Back to Journals » Infection and Drug Resistance » Volume 16
Asymptomatic Broncholithiasis and Aspergillus Infection: A Case Report and Literature Review
Authors Hu S, Yang X ![]() , Huang Y, Xu Z
, Huang Y, Xu Z
Received 1 March 2023
Accepted for publication 3 May 2023
Published 10 May 2023 Volume 2023:16 Pages 2911—2919
DOI https://doi.org/10.2147/IDR.S410155
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Songhua Hu, Xudan Yang, Yaqin Huang, Zhihao Xu
Department of Respiratory and Critical Care Medicine, The Fourth Affiliated Hospital, International Institutes of Medicine, Zhejiang University School of Medicine, Yiwu, 322000, People’s Republic of China
Correspondence: Zhihao Xu, Department of Respiratory and Critical Care Medicine, The Fourth Affiliated Hospital, International Institutes of Medicine, Zhejiang University School of Medicine, No. N1, Shangcheng Avenue, Yiwu, Zhejiang, 322000, People’s Republic of China, Email [email protected]
Abstract: Broncholithiasis coupled with Aspergillus infection is a rare disease of the respiratory system with complex pathogenesis and non-specific clinical manifestations that can be easily confused with other types of infectious diseases of the respiratory system. The lack of pertinent clinical manifestations in patients increases the risk of clinical misdiagnosis, omission, and incorrect treatment plan selection, which can result in permanent lung structural alterations and lung function decompensation and ultimately harm the lung. We report a rare case of asymptomatic broncholithiasis coupled with Aspergillus infection that was treated at our hospital and discuss the pathophysiology, diagnosis, differential diagnosis, and prognostic follow-up course. Furthermore, relevant studies from China and other countries, including this case, were reviewed. We gathered eight reports, summarized their significant diagnoses and treatments for broncholithiasis and broncholithiasis coupled with Aspergillus infection, and discussed their clinical features. Our study may help improve physicians’ awareness of these types of diseases and serve as a resource for future diagnosis and treatment.
Keywords: broncholithiasis, Aspergillus infection, obstructive pneumonia, infection
Introduction
Broncholithiasis refers to a condition characterized with the existence of calcified or ossified masses within the tracheobronchial tree, which may lead to intense respiratory irritation or obstructive symptoms.1 The most frequent causes of broncholithiasis include chronic inflammatory processes or granulomatous diseases, which cause calcification of mediastinal or peri-tracheal lymph nodes and their erosion and extrusion into the bronchial lumen.2 However, the previous studies reported that less than 3% of broncholithiasis cases have an identified source of infection. Endobronchial aspergillosis coupled with broncholithiasis is highly uncommon, with histoplasmosis being the most prevalent type in North America and Mycobacterium tuberculosis (Mtb) infection being the most prevalent in China. Aspergillus is a conditional pathogen that is often detected in patients with immunodeficiency or impaired immune function. Broncholithiasis can cause fungal infections in the bronchial lumen even in people with immunocompetent conditions. There are currently no comprehensive clinical recommendations or professional consensus, and only a small number of these cases have been recorded worldwide. Here, we report a case of asymptomatic broncholithiasis coupled with aspergillosis with a normal immune function that was found in our hospital. We also analyze the domestic and international literature to summarize the case’s clinical features, imaging characteristics, bronchoscopy performance, and therapeutic options.
Case Report
In July 2020, a 48-year-old male presented with a “lung shadow of 1 week (1w) on physical examination” at the Fourth Affiliated Hospital, Zhejiang University School of Medicine, other hospital chest computed tomography (CT) results showed inflammatory lesions in the upper lobe of the right lung (exact report not available). The patient had no uncomfortable symptoms such as fever, cough, or hemoptysis, and thus he was given levofloxacin tablets as an anti-infection treatment. The results of the chest CT were re-examined after 10 days of treatment and revealed that mediastinal lymph nodes had calcification, the upper lobe of the right lung had a lamellar shadow with calcification, corresponding bronchial stenosis, and possibly chronic inflammatory lesions. The two lungs also had a few speckled and cord-like hyperdense shadows (Figure 1A and B). The patient had a history of hypertension, fatty liver, and abnormal liver function, with no history of glucocorticoids, cytotoxic drugs, or immunosuppressive therapy. Personal history: smoked 10 cigarettes per day for more than 20 years.
 |
Figure 1 Chest computed tomography (CT), bronchoscopic changes, and pathological findings in July 2020. Notes: The chest CT shows a lamellar shadow in the upper lobe of the right lung with calcifications, corresponding bronchial stenosis, and possible chronic inflammatory lesions (A). Mediastinal window shows calcified foci in the lungs (B). A necrotic mass in the anterior segment of the upper lobe of the right lung on bronchoscopy (C). Pathology showed fungal mycelium with necrotic calcification, and the morphology was more consistent with Aspergillus (D and E). |
He was admitted with a temperature of 36.8°C, a respiratory rate of 20 breaths per minute, a heart rate of 72 beats per minute, a blood pressure of 143/90 mmHg, and a body mass index (BMI) of 26.08 kg/m2. He was in a clear state of mind and had regular breath sounds in his lungs, no dry rales, and no pleural friction sounds on auscultation. Physical examination of the heart, abdomen, and peripheral vasculature revealed no obvious abnormalities. Immunoglobulin (Ig) and antibody results showed that IgG was 7.39 g/L↓ and complement protein C4 was 0.11 g/L↓. Biochemical results revealed that alanine transaminase was 63 U/L↑ and γ-glutamyl transferase was 92 U/L↑. His routine blood test as well as other laboratory tests such as T, B, and natural killer lymphocyte subsets were normal. On the second day following admission, a bronchoscopy was performed. White pus was observed in the flushing of the right upper lobe lumen and a necrotic mass tissue was observed under a bronchoscope in the anterior portion of the right upper lobe (Figure 1C). The bronchial mucosa of the anterior segment of the right upper lobe was taken for pathological examination. Brushing and bronchoalveolar lavage fluid (BALF) examinations were also performed. Pathological biopsy showed fungal hyphae with necrotic calcification, the morphology was more consistent with Aspergillus (Figure 1D and E), indicating broncholithiasis and right upper lobe invasive aspergillosis. The BALF galactomannan (BALF-GM) test result was 1.4 μg/L (positive), fungal culture for Aspergillus fumigatus was found, bacterial culture was normal bacterial growth, Mtb DNA and tuberculosis (TB) smear examinations were negative, and no malignant cells were observed. The brush test results were also normal. A diagnosis of broncholithiasis and Aspergillus infection was made in conjunction with the examination results, and the patient was treated with voriconazole 200 mg bid antifungal therapy. Treatment was continued with oral voriconazole after discharge from the hospital. The chest CT was taken at each of the six follow-up visits, and the results revealed that the inflammatory lesions had been completely absorbed. During this period, the patient had no clinical symptoms and was in good general health.
A secondary bronchoscopy was carried out in February 2021 to determine whether to discontinue antifungal medication after six months of treatment. The patient was no longer prescribed voriconazole after BALF-GM test results and accompanying pathogenic smear and culture examinations were negative. In February 2022, one year after the termination of the voriconazole, the patient underwent one more examination, and a CT scan showed bronchiectasis in the upper lobe of the right lung, in which nodules with calcification were observed, measuring about 3.1×1.7 cm, which was larger than before. A faint lamellar shadow was seen next to the right lung hilar, and therefore infection was considered. Multiple foci of calcification were seen in the right lung hilar, and calcified lymph nodes were seen in the mediastinum (Figure 2A). Because the patient had no subjective symptoms despite these findings, suggesting that his condition was progressing, a third bronchoscopy was carried out. A stone-like mass was discovered in the anterior section of the upper right lung on bronchoscopy (Figure 2B), and white pus was seen on flushing. Bronchoscopic stone extraction failed because the stone was firmly attached to the tracheal wall and could not be moved or totally detached. Mucosal biopsy pathology showed chronic inflammation of the mucosa with calcification (Figure 2C). BALF revealed that erythrocytes were >100/Hp, nucleated cells were 6–10/Hp, the neutrophil percentage was 92%, and fungal culture was negative, and the rest of the bacterial smear and bacterial culture results were not abnormal. The final diagnosis was as follows: (1) broncholithiasis and (2) obstructive pneumonia; hence, the patient was given cefixime for anti-infection. After a month, the chest CT was retested, and the results showed a good prognosis.
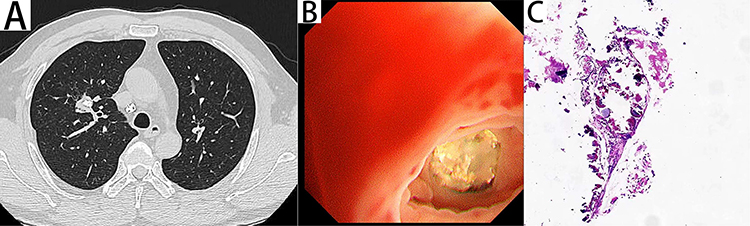 |
Figure 2 Chest computed tomography (CT), bronchoscopic changes, and pathological findings in February 2022. Notes: The chest CT shows bronchiectasis in the upper lobe of the right lung, in which nodules with calcification were seen, measuring about 3.1×1.7 cm; a faint lamellar shadow was seen next to the right hilar, with infection considered (A). Endoluminal stone obstruction in the anterior segment of the upper lobe of the right lung was observed bronchoscopically (B). Pathology showed chronic inflammation of the mucosa with calcification (C). |
Literature Review
The key words “broncholithiasis” and “Aspergillus” were searched in CNKI, Wanfang, Vipul, PubMed NCBI, and Web of Science databases. The search period was from the time of publication of the literature to February 2023, excluding cases without histopathological confirmation and clinical misdiagnosis. The present case and eight patients who matched the diagnostic criteria for broncholithiasis coupled with Aspergillus infection were included. Here, we provide a summary of this disease’s clinical traits, radiological traits, bronchoscopic symptoms, and therapeutic options along with relevant cases that have already been documented in the literature. Patients with broncholithiasis coupled with Aspergillus infection ranged in age from 9.6 to 67 years, with a median age of 52 years. Patients were predominantly females (5/8). Six of the eight (6/8; 75%) patients were non-smokers or ex-smokers, and only one (1/8; 12.5%) patient was a long-term smoker. Five patients had underlying diseases in varying degrees, of which lung diseases were TB (n = 2), allergic bronchopulmonary aspergillosis (n = 2), severe pneumonia (n = 2), type II respiratory failure (n = 1), and post-tracheal stenosis reconstruction and stenting (n = 1). Non-pulmonary comorbidities included aplastic anemia and post-hematopoietic stem cell transplantation (n = 1), hypertension, and liver function abnormalities. Among the documented cases, only two showed signs of immunodeficiency linked to the illness. The proportion of immunocompetent individuals with co-infection with Aspergillus was 75%, which is not entirely consistent with Aspergillus, which is often secondary to malignancies, hematological diseases, hormones, and immunosuppressive agents that lead to immunocompromise.3 Cough (4/8, 50%) and hemoptysis (4/8, 50%) were the most frequent clinical symptoms of the condition, and intravaginal stones were more likely to produce coughing and hemoptysis (4/5, 80%) than other forms of stones, which is consistent with the results of a previous report.4 Although fever and chills occur during bacterial infection, our case showed no clinical signs at any point in the progression of the illness. The physical examination did not reveal any pertinent indications except for a few descriptions of respiratory sound changes, which mostly depended on where the location of the stone, the blockage of the airway, and whether the trachea was structurally deformed locally.5 Table 1 presents an overview of the clinical characteristics of the eight patients.
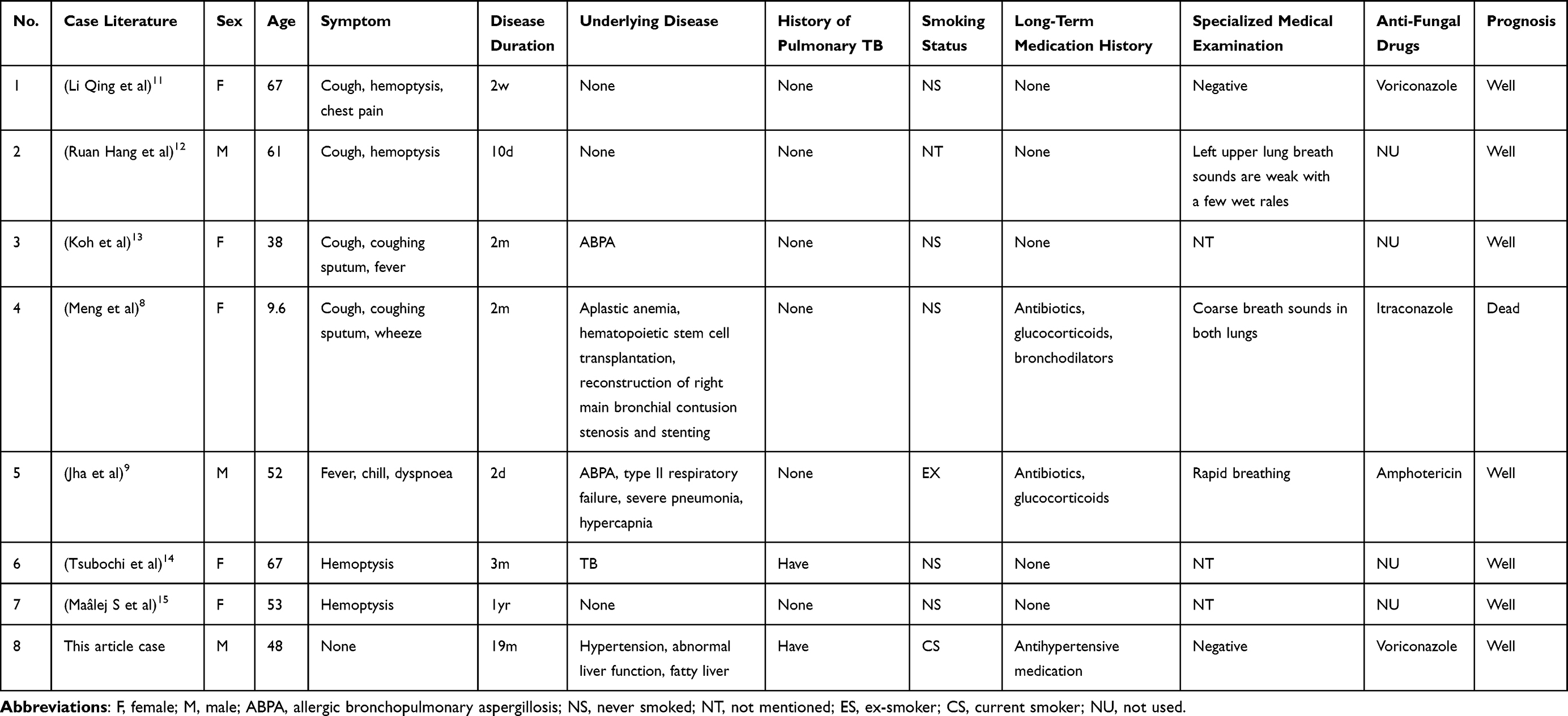 |
Table 1 Clinical Characteristics of the Eight Patients with Broncholithiasis Coupled with Aspergillus Infection |
Results from a CT scan revealed that the right lung (6/8, 75%) was more likely to have nodules with Aspergillus lesions than the left lung (2/8, 25%), with the right upper lobe (3/6, 50%) being the most frequently impacted, which was associated with airway anatomy and lymph node distribution.6 The image of the lung mainly presented calcified high-density shadow in or around the bronchial lumen (7/8, 87.5%), which is often combined with indirect signs of luminal obstruction such as bronchiectasis and obstructive pneumonia. Calcified nodules associated with obstructive findings on CT imaging provide a highly accurate prediction of broncholithiasis. However, primary endobronchial aspergilloma with calcification7 or tracheobronchial disease with calcification of the bronchial wall mimics bronchial stone imaging features on CT. Therefore, understanding typical radiological features of the disease may help obtain an accurate diagnosis and provide an appropriate treatment plan for the disease. Moreover, in the case reported by Meng, the CT was not typical because the stone was embedded in granulomatous tissue. Hence, chest CT had certain limitations8 when the necrotic granulomatous inflammatory tissue coexisted with the stone, making the diagnosis more challenging.
Bronchoscopically, the majority of stones were directly detectable (5/8; 62.5%), and aberrant bronchoscopic regions matched the results of the CT, but extraluminal stones were difficult to see using a bronchoscope and frequently showed up as bronchial mucosal congestion and edema. Besides, some stones may appear as mucus plugs because they are masked by inflammation in the bronchial wall, or they may be located in the distal part of narrow airways. Therefore, direct signs of stones cannot be observed bronchoscopically, which are pathologically definite after surgical operations (3/8; 37.5%). Although broncholithiasis is an endobronchial condition, bronchoscopy is not often effective in making the correct diagnosis in some cases. Broncholithiasis coupled with Aspergillus infection mainly relies on pathological examination. Pathological biopsy of all patients identified Aspergillus mycelia or spores. Histopathology and BALF culture both revealed signs of a fungus infection in our patient. Owing to the long-term presence of stones in the bronchial lumen, complications were observed in all cases except for extraluminal stones (7/8; 87.5%), which presented with bronchiectasis, obstructive pneumonia, and frequent respiratory infections. Before diagnosis, patients were treated with empirical antibiotics and bronchodilators, but none of the therapies worked. The presence of severe adhesions between the stone and the bronchial wall prevented successful bronchoscopic stone extraction in our patient. Since there were no signs of hemoptysis or other serious complications, we opted not to perform additional surgery while administering antifungal medication. Bronchoscopic stone extraction or surgical lobectomy were applied to treat the remaining seven cases — in conjunction with adjuvant antifungal medication in some cases — and all had a favorable prognosis without recurrence, except for the patient reported by Jha9 who died of immunocompromise due to severe underlying disease and long-term tracheal intubation, glucocorticoids, and carbapenem antibiotic therapy. The imaging characteristics and bronchoscopic symptoms in the eight patients are summarized in Table 2.
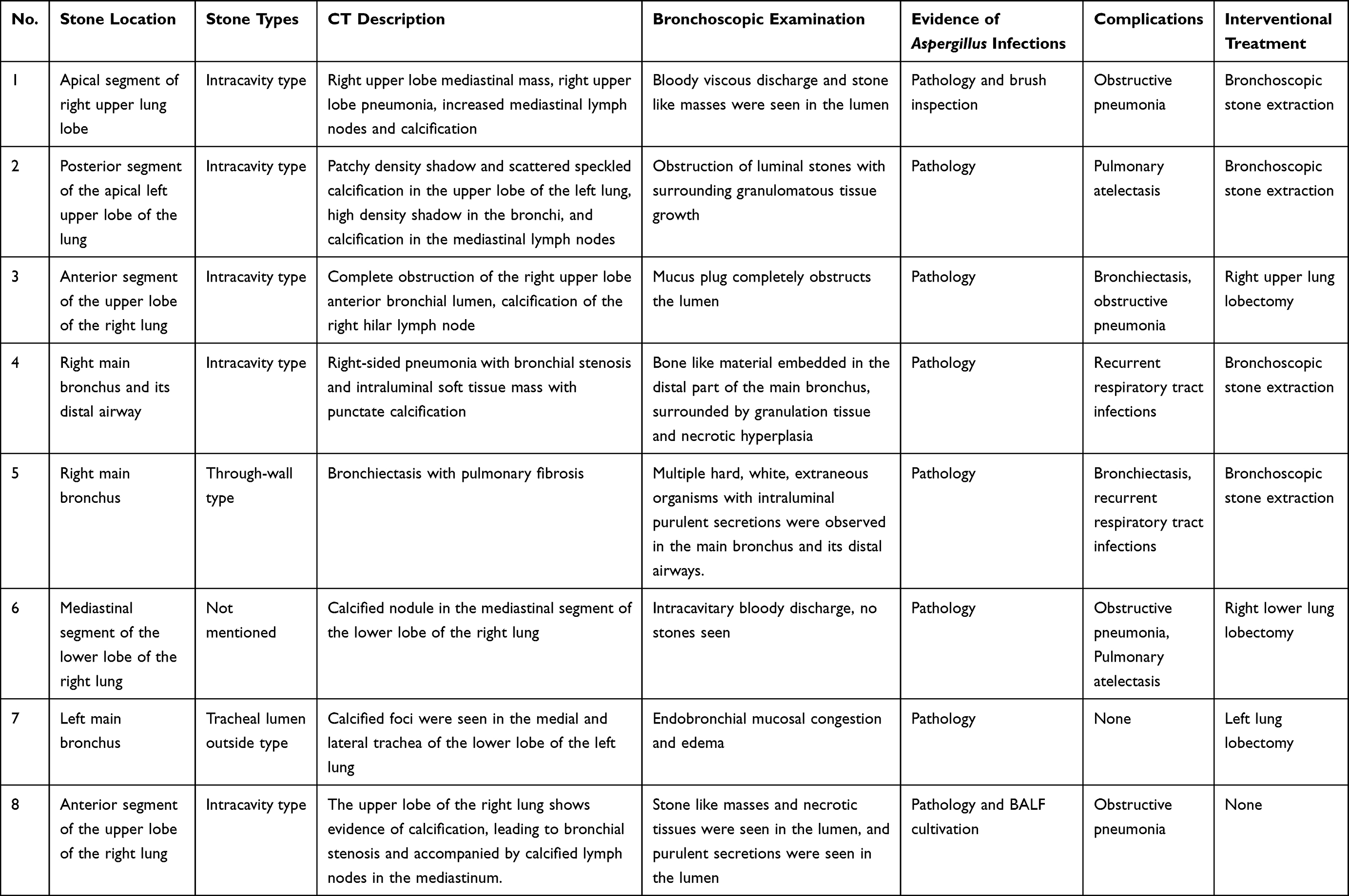 |
Table 2 Radiographic and Bronchoscopy Findings in the Eight Patients with Broncholithiasis Coupled with Aspergillus Infection |
Discussion
Broncholithiasis is a rare disease of the respiratory system characterized by formation of calcified or ossified masses in the bronchial lumen. Its pathogenesis is complex and any process affecting dystrophic calcification may lead to the development of calculi.10 Broncholithiasis is caused by chronic inflammatory or chronic granulomatous disease, resulting in necrotizing inflammation of the mediastinum or peritracheal lymph nodes, followed by calcification, under the influence of prolonged respiratory movement, swallowing action, coughing pressure, and heartbeat. A few calcified areas gradually erode and penetrate the bronchial wall, eventually detaching and falling into the bronchus. These foci then become embedded in the lobes or segments of the bronchus to form bronchial stones, which are thought to be the most common type of stone formation. Currently, less than 3% of confirmed infection types in broncholithiasis have been recorded worldwide. Mtb infections are abundant in China and Histoplasma is prevalent in North America; however, Aspergillus infection associated with broncholithiasis is incredibly rare. The prevalence of bronchial stones is higher in the right lung due to the unique anatomical structure of the airway and the distribution of lymph nodes in that area, especially in the upper and middle lobes of the right lung, which is consistent with the results of our case and the literature review. The most typical symptoms of broncholithiasis coupled with Aspergillus infection are cough and hemoptysis, while other symptoms such as fever and chills may appear when broncholithiasis is coupled with a bacterial infection that causes obstructive pneumonia and bronchiectasis. None of the seven reported cases of broncholithiasis had lithoptysis, a rare but distinctive sign of the disease. Furthermore, all the above cases were diagnosed passively, suggesting that the illness is very sneaky and is easily mistaken for other infectious diseases of the respiratory system, which results in clinical misdiagnosis and incorrect anti-infective treatment regimen selection, delaying the best time for treatment, extending the median time for patient diagnosis, and causing the illness to worsen and cause several additional related complications. In our case, the patient did not exhibit any symptoms during the entire period of sickness, and hence this situation is more likely to go unnoticed. Besides, the patient experiences irreversible lung structural alterations and lung function declines with time, which seriously affects the quality of life and causes long-term damage. Thus, clinicians should pay close attention to this type of illness.
The most crucial supplementary test for broncholithiasis is the chest high-resolution CT (HRCT) scan because it may display the elements of calcified foci in the bronchus as well as those of peribronchial calcification with airway compression features. It also enables the observation of more clearly calcified nodules in precise relation to the adjacent bronchi. When CT scans reveal thick calcifications in or around the bronchial lumen, this can be a significant indicator of the existence of bronchial stones, and this was validated by the imaging results of reported cases.8,11–15 Diagnosis can also be achieved by indirect indications of broncholithiasis, including bronchiectasis caused by stones, obstructive pneumonia, or calcification of the hilar or mediastinal lymph nodes. However, when primary endobronchial aspergilloma develops calcification, tracheobronchial diseases with calcification of the tracheal wall or endobronchial tumors forming calcified foci, such as carcinoid tumors and malignant tumors, may show similar imaging findings to bronchial calculi on CT. Additionally, if the stone is embedded in the granulation tissue, CT findings are uncharacteristic; thus, chest CT has some restrictions in these circumstances. Bronchoscopy combined with surgery and pathological examination is the main method to diagnose broncholithiasis coupled with Aspergillus infection. Due to its minimally invasive nature, bronchoscopy has become the preferred clinical examination. Direct bronchoscopy enables the direct visualization of endoluminal and transmural stones. However, the observation of extraluminal stones and those located in narrow distal airways may necessitate the presence of mucosal congestion and edema, as well as distorted bronchial stenosis, which may require additional surgical procedures to confirm the diagnosis. The pathological examination is the fundamental method used to determine whether an individual has Aspergillus infection; however, when bronchial stones calcify, the pathogenic and histological signs typically vanish, which presents some challenges for the clinical explanation of the origin of stones in the non-infected period. The Aspergillus mycelium or spores were discovered in all eight cases under the microscope.8,9,11–15 Our case is the first in which Aspergillus infection was detected through both histopathology and alveolar lavage fluid culture despite the absence of any clinical symptoms or underlying illness.
Aspergillus is a conditionally pathogenic mold, widely distributed in the air and environment, and is easily suspended and disseminated.16 Except for the higher incidence in immunodeficient patients, a rising trend of fungal infections has been reported in immunocompetent patients without underlying diseases. Broncholithiasis coupled with endobronchial Aspergillus infection is extremely uncommon. In our patient, microscopic results showed that the Aspergillus mycelium was restricted to the bronchus lumina and did not invade the airways’ basement membrane or necrotic tissue, we speculate that the pre-existing broncholithiasis may have been secondarily infected by Aspergillus, with subsequent inflammation progressing to the peripheral bronchi and obstructing the airways, resulting in later obstructive pneumonia. Calcification may occur within the fungal spheres of primary endobronchial aspergillomas, resulting in a lesion that closely resembles broncholithiasis. This can create a diagnostic challenge when differentiating new calcifications in infectious lesions from secondary infections associated with broncholithiasis. Although our patient denied a history of TB, the CT results showed an intrapulmonary fibrous streak shadow and mediastinal lymph node calcification, which indicated a previous experience of TB infection. Therefore, it was further confirmed that the patient may have had necrotic calcification of the bronchial lymph nodes around the lung lobes due to previous TB, and the calcified lymph nodes became embedded in the bronchi and formed bronchial stones. Despite the patient’s immunocompetence, the presence of stones altered the trachea’s structure, which impeded airflow and served as a breeding ground for Aspergillus. A review of the literature showed that the majority of patients had parenchymal abnormalities brought on by previous lung infections.8,9,13,14 Both broncholithiasis and Aspergillus infection contribute to the etiology of the illness; however, there is no consensus on the function of broncholithiasis and Aspergillus infection in the course of the disease since there are very few reported cases of each and a dearth of pertinent in-depth investigations, which warrants further exploration.
Surgical lobectomy and bronchoscopic stone extraction are the two main methods used in the treatment of broncholithiasis. Currently, it is believed that patients with asymptomatic stones may try conservative therapy, while those with free-moving stones and no difficulties may consider bronchoscopic removal of stones. However, when the bronchial stones have significant adhesions to the tracheal wall and symptoms such as severe hemoptysis or recurrent pneumonia occur, surgery should be considered.17 Besides treating broncholithiasis, the patient’s immune system and underlying illness should be considered while deciding on any extra antifungal therapy. Nonetheless, the current consensus among experts and thorough clinical guidelines in this field are lacking. Due to the long-term stimulating effect of stones and Aspergillus on the trachea, the structural destructive lesions of the bronchial wall may occur secondary to bronchial dilatation, and the presence of structural lesions further triggers a decrease in local resistance, making the stone site susceptible to co-infection with pathogenic microorganisms,18 resulting in a vicious circle. As in our case, untreated lithotripsy caused long-term bronchodilation that generated bacterial infection, which ultimately caused obstructive pneumonia. Early stone extraction — which reduces harmful bacteria and infections by correcting local structural alterations — is the best strategy to prevent these consequences.19 If no stone extraction is indicated, a periodic examination of chest CT and bronchoscopy should be performed to assess changes in the situation even if the stones are not clinically significant after controlling the fungal infection. At critical times in the course of the disease, bronchoscopy and BALF evaluations were conducted, and our patient received timely and thorough HRCT follow-up.
Conclusion
In summary, broncholithiasis coupled with Aspergillus infection involves intricate pathogenic processes. As a rare disease of the respiratory system, its detection and diagnosis rates have been increasing with the development of clinical treatment technology and the improvement of treatment levels in recent years. Currently, the best method available for clinical diagnosis of broncholithiasis is a combination of chest CT and bronchoscopy. Combining this method with surgical and pathological examinations can enhance the accuracy of broncholithiasis diagnosis and provide a precise identification of the pathogenic source. However, there is no universal agreement on the best way to examine stones, physicians typically make their decisions based on the patient’s condition and their training. Most patients with broncholithiasis are diagnosed based on a review of their medical history, imaging results, and bronchoscopic manifestations. For patients whose condition cannot be identified in time, a pathological examination performed after the surgical removal of lung lobes or segments can provide a conclusive diagnosis. Even if they have no painful symptoms or signs, patients with a high-density shadow in the bronchial cavity suggested by chest CT are advised to complete bronchoscopy and BALF pathogenesis as soon as possible to increase the effectiveness of clinical diagnosis. After controlling the infection, local structural changes such as lithotripsy should be corrected as early as possible to prevent complications. Chest CT and bronchoscopy should also be routinely rechecked to prevent reinfection. There is still a need for additional and more thorough research to determine whether adjuvant antifungal medication is still necessary after surgery.
Abbreviations
CT, computed tomography; BALF, bronchoalveolar lavage fluid; IgG, immunoglobulin G; ALT, alanine transaminase; γ-GT, γ-glutamyl transpeptidase; GM test, galactomannan test.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Patient Consent and Ethics Statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This study was approved by the Human Research Ethics Committee of the Fourth Affiliated Hospital, Zhejiang University School of Medicine, Approval No. K2022159. The patient provided informed consent for the publication of the case.
Acknowledgments
This research was funded by the China National Key Research and Development Program (Grant No. A16002).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jin Y, Jiang G, Jiang L, Ding JA. Diagnosis and treatment evaluation of 48 cases of broncholithiasis. Thorac Cardiovasc Surg. 2014;64(5):450–455. doi:10.1055/s-0034-1395388
2. Nishine H, Kurimoto N, Okamoto M, Inoue T, Mineshita M, Miyazawa T. Broncholithiasis assessed by bronchoscopic saline solution injection. Intern Med. 2015;54(12):1527–1530. doi:10.2169/internalmedicine.54.3722
3. Wang XH, Xiao Y, Cao XW. 侵袭性曲霉病危险因素及防控措施的研究进展 [Risk factors and advances in prevention and control measures of invasive aspergillosis]. China J Infect Control. 2018;17(1):82–86. Chinese.
4. Lim SY, Lee KJ, Jeon K, et al. Classification of broncholiths and clinical outcomes: clinical outcomes of brocholiths. Respirology. 2013;18(4):637–642. doi:10.1111/resp.12060
5. Li Q, Li QX, Chen L. 支气管结石的研究进展 [Research progress on broncholithiasis]. Pract J Cereb Pneum Vasc Dis. 2019;27(10):15–18. Chinese.
6. Seo JB, Song KS, Lee JS, et al. Broncholithiasis: review of the causes with radiologic-pathologic correlation. RadioGraphics. 2002;22:S199–S213. doi:10.1148/radiographics.22.suppl_1.g02oc07s199
7. Yeo CD, Baeg MK, Kim JW. A case of endobronchial aspergilloma presenting as a broncholith. Am J Med Sci. 2012;343(6):501–503. doi:10.1097/MAJ.0b013e3182425745
8. Meng C, Zhang Z, Liu X, et al. Diagnosis of pulmonary aspergillosis-related broncholithiasis in a child undergoing bronchoscopy: a case report. Medicine. 2019;98(10):e14623. doi:10.1097/MD.0000000000014623
9. Jha OK, Khanna A, Dabral C, Talwar D. Tombs of Aspergillus: a missed cause of recurrent respiratory infections in allergic bronchopulmonary aspergillosis. Indian J Crit Care Med. 2016;20(7):421–424. doi:10.4103/0972-5229.186228
10. Alshabani K, Ghosh S, Arrossi AV, Mehta AC. Broncholithiasis. Chest. 2019;156(3):445–455. doi:10.1016/j.chest.2019.05.012
11. Li Q, Li QX, Chen L. 支气管结石并曲霉菌感染1例报告并文献复习 [Broncholithiasis and Aspergillus infection: a case report and literature review]. China J Infect Control. 2020;19(5):475–480.
12. Ruan H, Li FJ, Xu W, Yan BD. 支气管结石合并曲霉感染一例 [Broncholithiasis and Aspergillus infection: a case report]. Chin J Tubere Respir Dis. 2020;43(6):532–533. Chinese.
13. Koh WJ, Han J, Kim TS, Lee KS, Jang HW, Kwon OJ. Allergic bronchopulmonary aspergillosis coupled with broncholithiasis in a non-asthmatic patient. J Korean Med Sci. 2007;22(2):365–368. doi:10.3346/jkms.2007.22.2.365
14. Tsubochi H, Endo S, Suhara K, Sohara Y. Endobronchial aspergillosis and actinomycosis associated with broncholithiasis. Eur J Cardio-Thoracic Surg. 2007;31(6):1144–1146. doi:10.1016/j.ejcts.2007.02.023
15. Maâlej S, Kwas H, Aouadi S, Zidi A, Ismail O, Drira I. Aspergillose endobronchique associée à une broncholithiase Endobronchial aspergillosis associated with broncholithiasis [Endobronchial aspergillosis associated with broncholithiasis]. Presse Med. 2010;39(12):1331–1333. French. doi:10.1016/j.lpm.2010.07.012
16. Wang SQ, Fan F, Shi DW. 疑似流感继发侵袭性肺曲霉菌感染1例报告 [Invasive pulmonary aspergillosis secondary to suspected influenza: a case report]. Chin J Clin Med. 2022;29(1):122–124. Chinese. doi:10.1186/s13020-022-00675-8
17. Menivale F, Deslee G, Vallerand H, et al. Therapeutic management of broncholithiasis. Ann Thoracic Surg. 2005;79(5):1774–1776. doi:10.1016/j.athoracsur.2003.10.124
18. Li X, Tong X, Fan H. 曲霉菌感染在支气管扩张症中的作用及其诊断与治疗 [Role of Aspergillus infection in bronchiectasis and its diagnosis and treatment]. West China Med J. 2022;37(1):1–7. Chinese.
19. Qiu J, Li J, Gao Y, Wang KJ. 支气管结石合并肺部盖尔森基兴奴卡菌感染1例 [One case of broncholithiasis with Nocardia cyriacigeorgica infection]. J Microb Infect. 2018;13(4):227–232. Chinese.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.