Back to Journals » Journal of Inflammation Research » Volume 19
Associations of Systemic Inflammatory Response Index (SIRI) and Systemic Inflammatory Index (SII) with Cerebral Atherosclerosis
Authors Yang C ![]() , Cai Q, Xie Y, Luo L, Huang Y, Zhang R, Liu Y
, Cai Q, Xie Y, Luo L, Huang Y, Zhang R, Liu Y
Received 9 October 2025
Accepted for publication 16 December 2025
Published 8 January 2026 Volume 2026:19 571202
DOI https://doi.org/10.2147/JIR.S571202
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ning Quan
Chunjiao Yang,* Qi Cai,* Yu Xie, Lei Luo, Yinfei Huang, Renwei Zhang, Yumin Liu
Department of Neurology, Zhongnan Hospital of Wuhan University, Wuhan, Hubei, 430000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yumin Liu, Email [email protected]
Background: Atherosclerosis is a chronic inflammatory disease and a leading cause of stroke. Systemic inflammatory biomarkers are recognized predictors of coronary artery disease. However, their association with cerebral atherosclerosis remains unclear. This study aims to investigate the relationship between systemic inflammatory indices and cerebral atherosclerotic burden.
Methods: A cohort of 5444 patients was enrolled. Cerebral atherosclerotic stenosis was evaluated using DSA, CTA, or MRA. The systemic inflammation response index (SIRI) and systemic immune-inflammation index (SII) were calculated and natural-log-transformed (ln-SIRI, ln-SII). The associations of ln-SIRI and ln-SII with the presence, severity (maximal stenosis degree) and extent (number of lesions) of cerebral atherosclerosis were evaluated using binary logistic regression, ordered logistic regression and restricted cubic spline models. Subgroup analyses were further conducted across clinically relevant strata to assess the consistency of these associations. Additionally, the diagnostic performance of both indices was evaluated using receiver operating characteristic (ROC) curve analysis.
Results: Patients with cerebral atherosclerotic stenosis had significantly higher ln-SIRI (OR: 1.27, 95% CI: 1.19– 1.35) and ln-SII (OR: 1.22, 95% CI: 1.15– 1.30) compared to the non-stenosis group (both p < 0.001). Both indices showed significant positive associations with the severity of the most stenotic lesion (ln-SIRI OR: 1.29, 95% CI: 1.22– 1.36; ln-SII OR: 1.26, 95% CI: 1.20– 1.33) and the number of affected sites (ln-SIRI OR: 1.27, 95% CI: 1.20– 1.34; ln-SII OR: 1.24, 95% CI: 1.18– 1.31), suggesting a significant graded association (p for trend < 0.001). Restricted cubic spline analyses revealed linear associations of ln-SIRI and ln-SII with cerebral atherosclerosis presence, severity and extent. In subgroup analyses stratified by age, comorbidities, and imaging modality, these associations remained consistent (all subgroup p < 0.05). ROC analysis indicated that both indices had modest discriminatory ability, with AUCs of 0.699 for ln-SIRI and 0.698 for ln-SII.
Conclusion: The systemic inflammatory indices ln-SIRI and ln-SII are significantly associated with the presence, severity and extent of cerebral atherosclerosis. These easily obtainable biomarkers may hold promise for improving risk stratification in cerebrovascular diseases.
Keywords: systemic immune-inflammation index, systemic inflammation response index, intracranial atherosclerosis, carotid artery diseases
Introduction
Cerebral atherosclerosis is a primary etiology of stroke. It is widely acknowledged as a chronic inflammatory disorder of the vascular wall, characterized by endothelial dysfunction, lipid accumulation within the intima, proliferation of smooth muscle cells, as well as processes of apoptosis and necrosis, accompanied by both localized and systemic inflammatory responses.1,2 Various immune cells, including monocytes, neutrophils, macrophages, T lymphocytes and endothelial cells, play important roles in the pathophysiology of this condition.3,4 By regulating the balance between pro- and anti-inflammatory responses, these cells contribute to lumen stenosis and plaque instability, influencing the progression of atherosclerosis.2,5,6
Novel inflammatory hematological indices, including the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), lymphocyte-to-monocyte ratio (LMR), systemic immune-inflammation index (SII) and systemic inflammatory response index (SIRI), have been linked to the severity and prognosis of cardiovascular and cerebrovascular diseases.7–9 Previous studies have specifically correlated SII and SIRI with the severity of coronary artery lesions and the risk of acute coronary syndrome.10,11 Furthermore, SIRI has been shown to be significantly positively correlated with the risk of stroke,12 and exhibits certain clinical value in predicting large cerebral infarctions.13 A large-scale Chinese study also revealed that SII is associated with an increased risk of both ischemic and hemorrhagic stroke.14 However, their association with the severity of intracranial and extracranial atherosclerosis remains unexplored. This study aimed to investigate the relationships of SII and SIRI with the burden of cerebral atherosclerosis, assessed by its presence, anatomical distribution, maximal stenosis severity and the number of affected arteries.
Methods
Study Population
This observational study included a cohort of 5444 patients hospitalized at Zhongnan Hospital of Wuhan University from January 1, 2017, to October 1, 2023. All participants aged over 18 years had a confirmed diagnosis of cerebral atherosclerosis or ischemic cerebrovascular disease. Patients were excluded if they had atrial fibrillation, valvular heart disease, patent foramen ovale, active malignancies, cerebral hemorrhage, subarachnoid hemorrhage, brain trauma, cerebral embolism, arterial dissection, moyamoya disease, vasculitis, intracranial aneurysms or arteriovenous malformations, intracranial space-occupying lesions, a history of cerebrovascular intervention, absence of vascular imaging assessments (including DSA, CTA, or MRA) or significant imaging artifacts, infection or stress, or incomplete clinical data (Figure 1).
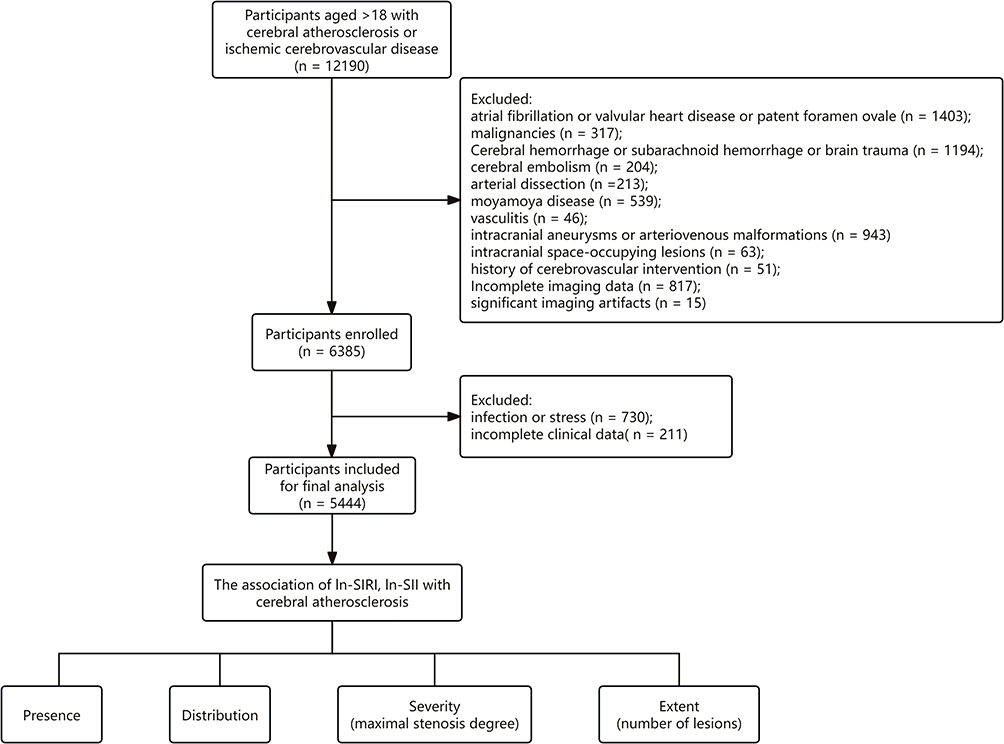 |
Figure 1 Flowchart. |
Data Collection
Data were retrospectively collected from the hospital’s electronic medical record system after obtaining ethical approval from the Institutional Review Board of Zhongnan Hospital of Wuhan University (Approval No. [2025242K]). The requirement for informed consent was waived by the Ethics Committee due to the retrospective nature of this study. Demographic information included age and gender. Comorbidities, such as hypertension, diabetes mellitus, coronary heart disease and hyperlipidemia, were identified using International Classification of Diseases (ICD) codes. Laboratory parameters were obtained from the first blood samples drawn after hospital admission, including complete blood count, lipid profile, tests of hepatic and renal function, blood glucose and coagulation.
Imaging Indicators and Analysis
The intracranial arterial system was defined to include the anterior, middle and posterior cerebral artery, the intracranial segment of the internal carotid artery (C6–C7), the V4 segment of the vertebral artery and the basilar artery. The extracranial arterial system comprised the common carotid artery, the extracranial internal carotid artery (C1–C5), the V1-V3 segment of the vertebral artery and the subclavian artery.
The degree of arterial stenosis was quantified using established methodologies. Extracranial stenosis was assessed according to the North American Symptomatic Carotid Endarterectomy Trial (NASCET) criteria,15 while intracranial stenosis was evaluated following the Warfarin-Aspirin Symptomatic Intracranial Disease (WASID) study protocol.16 For both, the stenosis percentage was calculated using the following formula: Stenosis (%)= [(Dn − Ds)/Dn] × 100%, where Ds was the diameter at the narrowest point of stenosis. The reference diameter Dn was defined as the diameter of the distal normal vessel for extracranial arteries (NASCET) and the diameter of the proximal normal segment for intracranial arteries (WASID).15,16
To comprehensively assess the atherosclerotic burden, a semi-quantitative scoring system was applied. Each arterial segment was graded from 0 to 4 based on its maximum stenosis: 0 (no plaque), 1 (plaque with <50% stenosis), 2 (50–69% stenosis), 3 (70–99% stenosis) and 4 (total occlusion).17 The overall atherosclerotic burden was evaluated based on two parameters: the maximum stenosis score, which reflected the severity of cerebral atherosclerosis and the number of arterial sites with stenosis ≥50%, which indicated the extent. All imaging analyses were conducted independently by two clinicians blinded to the clinical data.
Definition
The presence of stenosis was defined as ≥50% luminal narrowing in any of the assessed intracranial or extracranial arteries. Based on the anatomical distribution, patients were categorized into one of four groups:
The systemic inflammatory response index (SIRI) and systemic immune-inflammation index (SII) were calculated as follows:
Statistical Analysis
Prior to analysis, SIRI and SII underwent natural logarithm transformation (ln-SIRI, ln-SII) to approximate a normal distribution and reduce the impact of outliers for primary parametric analyses. Participants were categorized into quartiles based on the log-transformed values of SIRI and SII to align with the scale used in subsequent regression analyses.
Continuous variables were presented as mean ± standard deviation or medians (interquartile ranges, IQR) based on their distribution, which was assessed by the Kolmogorov–Smirnov test. Group comparisons across quartiles were performed using one-way ANOVA for normally distributed variables or the Kruskal–Wallis test otherwise, with the Mann–Whitney U-test for pairwise comparisons as needed. Categorical variables were summarized as numbers (percentages) and compared using the chi-square test.
Binary logistic regression was used to assess the associations of ln-SIRI and ln-SII with the presence of atherosclerotic stenosis, while ordered logistic regression was used to evaluate their relationships with the severity and extent of stenosis. Adjusted covariates were selected based on univariate significance (p ≤ 0.05; see Supplementary Table S1) or established clinical relevance in previous studies. Multicollinearity among covariates was evaluated using the variance inflation factor (VIF), with a threshold of VIF < 10 indicating acceptable collinearity.
Restricted cubic splines were constructed to flexibly model and visualize the non-linear relationship. Subgroup analyses evaluated the consistency of the associations. Additionally, ROC analysis assessed discriminatory ability. Sensitivity analyses were conducted by excluding patients with specific conditions to verify the robustness of the primary findings.
A two-tailed p-value  0.05 was considered statistically significant. All analyses were performed using Python (version 3.11.7) and R (version 4.5.1).
0.05 was considered statistically significant. All analyses were performed using Python (version 3.11.7) and R (version 4.5.1).
Results
Baseline Characteristics
The study included 5444 patients with a median age of 65 years (IQR 57–72) and 65.1% were male. Of these, 3176 patients (58%) presented with cerebral atherosclerotic stenosis. Baseline characteristics stratified by the presence of stenosis were summarized in Supplementary Table S1.
As shown in Table 1, higher quartiles of ln-SIRI were significantly associated with an increased proportion of males, a greater prevalence of atherosclerotic stenosis and symptomatic stroke, as well as increased levels of creatinine, D-dimer and fibrinogen. Similarly, elevated ln-SII was associated with an increased burden of atherosclerotic stenosis and stroke, alongside rising levels of creatinine, glucose, D-dimer and fibrinogen (Table 2). Specifically, coronary heart disease showed no significant association with ln-SIRI, whereas the prevalence of coronary heart disease, diabetes mellitus and hyperlipidemia did not differ significantly across ln-SII groups. Notably, superoxide dismutase (SOD) levels exhibited a decreasing trend with elevating ln-SIRI and ln-SII levels.
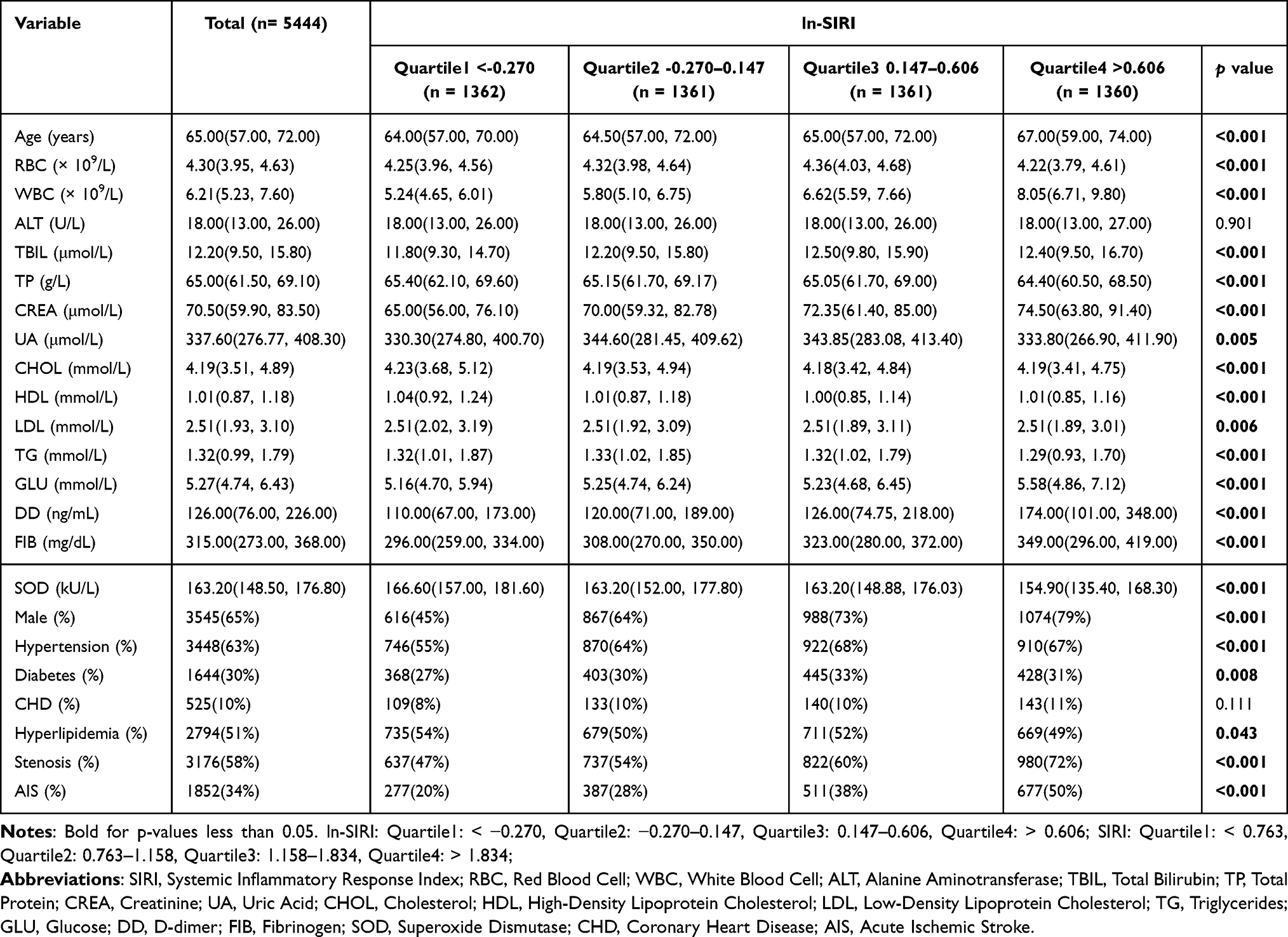 |
Table 1 Clinical Characteristics of Participants According to Ln-SIRI Quartile |
 |
Table 2 Clinical Characteristics of Participants According to Ln-SII Quartile |
Association Between Ln-SIRI, Ln-SII and the Risk of Cerebral Artery Stenosis
Levels of ln-SIRI and ln-SII were significantly elevated in patients with cerebral artery stenosis compared to those without. Furthermore, acute stroke was associated with higher levels of both indices, irrespective of the presence of atherosclerotic stenosis (Figure 2A and D). After adjusting for covariates, logistic regression analysis revealed a significant, dose-dependent increase in the odds of stenosis with rising ln-SIRI levels (OR: 1.27, 95% CI: 1.19–1.35; ORQuartile4: 1.95, 95% CI: 1.64–2.33; p for trend < 0.001; Table 3). A similar positive association was observed for ln-SII (OR: 1.22, 95% CI: 1.15–1.30; ORQuartile4: 1.71, 95% CI: 1.45–2.03; p for trend < 0.001; Table 3). Restricted cubic spline analyses confirmed a linear, positive correlation between both indices and stenosis risk (Figure 2B and E). Of note, this association remained significant in the subgroup of patients with acute stroke (Figure 2C, F and Figure S1).
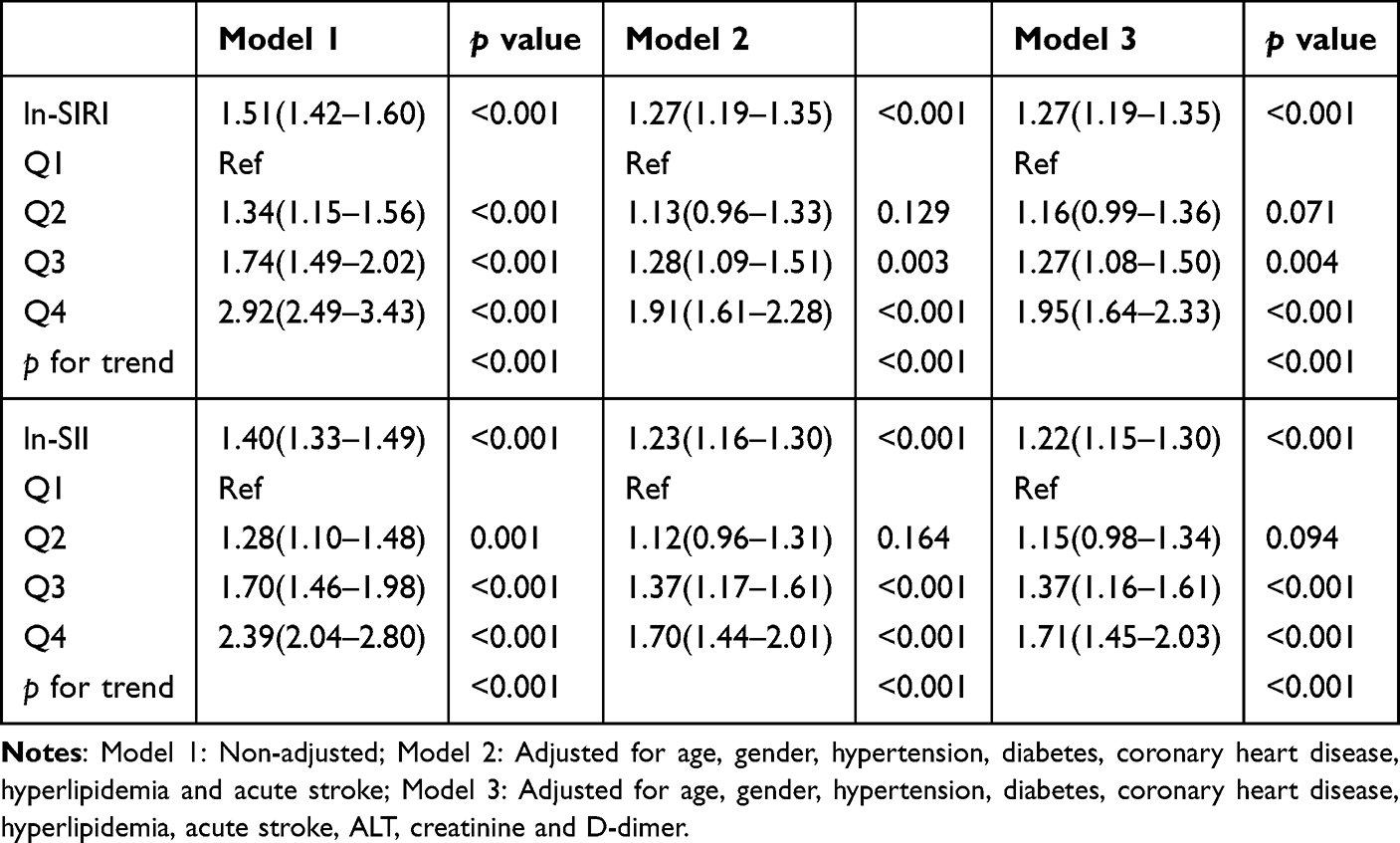 |
Table 3 Binomial Logistic Regression Analysis for the Correlations of Ln-SIRI, Ln-SII with Presence of Cerebral Artery Stenosis |
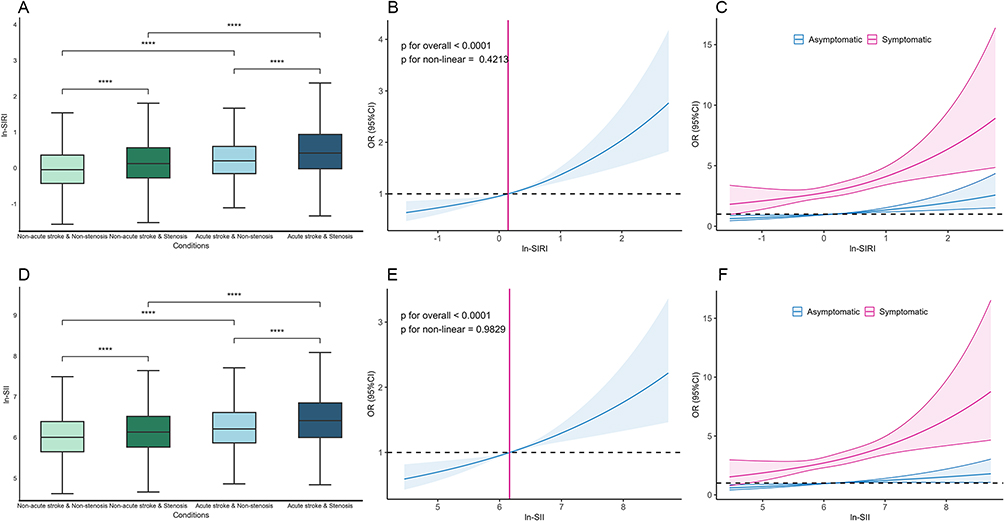 |
Figure 2 Association between ln-SIRI, ln-SII and presence of any cerebral artery stenosis. Distribution of ln-SIRI (A) and ln-SII (D) across four clinical groups based on symptomatic stroke status and stenosis presence (≥50%). Restricted cubic spines (RCS) analysis of the relationship between ln-SIRI (B), ln-SII (E) and risk of cerebral artery stenosis, adjusted for age, gender, hypertension, diabetes, coronary heart disease, hyperlipidemia, ALT, creatinine and D-dimer. RCS analysis of ln-SIRI (C) and ln-SII (F) with stenosis risk stratified by symptomatic stroke status, with the same covariate adjustments. p-value annotation legend: ns: 0.05 < p ≤ 1; *: 0.01 < p ≤ 0.05; **: 0.001 < p ≤ 0.01; ***: 0.0001 < p ≤ 0.001; ****: p ≤ 0.0001. |
Association Between Ln-SIRI, Ln-SII and the Distribution of Cerebral Artery Stenosis
Levels of ln-SIRI and ln-SII were significantly higher in combined stenosis (IECAS) group compared to intracranial artery stenosis (ICAS) group or extracranial artery stenosis (ECAS) group. However, no statistically significant difference was detected between the ICAS and ECAS groups (Figure 3A and D). RCS analysis revealed that higher levels of both indices were associated with an elevated risk of stenosis in both intracranial and extracranial arteries. (Figure 3B, C, E and F). Furthermore, a consistent pattern of association was also observed stratified by anterior versus posterior circulation. In both vascular territories, the inflammatory indices were positively associated with stenosis, showed no significant difference between each other, and were highest in cases of combined stenosis. These associations were similarly reflected in RCS analyses (Figure S2).
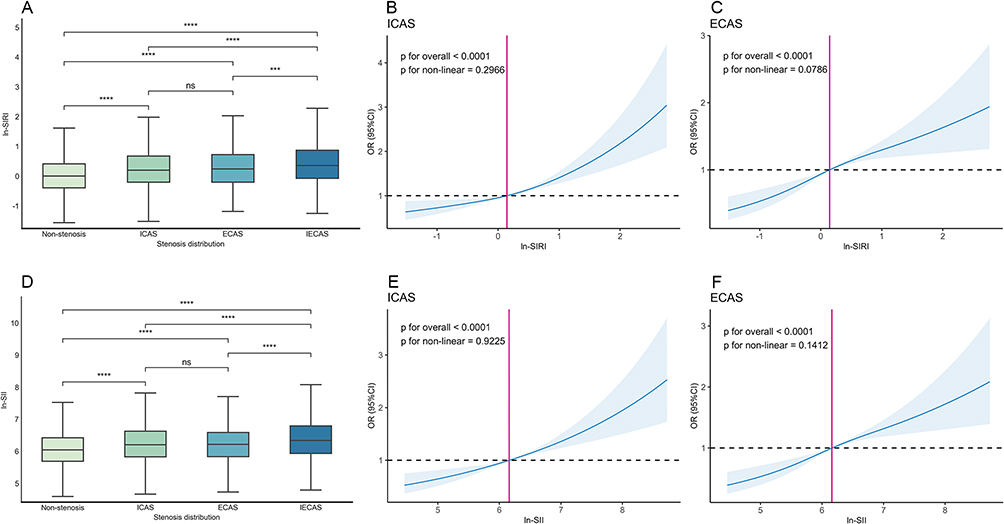 |
Figure 3 Association between ln-SIRI, ln-SII and the distribution of cerebral artery stenosis. Distribution of ln-SIRI (A) and ln-SII (D) across stenosis groups: non-stenosis, ICAS, ECAS and IECAS. Restricted cubic spline (RCS) analysis of ln-SIRI with risk of intracranial (B) and extracranial (C) artery stenosis. RCS analysis of ln-SII with risk of intracranial (E) and extracranial (F) artery stenosis. All models adjusted for age, gender, hypertension, diabetes, coronary heart disease, hyperlipidemia, acute stroke, ALT, creatinine and D-dimer. Abbreviations: Non-stenosis: no stenosis ≥50% in any artery; ICAS: ≥50% stenosis exclusively in intracranial arteries; ECAS: ≥50% stenosis exclusively in extracranial arteries; IECAS: stenosis ≥50% in both intracranial and extracranial arterial territories. p-value annotation legend: ns: 0.05 < p ≤ 1; *: 0.01 < p ≤ 0.05; **: 0.001 < p ≤ 0.01; ***: 0.0001 < p ≤ 0.001; ****: p ≤ 0.0001. |
Association Between Ln-SIRI, Ln-SII and the Severity of Cerebral Artery Stenosis
Elevated levels of both ln-SIRI and ln-SII were associated with a higher prevalence of severe stenosis or occlusion. Specifically, 60.3% of patients in the ln-SIRI Q4 group and 58.6% in the ln-SII Q4 group had severe stenosis or occlusion (Figure 4A and C). After adjustment for covariates, ordered logistic regression analysis revealed a significant, dose-dependent association between increasing levels of ln-SIRI and stenosis severity (OR: 1.29, 95% CI: 1.22–1.36; ORQuartile4: 1.91, 95% CI: 1.65–2.21; p for trend < 0.001; Table 4). A similar association was observed for ln-SII (OR: 1.26, 95% CI: 1.20–1.33; ORQuartile4: 1.78, 95% CI: 1.55–2.05; p for trend < 0.001; Table 4). Furthermore, RCS analysis indicated a positive relationship between the severity of cerebral artery stenosis and elevated ln-SIRI and ln-SII levels (Figure 4B and D).
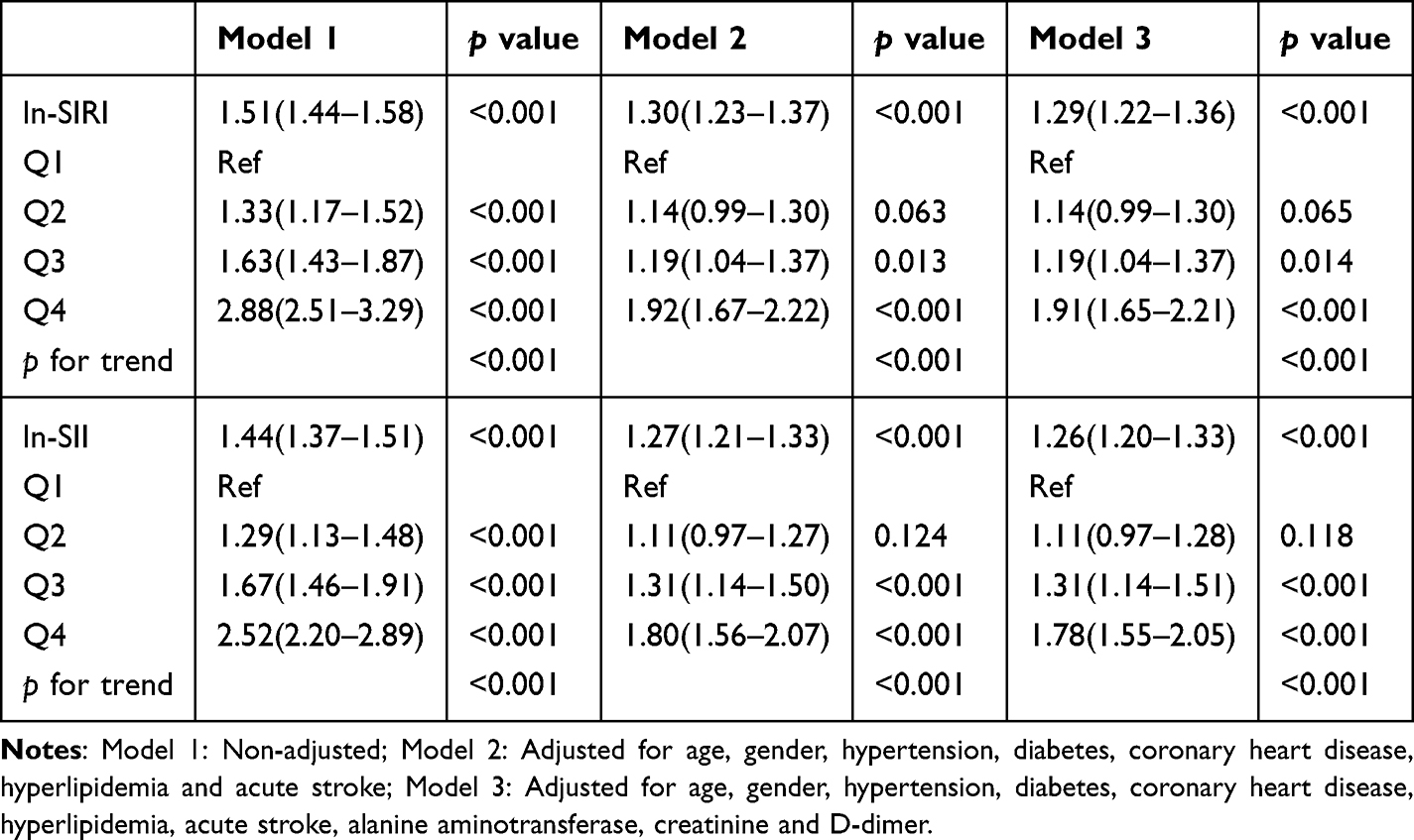 |
Table 4 Ordinal Regression Analysis for the Correlations of Ln-SIRI, Ln-SII with the Severity of Cerebral Artery Stenosis |
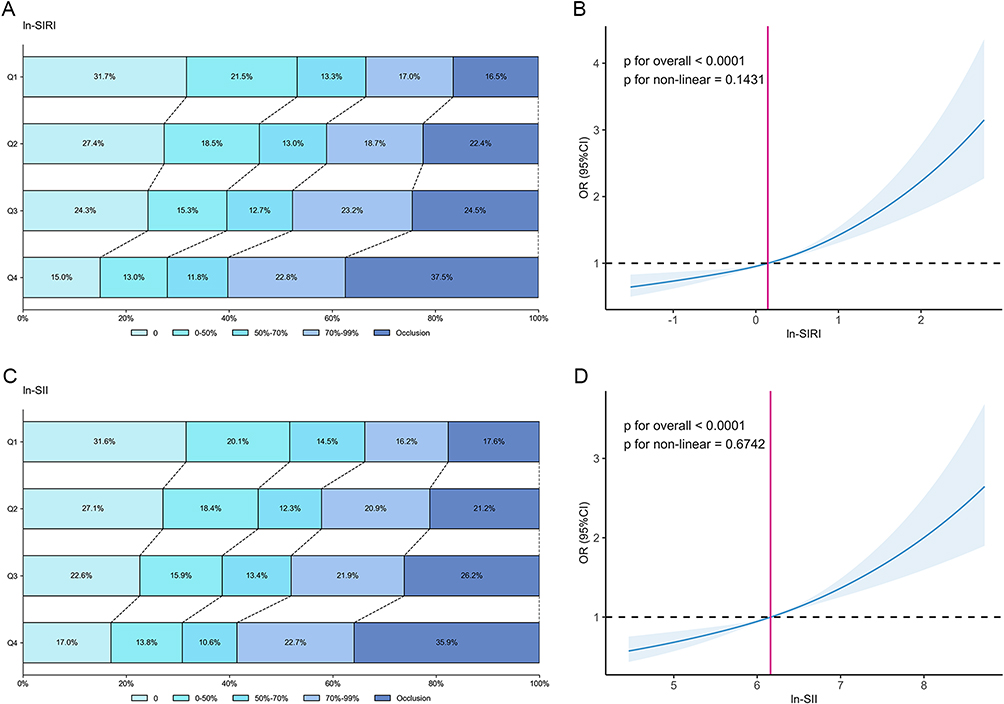 |
Figure 4 Association between ln-SIRI, ln-SII and the severity of cerebral artery stenosis. The proportions of individuals with the most severe stenosis in the interquartile grouping of ln-SIRI (A) and ln-SII (C). Restricted cubic spines analysis of the correlation between ln-SIRI (B), ln-SII (D) and the severity of cerebral artery stenosis (based on ordinal logistic regression) after adjusting for age, gender, hypertension, diabetes, coronary heart disease, hyperlipidemia, acute stroke, ALT, creatinine and D-dimer. |
Association Between Ln-SIRI, Ln-SII and the Extent of Cerebral Artery Stenosis
Higher levels of ln-SIRI and ln-SII were associated with a greater number of stenotic vessels. The proportion of patients with multi-vessel stenosis (≥3 affected sites) was highest in the top quartiles of both ln-SIRI (39.8%) and ln-SII (38.5%) (Figure 5A and C). Ordered logistic regression confirmed a significant, dose-dependent relationship. After adjustment for covariates, patients in the highest ln-SIRI quartile (Q4) had nearly twice the odds of having more extensive stenosis compared to those in the lowest quartile (Q1) (ORQuartile4: 1.82; 95% CI: 1.57–2.12; p for trend < 0.001; Table 5). A similar positive association was observed for ln-SII (ORQuartile4: 1.71; 95% CI: 1.48–1.98; p for trend < 0.001; Table 5). Restricted cubic spline analysis further supported a positive, linear relationship between the levels of both inflammatory indices and the number of stenotic sites (Figure 5B and D).
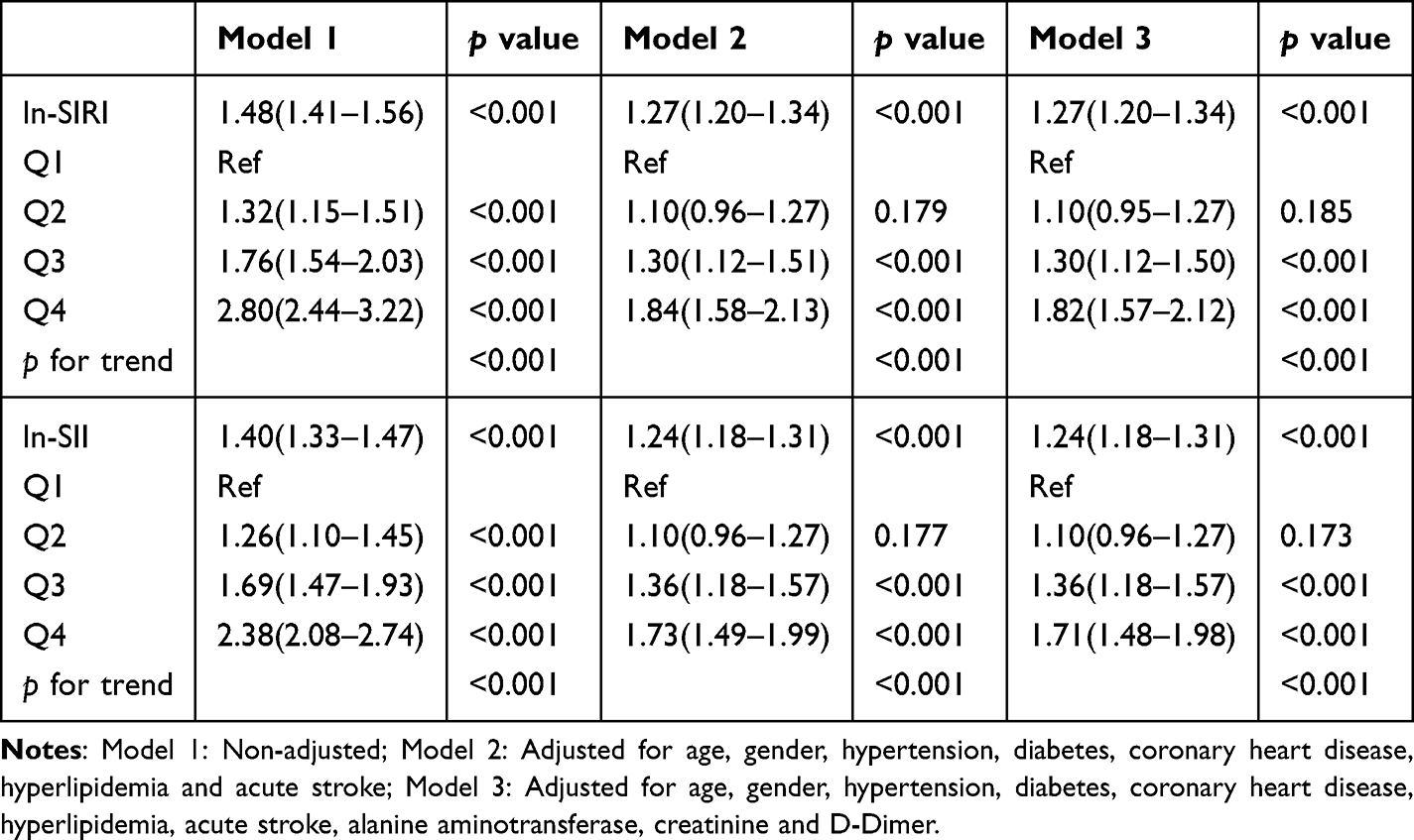 |
Table 5 Ordinal Regression Analysis for the Correlations of Ln-SIRI, Ln-SII with the Number of Locations of Cerebral Artery Stenosis |
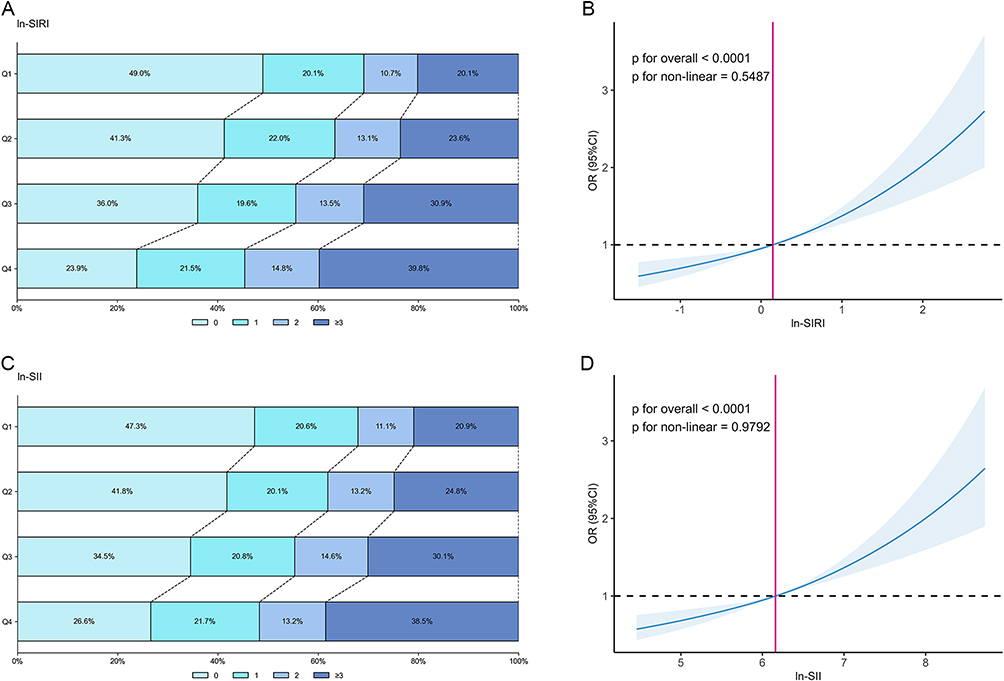 |
Figure 5 Association between ln-SIRI, ln-SII and extent of cerebral artery stenosis. The proportions of individuals with different number of stenosis in the interquartile grouping of ln-SIRI (A) and ln-SII (C). Restricted cubic spine analysis of the correlation between ln-SIRI (B), ln-SII (D) and the number of locations of cerebral artery stenosis (based on ordinal logistic regression) after adjusting for age, gender, hypertension, diabetes, coronary heart disease, hyperlipidemia, acute stroke, ALT, creatinine and D-dimer. |
Subgroup Analysis
Subgroup analyses indicated that elevated ln-SIRI and ln-SII were consistently associated with an increased risk of atherosclerotic stenosis across all subgroups (all subgroup p < 0.05; Figure 6A and B). Notably, even in the lower LDL-C subgroup (<1.8 mmol/L), ln-SIRI remained a significant risk indicator (OR: 1.46, 95% CI: 1.21–1.75). However, the association was significantly stronger in patients with higher LDL-C (≥1.8 mmol/L; OR: 1.88, 95% CI: 1.71–2.06), as indicated by a statistically significant interaction (p for interaction < 0.05).
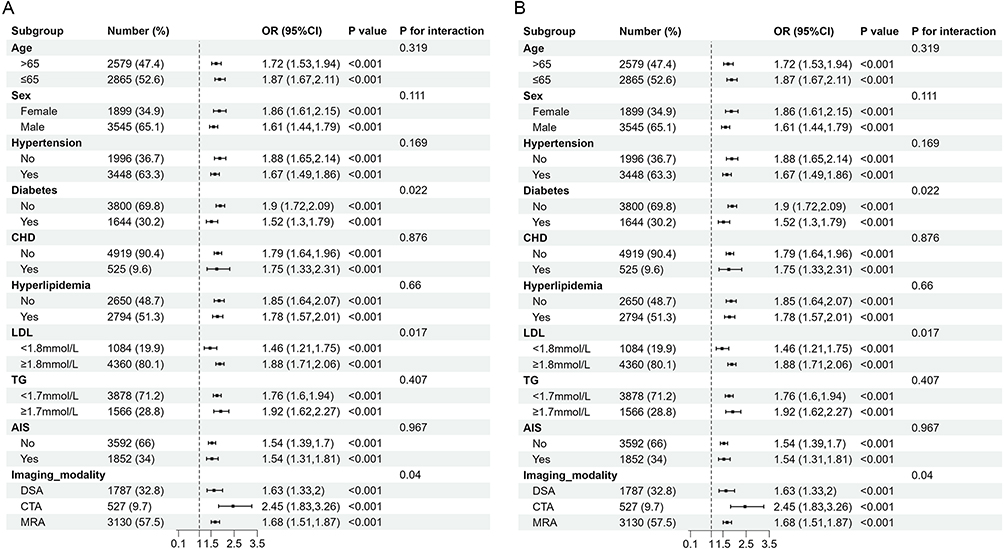 |
Figure 6 The association between ln-SIRI (A), ln-SII (B) and the presence of any cerebral artery stenosis in subgroups based on age, sex, hypertension, diabetes, coronary heart disease, hyperlipidemia, LDL, TG, acute ischemic stroke and imaging modalities. Abbreviations: CHD, coronary heart disease; AIS, acute ischemic stroke; LDL, low-density lipoprotein cholesterol; TG, triglycerides. |
ROC Analysis
The discriminatory performance of ln-SIRI and ln-SII for identifying cerebral atherosclerotic stenosis was evaluated using ROC analysis. The unadjusted AUC for ln-SIRI was 0.613 (95% CI: 0.598–0.628). After adjustment, the AUC increased to 0.699 (95% CI: 0.686–0.713) (Figure 7A). Similarly, ln-SII showed an unadjusted AUC of 0.596 (95% CI: 0.580–0.611), which improved to 0.698 (95% CI: 0.684–0.712) in the adjusted model (Figure 7B and Table S2).
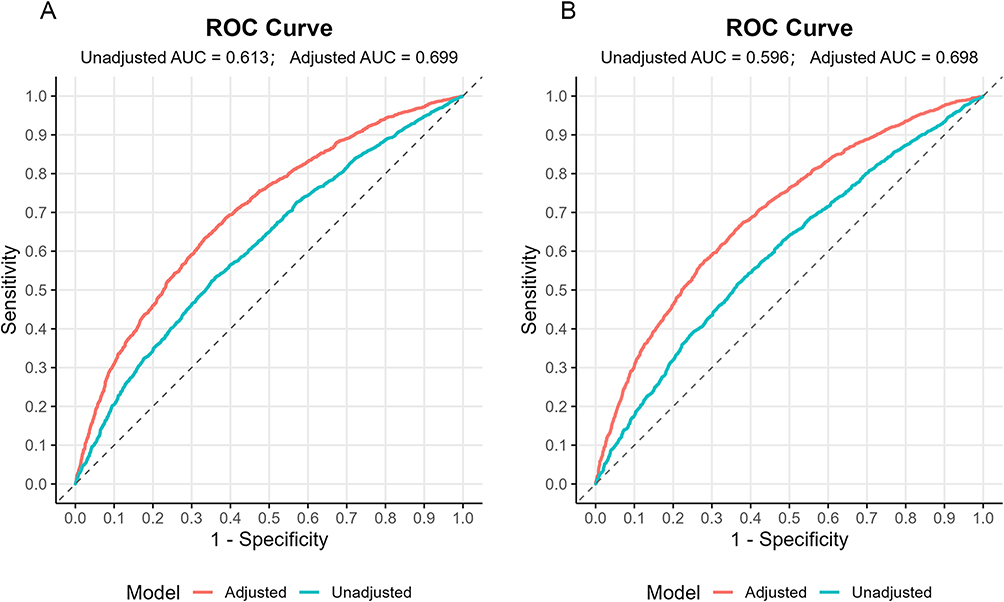 |
Figure 7 ROC curve of ln-SIRI (A), ln-SII (B) for identifying cerebral atherosclerotic stenosis before and after adjustment. The adjusted curves were derived from logistic regression models incorporating age, sex, hypertension, diabetes, coronary heart disease, hyperlipidemia, acute stroke, ALT, creatinine, and D-dimer. |
Sensitivity Analysis
To assess the robustness of our primary findings, sensitivity analyses were performed by excluding patients with acute stroke. After excluding these individuals, the associations between elevated ln-SIRI and ln-SII levels and the presence, severity, and extent of cerebral atherosclerotic stenosis remained statistically significant (Table S3). Similarly, the results did not change when we excluded participants who underwent DSA (Table S3). Notably, sensitivity analyses performed on the raw inflammatory indices (SIRI and SII, without log-transformation) also yielded significant associations (Table S4).
Discussion
This study stated that elevated levels of the systemic inflammatory biomarkers SIRI and SII are associated with the presence, severity and extent of cerebral atherosclerosis. The significant association observed even in patients without acute stroke indicates that this relationship is not merely a consequence of acute cerebral injury but is likely linked to the chronic inflammatory process of atherosclerosis itself. The positive correlations of ln-SIRI and ln-SII with both the maximum stenosis grade and the number of affected arterial sites suggested that these indices may reflect the overall burden of cerebral atherosclerosis.
SIRI and SII, as novel biomarkers of inflammation, have been demonstrated to be significantly associated with atherosclerosis and its complications.10,18 In the context of coronary artery disease, both indices have been identified as independent risk factors for coronary heart disease (CHD)19 and exhibit strong correlations with CHD severity,10,20,21 as well as all-cause mortality.22 Regarding cerebrovascular conditions, SIRI has been closely linked to carotid atherosclerosis23,24 and has shown significant correlations with functional outcomes at discharge and six months following hospitalization in patients with acute ischemic stroke.8,25 Similarly, SII is independently associated with subclinical carotid atherosclerosis24,26,27 and serves as an independent predictor for the presence of vulnerable carotid plaques.28 Moreover, SII has been found to be a predictor of the severity of large artery atherosclerosis - type strokes.29 Consistent with these prior findings, our study suggested that ln-SIRI and ln-SII are strongly associated with the presence of stenosis in both intracranial and extracranial arteries. Importantly, after excluding patients with acute stroke, which is a key confounder that elevates inflammatory markers, the association with the severity and extent of atherosclerotic stenosis persisted. Restricted cubic spline analysis further confirmed this association. This is consistent with cerebral atherosclerosis being a chronic inflammatory response and both indices can reflect the burden of cerebral atherosclerosis.
Atherosclerosis is a multifaceted chronic inflammatory process involving diverse immune cells and inflammatory mediators.30 Recent studies have identified novel serum biomarkers, such as C-X-C chemokine ligand 9, hepatocyte growth factor, resistin, stem cell factor and vascular endothelial growth factor A, that are associated with intracranial atherosclerosis and the incidence of subsequent clinical events.31 However, the clinical utility of these biomarkers is often constrained by challenges in acquisition and evaluation.
In contrast, SIRI and SII, derived from peripheral blood cell counts, including monocytes, neutrophils, lymphocytes and platelets, offer greater accessibility and feasibility for dynamic clinical monitoring. Monocytes and macrophages are integral to the innate immune response in atherosclerosis. Specifically, M1 macrophages promote immune cell recruitment, inflammatory activation and plaque destabilization by secreting pro-inflammatory cytokines such as tumor necrosis factor-alpha (TNF-α), interleukin-6 (IL-6) and interleukin-1 beta (IL-1β),32 whereas M2 macrophages facilitate tissue repair and inflammation resolution via releasing anti-inflammatory mediators including interleukin-10 (IL-10) and transforming growth factor-beta (TGF-β).33 Lymphocytes, key players in adaptive immunity, modulate immune responses throughout the initiation and progression of atherosclerosis.34 Neutrophils predominantly engage in post-plaque rupture processes by facilitating the clearance of necrotic debris. Moreover, the interplay between neutrophils and activated platelets leads to the formation of neutrophil extracellular traps (NETs), which play a pivotal role in accelerating thrombotic events.30 Platelets contribute to immune cell infiltration, participate in the formation of macrophage-derived foam cells and influence cholesterol metabolism. Upon activation, platelets release platelet-activating factor (PAF), which mediates strong adhesion among platelets, leukocytes and the vascular endothelium, thereby modulating the plaque’s microenvironment.35,36
Furthermore, our study suggested that ln-SIRI and ln-SII remain significantly associated with the presence of cerebral atherosclerotic stenosis, even among patients whose LDL-C or TG levels have met guideline-recommended targets. Previous studies have established that many patients continue to harbor residual inflammatory risk despite intensive lipid-lowering therapy with high-dose statins combined with PCSK9 inhibitors.37 High-sensitivity C-reactive protein (hsCRP) has been widely used in cardiovascular and cerebrovascular research to evaluate residual inflammatory risk.38–41 Elevated hsCRP (≥2 mg/L) has been linked to a pro-inflammatory and unstable plaque phenotype in carotid arteries.42 However, recent large-scale studies suggest that SIRI and SII perform comparably to or even better than CRP in predicting adverse cardiovascular and cerebrovascular events.43 Among hsCRP, inflammatory burden index (IBI), NLR, and SIRI, SIRI was the only index independently associated with stroke.44 Moreover, SII has been identified as an independent predictor of long-term outcomes in patients after carotid stent implantation, outperforming CRP in predictive accuracy.45 Compared with CRP, SIRI and SII integrate multiple hematological parameters, providing a more systematic and comprehensive assessment of inflammatory status. Both indices can be derived from routine complete blood counts, offering clear advantages in accessibility, simplicity, and low cost. Nevertheless, standardized cut-off values for SIRI and SII have yet to be established, and validation data remain limited. Further studies are needed to refine and validate these promising inflammatory biomarkers.
ROC analysis suggested that ln-SIRI and ln-SII were associated with AUC values of 0.699 and 0.698, respectively, with corresponding cut-offs of 0.56 for ln-SIRI and 6.254 for ln-SII. They could potentially serve as adjunctive tools to complement conventional risk stratification. For individuals exceeding these thresholds, enhanced monitoring may be considered. Additionally, during follow-up, an observed upward trend in these markers might serve as a dynamic, early-warning signal.
This study possesses several notable strengths. Its substantial sample size enhances the statistical power and robustness of the findings. Furthermore, to our knowledge, it represents the first systematic evaluation of the associations of SIRI and SII with the presence and severity of both intracranial and extracranial atherosclerosis, providing novel evidence clarifying the link between systemic inflammation and atherosclerotic burden.
Several limitations should also be considered. The single-center retrospective, cross-sectional design may limit the generalizability of our findings to broader populations and restrict causal inference. Although we adjusted for key clinical and laboratory variables, residual confounding from unmeasured or inaccurately recorded factors, such as detailed lifestyle habits (smoking, alcohol consumption) and specific medication use (statins, NSAIDs), cannot be ruled out. Moreover, the use of different imaging modalities may introduce variability due to their differing sensitivities and specificities, although sensitivity analyses indicated that our main findings remained robust. Finally, the log-transformation applied to SIRI and SII, while statistically appropriate for handling skewed data, may compress differences at higher values and implies a nonlinear relationship with the outcome, a point that warrants attention in clinical interpretation. Future multicenter, prospective cohort studies with longitudinal monitoring of SIRI and SII are warranted to validate these findings, establish their prognostic utility and elucidate their temporal relationship with the progression of cerebrovascular atherosclerosis.
Conclusion
In conclusion, ln-SIRI and ln-SII were significantly associated with the presence, severity and extent of cerebral atherosclerosis. Regular assessment of ln-SIRI and ln-SII levels may potentially improve the early identification and proactive management of high-risk individuals. Further prospective studies are needed to validate their clinical utility.
Abbreviations
SIRI, systemic inflammatory response index; SII, systemic immune-inflammation index; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; LMR, lymphocyte-to-monocyte ratio; DSA, digital subtraction angiography; CTA, computed tomography angiography; MRA, magnetic resonance angiography; RCS, restricted cubic spline; ICAS, Intracranial atherosclerotic stenosis; ECAS, Extracranial atherosclerotic stenosis; IECAS, Combined intracranial and extracranial stenosis; IQR, interquartile ranges; OR Odds ratio; CI, Confidence interval; LDL-C, low-density lipoprotein cholesterol; SOD, superoxide dismutase; CHD, coronary heart disease.
Data Sharing Statement
The datasets used and/or analyzed in this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This study was conducted in accordance with the principles of the Declaration of Helsinki. This retrospective study was reviewed and approved by the Clinical Research Ethics Committee of Zhongnan Hospital of Wuhan University (Ref. No.[2025242K]). Written informed consent for participation was not required for this study in accordance with the institutional requirements.
Author Contributions
CY: Conceptualization, Methodology, Formal analysis, Investigation, Data Curation, Writing - Original Draft, Visualization; QC: Conceptualization, Methodology, Investigation, Data Curation, Writing - Review & Editing; YX: Investigation, Writing - Review & Editing; LL: Investigation, Data Curation, Writing - Original Draft; YH: Investigation, Writing - Original Draft; RZ: Investigation, Writing - Review & Editing; YL: Conceptualization, Writing - Review & Editing, Supervision. All authors have agreed on the final version submitted for publication; agreed on the journal to which the article has been submitted and agree to be accountable for all aspects of the work.
Funding
The study did not receive any funding.
Disclosure
The authors declare no competing interests.
References
1. Herrero-Fernandez B, Gomez-Bris R, Somovilla-Crespo B, Gonzalez-Granado JM. Immunobiology of atherosclerosis: a complex net of interactions. Int J Mol Sci. 2019;20(21):5293. doi:10.3390/ijms20215293
2. Bäck M, Yurdagul A, Tabas I, Öörni K, Kovanen PT. Inflammation and its resolution in atherosclerosis: mediators and therapeutic opportunities. Nat Rev Cardiol. 2019;16(7):389–15. doi:10.1038/s41569-019-0169-2
3. Mehu M, Narasimhulu CA, Singla DK. Inflammatory cells in atherosclerosis. Antioxidants. 2022;11(2):233. doi:10.3390/antiox11020233
4. Su C, Lu Y, Wang Z, et al. Atherosclerosis: the involvement of immunity, cytokines and cells in pathogenesis, and potential novel therapeutics. Aging Dis. 2023;14(4):1214–1242. doi:10.14336/AD.2022.1208
5. Saba L, Cau R, Vergallo R, et al. Carotid artery atherosclerosis: mechanisms of instability and clinical implications. Eur Heart J. 2025;46(10):904–921. doi:10.1093/eurheartj/ehae933
6. Gusev E, Sarapultsev A. Atherosclerosis and inflammation: insights from the theory of general pathological processes. Int J Mol Sci. 2023;24(9):7910. doi:10.3390/ijms24097910
7. Rajakumar HK, Coimbatore Sathyabal V, Vasanthan M, Dasarathan R. The predictive role of Systemic Inflammation Response Index (SIRI), Neutrophil-Lymphocyte Ratio (NLR), and Platelet-Lymphocyte Ratio (PLR) in the prognosis of acute coronary syndrome in a tertiary care hospital. Heliyon. 2024;10(20):e39029. doi:10.1016/j.heliyon.2024.e39029
8. Zhang YX, Shen ZY, Jia YC, et al. The association of the neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, lymphocyte-to-monocyte ratio and systemic inflammation response index with short-term functional outcome in patients with acute ischemic stroke. J Inflamm Res. 2023;16:3619–3630. doi:10.2147/JIR.S418106
9. Liu H, Wang P, Wu LH, et al. Evaluating immune-inflammatory indices for risk stratification in cardiovascular disease: an umbrella review of systematic reviews and meta-analyses. Diagnostics. 2025;15(22):2862. doi:10.3390/diagnostics15222862
10. Dziedzic EA, Gąsior JS, Tuzimek A, et al. Investigation of the Associations of Novel Inflammatory Biomarkers—Systemic Inflammatory Index (SII) and Systemic Inflammatory Response Index (SIRI)—with the severity of coronary artery disease and acute coronary syndrome occurrence. IJMS. 2022;23(17):9553. doi:10.3390/ijms23179553
11. Dong W, Gong Y, Zhao J, Wang Y, Li B, Yang Y. A combined analysis of TyG index, SII index, and SIRI index: positive association with CHD risk and coronary atherosclerosis severity in patients with NAFLD. Front Endocrinol. 2024;14:1281839. doi:10.3389/fendo.2023.1281839
12. Tian A, Zheng Y, Jin J, Huang C. Association of systemic inflammatory response index and stroke: a cross-sectional study of NHANES, 2005-2018. Front Neurol. 2025;16:1538352. doi:10.3389/fneur.2025.1538352
13. Jiao YX, Mu SZ, Kang B. Association between systemic inflammation response index and large hemispheric infarction: development of a predictive diagnostic model - A retrospective study. J Inflamm Res. 2025;18:11951–11962. doi:10.2147/JIR.S537552
14. Xu M, Chen R, Liu L, et al. Systemic immune-inflammation index and incident cardiovascular diseases among middle-aged and elderly Chinese adults: the Dongfeng-Tongji cohort study. Atherosclerosis. 2021;323:20–29. doi:10.1016/j.atherosclerosis.2021.02.012
15. North American Symptomatic Carotid Endarterectomy Trial. Methods, patient characteristics, and progress. Stroke. 1991;22(6).
16. Ob S, Gj J, Mj L, Ha S, Mi C. A standardized method for measuring intracranial arterial stenosis. AJNR Am J Neuroradiol. 2000;21(4).
17. Kong Q, Ma X, Wang C, Du X, Ren Y, Wan Y. Total atherosclerosis burden of baroreceptor-resident arteries independently predicts blood pressure dipping in patients with ischemic stroke. Hypertension. 2020;75(6):1505–1512. doi:10.1161/HYPERTENSIONAHA.120.15036
18. Tang J, xin LT, Deng L, Cheng HX, Yuan HP, Zhao H. Inflammatory indices AISI and SIRI in atherosclerosis risk stratification: validation across community and intensive care populations. Annals Med. 2025;57(1):2530792. doi:10.1080/07853890.2025.2530792
19. Ramezankhani A, Tohidi M, Hadaegh F. Association between the systemic immune-inflammation index and metabolic syndrome and its components: results from the multi-ethnic study of atherosclerosis (Mesa). Cardiovasc Diabetol. 2025;24(1):78. doi:10.1186/s12933-025-02629-4
20. Candemir M, Kiziltunç E, Nurkoç S, Şahinarslan A. Relationship between systemic immune-inflammation index (SII) and the severity of stable coronary artery disease. Angiology. 2021;72(6):575–581. doi:10.1177/0003319720987743
21. Liu Y, Ye T, Chen L, et al. Systemic immune-inflammation index predicts the severity of coronary stenosis in patients with coronary heart disease. Coron Artery Dis. 2021;32(8):715–720. doi:10.1097/MCA.0000000000001037
22. Duan C, Du Y, Chen J, Shi S, Zhang X, Hu Y. Dynamic and static effects of the systemic inflammatory response index on all-cause mortality in individuals with atherosclerotic cardiovascular disease: evidence from national health and nutrition examination survey. Mediators Inflamm. 2025;2025:5343213. doi:10.1155/mi/5343213
23. Chen Q, Che M, Shen W, Shao L, Yu H, Zhou J. Comparison of the early warning effects of novel inflammatory markers SIRI, NLR, and LMR in the inhibition of carotid atherosclerosis by testosterone in middle-aged and elderly han chinese men in the real world: a small sample clinical observational study. Am J Mens Health. 2023;17(3):15579883231171462. doi:10.1177/15579883231171462
24. Wang L, Ji J, Wang J, et al. Associations between inflammatory markers and carotid plaques in CKD: mediating effects of eGFR-a cross-sectional study. BMC Nephrol. 2024;25(1):374. doi:10.1186/s12882-024-03826-1
25. Zhu F, Wang Z, Song J, Ji Y. Correlation analysis of inflammatory markers with the short-term prognosis of acute ischaemic stroke. Sci Rep. 2024;14(1):17772. doi:10.1038/s41598-024-66279-4
26. Wang W, Guo XL, Qiu XP, Yu YJ, Tu M. Systemic immune-inflammation index mediates the association between metabolic dysfunction-associated fatty liver disease and sub-clinical carotid atherosclerosis: a mediation analysis. Front Endocrinol. 2024;15:1406793. doi:10.3389/fendo.2024.1406793
27. Çırakoğlu ÖF, Yılmaz AS. Systemic immune-inflammation index is associated with increased carotid intima-media thickness in hypertensive patients. Clin Exp Hypertens. 2021;43(6):565–571. doi:10.1080/10641963.2021.1916944
28. Zhang L, Xu X, Zhang X, Jiang S, Hui P. Systemic immune-inflammation index is associated with ulcerative plaque in patients with acute ischemic stroke: a single center exploratory study. J Clin Ultrasound. 2024;52(3):295–304. doi:10.1002/jcu.23632
29. Liu K, Yang L, Liu Y, et al. Systemic immune-inflammation index (SII) and neutrophil-to-lymphocyte ratio (NLR): a strong predictor of disease severity in large-artery atherosclerosis (LAA) stroke patients. JIR. 2025;18:195–202. doi:10.2147/JIR.S500474
30. Xing Y, Lin X. Challenges and advances in the management of inflammation in atherosclerosis. J Adv Res. 2025;71:317–335. doi:10.1016/j.jare.2024.06.016
31. Yang D, Liu M, Khasiyev F, et al. Immune markers are associated with asymptomatic intracranial large artery stenosis and future vascular events in NOMAS. Stroke. 2023;54(12):3030–3037. doi:10.1161/STROKEAHA.123.044237
32. Zhang L, Li J, Kou Y, et al. Mechanisms and treatment of atherosclerosis: focus on macrophages. Front Immunol. 2024;15:1490387. doi:10.3389/fimmu.2024.1490387
33. Kim KW, Ivanov S, Williams JW. Monocyte recruitment, specification, and function in atherosclerosis. Cells. 2020;10(1):15. doi:10.3390/cells10010015
34. Jones PW, Mallat Z, Nus M. T-Cell/B-Cell interactions in atherosclerosis. Arterioscler Thromb Vasc Biol. 2024;44(7):1502–1511. doi:10.1161/ATVBAHA.124.319845
35. Kong P, Cui ZY, Huang XF, Zhang DD, Guo RJ, Han M. Inflammation and atherosclerosis: signaling pathways and therapeutic intervention. Signal Transduct Target Ther. 2022;7(1):131. doi:10.1038/s41392-022-00955-7
36. Nording H, Baron L, Langer HF. Platelets as therapeutic targets to prevent atherosclerosis. Atherosclerosis. 2020;307:97–108. doi:10.1016/j.atherosclerosis.2020.05.018
37. Ridker PM, Bhatt DL, Pradhan AD, et al. Inflammation and cholesterol as predictors of cardiovascular events among patients receiving statin therapy: a collaborative analysis of three randomised trials. Lancet. 2023;401(10384):1293–1301. doi:10.1016/S0140-6736(23)00215-5
38. Su BJ, Dong Y, Tan CC, et al. Elevated Hs-CRP levels are associated with higher risk of intracranial arterial stenosis. Neurotox Res. 2020;37(2):425–432. doi:10.1007/s12640-019-00108-9
39. Zhang N, Xiang Y, Zhao Y, et al. Association of triglyceride-glucose index and high-sensitivity C-reactive protein with asymptomatic intracranial arterial stenosis: a cross-sectional study. Nutr Metab Cardiovasc Dis. 2021;31(11):3103–3110. doi:10.1016/j.numecd.2021.07.009
40. Liu H, Wang M, Xiang X, et al. Association of residual inflammatory risk with stroke recurrence in patients with acute ischaemic stroke or transient ischaemic attack. Eur J Neurol. 2022;29(8):2258–2268. doi:10.1111/ene.15344
41. Yu Y, Pan Y, Lou Y, et al. Residual inflammatory risk predicts long-term outcomes following stenting for symptomatic intracranial atherosclerotic stenosis. Stroke Vasc Neurol. 2024;9(4):407–417. doi:10.1136/svn-2023-002421
42. Kraaijenhof JM, Mol BM, Nurmohamed NS, et al. Plasma C-reactive protein is associated with a pro-inflammatory and adverse plaque phenotype. Atherosclerosis. 2024;396:118532. doi:10.1016/j.atherosclerosis.2024.118532
43. Qin P, Ho FK, Celis-Morales CA, Pell JP. Association between systemic inflammation biomarkers and incident cardiovascular disease in 423,701 individuals: evidence from the UK biobank cohort. Cardiovasc Diabetol. 2025;24(1):162. doi:10.1186/s12933-025-02721-9
44. Valibeygi A, Fardaei M, Niknejad S. Association between stroke and systemic inflammation response index (SIRI): a national health and nutrition examination survey (NHANES) study 2015-2020. BMJ Neurol Open. 2025;7(1):e000718. doi:10.1136/bmjno-2024-000718
45. Morikawa S, Okumura K, Inoue N, Ogane T, Takayama Y, Murohara T. Systemic immune-inflammation index as a predictor of prognosis after carotid artery stenting compared with C-reactive protein. PLoS One. 2023;18(7):e0288564. doi:10.1371/journal.pone.0288564
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Atherogenic and Inflammatory Markers in Recent Small Subcortical Infarcts: Associations with Location, Morphology, and Short-Term Recurrence
Huang C, Geng J, Fan J, Tian B, Wang K, Zhang Y, Zhou X, Zhu X, Sun Z
Journal of Inflammation Research 2025, 18:5881-5893
Published Date: 1 May 2025