insulin Resistance and Atherosclerosis: implications for Insulin-Sensitizing Agents. Endocr Rev. 2019;40(6):1447–1467. doi:10.1210/er.2018-00141
42. Farnier M, Zeller M, Masson D, Cottin Y. Triglycerides and risk of atherosclerotic cardiovascular disease: an update. Arch Cardiovasc Dis. 2021;114(2):132–139. doi:10.1016/j.acvd.2020.11.006
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.