Back to Journals » Nature and Science of Sleep » Volume 17

Associations of Sleep-Disordered Breathing and Insomnia with Incident Metabolic Syndrome – The Hispanic Community Health Study/Study of Latinos
Authors Wang Y, Lyu W ![]() , Feng X, Tang X
, Feng X, Tang X ![]() , Zhang Y
, Zhang Y ![]() , Ren R
, Ren R
Received 23 June 2025
Accepted for publication 14 October 2025
Published 11 November 2025 Volume 2025:17 Pages 2919—2931
DOI https://doi.org/10.2147/NSS.S546410
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sarah L Appleton
Yongming Wang, Wenqi Lyu, Xujun Feng, Xiangdong Tang, Ye Zhang, Rong Ren
Sleep Medicine Center, Mental Health Center, Department of Respiratory and Critical Care Medicine, West China Hospital, Sichuan University, Chengdu, People’s Republic of China
Correspondence: Rong Ren, Email [email protected] Ye Zhang, Email [email protected]
Introduction: Metabolic syndrome (MS) is a common disease associated with multiple cardiovascular risk factors. Sleep-disordered breathing (SDB) and insomnia are associated with several metabolic components, such as hypertension, diabetes, dyslipidemia, and obesity. Although studies have shown an association between these sleep disorders and MS, the longitudinal relationship in the US Hispanic/Latino population is still unknown. This study aimed to examine the longitudinal associations of SDB and insomnia, individually and jointly, with incident MS risk over a 6-year follow-up period in a Hispanic/Latino cohort.
Methods: We conducted Cox regression analysis in 4625 participants (mean age 44.5± 13.4 years, 60.3% women) who did not have MS at baseline, from the main Hispanic Community Health Study/Study of Latinos study, adjusting for potential covariates, such as age, sex, BMI, and smoking status. MS was defined by the NCEP ATP-III standard, and SDB (apnea–hypopnea index ≥ 5) and insomnia (Women’s Health Initiative Insomnia Rating Scale score ≥ 9) were assessed during baseline.
Results: The prevalence of incident MS with an average 6-year interval was found to be 23.6%. In the fully adjusted model, SDB showed a significant association with incident MS (HR 1.31, 95% CI 1.10– 1.56), and the comorbidity of SDB and insomnia (COMISA) was associated with an even higher risk of incident MS (HR 1.40, 95% CI 1.14– 1.72), while insomnia alone showed no significant association.
Conclusion: SDB and COMISA were associated with incident MS in the Hispanic/Latino population, and COMISA had a stronger association with MS. These findings underscore the importance of addressing sleep disorders as modifiable risk factors in the prevention and management of MS among the Hispanic/Latino population in the USA.
Keywords: sleep-disordered breathing, insomnia, metabolic syndrome, Hispanic
Introduction
Metabolic syndrome (MS) is a collection of components characterized by physiological traits, such as high blood pressure, increased levels of fasting plasma glucose, excess abdominal fat, and abnormal lipid levels.1 In recent years, research has shown that an estimated 34.7% of the population in the USA had MS, with a significant increase observed among the Hispanic population compared to other ethnic groups between 2011 and 2016.2 It is thus imperative to investigate the risk factors influencing the development of MS within the Hispanic population.
Sleep-disordered breathing (SDB) and insomnia are the two most common sleep disorders. They are highly correlated with the development of hypertension, diabetes, and dyslipidemia,3–9 as well as with obesity.10,11 As these are components of MS, a higher prevalence of sleep disorders may contribute to a higher risk of MS. Research has shown that SDB can lead to a higher prevalence of MS.12 A recent meta-analysis including 13 studies using the National Cholesterol Education Program (NCEP) Adult Treatment Panel-III (ATP-III) diagnostic criteria, with a total of 7934 participants, demonstrated a significant association between obstructive sleep apnea (OSA) and MS, independent of body mass index (BMI).13 Short sleep duration and insomnia are also significantly associated with MS.14,15 The mechanisms may include intermittent hypoxia caused by SDB, which, in turn, activates the sympathetic nervous system and increases inflammatory responses, leading to increased blood pressure and insulin resistance.16 The decline in sleep quality and sleep disruptions may affect appetite regulation and energy balance, potentially leading to weight gain and obesity.17 However, most of the previous studies were cross-sectional and conducted in non-Hispanic populations. So far, only one cross-sectional study has investigated the relationship between SDB and MS in a Hispanic/Latino population in the USA, and it found that SDB was independently associated with MS.18 Although one multi-ethnic longitudinal study, which integrated the Brazilian Episono and Swiss HypnoLaus cohorts and included 1853 participants free of MS at baseline, showed that OSA – a major subtype of SDB – is an independent risk factor for incident MS,19 it did not address the US Hispanic/Latino population or explore the role of insomnia. The longitudinal causality of SDB and insomnia with MS in the US Hispanic population is still not clear.
Furthermore, the comorbidity of SDB and insomnia, known as COMISA, is highly prevalent, with 30–40% of patients with chronic insomnia meeting the diagnostic criteria for SDB. This comorbidity may involve an interaction where each condition exacerbates the other.20 Research has indicated that COMISA may result in a greater impairment of sleep quality compared to either SDB or insomnia alone.3 Given the impact of SDB and insomnia on metabolism, we hypothesize that COMISA may contribute to a higher risk of developing MS.
Thus, we aimed to examine the longitudinal associations of SDB and insomnia, both individually and jointly, with incident MS risk in a Hispanic/Latino population in the USA, given that the Hispanic population is one of the largest ethnic groups in the USA and has a relatively high prevalence of MS and sleep disorders.2,21 Information for this investigation was obtained from the Hispanic Community Health Study/Study of Latinos (HCHS/SOL), which is the most extensive study on cardiovascular risk factors and sleep patterns within the US Hispanic/Latino community.
Method
Study Population
The HCHS/SOL is a community-based cohort study conducted in Hispanic/Latino populations in the USA. Data from the Visit 1 survey were acquired during the period 2008–2011, in which 16,415 eligible individuals were included. Information from Visit 2 was gathered between 2014 and 2017, with a focus on re-evaluating 11,623 subjects from the baseline sample. Our study utilized a sample from the HCHS/SOL main study, consisting of 12,647 participants at Visit 1 and 8816 participants at Visit 2. Both the structure and execution of this investigation have been published22,23 and approved by the institutional ethics committees of the involved organizations. Of the 8816 included Visit 2 participants, we first excluded individuals with baseline MS (n=3510), then we further excluded missing data for MS (n=39), for SDB (n=524), and for insomnia (n=118) based on the study’s exclusion criteria, yielding an analytic sample of 4625, as illustrated in Figure 1.
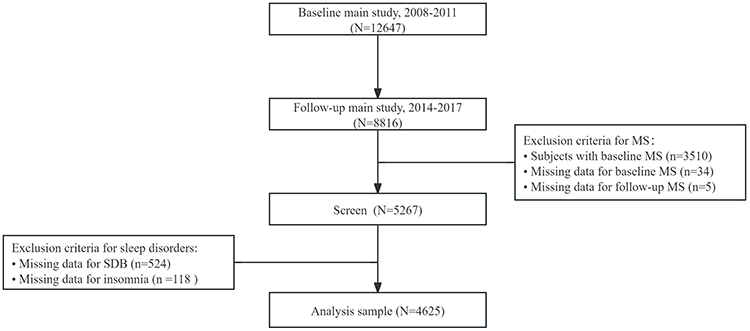 |
Figure 1 Sample flowchart. Abbreviations: SDB, sleep-disordered breathing; MS, metabolic syndrome. |
During the first visit, participants were assessed using questionnaires for sleep symptoms and a validated home sleep apnea test device, called the Apnea Risk Evaluation System (ARES), for any sleep disturbances.24,25 Trained scorers at a central sleep reading center evaluated the sleep records, remaining blinded to all additional data. Blood samples were gathered at each location following a standardized procedure and sent daily to the central laboratory for analysis. Blood samples were used to measure cholesterol levels, while fasting blood samples were collected shortly after arrival to measure fasting glucose. These indicators were then used for the subsequent diagnosis of MS.23 Every participant provided written consent prior to their involvement in the study.
Metabolic Syndrome
MS was defined by a revised NCEP ATP-III standard at baseline and Visit 2, as it is most commonly used in the clinic and is consistent with previous research. A diagnosis of MS was made in the HCHS/SOL cohort when an individual met three or more of the following criteria: average systolic blood pressure (SBP) ≥130 mmHg or average diastolic blood pressure (DBP) ≥85 mmHg or self-report of using antihypertensive medications, where the average SBP and DBP were both derived from three blood pressure measurements; fasting glucose ≥100 mg/dL or self-report of using antidiabetic medications; triglycerides ≥150 mg/dL; high-density lipoprotein (HDL) cholesterol levels <40 mg/dL for men or <50 mg/dL for women; and waist circumference ≥102 cm for men or ≥88 cm for women. We defined the number of MS components present in each participant at baseline as MS components, n. Then, we defined the incident MS as the participants who were not diagnosed with MS at Visit 1, but were diagnosed as having MS at Visit 2.
Sleep-Disordered Breathing (SDB)
SDB was measured by the Apnea Risk Evaluation System Unicorder (ARES™), which is worn on the forehead and does not require additional wires to external devices such as an oximeter probe. The instrument measures oxygen saturation (SpO2) and pulse rate from reflectance oximetry, air flow from a nasal cannula and pressure transducer, snoring levels via a calibrated acoustic microphone, and head movement actigraphy and head position from accelerometers. The ARES enables the calculation of the apnea–hypopnea index (AHI), which indicates the frequency of breathing interruptions during sleep. The AHI was calculated based on the average number of all apneas and hypopneas associated with a 3% desaturation per hour of sleep. The ARES showed consistently high sensitivity and specificity for both in-laboratory and at-home recordings.25 Furthermore, a validation study demonstrated good agreement between the AHI measured by this monitor and by polysomnography.26 In this research, SDB is defined as an AHI value equal to or greater than five events per hour.
Insomnia
The standard for assessing insomnia in our research is derived from the Women’s Health Initiative Insomnia Rating Scale (WHIIRS),27 which is a standardized tool measuring individuals’ perceived symptoms of insomnia, and was created and validated using a diverse racial and ethnic population.28 Insomnia was defined as a WHIIRS score equal to or greater than 9.
Covariates
Potential confounders, including sociodemographic factors such as age, sex, education level, and ethnic background, at baseline, were taken into account. We also adjusted for unhealthy behaviors such as alcohol and cigarette use (categorized as never use, former use, and current use) and BMI for obesity.
Statistical Analysis
The Visit 1 sample characteristics are presented as the number of subjects for categorical variables or the mean and standard deviation for continuous variables, according to four groups (control, insomnia, SDB, COMISA) (Table 1). Data were analyzed by the chi-squared and Kruskal–Wallis tests. The Visit 2 medication and laboratory data are also presented according to the four groups (Table S1). Furthermore, the sample characteristics according to subjects with or without incident MS are shown in Tables S2 and S3. The incidence rates of several components of MS during follow-up are also depicted by sex, age, and BMI using histograms (Figures S1–S3). We applied Bonferroni correction to adjust for multiple comparisons between continuous variables.
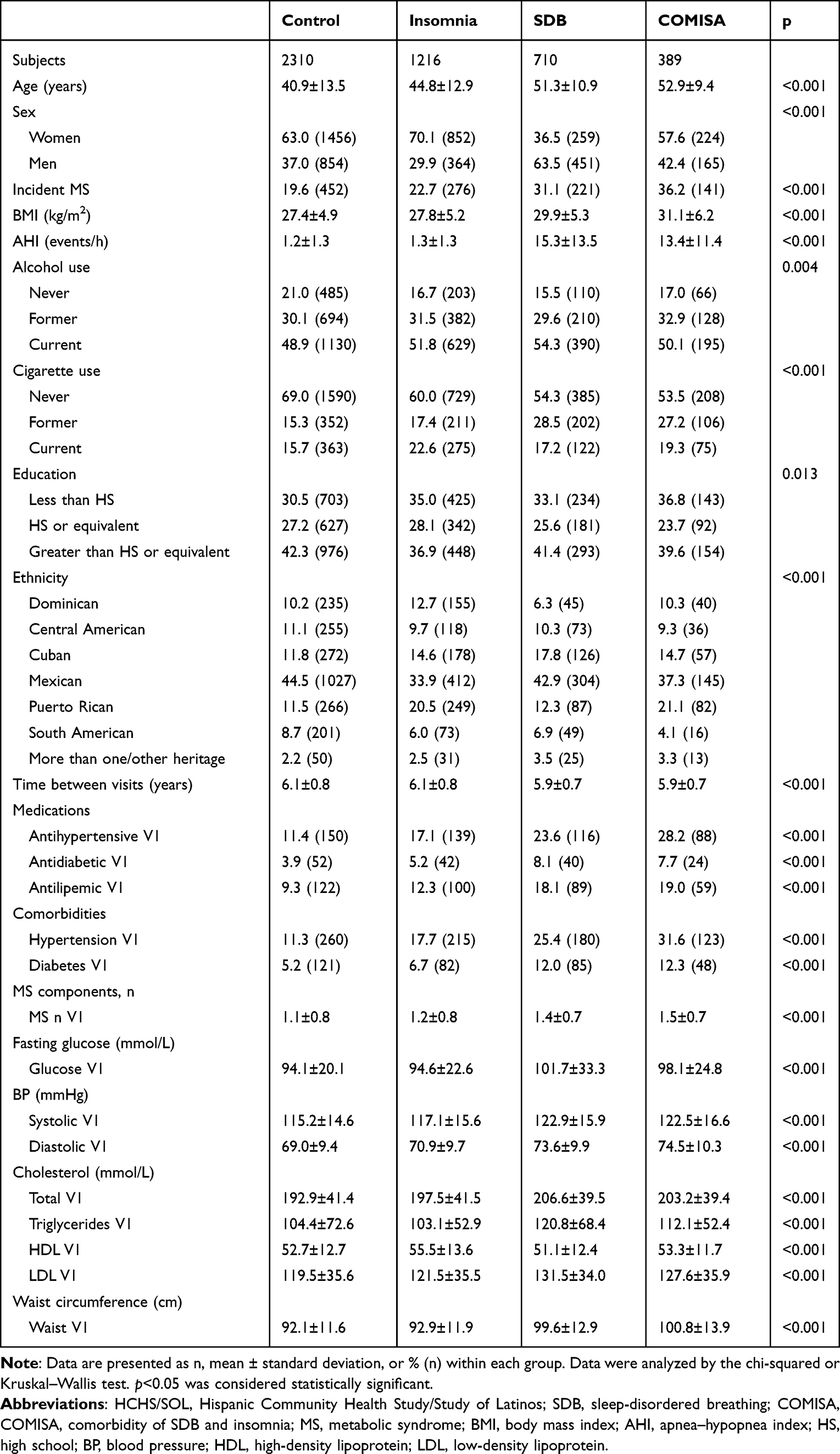 |
Table 1 HCHS/SOL (2008–2017) Sample Characteristics at Visit 1 in Different Sleep Disorders |
In the primary analyses, Cox regression models were employed to ascertain the risk of incident MS associated with SDB and insomnia at an average follow-up of 6 years, with the influence of covariates held constant. In sequential models, Model 1 controlled only for sleep disorders; Model 2 added age, sex, BMI, alcohol use, cigarette use, education, and ethnicity; and Model 3 further added MS components, n. The results of Cox regression are presented as the hazard ratio (HR) and 95% confidence interval (CI). Subgroup analysis was also conducted, considering the different severity of SDB (Table S4). We also performed tests for the proportional hazard assumption through log–log plots (Figure S7). These curves are generally parallel, suggesting that the effect of the examined factors on survival risk remained consistent across time. The survival risk for all four groups changed proportionally, and this risk ratio did not vary over time.
We performed sex-stratified analysis on the different prevalence of incident MS in women and men, and age-stratified analysis, considering that age is a major risk factor in sleep and metabolic disorders. We also conducted stratified analysis according to BMI (non-obese: BMI <28 kg/m2; obese: BMI ≥28 kg/m2). Then, the interaction terms were employed to explore possible effects. The results were represented as forest plots.
Survival analysis was performed, and Kaplan–Meier survival curves of the whole sample are presented according to the different sleep disorder groups. We also conducted this analysis in different sex, age, and BMI groups (Figures S4–S6).
All statistical analyses were conducted in SPSS 27, and all tests were two sided, with p values <0.05 being considered statistically significant.
Results
Sample Characteristics
The prevalence of incident MS over an average interval of 6 years was found to be 23.6% (n=1090). Table 1 presents the sample characteristics at baseline in the different sleep disorder groups, comprising control, insomnia, SDB, and COMISA. Among these four groups, the COMISA group exhibited the highest incidence rate (36.2%, n=141) of MS. Compared to the control group, the SDB and COMISA groups also exhibited higher mean age, BMI, prevalence of hypertension and diabetes, and antihypertensive medication use, and had more MS components and worse laboratory data, including higher fasting glucose, blood pressure, total cholesterol, triglycerides, and LDL.
Sleep Disorders and Incident Metabolic Syndrome
In the main analysis, we used Cox regression models to explore the relationship between the two sleep disorders and incident MS. Table 2 shows the adjusted HR in three models. In the fully adjusted model, insomnia was not associated with incident MS, but SDB (HR 1.31, 95% CI 1.10–1.56) and COMISA (HR 1.40, 95% CI 1.14–1.72) showed a significantly higher risk of incident MS.
 |
Table 2 Effect Estimates from Cox Regression Models for the Association Between Sleep Disorders and 6-Year Incident MS in HCHS/SOL (2008–2017) |
In Figure 2, we present fully adjusted data with forest plots. In sex-stratified analysis, insomnia showed no association with incident MS in either sex. Women showed significant associations with incident MS in the SDB and COMISA groups, but men did not have such associations in these two groups. In the age-stratified analysis, insomnia showed no significant association with incident MS in either age group. SDB was associated with incident MS only in the young group. The COMISA group showed a significant association with incident MS in both age groups. In the BMI-stratified analysis, the obese group showed a significant association with incident MS, and both non-obese and obese groups were significantly associated with incident MS in the COMISA group, while insomnia also failed to show an association.
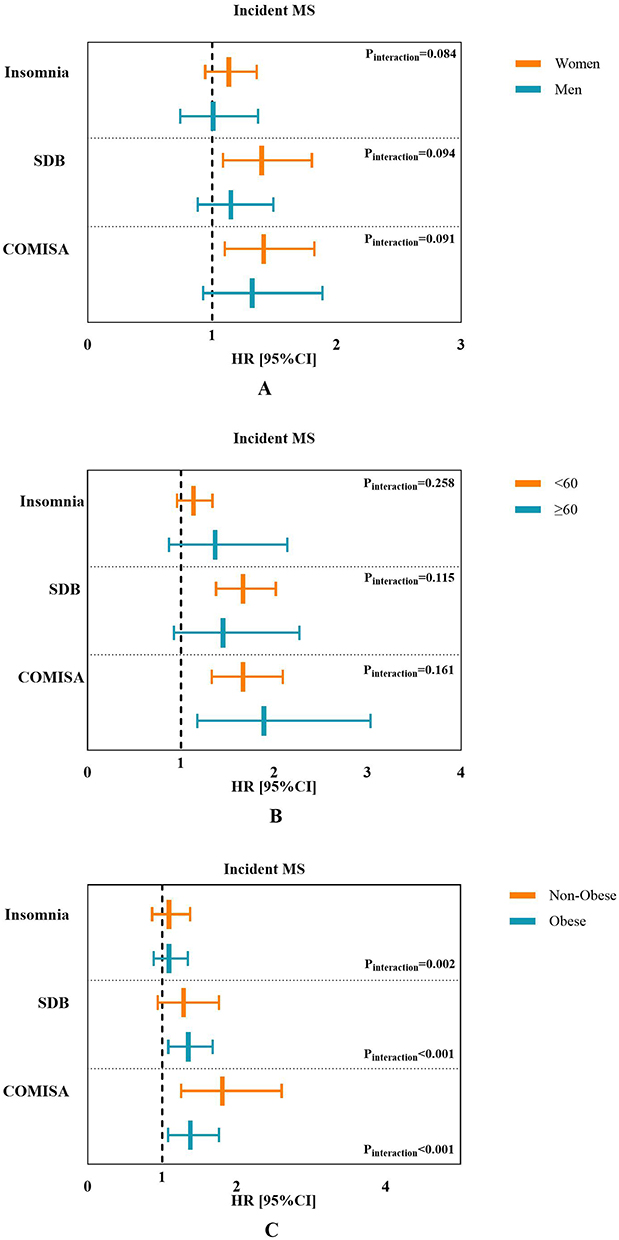 |
Figure 2 Stratified analysis on associations between SDB, insomnia, and incident MS (n=1090) from the HCHS/SOL (2008–2017) based on (A) age, (B) sex, and (C) BMI. Cox regression adjusted for age, sex, BMI, alcohol use, cigarette use, education, ethnicity, time between visits, and MS components, n. Abbreviations: SDB, sleep-disordered breathing; COMISA, comorbidity of SDB and insomnia; MS, metabolic syndrome; HCHS/SOL, Hispanic Community Health Study/Study of Latinos; BMI, body mass index; HR, hazard ratio; CI, confidence interval. |
The survival analysis for the prevalence of incident MS is shown in Figure 3. In the whole sample, the survival rate without incident MS was highest in the control group and lowest in the COMISA group. The insomnia, SDB, and COMISA groups all showed a steeper trend than the control group.
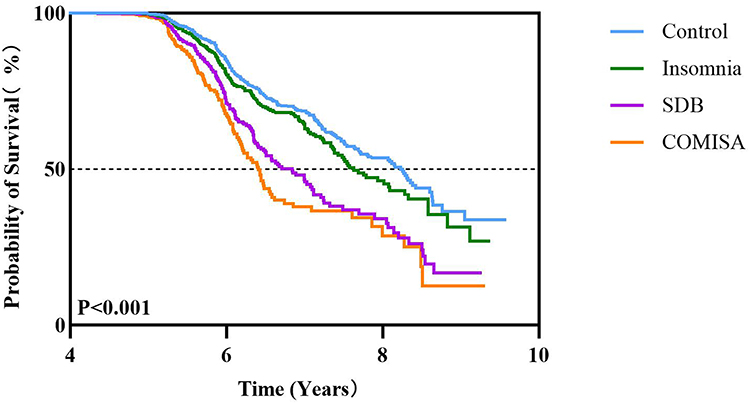 |
Figure 3 Survival analysis of incident MS prevalence from the HCHS/SOL (2011–2017). Kaplan–Meier curves from onset of MS (n=4625). Abbreviations: MS, metabolic syndrome; HCHS/SOL, Hispanic Community Health Study/Study of Latinos; SDB, sleep-disordered breathing; COMISA, comorbidity of SDB and insomnia. |
Supplementary Material
The medications and laboratory data at Visit 2 according to the four groups (control, insomnia, SDB, COMISA) demonstrated a similar trend to that in the main study, as presented in Table S1. The sample characteristics according to patients with or without incident MS showed that women were more likely to develop incident MS, and the participants who had developed incident MS had worse laboratory data (Tables S2 and S3). In the subgroup analysis for SDB, we found that only the mild (5≤AHI<15) group showed a significant association with incident MS after fully adjusting for covariates (Table S4). Besides, in the analyses of several MS components, including hypertension, diabetes, and dyslipidemia, we found that the COMISA group had the highest incidence of hypertension and diabetes, followed by SDB and insomnia (Figures S1–S3). Survival analysis in the subgroups showed that the COMISA group had the lowest rate of not having incident MS, followed by the SDB, insomnia, and control groups (Figures S4–S6).
Because continuous positive airway pressure (CPAP), the first-line treatment for SDB, may act as a potential confounding factor in the association between SDB and MS, it requires explicit consideration in our analytical framework. In our cohort, only 27 participants reported receiving CPAP therapy; thus, these 27 individuals were retained in the primary analysis to preserve statistical power and minimize the risk of introducing selection bias. However, we conducted a sensitivity analysis that excluded the 27 CPAP users to verify the robustness of our primary findings. The results showed that the association between SDB and incident MS remained statistically significant, and its magnitude was consistent with that observed in the primary analysis (Table S5). Furthermore, we analyzed the impact of insomnia with different sleep durations on MS, and the results remained negative (Table S6). We also reran the Cox regression analysis to examine the association between different severities of SDB and incident MS, and the results remained unchanged (Table S7).
Discussion
The findings of this population-based sample of Hispanic/Latino adults in the USA indicate that SDB and COMISA have significant associations with incident MS, after controlling for possible covariates. Moreover, this relationship is more obvious in women and younger people.
Previous studies exploring the relationship between SDB or insomnia and MS were mostly conducted in non-Hispanic populations. With regard to SDB, the majority of these studies found a significant relationship between SDB and MS.13,18,29,30 For example, a case–control study exploring the relationship between SDB and MS indicated that SDB is an independent risk factor for MS, with the presence of SDB showing an approximately nine-fold higher risk of having MS.29 A meta-analysis including a total of 7934 samples from 13 studies also indicated that SDB is associated with MS, independently of BMI.13 Meanwhile, a prospective association between SDB and MS was found in a cohort study from two population-based samples.19 Furthermore, a cross-sectional study using the baseline data of HCHS/SOL reported a significant association between SDB and MS in a Hispanic/Latino group.18 Our results are consistent with these studies, and further explored the association of SDB with incident MS in a cohort of the Hispanic/Latino population in the USA with an average interval of 6 years, indicating that SDB is a risk factor for the development of MS. In addition, our study found that after fully adjusting for covariates, mild SDB was significantly associated with incident MS, while moderate/severe SDB showed no significant association. This counterintuitive finding may be attributed to the demographic characteristics of our study cohort, specifically the high proportion of women (n=2791, 60.3%), a group that is well documented as having a higher prevalence of less severe SDB. To further validate this hypothesis, we conducted a sex-stratified subgroup analysis to explore the relationship between SDB severity strata and MS risk between the sexes. The results of this analysis revealed that only mild SDB in women was significantly associated with incident MS (Figure S8). This sex-specific association not only supports the role of the sex composition of the cohort in driving the primary finding but also provides a partial mechanistic insight into why moderate/severe SDB failed to show a significant association with incident MS in the overall cohort. Furthermore, this finding may also suggest reverse causality in the SDB-MS relationship. As previously discussed, SDB can disrupt multiple metabolic factors that predispose individuals to MS. However, prior work has also shown that pre-existing metabolic diseases, including components linked to MS, can trigger or worsen SDB via both weight-dependent and weight-independent physiological mechanisms.31 Such bidirectional interplay implies that reverse causality, where metabolic dysfunction precedes and modulates SDB severity, may be an additional driver of our observed associations. This may be particularly relevant to our baseline assessment, which lacked more sensitive markers of subclinical MS (eg, homeostatic model assessment of insulin resistance). However, owing to the lack of follow-up SDB data, we are unable to explore this further. Future studies should focus on the causal relationship between MS and SDB and its phenotypic differences to further explore its mechanisms. Our results also indicate that mild SDB could potentially represent a distinct pathophysiology, such as the effects of intermittent hypoxia patterns. Analysis of novel indicators such as hypoxic load may help to explain this issue; however, our current database limited this analysis. More research is needed to explore this aspect further. Considering that the prevalence of MS and SDB is significantly higher among Hispanics,2 our research highlights the importance of prevention of SDB in Hispanic/Latino groups in the USA.
Regarding insomnia, the previous literature is inconsistent. Some studies have demonstrated that insomnia and related symptoms are associated with an increased risk of MS. For example, one community study including 812 participants showed that the symptoms of insomnia, such as difficulty in falling asleep and unrefreshing sleep, instead of the syndrome definition of insomnia, are significantly associated with the development of MS,32 and one meta-analysis demonstrated a U-shaped association between sleep duration and MS, with short sleep duration being associated with MS.33 In contrast, a longitudinal study found that insomnia or short sleep duration (sleep duration <6 h) had no relationship with incident MS after adjusting for confounders.34 Our results are consistent with the latter longitudinal study, showing that insomnia exhibited no significant association with incident MS after adjusting for covariates. This inconsistency may partly be explained by the different definitions of insomnia in previous studies and the current study. The use of different insomnia criteria can contribute to the varying findings across studies. Our study utilized WHIIRS, which is a standardized tool that measures individuals’ perceived symptoms of insomnia. It was created and validated using a diverse racial and ethnic population, making it a valid tool for capturing insomnia in varied groups.28 However, the WHIIRS remains unable to fully capture the diagnostic criteria for clinical insomnia, a limitation that may explain discrepancies between our findings and those of certain prior studies. A key gap in the WHIIRS is its failure to assess daytime impairment (eg, fatigue, poor concentration, mood dysregulation). Critically, this daytime impairment is not merely a secondary “symptom of poor sleep”; rather, it functions as two distinct, clinically relevant factors: an active driver of metabolic disturbance, and a robust marker of the physiological dysregulation that underpins clinical insomnia. A study demonstrated that insomnia patients with severe daytime fatigue exhibited higher evening cortisol levels than those with mild or no daytime impairment.35 Beyond its physiological consequences, daytime impairment also exerts a direct influence on health-related behaviors. Specifically, it promotes the adoption of unhealthy behaviors, such as prolonged sedentary behavior and increased consumption of high-sugar, high-fat foods, both of which are independent risk factors for MS.36 Insomnia phenotype heterogeneity (eg, short sleep duration versus normal sleep duration) may provide another explanation for the inconsistency among different studies. To explore this possibility, we further analyzed the impact of insomnia with different sleep durations on MS, and the results remained negative (Table S6). However, our database only relied on self-report sleep data, and objective measurements such as polysomnography are needed to explore different dimensions in future studies. On the other hand, different symptoms of insomnia may also exert divergent trends; however, because of data limitations, we were unable to conduct an analysis of this aspect. Research is needed to explore this relationship in US Hispanic populations in the future.
In our analysis, we further found that COMISA had an even higher risk of incident MS than SDB and insomnia alone. As the two most common sleep disorders, about 28–49% of people with SDB have comorbid insomnia, and 29–51% of patients with insomnia also have SDB, worldwide.37 Multiple studies have confirmed the adverse effects of COMISA on several cardiometabolic diseases, including hypertension and diabetes,6,38–40 which are MS factors. A survival analysis using data from the Sleep Heart Health Study (SHHS) revealed that the presence of COMISA was associated with elevated rates of hypertension compared to individuals without insomnia or SDB.38 Through analysis of the HCHS/SOL cohort, Li et al6 demonstrated a significant association of SDB and insomnia with incident hypertension in the Hispanic/Latino population, and COMISA showed an even higher odds ratio for incident hypertension compared to SDB or insomnia alone. Previous research had already suggested a bidirectional relationship between SDB and insomnia,20 considering that they share risk factors and symptoms. Thus, these conditions may interact to exacerbate each other, leading to a synergistic impact on health impairment, including the development of MS. Although SDB is already regarded as a major risk factor for cardiovascular diseases, we cannot ignore the synergistic impact of insomnia and SDB. It is necessary to strengthen screening for COMISA.
In this study, we found that women had a higher risk of MS. This finding is consistent with a study that found a stronger association between SDB and MS in Hispanic/Latino women based on data from the first visit, although the prevalence of SDB was higher in men.18 A previous longitudinal study also found that SDB is independently attributed to diabetes and showed a more significant association in women. This may be because women undergo hormonal changes such as pregnancy, which may contribute to insulin resistance and obesity.41 The degree of obesity in women is often higher than in men with a similar severity of SDB,42 which may also influence the metabolic factors. Meanwhile, we cannot exclude the possibility that the damage from SDB in women is more severe than that in men. Our results also showed that COMISA is more significantly associated with incident MS in women. It has been proved that women with SDB have more insomnia-like symptoms,43 and such a phenotype is associated with a higher risk of cardiovascular disease.44 This is consistent with our study. Women with SDB usually have a lower AHI and atypical symptoms compared to men, leading to a seriously inadequate rate of diagnosis and treatment. Thus, it is important to improve screening and treatment for women with SDB in the Hispanic/Latino population.
We also found that, among SDB patients, only the younger group (<60 years) showed a significant association with incident MS. In a previous age-stratified analysis of SDB and cardiovascular risk in the US population, it was found that OSA, particularly in younger individuals, showed a significant association with increased incidence of hypertension, angina/angina pectoris, and overall cardiovascular disease prevalence factors,45 which are known risk factors for the development of MS. This may be related to a lack of appropriate screening and primary care, as SDB is commonly regarded as a risk factor primarily for older adults. These findings partly explain our results and also emphasize the importance of strengthening SDB risk screening in younger adults.
Furthermore, the interaction between obesity and SDB is significant, which means that the obese state plays an important role in the relationship between SDB and MS. That is, not only is obesity a risk factor for SDB, but individuals with obesity may be more likely to develop MS under the influence of SDB. We also conducted a mediation analysis and found that the mediating effect of BMI accounted for 62.1% of the outcome. This result suggests that obesity is indeed an important mediator in the development of MS caused by SDB, but the pathophysiological mechanisms of SDB itself should not be overlooked, as our results also demonstrate that SDB is an independent risk factor for incident MS, which is consistent with a previous meta-analysis.13 Previous research has also demonstrated that SDB is associated with incident MS, mainly through the mediation of nocturnal hypoxemia.19 This further clarifies the boundary of “obesity” in this process, emphasizing that the influence of obesity on MS does not completely obscure the independent association between SDB and MS.
Our research has several strengths, including the large sample of Hispanic/Latino people in the USA, the use of standard ARES and scale monitoring to diagnose SDB and insomnia in participants, and the determination of related complications through laboratory tests; and the use of standardized diagnosis criteria for MS. However, our study still has several limitations. First, a relatively high prevalence of obesity was observed in SDB, and this finding undoubtedly exerts a potential influence on the probability of being diagnosed with MS, given that obesity serves as both a key risk factor for SDB and a core diagnostic component of MS, creating inherent overlap between the two conditions. Although several rigorous strategies were implemented to mitigate this confounding effect, including multivariate adjustment, stratified analysis, and mediation effect models, certain limitations remain; for example, more precise metrics of adiposity, such as visceral adipose tissue area, were not incorporated owing to constraints in data collection. Second, the home sleep apnea test device (ARES) used in our study did not assess arousals or sleep architecture, which may lead to an underestimation of disease severity. This is due to the potential overestimation of sleep time and the failure to recognize hypopneas that are not associated with desaturation. Third, although Levine et al27 used WHIIRS to explore insomnia with incident hypertension and diabetes, WHIIRS still needs to be used with caution when interpreting insomnia in all populations, since it was derived from a group of women with a mean age of 62 years. In addition, WHIIRS assesses only night-time insomnia symptoms and does not capture daytime consequences such as fatigue, low mood, reduced energy, or impaired concentration, which may limit its ability to identify clinically significant insomnia. Fourth, although the analyses used prospective data and carefully controlled for potential confounders, the observational design of the study presents limitations. As such, it restricts our ability to fully explore potential mediating mechanisms, such as circadian disruption, diet, depression, and anxiety. MS assessment at two time-points precludes analysis of transitional metabolic states or the exact timing of onset. Future research is needed to explore the onset and progression of MS, as well as the effects of treatment and preventive measures such as CPAP. This will allow for a more precise understanding of the influence of sleep disorders on metabolic and cardiovascular risk in individuals.
In conclusion, our study demonstrated that SDB has a significant association with the development of MS. Moreover, COMISA has an even stronger association. This suggests that addressing sleep disorders, especially SDB and COMISA, could play a crucial role in both preventing and managing MS among the Hispanic/Latino population in the USA, and also indicates modifiable targets for clinical interventions.
Data Sharing Statement
The data used in this study are publicly available and can be accessed through the Hispanic Community Health Study/Study of Latinos. All data and materials supporting the results and analyses in this paper are available upon reasonable request to the corresponding author. Alternatively, the data may be accessed via https://biolincc.nhlbi.nih.gov/studies/hchssol/?q=hchs.
Ethics Statement
This study, which utilizes publicly available data, is part of the project titled “Coordinated collection of a multicenter clinical sample pool for insomnia disorder, narcolepsy, sleep apnea, and related data extraction”, approved by the Biomedical Ethics Committee of West China Hospital, Sichuan University (approval no. 2023(2357)). All participants provided informed consent prior to data collection, and the study adhered to the ethical principles outlined in the Declaration of Helsinki.
Acknowledgments
The authors thank the staff and participants of the Hispanic Community Health Study/Study of Latinos for their contributions. The HCHS/SOL is a collaborative study supported by contracts from the National Heart, Lung, and Blood Institute to the University of North Carolina (HHSN268201300001I/N01-HC-65233), University of Miami (HHSN268201300004I/N01-HC-65234), Albert Einstein College of Medicine (HHSN268201300002I/N01-HC-65235), University of Illinois Chicago (HHSN268201300003I/N01-HC-65236, Northwestern University), and San Diego State University (HHSN268201300005I/N01-HC-65237). The following institutes/centers/offices have contributed to the HCHS/SOL through a transfer of funds to the National Heart, Lung, and Blood Institute: National Institute on Minority Health and Health Disparities, National Institute on Deafness and Other Communication Disorders, National Institute of Dental and Craniofacial Research, National Institute of Diabetes and Digestive and Kidney Diseases, National Institute of Neurological Disorders and Stroke, National Institutes of Health Institution–Office of Dietary Supplements, and UC San Diego, National Institute on Aging (R01AG075758, R56 2-AG048642, RF1AG054548, RF1AG061022, RF1NS127266, R01AG061088, RF1AG077639). The funding agency had a role in the design and conduct of the HCHS/SOL; in the collection, analysis, and interpretation of HCHS/SOL data; and in the review and approval of this paper. The views expressed in this paper are those of the authors and do not necessarily represent the views of the National Heart, Lung, and Blood Institute; the National Institutes of Health; or the US Department of Health and Human Services.
Author Contributions
YMW: conceptualization, data curation, formal analysis, investigation, methodology, validation, visualization, writing – original draft. WQL: validation, supervision, writing – review and editing. XJF: validation, supervision, writing – review and editing. YZ: validation, supervision, writing – review and editing. XDT: validation, supervision, writing – review and editing. RR: conceptualization, validation, supervision, writing – review and editing. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Our work was supported by the National Natural Science Foundation of China (82170100, 82120108002, 82341249, 82170099).
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Eckel RH, Grundy SM, Zimmet PZ. The metabolic syndrome. Lancet. 2005;365(9468):1415–1428. doi:10.1016/S0140-6736(05)66378-7
2. Vaduganathan M, van Meijgaard J, Mehra MR, Joseph J, O’Donnell CJ, Warraich HJ. Prescription fill patterns for commonly used drugs during the COVID-19 Pandemic in the United States. JAMA. 2020;323(24):2524–2526. doi:10.1001/jama.2020.9184
3. Marin JM, Villar I, Forner M, et al. Association between treated and untreated obstructive sleep apnea and risk of hypertension. JAMA. 2012;307(20):2169–2176. doi:10.1001/jama.2012.3418
4. Reichmuth KJ, Austin D, Skatrud JB, Young T. Association of sleep apnea and type II diabetes: a population-based study. Am J Respir Crit Care Med. 2005;172(12):1590–1595. doi:10.1164/rccm.200504-637OC
5. Barros D, Garcia-Rio F. Obstructive sleep apnea and dyslipidemia: from animal models to clinical evidence. Sleep. 2019;42(3). doi:10.1093/sleep/zsy236
6. Li X, Sotres-Alvarez D, Gallo LC, et al. Associations of sleep-disordered breathing and insomnia with incident hypertension and diabetes. the hispanic community health study/study of latinos. Am J Respir Crit Care Med. 2021;203(3):356–365. doi:10.1164/rccm.201912-2330OC
7. Redline S, Sotres-Alvarez D, Loredo J, et al. Sleep-disordered breathing in Hispanic/Latino individuals of diverse backgrounds. The Hispanic community health study/study of Latinos. Am J Respir Crit Care Med. 2014;189(3):335–344. doi:10.1164/rccm.201309-1735OC
8. Cappuccio FP, D’Elia L, Strazzullo P, Miller MA. Quantity and quality of sleep and incidence of type 2 diabetes: a systematic review and meta-analysis. Diabet Care. 2010;33(2):414–420. doi:10.2337/dc09-1124
9. Zhan Y, Zhang F, Lu L, et al. Prevalence of dyslipidemia and its association with insomnia in a community based population in China. BMC Public Health. 2014;14:1050. doi:10.1186/1471-2458-14-1050
10. Peppard PE. Longitudinal study of moderate weight change and sleep-disordered breathing. JAMA. 2000;284(23):3015. doi:10.1001/jama.284.23.3015
11. Gami AS, Caples SM, Somers VK. Obesity and obstructive sleep apnea. Endocrinol Metab Clin North Am. 2003;32(4):869–894. doi:10.1016/s0889-8529(03)00069-0
12. Giampa SQC, Lorenzi-Filho G, Drager LF. Obstructive sleep apnea and metabolic syndrome. Obesity. 2023;31(4):900–911. doi:10.1002/oby.23679
13. Qian Y, Xu H, Wang Y, Yi H, Guan J, Yin S. Obstructive sleep apnea predicts risk of metabolic syndrome independently of obesity: a meta-analysis. Arch Med Sci. 2016;12(5):1077–1087. doi:10.5114/aoms.2016.61914
14. Iftikhar IH, Donley MA, Mindel J, Pleister A, Soriano S, Magalang UJ. Sleep duration and metabolic syndrome. an updated dose-risk metaanalysis. Ann Am Thorac Soc. 2015;12(9):1364–1372. doi:10.1513/AnnalsATS.201504-190OC
15. Zhang Y, Jiang X, Liu J, Lang Y, Liu Y. The association between insomnia and the risk of metabolic syndrome: a systematic review and meta-analysis. J Clin Neurosci. 2021;89:430–436. doi:10.1016/j.jocn.2021.05.039
16. Drager LF, Polotsky VY, O’Donnell CP, Cravo SL, Lorenzi-Filho G, Machado BH. Translational approaches to understanding metabolic dysfunction and cardiovascular consequences of obstructive sleep apnea. Am J Physiol Heart Circ Physiol. 2015;309(7):H1101–11. doi:10.1152/ajpheart.00094.2015
17. Van Cauter E, Knutson KL. Sleep and the epidemic of obesity in children and adults. Eur J Endocrinol. 2008;159(S1):S59–66. doi:10.1530/EJE-08-0298
18. Richard SL, Renn BN, Tran DT, Kim J, Feng D. Metabolic syndrome, modifiable lifestyle factors, and sleep-disordered breathing: the hispanic community health study. Ann Behav Med. 2024;58(3):179–191. doi:10.1093/abm/kaad071
19. Hirotsu C, Haba-Rubio J, Togeiro SM, et al. Obstructive sleep apnoea as a risk factor for incident metabolic syndrome: a joined Episono and HypnoLaus prospective cohorts study. Eur Respir J. 2018;52(5):1801150. doi:10.1183/13993003.01150-2018
20. Sweetman A, Lack L, McEvoy RD, et al. Bi-directional relationships between co-morbid insomnia and sleep apnea (COMISA). Sleep Med Rev. 2021;60:101519. doi:10.1016/j.smrv.2021.101519
21. Chen X, Wang R, Zee P, et al. Racial/ethnic differences in sleep disturbances: the multi-ethnic study of atherosclerosis (Mesa). Sleep. 2015;38(6):877–888. doi:10.5665/sleep.4732
22. LaVange LM, Kalsbeek WD, Sorlie PD, et al. Sample design and cohort selection in the hispanic community health study/study of Latinos. Ann Epidemiol. 2010;20(8):642–649. doi:10.1016/j.annepidem.2010.05.006
23. Sorlie PD, Aviles-Santa LM, Wassertheil-Smoller S, et al. Design and implementation of the Hispanic community health study/study of Latinos. Ann Epidemiol. 2010;20(8):629–641. doi:10.1016/j.annepidem.2010.03.015
24. Westbrook PR, Levendowski DJ, Cvetinovic M, et al. Description and validation of the apnea risk evaluation system: a novel method to diagnose sleep apnea-hypopnea in the home. Chest. 2005;128(4):2166–2175. doi:10.1378/chest.128.4.2166
25. Ayappa I, Norman RG, Seelall V, Rapoport DM. Validation of a self-applied unattended monitor for sleep disordered breathing. J Clin Sleep Med. 2008;4(1):26–37. doi:10.5664/jcsm.27075
26. Louis J, Auckley D, Miladinovic B, et al. Perinatal outcomes associated with obstructive sleep apnea in obese pregnant women. Obstet Gynecol. 2012;120(5):1085–1092. doi:10.1097/AOG.0b013e31826eb9d8
27. Levine DW, Kaplan RM, Kripke DF, Bowen DJ, Naughton MJ, Shumaker SA. Factor structure and measurement invariance of the women’s health initiative insomnia rating scale. Psychol Assess. 2003;15(2):123–136. doi:10.1037/1040-3590.15.2.123
28. Levine DW, Kripke DF, Kaplan RM, et al. Reliability and validity of the women’s health initiative insomnia rating scale. Psychol Assess. 2003;15(2):137–148. doi:10.1037/1040-3590.15.2.137
29. Coughlin SR, Mawdsley L, Mugarza JA, Calverley PM, Wilding JP. Obstructive sleep apnoea is independently associated with an increased prevalence of metabolic syndrome. Eur Heart J. 2004;25(9):735–741. doi:10.1016/j.ehj.2004.02.021
30. Xu S, Wan Y, Xu M, et al. The association between obstructive sleep apnea and metabolic syndrome: a systematic review and meta-analysis. BMC Pulm Med. 2015;15:105. doi:10.1186/s12890-015-0102-3
31. Framnes SN, Arble DM. The bidirectional relationship between obstructive sleep apnea and metabolic disease. Front Endocrinol. 2018;9:440. doi:10.3389/fendo.2018.00440
32. Troxel WM, Buysse DJ, Matthews KA, Kip KE, Strollo PJ. Sleep symptoms predict the development of the metabolic syndrome. Sleep. 2010;33(12):1633–1640. doi:10.1093/sleep/33.12.1633
33. Ju SY, Choi WS. Sleep duration and metabolic syndrome in adult populations: a meta-analysis of observational studies. Nutr Diabetes. 2013;3(5):e65. doi:10.1038/nutd.2013.8
34. Peila R, Xue X, Feliciano EMC, et al. Association of sleep duration and insomnia with metabolic syndrome and its components in the women’s health initiative. BMC Endocr Disord. 2022;22(1):228. doi:10.1186/s12902-022-01138-9
35. Dressle RJ, Feige B, Spiegelhalder K, et al. HPA axis activity in patients with chronic insomnia: a systematic review and meta-analysis of case-control studies. Sleep Med Rev. 2022;62:101588. doi:10.1016/j.smrv.2022.101588
36. Triplett OM, Morrell HER, Dyk TRV. Insomnia severity and obesity mediated by health behaviors in adolescents. J Pediatric Psychol. 2024;50(3):243–253. doi:10.1093/jpepsy/jsae098
37. Zhang Y, Ren R, Lei F, et al. Worldwide and regional prevalence rates of co-occurrence of insomnia and insomnia symptoms with obstructive sleep apnea: a systematic review and meta-analysis. Sleep Med Rev. 2019;45:1–17. doi:10.1016/j.smrv.2019.01.004
38. Lechat B, Appleton S, Melaku YA, et al. Comorbid insomnia and sleep apnoea is associated with all-cause mortality. Eur Respir J. 2022;60(1):2101958. doi:10.1183/13993003.01958-2021
39. Wu H, Guo Y. Risk of resistant hypertension associated with insomnia in patients with obstructive sleep apnea. Sleep Med. 2023;101:445–451. doi:10.1016/j.sleep.2022.12.001
40. Guo J, Redline S, Stone KL, Xiao Y. Redefining comorbid insomnia and sleep apnea: the association of sleep breathing impairment and insomnia with incident diabetes. Ann Am Thorac Soc. 2023;20(12):1791–1800. doi:10.1513/AnnalsATS.202302-171OC
41. Sivan E, Boden G. Free fatty acids, insulin resistance, and pregnancy. Curr Diabet Rep. 2003;3(4):319–322. doi:10.1007/s11892-003-0024-y
42. Bonsignore MR, Saaresranta T, Riha RL. Sex differences in obstructive sleep apnoea. Eur Respir Rev. 2019;28(154):190030. doi:10.1183/16000617.0030-2019
43. Anttalainen U, Grote L, Fietze I, et al. Insomnia symptoms combined with nocturnal hypoxia associate with cardiovascular comorbidity in the European sleep apnea cohort (ESADA). Sleep Breath. 2019;23(3):805–814. doi:10.1007/s11325-018-1757-9
44. Saaresranta T, Hedner J, Bonsignore MR, et al. Clinical phenotypes and comorbidity in European sleep apnoea patients. PLoS One. 2016;11(10):e0163439. doi:10.1371/journal.pone.0163439
45. Strenth C, Wani A, Alla R, Khan S, Schneider FD, Thakur B. Obstructive sleep apnea and its cardiac implications in the United States: an age-stratified analysis between young and older adults. J Am Heart Assoc. 2024;13(12):e033810. doi:10.1161/JAHA.123.033810
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.