Back to Journals » Infection and Drug Resistance » Volume 16
Asymptomatic Malaria During Pregnancy: Prevalence, Influence on Anemia and Associated Factors in West Guji Zone, Ethiopia – A Community-Based Study
Authors Gemechu T ![]() , Dedecha W, Gelchu M
, Dedecha W, Gelchu M ![]() , Husen O, Jarso H
, Husen O, Jarso H ![]()
Received 21 August 2023
Accepted for publication 14 October 2023
Published 19 October 2023 Volume 2023:16 Pages 6747—6755
DOI https://doi.org/10.2147/IDR.S431877
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Tibeso Gemechu,1 Wako Dedecha,1 Miesa Gelchu,2 Oliyad Husen,1 Habtemu Jarso3
1Department of Medical Laboratory Science, Institute of Health, Bule Hora University, Bule Hora, Ethiopia; 2Department of Public Health, Institute of Health, Bule Hora University, Bule Hora, Ethiopia; 3Department of Public Health, School of Health Science, Madda Walabu University Shashemene Campus, Shashemene, Ethiopia
Correspondence: Tibeso Gemechu, Email [email protected]
Background: Pregnant women with asymptomatic malaria parasitemia are at increased risk of anaemia, stillbirth, miscarriage, and preterm delivery. The asymptomatic nature of the population makes diagnosis difficult, and there is generally a lack of urgency to address this specific outcome.
Objective: This study aimed to determine the prevalence of asymptomatic malaria and associated factors among pregnant women in West Guji Zone, Oromia, Ethiopia.
Methods: A community-based cross-sectional study was conducted among randomly selected 557 asymptomatic pregnant women in the West Guji Zone from February to March 2022. A standardized questionnaire was used to collect information on socio-demographic and obstetric characteristics. Approximately 2 milliliters of peripheral blood was collected for microscopy to identify species and parasite density. Epi-Data and SPSS were used for data entry and analysis respectively. Binary logistic regression was used to identify risk factors.
Results: The prevalence of malaria among asymptomatic pregnant women was 24.10% (95% CI: 20.55%-27.65%). The prevalence of Plasmodium vivax and falciparum prevalence was 73 (54.5%) and 61 (45.5%), respectively. Of the study subjects, 105 (78.4%) had mild parasitemia and 29 (21.6%) had moderate parasitemia. Pregnant women with Plasmodium infection were anaemic in two-thirds (66.5%) of cases. Living near standing water (AOR=2.6, 95% CI: 1.74– 3.96), having a history of Plasmodium species infection (AOR=2.12, 95% CI: 1.36– 3.31), not using indoor residual spraying (AOR=2.0, 95% CI: 1.32– 3.14), and not using insecticide-treated bed nets (AOR=1.62, 95% CI: 1.02– 2.55) were all factors that were significantly associated with asymptomatic infection. Pregnant women with Plasmodium infection had a significantly higher rate of anaemia than those who were not infected (OR = 6.31, p = 0.000).
Conclusion: Pregnant women had a significant prevalence of asymptomatic Plasmodium infection. Regular screening, appropriate treatment for those who test positive, and health education for pregnant women should be provided by the West Guji Zone Health Bureau.
Keywords: prevalence, asymptomatic malaria, plasmodium infection, pregnant women, anaemia, Ethiopia
A Letter to the Editor has been published for this article.
Background
Malaria is one of the aetiological factors responsible for the high incidence of anaemia during pregnancy in sub-Saharan Africa.1 Malaria in these regions of Africa is predominantly asymptomatic during pregnancy, yet it causes severe maternal anaemia and low birth weight babies. In 2020, about 13.3 million pregnant women in sub-Saharan Africa were infected with malaria and gave birth to about 961,000 newborns with low birth weight.2 Approximately 30 million women become pregnant each year in malaria-endemic areas of Africa, where the disease is most prevalent. These women and their unborn children are at risk from malaria, which can cause up to 200,000 neonatal deaths each year.3
Pregnant women in malaria-endemic areas are at greater risk of developing asymptomatic Plasmodium infection than other people.4 Depending on the endemicity of malaria in an area, 1–50% of pregnant women can be expected to carry malaria parasites, particularly in the placenta, without being aware of it.5,6 Placenta sequestration of Plasmodium falciparum is associated with low birth weight, preterm delivery, miscarriage and stillbirth in pregnant women.7
Studies from Nigeria, Ghana and Malawi reported the prevalence of asymptomatic malaria in pregnant women to be 77.6%,8 5.5%9 and 40.6%,10 respectively. In Ethiopia, the prevalence of asymptomatic malaria among pregnant women was reported from Arba Minch town (9.4%),11 North Shewa (5.7%)12 and Merti District (3.6%).13 Of all severe anaemia in pregnant women in Africa, malaria is estimated to cause 25%.14,15 Studies from India16 and Merti District13 found the prevalence of anaemia during pregnancy to be 23% and 28%, respectively. Malaria is known to destroy parasitized and non-parasitized erythrocytes resulting in haemolytic anaemia.17 Previous studies have found the following variables to be significantly associated with asymptomatic malaria in pregnant women: sex, age, ITN use and haemoglobin level.12,18
A national strategic plan for malaria prevention and control faces the challenges of asymptomatic malaria and increasing drug resistance, particularly to artemisinin-based combination therapy (ACT).19–21 Currently, WHO aims to increase access to intermittent preventive treatment with sulfadoxine-pyrimethamine (IPT-SP) for pregnant women in all areas of moderate to high malaria transmission in Africa as part of the antenatal care (ANC) service package, but these activities are not being applied to pregnant women as ANC services in Ethiopia.22 This remains a challenge for the malaria elimination programme to be effective as planned by WHO and other relevant stakeholders. Data on malaria prevalence and risk factors at institutional level are variable. However, data on asymptomatic malaria among pregnant women at the community level in general and in the current study area particularly are limited. Therefore, this study aimed to determine the prevalence of asymptomatic malaria and associated risk factors among pregnant women in West Guji Zone, Oromia, Ethiopia.
Methods and Materials
Study Area and Study Period
The study was conducted in the West Guji Zone from February to March 2022. It is one of the 21 zones in the Oromia Regional State, located in southern Ethiopia. The administrative center of the zone is the town of Bule Hora, 467 kilometres from Addis Ababa, Ethiopia’s capital. According to the census conducted by Central Statistical Agency of Ethiopia (CSA) 2007, the total population of the zone was estimated at 1,300,707 (638,648 males and 662,060 females). In terms of public health facilities, West Guji has 196 health posts, 42 health centres, and 3 public hospitals.
Study Design and Population
A community-based cross-sectional survey was conducted among pregnant women living in selected kebeles of the West Guji Zone.
Inclusion and Exclusion Criteria
This study included all pregnant women who were permanent residents of the selected kebeles in the West Guji zone, had axillary temperature below 37°C, and had no symptoms or signs of malaria. Pregnant women who had taken antimalarial medication within the previous two weeks were excluded.
Sample Size
Using a single population proportion formula, the sample size for the prevalence was calculated using the following assumptions: a prevalence of asymptomatic malaria in pregnant women of 9.4% from the Southern Ethiopia Arba Minch study,23 a 95% confidence interval, and a 5% margin of error. This gave a sample size of 132 for the prevalence objective. The sample size for the second objective was calculated using the double population proportion formula in Epi-Info Version 7 StatCalc. The sample size calculation for the second objective used 80% power and a 95% confidence interval (CI). The sample size was estimated using factors associated with asymptomatic malaria from previous studies such as parity, haemoglobin, and ITN use.12,23 The maximum calculated sample size was 337, which was larger than the sample size calculated for the first objective. By adding 10% non-response, the sample size became 371. To account for the design effect, the sample size obtained was multiplied by 1.5, resulting in a final sample size of 563 (Table 1).
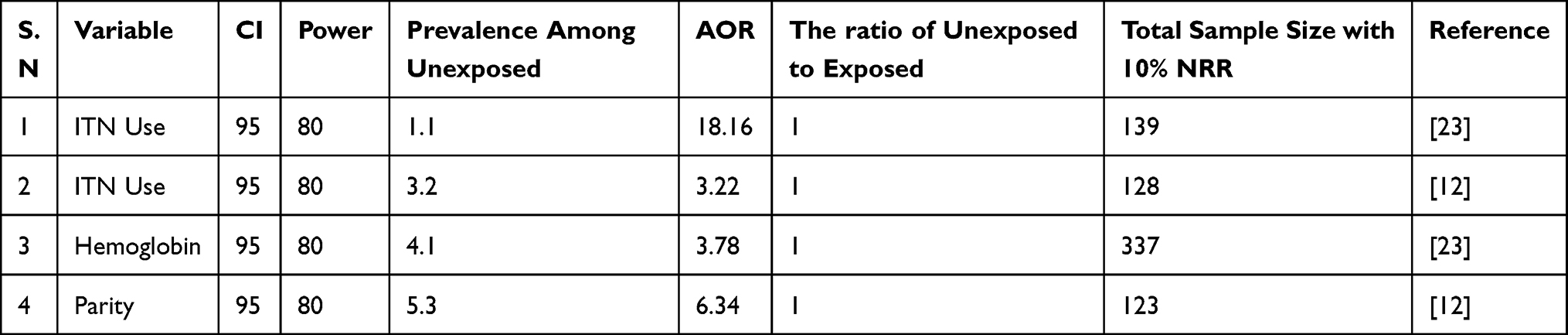 |
Table 1 Sample Size Determination for the Second Objective |
Sampling Technique
Three districts, Duda Dawa, Melka Soda, and Galana, were purposively selected from the malaria area of West Guji Zone. Nine kebeles (the smallest administrative unit in Ethiopia) were randomly selected from the three selected malaria districts using a simple random sampling technique (lottery method). As there were slightly fewer pregnant women (N=557) in the kebele than the sample size (563) predicted, all pregnant women in the selected kebeles were included in the study. The distribution of pregnant women in the selected kebeles was as follows Q/Misoma (N=74), Mad/Fincawa (N=55), Bur/Magada (N=62), Soda Garmama (N=68), Hidi Nagelle (N=57), Baya Gundi (N=43), Medhiba (N=70), Didole Harra (N=75), and Welene Bokosa (53).
Variables
Dependent variables
Prevalence of asymptomatic malaria in pregnant women.
Prevalence of anemia in asymptomatic malaria cases.
Independent Variables
Age, educational level, ITN, marital status, occupation, indoor residual spraying (IRS), ANC attendance, distance from stagnant water, previous history of malaria infection.
Data Collection and Laboratory Processing
Pregnant women who gave their consent allowed their blood samples to be taken by a laboratory technician (BSc), which were then labelled, stored in cool boxes, and taken to the laboratory for analysis. Pregnant women with asymptomatic malaria parasitemia were diagnosed using RDT (Carestart TM Malaria Pf/Pv (HRP2/PLDH) Ag Combo RDT) and Giemsa-stained blood smear microscopy. The number of parasites per 200 white blood cells on a thick blood smear was counted to determine the asexual parasite density per microlitre (l) of blood, assuming a standard total white blood cell (WBC) count of 8000/l. The degree of parasite density was classified as mild when the parasite count was between 1–999 parasites/μL, moderate when the parasite count was between 1000–9999/μL, and severe when the count was >10,000/μL respectively.24,25 A complete blood count was performed to diagnose anaemia. For haemoglobin, the WHO cut-off value of 11 g/dL for pregnant women was used as the cut-off value indicating anaemia.26
Quality Assurance
The structured questionnaire was first drafted in English and then translated into the local languages (Amharic and Afan Oromo). Prior to actual data was collected, the questionnaire was pre-tested and updated on 5% of the total sample size in the Suro District. Data collectors were trained prior to actual data collection. The researchers checked the accuracy and consistency of the data before data analysis. Microscopic slides were examined by two qualified laboratory technicians. Before a negative conclusion was reached, 100 microscopic fields of the smear were examined. A third senior parasitologist resolved disagreements between the first and second readings. The RDTs were used according to the manufacturer’s recommendations. The readers of the smear microscopy were blinded to the results of the RDTs.
The laboratory staff who performed the RDTs and light microscopy were trained in quality assurance and malaria diagnosis. The rapid test kits were checked for the expiration date, appropriate collection methods, and the presence of built-in controls.
Data Analysis
Data were coded, entered into Epidata version 3.1, cleaned up, and analyzed using SPSS for Windows version 25. Both descriptive and inferential statistics were used to analyze the data. Frequencies and summary statistics such as means, standard deviations and percentages were generated to describe the study population in terms of the relevant variables. Binary logistic regression analysis was used to assess the degree of association between the dependent and independent variables.
Those variables that showed a significant association in the bivariate analysis (p-value < 0.25) were subjected to multivariable analysis. The backward stepwise method was used. The adjusted odds ratio (AOR) was used to report the strength of the association, and a p-value less than 0.05 was used to determine significance.
Operational Definition
- Asymptomatic malaria: Presence of malaria without clinical signs and symptoms among pregnant women.
- Parasitemia: The presence of malaria parasites in the blood.
- Sequestration: Movement of P. falciparum-infected red blood cells into small vessel walls and capillaries to avoid clearance by the spleen.
- Anaemia: a decrease in red blood cells.
- History of Plasmodium infection: Previous infection with the Plasmodium parasite in the last three years.
- Not using ITN: Pregnant women who have not used ITN at all during the data collection.
- Not using indoor residual spraying: Those pregnant women who did not use indoor residual spraying at all during the data collection.
- Living near stagnant water: This is the distance that female Anopheles mosquitoes walk or fly from the breeding site or stagnant water. We used the maximum distance of two kilometres from stagnant water as close. A flight distance of 1 to 1.5 km for Anopheles arabieinsis and 661 m for A. gambiensis and A. funestus is supported by studies.27,28
- ANC attendance: is the follow-up that women should have after their pregnancy.
Results
Socio-Demographic Characteristics of Study Participants
A total of 557 pregnant women from three selected malaria districts in the West Guji Zone were enrolled in the study. The mean age of the participants was 28 years with a standard deviation of 10.85 years. The majority of participants (33.9%) were in the age group of 21–25 years. All study participants were married. The largest proportion of study participants had a primary education (39%) followed by a secondary education (34.5%). In terms of employment status, 91.2% were unemployed. Approximately 25.5% of the study participants lived in urban areas. More than two thirds (69.8%) of the study participants were in the second trimester of pregnancy. The majority (64.5%) of study participants had no ANC follow-up (Table 2).
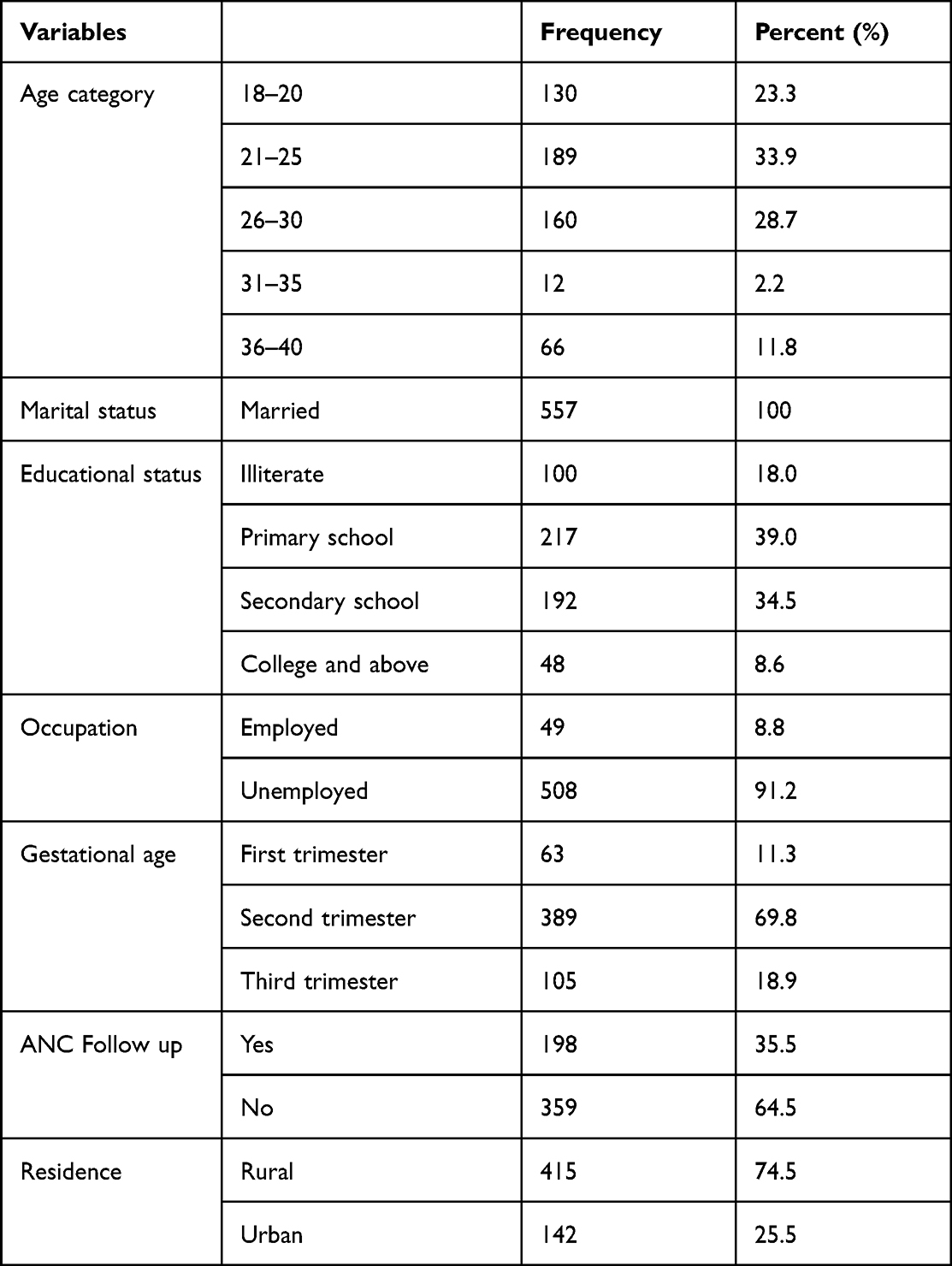 |
Table 2 Distribution of Socio-Demographic and Obstetric Characteristics of Pregnant Women |
Prevalence of Malaria in Pregnant Women
Of 557 asymptomatic pregnant women enrolled in the study, 134 (24.1%) were positive for Plasmodium species. A similar result was obtained by both RDT (Carestart TM Malaria Pf/Pv (HRP2/PLDH)) and Giemsa-stained smear microscopy. The most common parasite found was Plasmodium vivax 73 (54.5%), followed by Plasmodium falciparum 61 (45.5%). The majority of pregnant women (78.4%) had mild parasitemia, while 21.6% had moderate parasitemia for Plasmodium parasites.
Prevalence of Anaemia in Pregnant Women
The prevalence of anaemia among pregnant women was 190 (34.1%). Two thirds (66.4%) of the pregnant women who tested positive for Plasmodium species had anaemia. However, only almost a quarter (23.9%) of pregnant women who tested negative for Plasmodium species had anaemia. The difference in the prevalence of anaemia between Plasmodium positive and negative women is statistically significant (p <0.001).
Factors Associated with Asymptomatic Malaria in Pregnant Women
Of the variables assessed, living near stagnant water, having a history of Plasmodium species infection, not using indoor residual spraying and not using insecticide-treated bed nets were variables significantly associated with asymptomatic Plasmodium infection (API) (Table 3).
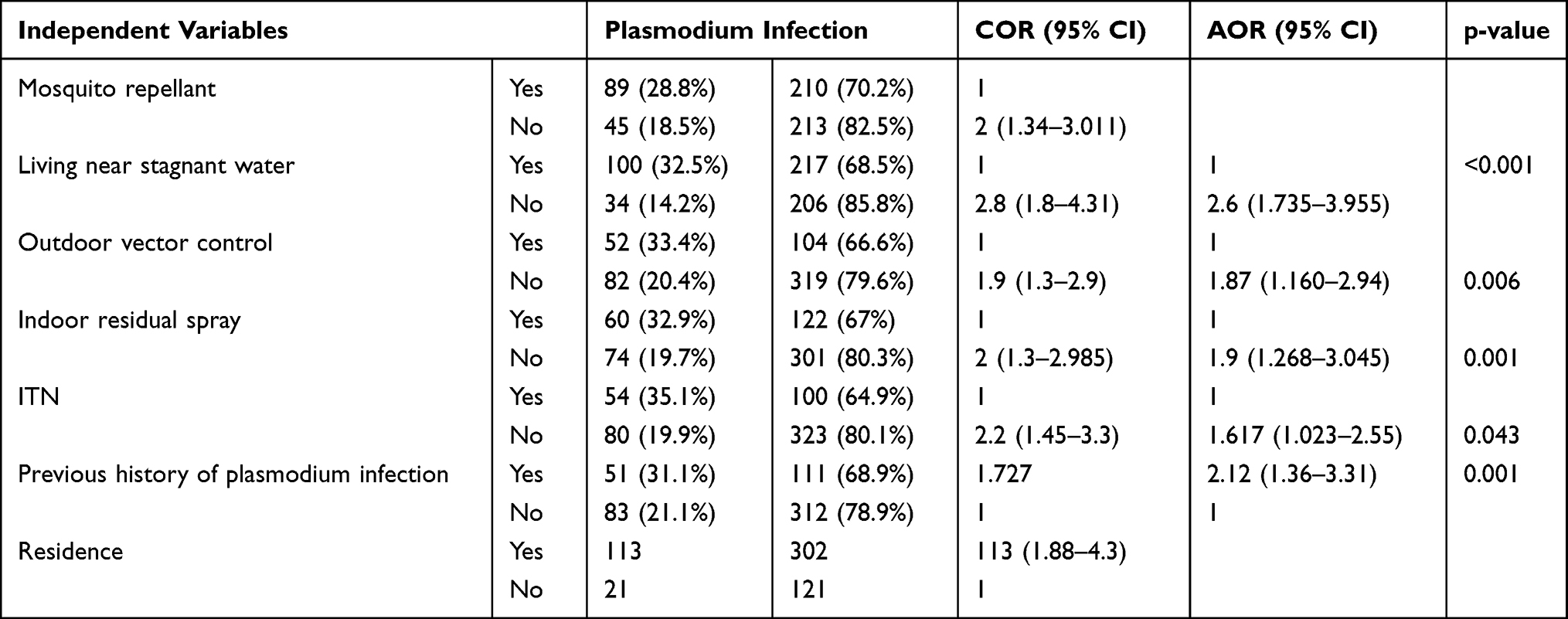 |
Table 3 Factors Associated with Asymptomatic Malaria Among Pregnant Women |
Discussion
The prevalence of asymptomatic Plasmodium infection in the current study was 24.1% by both Giemsa-stained blood smear microscopy and RDT (Carestart TM Malaria Pf/Pv (HRP2/PLDH)). This finding is consistent with other studies in Nigeria (22.4–22.7%).1,29 On the other hand, the finding of the current study was higher compared to studies in Republic of Congo (7%),30 Colombia (4.2%),31 Arba Minch, Ethiopia (9.1%),11 Bangladesh (2.3%)32 and Merti district, Ethiopia (3.6%).13 The higher prevalence of asymptomatic parasitemia among pregnant women found in this study may be due to the fact that the current investigation was conducted during a significant malaria transmission season and the study area of the present study is one of the high malaria transmission areas in Ethiopia. In a high malaria transmission area, individuals frequently exposed to malaria develop protective immunity that renders Plasmodium infection asymptomatic.11 In addition, all malaria areas, including Ethiopia, are currently experiencing an increase in malaria cases and transmission.2 On the other hand, our result was lower compared to studies in Colombia (79%) and Venezuela (71.2%).33,34 The discrepancy in results could be due to differences in malaria control strategies, sample size, altitude and temperature.35
In the current study, the prevalence of P. vivax (54.5%) is higher than that of P. falciparum (45.5%). This may be due to the relapsing behavior of the parasite, which makes the infected person a carrier for life, unless the patient takes primaquine, which is not currently used in Ethiopia. On the other hand, resistance to P.vivax for Chloroquine may be emerging. In addition, the higher prevalence of P.vivax than P. Falciparum has been reported in other similar studies in Africa, including Ethiopia.18,36
Factors identified in the current study as being associated with asymptomatic Plasmodium infections (API) in the study area included use of ITNs, indoor residual spraying, history of Plasmodium infection, and living near vector breeding sites. Compared with pregnant women who used ITNs, those who did not use were 1.6 times more likely to develop API. This finding is similar to reports from Nigeria29 and southern Ethiopia.11
In the current study, we observed some people using ITNs to temporarily store grain in the house. Educating pregnant mothers about the importance of using ITNs is important in reducing malaria transmission.
Living near stagnant water is another factor significantly associated with the prevalence of asymptomatic Plasmodium infection (API). Compared with pregnant women living far from vector breeding sites, those living close to them had a 2.6 times higher risk of having API. Studies conducted in the Merti district13 and Arbaminch11 support this finding.
Another factor that was significantly associated with asymptomatic plasmodium infections was indoor residual spraying (IRS). Compared to women who used an IRS in their home, pregnant women who did not use an IRS had twice the risk of developing Plasmodium parasitemia. Finally, asymptomatic Plasmodium infection is highly correlated with a history of Plasmodium parasitemia. Compared with women who had never had malaria, pregnant women with a history of Plasmodium infection were twice as likely to develop API. This finding is consistent with a previous study conducted in Merti District where there was a significant association between API and a history of malaria.13 This may be due to the relapsing behavior of Plasmodium vivax and the recrudescence behavior of P. falciparum, where the parasite is likely to be present in the blood after apparent cure.37
Asymptomatic Plasmodium infection is a major cause of anaemia in areas where malaria is endemic. The new findings also show that maternal anaemia can be significantly worsened by Plasmodium infection in pregnant women. Pregnant women with anaemia have been associated with asymptomatic Plasmodium infection in other studies from the Merti district13 and India.16 In this study, 34.1% of all pregnant women had anaemia, which is higher than the percentages found in studies from India (23%)16 and Merti district (28.0%).13 However, it is lower than that reported in Nigeria (38.85%). Of the pregnant women who tested positive for Plasmodium species, 66.4% were anaemic. This finding is lower compared to a study in Merti District (92.3%).13 The difference may be due to the different in sample sizes used. The current study examined approximately 557 pregnant women, which is larger than the 364 sample size used in the Merti District. Anemia may not depend on API alone, as other causes such as malnutrition,38 Helminthiasis,39 and other variables may also have significant contributions, although Plasmodium infection during pregnancy contributes more to anaemia.
Limitation of the Study
The current study is cross-sectional and cannot distinguish between cause and effect. We also omitted the PCR molecular test for the Plasmodium parasite due to lack of resources.
Conclusion
The prevalence of asymptomatic Plasmodium infection and anaemia during pregnancy is high in the study area. Living near standing water, having a history of Plasmodium species infection, not using indoor residual spraying, and not using insecticide-treated bed nets (AOR=1.62, 95% CI: 1.02–2.55) were all factors that were significantly associated with asymptomatic Plasmodium infection. Regular screening, appropriate treatment of those who test positive, and management of asymptomatic Plasmodium infection in the study area are needed. Further study should be done using highly sensitive and specific test (molecular technique) to identify the exact prevalence of asymptomatic malaria in the study area.
Abbreviation
BHU, Bule Hora University; ART, Artemisinin-based Combination Therapy; OR, Odd ratio; SSA, Sub-Sahara African; WHO: World Health Organization; ANC, Antenatal Care; EDTA, Ethylene Diamine Tetra Acetic Acid; RDT, Rapid Diagnostic Test; ITN, Insecticide Treated Nets; LBW, Low Birth Weight; IRS, indoor residual spray; API, asymptomatic plasmodium infection.
Data Sharing Statement
All necessary data sets on which the conclusion of this paper is based are included in the manuscript.
Ethical Approval
The study protocol was approved by the Ethical Review Board (IRB) of Bule Hora University. The study was conducted in accordance with Helsinki Declaration. All study participants gave written, informed consent. For those under the age of 18, their husbands gave written informed consent, and the participants gave their assent. Each study participant’s information was kept confidential and used only for research purposes. Lab test results were also kept confidential. The results of participants with parasitic infections were reported to the study participants. The pregnant women who tested positive for the Plasmodium parasite were referred to the ANCs in the surrounding health facilities for treatment and medical advice, and then followed up to ensure proper treatment.
Acknowledgment
First of all, we would like to thank Bule Hora University for funding this research. We would also like to thank the Municipality of Bule Hora for their assistance in collecting the sample. Finally, we would like to thank the participants for their willingness to participate in the study.
Author Contributions
All authors have made a substantial contribution to the work reported, be it in the conception, design, conduct, collection, analysis, and interpretation of data, or in all these areas; have been involved in drafting, revising, or critically reviewing the article; have given final approval for the version to be published; have agreed on the journal to which the article will be submitted; and agree to take responsibility for all aspects of the work.
Funding
Funding has been received for this paper from the Bule Hora University (grant number 6223).
Disclosure
The authors have no competing interests in this work and no competing interests in any activities related to this research. The funder was not involved in manuscript writing, editing, approval, or decision to publish.
References
1. Ogbu GI, Aimakhu CO, Anzaku SA, Ngwan S, Ogbu DA. Prevalence of malaria parasitaemia among asymptomatic women at booking visit in a tertiary hospital, North-central Nigeria. Circulation. 2015;2(29):34–36.
2. World Health Organization. World Malaria Report 2022. World Health Organization; 2022.
3. Liu L, Johnson HL, Cousens S, et al. Global, regional, and national causes of child mortality: an updated systematic analysis for 2010 with time trends since 2000. The Lancet. 2012;379(9832):2151–2161. doi:10.1016/S0140-6736(12)60560-1
4. Gajida A, Iliyasu Z, Zoakah A. Malaria among antenatal clients attending primary health care facilities in Kano state, Nigeria. Ann Afr Med. 2010;9(3). doi:10.4103/1596-3519.68352
5. Brabin BJ. An analysis of malaria in pregnancy in Africa. Bull World Health Organ. 1983;61(6):1005.
6. Steketee RW, Nahlen BL, Parise ME, Menendez C. The burden of malaria in pregnancy in malaria-endemic areas. Am J Trop Med Hyg. 2001;64(1_suppl):28–35. doi:10.4269/ajtmh.2001.64.28
7. Bauserman M, Conroy AL, North K, Patterson J, Bose C, Meshnick S. An overview of malaria in pregnancy. In: Seminars in Perinatology. Elsevier; 2019.
8. Igwe NM, Joannes UOU, Chukwuma OB, et al. Prevalence and parasite density of asymptomatic malaria parasitemia among unbooked paturients at Abakaliki, Nigeria. J Basic Clin Rep Sci. 2014;3(1):44–48. doi:10.4103/2278-960X.129279
9. Laube W, Awo MA, Derbile EK. Smallholder integration into the global shea nut commodity chain in northern Ghana. ZEF Working Paper Series; 2017.
10. Keskinen J. Effect of environmental factors on the prevalence of submicroscopic malaria among Malawian pregnant women; 2017.
11. Nega D, Dana D, Tefera T, Eshetu T, Luty AJF. Prevalence and predictors of asymptomatic malaria parasitemia among pregnant women in the rural surroundings of Arbaminch Town, South Ethiopia. PLoS One. 2015;10(4):e0123630. doi:10.1371/journal.pone.0123630
12. Feleke DG, Adamu A, Gebreweld A, Tesfaye M, Demisiss W, Molla G. Asymptomatic malaria infection among pregnant women attending antenatal care in malaria endemic areas of North-Shoa, Ethiopia: a cross-sectional study. Malar J. 2020;19(1):1–6. doi:10.1186/s12936-020-3152-9
13. Subussa BW, Eshetu T, Degefa T, Ali MM. Asymptomatic Plasmodium infection and associated factors among pregnant women in the Merti district, Oromia, Ethiopia. PLoS One. 2021;16(3):e0248074. doi:10.1371/journal.pone.0248074
14. Schantz-Dunn J, Nour NM. Malaria and pregnancy: a global health perspective. Rev Obstet Gynecol. 2009;2(3):186.
15. Desai M, ter Kuile FO, Nosten F, et al. Epidemiology and burden of malaria in pregnancy. Lancet Infect Dis. 2007;7(2):93–104. doi:10.1016/S1473-3099(07)70021-X
16. Corrêa G, Das M, Kovelamudi R, et al. High burden of malaria and anemia among tribal pregnant women in a chronic conflict corridor in India. Confl Health. 2017;11:1–9. doi:10.1186/s13031-017-0113-1
17. Haldar K, Mohandas N. Malaria, erythrocytic infection, and anemia. ASH Educ Prog Book. 2009;2009(1):87–93.
18. Golassa L, Baliraine FN, Enweji N, Erko B, Swedberg G, Aseffa A. Microscopic and molecular evidence of the presence of asymptomatic Plasmodium falciparum and Plasmodium vivax infections in an area with low, seasonal and unstable malaria transmission in Ethiopia. BMC Infect Dis. 2015;15(1):310. doi:10.1186/s12879-015-1070-1
19. Bottius E, Guanzirolli A, Trape J-F, Rogier C, Konate L, Druilhe P. Malaria: even more chronic in nature than previously thought; evidence for subpatent parasitaemia detectable by the polymerase chain reaction. Trans R Soc Trop Med Hyg. 1996;90(1):15–19. doi:10.1016/S0035-9203(96)90463-0
20. Oladipo HJ, Tajudeen YA, Oladunjoye IO, et al. Increasing challenges of malaria control in sub-Saharan Africa: priorities for public health research and policymakers. Anna Med Surg. 2022;81:104366. doi:10.1016/j.amsu.2022.104366
21. Golassa L, Enweji N, Erko B, Aseffa A, Swedberg G. Detection of a substantial number of sub-microscopic Plasmodium falciparum infections by polymerase chain reaction: a potential threat to malaria control and diagnosis in Ethiopia. Malar J. 2013;12:1–10. doi:10.1186/1475-2875-12-352
22. World Health Organization. WHO Policy Brief for the Implementation of Intermittent Preventive Treatment of Malaria in Pregnancy Using Sulfadoxine-Pyrimethamine (Iptp-SP). Geneva: World Health Organization; 2013.
23. Ngasala BE, Kihamia CM. Prevalence of asymptomatic malaria infection and use of different malaria control measures among primary school children in Morogoro Municipality, Tanzania. Malar J. 2015;14:1–7. doi:10.1186/1475-2875-14-1
24. Nwagha UI, Ugwu VO, Nwagha TU, Anyaehie BU. Asymptomatic plasmodium parasitaemia in pregnant Nigerian women: almost a decade after roll back malaria. Trans R Soc Trop Med Hyg. 2009;103(1):16–20. doi:10.1016/j.trstmh.2008.07.016
25. McKenzie FE, Prudhomme WA, Magill AJ, et al. White blood cell counts and malaria. J Infect Dis. 2005;192(2):323–330. doi:10.1086/431152
26. World Health Organization. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity. World Health Organization; 2011.
27. Braack L, Coetzee M, Hunt R, Biggs H, Cornel A, Gericke A. Biting pattern and host-seeking behavior of Anopheles arabiensis (Diptera: culicidae) in northeastern South Africa. J Med Entomol. 1994;31(3):333–339. doi:10.1093/jmedent/31.3.333
28. Midega JT, Mbogo CM, Mwambi H, et al. Estimating dispersal and survival of Anopheles gambiae and Anopheles funestus along the Kenyan coast by using mark–release–recapture methods. J Med Entomol. 2007;44(6):923–929. doi:10.1093/jmedent/44.6.923
29. Emiasegen SE, Giwa FJ, Ajumobi O, Ajayi IO, Ahmed SA, Olayinka AT. Asymptomatic Plasmodium falciparum parasitaemia among pregnant women: a health facility based survey in Nassarawa-Eggon, Nigeria. Malaria World J. 2017;8:8.
30. Francine N, Damien B, Anna F, Michael K, Christevy VJ, Felix -K-K. Characterization of asymptomatic Plasmodium falciparum infection and its risk factors in pregnant women from the Republic of Congo. Acta Trop. 2016;153:111–115. doi:10.1016/j.actatropica.2015.10.009
31. Vásquez A-M, Zuluaga-Idárraga L, Arboleda M, et al. Malaria in pregnancy in endemic regions of Colombia: high frequency of asymptomatic and peri-urban infections in pregnant women with malaria. Infect Dis Obstet Gynecol. 2020;2020:1–10. doi:10.1155/2020/2750258
32. Khan WA, Galagan SR, Prue CS, et al. Asymptomatic Plasmodium falciparum malaria in pregnant women in the Chittagong Hill Districts of Bangladesh. PLoS One. 2014;9(5):e98442. doi:10.1371/journal.pone.0098442
33. Arango EM, Samuel R, Agudelo OM, Carmona-Fonseca J, Maestre A, Yanow SK. Molecular detection of malaria at delivery reveals a high frequency of submicroscopic infections and associated placental damage in pregnant women from northwest Colombia. Am J Trop Med Hyg. 2013;89(1):178. doi:10.4269/ajtmh.12-0669
34. Romero M, Leiba E, Carrión-Nessi FS, et al. Malaria in pregnancy complications in Southern Venezuela. Malar J. 2021;20:1–8. doi:10.1186/s12936-021-03728-9
35. Tegegne Y, Asmelash D, Ambachew S, Eshetie S, Addisu A, Jejaw Zeleke A. The prevalence of malaria among pregnant women in Ethiopia: a systematic review and meta-analysis. J Parasitol Res. 2019;2019. doi:10.1155/2019/8396091
36. Twohig KA, Pfeffer DA, Baird JK, et al. Growing evidence of Plasmodium vivax across malaria-endemic Africa. PLoS Negl Trop Dis. 2019;13(1):e0007140. doi:10.1371/journal.pntd.0007140
37. de Deus Vieira G, Gim KNM, Zaqueo GM, et al. Reduction of incidence and relapse or recrudescence cases of malaria in the western region of the Brazilian Amazon. J Infec Dev Count. 2014;8(09):1181–1187. doi:10.3855/jidc.4422
38. Lubis Z, Jumirah J, Fitria M. Chronic energy malnutrition and anemia in pregnant women in medan.
39. Molla E, Mamo H. Soil-transmitted helminth infections, anemia and undernutrition among schoolchildren in Yirgacheffee, South Ethiopia. BMC Res Notes. 2018;11(1):1–7. doi:10.1186/s13104-018-3679-9
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.