Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 14
Asymptomatic Hyperuricemia and Metabolically Unhealthy Obesity: A Cross-Sectional Analysis in the Tianning Cohort
Authors Yu J ![]() , Sun H, Zhu J, Wei X, Shi H, Shen B, Ren L, He Y, Zhang R, Zhang M
, Sun H, Zhu J, Wei X, Shi H, Shen B, Ren L, He Y, Zhang R, Zhang M ![]() , Peng H
, Peng H ![]()
Received 14 January 2021
Accepted for publication 10 March 2021
Published 25 March 2021 Volume 2021:14 Pages 1367—1374
DOI https://doi.org/10.2147/DMSO.S301363
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Jia Yu,1,* Hongyan Sun,2,* Jinhua Zhu,3,* Xintong Wei,1 Hongfei Shi,2 Bin Shen,3 Liyun Ren,1 Yan He,1 Rongyan Zhang,3 Mingzhi Zhang,1 Hao Peng1,4
1Department of Epidemiology, School of Public Health, Medical College of Soochow University, Suzhou, People’s Republic of China; 2Center for Disease Prevention and Control of Tianning District, Changzhou, People’s Republic of China; 3Center for Disease Prevention and Control of Wujiang District, Suzhou, People’s Republic of China; 4Jiangsu Key Laboratory of Preventive and Translational Medicine for Geriatric Diseases, Soochow University, Suzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hao Peng
Department of Epidemiology, School of Public Health, Medical College of Soochow University, 199 Renai Road, Industrial Park, Suzhou, 215123, People’s Republic of China
Tel +86 512 6588 0078
Fax +86 512 6588 0052
Email [email protected]
Objective: The relationship between obesity and hyperuricemia has been demonstrated by many studies. However, whether or to what extent metabolic condition influents the association between obesity and hyperuricemia was not clear. Here, we aimed to examine the association between obese-metabolic phenotype and hyperuricemia in a large sample of Chinese adults.
Methods: According to BMI and metabolic syndrome, obese-metabolic phenotype was defined as metabolically unhealthy obesity (MUO), metabolically healthy obesity (MHO), metabolically unhealthy non-obesity (MUNO) and metabolically healthy non-obesity (MHNO)in the Tianning cohort (N=5072). We conducted a cross-sectional analysis between obese-metabolic phenotype and hyperuricemia, followed by a Mendelian Randomization analysis using GWAS summary data to confirm the causality between uric acid and BMI.
Results: The average level of serum UA showed 41.87-higher μmol/L in participants with MHO (β=41.87, P< 0.001) and 63.18-higher μmol/L in participants with MUO (β=63.18, P< 0.001), compared to those with MHNO. Compared to participants with MHNO, those with MUO had the highest likelihood to have hyperuricemia (OR=4.56, P< 0.001), followed by those with MHO (OR=3.32, P< 0.001). Mendelian randomization analysis indicated that uric acid was more likely to be a consequence of BMI (β=0.059, P=6.54× 10− 154).
Conclusion: MUO, in comparison with MHO, was significantly associated with hyperuricemia in Chinese adults.
Keywords: metabolic syndrome, obesity, serum uric acid, hyperuricemia
Introduction
Asymptomatic hyperuricemia is considered a benign laboratory finding with little clinical relevance in the absence of gout or nephrolithiasis in clinical practice but a good predictor of risks of hypertension, diabetes, gout, chronic kidney disease (CKD), and cardiovascular disease (CVD).1 It affects nearly 13.3% of the general population in China and is double prevalent among those with obesity,2,3 which is very popular worldwide and a major contributor to morbidity and mortality of CVD.4–6 The relationship between obesity and serum uric acid (UA) has been demonstrated by substantial evidence. For example, UA could be produced and secreted by adipose tissue7 and was elevated in high-fat diet-induced obese mice.8 In humans, an obesity-related genetic variant (rs545854) was associated with serum UA levels and the susceptibility to hyperuricemia.9 Obesity at childhood was associated with an elevated level of serum UA at young adulthood.10 However, the precise mechanisms contributing to elevation of uric acid in individuals with obesity are not very clear.7 Metabolic adaptations may occur in our body in response to obesity11 and the altered metabolic states have been considered to play important roles in diverse aspects of health, eg, inflammation, insulin resistance, oxidative stress, and purine metabolism.12–15 Metabolic states may, therefore, affect the contribution of excessive adipose to UA production and secretion. Indeed, about 10–30% of obese individuals have normal blood pressure, blood lipids, and fasting glucose, all indicate a relatively healthy metabolic status.16–19 Individuals with metabolically healthy obesity (MHO), a subset of obesity, have relatively lower metabolic and cardiovascular risks despite the presence of excessive fat mass than other obese ones, those with metabolically unhealthy obesity (MUO) in particular.17,20 However, the association between MUO, in comparison to MHO, and hyperuricemia has not been well studied, although some studies reported an association between general obesity and hyperuricemia.21,22 Whether or to what extent metabolic condition influents the association between obesity and hyperuricemia was not clear. Therefore, we aimed to examine the association between asymptomatic hyperuricemia and MUO in more than five thousand Chinese adults in Tianning cohort. We also examined the causality between obesity and hyperuricemia by Mendelian randomization analysis using GWAS summary data.
Method
The methods of participant’s selection and data collection were detailed in the Supplementary Materials and briefly described below.
Study Participants
The protocols of the Tianning Cohort study were approved by the Ethics Committee of Soochow University (approval No. ECSU-201800051) and described in detail elsewhere.23 This study was conducted following the Declaration of Helsinki. In brief, a total of 5199 Chinese adults were included in 2018, after giving a signed written informed consent. After excluding participants with missing data on either BMI or metabolic syndrome components (N=127), a total of 5072 participants were included in the final analysis. All participants were free of diagnosed gout.
Data Collection
Data on demographic information (age, sex), social-economic statues (education level), lifestyle risk factors (cigarette smoking, alcohol consumption, physical activity, sleep quality), and personal medical history were gathered applying standard questionnaires in the Chinese language administered by trained staff. Physical examinations including body weight, height, waist circumference, and blood pressures were performed by physicians according to standard protocols. Biochemical markers including serum UA and creatinine were measured using commercial reagents (Siemens Healthcare Diagnostic Inc., Co Antrim, UK). The estimated glomerular filtration rate (eGFR) was used to assess kidney function. Asymptomatic hyperuricemia was commonly diagnosed as serum UA above 420 μmol/L (7.0 mg/dl) for men and above 360 μmol/L (6.0 mg/dl) for women. This definition has been widely used in prior studies.24
Definition of Metabolically Healthy and Unhealthy Obesity
Typically, metabolic disorders included increased blood pressure, dyslipidemia, hyperglycemia, and central obesity, according to the Joint Interim Statement of the International Diabetes Federation Task Force on Epidemiology and Prevention.25 The definitions of each metabolic disorder were described in Supplementary Table S1. Body mass index (BMI) was calculated by dividing weight in kilograms by the square of height in meters (kg/m2). Obesity was diagnosed as BMI≥28 kg/m2.26 Obese participants with ≥3 of 5 metabolic disorders were defined as MUO and those with less than 3 metabolic disorders were treated as MHO. Non-obese participants with ≥3 of 5 metabolic disorders were defined as metabolically unhealthy non-obesity (MUNO) and those with less than 3 metabolic disorders were treated as metabolically healthy non-obesity (MHNO).
Statistical Analysis
Characteristics were presented in participants with MUO, MHO, MUNO and MHNO, respectively. To examine the association between serum UA and obesity status, we constructed a linear regression model in which serum UA was the dependent variable and obesity status (MUO vs MHO vs MUNO vs MHNO as a reference) was the independent variable, adjusting for age, sex, education level, cigarette smoking, alcohol consumption, eGFR, physical activity, and sleep quality. To facilitate data interpretation, a logistic regression model was similarly constructed to examine the association between obesity status and prevalent hyperuricemia. To examine whether and to what extent metabolic states modify the association between BMI and hyperuricemia, we performed subgroup analysis by metabolic states and tested the heterogeneity by introducing an interaction term of BMI×metabolic states. To examine whether the results differed between genders, we separately conduced sex-specific association of obesity types with SUA and hyperuricemia. To examine whether CKD or CVD influent our results, participants with prevalent CKD or CVD were excluded. All statistical analyses were conducted using SAS statistical software, version 9.4 (SAS Institute, Cary, NC). A two-tailed P-value less than 0.05 was considered statistically significant.
Mendelian Randomization Analysis
To further clarify the causal association between obesity and hyperuricemia, we conducted a Mendelian Randomization analysis using summary data from genome-wide association studies (GWAS). Generalized Summary-data-based Mendelian Randomization (GSMR) method27 was implemented in GCTA using the GWAS datasets of BMI and UA.28 The GWAS data of serum UA was extracted from the CKDGen Consortium (http://ckdgen.imbi.uni-freiburg.de).29
Result
Baseline Characteristics
A total of 5072 participants (mean age 51.0±15.6 years, ranged from 18 to 96 years, 41.42% men) were included in our study. Of them, 617 (12.16%) participants were obese including 195 individuals with MHO and 422 individuals with MUO. Their baseline characteristics are shown in Table 1. The average level of serum UA in participants with MUO was 392±94 μmol/L which was significantly higher than that in participants with MHO (364±93μmol/L), MUNO (354±89μmol/L) and MHNO (317±82μmol/L). As expected, almost all characteristics inducing demographics, lifestyles, and metabolic factors were differentially distributed among the four obese-metabolic states (all P<0.05). Notably, compared with participants with MHO, those with MUO seemed to be older, current drinkers, hypertensive, diabetic have higher levels of blood pressure, lipids, and lower eGFR (all P<0.05).
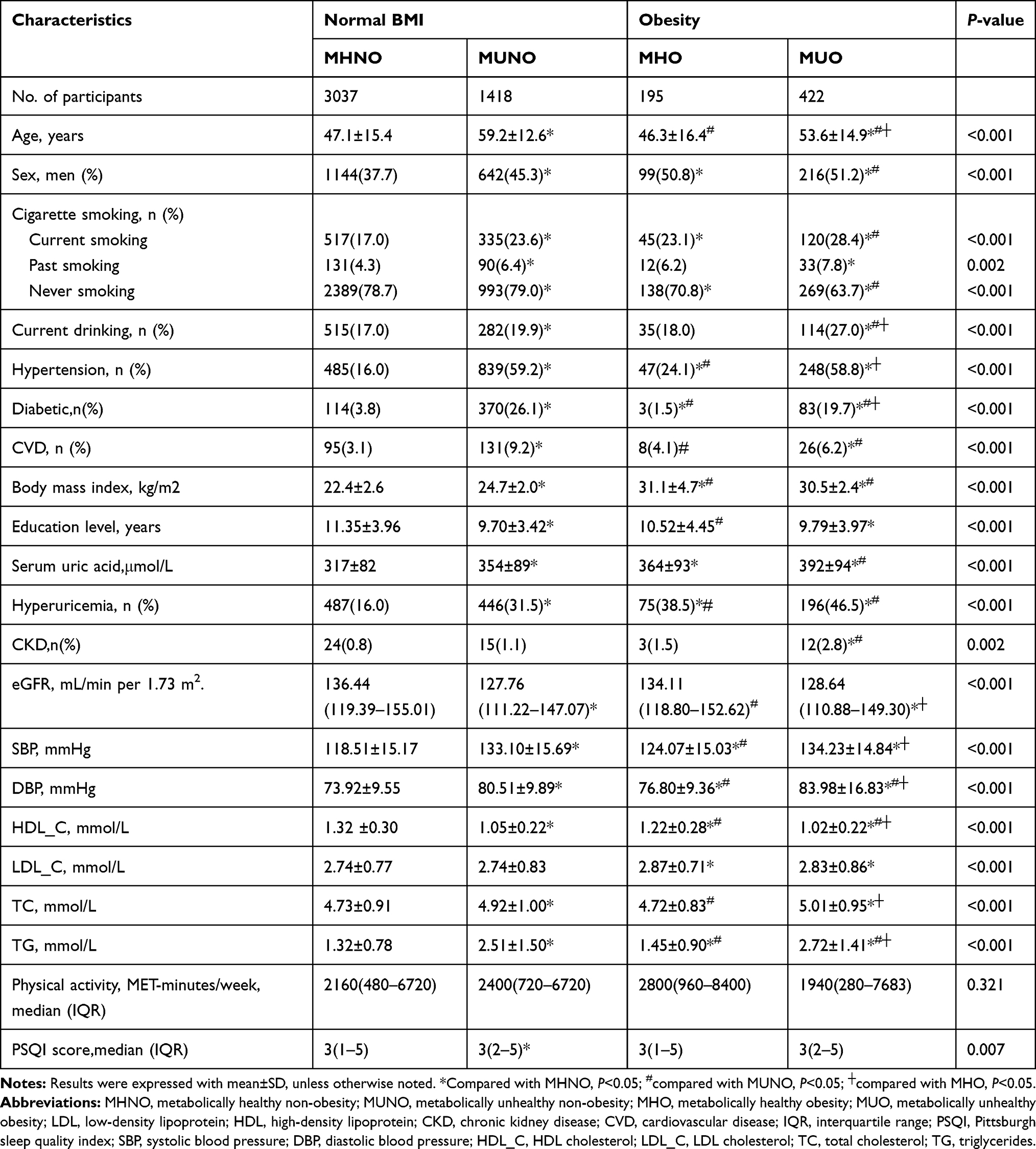 |
Table 1 Baseline Characteristics of Study Participants According to Obesity Status |
Association Between MUO and Hyperuricemia
Table 2 shows the associations of obese-metabolic status with serum UA and hyperuricemia. After adjusting for age, sex, education level, cigarette smoking, alcohol consumption, eGFR, physical activity, and sleep quality, the average level of serum UA showed 41.87-higher μmol/L in participants with MHO (β=41.87, P<0.001) and 63.18-higher μmol/L in participants with MUO (β=63.18, P<0.001), compared to those with MHNO. The risks of prevalent hyperuricemia were similarly distributed among the three groups. Compared to participants with MHNO, those with MUO had the highest likelihood to have hyperuricemia (OR=4.56, P<0.001), followed by those with MHO (OR=3.32, P<0.001).
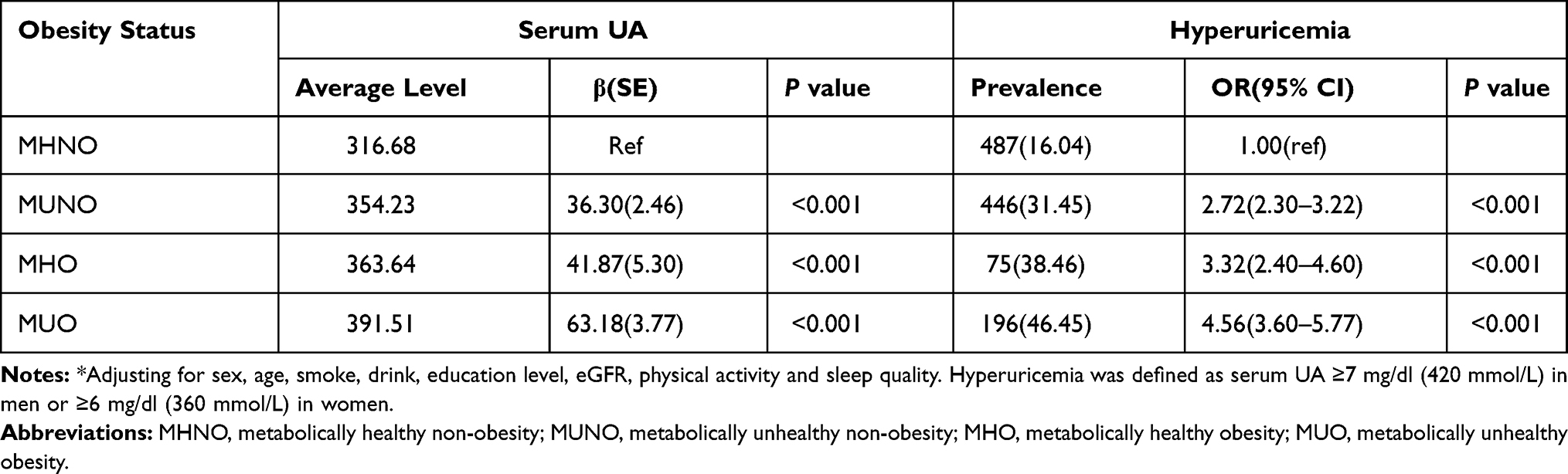 |
Table 2 Multivariate * Adjusted Associations of Serum Uric Acid/Hyperuricemia with Obesity Related Phenotypes |
Results of Sensitivity Analysis
We have separately conduced sex-specific association of obesity types with SUA and hyperuricemia, and the results were consistent with the gender-neutral analysis. Compared to participants with MHNO, those with MUO had the highest likelihood to have hyperuricemia in female (OR=6.71, P<0.001) and male (OR=3.03, P<0.001), followed by those with MHO in female (OR=3.65, P<0.001) and male (OR=3.01, P<0.001), respectively. And the risk of hyperuricemia is higher in women with MUO than in men with MUO. (Supplementary Table S2) After excluding participants with prevalent CKD and CVD, our results did not change a lot. These results indicated that the association between hyperuricemia and obesity-metabolic phenotype may be unlikely to be driven by these conditions (Supplementary Table S3).
Results of Mendelian Randomization Analysis
The causal relationship between uric acid and BMI is shown in Figure 1. The GSMR model with BMI as the exposure and uric acid as the outcome found a significant causal effect (β=0.059, P=6.54×10−154). Otherwise, the causal effect of uric acid on BMI was not statistically significant (β=0.009, P=0.70). These causal effect signals were unlikely to be driven by potential pleiotropy as indicated by the HEIDI-outlier analysis (all P>0.05).
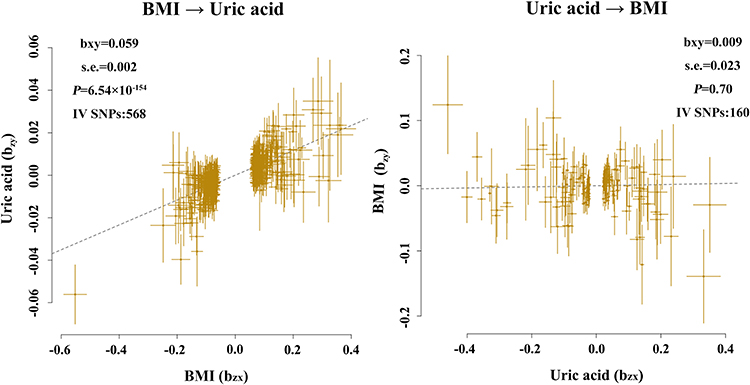 |
Figure 1 Casual association between uric acid and BMI. Abbreviations: bxy, regression effect size; IV SNPs, the number of SNPs being used as instrumental variables; s.e., standard error. Note: All of them HEIDI test P-value more than 0.05. |
Discussion
In a large sample of Chinese adults in the Tianning cohort, we found that hyperuricemia was higher prevalent in participants with metabolically unhealthy obesity than those with metabolically healthy obesity, as well as those with a normal BMI. The Mendelian Randomization analysis further demonstrated that elevated uric acid was more likely to be a result rather than a cause of elevated BMI. These findings suggested that metabolic condition and serum uric acid should be regularly monitored to prevent hyperuricemia in obese populations, those with metabolic syndrome in particular.
As established risk factors of CVD, deciphering the roles of obesity, metabolic syndrome, and hyperuricemia in the etiology network would undoubtedly improve the prevention and management of CVD.5,30,31 The association between obesity and hyperuricemia has been extensively studied,32,33 but few studies took into account the effects of metabolic status. In line with our study, however, obesity with varied metabolic status has been associated with other disorders, such as depression, CVD, carotid atherosclerosis, and CKD. A study including 18,025 subjects showed that both obesity and metabolic syndrome had a synergistic association with depression.34 A cohort study including more than five thousands middle-aged and elderly individuals in Netherlands suggested that metabolically healthy obesity subjects were not at significant increased risk of CVD compared to normal weight individuals without metabolic syndrome, but the risk of CVD in metabolically unhealthy obesity group were significantly increase.35 However, a cohort study of metabolically healthy participants in Korea and their findings indicated that metabolically healthy obesity is not a harmless condition and it can induce the development of carotid atherosclerosis.36 A cohort study including 41,194 Koreans found that participants with metabolically unhealthy obesity were at the highest risk of incident CKD than those with metabolically healthy obesity and a normal BMI.37 In our study, we found that hyperuricemia was most likely to be suffered by participants with metabolically unhealthy obesity, followed by those with metabolically healthy obesity, compared to individuals with a normal BMI. Our study, together with other studies, suggested that obese metabolic phenotypes deserved the attention of clinicians.
Although the association between obesity and hyperuricemia has been reported by many studies, but the causal relationship between them was still not very clear. A study examined the temporal relationship between obesity and hyperuricemia using cross-lagged panel analysis found that the path from uric acid to BMI was more significant than the other path from BMI to uric acid.33 In stark contrast, some studies found an association between BMI and uric acid with the other direction. For instance, an animal study demonstrated that the production of uric acid is augmented in obese mice.7 A bidirectional Mendelian randomization in adult Caucasians revealed that elevated uric acid was a consequence rather than a cause of obesity.38 Using GWAS summary data, we conducted a Mendelian randomization analysis and found causality with the same direction.
Since there were a sex difference in the association between SUA and metabolic syndrome components and cardiovascular mortality,39 we have analyzed the association between obese-metabolic phenotypes and hyperuricemia for different genders. The results in male and female were consistent with the results in all participants, and the risk of hyperuricemia is higher in women with MUO than in men with MUO. In line with our study, a cross-sectional examination in a military cohort of 6738 men and 766 women showed that the association between each SUA level and elevated serum alanine aminotransferase may differ by sex among military young adults, but the mechanism for the sex difference was unclear.40 Another research used the same cohort suggested that the association between hyperuricemia and various cardiometabolic abnormalities in young adults may differ by sex.41 But the mechanism for the sex difference requires further investigations.
Uric acid is the catabolic product of exogenous dietetic compounds and endogenous purines.42 Its serum levels mainly relied on liver production and kidney elimination to maintain balance.43 Therefore, many disorders, eg, CKD or CVD, may modify the association between obesity and hyperuricemia. Our sensitivity analysis found that excluding participants with CKD or CVD did not change the association between obese-metabolic phenotypes and hyperuricemia. This finding indicated that the association between different metabolic status in obesity and hyperuricemia may not be driven by these conditions.
The mechanisms underlying the identified association between obesity in different metabolic status and serum uric acid are unclear. Insulin resistance may be involved. It is increasingly prevalent as the number of metabolic disorders and more prevalent in obese participants than those with a normal BMI.44,45 Hyperinsulinemia could reduce renal serum uric acid excretion and thereby leading to subsequent hyperuricemia.46 Obesity and metabolic status should be regularly monitored when assessing the risk of hyperuricemia and the treatment of metabolic syndrome is of great importance for cardiovascular promotion in obese community members, because metabolically healthy obesity is not a healthy state where hyperuricemia is already increased prevalent compared with non-obese participants. Further, it is not clear whether individuals with metabolically healthy obesity can maintain insulin sensitivity during the entire life or whether metabolically healthy obesity simply represents delayed onset of obesity-related insulin resistance.45 The underlined mechanisms warranted further investigation.
The strengths of our study include a relatively large sample size, comprehensive adjustment for covariates including sleep and physical activity both have been associated with insulin resistance,47,48 and Mendelian randomization analysis to compensate for the limitations of cross-sectional analysis. Several limitations of our study should be considered. First, we did not have dietary data on purine intake. Whether or to what extent our results were affected by diet is unclear. Second, we did not focus on whether type 1 diabetes would have an impact on our results. The results need to be explored in further study.
In conclusion, metabolically unhealthy obesity, in comparison with metabolically healthy obesity, was significantly associated with hyperuricemia in Chinese adults. Metabolic condition and serum uric acid should be regularly monitored to prevent hyperuricemia in obese populations, those with metabolic syndrome in particular.
Data Sharing Statement
The datasets used during the current study are available from the corresponding author on reasonable request at [email protected].
Acknowledgments
We are deeply appreciative of the participants in this study and thank all staffs for their support and assistance. Especially, we thank the Center for Disease Prevention and Control of Tianning District for their support in the recruitment of participants.
Author Contributions
All authors have read and approved the submission, contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work. These authors contributed equally to this work and should be considered as co-first authors: Jia Yu, Hongyan Sun, and Jinhua Zhu.
Funding
This study was supported by the National Key Research and Development Program of China (NO. 2017YFC1307600), the National Natural Science Foundation of China (NO. 81903384, 81872690), the Natural Science Foundation of Jiangsu Province (NO. BK20180841), the Suzhou Science and Technology Project (NO. SS201853), and a Project of the Priority Academic Program Development of Jiangsu Higher Education Institutions. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors report no conflicts of interest for this work and state they have financial associations that might pose a conflict of interest in connection with the submitted article.
References
1. Joosten LAB, Crişan TO, Bjornstad P, Johnson RJ. Asymptomatic hyperuricaemia: a silent activator of the innate immune system. Nat Rev Rheumatol. 2019;16(2):75–86. doi:10.1038/s41584-019-0334-3
2. Liu R, Han C, Wu D, et al. Prevalence of hyperuricemia and gout in Mainland China from 2000 to 2014: a systematic review and meta-analysis. Biomed Res Int. 2015;2015:762820. doi:10.1155/2015/762820
3. Tian S, Liu Y, Xu Y, Feng A. Does obesity modify the epidemiological association between hyperuricemia and the prevalence of hypertension among Northern Chinese community-dwelling people? A Chinese population-based study. BMJ Open. 2019;9(11):e031803. doi:10.1136/bmjopen-2019-031803
4. Lee SK, Kim SH, Cho GY, et al. Obesity phenotype and incident hypertension: a prospective community-based cohort study. J Hypertens. 2013;31(1):145–151. doi:10.1097/HJH.0b013e32835a3637
5. Ortega FB, Lavie CJ, Blair SN. Obesity and cardiovascular disease. Circ Res. 2016;118(11):1752–1770. doi:10.1161/CIRCRESAHA.115.306883
6. Chen-Xu M, Yokose C, Rai SK, Pillinger MH, Choi HK. Contemporary prevalence of gout and hyperuricemia in the United States and decadal trends: the national health and nutrition examination survey, 2007–2016. Arthritis Rheumatol (Hoboken, NJ). 2019;71(6):991–999. doi:10.1002/art.40807
7. Tsushima Y, Nishizawa H, Tochino Y, et al. Uric acid secretion from adipose tissue and its increase in obesity. J Biol Chem. 2013;288(38):27138–27149. doi:10.1074/jbc.M113.485094
8. Lee Y-S, Kim S-H, Yuk HJ, Lee G-J, Kim D-S. (Pall.) Kuntze (New Zealand Spinach) prevents obesity and hyperuricemia in high-fat diet-induced obese mice. Nutrients. 2018;10(8):1087. doi:10.3390/nu10081087
9. Ma Z, Wang Y, Xu C, et al. Obesity-related genetic variants and hyperuricemia risk in Chinese men. Front Endocrinol (Lausanne). 2019;10:230. doi:10.3389/fendo.2019.00230
10. Kuwahara E, Murakami Y, Okamura T, et al. Increased childhood BMI is associated with young adult serum uric acid levels: a linkage study from Japan. Pediatr Res. 2017;81(2):293–298. doi:10.1038/pr.2016.213
11. Cuthbertson DJ, Steele T, Wilding JP, et al. What have human experimental overfeeding studies taught us about adipose tissue expansion and susceptibility to obesity and metabolic complications? Int J Obe (Lond). 2017;41(6):853–865. doi:10.1038/ijo.2017.4
12. Sun R, Huang J, Yang N, et al. Purine catabolism shows a dampened circadian rhythmicity in a high-fat diet-induced mouse model of obesity. Molecules (Basel, Switzerland). 2019;24(24):4524. doi:10.3390/molecules24244524
13. Fabbrini E, Serafini M, Colic Baric I, Hazen SL, Klein S. Effect of plasma uric acid on antioxidant capacity, oxidative stress, and insulin sensitivity in obese subjects. Diabetes. 2014;63(3):976–981. doi:10.2337/db13-1396
14. Rani V, Deep G, Singh RK, Palle K, Yadav UC. Oxidative stress and metabolic disorders: pathogenesis and therapeutic strategies. Life Sci. 2016;148:183–193. doi:10.1016/j.lfs.2016.02.002
15. Kammoun HL, Kraakman MJ, Febbraio MA. Adipose tissue inflammation in glucose metabolism. Rev Endocr Metab Disord. 2014;15(1):31–44. doi:10.1007/s11154-013-9274-4
16. Primeau V, Coderre L, Karelis AD, et al. Characterizing the profile of obese patients who are metabolically healthy. Int J Obes (Lond). 2011;35(7):971–981. doi:10.1038/ijo.2010.216
17. Muñoz-Garach A, Cornejo-Pareja I, Tinahones FJ. Does metabolically healthy obesity exist? Nutrients. 2016;8(6):320. doi:10.3390/nu8060320
18. Karelis AD. Metabolically healthy but obese individuals. Lancet. 2008;372(9646):1281–1283. doi:10.1016/S0140-6736(08)61531-7
19. Phillips CM. Metabolically healthy obesity: definitions, determinants and clinical implications. Rev Endocr Metab Disord. 2013;14(3):219–227. doi:10.1007/s11154-013-9252-x
20. Chen HH, Tseng YJ, Wang SY, et al. The metabolome profiling and pathway analysis in metabolic healthy and abnormal obesity. Int J Obes (Lond). 2015;39(8):1241–1248. doi:10.1038/ijo.2015.65
21. Chen Y, Zhang N, Sun G, et al. Metabolically healthy obesity also has risk for hyperuricemia among Chinese general population: a cross-sectional study. Obes Res Clin Pract. 2016;10(Suppl 1):S84–s95. doi:10.1016/j.orcp.2016.03.008
22. Kim IY, Han K-D, Kim DH, et al. Women with metabolic syndrome and general obesity are at a higher risk for significant hyperuricemia compared to men. J Clin Med. 2019;8(6):837. doi:10.3390/jcm8060837
23. Yu J, Sun H, Shang F, et al. Association between glucose metabolism and vascular aging in Chinese adults: a cross-sectional analysis in the Tianning Cohort Study. Clin Interv Aging. 2019;14:1937–1946. doi:10.2147/CIA.S223690
24. Sui X, Church TS, Meriwether RA, Lobelo F, Blair SN. Uric acid and the development of metabolic syndrome in women and men. Metabolism. 2008;57(6):845–852. doi:10.1016/j.metabol.2008.01.030
25. Alberti KGMM, Eckel RH, Grundy SM, et al. Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation. 2009;120(16):1640–1645. doi:10.1161/CIRCULATIONAHA.109.192644
26. Zhou B-F. Predictive values of body mass index and waist circumference for risk factors of certain related diseases in Chinese adults--study on optimal cut-off points of body mass index and waist circumference in Chinese adults. Biomed Environ Sci. 2002;15(1):83–96.
27. Zhu Z, Zheng Z, Zhang F, et al. Causal associations between risk factors and common diseases inferred from GWAS summary data. Nat Commun. 2018;9(1):224. doi:10.1038/s41467-017-02317-2
28. Cuéllar-Partida G, Lundberg M, Kho PF, et al. Complex-traits genetics virtual lab: a community-driven web platform for post-GWAS analyses. bioRxiv. 2019;518027. doi:10.1101/518027.
29. Tin A, Marten J, Halperin Kuhns VL, et al. Target genes, variants, tissues and transcriptional pathways influencing human serum urate levels. Nat Genet. 2019;51(10):1459–1474. doi:10.1038/s41588-019-0504-x
30. Kachur S, Lavie CJ, de Schutter A, Milani RV, Ventura HO. Obesity and cardiovascular diseases. Minerva Med. 2017;108(3):212–228. doi:10.23736/s0026-4806.17.05022-4
31. Ndrepepa G. Uric acid and cardiovascular disease. Clin Chim Acta. 2018;484:150–163. doi:10.1016/j.cca.2018.05.046
32. Ali N, Perveen R, Rahman S, et al. Prevalence of hyperuricemia and the relationship between serum uric acid and obesity: a study on Bangladeshi adults. PLoS One. 2018;13(11):e0206850. doi:10.1371/journal.pone.0206850
33. Han T, Meng X, Shan R, et al. Temporal relationship between hyperuricemia and obesity, and its association with future risk of type 2 diabetes. Int J Obes (Lond). 2018;42(7):1336–1344. doi:10.1038/s41366-018-0074-5
34. Moazzami K, Lima BB, Sullivan S, Shah A, Bremner JD, Vaccarino V. Independent and joint association of obesity and metabolic syndrome with depression and inflammation. Health Psychol. 2019;38(7):586–595. doi:10.1037/hea0000764
35. Dhana K, Koolhaas CM, van Rossum EF, et al. Metabolically healthy obesity and the risk of cardiovascular disease in the elderly population. PLoS One. 2016;11(4):e0154273. doi:10.1371/journal.pone.0154273
36. Kim TJ, Shin HY, Chang Y, et al. Metabolically healthy obesity and the risk for subclinical atherosclerosis. Atherosclerosis. 2017;262:191–197. doi:10.1016/j.atherosclerosis.2017.03.035
37. Jung CH, Lee MJ, Kang YM, et al. The risk of chronic kidney disease in a metabolically healthy obese population. Kidney Int. 2015;88(4):843–850. doi:10.1038/ki.2015.183
38. Lyngdoh T, Vuistiner P, Marques-Vidal P, et al. Serum uric acid and adiposity: deciphering causality using a bidirectional Mendelian randomization approach. PLoS One. 2012;7(6):e39321. doi:10.1371/journal.pone.0039321
39. Lin GM, Li YH, Zheng NC, et al. Serum uric acid as an independent predictor of mortality in high-risk patients with obstructive coronary artery disease: a prospective observational cohort study from the ET-CHD registry, 1997–2003. J Cardiol. 2013;61(2):122–127. doi:10.1016/j.jjcc.2012.09.004
40. Lin JW, Tsai KZ, Chen KW, et al. Sex-specific association between serum uric acid and elevated alanine aminotransferase in a military cohort: the CHIEF study. Endocr Metab Immune Disord Drug Targets. 2019;19(3):333–340. doi:10.2174/1871530319666181129163802
41. Lin YK, Lin YP, Lee JT, et al. Sex-specific association of hyperuricemia with cardiometabolic abnormalities in a military cohort: the CHIEF study. Medicine. 2020;99(12):e19535. doi:10.1097/md.0000000000019535
42. Fathallah-Shaykh SA, Cramer MT. Uric acid and the kidney. Pediatr Nephrol. 2014;29(6):999–1008. doi:10.1007/s00467-013-2549-x
43. Maiuolo J, Oppedisano F, Gratteri S, Muscoli C, Mollace V. Regulation of uric acid metabolism and excretion. Int J Cardiol. 2016;213:8–14. doi:10.1016/j.ijcard.2015.08.109
44. Bonora E, Kiechl S, Willeit J, et al. Prevalence of insulin resistance in metabolic disorders: the Bruneck Study. Diabetes. 1998;47(10):1643–1649. doi:10.2337/diabetes.47.10.1643
45. Blüher M. The distinction of metabolically ‘healthy’ from ‘unhealthy’ obese individuals. Curr Opin Lipidol. 2010;21(1):38–43. doi:10.1097/MOL.0b013e3283346ccc
46. Li C, Hsieh MC, Chang SJ. Metabolic syndrome, diabetes, and hyperuricemia. Curr Opin Rheumatol. 2013;25(2):210–216. doi:10.1097/BOR.0b013e32835d951e
47. Sweatt SK, Gower BA, Chieh AY, Liu Y, Li L. Sleep quality is differentially related to adiposity in adults. Psychoneuroendocrinology. 2018;98:46–51. doi:10.1016/j.psyneuen.2018.07.024
48. Reutrakul S, Van Cauter E. Sleep influences on obesity, insulin resistance, and risk of type 2 diabetes. Metabolism. 2018;84:56–66. doi:10.1016/j.metabol.2018.02.010
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.